Like other coronaviruses, this virus predominantly affects "Over 50" age category and might speed up death for those who have
other serious conditions.
As of April 5, 2020 COVID-19 deaths currently does not distort the statistics of death in the USA as the number of death from the
virus is still statistically insignificant . So the question arise, why such drastic measures were taken outside known hot
spots such ad New York metropolitan area. It might make sense to classify regions into three category "high risk (hot spots),
medium risk and low risk and treat them differently.
Another question why politicians like Cuomo overhype the treat and want tremendous amount of ventilators. Ventilator treatment will
not make a survival difference to patients who are frail and that's the majority of COVID-19 patients. Typically around 50% on those
who were put on ventilator dies while on ventilators (Mortality
rate of COVID-19 patients on ventilators Physician's Weekly .) For those who survives signicant percentage will die too. As
of Apr 5 there were only 38K hospitalized patients in the USA. Why Cuomo wants another 40K ventilators is a little bit unclear. Peak
ventilator use is predicted to be 19,481 (95% UI 9,767 to 39,674) ventilators
(https://gineersnow.com/industries/medical/forecast-deaths-hospitals-ventilators-covid-19-impact-usa )
"What the authorities know that a regular overseer of events don't?
Peak ventilator use is predicted to be 19,481 (95% UI 9,767 to 39,674) ventilators. The mortality figures from the Italian health ministry certain are surprising to say the least, and not in a way that support the
MSM hysteria on this.
That suggests that the data we are getting from MSM is incomplete, hyped (especially about R0 and mortality) and does
not allow to objectively size the treat. Only very crude numbers of cases and deaths are available and very little information about
testing rates, pre-conditions for development of pneumonia (smoking and poor air quality are two factor suspected but
nothing definitive known), very limited information is provided about the average ages of people who is being hospitalized (probably
over 70), and especially those in intensive care. The question is who is dying from it ?
One important finding from the China study that is ignored by neoliberal MSM is the near absence of cases among children. The
10-19 age bracket comprised only one percent of all infections, and a single death. Children under 10 made up less than one percent,
with no deaths reported
Joseph Stalin once said �a single death is a tragedy� and �a million deaths is a statistic.� The observation was chilling because
it has a grain of truth about how we process tragedies. The same is sometimes true legally. If a government kills one person, it is
a murder.
In no way the Coronavirus death statistics are reliable. One of the big problems is the reliability of the data. To figure
out a death toll you need to estimate how many people have the virus, and how many people died as a result. Both of those are very difficult
problems, the first because testing is spotty and carries inherent systematic error. The second because of comorbidities and the possibility
of attributing deaths from other viruses to this one. Accounting trick of assigning every death with a positive test to COVID-19 has,
effectively, reassigned normal (cancer, diabetes, etc.) deaths to COVID-19.
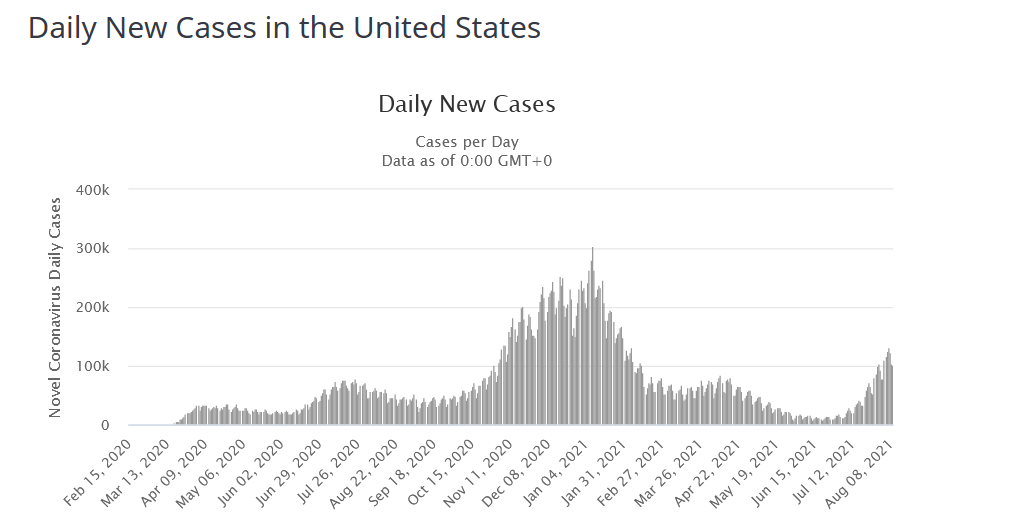
The best way to estimate if a new disease is a significant danger is to compare death rate with the previous year (or average
of 10 previous years) for a week or month with the current. For GB and Italy based on this metric increase of mortality caused by COVID-19
is statistically insignificant:
But it is clearly looks like the amount of hysteria and panic is utterly disproportionate to the number of deaths. For this amount
of panic I would expect hundreds of thousands of dead in the USA alone. Note that over 200K Americans die each year of preventable medical
error. Does anyone panic about that, even though many of those errors are far easier to eliminate than a virus?
First of all it looks like that are at least two stains of this virus with different morality: S and L.
Second, the fact that swab tests produce a lot of false positives complicates correct estimation of mortality ? In any case
what is measured is the mortality among tested patients, which is always higher then that mortality among infected patients, because
outside cruise ships not all people are tested.
But the most important issue is that most countries include in COVID-19 death statistics all deaths "with the virus" along with all
deaths "from the virus" The best definition would be: novel coronavirus antibodies test positive (proof of recent infection) plus
ARDS (radiologically, if not pathologically, confirmed).
This happens because the majority of diseased patients are old and have at least one life threatening medical condition and virus
was just the last straw that broke the camel neck. "Real" deaths from virus are deaths from virus pneumonia. They are probably a small
fraction of the total deaths, as deaths are heavily biased toward older (over 70) population.
It seems hard to get any hands on this. It�s like a greased pig.
Again, there are very strong reasons to suspect that neoliberal MSM are deceiving us and the mortality figure promoted by MSM are
over inflated: Patients who have been tested for SARS-CoV-2 are disproportionately those with severe symptoms and bad outcomes. Projecting
the Diamond Princess mortality rate onto the age structure of the U.S. population, the death rate among people infected with Covid-19
would be 0.125% (statnews.com):
That raises question what if majority whose who died, died of the coronavirus have such serious medical conditions that the
coronavirus just was the last straw that broke the camel back and flu would do for them the same. In other words the number
of deaths can well be pure hype and the real mortality from this virus is close to mortality from a severe epidemic of the seasonal
flu.
It looks like there are two main mutations of this coronavirus: "L" and "S". The L is more common (especially in the USA) and
the S (Wuhan mutation) is more lethal. All-in-all there are around two dozens of mutation (Chinese figures)
Symptoms vary. Slightly elevated temperature and early development of dry cough are two more typical symptoms. If shortness of breath
is present this is a real warning sign. Loss of smell is a very important symptom and usually means that the patient is infected.
In France they do not even test such people. Those two presentation gives you general information about symptoms:
Three typical symptoms include a slight fever (99-102F, around 98% of patients), dry cough (60% of patients), fatigue (90% of patients).
Shortness of breath (labored breathing) allow to distinguish severe form from mild form of the disease and means that lungs are affected
Symptoms usually appear 2 to 14 days after you�re exposed to the virus (incubation period). Some of the less common symptoms
include muscle pain, vomiting, abdominal pain, headache, dizziness and nausea.
Less the a third of patients difficulty breathing, and it takes about five days (on average) for a patient to have difficulty breathing
after first showing symptoms. This probably suggest
pneumonia .
There are several YouTube presentations of various quality that might help to understand this disease, for example:
Several symptoms associated with common colds � such as a headache or sore throat � were seen in only a small number of cases.
Typically symptoms are evident on the fifth day of the disease or earlier. Most people recover in 3-4 weeks. Recovered people are
immune to the disease.
Historically only around 14% of COVID-19 infections show severe symptoms (which means cases that they require medical attention and
prescription drugs.) Some cases are without symptoms. Here are the currently available historical data for the sample of 44 415 cases:
The main sophisticated feature this virus is that it spread from infected people which show little or no symptoms of the diseases
(during incubational period) which is typically from five to seven days with the longest period being 14 day (What
Doctors Treating Covid-19 in Wuhan Say About The Virus - Bloomberg , Mar 5, 2020):
Cynically speaking "this pandemic is nothing to worry about for people of breeding age. If anything, it will reduce long term health
care costs by running through the old people." (comment
onunz.com )
Effects of COVID-19 are similar to OC43 (one of four other mild coronaviruses probably responsible for 25% of all �common colds�,
which causes 15% severe cases and 0.2% fatal cases). As Marc Lipsitch, an infectious disease epidemiologist at Harvard�s T.H.
Chan School of Public Health
points out ,
deaths are the most obvious and easy thing to catch, whereas infected people who stay at home and those with no symptoms are incredibly
hard to account for. That tends to skew the fatality rate higher, especially earlier on in an epidemic.
The path of spreading currently is not very clear but probably include both droplets and infected surfaces (shopping cart handles,
any ATM or payment device, parking meters) ... and then touching your nose eyes, and face in general:
Median time for recovery is one month. Observed susceptibility is abound 20-60% of population. Which means
that 40 to 80% of population are immune and is not getting sick after contact with s sick person (worst case was Wuhan personnel where
60% got infects; the other worst case scenario was Diamond Princess cruse chip where only 20% got infected).
The main danger is traveling with the infected person and living in the same household. In households children are as likely to be
infected as adults.
Also some percentage of infected people never show any symptoms and the majority (over 80%) of cases never show symptom worse than
a typical flu and continue regular life routine. That creates preconditions for a rapid spread of the disease and converting it into
pandemic. In countries like the USA the situation is worsened by neoliberals cruel treatment of workers and lack of sick leaves (Wal-Mart
and other retail giants ) , when people are often forced to work with flu like symptoms, this spreading the disease both at work and
during the commute, if the use public transportation. Those greedy bastards from Wal-Mart merge sick leaves with vacations (which are
also not easy to get from mangers) [Slate [.
Part time workers which are now substantial and growing part of the workforce are often work on really slave conditions, without
any vacations of pay leaves. There is no national paid leave policy in the USA, making it in this respect a third world country.
The most typical complication is bacterial pneumonia which is often deadly for older people and people with weakened immune system
( lasts from 6 to 41 days since admission for fatal cases):
Without complication the symptoms of the flu disappears in approximately two to four weeks (four to six weeks if we count incubation
period). Like typically for coronavirus recovery includes a period of severe cough. That's a typical scenario for most healthy people.
In this sense, it is nothing more then highly infectious seasonal flu. Like is the case with all influenza viruses mortality is higher
in older population. China's CCDC found that the virus has the highest fatality rate around 15% for people aged 80 or older with co-occurring
medical conditions.
So only for seniors it does represent a "clear and present danger" (with mortality reaching 8.0% for people over 70 I am a little
bit concerned about Democratic Candidates in this sense ;-). But such mortality in not atypical -- such people usually have a couple
of chronic diseases which make the prognosis far worse.
Chances of complication are lower for people without chronic diseases, and people living outside densely populated and heavily polluted
cities. As this virus can be called "virus pneumonia" it is more dangerous for males. So far we have 2.8% vs. 1.7% morality for make
and female, correspondingly. In a sense virus has clear feminist bias.
In any cases mortality for this virus for people below 80 is in single digits ( and on average does not exceed 2 to 3% or approximately
25 times higher then seasonal flu: nearly 1800 people have died for over 70,000 have been infected ). The most compressive data about
the epidemics I found do far are provided in the following discussion in Quora
How serious is the 2019�20 Wuhan coronavirus
- Quora which I encourage to read in full. It does provides a lot of interesting data.
Young and healthy people, meanwhile, typically experience mild flu-like symptoms (some infected people do not display any symptoms
-- asymptomatic cases -- dangerous because they still spread the virus) and are not in danger, according to
the BBC . WHO recently stated that the virus manifests
as only a minor infection in four out of five people who contracted it , according to
the Guardian.
The most cruel natural experiment with the virus was its spread the Diamond Princess cruise ship (closed space, high level of contact
between passengers, lack of qualified medical personnel and supplies, etc) Six people died (0.2% mortality) and around 700 people were
infected out of 3700. For all other the immune system managed to kill the virus. Which suggests susceptibility rate of around 20%.
One of the defining feature of this virus is high infection rate of people who came into a contact with the virus. But even in this
area while the virus is dangerous and protective measure were not taken, it is not catastrophically so.
We can view the epidemic on the Diamond Princess cruise ship as the worst case scenario (with much older then the average population;
very close contact with infected people of the rest population of the ship via common areas) ended
Patients are generally given supportive care for their symptoms, such a fluids and pain relievers. In acute cases hospitalized patients
may need oxygen to support breathing.
Patients are still prescribed existing antiviral drugs which have shown their effectiveness. The main treatment is aimed at reducing
the severity of symptoms and is similar to the treatment of traditional seasonal respiratory diseases, but the course of the duration
of the disease (with acute period typical for many virus infection around seven days) and the speed of the recovery after it depends
on the strength of the individual's immune system.
Planning is the most important aspect of the virus response, and countries need to know ahead of time how they are going
to handle each patient entering a fever clinic, detect suspected cases, confirm if they have the virus in labs and isolate possible
cases. For old people around 15% of cases advance to pneumonia, and it could be really bad
As old patients are the most severely affected and tend to overburden the local hospitals, the imposition of a voluntary quarantine
on retired population in areas of active spread of infection is a sound measure. Two Japanese passengers - an 87-year-old man and an
84-year-old woman - were the first to die from the disease on February 19 pm Daemon Princess cruise ship. In the USA out six deaths
at least four have been among residents of a long-term care facility called Life Care Center, where more than 50 residents and staff
members had shown symptoms of the virus.
Coronaviruses do not have such a very high infection rates and typically epidemic is limited to the spring season and subside in
summer. So epidemic last three-five months. But the period from infection to first symptom can last a week during which the person possibly
can infect other people creating an illusion of high infection rates. The fact that the virus can be infectious even during the
incubation period has not been proven
Currently patients are recommended to take medications that are prescribed for the prevention of seasonal respiratory virus infections.
These are medications that produce endogenous interferon.
If coronavirus COVID-19 is like other Coronaviruses it probably, like President Trump suggested, will �go away� in April, as temperatures
increase and there will be a lot of sunny days. So far is did not reach the size of a typical flu epidemic with 8,000-plus deaths in
US alone.
Most Coronaviruses are seasonal, but there was an outbreak in Dominical Republic resorts in summer 2018 which was atypical. So it
it�s not yet clear if the new virus will follow the same pattern � and experts caution against banking on the weather to resolve this
outbreak (Will the New Coronavirus
'Go Away' in April - FactCheck.org )
Per country, currently the worst mortality was observed is 4.4% (Iran.) but that only can means that the number of cases are
underreported or there are many cases that are asymptomatic and not included in statistics. For the graphic map, see
First of all, there is no reasons to panic. This is not another Black Death epidemics. Far from it. It looks like healthy people
younger then 60 have little to fear but fear itself. Outside New York metropolitan area (and selected hot spots in other large cites)
chances to get pneumonia are approximately the same as to get into serious auto crash. Children are rarely infected and typically are
infected in family not in school setting:
The main mechanism of transmission is religious congregations, meetings and conferences as well as intra-family transmission.
With minimum precautions chances to get infection in public transport (wearing mask in obligatory safety measure) and office are
minimal. Transmission "hand to nose of eyes" can be effectively blocked with soup and hand sanitizers. Most shops now offer
iether sanitizer or wipes as a courtesy for customers.
But fear is addictive and it looks like panic, including panic buying had spread in the USA, fueled by irresponsible MSM fearmongering.
For example, reporting deaths from the virus neoliberal MSM do not split it by age groups as this would decrease the level of fear in
the population ( and their profits ). In reality only severe and critical cases (when a patient develops virus pneumonia) matter.
All other cases should be treated like flu cases are treated. Mortality for this virus is highly age dependent. This coronavirus
pandemic is no nothingburger, it is a flu-epidemic-level spike in death of the elderly and infirm.
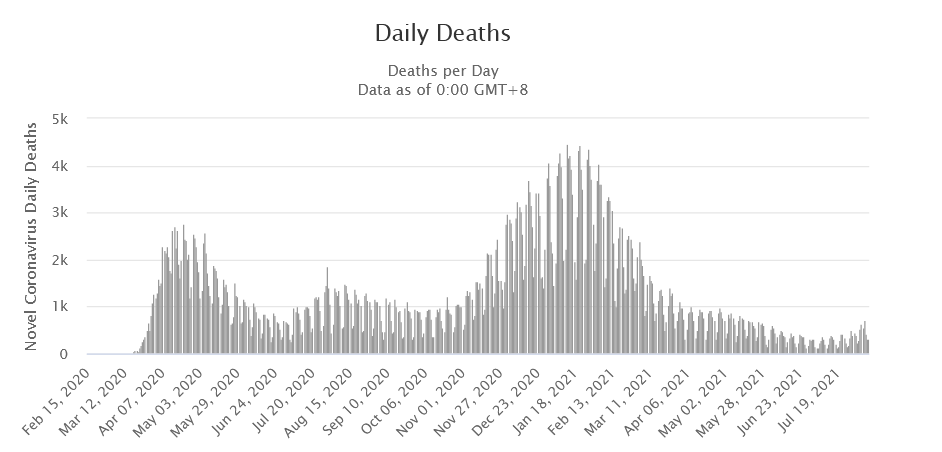
Another dirty trick that MSM resort to inflate panic to report just the number of death from the virus, not the deviation from
the average number of deaths for a week or a month or so artificially increases panic. Around 8K people dies in the USA any particular
day without any epidemic. So far maximum deviation from average mortality in any particular day of this epidemics was less then
20%. In many countries (including EU and GB) average weekly mortality is down not up.
Panic and fear artificially incited by neoliberal MSM are also amplified by cowardice to face the risks immanent in any epidemics
(as well as driving the car) is doing more damage than the disease itself. They provoked the wave of panic hoarding in the USA
which started in February with isopropyl alcohol and hand sanitizer (which in early March reached $60 for 8 ounces bottle on Amazon
;-) As of March 16 it is still in full force with empty shelves in supermarkets as it gradually spread starting from March 10 to many
other products categories including paper towels, bathroom tissue, all types of sanitizers and non perishable food. Especially puzzling
and irrational is hoarding bathroom tissue.
Sometime neoliberal MSM coverage of epidemics looks like a complete 100% departure from reality. More people will die in Yemen
and Syria each day going forward, and no one cares. Many old people will serious chronic condition who are die from coronavirus induced
pneumonia would die from flu induced pneumonia the same year as they are too weak to resist even flu. Winter is a very bad season
for such people in any case.
Of course, another extreme is fatalism as expressed by Paul Bogdanich in his post at
moonofalabama.org (Mar 11 2020 )
And unlike fatalists thinking, we do not need to apply to our life the moral metrics which are appropriate only to communities who
live on a verge of survival. Loosing some part of annual national income to save lives via quarantine is affordable. Mass testing is
a sure way to improve cost efficiency of quarantines and similar measures during virus epidemics. Retired people can and should stay
home and avoid situation where they can catch the infection. Reckless behaviour during virus epidemics is a crime and need to
be punished appropriately.
But it is true that the panic can do more damage than the virus itself. And that we need an objective perspective to access the level
of threat inherent in this virus epidemics. In the USA a reasonable threshold for classifying the treat as serious are probably
events that exceed car fatalities. In 2016 National Highway Traffic Safety Administration (NHTSA) registered 37,461 killed, an
average of 102 per day.
We are still in single digits of victims per day with COVID-19. It did proved high infectious. But there is highly infectious and
highly deadly pathogens are two distinct group that do not mix. It is as if viruses need to make choice between high mortality
and high transmission: viruses that kill their host, before the host infects others, die with the host and this can't kill many
hosts without eliminating themselves as well.
With this coronavirus, there seems to be a larger then usual window (aka incubation period) during which a person can be infected
and transmitting the virus, without having symptoms. In a way this is a rather "clever" virus. But long incubation period does not eliminates
biological reason why highly infectious viruses should evolve to become less deadly in order to succeed.
While the US government of Mar 13 declared the coronavirus a US national emergency and offered $50 billion for support of state
and local governments to fight the virus with FEMA, additional measures will not have an immediate effect. But they will
definitely slow down the spread of virus "flattening" the epidemics curve and this allowing more patients to survive.
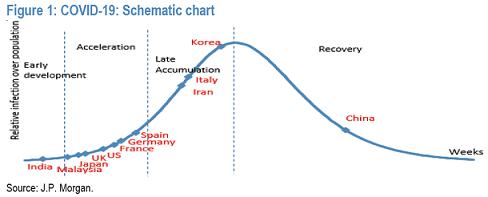
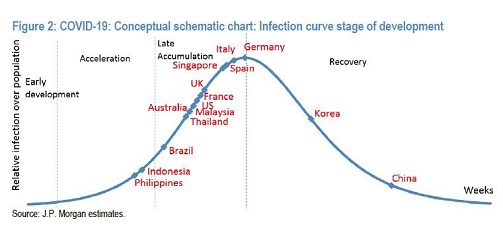
The current dynamic of epidemic in the USA and the world so far is exponential growth of cases with most infections clustered in
just half-dozen countries. Which is typical for an early stage of virus epidemic. Excluding China which now is past its peak and
is in decline, the other fastest growing hotspots are Italy, Iran, Spain and France. As of Mar 10, 2020 in the USA -- only three
states -- Washington State, New York, and California have over 100 cases
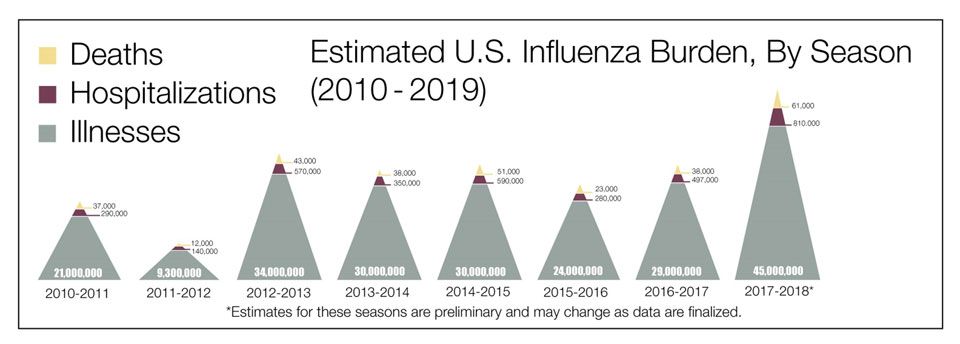
A typical flu epidemic in the USA infects tens of million people and cause approx
20-50K fatalities per year (somewhere
between 0.1% and 1%) but does not create any headlines in neoliberal MSM. According to the CDC�s weekly US flu report of
February 22, 2020,
For comparison the mortality rate in South Korea, where more than 1,100 tests have been administered per million residents, comes
out to just 0.6% and concentrated in the old and/or with chronic conditions. In view of USA media hysteria about Coronavirus COVID-19,
we need to concentrate on facts, not fears. Here is
Craig Murray comparison with the Hong Kong flu pandemic of 1968/9:
Masks are less useful as a protection, but they are very useful for preventing people with no symptom infecting others. Most surgical
masks are too loose to prevent inhalation of the virus. But they diminish the number of infected droplets you inhale (with proper fitting
and during initial hour or two substantially), and do prevent you from touching your nose, and for many people that alone is a valuable
service.
So wearing one is an important service to other people: if you are infected but has no symptoms that helps to prevent infecting others.
In areas where there are active cases such as NYC or Seattle wearing masks is a necessary and useful precaution.
The most effective are the so-called N95 masks, which block 95 percent of very small particles.
Also the dynamic of the disease might be different and more severe if the virus initially gets directly in lungs then when it initially
infect via other parts of the body.
As they can prevent you from passing along any infection wearing masks in public places need to be mandatory. Masks can be
reusable as to provide disposable masks for all population is a difficult and resources consuming task. You can wash them.
Detergent and hot water kills the virus instantly.
The advice to avoid masks outright is wrong. There is a place for them, but of course they�re just not a panacea. And it true that
if used improperly without washing/rubbing with alcohol your hands after removing they may actually increase your risk. The general
problem is that is difficult to follow a proper "decontamination procedure" or what you do when you replace the mask with a new one
or remove it completely create substantial burden on people and that means that few will be following it.
Also the period during which a single mask is effective is limited to approx two hours or so (enough for commute and shopping).
After this period expire it needs to be disposed or disinfected (soap or soaking in 40% or higher alcohol mix is enough
to kill all bacteria/viruses)
In the USA epidemic started much later then in China (in late February, instead of November or early December in China) and as such
closer to warm season, which should probably make it less severe. Every industrialized country in the world probably had been studying
coronavirus after MERS and SARS. Some purely to defend against outbreaks, others to weaponized it. So a lot of information was available
and some of it was used.
China made a few missteps at the start so its doubtful they knew what they were dealing with at the start other having a sudden batch
of pneumonia due to a new virus. They reacted the same as any rational well organized country would react.
The USA started with full information about the virus and still CDC managed to botch production of test kits, which definitely made
the epidemics more severe as fewer infected people were detected at early stages. Also travel restriction were ad hoc (compare
with Israel mandatory 14 days quarantine for all air passengers)
Deaths from is mostly limited to people with pre-existing health problems for whom pneumonia is deadly.
If we compare with the SARS coronavirus, which caused an outbreak of SARS in 2002-2003, we can state the its mortality rate
of this new coronavirus is much lower. 17 years ago, the mortality rate from SARS was about 10%.
According to the South China Morning Post, the first case of someone suffering from what later came to be known as Covid-19
occurred in China on November 17. The number of cases
grew in December,
with the majority cases in Wuhan . The Chinese
informed the World Health
Organization of new pneumonia cases of unknown etiology on Dec 30, 2019. This is the 1st mention of the coronavirus before they knew
what it was, from Reuters.com, Dec 30 2019:
Later they established that four of the five initial patients that they managed to trace have no contact with the wet market
(which since was demolished). While the market was the first 'cluster' of cases it was not the source of the outbreak. Some suggest
that the virus may originate in the USA:
In China solidarity and nationwide effort, including sending medics to Wuhan, played an important role in eradiating the epidemic:
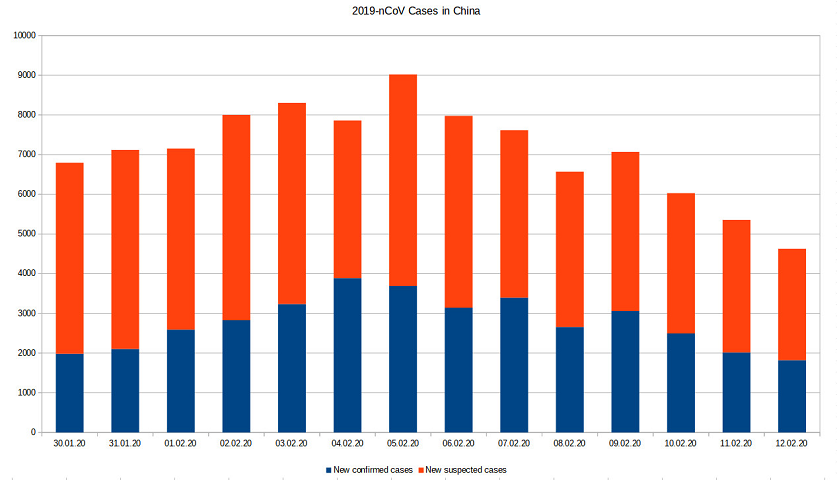
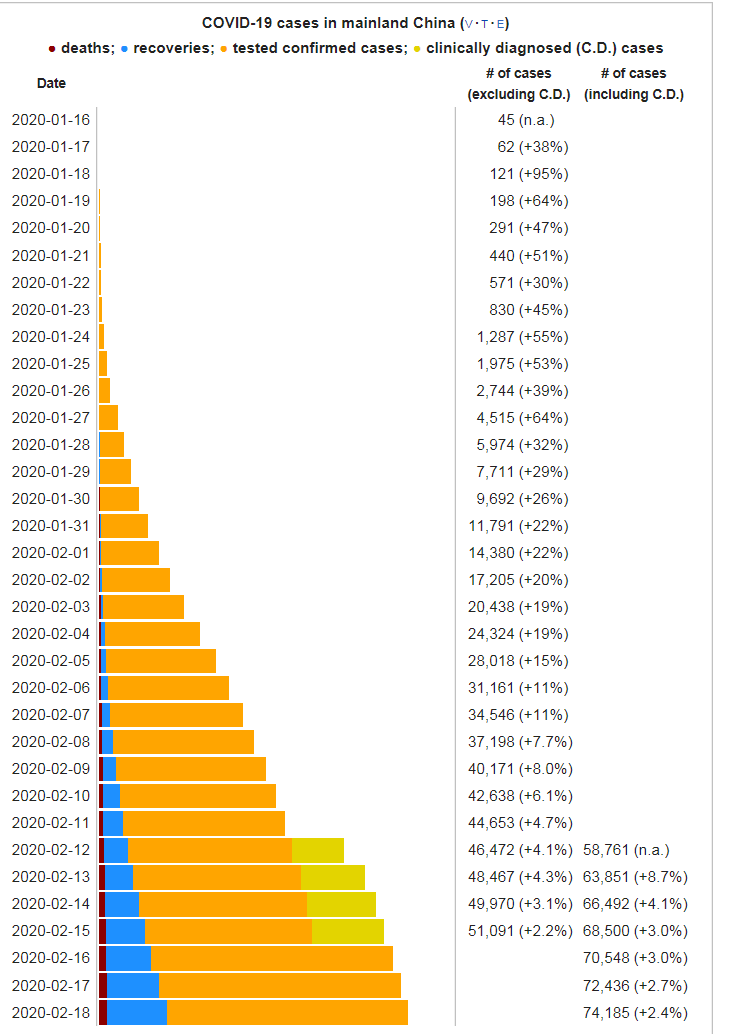
As of February 15, 2020 (01:30 UTC), there were 67K confirmed cases of infection, of which 66K were within mainland China.
After that epidemics quickly dissipated with less then 200 cases a day reported recently
Wuhan is eleven million city and it has less then 100K cases as of Feb 2020 (approximately two months after the epidemics started;
it started with zero protective measures in place and run wild probably for a month or so ), so we should probably have hope to survive
;-)
On Mar 17 Washington Post reporter based in Peking provided the first-hand evidence that life in Peking is returning to normal. Restaurants
have reopened.
Sept. 7, 2019)
The early symptoms include fatigue, nausea, vomiting, coughing and fever, escalating to shortness of breath, which can become
so extreme it can prompt an emergency room visit or require hospitalization. Some patients have needed supplementary oxygen, including
a ventilator in as many as a third of cases
analyzed in The New England Journal of Medicine. On lung scans, the illness looks like a bacterial or viral pneumonia that has attacked
the lungs, but no infection has been found in testing
May be smoking e-cigarette makes people especially vulnerable to some early COVID-19 strain (there are around seven strains of this
virus, some more lethal then others).
May be smoking makes people especially susceptible to COVID-19 pneumonia. That means that one of the first thing to do
is to stop smoking
As NYT reported "The Centers
for Disease Control and Prevention and state agencies have reported 2,506 lung injury cases that required hospitalization
and 54 deaths linked to vaping." but those infections were concentrated on young population, typically less then 35
years old:
Patients with vaping-related lung injuries typically show up in emergency rooms with shortness of breath after several days of
symptoms that resemble flu or pneumonia.
Like COVID-19 this also was global epidemic with cases in United States, Canada, Europe, Australia, India (2019�20
vaping lung illness outbreak - Wikipedia ):
Though this is the first time that vaping products have been linked to an outbreak of lung illness, at least 19 cases of vaping-associated
pulmonary injuries had been reported worldwide prior to 2019. The first case of
e-cigarettes inducing lipoid pneumonia was documented
in the medical literature in 2012, though the causative agent was identified as
glycerin , not vitamin E acetate.
...News media featured hospitalized lung vaping illness patients in narratives including the following:
Vomiting, coughing up blood, and lipoid pneumonia
Nausea, chest pains, and shortness of breath, and acute respiratory distress syndrome necessitating
extracorporeal membrane oxygenation
(ECMO)
Shoulder and back pain, double lung collapse
Vomiting, fever, sweating, painful coughing, bronchitis ,
double
pneumonia in a patient who had vaped THC
Vomiting up food, oil and water in the lungs, requiring supplemental oxygen for daily activities
Severe pain in the side, lung collapse, "black spots" on the lungs in a patient using about half a
Juul mint pod a day for about 18 months.
Chest and back pain from recurrent pneumothoraces
(air in the chest outside the lungs)
Trouble breathing, necessitating a ventilator
and medically induced coma. The 18-year-old patient says she bought vaping products from a
smoke shop that did not ask for her
ID card , enabling her to lie that she was 22.
Dizziness, vomiting, abdominal pain, difficulty breathing, necessitating supplemental oxygen.
Breathing problems mistaken for the flu or stomach
virus , eventually requiring ECMO
Difficulty breathing, requiring supplemental oxygen and steroids, diagnosed as
popcorn lung .
Dizziness and vomiting, problems breathing diagnosed as
pneumonitis
Patient discovered unresponsive in bedroom, mucus and blood coming from lungs,
cardiac arrest
Double lung transplant for a
17-year-old from Michigan on October 15, 2019, believed to be the first such procedure due to vaping
Misinformation and fearmongering from MSM and online sources about the coronavirus get is new term from the WHO -- an "infodemic"
(Wikipedia ):
On 2 February, the WHO declared there was a "massive infodemic" accompanying the outbreak and response, citing an over-abundance
of reported information, accurate and false, about the virus that "makes it hard for people to find trustworthy sources and reliable
guidance when they need it ."
The WHO stated that the high demand for timely and trustworthy information has incentivised the creation of a direct WHO 24/7
myth-busting hotline where its communication and social media teams have been monitoring and responding to misinformation through
its website and social media pages
Some members of alternative press such as
Zero Hedge (who probably act as a short sellers) also are guilty is spreading the hysteria.
The main concern is that the epidemic might lead to the economic downturn. Also it generated a wave of xenophobia. As Wikipedia states
"Xenophobia and racism against people of Chinese and East Asian descent have arisen as a result of the outbreak, with fear and hostility
occurring in several countries."
In reality this new type of coronaviruses has the average mortality around 1%. So the threat for the population is low.
LISTEN CBC Radio cuts off expert when he questions Covid19 narrative � OffGuardian
CBC Radio � Cross Country Checkup, March 15 2020
Duncan McCue (DM, Host): Dr Joel Kettner is on the line from Manitoba. Hi, Dr Kettner welcome to Checkup.
You teach at the University of Manitoba and are former Chief Medical Officer of Manitoba, I understand. So what do you think of how
we are coping right now?
Dr Joel Kettner (JK): Well I don�t know what to think, frankly, but I�ll tell you what I do think. First, I wanna
say that in 30 years of public health medicine I have never seen anything like this, anything anywhere near like this. I�m not talking
about the pandemic, because I�ve seen 30 of them, one every year. It is called influenza. And other respiratory illness viruses,
we don�t always know what they are. But I�ve never seen this reaction, and I�m trying to understand why. I have to say that I really
feel for my colleagues that are in public health practice. it is easy for me to sit in the armchair of my office and look at this
and observe it, and be critical and have ideas. But I really feel for them for three reasons.
One is that the data they are getting is incomplete to really make sense of the size of the threat. We are getting very crude
numbers of cases and deaths, very little information about testing rates, contagious analysis, severity rates, who is being hospitalised,
who is in intensive care, who is dying, what are the definitions to decide if someone died of the coronavirus or just died with the
coronavirus.
There is so much important data that is very hard to get to guide the decisions on how serious a threat this is.
The other part is we actually do not have that much good evidence for the social distancing methods. It was just a couple of review
in the CDC emerging infectious disease journal, which showed that although some of them might work, we really don�t know to what
degree and the evidence is pretty weak.
The third part is the pressure that is being put on public health doctors and public health leaders. And that pressure is coming
from various places. The first place it came from was the Director-General of the World Health Organization (WHO) when he said
�This is a grave threat and a public enemy number one� , I have never heard a Director-General of WHO use terms like that.
Then when he announced the pandemic he said he was doing it �because of a grave alarming quick spread of the disease and an
alarming amount of inaction around the world� that puts a huge pressure on public health doctors and leaders and advisors and
huge pressure on governments and then you get this what seems like a cascade of decision making that really puts pressure on the
countries and governments � provincial, state � to sort of�to keep up with this action that Dr Hoffman [an earlier guest on the programme]
said that we are trying to avoid, or should avoid, which is an overreaction. I don�t know what is an appropriate reaction, but
I do know that I am having trouble trying to figure this out and I�
[INTERRUPTED BY HOST]
The 2003 SARS outbreak, about which there was a similar panic, apparently ended up killing primarily East Asians.
This virus is different. First of all it origin in unclear. the The patient number 1, the person who first carried the virus, has
not been found. Several early paciets that Chinese authorities managed to trace have had no contact with Wuhan market.
Myth:
The novel coronavirus SARS-CoV-2 is a Chinese virus that comes from bats. It infected people because Chinese people eat bats.
Facts:
The source of the virus is actually not known. The patient number 1, the person who first carried the virus, has not been found.
The Wuhan wet market where exotic animals are sold
was not the source of the outbreak:
Our brave neocon Secretary of State accused China that it did not notified the USA promptly enough. That move backfired in
his face:
vk | Mar 19 2020 14:22 utc
26
China
rebuts accusation of cover-up, says it first notified U.S. of coronavirus on Jan. 3
Now we know whose government covered up the epidemic for two months...
Jackrabbit
29
While origin is an open question(*), USA response to the virus raises appears to be calculated and self-serving.
The Empire Games Covid-19
===
* I haven' seen anyone dispute China's claim that USA has 5 strains and therefore must be the source.
!!
Those media that are exaggerating the outbreak and trying to dramatize the situation are plainly selfish and immoral. Now is the
time to help China not to blame its government. Here is one comment from the Moon of Alabama blog on the topic:
SCMP constant China bashing...
https://www.scmp.com/news/china/diplomacy/article/3071170/coronavirus-will-ultimately-strengthen-xi-and-chinese
What's Happening with Coronavirus (YouTube)
https://www.youtube.com/watch?time_continue=137&v=QW0Q8cSBpUA&feature=emb_logo
"Jude Blanchette, who holds the Freeman Chair in China Studies at the Center for Strategic and International Studies (CSIS)
in Washington."
The above idiots, yes Idiots> (Blanchette and Stephen Morrison) not only ignorance but behind time...
Posted by: JC | Mar 6 2020 4:40 utc |
49
Reaction on the USA MSM on COVID-19 epidemics in China suggests that this incident was used as a start of a anti-China propaganda
campaign, explaining pre-existing China-gate propaganda. Similar to Russiagate. With the draconian measures already taking and the daily
increase of cases less 3% some expect already start doubting that travel restrictions continue to make sense post February, 2020. World
Health Organization Director-General Tedros Ahanom Ghebreyesus declare in mid February that he personally opposes travel bans. Zero
Hedge quoted him in its article the following way:
�We reiterate our call to all countries not to impose restrictions that unnecessarily interfere with international travel and
trade. Such restrictions can have the effect of increasing fear and stigma, with little public health benefit.�
The Quartz story by Youyou Zhou adds to that the opinion of another expert -- Scott Gottlieb, former head of the US Food
and Drug Administration [US
citizen dies of Wuhan virus in first confirmed non-Chinese fatality , , Quartz, February 8, 2020]:
Scott Gottlieb, former head of the US Food and Drug Administration,
told CNBC , �We will see more cases in the US and a lot will be undetected.� He added, however, that he did not expect an
epidemic-level crisis in America.
Dr Nicholls seems to me to be an expert with apparently world-class credentials and no obvious agenda when addressing an audience of
wealthy investors seeking guidance and facts:
https://www.sott.net/article/429100-Coronavirus-Expert-in-Leaked-Analysis-This-is-Just-a-Severe-Localized-Common-Cold
The USA intelligence agencies again proved to be quite useless in this calamity. Here is a couple of interesting posts from Moon
of Alabama on the topic:
kiwiklown , Mar 22 2020 10:11 utc |
128
@Jackrabbit | Mar 21 2020 22:32 utc | 50
"These officials "failed us" in the same way that our media "fails us": they serve the interests of the EMPIRE-FIRST
Deep State."
Yuppp. Our error is to assume all 17 intelligence agencies; the presstitudes; and US "leadership" exist to serve the American
people. And so, yes, they "fail" the people. But, from the point of view of the controllers of those agencies and of those "leaders",
they hardly ever fail !!!
While the people argue over virulent minutae, they are once again helping themselves to the US Treasury.... Trillions of USDs....
LOL
kiwiklown , Mar 22 2020 10:36 utc |
132
@Jackrabbit | Mar 21 2020 23:10 utc | 54
"Caitlin Johnstone also sees the response being manipulated to focus hate on China...."
Yuppp, blaming China, hating on China achieves several objectives:
it misdirects Americans from blaming Trump's "leadership";
it excuses Trump's mismanagement ("...the Chinese LIED...")
it absolves the CDC, 17 "intelligence" agencies, etc;
it continues The Great China Pivot started by Great Pretender Obama;
it uses current fear to mobilise Americans to hate China more;
it prepares Americans for when war on China becomes feasible;
Just look at how US leadership has been hating on Russia for the last 100 years, waiting to whack them with a sneak attack
if feasible.
kiwiklown , Mar 22 2020 11:25 utc |
137
@Jackrabbit | Mar 22 2020 2:45 utc | 79
".... was then told to STOP TESTING...... A medical person would not try to suppress testing. That would be a "management
decision" and its the Nation Security Council that was running the show (and which had classified all discussions related to
virus preparations)...."
Thanks for reminding us of Dr Chu's story. What if the US leadership:
Knew the coronavirus was already out in the wild in the US by Sep 2019;
Decided to set up China to be the "origin" to be blamed;
Realized that a "pandemic" can be the cover for kicking the table over to do the Great Financial Reset;
Li Wenliang was ophthalmologist, not epidemiologist. He noticed some clustering of pneumonia infections and thought that they
are the return of SARC virus. He shared this hypothesis (which was unsubstantiated rumor) with several colleagues in his private WeChat
group on Dec 30, 2019 and was summoned to policy who asked him to not spread this misinformation and allowed him to return to work.
Later he became infected (he started coughing on jan 10) and died February 7 from this pneumonia. Being just 34 he probably among half-dozen
youngest victim of the virus at the time (mostly medical workers). In any case his post to WeChat now is considered to mark
the beginning of epidemics in China.
Here are some interesting details that were misreported by neoliberal MSM:
Godfree Roberts March 4,
2020 at 11:43 pm GMT
Great survey. Some quibbles:
Before going down himself in the line of duty, Dr. Li faced a harsh reprimand from representatives of the Chinese Communist
Party. Dr. Li was accused of spreading rumors and illegally threatening the social order with his tweets and posts and personal
interventions. Nevertheless, Dr. Li was soon vindicated in calling attention to the coming plague .
Not really. Li was a junior ophthalmologist at a Wuhan hospital who overheard a rumor that SARS had broken out again. Li did
not inform China's CDC, which was already investigating it. Instead, Li used social media to repeat the rumor to family and friends
and they told their friends .
Li was wrong professionally: it was not SARS, as he asserted in his tweets. Li was wrong legally: it is illegal to spread
rumors likely to cause panic. Li was neither harshly questioned nor convicted of anything. After an hour of questioning the police
concluded that he had merely acted irresponsibly and he was allowed to return to work.
The Wuhan Coronavirus epidemic of 2020 is causing the once-firm ground beneath many established institutions to shake
uncontrollably. One of those institutions, the Chinese communist government, is encountering its Chernobyl moment .
Every multilateral public health body that has studied the outbreak has praised the timeliness, thoroughness, and effectiveness
of China's response. Don't be fooled by our media's selective use of outbursts on Chinese social media. This may be seen as much
a triumph for China as a failure for its principal critic, the US. China's government was, and remains, the most trusted on earth.
The fact that ground zero of the Novel Coronavirus is Wuhan, home of China's newest and most sophisticated microbiology
laboratory, naturally casts a shadow of doubt over narratives minimizing the role of human agency in creating the new strain
of Coronavirus .
Ron Unz's comments, above, cast a much darker shadow, given America's track record of waging biological warfare on China, Cuba,
et al.
Clearly the Party initially failed the people by not intervening early and decisively enough after the first cases of
Coronavirus illness began to show up .
The Chinese Communist Party took half the time to intervene in this outbreak that the American Capitalist Party took to intervene
in the its home-brewed H1N1 outbreak. See the two timelines here: https://youtu.be/rJiKxV4rTCQ
Jeremygg5
March 9, 2020 at 4:42 am GMT
Dr Li Wenliang was NOT a whistleblower. He wrote to his private chat group about the re-emergence of SARS at 5:35pm on Dec
30 2019. However the health authority of Wuhan received the genetic report of the virus earlier the day, and released two official
announcements the same day afternoon to thousands of medical personnel. Dr Li was an eye doctor and probably saw the memo, and
wrote to his private chat group saying that it was SARS. He was reprimanded because the disease was still unknown at that time.
Two emergency notices issued on Dec 30:
� 《关于做好不明原因肺炎救治工作的紧急通知》the emergence of a kind of pneumonia of unknown origin , get organized to
deal with it, administer aid immediately without passing on responsibility to other units with focus on strengthening breathing,
infection control, and other relevant medical disciplines. Report cases without delay.
� 《市卫生健康委关于报送不明原因肺炎救治情况的紧急通知》
d dan March 9,
2020 at 5:34 am GMT
@Tony
Hall
" Dr. Li who was reprimanded for refusing to go along with the CCP denial of the Novel Coronavirus's existence."
What a dumb author who still can manage to make two mistakes in half a sentence, even after so many rounds of clarifications
by so many people.
CCP did not deny the existence of COVID-19, they were investigating it at that time. And Dr Li was not reprimand for refusing
to go along, but was reprimanded because he was shouting fire in a crowded cinema, a type of speech that US Supreme Court won't
allow too.
Parfois1
March 9, 2020 at 6:43 am GMT
@Tony
Hall
I look at the treatment of Dr. Li who was reprimanded for refusing to go along with the CCP denial of the Novel Coronavirus's
existence. The attack on Dr. Li as a Chinese version of a "conspiracy theorist," when he was in fact a whistle blower, speaks
to me of similar patterns I perceive in the West. Dr. Li is a symbol of the assault on free expression on both China and the
so-called West.
You took no notice of Godfree Roberts clarification about Li's involvement, namely the fact that he was spreading a rumour
about which he had no authority or expertise to speak about when the medical competent bodies were still studying the nature of
the viral infections. He was wrong on both counts anyway: by spreading a rumour and that it was a false rumour. Besides, as far
as I remember the sequence of events, by the time the rumour started the medical authorities were about to, or in the cusp of,
making a public announcement about the virus.
Here is the fragment of his interview via WeChat (He
Warned of Coronavirus. Here�s What He Told Us Before He Died. DatelineNews24 :
On Dec. 31, when you told people in the WeChat group about the SARS-like virus, did you do so because you had seen
the high risk of human-to-human transmission?
I suspected that, and it�s always better to be cautious and take protective measures.
Why were you so suspicious at that point? Had you already received any news or heard anything?
Because there were already patients being treated under quarantine.
Was that at the end of December?
Yes.
Were there other doctors who shared the information and reminded others to protect themselves from this mysterious pneumonia?
There were discussions among our colleagues.
What was everybody talking about? How did they evaluate the situation at that point?
It was that SARS might come back. We needed to be ready for it mentally. Take protective measures.
Looking back at what has happened, do you think the situation would be very different now if the Wuhan government hadn�t
stopped you from warning others and sharing the information? Do you think it would have been better if the information had been more
public and transparent, for the public and for doctors?
If the officials had disclosed information about the epidemic earlier, I think it would have been a lot better. There should be
more openness and transparency.
How did you feel when the police accused you of spreading rumors?
The police believed this virus was not confirmed to be SARS. They believed I was spreading rumors. They asked me to acknowledge
that I was at fault.
I felt I was being wronged, but I had to accept it. Obviously I had been acting out of good will. I felt very sad seeing so many
people losing their loved ones.
Neoliberal MSM, which are practically always are stock market cheerleaders, trying to derail Trump behaved horribly in this respect
spreading unsubstantiated rumors and fear (China fearmongering was especially pronounced and evil). Such rumors along with disruption
of long, created by neoliberal globalization supply chains and severe downturn in transportation (especially airlines) and tourist
(especially cruse ships) and hospitality sectors are accelerating economic downturn which many economists expected in late 2020 early
2021.
See The threat of "Coronavirus recession"
In this sense Trump has a point when is called MSMS the coverage of Coronavirus epidemics a hoax (Trump
campaign blasts media for 'massively dishonest' claim POTUS called coronavirus a 'hoax' Fox News ). And Trump hit the nail in his
famous "Caronavirus " (innocent misspelling) twit: "
Low Ratings Fake News MSDNC (Comcast) & @CNN are doing everything possible to make the Caronavirus look as bad as possible
The main danger is China slow down which affects global production chains and might create a snowball effect. But the slowdown was
just two month long. But as of March 1, 2020 China is back to over 80% of production. Still some unpleasant surprises are possible:
HHH 02/29/2020 at 4:24
pm
If this virus shows up and hits hard in say Saudi Arabia and other oil producing nations the narrative will totally change .
It will go from just demand destruction from consuming nations to no supply coming out of producing nations.
If supplies chains seize up. For any extend amount of time 1-3 months. Things will get a whole lot more interesting than
they already are.
If the numbers being reported out of Iran are anywhere close to reality the middle east is in for a rocky ride as this
virus spreads.
Frightened people often behave irrationally and that typically contributes to the economic downturn as well. Not the US economy
was especially healthy before this event. In August, a survey of economists by the National Association for Business Economics
72% of analysts expected a US recession by the end of 2021. Of them 38% believed a recession will strike by the end of this year.
A UN report published in September similarly warned of a worldwide recession this year.
20210812 : No, the Unvaccinated Aren't Selfish or Ignorant. Here's Why I'm not Vaxxed - Opinion by Suri Kinzbrunner ( Aug 12, 2021 , www.msn.com )
20210812 : More Dangerous Side Effects Potentially Linked To mRNA Vaccines, EU Warns www.zerohedge.com )
20210805 : Pfizer says immunity can drop to 83% within four months in people who got its COVID-19 shot www.msn.com )
20210805 : Delta plus and other new mutations of the coronavirus news.yahoo.com )
20210803 : Where is the delta variant in the U.S.- This CDC map might give you a clue www.msn.com )
20210801 : Social pressure in the wrong direction: A hospital in in Missouri, Ozarks Healthcare, had to create a "private setting" for patients afraid of being seen getting vaccinated against COVID-19 www.msn.com )
20210801 : UK scientists believe it is 'almost certain' a coronavirus variant will emerge that beats current vaccines by Mick Krever ( Aug 01, 2021 , www.msn.com )
20210801 : 2 major San Francisco hospitals reported that 233 staff members tested positive for COVID-19 www.msn.com )
20210801 : CDC's new mask guidance for fully vaccinated suggests wearing mask in indoor areas www.msn.com )
20210730 : The Unhinged Fearmongering Over Kids and COVID Has Reached New and Absurd Levels, by Matt Vespa ( Jul 20, 2021 , townhall.com )
20210730 : CDC Data Shows Delta Variant Breakthrough Cases Equally Contagious as In Unvaccinated People www.msn.com )
20210730 : CDC mask decision followed stunning findings from Cape Cod beach outbreak www.msn.com )
20210730 : CDC Warns Vaccinated People Can Pass COVID to Others www.msn.com )
20210730 : Animals can be a reservoir of COVID-18 and the source of new mutations: researchers Find new COVID Mutations in NYC Sewage, Pointing to Possible Dog, Rat Infections www.msn.com )
20210729 : Thai study looks at CoronaVac vaccine vs. natural immunity to SARS-COV-2 variants www.news-medical.net )
20210729 : According to the CDC's guidelines for the fully vaccinated, those infected with the delta variant can spread it to others. www.msn.com )
20210729 : Israeli study says the Pfizer vaccine is losing effectiveness. But some experts think it's a fluke www.msn.com )
20210729 : Your Vaccinated Immune System Is Ready for Breakthroughs www.msn.com )
20210729 : Drugs cleared or recommended in the U.S. for Covid-19 patients www.wsj.com )
20210729 : Covid Treatment Options Remain Elusive, Despite Months of Effort and Rising Delta Cases by Joseph Walker ( Jul 29, 2021 , www.wsj.com )
20210724 : 64 Percent of Unvaccinated Americans Say COVID Shot Ineffective Against Variants- Poll www.msn.com )
20210724 : The World Health Organization in late June 2021 urged people to again wear masks indoors even those who are fully vaccinated due to the threat of breakthrough infections www.msn.com )
20210724 : In Oregon, about 10 percent of the breakthrough infections reported to the state were in people living in nursing homes or congregate care facilities, and the majority of deaths were older people. newsdeal.in )
20210724 : What Do Breakthrough COVID Cases Tell Us About What s Safe And What s Risky- by Arun Rath ( Jul 20, 2021 , www.wgbh.org )
20210723 : GOP Sen. Rand Paul says he refuses to take the COVID-19 vaccine, claims he already has 'natural immunity' www.msn.com )
20210723 : Klobuchar targets vaccine misinformation with Section 230 bill www.msn.com )
20210723 : COVID Propaganda Roundup- Children's Risk of COVID Death 2 in 1,000,000 www.zerohedge.com )
20210723 : 20% Of New Los Angeles COVID Cases Are In Vaccinated People As Delta Variant Spikes by Cammy Pedroja ( Jul 23, 2021 , www.msn.com )
20210723 : 'I think people are underestimating how bad this is going to get'- Dr. Ashish Jha on the delta variant www.msn.com )
20210723 : Authorites failed to understand what the most porbable path of Delta variant is that it will become endemic www.forbes.com )
20210721 : How many breakthrough cases are there, by Katelyn Jetelina ( Jul 20, 2021 , yourlocalepidemiologist.substack.com )
20210721 : Is the COVID-19 vaccine riskier than the coronavirus? What a new poll suggests www.msn.com )
20210721 : Attorney Files Lawsuit Against CDC Based on "Sworn Declaration" from Whistleblower Claiming 45,000 Deaths Are Reported to VAERS All Within 3 Days of COVID-19 Shots www.zerohedge.com )
20210721 : Immunity provided by COVID-19 vaccines likely to 'wane, not plummet,' CDC director tells Congress www.msn.com )
20210721 : Preliminary NYU Study Suggests Johnson Johnson COVID Vaccine May Not Be As Effective Against Delta Variant www.msn.com )
20210721 : COVID-19 Delta variant highly transmissible among fully vaccinated people www.thehealthsite.com )
20210721 : Mandatory vaccination with experimental vaccines is questionable and should have us all worried. www.moonofalabama.org )
20210721 : 40% of People Being Admitted to Hospital with Covid-19 in England Have Been Fully Vaccinated (VIDEO) by Cristina Laila ( Jul 19, 2021 , www.thegatewaypundit.com )
20210720 : It's not Facebook, or Biden. It's people, finally wising up that the advantages of vaccination are temporary at best and you subject yourself to some additional risk by taking the vaccine for zero decrease in chances of serious illnesses or mortality for people younger then 30 www.msn.com )
20210720 : Stanford scientist Yvonne Maldonado enrolls children as young as 2 in Pfizer vaccine trials twitter.com )
20210720 : Stanford scientist Yvonne Maldonado enrolls children as young as 2 in Pfizer vaccine trials twitter.com )
20210720 : Delta variant accounts for 83% of new cases in US, CDC director says www.msn.com )
20210720 : Myocarditis and Pericarditis Following mRNA COVID-19 Vaccination www.cdc.gov )
20210720 : 40% of People Being Admitted to Hospital with Covid-19 in England Have Been Fully Vaccinated (VIDEO) by Cristina Laila ( Jul 19, 2021 , www.thegatewaypundit.com )
20210719 : De Blasio Says Mask Mandate Not The Solution To Growing COVID Cases, 'Vaccination Is' www.msn.com )
20210719 : What the Delta variant could mean for the Pfizer vaccine www.msn.com )
20210719 : Here's what vaccinated people need to know as Covid case counts rise www.msn.com )
20210719 : Look like Delta variant is less toxic then previous and led to fewer deaths and hospitalization, as often happen with later mutations of the viruses. www.zerohedge.com )
20210719 : Breakthrough COVID case in California: 74 vaccinated Californias have died abc7.com )
20210719 : Bob Wachter on Twitter- -If you're wondering how bad Delta really is, even in highly vaccinated SF (76% of gt;age 12 fully v twitter.com )
20210719 : New numbers released on COVID-19 breakthrough cases in Lexington foxlexington.com )
20210719 : Officials and neoliberal MSM changed the narrative: Vaccines now no longer designed to prevent infection, they are designed to prevent hospitalization and deaths www.msn.com )
20210718 : Breakthrough COVID cases in California abc7.com )
20210718 : Scientists identify breakthrough cases of SARS-CoV-2's delta variant in fully vaccinated individuals www.news-medical.net )
20210718 : COVID-19 Breakthrough Case Investigations and Reporting - CDC www.cdc.gov )
20210718 : What to know about the recent COVID-19 trends in Massachusetts by Nik DeCosta-Klipa ( Jul 15, 2021 , www.boston.com )
20210718 : CDC doesn't track all breakthrough cases leaving a gap in data by Libby Hendren ( Jul 16, 2021 , www.khou.com )
20210718 : Poor record-keeping limits 'breakthrough' COVID-19 case documentation - Poynter www.poynter.org )
20210716 : The calculus for school-age children will be different because their Covid risks are so much lower, and trial data won't identify 1 in 50,000 events. There's no need for K-12 schools to mandate vaccines www.wsj.com )
20210716 : Covid-19 Immune Response after infection could be long lasting, but variants present risks for both vaccinated and those who recovered from COVID-19 researchers say www.wsj.com )
20210716 : Covid will effectively act as a "second circulating flu this winter," and will eventually become endemic virus www.forbes.com )
20210715 : Natural Infection May Offer Better Protection Against Delta Variant, Israeli Health Ministry Says www.zerohedge.com )
20210715 : Moderna (MRNA) Targets HIV, Cancer, Flu, Zika After Covid Vaccine - Bloomberg www.bloomberg.com )
20210714 : Pfizer wants to administer the third (booster) short to vaccinationated people; Regulators Signal Caution www.bloomberg.com )
20210714 : Drugmakers Spending on Stock, Dividends and Executive Pay Exceeds Research, Democrats Say - www.nakedcapitalism.com )
20210714 : Delta Variant Could Push U.S. Covid Immunity To 85%, Says Former FDA Head www.forbes.com )
20210714 : As Delta variant spreads Pfizer vaccine protection takes a hit, Israeli government says by Ivana Kottasová ( Jul 07, 2021 , www.cnn.com )
20210714 : Fact Check-Claim that vaccinated people are six times more likely to die from the Delta variant than those who are unvaccinat www.reuters.com )
20210714 : America Will Not Achieve Herd Immunity www.fairobserver.com )
20210713 : AstraZeneca, J J Working On 'Modifications' To Eliminate Potentially Deadly Side Effects - ZeroHedge www.zerohedge.com )
20210713 : NJ COVID vaccine- Rare 'breakthrough infections' among vaccinated www.northjersey.com )
20210713 : Delta variant now dominant COVID-19 strain in NJ www.msn.com )
20210712 : Once more on vaccine hesitancy - Angry Bear by Eric Kramer ( May 12, 2021 , angrybearblog.com )
20210712 : Fact Check- Have 966 People Died After Receiving the COVID vaccine- www.newsweek.com )
20210712 : The CDC just warned of 3 new coronavirus vaccine side effects www.msn.com )
20210712 : F.D.A. Will Attach Warning of Rare Nerve Syndrome to Johnson Johnson Vaccine by Sharon LaFraniere and Noah Weiland ( Jul 12, 2021 , www.msn.com )
20210712 : If people read that they're going to need a booster shot in a few months anyway, why would they bother getting vaccinated now? www.zerohedge.com )
20210709 : Heart inflammation link to Pfizer and Moderna jabs www.msn.com )
20210709 : Could Pfizer and Moderna Be in Trouble After the Latest COVID Vaccine Findings www.msn.com )
20210709 : Delta Variant Hotspot- These Colorado Music Festival Goers Don't Care www.npr.org )
20210709 : Why The Delta Variant Is So Contagious- A New Study Sheds Light - Goats and Soda - NPR www.npr.org )
20210709 : Los Angeles County reports 165 percent spike in COVID-19 cases in a week. According to the Centers for Disease Control and Prevention, the variant now makes up the majority of new cases in the United States www.msn.com )
20210708 : The Alpha version of supposed SARS-CoV-2 was supposedly the most transmissible and infectious pathogen ever. With a transmission rate of at least 3.8 and reported to be perhaps as high as 9. Does this mean that Delta has transmissin rate over 12? www.zerohedge.com )
20210708 : Can vaccines guide coronavirus evolution in the direction of evading and bypassing the antibodies produced by the vaccine. www.quantamagazine.org )
20210708 : Delta Could Disrupt Emerging World's Post-COVID Recovery, Goldman Warns www.zerohedge.com )
20210706 : Dangerous Delta COVID-19 Variant Infecting Vaccinated Adults In Israel www.huffpost.com )
20210706 : Fact Check-Claim that vaccinated people are six times more likely to die from the Delta variant than those who are unvaccinat www.reuters.com )
20210706* Israeli officials say Pfizer vaccine less effective as Delta variant spreads ( Jul 06, 2021 , www.bostonglobe.com ) [Recommended] 20210705 : Swiss team retracted a paper on the little benefit of massive vaccination www.moonofalabama.org )
20210705 : Side effects of Pfizer vaccine www.moonofalabama.org )
20210705 : "National security" and "national interest" pretext to keeping the deal with vaccine maker secret www.moonofalabama.org )
20210705 : I am seeing more of is pressure to take the vaccine in US even though the infection numbers are going down in most states www.moonofalabama.org )
20210705 : Covid-19 hyperinflammation and post-Covid-19 illness may be rooted in mast cell activation syndrome www.moonofalabama.org )
20210705 : Considering the billions of profit made by Pfizer, and the complete politicization of the authorizations, there is no reason to be optimistic about the West's intentions. www.moonofalabama.org )
20210704 : U.K. Plans to Introduce Covid-19 Booster Shots in September www.wsj.com )
20210704 : How Many Have Died From COVID Vaccines undercurrents723949620.wordpress.com )
20210704 : It's not the spike protein collecting in ovaries. It is the "lipid shell." The lipid is going to the ovaries and bone marrow www.unz.com )
20210703 : Breakthrough infections, which occur when fully vaccinated people are infected by the pathogen that their shots were designed to protect against www.theatlantic.com )
20210703 : Delta Variant Fuels Missouri's Covid-19 Uptick www.wsj.com )
20210703 : COVID-19 Breakthrough Case Investigations and Reporting www.cdc.gov )
20210703 : Delta variant likely to become dominant coronavirus strain in US, former FDA chief says news.yahoo.com )
20210703 : Why Vaccinated Athletes Are Testing Positive for Coronavirus www.wsj.com )
20210703 : CDC Says Delta Strain Likely to Dominate in US www.bloomberg.com )
20210703 : The return of masks due to the threat posed by Delta mutation of the coronavirus: Delta does not care whether you are vaccinated or not www.zerohedge.com )
20210703 : Charlatans are a plague in modern science www.moonofalabama.org )
20210702 : Delta Variant's Spread Prompts Reconsideration of Mask Guidance www.nytimes.com )
20210702 : Delta Variant's Spread Prompts Reconsideration of Mask Guidance www.nytimes.com )
20210702 : Some Vaccinated People Are Dying of Covid-19. That suggests that Delta is displaying a worrying ability to evade the vaccine and cause severe illness www.msn.com )
20210702 : Mom details 12-year-old daughter's extreme reactions to COVID vaccine, says she's now in wheelchair www.foxnews.com )
20210701 : Mother weeps as she tells senator how Pfizer shot left her daughter wheelchair-bound www.lifesitenews.com )
20210701 : Why chidren needs to be vaccinated? Before Maddie got her final dose of the vaccine, she was healthy, got straight As, had lots of friends and had a life www.zerohedge.com )
20210701 : Percentage of false positives for Covid PCR tests at 40 cycles of amplification www.zerohedge.com )
20210701* Experts -- US COVID-19 positivity rate high due to 'too sensitive' tests by Marlene Lenthang ( Aug 30, 2020 , www.msn.com ) [Recommended] 20210701 : Fauci: There Are Now Two Americas, The Vaccinated The Unvaccinated ; ZH commenter: There are now two Americas. One that's retarded. And one that wants Fauci on a lamppost. www.zerohedge.com )
20210630 : Panic Porn Dressed Up As Science -- Exposing The Truth About The Delta Variant www.zerohedge.com )
20210630 : Twelve year was enrolled in the Pfizer vaccine clinical trial. She's now in a wheelchair, has an NG tube, and is suffering from severe memory loss, along with many other issues. citizenfreepress.com )
20210628 : Coronavirus Vaccine Updates- FDA adds warning to vaccines about risk of heart inflammation www.msn.com )
20210628 : Pfizer-BioNTech vaccine recipients have lower antibody levels targeting the Delta variant medicalxpress.com )
20210628 : Fully vaccinated people have gotten the Delta COVID variant. Should we be worried- www.msn.com )
20210628 : Delta variant outbreak in Israel infecting vaccinated adults nypost.com )
20210628 : Delta variant outbreak in Israel infecting vaccinated adults nypost.com )
20210628 : Experts "extremely worried" about Delta variant, by BETH MOLE ( Jun 15, 2021 , arstechnica.com )
20210626 : Israel which used Pfizer vaccine says the Delta variant is infecting vaccinated people, who represent as many as 50% of new cases; but they're less severe www.businessinsider.in )
20210626* 26 fully vaccinated people have died from Delta variant ( Jun 26, 2021 , news.yahoo.com ) [Recommended] 20210626 : GOP Sen. Ron Johnson Under Fire for Holding Event on Adverse Reactions to COVID Vaccines by Natalie Colarossi ( Jun 26, 2021 , www.msn.com )
20210626 : How the Pfizer-BioNTech Covid-19 Vaccine Works - The New York Times www.nytimes.com )
20210626 : WHO official suggested that there will be mutations of the Indian variant which would evade the protection offered by current vaccines, making vaccination "do good" gesture with significant health risks. www.zerohedge.com )
20210626 : Are existing COVID-19 vaccines already statistically less safe the vaccines against other epidemic diseases www.zerohedge.com )
20210626 : VAERS data www.zerohedge.com )
20210626 : WHO Stealth Edits Page Warning Against Vaccinating Children www.zerohedge.com )
20210626 : New virus mutations spread within the USA. Efficiency of the first generation of vaccines is in question as this is not the first and not the last mutation www.bloomberg.com )
20210626 : COVID-19- Pfizer jab recipients have lower antibodies targeting Indian variant, study suggests news.sky.com )
20210626 : Pfizer and Moderna vaccines will still work against B.1.617 and South Africa B.1.351. but oftter mostly protection from virus pneumonia illness, while losing the ability to stop mild infections www.npr.org )
20210626 : CDC has found a "likely association" between a handful of cases of heart inflammation and the mRNA COVID-19 vaccines www.zerohedge.com )
20210626 : Covid boosters in the fall- Here's what you should know www.cnbc.com )
20210626 : Pfizer Vaccine Provides Less Protection Against Variant From India, Study Shows www.webmd.com )
20210626 : On Friday, Italy halted the administration of the AstraZenika vaccine for those under the age of 60. The decision followed the death of a perfectly healthy 18-year-old named Camilla Canepa www.zerohedge.com )
20210626 : Alternatives to vaccination www.zerohedge.com )
20210626 : Possible but unproven side effects of vaccination www.zerohedge.com )
20210626 : Some facts that have not changed since 2019 outbreak www.zerohedge.com )
20210626 : Eric Clapton says COVID VACCINE damaged his Immune system www.zerohedge.com )
20210626 : According to Dr. Michael Yeadon kids are 50 times more likely to die from the shot then they are from the WuFlu www.zerohedge.com )
20210626 : Cole Beasley, wide receiver with the Buffalo Bills, caused a stir on Friday when he shared a statement on Twitter in which he asserted that he would not be getting the Covid vaccine www.zerohedge.com )
20210626* Surgeon Fired From College Of Medicine For Voicing Concerns About COVID Shots For Kids ( Jun 26, 2021 , www.zerohedge.com ) [Recommended] 20210625 : Delta Variant Outbreak in Israel Infects Some Vaccinated Adults - WSJ www.wsj.com )
20210625 : Pfizer, Moderna linked to heart disease in young recipients as vaccine rates slump www.msn.com )
20210624* Exclusive- Athlete Who Recovered From COVID Facing Very Different Future After Second Dose of Pfizer Vaccine Triggers Myoca by Megan Redshaw ( Jun 22, 2021 , peckford42.wordpress.com ) [Recommended] 20210624 : Current Reality Can Only Be Described As Anarchic Surrealism: Israel, which used Pfizer vaccines, and had only last week removed indoor mask mandates, has now reinstituted them, and is asking its citizens not to go abroad www.zerohedge.com )
20210624 : CDC panel finds 'likely' link between mild heart inflammation in adolescents and COVID-19 vaccine www.msn.com )
20210622 : Eric Clapton shares his feelings candidly about the past year of Covid lockdown www.unz.com )
20210622 : When I got pregnant the first time, my obgyn hands me a list of common foods and drinks to avoid, and now the government wants to inject an experimental drug into me? No thanks www.unz.com )
20210621 : Vaccines Exhibit Reduced Efficacy Against Delta Variant, WHO Doctor Warns www.zerohedge.com )
20210620 : Taibbi- Why Has -Ivermectin- Become A Dirty Word www.zerohedge.com )
20210618 : Manipution of death stats sure to effect of baby boom of 1946-1964 www.zerohedge.com )
20210618 : Hospitals See Surge In Double-Lung Transplants www.zerohedge.com )
20210618 : CDC Further Investigating Heart Inflammation Cases After Pfizer, Moderna Covid-19 Vaccination www.forbes.com )
20210618 : Delta Variant- Pfizer, AstraZeneca Vaccines Shown around80% effectivness after two doses in preventing hospitalizations www.bloomberg.com )
20210614 : Japanese research showed that the Pfizer lipid nano-particle package, presumably with its mRNA cargo intact, did NOT remain in situ in the deltoid muscle, but within hours had spread via the circulation to most of the body www.unz.com )
20210614 : I still prefer to wait for more traditional vaccines to be approved, if I have to be vaccinated at all www.unz.com )
20210612 : CDC To Meet On Rare Heart Inflammation Following COVID Vaccine science.slashdot.org )
20210612 : CDC advisers to review heart inflammation link to mRNA COVID jabs - Business and Economy News - Al Jazeera www.aljazeera.com )
20210612 : Melbourne Lockdown Extended on Warning of Virus' Quick Spread www.bloomberg.com )
20210612 : Plunge protection team in action? CDC To Hold -Emergency Meeting- After 100s Suffer Heart Inflammation Following COVID Vaccines www.zerohedge.com )
20210612 : The Power of Natural Immunity www.wsj.com )
20210612 : Merck Inks Molnupiravir Supply Pact With US Government For COVID-19 finance.yahoo.com )
20210612 : Pfizer to expand tests of COVID-19 vaccine in children below 12 - Coronavirus pandemic News - Al Jazeera www.aljazeera.com )
20210612 : CDC To Hold -Emergency Meeting- After 100s Suffer Heart Inflammation Following COVID Vaccines www.zerohedge.com )
20210612 : Gangrene, Hearing Loss Show Delta Variant May Be More Severe by Bhuma Shrivastava ( Jun 08, 2021 , www.bloomberg.com )
20210609 : Israel Vaccination Statistics from The Lancet www.zerohedge.com )
20210608* Science has lost its way, at a big cost to humanity by MICHAEL HILTZIK ( Oct 27, 2013 , www.latimes.com ) [Recommended] 20210530 : Vir Biotechnology CEO on its covid-19 drug candidate winning FDA nod for emergency use finance.yahoo.com )
20210530 : Widespread lack of vitamin D is the root cause of so many problems. www.zerohedge.com )
20210529 : Is Ivermectin The New Penicillin www.zerohedge.com )
20210529 : He said he refused to do surgery on anyone not vaxed for Covid www.zerohedge.com )
20210528 : Immunity to the coronavirus may persist for years, what it could mean for vaccination efforts finance.yahoo.com )
20210528 : Immunity to the coronavirus may persist for years, what it could mean for vaccination efforts finance.yahoo.com )
20210528 : Doctors Claim A Cocktail Of Cheap Drugs Could Help India Extinguish COVID Crisis www.zerohedge.com )
20210528 : One of my friends in the USSA who was fully vaccinated (Phizer I think) within the past 3 months just got a positive COVID test www.moonofalabama.org )
20210528 : Scott Atlas -- Lockdowns Not Only A Heinous Abuse Of Power, They Also Failed To Protect The Elderly www.zerohedge.com )
20210528 : SARS-CoV-2 spike S1 subunit induces hypercoagulability www.news-medical.net )
20210528 : The spike proteins of SARS-CoV-2 variants identified in India www.news-medical.net )
20210528 : Johns Hopkins Prof- Half Of Americans Have Natural Immunity; Dismissing It Is -Biggest Failure Of Medical Leadership www.zerohedge.com )
20210528 : Medical science has made such tremendous progress that there is hardly a healthy human left. ~ Aldous Huxley www.youtube.com )
20210528 : Don t mention Ivermectin; It ll Affect the Vaccine Rollout www.moonofalabama.org )
20210528 : CDC's Absurd Guidelines For Summer Camps- A Recipe For Dystopian Fun www.zerohedge.com )
20210527 : Ohio sees COVID vaccination rate soar 45% since announcing Vax-A-Million lottery www.msn.com )
20210524 : I never saw the 1973 movie Soylent Green but below is the last Wiki line about the movie that resonates with my perspective of the Western brainwashed becoming a new income stream for Big Health just like wars are income streams for the MIC www.moonofalabama.org )
20210524 : NIAD started working on coronavirus vaccine with Moderna in Maryland in Jan 2020 www.wusa9.com )
20210524 : CDC is Investigating Heart Problems in a Few Young Covid-19 Vaccine Recipients by Apoorva Mandavilli by Apoorva Mandavilli ( May 22, 2021 , www.nytimes.com )
20210522 : Cases of vaccinated people getting COVID are not that rare www.zerohedge.com )
20210522 : Indian mutation of the virus can became dominant in UK and probably in the world dailymail.co.uk )
20210522 : Last December, Yeadon, a British national, filed a petition with the European Medicines Agency (EMA) to immediately suspend testing on these experimental vaccines due to many safety concerns principia-scientific.com )
20210522 : The ex-Pfizer scientist who became an anti-vax hero www.reuters.com )
20210522 : TEENAGE SON HOSPITALIZED WITH BRAIN BLOOD CLOTS AFTER PFIZER MRNA VAXX 2021-05-11 ugetube.com )
20210522 : South African COVID-19 variant can 'break through' Pfizer vaccine -- Israel study www.channelnewsasia.com )
20210522* Michael Yeadon -- No need of vaccine, COVID-19 pandemic effectively over - FoxExclusive ( May 22, 2021 , foxexclusive.com ) [Recommended] 20210522 : America's Frontline Doctors files motion for temporary restraining order against use of COVID vaccine in children www.americasfrontlinedoctors.org )
20210522 : Pfizer is already demanding military bases as collateral for their covid vaccines www.zerohedge.com )
20210522 : The fact that they can run 40+ cycles and get a negative result shows that this test is actually garbage www.zerohedge.com )
20210522 : Caught Red-Handed- CDC Changes Test Thresholds To Virtually Eliminate New COVID Cases Among Vaxx'd - ZeroHedge www.zerohedge.com )
20210522* Warning about Faucism From Former Pfizer Chief Scientist by Michael Yeadon ( May 18, 2021 , www.investmentwatchblog.com ) [Recommended] 20210522 : Lysenkoism on the march -- CDC Changes Test Thresholds To Virtually Eliminate New COVID Cases Among Vaxx'd www.zerohedge.com )
20210518 : Sweden Records More Than 30K Cases Of Side Effects Tied To COVID Jabs - ZeroHedge www.zerohedge.com )
20210515 : Colorado vaccination site shuts down early after 11 people have 'expected' adverse reactions to the Covid-19 vaccine, officia www.cnn.com )
20210515 : COVID Deaths Plummet As Excess Mortality Falls To Pre-Pandemic Levels - ZeroHedge www.zerohedge.com )
20210513 : Blood Expert Says He Found Why Some Covid-19 Vaccines Trigger Rare Clots - WSJ www.wsj.com )
20210513 : Pfizer-BioNTech vaccine is 97% effective against symptomatic infection and 86% effective against asymptomatic infection. www.wsj.com )
20210512 : Germany introduces surveillance of "Covid deniers" and "anti-Vaxxers www.moonofalabama.org )
20210511 : India Struggles to Keep Pace With Coronavirus Variants www.wsj.com )
20210511 : Professor Explains Flaw In Many Models Used For COVID-19 Lockdown Policies - ZeroHedge www.zerohedge.com )
20210510 : Why is healthy 24-year-old Jennifer Gates jumping the line to get the vaccination twitter.com )
20210510 : Pfizer-BioNTech Covid Shot Cleared for Adolescents in U.S. - Bloomberg www.bloomberg.com )
20210510 : Pfizer CEO Says Third Covid Vaccine Dose Likely Needed Within 12 Months science.slashdot.org )
20210509 : Death of fully vaccinated US expert in India sparks worry over Pfizer s efficacy against COVID-19 double mutant www.globaltimes.cn )
20210509 : How a Researcher 'Clinging To the Fringes of Academia' Helped Develop a Covid-19 Vaccine science.slashdot.org )
20210509 : Teens Fully Protected By Pfizer's COVID-19 Vaccine, Company Says science.slashdot.org )
20210509 : Scientist Behind COVID-19 mRNA Vaccine Says Her Team's Next Target Is Cancer science.slashdot.org )
20210509 : Variant From the UK Likely Accounts for Up To 30% of Covid Infections in US, Fauci Says science.slashdot.org )
20210509 : Florida Governor Issues Executive Order Prohibiting COVID-19 Vaccine Passports science.slashdot.org )
20210509 : Reaching 'Herd Immunity' Is Unlikely in the US, Experts Now Believe science.slashdot.org )
20210509 : Economists Disagree Over How Much Covid-19 'Herd Immunity' Needed for Recovery www.wsj.com )
20210509 : DOES COVID-19 REALLY CAUSE ARDS? www.moonofalabama.org )
20210508 : Dr. Henry Ealy and his team started looking at CDC data on COVID-19 cases and fatalities in mid-March 2020, quickly realizing the agency was vastly exaggerating fatalities www.zerohedge.com )
20210507 : Vaccines offer little protection to elderly: an unvaccinated health-care worker set off an outbreak in a mostly vaccinated Kentucky nursing home www.theatlantic.com )
20210507 : What Are No-Vaxxers Thinking by DEREK THOMPSON ( May 07, 2021 , www.theatlantic.com )
20210507 : Seychelles, World's Most Vaccinated Country, Hit by Covid Surge....Including Among the Vaccinated - www.nakedcapitalism.com )
20210507 : Democrats plan to make it suck more to not be vaccinated. www.theatlantic.com )
20210506 : Recognizing the broad potential of mRNA science, we set out to create an mRNA technology platform that functions very much like an operating system on a computer. It is designed so that it can plug and play interchangeably with different programs www.zerohedge.com )
20210506 : Aldous Huxley Foresaw Our Despots - Fauci, Gates, The Vaccine Crusaders www.zerohedge.com )
20210503 : Not a single resource on the Pfizer Executive team or Board of Directors has been injected with the Pfizer (experimental poison yet) vaccine yet. - C Weissman www.zerohedge.com )
20210503 : Coronavirus- One Pfizer jab wards off variants for some by Alexandra Thompson ( Apr 30, 2021 , news.yahoo.com )
20210503 : Pfizer vaccine effective against Indian variant of Covid-19 - The Doha Globe thedohaglobe.com )
20210503 : Pfizer says South African variant could significantly reduce protective antibodies - Reuters www.reuters.com )
20210503 : Pfizer vaccine neutralizes Brazilian virus variant in new study thehill.com )
20210503 : South African variant can break through Pfizer vaccine- Study - Coronavirus pandemic News - Al Jazeera www.aljazeera.com )
20210503 : S. African Variant Challenges Pfizer, Moderna Vaccines www.webmd.com )
20210503 : -I Just Wanted A Little More Time- - Texas Nurse Was Fired For Refusing COVID Vaccine - ZeroHedge www.zerohedge.com )
20210503 : COVID-19 Vaccines vs Variants "Determining How Much Immunity Is Enough - Vaccination - JAMA - JAMA Network jamanetwork.com )
20210503 : Evidence for increased breakthrough rates of SARS-CoV-2 variants of concern in BNT162b2 mRNA vaccinated individuals www.medrxiv.org )
20210503 : mRNA based vaccines are mis-named, they are a gene therapy, triggering the manufacture of antigens to work on virus. www.zerohedge.com )
20210503 : There is significant cross-immunity between coronaviruses www.zerohedge.com )
20210503 : Some scientists have used the term vaccine resistance to describe the reduced efficacy of COVID-19 vaccines against some variants jamanetwork.com )
20210503 : The Head of EMA is a pharma shill www.moonofalabama.org )
20210503 : Variants vs. Vaccines - Southwestern Vermont Health Care svhealthcare.org )
20210503 : COVID-19 Vaccines And Coronavirus Mutations www.npr.org )
20210503 : Children and mRNA vaccine www.zerohedge.com )
20210503 : EU starts legal action against AstraZeneca over vaccine shortfalls off-guardian.org )
20210503 : Why authorities ask vaccinated people wear masks and obey social distancing rules? www.zerohedge.com )
20210503* Teachers abusing kids. Disgusting. Pfizer and Moderna experimenting on kids. Criminal ( May 03, 2021 , off-guardian.org ) [Recommended] 20210502 : 15-Year-Old Boy Dies Of Heart Attack Two Days After Taking Pfizer Vaccine, Had No History Of Allergic Reactions www.zerohedge.com )
20210502 : If anyone had listened to Dr. Fauci or any of the mainstream press, they would think the vaccine is totally 100% safe and effective. But it is not 100% safe and 100% effective and we probably need to live with those limitation www.zerohedge.com )
20210430 : Pfizer, BioNTech seek EU authorisation on Covid-19 shot for younger teens, Europe News Top Stories www.straitstimes.com )
20210430 : Biden's administration push vaccine to children www.wsj.com )
20210430 : More then half of adults in the U.S. had gotten at least one dose of a vaccine, according to the CDC. That proportion ranged from 72% in New Hampshire to 39% in Mississippi. www.wsj.com )
20210430 : Keyboard warriors attack Joe Rogan after he DOES NOT recommend young healthy people get Covid-19 vaccine www.rt.com )
20210429 : The Pfizer vaccine could cause severe neurodegenerative diseases caused by brain prions created by the mRNA-style vaccine www.zerohedge.com )
20210429 : Pfizer Vaccine might cause Neurodegenerative Diseases nationalfile.com )
20210429 : Slowly But Surely, The Truth Is Coming Out: Pfizer CEO admitted that fully vaccinated people will need a third shot of the vaccine within 12 months If you don t want to believe me, perhaps you will believe the CEO of Pfizer. This week, he admitted that fully vaccinated people If you don t want to believe me, perhaps you will believe the CEO of Pfizer. This week, he admitted that fully vaccinated people This week, he admitted that fully vaccinated people will need a third shot of the vaccine within 12 months www.zerohedge.com )
20210428 : Joe Rogan is being attacked by Fauci the White House for daring to have an honest discussion about Covid-19 vaccines by Zachary Leeman ( Apr 28, 2021 , www.rt.com )
20210428 : I think efficiency will drop over time requiring frequent booster shots as well as new virus strains that render the current vaccine useless. Time will tell. www.zerohedge.com )
20210427 : What We Know About India s Double Mutant Covid-19 Variant www.wsj.com )
20210427 : No clear link between vaccinations and deaths has been found to date www.moonofalabama.org )
20210427 : Russia delivered 200,000 doses of Sputnik V gratis to Slovakia with a contract to deliver 2M more doses. The US/NATO agents busted a gasket, replaced the prime minister and prevented Slovakia from using any of the vaccines. They even refused to return the 200,000 doses so that Russia could use them somewhere else. turcopolier.com )
20210427 : Regarding the three articles posted on covid and thrombosis. www.moonofalabama.org )
20210427 : The Pandemic and irrational exuberance about vaccines www.moonofalabama.org )
20210427 : The Gamaleya Center statement - Official website vaccine against COVID-19 Sputnik V sputnikvaccine.com )
20210426* Genetic Vaccines -- Are They the New Thalidomide by Dr. Lee Merritt ( Apr 26, 2021 , thenewamerican.com ) [Recommended] 20210426 : Thirty-six deaths were recorded in the first quarter of 2020 versus 1,754 in the first quarter of 2021 www.zerohedge.com )
20210425 : No Jab For Me nojabforme.info )
20210415 : It's all positive about coronavirus vaccines www.zerohedge.com )
20210415 : 3rd Dose Of Pfizer's COVID Vaccine -Likely- Needed To Combat Mutant COVID Strains, CEO Says - ZeroHedge www.zerohedge.com )
20210415 : The powerful technology behind the Pfizer and Moderna vaccines - PBS NewsHour www.pbs.org )
20210415 : We have a therapy that can fight COVID-19. The medications have been around for 50 years, they are cheap, FDA and TGA approved, and have an outstanding safety profile www.zerohedge.com )
20210413 : above a threshold of 33 cycles www.cdc.gov )
20210413 : Moderna Shot remains 90% Effective After Six Months www.bloomberg.com )
20210413 : VA Study- How Long Does COVID-19 Vaccine Immunity Last angrybearblog.com )
20210412 : Covid-19 Drug Prevents Symptomatic Disease in Study, Regeneron Says - WSJ www.wsj.com )
20210411 : Investigate Good, Existing Covid Therapies - WSJ www.wsj.com )
20210409* Distrust of the establishment plays a role in vaccine hesitancy, but it's probably time to back off on the prevailing commentary suggesting that those avoiding vaccines are irresponsible, uninformed or politically manipulated ( Apr 09, 2021 , www.wsj.com ) [Recommended] 20210403 : At the hospital where my sister works they have had to ask them to stop shipping the vaccine. Not many are lining up to take it. Seems like we have an overabundance of it here in Houston www.zerohedge.com )
20210403 : COVID19 PCR Tests are Scientifically Meaningless by Torsten Engelbrecht and Konstantin Demeter ( Jun 27, 2020 , off-guardian.org )
20210403 : SARS-CoV-2, contained in simulated saliva was inactivated quickly under sunlight exposure; may be as quickly as several minutes. www.zerohedge.com )
20210403 : The time of survival of virus under direct sun radiation might be less then five minutes www.zerohedge.com )
20210403 : Merck (MRK) Molnupiravir Pill Could Change the Fight Against Covid by Cynthia Koons and Riley Griffin ( Mar 25, 2021 , www.bloomberg.com )
20210402 : Vaccines advance one funeral at a time www.moonofalabama.org )
20210402 : Vaccine safety: science is not about consensus. It is about what can be proved with a repeatable experiment www.moonofalabama.org )
20210402 : The experimental mRNA injections are not vaccines. They do not prevent transmission. Their main purpose is to mitigate symptoms so that the sick person does not get sick enough to require hospitalisation and emergency approval was given on that basis. www.moonofalabama.org )
20210401 : Pfizer, BioNTech Say Shot Still 91.3% Effective Six Months After Vaccination www.wsj.com )
20210401 : NYT reporter against the Atlantic vaccine cheerleaders www.theatlantic.com )
20210331 : Possible unanticipated effect of vaccinated people on the creation of new variants of COVID-19 www.unz.com )
20210331 : EU Regulator Sees Possible Link Between Astra Shot and Clots - Bloomberg www.bloomberg.com )
20210331 : The "Unvaccinated" as outcasts by C.J. Hopkins ( Mar 31, 2021 , www.unz.com )
20210331 : The pawpaw and the goat are both listed in stable condition for now. www.unz.com )
20210330 : You are not vaccinated, don't come near me! www.unz.com )
20210330 : The danger of severe anaphylaxis is very small but real www.unz.com )
20210330 : Neoliberal establishemnt fiasco with lockdown now translates into dustrust of vaccines and motives behind mass vaccination www.unz.com )
20210330 : There is something rotten in the state of Covid www.moonofalabama.org )
20210330 : Pfizer-BioNTech COVID-19 Vaccine Frequently Asked Questions - FDA www.fda.gov )
20210330 : Reactions and Adverse Events of the Pfizer-BioNTech COVID-19 Vaccine - CDC www.cdc.gov )
20210327 : Why vaccines are the only game in town. Why treatments were almost completly abandoned? www.moonofalabama.org )
20210327 : It looks like the vaccinated will be the petri dishes from which the variants arise, but the unvaccinated who will be vilified www.moonofalabama.org )
20210327 : I don't know how important or reliable this is, but Pfizer does have an impressive rap sheet as a corporate criminal www.moonofalabama.org )
20210327 : New York Times Does Public Relations Work for the Pharmaceutical Industry by DEAN BAKER ( Mar 21, 2021 , cepr.net )
20210326 : Are PCR tests picking up spike proteins from the mRNA vaccines? www.zerohedge.com )
20210326 : Looking from your comment, you're in the camp of not taking the Covid vaccine. I gather that it's not because you don't believe in science, but because it's too early and a part of you don't believe in the process. www.unz.com )
20210326 : Rutgers University is requiring students to be vaccinated against COVID-19 by Aarthi Swaminathan ( Mar 26, 2021 , finance.yahoo.com )
20210322 : How very little is known, still, concerning viral transmission www.moonofalabama.org )
20210322 : Drug companies defend vaccine monopolies in face of global outcry: As immunization gap widens between rich and poor countries, the industry faces a battle over patents and know-how www.washingtonpost.com )
20210315 : Pfizer CEO Albert Bourla On Covid Vaccine- Extended Interview - NBC Nightly News www.youtube.com )
20210315 : Gravitas -- Pfizer's abusive vaccine deals www.youtube.com )
20210315 : Why there is such a mad rush toward vaccination for the varus which is only moderatly lethal with infections concentrated in large cities? Could someone clarify if Dr. Bossche referring to all the COV2 vaccines or just the mRNA ones (i.e. Pfizer and Moderna)? thehighwire.com )
20210315 : US worrying about vaccine competition is so stupid and amoral www.moonofalabama.org )
20210315 : U.S. And Its Five Eye Partners Use 'Persuasion', Sabotage And Disinformation To Gain Vaccine Supremacy www.moonofalabama.org )
20210315 : The vaccine situation they are analyzing is very much like the GMO experimentation www.moonofalabama.org )
20210315 : The difference between traditional vaccines and mRNA vaccines www.moonofalabama.org )
20210315 : Moderna we know is funded by DARPA, In-Q-Tel, Bill Gates, Jeffrey Epstein. In existence for thirty or forty years, depending which story you desire to believe. Never had a saleable product until now. Trust us. www.moonofalabama.org )
20210315 : It's Profit over People yet again, and such shouldn't be any surprise. www.moonofalabama.org )
20210315 : Indian Vaccine Manufacturers: U.S. Use of Wartime Export Controls Threatens World Vaccine Production www.moonofalabama.org )
20210315 : If you go to the US CDC website you will see that all current vaccines for Covid are only under "emergency" approval. It is also clearly stated that they will not work in all cases and that the Pharma Industry is not liable when they cause harm. www.moonofalabama.org )
20210315 : I'm not an epidemiologist nor medically trained on trial procedures and norms but i have the following questions www.moonofalabama.org )
20210315 : I am absolutely appalled by the blinkered focus on vaccines to the detriment of therapeutic treatment. www.moonofalabama.org )
20210315 : Gosh, there's so much enthusiasm for inoculation around here one almost forgets that there are many of us, even inside the industry, who don't want ANY of these injections. www.moonofalabama.org )
20210315 : Can mass mRNA vaccinations to speed coronavirus mutations www.moonofalabama.org )
20210314 : Study carefully the graphs of deaths in retirement homes in Ireland www.zerohedge.com )
20210314 : Several nations halt distribution of AstraZeneca Covid vaccine www.zerohedge.com )
20210314 : Professor of Government Ethics helped cover up COVID nursing home deaths - ZeroHedge www.zerohedge.com )
20210314 : SINCE NO QUANTIFIED VIRUS ISOLATES OF THE 2019-nCoV were available for CDC use at the time the test was developed and this study conducted, assays designed for detection of the 2019-nCoV RNA were tested with characterized stocks of in vitro transcribed full length RNA.. www.brighteon.com )
20210312 : Norway Investigates Whether AstraZeneca Vaccine Caused Deadly Blood Clots - ZeroHedge www.zerohedge.com )
20210312 : Covid 19 live updates- WHO says no link between blood clots and Oxford-AstraZeneca vaccine as more nations suspend its use - www.washingtonpost.com )
20210309 : Western media should investigate deaths and serious injuries related to Pfizer vaccine www.moonofalabama.org )
20210303 : Something about vaccination: four scouts who, in their quest for a good deed, helped an old lady to cross the street, and reported to their guide. All four of you were needed for that, asked an amazed guide. Well, she put up quite a strong resistance www.unz.com )
20210301 : A lot of people are beginning to understand how dysfunctional the USA government has become www.moonofalabama.org )
20210301 : A European court declares the RT-PCR test worthless. In the eyes of this court, then, a positive test does not correspond to a Covid case. The two most important reasons for this, said the judges, are that, "the test's reliability depends on the number of cycles used '' and that "the test's reliability depends on the viral load present .' www.moonofalabama.org )
20210228 : The global Pfizer jab is deadly effective. www.moonofalabama.org )
20210228 : Danger of mRNA vaccines to elderly under spotlight after 16 deaths in Switzerland www.moonofalabama.org )
20210227 : So, why not take a Big Pharma vaccine? www.moonofalabama.org )
20210224 : One-Third of Deaths Reported to CDC After COVID Vaccines Occurred within 48 Hours of Vaccination www.moonofalabama.org )
20210205 : With a Cycle Threshold over 35, you can get a positive PCR test out of a dog's ass www.zerohedge.com )
20210203 : Extra death stats sugessts the the pandemic was overblown www.unz.com )
20210129 : Coronavirus variants- What they do and how worried you should be - Ars Technica arstechnica.com )
20210127 : Merck Scraps COVID Vaccines; Says It's More Effective To Get The Virus And Recover www.moonofalabama.org )
20210126 : WHO must have known how PCR test worked in Jan 2020. Now they admit, a year later, that tests are misleading. off-guardian.org )
20210124 : The WHO's revised guidance effectively says the majority of infection data from PCR testing is meaningless. turcopolier.typepad.com )
20210124 : The COVID-19 RT-PCR Test- How to Mislead All Humanity. Using a -Test- To Lock Down Society - Global ResearchGlobal Research - www.globalresearch.ca )
20210122 : Israel's Fauci Warns Pfizer's COVID Vaccine Only Half As Effective As Advertised www.zerohedge.com )
20210121 : The short answer to both of these questions regarding the COVID-19 'casedemic' and the fallacy of asymptomatic PCR testing is YES and YES! www.zerohedge.com )
20210121 : Right On Cue For Biden, WHO Admits High-Cycle PCR Tests Produce COVID False Positives - ZeroHedge www.zerohedge.com )
20210120 : Those healthcare workers know their system. They're not stupid. www.moonofalabama.org )
20210120 : Hacked emails allegedly detail how EU drug regulator was pressured to approve Pfizer jab despite 'problems' with the vaccine www.moonofalabama.org )
20210119 : Three critical video www.unz.com )
20210117 : Personal social distancing alarms 'no jab, no job' show that individual freedoms at work will be the next victims of Covid www.rt.com )
20210114 : 19% or 95%? US expert challenges Pfizer vaccine's efficacy, triggers debates in China www.moonofalabama.org )
20210111 : COVID Gone Crazy - An Epidemic Of 'Positive' Tests www.zerohedge.com )
20210110 : One possible trap is that the French Government have signed one of the secret "accords" that give big Pharma the "right" (ability) to sue the French or other Governments if for any reason they do not make the profit they "expected or wanted" to make. www.moonofalabama.org )
20210110 : Miami Beach OB-Gyn doctor's death 18 days after Pfizer COVID-19 vaccine under investigation www.moonofalabama.org )
20210109 : An interview with Professor Dolores Cahill about the potentially lethal effects of mRNA vaccines: thewallwillfall.org )
20210109 : The PCR test should be trashed immediately, worldwide, and it should be considered a criminal act for anyone to be sent to quarantine because this test was positive off-guardian.org )
20210104 : What Vaccine Trials- OffGuardian off-guardian.org )
20201229 : Major Covid Vaccine Glitch Emerges- Most Europeans, Including Hospital Staff, Refuse To Take It - ZeroHedge www.zerohedge.com )
20201229 : US Demanding Iran's Vaccine Payments Go Through Its Banks www.moonofalabama.org )
20201228 : https://twitter.com/EstulinDaniel/status/1343206888020856840 twitter.com )
20201225 : The origins of the RT-PCR on which it is based our whole strategy against the Covid-19 pandemic, how it was created and in a rush published in a scientific private review, without obliged previous peer review, and which the conflict of interests are and how some people are profiting from this pandemic: www.moonofalabama.org )
20201222 : Top German virologist casts doubt on fears of new 'highly contagious' UK Covid-19 strain -- RT World News www.rt.com )
20201222 : B.1.1.7 mutation which has approx 70% higher transmissibility will probably soon displace the original variant of COVID-19. At least in Britain. www.moonofalabama.org )
20201221 : British medical journal The Lancet published research on Phase I and Phase II clinical trials of the vaccine, revealing no adverse effects in patients and triggering an effective immune response sputniknews.com )
20201221 : CDC Launches Probe, Issues New Guidelines After Thousands Negatively Affected Following New Covid Vaccine" www.moonofalabama.org )
20201221 : WHO (finally) admits PCR tests create false positives OffGuardian off-guardian.org )
20201220 : What is questionable about the corona virus vaccines? www.moonofalabama.org )
20201218 : The hunt for profit and power has now resulted in people being used as live test animals for a "vaccine" that is totally unnecessary. www.moonofalabama.org )
20201218 : I am also hearing considerable chatter that many medical professionals including doctors and nurses are going to REFUSE to take the poorly tested and questionable Covid vaccine for fear of damaging side effects www.moonofalabama.org )
20201217 : Is there a decease that a claim that vitamins C and D are a panacea for it would not be heard? www.unz.com )
20201213 : The paper that established the Drosten PCR test for the Wuhan strain of coronavirus that has subsequently been adopted with indecent haste by the Merkel government along with WHO for worldwide use -- resulting in severe lockdowns globally and an economic and social catastrophe was never peer-reviewed before its publication by Eurosurveillance journal. www.moonofalabama.org )
20201213 : If PcR test runs with more than 25 cycles, you are likely to get many false positives and at 40 you get mainly false postives www.moonofalabama.org )
20201213 : Protocols Strategies to manage COVID-19 Pandemic Dr Peter McCullough www.moonofalabama.org )
20201212 : Russian Cooperation Saves British Vaccine www.moonofalabama.org )
20201212 : '95% Effective' May Not Mean What You Think It Means by Thomas Neuburge ( Dec 10, 2020 , www.nakedcapitalism.com )
20201210 : To my knowledge, Pfizer/BioNTech has yet to release any samples of written materials provided to patients, so it is unclear what, if any, information regarding (potential) fertility-specific risks caused by antibodies is included www.zerohedge.com )
20201210 : Cycle threshold is everything with the PCR test. Anything above 35 is rubbish. 97% false positives. www.zerohedge.com )
20201210 : For The First Time, A US State Will Require Disclosure Of PCR 'Cycle Threshold' Data In COVID Tests - www.zerohedge.com )
20201206* Tested 'Positive' For COVID-19- Be Sure To Ask This Question ( Dec 06, 2020 , www.zerohedge.com ) [Recommended] 20201205 : -This Gives Some Hope- - Japanese Study Finds 98% Of COVID Patients Still Have Antibodies 6 Months Later - www.zerohedge.com )
20201202 : A global team of experts has found 10 FATAL FLAWS in the main test for Covid and is demanding it's urgently axed. As they sho www.rt.com )
20201202 : Most labs are running upwards of 40 cycles and that created a lot of false postives; you need to know Ct (cycle threshhold) to make a jusdgement www.moonofalabama.org )
20201130 : Landmark legal ruling finds that Covid tests are not fit for purpose. So what do the MSM do- They ignore it -- RT Op-ed www.rt.com )
20201128 : Post-2008 First World capitalism: the zombification and then definitive death of the petite-bourgeoisie: www.moonofalabama.org )
20201128 : mRNA technology is only effective theoretically. In the real world, it potentially has devastating effects on the human body. www.moonofalabama.org )
20201123 : What's Not Being Said About Pfizer Coronavirus Vaccine www.moonofalabama.org )
20201120 : WHO Rejects Gilead Remdesivir Drug Trump Took to Treat COVID-19 www.newsmax.com )
20201119 : Far Deadlier Strain Of Coronavirus Discovered In South Australia - www.zerohedge.com )
20201102 : A significant number of countries (e.g. Austria, Denmark, Germany [partial, Hesse Berlin only], Greece, Hungary, Norway) never had any excess mortality problem. www.moonofalabama.org )
20201102 : rtPCR testing, under the current state of knowledge, is the equivalent of measuring a patient's temperature with a thermometer but no doctor knows the average body temperature, and its natural healthy interval, nor would the thermometer provide a number on a scale, merely reporting that a patient has something other than "0". This would constitute a USELESS thermometer. www.moonofalabama.org )
20201031 : Democracy Dies in Darkness. And also at the Washington Post, these days... greenwald.substack.com )
20201021 : COVID19 PCR Tests Are Scientifically Meaningless www.globalresearch.ca )
20201015 : Three scientists give their best advice on how to protect yourself from COVID-19 www.cbsnews.com )
20201006 : Discussion of Trump's illness tends to obscure the reality that he, unlike most Americans and others who suffer from the virus, is getting proper treatment and all the necessary care to deal with the virus. www.moonofalabama.org )
20201006 : 'False' positive Covid-19 tests saw non-contagious people counted as fresh infections triggered 2nd wave alarm Belgian media -- RT World News www.rt.com )
20201005 : How to end the pandemic this year - The Japan Times japantimes.co.jp )
20201003 : Following PCR-confirmation of the President's diagnosis, as a precautionary measure he received a single 8 gram dose of Regeneron's polyclonal antibody cocktail www.moonofalabama.org )
20201002 : Covid-19 triggered wave of 'fraud and quackery' in medical research, leading ethicist warns -- RT World News www.rt.com )
20200928* No wonder Pompey and his friend Jeffries won't give up on Syria! No wonder ( Sep 28, 2020 , turcopolier.typepad.com ) [Recommended] 20200928* Truth be told: political operatives own and run our MSM. This is why the press is called the 'Fourth Estate' ( Aug 21, 2020 , www.unz.com ) [Recommended] 20200924 : What to know before getting a COVID-19 antibody test by Keith Zubrow ( Jun 28, 2020 , www.cbsnews.com )
20200924 : COVID-19 antibodies may last for at least 4 months, Icelandic study suggests by Akshay Syal ( Sep 24, 2020 , www.nbcnews.com )
20200924 : If the PCR Test Is Unreliable - Why Are Health Officials Demanding the Public Be Tested- www.blacklistednews.com )
20200923 : Your Coronavirus Test Is Positive. Maybe It Shouldn t Be by Apoorva Mandavilli ( Aug 29, 2020 , www.nytimes.com )
20200923 : DNA Amplification Through Polymerase Chain Reaction www.thoughtco.com )
20200920 : NYT First Reinforces, Then Silently Debunks Its False Claims About Russia's Covid-19 Vaccine www.moonofalabama.org )
20200917 : Dr. Quack- CDC's Redfield Claims Masks -- Guaranteed To Protect Against COVID www.zerohedge.com )
20200911 : Coronavirus measures more divisive for UK than Brexit � poll -- RT UK News www.rt.com )
20200906* Inactive fragments on virus RNA trigger false positives in most common COVID test due to way too many cycles of amplification which amplifies noise along with the signal and efffectly turns noise (inactive fragments on RNA) into signal, new study finds ( Sep 05, 2020 , www.zerohedge.com ) [Recommended] 20200906 : Wrote a memoir of a incubation patient. The coronavirus Hospital staff are pressured to hook you up to the tubes... www.zerohedge.com )
20200824 : Angry Bear " Some of the Gilead Remdesivir Results from Recent Studies angrybearblog.com )
20200824 : Anthropologist Wade Davis on how COVID-19 signals the end of the American era www.moonofalabama.org )
20200822 : Viruses, Plagues, and History- Past, Present and Future- Oldstone M.D., Michael B. A.- 9780195327311- Amazon.com- Books www.amazon.com )
20200819 : Russia's Ministry of Health names three drugs that can treat new Chinese coronavirus www.rt.com )
20200813 : America's Obesity Epidemic Threatens Effectiveness of Any COVID Vaccine www.zerohedge.com )
20200812 : New Study Finds Potential Reason Why COVID-19 Occurs Less In Children www.zerohedge.com )
20200803 : Red Flags Soar As Big Pharma Will Be Exempt From COVID-19 Vaccine Liability Claims - www.zerohedge.com )
20200803 : Next big COVID-19 treatment may be manufactured antibodies www.msn.com )
20200802 : Red Flags Soar As Big Pharma Will Be Exempt From COVID-19 Vaccine Liability Claims www.zerohedge.com )
20200802 : Obese People Are Twice As Likely To Die From Covid www.zerohedge.com )
20200802 : The Coronavirus Recovery Handbook: 19 Rehab Exercises for Mild to Severe Cases of COVID-19 www.moonofalabama.org )
20200801 : Russia preparing mass vaccination against coronavirus for October www.msn.com )
20200801* Length of interaction with tan infected person matter ( Aug 01, 2020 , www.zerohedge.com ) [Recommended] 20200727 : The problem of false positives from Covid-19 tests means UK is inflating its numbers � and taking wrong decisions by Rob Lyons ( Jul 27, 2020 , www.rt.com )
20200727 : How and when to wear masks www.theamericanconservative.com )
20200727 : One element of being a proper person is having some regard for the wellbeing of other people. www.theamericanconservative.com )
20200725 : Corporate Insiders Pocket $1 Billion in Rush for Coronavirus Vaccine www.msn.com )
20200724 : Cold Wars Profit by Craig Murray ( Jul 24, 2020 , consortiumnews.com )
20200724 : Study identifies six different types of COVID-19 www.msn.com )
20200723 : COVID-19/nCOV/SARS-2 immunity comes from T-cell and B-cell activity www.moonofalabama.org )
20200721 : Scientists report that airborne coronavirus is probably infectious www.msn.com )
20200720 : Russian Elite Received 'Experimental' COVID-19 Vaccine As Early As April - www.zerohedge.com )
20200720 : Oxford-AstraZeneca COVID-19 Vaccine Trials Show -No Adverse Effects- - www.zerohedge.com )
20200720 : Trust in US famacuticals eloparates: the Big Pharma mafia and its political apparatchiks in the West promote expensive patented drugs like Remdesivir, as opposed to inexpensive alternatives, as well as the Holy Grail for Big Pharma - a highly profitable vaccine www.moonofalabama.org )
20200718 : COVID-19- What Does Being Positive Really Mean- What Are We Really Detecting- - Fort Russ fort-russ.com )
20200718 : Lee Camp- The Life-Saving COVID-19 Drugs You've Never Heard Of (and Why) www.mintpressnews.com )
20200715 : These Are the Drugs and Vaccines That Might End the Coronavirus Pandemic www.bloomberg.com )
20200714 : C has it correct. Everything besides death rates is meaningless. Unfortunately, the deaths need to be genuine Covid deaths not just any death. www.moonofalabama.org )
20200711 : Right to Repair Advocates Accuse Medical Device Manufacturers of Profiteering - Slashdot news.slashdot.org )
20200711 : The Great Covid-19 Deception and What You Need to Know to Survive by Gary Heavin ( Jul 11, 2020 , www.unz.com )
20200710 : Vitamin D deficit potencially increases the probablity to catch COVID-19 www.moonofalabama.org )
20200710 : AR Comes to the Fight Against Covid-19 www.afr.com )
20200710 : LancetGate- -Scientific Corona Lies- Big Pharma Corruption - Hydroxychloroquine Versus Remdesivir - www.zerohedge.com )
20200709 : Vitamin D may be a good defense against the coronavirus, according to several new reports. Here's what you need to know- www.msn.com )
20200708 : Copper will not protect you from coronavirus despite killing germs - Insider www.insider.com )
20200707 : Approximately one in every 12 individuals, or 500 million people worldwide, is living with chronic viral hepatitis www.moonofalabama.org )
20200707 : Why closed spaces are them main avenue of COVID-19 propagation www.moonofalabama.org )
20200705 : The main benefit of herd immunity is that it will allow the country to function again. And that would be good for everyone, healthy and sickly alike. www.unz.com )
20200703 : Hydroxychloroquine lowers COVID-19 death rate, Henry Ford Health study finds - Detroit News turcopolier.typepad.com )
20200703 : The current reserach suggests that while the G614 variant may be more infectious, it is not more pathogenic. www.moonofalabama.org )
20200702 : Public Outcry Follows Gilead Decision to Charge $3000 for COVID Drug that Costs Pennies to Produce www.mintpressnews.com )
20200629* Gilead Will Charge More Than $3,000 For A Course Of COVID-19 Drug Remdesivir ( Jun 29, 2020 , www.zerohedge.com ) [Recommended] 20200628 : New COVID19 treatment protocol specifically targets the cytokine storm and they use heparin for the blood clots www.moonofalabama.org )
20200628 : European study links genes, blood type with risk of severe coronavirus infection www.blogger.com )
20200628 : Genomewide Association Study of Severe Covid-19 with Respiratory Failure www.blogger.com )
20200628 : Coronavirus Causes Weaponized 'Tentacles' To Sprout From Infected Cells, Directly Inject Virus Into New Ones www.zerohedge.com )
20200628 : Diabetes is linked to a higher risk of death from the new coronavirus www.blogger.com )
20200628 : Nobel Prize winner Dr Michael Levitt postulated that the virus burns out when it has infected 15-20% of the population www.blogger.com )
20200623 : Stanford Prof Median Infection Fatality Rate Of COVID-19 For Those Under-70 Is Just 0.04% www.zerohedge.com )
20200622 : It seems France is taking the COVID19 epidemic more seriously than others www.moonofalabama.org )
20200622 : Protesters douse French health ministry with red paint news.yahoo.com )
20200620 : Everything You Need to Know About Herd Immunity elemental.medium.com )
20200618 : Most Coronavirus Tests Cost About $100. Why Did One Cost $2,315? U.S. health care prices are unregulated, opaque and unpredictable angrybearblog.com )
20200617 : Polio vaccine may be useful to prep the body for COVID19. www.moonofalabama.org )
20200616 : Hope for patients with severe COVID-19 pneumonia www.msn.com )
20200616 : Coronavirus- Dexamethasone proves first life-saving drug by Michelle Roberts ( Jun 16, 2020 , www.bbc.com )
20200616 : Another topic doctors talk about privately are the well-known "bad doctors" who keep getting free passes mistake after mistake, and often sit on hospital quality review committees. turcopolier.typepad.com )
20200615 : These San Francisco doctors flew to New York to fight the coronavirus -- and they have a warning for us www.cnbc.com )
20200613 : We Don't Need No Stinking Vaccine For COVID-19 www.zerohedge.com )
20200613 : CDC Reiterates Mask Recommendations as Virus Continues to Spread - Bloomberg www.bloomberg.com )
20200610 : Coronavirus vaccine developers are chasing outbreaks before they disappear Washpost - Sic Semper Tyrannis turcopolier.typepad.com )
20200610* Yale has published research that shows HCH + AZ has 50-fold benefits and insignificant risks ( Jun 10, 2020 , www.moonofalabama.org ) [Recommended] 20200608 : Doctors were allowed to consider PCR results as a factor, cautioned not to rely on them. In current situation PCR results became the definition of COVID www.moonofalabama.org )
20200602 : Unnatural end of social distancing: Where do this week's riots leave 'social distancing'? www.rt.com )
20200526 : COVID19 New Practical Results on Airborne Transmission Indoors by Lambert Strether ( May 25, 2020 , www.nakedcapitalism.com )
20200525 : Two postulates of the establishment's propaganda on coronavirus www.moonofalabama.org )
20200524* Private Equity Is Ruining Health Care, Covid Is Making It Worse: Investors have been buying up doctor s offices, cutting costs, and, critics say, putting pressure on physicians by Heather Perlberg ( May 20, 2020 , www.bloomberg.com ) [Recommended] 20200523 : The more you know Over a third of Americans apprehensive about Covid-19 vaccine, citing rushed development trust issues -- RT www.rt.com )
20200522 : Global report: don't count on vaccine, US scientist warns, as cases pass 5m www.theguardian.com )
20200522 : Washington State conned out of a likely 'hundreds of millions of dollars' by Nigerian scammers www.rt.com )
20200522 : Washington officials admit to counting GUNSHOT DEATHS in Covid-19 tally, say virus death toll likely underreported despite lapses www.rt.com )
20200510 : Can pulse oximeters detect coronavirus How they work and more by Dale Smith ( May 08, 2020 , www.cnet.com )
20200507 : Coronavirus Mutates Into Now-Dominant, More Contagious Form As Doctors Ponder 'East Coast vs. West Coast' Strains www.zerohedge.com )
20200507 : SARS-CoV-2 is so good at infecting the upper respiratory tract that there might even be a second receptor that the virus could use to launch its attack. www.unz.com )
20200507 : A new strain has come Meet Spike D614G, the new improved coronavirus www.rt.com )
20200506 : The accuracy of existing tests used to detect COVID-19 is at 70%-80% thenewkremlinstooge.wordpress.com )
20200506 : Russian virusolog about an interesting form of institutional idiotism: enforcing wearing of masks outside closed spaces vz.ru )
20200505 : There may be hope in an engineered antibody that targets the viral spike protein www.moonofalabama.org )
20200505 : What does an anti-body test do? turcopolier.typepad.com )
20200503 : GSK partnered with Bill Gates to produce the Covid-19 Vaccine. GSK has been found guilty for several criminal federal offenses, bribes and health violations, and paid Billions in lawsuits including for birth defects brain damage. twitter.com )
20200503 : The spike elements of SARS-CoV-2 coronavirus are mutating www.moonofalabama.org )
20200503 : Ignorant Italians majors do not understand that 99% of coronavirus infections happened in closed spaces. www.youtube.com )
20200430 : The danger of untested vaccine for coronavirus. Rumsfeld and Geliad. We need a new definition for the term vulture capitalist. www.moonofalabama.org )
20200429 : The number who fist responders tested positive fpr coronavirus antibodies is 10% for NYPD and 17% for FDNY/EMP www.zerohedge.com )
20200428 : Four of the coronavirus antibody tests produced false-positive rates ranging from 11 percent to 16 percent; many of the rest hovered around 5 percent www.nytimes.com )
20200428* Consumer Beware Coronavirus Antibody Tests Are Still A Work In Progress ( Apr 28, 2020 , www.nakedcapitalism.com ) [Recommended] 20200428* Coronavirus Fact-Check #4: "Why are so many healthcare workers dying?" ( Apr 28, 2020 , off-guardian.org ) [Recommended] 20200428* Who is at RISK from COVID-19 -- UK DOCTOR -- Covid-19 Vlog #15 ( Apr 28, 2020 , www.youtube.com ) [Recommended] 20200426* Who is an idiot here: What's not fair is that you go out running, you bloody idiot! shouted a Spanish woman apparently filming the encounter ( Apr 26, 2020 , en.as.com ) [Recommended] 20200425 : Watching a fight yesterday in Walmart between couple of fat American female over bathroom tissue www.zerohedge.com )
20200419 : I can take it off if you'd like twitter.com )
20200419 : Greatest health care system in the world: twitter.com )
20200418 : As one caustic virologist observed, getting out into the open air is a good defense against respiratory transmitted infections: avoiding infection is a walk in the park www.unz.com )
20200413* American health care, as we call it today, and for all its high-tech miracles, has evolved into one of the most atrocious rackets the world has ever seen. By racket, I mean an enterprise organized explicitly to make money dishonestly by James Howard Kunstler ( Apr 13, 2020 , www.zerohedge.com ) [Recommended] 20200413* The Whistle-giver: the story of Ai Fen, the director of the emergency department of Wuhan Central Hospital ( Apr 13, 2020 , scienceintegritydigest.com ) [Recommended] 20200411* The country that glorifies profit at any cost and ruthless unethical competition will fare bad in case of any virus epidemic. That includes "Typhoid Mary" cases of selfish anti-social behaviour ( Apr 11, 2020 , www.moonofalabama.org ) [Recommended] 20200411* 'Never in my country': COVID-19 and American exceptionalism by Jeanne Morefield ( Apr 07, 2020 , responsiblestatecraft.org ) [Recommended] 20200410* Tucker: In crisis, nothing is more important than staying connected to reality ( Apr 10, 2020 , www.youtube.com ) [Recommended] 20200409* And b has posted previously directions for making masks. The advantage is you can throw them in the washing machine to clean, or even hand wash as they are small items ( Apr 09, 2020 , www.moonofalabama.org ) [Recommended] 20200406* Wearing a mask is a rare case when a selfish motive to save your own life produce a greater good ( Apr 06, 2020 , www.unz.com ) [Recommended] 20200405* The big mistake in the U.S. and Europe, in my opinion, is that people aren't wearing masks ( Apr 05, 2020 , www.sciencemag.org ) [Recommended] 20200330* If you get COVID-19 infection in the shop, office or transport, you probably will be sick two weeks, but if you get if from your wife - probably four, and mother-in-law -- six ( Mar 30, 2020 , time.com ) [Recommended] 20200329* Why Didn't We Test Our Trade's 'Antifragility' Before COVID-19 by Gene Callahan and Joe Norman ( Mar 28, 2020 , www.theamericanconservative.com ) [Recommended] 20200328 : Meet The 'Covidiot' A Dense Creature That Ignores Simple Instructions, Endangers Others www.zerohedge.com )
20200328 : No Refunds: Costco Hoarders Discover They Can't Return Toilet Paper www.zerohedge.com )
20200328 : What I have found when yesterday I ventured into Wal-Mart to shop with the other deplorable people that the elite child molesters, sexual perverts, and sociopaths out in Hollyweird, NYC and Washington like to look down on www.unz.com )
20200327* Not Just China U.S. Reliance on Foreign Medical Supplies is Staggering by Alan Tonelson ( Mar 27, 2020 , www.theamericanconservative.com ) [Recommended] 20200326* Reflections on a Century of Junk Science ( Mar 26, 2020 , www.unz.com ) [Recommended] 20200324* The US Department of Justice announced Sunday it had shut down a website claiming to sell a coronavirus vaccine ( Mar 22, 2020 , news.yahoo.com ) [Recommended] 20200324* Joe Rogan Experience #1439 - Michael Osterholm ( Mar 24, 2020 , www.youtube.com ) [Recommended] 20200322* Intelligence agencies and the virus ( Mar 22, 2020 , www.moonofalabama.org ) [Recommended] 20200321* Tucker Senator Burr sold shares after virus briefing ( Mar 21, 2020 , www.youtube.com ) [Recommended] 20200321* Don't forget our congress critter Senator Kelly Loeffler ( Mar 21, 2020 , caucus99percent.com ) [Recommended] 20200319* I look to the narrative we get in North America, irrespective of the topic, and the pattern is the same ( Mar 19, 2020 , www.unz.com ) [Recommended] 20200316* The USA now experience the period when the medical personnel became the most prominent victim of the authorities incompetence ( Mar 15, 2020 , angrybearblog.com ) [Recommended] 20200314 : Neoliberal civilization depends on toilet paper it seems. Toilet paper is the bellwether commodity of our age www.moonofalabama.org )
20200314* Honest Government Ad ( Mar 14, 2020 , youtu.be ) [Recommended] 20200312 : Italy Closed; Wall Street Hosed; Trump Exposed www.medpagetoday.com )
20200311* Joe Rogan interview today with Michael Osterholm is an internationally recognized expert in infectious disease epidemiology ( Mar 11, 2020 , www.moonofalabama.org ) [Recommended] 20200310 : How US counts the sick when CDC test kits are unreliable amd by-and-large unavailble? www.moonofalabama.org )
20200310 : Facebook and idiocy of population www.moonofalabama.org )
20200310* Soap is probably more effective or as effective against COVID-19 as alcohol-based hand sanitizer ( Mar 10, 2020 , www.moonofalabama.org ) [Recommended] 20200309 : The Great Chinese Bat Flu Panic of 2020 Dissident Voice dissidentvoice.org )
20200309 : Simply 17 coronavirus jokes to help take the edge off (a little bit) The Poke thepoke.co.uk )
20200309* COVID-19 and the Working Class by Jack Rasmus ( Mar 09, 2020 , www.counterpunch.org ) [Recommended] 20200309* Momento Mori - Unpopular Thoughts on Corona Virus by Craig Murray ( Mar 09, 2020 , craigmurray.org.uk ) [Recommended] 20200307 : Stealing sanitizer from clinics www.theamericanconservative.com )
20200307 : Funny, I thought conservatives told us that empty shelves and sky-high black market prices only happen when socialists are in charge. www.theamericanconservative.com )
20200307 : CDC Catch 22 www.theamericanconservative.com )
20200307 : At least if we're all gonna die of coronavirus, there's no point in worrying about climate change www.theamericanconservative.com )
20200307 : Silver lining in the dark cloud www.nakedcapitalism.com )
20200307* The Neoliberal Plague by Rob Urie ( Mar 07, 2020 , www.counterpunch.org ) [Recommended] 20200304* Why Are We Being Charged? Surprise Bills From Coronavirus Testing Spark Calls for Government to Cover All Costs by Jake Johnson ( Mar 03, 2020 , www.commondreams.org ) [Recommended] 20200304* Nowcasting COVID-19 for public health control: learning from the Chinese experience for global preparedness by Gabriel Leung ( Feb 27, 2020 , lshtm.ac.uk ) [Recommended] 20200303* Coronavirus hype vs reality ( Mar 03, 2020 , angrybearblog.com ) [Recommended] 20200228 : The 20th century model of [pandemic] containment was protecting lives. The 21st century model is protecting markets www.nakedcapitalism.com )
20200228 : No matter what happens with the coronavirus, I'm sure Trump has it under control by Alexandra Petri ( Feb 27, 2020 , www.washingtonpost.com )
20200228* The impact of coronavirus on Trump reelection chances ( Feb 28, 2020 , angrybearblog.com ) [Recommended] 20200226 : Studying the mortality stats, at first glance, this looks like a sound chemical attempt to resolve the pension fund crisis off-guardian.org )
20200225* Coronavirus Hysteria reaches tipping point by Catte Black ( Feb 25, 2020 , off-guardian.org ) [Recommended] 20200223 : Intelligence agencies who invested hundred of millions in face recognition technology will not be happy www.zerohedge.com )
20200215 : A strong argument against "bioweapon origin of Coronavirus" www.unz.com )
20190909 : Will NPR Now Officially Change Its Name to National Propaganda Radio? by Edward Curtin ( Sep 08, 2019 , off-guardian.org )
20190723 : Some thoughts about Mueller testimony turcopolier.typepad.com )
20190627 : Something about neoliberal MSM www.moonofalabama.org )
20190131 : Do you think that the Guardian will shortly report that Iraq's WMD were snuck out of Iraq and hidden in Venezuela all those years ago? www.nakedcapitalism.com )
[an error occurred while processing this directive]
Aug 10, 2021
I'm not vaccinated against COVID-19. The decision wasn't a drastic one; I thought of it as a
personal decision that every person should make in consultation with a trusted health
professional, which is what I did. It didn't occur to me that this decision merited
justification to others. But that was before the current climate of social and political
pressure, before the Delta surge, and before unvaccinated people like me started getting blamed
for vaccine-resistant variants. Now I feel that explaining my decision has become
necessary.
In explaining my decision, my hope is not to convince people to change their
minds about whether to vaccinate but rather to help others understand why some may choose
differently.
Let me start by saying that I agree that the COVID-19 vaccine is an important tool in
reducing the severity of cases, hospitalizations, and deaths due to COVID-19. In general, I am
supportive of the availability and accessibility of safe, potentially life saving medications
and preventative measures for anyone at risk of any serious illness. The more options when it
comes to preventing and treating COVID-19, the better! But this does not mean that all options
should necessarily be utilized by all people en masse, and this is how I arrived at my current
decision to opt out of the vaccine.
The reported adverse events and risks of the authorized COVID-19 vaccines are rare, and
most people don't seem to have any serious adverse reactions. But though rare, the risks are
still real . Cardiac issues, blood clotting, stroke, and autoimmune disorders are all
acknowledged adverse events that can occur as a result of the COVID-19 vaccine.
A colleague of my parents reportedly died from complications of the Moderna vaccine, a
friend suffered from deep vein thrombosis, and a teenage nephew of another friend now has
chronic cardiac issues. These are three examples from my immediate network of family and
friends, and I know many others with their own stories. And while it's true that these are
anecdotes and do not represent the majority, they are powerful nonetheless.
Now, we know that age, weight, and other comorbidities play a role in how COVID-19 impacts
the individual, and for someone at serious risk from COVID-19, these rare risks are probably
worth it. But what about for someone who is not at risk from COVID-19? The risk/benefit
analysis for otherwise healthy, young individuals may be a different calculus.
Public health messaging has consistently portrayed the vaccines are safe and effective, and
therefore everyone eligible should get vaccinated. But companies like Moderna and Pfizer are protected from lawsuits
related to their COVID-19 vaccines until 2024.
It's just one of the many facets of the inconsistent public health messaging and moving of
goalposts when it comes to the vaccine and herd immunity, which makes it hard to trust such
guidance. A cocktail of mixed messages on who is at risk from COVID-19 and dubious masking
guidance coupled with a lack of clear messaging on what exactly is the goal and rationale of
these measures and policies adds to the skepticism many of us feel. The focus has now
shifted from deaths and hospitalizations due to COVID-19 to a new hyper-focus on breakthrough
cases, though the majority of them are benign.
But even while the experts push the vaccine, they have undermined it by arguing that
vaccinated individuals spread the virus as effectively as unvaccinated individuals. It begs the
question: If everyone now has to wear a mask because everyone is now back to being suspected
asymptomatic carriers, why get the vaccine at all?
The personal risk/benefit analysis still plays a role and preventing serious illness is
definitely important, but getting the vaccine to protect others (and calling unvaccinated
adults selfish) no longer seems to be relevant if the vaccinated can spread it, too. In
fact, some experts have advised only individuals at high risk of serious illness from COVID-19
to get vaccinated, in order to prevent the evolution of even more vaccine resistant
variants.
Along with the mixed messages is the obvious role that politics has played in COVID-19
policy. There was Kamala
Harris saying she wouldn't trust a vaccine produced by President Trump -- then doing an
about face. There was the way that Democratic politicians and even the CDC itself justifying Black Lives Matter protests
during lockdown while criticizing Trump rallies as "super spreader" events. Most recently
former President Obama hosted a huge, maskless birthday party in the midst of renewed mask
mandates and concern over the spread of infection.
The inconsistent policies and public responses, the repeated "do as I say, not as I do" from
those pushing restrictions, has led many like me to skepticism of any government issued
guidance. And adding bribes, mandates, and censorship to the mix has only served to heighten
that sense of mistrust. Perhaps most unnerving has been seeing experts who question and warn
about adverse reactions to the vaccine being censored or blacklisted.
Why censor the adverse effects? Why not publicize them so we can make informed
decisions?
Still, I didn't arrive at my decision on my own. I am lucky to have a relationship with a
health professional who I feel comfortable asking questions without fear of judgment. I trust
her guidance, having built a history with her and knowing that she has my best interests in
mind. In fact, had she unequivocally recommended the vaccine specifically for me to the best of
her clinical judgment, I would have gotten vaccinated that day.
Unequivocal recommendation, however, was not the message I received in my case as a young,
otherwise healthy individual, who was also pregnant.
Another doctor I consulted with also generally recommends vaccination, but added that in my
case, the concerns are understandable and waiting made sense. He connected me with an
obstetrics clinic that has experience treating COVID-19 in pregnancy in the event I should
require it, since the location where I normally receive medical care does not offer treatment
unless hospitalization is required.
The bottom line for me, and perhaps others who are similarly ambivalent about the COVID-19
vaccine, is that trustworthy information and guidance is key. And those of us opting out of the
vaccine are not doing so out of ignorance or selfishness. We have simply been paying attention
to the mixed messages, the hypocrisy, the changing standards, and the censoring of
counter-evidence. And we have not been convinced that this is something we need to do, for our
own good or that of our communities or country.
The COVID-19 vaccine remains one effective tool among many in the fight against COVID-19.
Clear, transparent information about what the vaccine does, what its risks and limitations are,
and what other options exist especially for prevention and early outpatient treatment are what
is needed to restore trust.
The mandates, bribes, social pressure, censorship, and ever changing policies that don't
present clear scientific rationale need to stop. But at least the doctor/patient relationship
should be prioritized in the meantime, so that we as individuals can make informed decisions
for ourselves, enabling us all to emerge sooner rather than later from this seemingly never
ending health crisis.
Suri Kinzbrunner previously worked as a teacher and preschool director and is
currently homeschooling her 7 children. She studied cognitive neuroscience as an undergraduate
at the George Washington University in Washington D.C. and worked briefly in this field before
becoming a parent. She is especially passionate about issues related to parenting and
education.
The views in this article are the writer's own.
According to Reuters ,
three new conditions have been reported by a small number of people after vaccination with jabs
from Pfizer and Moderna. The ailments include Erythema multiforme, a form of allergic skin
reaction; glomerulonephritis, or kidney inflammation; and nephrotic syndrome, a renal disorder
that leads to heavy urinary protein losses. All of the cases are being studied by the EMA to
determine whether the vaccines might be linked to the conditions.
That probably is not true for Delta variant. Israel data suggest that it stops to something
between 60and 70 percents. So approximately one third of vaccinated can be infected with
Delta.
The effectiveness of Pfizer's COVID-19 shot can drop to 83.7% within four to six months
after getting the second dose of its vaccine. This is the latest indication that
vaccine-induced immunity to the virus can wane and some kind of boost may be necessary in the
future.
New research published Wednesday as a preprint indicates that the Pfizer Inc. shot provides
96.2% protection for the first two months, 90.1% effectiveness between the second and fourth
months, and 83.7% of protection for the fourth, fifth, and six months.
"We will need a booster eight to 12 months from the second dose," Pfizer CEO Albert Bourla
said Wednesday, according to a FactSet transcript of the company's second-quarter earnings
call.
The drug maker has been making the case for booster shots, citing limited data from its own
clinical research and real-world data out of Israel, where Pfizer's vaccine is the predominant
shot in circulation.
... ... ...
When speaking to investors this week, company officials attributed waning immunity levels in
Israel to the much earlier vaccination campaign that rolled out in that country. (In fact,
Israel announced Thursday that a third dose will now be available to people who are at least
60.) Pfizer also mentioned that there will be data in a few months coming out of the U.K.,
where doses were sometimes spaced out, that indicates "long-lasting protection."
... ... ...
Pfizer is expected to generate $33.5 billion in COVID-19 vaccine revenue this year, and Wall
Street analysts have already baked boosters into their financial models for Pfizer and BioNTech
SE which developed the vaccine with Pfizer.
"The largest remaining uncertainty is whether this third boost is simply the third dose in a
three-vaccine schedule to achieve lasting, broad protection or is the first of a periodic
(annual) boosted vaccine," SVB Leerink analysts told investors on Thursday.
The fact Delta remains dominant worldwide, and this is a sign Delta Plus might not overtake
it soon. Delta Plus (also known as AY.1) has an extra mutation in the code for its spike protein,
which helps the coronavirus access human cells. India's health ministry said last month that
Delta Plus appeared to spread more easily than Delta and might be able to bind more easily to
lung cells or resist antibody drugs.
In the US, Delta Plus cases peaked in late June at less than 5% of the nation's sequenced
cases, according to Outbreak.info .
Health experts say it's a sign Delta Plus isn't outcompeting other variants.
Public Health England suggested June that there was no evidence Delta Plus' extra mutation
made the virus any more severe or reduced vaccine effectiveness relative to Delta.
While Delta seems to have challenged how well vaccines prevent infection and transmission,
recent CDC data indicates coronavirus shots still reduce the risk of getting COVID-19 several
times, and the risk of hospitalization or death by vaccinated within the last six months by an
order of magnitude, although the protective effect of Pfizer and other vaccines fade with
time.
On Tuesday South Korea announced that it had detected two cases of the Delta Plus variant,
one in a man who had recently returned from the U.S.,
Reuters reports. Some experts believe the Delta Plus variant could be more contagious than
the Delta variant.
The Lambda variant, which originated from Peru last year, has
already been detected in the U.S.
Recent studies indicated that Lambda could be more resistant to the current COVID-19
vaccines, according to
Reuters .
The Centers for Disease
Control Prevention has a COVID-19 case tracker
that shows the percent of the total population vaccinated against COVID-19. The map shows the
percent of the total population fully vaccinated and then compares it with the cases per
100,000 people.
For example, much of the Northeast has a high number of vaccinations and low number of
cases per 100,000 people. So the area is green on the map.
However, the Southeastern U.S. is mainly colored in red due to low vaccinations and a
high number of people infected.
... ... ...
The CDC advises caution about
traveling to areas with low vaccination rates and a higher number of cases per 100,000
people.
Something very strange has been happening in Missouri: A hospital in the state, Ozarks
Healthcare, had to create a "private setting" for patients afraid of being seen getting
vaccinated against COVID-19. In a video produced by the hospital, the physician Priscilla Frase
says, "Several people come in to get vaccinated who have tried to sort of disguise their
appearance and even went so far as to say, 'Please, please, please don't let anybody know that
I got this vaccine.'" Although they want to protect themselves from the coronavirus and its
variants, these patients are desperate to ensure that their vaccine-skeptical friends and
family never find out what they have done.
The Atlantic Missouri is suffering one of the worst COVID-19 surges in the country. Some
hospitals are rapidly running out of ICU beds. To Americans who rushed to get vaccinated at the
earliest opportunity, some Missourians' desire for secrecy is difficult to understand. It's
also difficult to square with the common narrative that vaccine refusal, at least in
conservative areas of the country, is driven by a lack of respect or empathy from liberals
along the coasts. "Proponents of the vaccine are unwilling or unable to understand the thinking
of vaccine skeptics -- or even admit that skeptics may be thinking at all," lamented a recent
article in the conservative National Review.
Writers across the political spectrum have urged deference and sympathy toward holdouts'
concerns about vaccine side effects and the botched CDC messaging about masking and airborne
transmission early in the pandemic. But these takes can't explain why holdouts who receive
respect, empathy, and information directly from reliable sources remain unmoved -- or why some
people are afraid to tell their loved ones about being vaccinated.
What is going on here? Sociology suggests that pundits and policy makers have been looking
at vaccine refusal all wrong: It's not an individual problem, but a social one. That's why
individual information outreach and individual incentives -- such as Ohio's Vax-a-Million
program, intended to increase vaccine uptake with cash prizes and college scholarships --
haven't worked. Pandemics, by definition, are collective problems. They propagate and kill
because people live in communities. As a result, addressing pandemics requires understanding
interpersonal dynamics -- not just what promotes trust among people, but which behaviors convey
status or lead to ostracism.
Shifting from an individual to a relational perspective helps us understand why people
are seeking vaccination in disguise. They want to save face within the very specific set of
social ties that sociologists call "reference groups" -- the neighborhoods, churches,
workplaces, and friendship networks that help people obtain the income, information,
companionship, mutual aid, and other resources they need to live. The price of access to those
resources is conformity to group norms. That's why nobody strives for the good opinion of
everyone; most people primarily seek the approval of people in their own reference
groups.
An analysis by British academics, published by the UK Government's official scientific
advisory group, says that they believe it is "almost certain" that a SARS-Cov-2 variant will
emerge that "leads to current vaccine failure." SARS-CoV-2 is the virus that causes
Covid-19.
The analysis has not been peer-reviewed, the early research is theoretical, and does not
provide any proof that such a variant is in circulation now. Documents like it are released "as
pre-print publications that have provided the government with rapid evidence during an
emergency."
The paper is dated July 26, and was published by the British government on Friday.
The scientists write that because eradication of the virus is "unlikely," they have "high
confidence" that variants will continue to emerge. They say it is "almost certain" that there
will be "a gradual or punctuated accumulation of antigenic variation that eventually leads to
current vaccine failure."
They recommend that authorities continue to reduce virus transmission as much as possible to
reduce the chance of a new, vaccine-resistant variant.
They also recommend that research focus on new vaccines that not only prevent hospital
admission and disease, but also "induce high and durable levels of mucosal immunity."
The goal, they say, should be "to reduce infection of and transmission from vaccinated
individuals," and to "reduce the possibility of variant selection in vaccinated individuals."
Research is already underway at several companies that make the Covid-19 vaccines to address
new variants.
The views were expressed in a paper "by group of academics on scenarios for the longer
term evolution of SARS-CoV-2," and discussed and published by the UK's Scientific Advisory
Group for Emergencies (SAGE).
They write that some variants that have emerged over the past few months "show a reduced
susceptibility to vaccine-acquired immunity, though none appears to escape entirely."
But they caution that these variants emerged "before vaccination was widespread," and that
"as vaccines become more widespread, the transmission advantage gained by a virus that can
evade vaccine-acquired immunity will increase."
This is an issue that SAGE has warned about before.
In minutes from its July 7 meeting, SAGE scientists wrote that "the combination of high
prevalence and high levels of vaccination creates the conditions in which an immune escape
variant is most likely to emerge." It said at the time that "the likelihood of this happening
is unknown, but such a variant would present a significant risk both in the UK and
internationally."
Hundreds of staffers at two major hospitals in San Francisco have tested positive for
coronavirus in July, with most of them being breakthrough cases of the highly infectious Delta
variant, The New York
Times reported Saturday evening.
The University of California, San Francisco Medical Center told media outlets that 183 of
its 35,000 staffers tested positive. Of those infected, 84% were fully vaccinated, and just two
vaccinated staff members required hospitalization for their symptoms.
At Zuckerberg San Francisco General Hospital, at least 50 members out of the total 7,500
hospital staff were infected, with 75-80% of them vaccinated. None of those staffers required
hospitalization.
... ... ...
Day also
told ABC7 News that at least 99% of the cases at UCSF were traced back to community spread,
but that hospital officials are still investigating and conducting contact tracing.
He added that most of the cases presented mild to moderate symptoms, and some were
completely asymptomatic. He said the cases were spread among doctors, nurses, and ancillary
staff.
"We sort of are seeing that across the board," he said. "We have so far not detected any
patient-to-staff or staff-to-patient transmission right now."
The Delta variant has also been known to spread among vaccinated people in breakthrough
cases, prompting the agency this week to recommend that even fully vaccinated people
wear masks indoors in areas with high transmission rates.
The CDC emphasized that getting vaccinated is still highly beneficial and is a crucial
component to combatting the coronavirus - even the Delta variant.
"Getting vaccinated continues to prevent severe illness, hospitalization, and death, even
with Delta," CDC Director Rochelle Walensky told media on Tuesday.
4 This is what Republicans said as Capitol police told their stories on the Hill Russia
Calls Joe Biden's Comments on Nation's Economy 'Inherently
A reversal in federal health guidance calling for fully vaccinated individuals to don masks
in certain indoor areas amid high and substantial viral spread has left some experts
divided.
The Centers for Disease Control and Prevention (CDC) rolled out the latest guidance on
Tuesday, with agency head Dr. Rochelle Walensky citing "worrisome" new science necessitating
the update.
"In recent days, I have seen new scientific data from sequenced outbreak investigations
showing that the delta variant behaves uniquely differently from past strains of the virus that
cause COVID-19," Walensky told reporters over a call. "Information on the delta variant from
several states and other countries indicate that in rare occasions, some vaccinated people
infected with the delta variant after vaccination may be contagious and spread the virus to
others."
Notable quotes:
"... If there's any demographic that isn't at risk, it's children. Children were never an issue when it came to COVID. Their caseload was never the majority, the plurality, or even a fraction that you could call 'significant.' ..."
"... If they do contract COVID, it's usually not a bad case. A child's survival rate is a whopping 99.995 percent when it comes to infection. They're virtually bulletproof. ..."
"... Since the start of the pandemic, only 335 kids under the age of 18 have died from COVID. Is one too many? Of course. It's tragic but hardly cause for a national panic. By this logic, we can no longer drive automobiles. Too much death. ..."
"... Schools have also never been a source of super spread. The schools in Irvine, California reopened in September of 2020. A report last March noted at the time, that of the 23,000 students in the Irvine School District, just 17 contracted COVID. How many of the 3,000 employees? Only three. And this was when the vaccine was not readily available. ..."
"... Should people still be careful? Sure, but this isn't a 'Apocalypse Now' mentality. ..."
They have nowhere to go. The liberal media and the experts see another avenue to lock us
down -- and they're going full bore. The Delta variant, which doesn't make you sicker nor is it
more lethal, is a problem for the unvaccinated. But we're not locking down again. No way.
There's a midterm election coming up, so no -- not even Joe Biden is going to back such a move.
It's the same reason why there will be no mandatory vaccination protocol. There's an election
coming up. If this were a national emergency, politics be damned -- everyone gets a shot,
right? They're readily available to everyone who can get them. That should be the mindset. It's
not. Why? Because obviously, it's not a do-or-die situation. If a mandatory vaccination mandate
is being kept in the desk until after an election, it's all politics. We've known this for
months.
And now, they're trying to gaslight us on children and COVID. Fellas, I have bad news. We've
been paying attention. If there's any demographic that isn't at risk, it's children.
Children were never an issue when it came to COVID. Their caseload was never the majority, the
plurality, or even a fraction that you could call 'significant.' This notion that children
are under threat is science fiction and it doesn't help that a hyper-partisan Surgeon General,
Vivek Murthy, who was not shy about wanting to declare gun violence a national health issue, is
peddling this fearmongering.
The science is clear. Children generally do not get it or spread it. If they do contract
COVID, it's usually not a bad case. A child's survival rate is a whopping 99.995 percent when
it comes to infection. They're virtually bulletproof.
Since the start of the pandemic, only 335 kids under the age of 18 have died from COVID.
Is one too many? Of course. It's tragic but hardly cause for a national panic. By this logic,
we can no longer drive automobiles. Too much death.
Schools have also never been a source of super spread. The schools in Irvine, California
reopened in September of 2020. A report last March noted at the time, that of the 23,000
students in the Irvine School District,
just 17 contracted COVID. How many of the 3,000 employees? Only three. And this was when
the vaccine was not readily available.
The vaccines right now are not available for kids under the age of 12. They're not at-risk.
They're not carriers. Should people still be careful? Sure, but this isn't a 'Apocalypse
Now' mentality. Also, the store-bought masks that people, like Fauci, are saying kids
under three should wear don't stop the spread of COVID. Fauci mentioned
that in his emails .
After the virus infects a person itdoes not care whther the person vaccinated or not. The
person spread virus like any other infected person, depending of course on the severity of
symptoms, which supposedly should be lighter n vaccinated people. Is this so difficult to
understand that for vitus any infected person is a lunchpad for infections, vaccinated or
unvaccinated... A lot of pseudoscience is typical for neoliberal MSM.
Data from the U.S. Centers for Disease Control and Prevention (CDC) shows that the Delta
variant of COVID-19 is equally contagious whether it's contracted by a vaccinated or
unvaccinated person.
A week after the crowds descended upon Provincetown, Massachusetts, to celebrate the Fourth
of July -- the holiday President Joe Biden hoped would mark the nation's liberation from
COVID-19 -- the manager of the Cape Cod beach town said he was aware of "a handful of positive
COVID cases among folks" who spent time there.
"We are in touch with the Health Department and Outer Cape Health Services and are closely
monitoring the data," Alex Morse told reporters.
The announcement wasn't unusual with roughly half of the country still unvaccinated and
flare-ups of the virus popping up in various states.
But within weeks, health officials seemed to be on to something much bigger. The outbreak
quickly grew to the hundreds and most of them appeared to be vaccinated.
MORE:
Vast majority of ICU patients with COVID-19 are unvaccinated, ABC News survey finds
As of Thursday, 882 people were tied to the Provincetown outbreak. Among those living in
Massachusetts, 74% of them were fully immunized, yet officials said the vast majority were also
reporting symptoms. Seven people were reported hospitalized.
The initial findings of the investigation led by the Massachusetts Department of Public
Health, in conjunction with the Centers for Disease Control and Prevention, seemed to have huge
implications.
CDC Warns Vaccinated People Can Pass COVID to Others Even if you're vaccinated, you should
wear a mask in places of high transmissibility -- and you could give COVID to someone else.
These eyebrow-raising facts were revealed yesterday by the CDC.
In response, CDC Director Dr. Rochelle Walensky joined SiriusXM's Doctor Radio Reports and
opened up to show host Dr. Marc Siegel about the delta variant and evidence that it's something
that fully vaccinated people may pass along to others, and the idea of making COVID-19 vaccines
mandatory.
Read on for five live-saving pieces of advice -- and to ensure your health and the health of
others, don't miss these:
Sure Signs You Have "Long" COVID and May Not Even Know It .
Their work is funded through a more than $300,000 contract with the city. The Missouri
Department of Health and Senior Services with the University of Missouri is assisting in
analyzing the data, through a
$2 million National Institutes of Health grant .
The team began testing rat feces for the coronavirus to see whether that was the source of
the new spike protein mutations -- but nothing matched their initial finding.
They then surveyed the sewage, using a process called "deep sequencing," for animal DNA.
They found evidence of various mammals, such as cows, pigs and sheep, which likely came from
human food consumption, along with evidence of dogs, cats and rats.
But most of the mutations were found over three different wastewater plants spanning months.
That meant the "animal reservoir" would have to be living in or near the sewershed; largely
constrained to their geographic location; and in big enough numbers to sustain an epidemic for
six months.
The most likely culprits: rats and dogs.
"These novel lineages could be relevant to public health and necessitate further study," the
researchers wrote in the study.
As for the mutations themselves, their origin remains an open question.
The researchers hypothesize that since not all COVID-19 cases were diagnosed and not all
positive samples were sequenced, the "cryptic lineages" could come from "asymptomatic,
vaccinated, immunosuppressed, pediatric, or chronically infected patients who are not being
sampled in clinical settings."
COVID-19 could also linger in different areas of the body, such as the gut, long after it's
been cleared in other areas, like the respiratory tract -- potentially explaining the presence
in wastewater.
... ... ...
Signs of More Rats
If the new spike protein mutations the researchers discovered points to an outbreak of
coronavirus among city rats, they would not be the first animal to contract the virus.
There have been reports of dogs, cats and even a New York City tiger catching the virus,
according to the CDC .
A
study published Wednesday by the U.S. Department of Agriculture's Animal and Plant Health
Inspection Service found that white-tailed deer populations in New York, Michigan, Illinois and
Pennsylvania had coronavirus antibodies, meaning they had previously contracted the virus,
although they did not show signs of an active infection.
In November,
Denmark culled 17 million minks after the virus jumped from a human handler to the minks,
then back to humans. In Michigan, a taxidermist became infected with coronavirus and, after his
test results were sent to a lab, it was determined that there was a mutation in his sample that
came from an infected mink.
The authors of this study reported that the WT strain of SARS-CoV-2 was best neutralized by
Natural Infection 2020 when compared to CoronaVac and Natural Infection 2021 sera. However, the
Alpha variant was best neutralized by Natural Infection 2021 sera, when compared to CoronaVac
and Natural Infection 2020 sera.
In the case of the Beta variant, this form of SARS-CoV-2 was best neutralized by Natural
Infection 2020 and 2021 sera with higher NAb titer levels. Although the Delta variant was
neutralized well by Natural Infection 2020 and 2021 sera, levels of NAb titers were much lower
when compared with the Alpha and Beta variants.
In summary, the results of the current study indicate that NAb titers elicited by CoronaVac
are much lower when compared to natural infection.
If a vaccinated person experiences any symptoms of COVID-19 listed by the CDC, the public
health agency recommends getting tested and isolating from others until a result is received.
If the test is positive, an infected vaccinated person should isolate at home for 10 days.
According to the CDC's guidelines
for the fully vaccinated, those infected with the delta variant can spread it to
others.
The existence of breakthrough cases doesn't mean that vaccines aren't doing their job,
experts say. In fact, merely coming down with a mild infection rather than a severe one is
often evidence that the vaccine is doing its job in helping your immune system fight the virus.
Since the existing vaccines were developed to combat the alpha variant of SARS-CoV-2, it makes
sense that they're not as effective in combating the delta variant, whose mutations have shown
to some extent to evade the immune response from the vaccines. Yet all the COVID-19 vaccines
are mostly able to stop the infection worsening.
"In a vaccinated person, what will happen is that we already have cells that very
specifically recognize an infected cell, and can aggressively target that infection so that the
virus can no longer replicate," said Dr. Nicole Baumgarth, a professor of Immunology and
Infectious Diseases at University of California–Davis. "Even if we cannot stop the
infection from happening, [the vaccine] stops it very early in its tracks; the less virus
replication you have, the less symptoms you will have, the less disease and it gets easier for
the immune system to mop up the little bit of virus."
Signs of infection, like a fever, develop when the immune system has been activated to fight
it.
"Some of the signs of disease are actually signs that the immune system has been activated,"
Baumgarth said. "That's one response to the body to fight the viruses, to increase the
temperature."
Baumgarth said it is in fact accurate to think of a breakthrough infection as a "booster
shot." However, Baumgarth would not advocate for people to purposely expose themselves to the
virus. Yet a mild breakthrough case does build one's immunity against the virus.
Of course, given the possibility of spreading the virus further, it is best not to get
infected at all.
Last week, Israel's health ministry
released preliminary data suggesting that the Pfizer-BioNTech COVID-19 vaccine's ability to
protect against a mild coronavirus infection may have decreased precipitously, even though it
remains effective against severe illness and death from COVID-19. The reason for the decrease
in the vaccine's effectiveness may be both because of transient immunity and the virulent
delta variant of SARS-CoV-2, which is more adept at overcoming the vaccine's defenses.
The delta variant is now the dominant strain of SARS-CoV-2 in Israel, where researchers now
estimate that the two-shot Pfizer vaccine is only 39% effective in preventing an infection
within the country. That is about half as effective as the vaccine was two weeks ago, when it
purportedly exhibited
64% effectiveness against coronavirus infection in Israel -- though at that point in time,
the delta variant was less widespread. Upon its public release in late 2020, Pfizer-BioNTech's
mRNA
vaccine was reported to have an efficacy of 95%.
On a positive note, research data shows that the Pfizer vaccine is still effective at
preventing serious illness; at least 88 percent effective in protecting against
hospitalization; and 91 percent effective at preventing severe illness.
The key issue problem is whether Delta can successfully spread in fully vaccinated
population? If the answer is yes, then the current policy is stupid. Another important question
is whether the current generation of vaccines provides any real benefits for people younger then
30?
In short, the article like this looks like another attempt to change the narrative as it
demonstrates abandonment of the previous idea of herd immunity. Suddenly, because of
proliferation of breakthrough infections, it is not longer a goal.
Post-vaccination infections, or breakthroughs,
might occasionally turn symptomatic , but they
aren't shameful or aberrant . They also aren't proof that the shots are failing .
These cases are, on average, gentler and less symptomatic;
faster-resolving, with less virus lingering -- and, it appears, less likely to pass the
pathogen on. The immunity offered by vaccines works in iterations and gradations, not
absolutes. It does not make a person completely impervious to infection. It also does not
evaporate when a few microbes breach a body's barriers. A breakthrough, despite what it might
seem, does not cause our defenses to crumble or even break ; it does not erase the
protection that's already been built. Rather than setting up fragile and penetrable shields,
vaccines reinforce the defenses we already have , so that we can encounter the virus
safely and potentially build further upon that protection.
To understand the anatomy of a breakthrough case, it's helpful to think of the human body as
a castle. Deepta Bhattacharya, an immunologist at the University of Arizona, compares
immunization to reinforcing such a stronghold against assault.
Without vaccination, the castle's defenders have no idea an attack is coming. They might
have stationed a few aggressive guard dogs outside, but these mutts aren't terribly discerning:
They're the system's
innate defenders , fast-acting and brutal, but short-lived and woefully imprecise.
They'll sink their teeth into anything they don't recognize, and are easily duped by stealthier
invaders. If only quarrelsome canines stand between the virus and the castle's treasures,
that's a pretty flimsy first line of defense. But it's essentially the situation that many
uninoculated people are in. Other fighters, who operate with more precision and punch -- the
body's adaptive
cells -- will eventually be roused. Without prior warning, though, they'll come out in full
force only after a weeks - long delay , by which time the virus
may have run roughshod over everything it can. At that point, the fight may, quite literally,
be at a fever pitch, fueling worsening symptoms.
Post-vaccination infections, or breakthroughs,
might occasionally turn symptomatic , but they
aren't shameful or aberrant . They also aren't proof that the shots are failing .
These cases are, on average, gentler and less symptomatic;
faster-resolving, with less virus lingering -- and, it appears, less likely to pass the
pathogen on. The immunity offered by vaccines works in iterations and gradations, not
absolutes. It does not make a person completely impervious to infection. It also does not
evaporate when a few microbes breach a body's barriers. A breakthrough, despite what it might
seem, does not cause our defenses to crumble or even break ; it does not erase the
protection that's already been built. Rather than setting up fragile and penetrable shields,
vaccines reinforce the defenses we already have , so that we can encounter the virus
safely and potentially build further upon that protection.
To understand the anatomy of a breakthrough case, it's helpful to think of the human body as
a castle. Deepta Bhattacharya, an immunologist at the University of Arizona, compares
immunization to reinforcing such a stronghold against assault.
Without vaccination, the castle's defenders have no idea an attack is coming. They might
have stationed a few aggressive guard dogs outside, but these mutts aren't terribly discerning:
They're the system's
innate defenders , fast-acting and brutal, but short-lived and woefully imprecise.
They'll sink their teeth into anything they don't recognize, and are easily duped by stealthier
invaders. If only quarrelsome canines stand between the virus and the castle's treasures,
that's a pretty flimsy first line of defense. But it's essentially the situation that many
uninoculated people are in. Other fighters, who operate with more precision and punch -- the
body's adaptive
cells -- will eventually be roused. Without prior warning, though, they'll come out in full
force only after a weeks - long delay , by which time the virus
may have run roughshod over everything it can. At that point, the fight may, quite literally,
be at a fever pitch, fueling worsening symptoms.
... ... ...
The choice isn't about getting vaccinated or getting infected. It's about
bolstering our defenses so that we are ready to fight an infection from the best position
possible -- with our defensive wits about us, and well-armored bodies in tow.
Three antiviral monoclonal antibody treatments to prevent severe Covid-19 and
hospitalization. Shipments of one such drug are paused because it wasn't effective against
variants, but doctors can continue prescribing the two others: Regeneron Pharmaceuticals
Inc.'s REGEN-COV and Vir Biotechnology Inc. and GlaxoSmithKline PLC's sotrovimab.
The antiviral remdesivir , made by Gilead Sciences Inc., to help clear the virus in
hospitalized patients.
Convalescent plasma , a highly concentrated solution of antibodies taken from recovered
Covid-19 patients, also for use in hospitals.
The immune-suppressing rheumatoid arthritis drugs baricitinib and tocilizumab , to rein
in the potentially lethal inflammation experienced by many hospitalized patients.
Dexamethasone , a generic steroid, recommended for use in severely ill patients. It is
now the most common treatment in hospitalized patients.
Notable quotes:
"... Federal officials concentrated their resources on quickly developing vaccines, with success. However, a relative dearth of drug research focused on coronaviruses, despite previous outbreaks, held back a fast response on treatments ..."
"... Red Texas btw had 1,387 new cases today. A state with 30 million people. 5 (yes that's five) deaths. The fourth straight day new cases fell. Weird how those stats aren't making it into the fear-mongering articles. ..."
"... Israel is struggling with a fourth wave of infections, and the Israeli Health Ministry announced at that Pfizer vaccine is only 39% effective against the Delta variant there. People who have had Covid and recovered are not being reinfected at a high rate. ..."
"... Time to stop the fear-mongering and hysteria. There is risk to everything in life, and you can't hide under the bed for the rest of your lives because something might happen. Let's get back to normal and stop being held prisoner by confused people like Fauci who don't understand their 15 minutes of fame are long over. ..."
Federal officials concentrated their resources on quickly developing vaccines, with
success. However, a relative dearth of drug research focused on coronaviruses, despite previous
outbreaks, held back a fast response on treatments . Scattered U.S. clinical trials
competed against each other for patients. When effective yet hard-to-administer drugs were
developed, a fragmented American healthcare system struggled to deliver them to patients.
Covid-19 cases, and the need for treatments, are continuing. U.S. hospitals are bracing for
new surges of cases with the
Delta variant spreading
... The Biden administration recently said it would
spend $3.2 billion to support the development of Covid-19 antiviral pills.
... ... ...
A lack of knowledge among healthcare providers has made it difficult to get even the
available treatments. When Bob Bellin of Austin, Texas, tested positive for Covid-19 last
December, he remembered that then-President Donald Trump had
taken a monoclonal antibody treatment from Regeneron Pharmaceuticals Inc.
Suffering from a mild cough and a headache, the retiree was worried about his chances of
developing a bad case of the virus because he has a compromised immune system condition. He
says he called a telemedicine provider to inquire about antibody treatment, but the physician
assistant on the call initially didn't know about it. After some pleading, the healthcare
worker agreed to research the drug's availability, he says.
Several minutes later, she got back to him with the names of sites where he could get the
antibody treatment. The next week, Mr. Bellin received the infusion over a three-hour visit. A
week later, he started his regular running routine again.
... ... ...
Remdesivir, first authorized by the Food and Drug Administration in May 2020 and later
granted full approval, is now given to roughly half of all hospitalized patients. Yet patients
often recover slowly regardless of whether they receive the treatment or not, doctors say.
"The effect of remdesivir is something a statistician can show you in a trial of 1,000
people, but it's not something where you really can see a day-to-day impact on your patients,"
says Dr. Griffin of ProHealth.
... ... ...
The Recovery study, which has examined at least 12 drugs so far, found the most effective of
all Covid-19 treatments for hospitalized patients to date, dexamethasone, which cut the risk of
death in patients on ventilators by a third. The Oxford scientists
reported the results in June 2020 , less than three months after they first began
evaluating it.
... ... ...
Last November, the FDA authorized the first drugs designed specifically to target Covid-19
in people who weren't hospitalized based on preliminary trial results. These monoclonal
antibodies were modeled after the natural antibodies people produce to fight the new
coronavirus.
Researchers at companies including Regeneron and Eli Lilly & Co. developed these monoclonal
antibody therapies in less than a year, compared with the decade or longer it usually takes to
bring a drug to market. The work was sped by earlier research by Regeneron and others to
develop antibodies for the MERS virus. The new drugs worked well in early Covid-19 patients,
reducing the risk of hospitalization or death by 70% in trials.
Yet of the nearly one million doses shipped to hospitals and clinics from November through
early May, just 49% were used by patients over the period.
One factor in their limited use was the fact that influential panels that issue Covid-19
treatment guidelines balked at endorsing them before full clinical trial data was available.
The NIH and the Infectious Diseases Society of America didn't recommend using the drugs until
February and March, respectively, after Lilly provided results from a Phase 3 study.
... ... ...
The hospital treated 1,469 patients with the drugs through early July, and as many as 30
people a day at the peak, says Jonathan Parsons, a pulmonologist and executive vice chair of
clinical operations for Wexner's internal medicine department.
Of the patients treated so far, 4.8% have gone on to be hospitalized, compared with an
estimated 8% to 9% for similar patients not infused with the drug, he says.
Looking ahead, the best solution would be an antiviral that can be taken early in the
disease as a pill, doctors say.
Finding highly effective treatments with tolerable side effects is likely to take years and
require more coordination between government, universities and industry...
B
BRIAN OCONNOR SUBSCRIBER 7 hours ago
The posts below are sad - Trump, Trump, Trump. A man who's been gone for eight months. I
guess that's better than dealing with Biden's endless problems. I suppose letting in
thousands of illegals, many with covid, still isn't an issue?
Love the constant blaming of "delta" on unvaxxed Trump supporters. Sure, it's mostly red
states, but the enormous fact that keeps getting ignored is the fact over 60% of whites have
vaxxed. African Americans? 9%. Yes 9%. That means millions of adult AAs who can get shots,
won't.
Not surprising is AAs make up a large portion of the current hospital load (which still
isn't bad). Of course all the media and the people making this political want to say
is...it's "red states". I guess they don't want to offend Biden's voting base?
Red Texas btw had 1,387 new cases today. A state with 30 million people. 5 (yes that's
five) deaths. The fourth straight day new cases fell. Weird how those stats aren't making it
into the fear-mongering articles.
jack Canzonetta SUBSCRIBER 1 hour ago
FDA, CDC, FAUCI all downplayed Regeneron's treatment--a super treatment --I also asked my
about DR above Regeneron's treatment .. We were discussing a plan in case I contracted the
Wuhan lab virus, he didn't say much Regeneron - I also found out the outlets to receive it
were limited and they had produced many of product.. Fauci was singing only one note--Moderna
--
Catherine G Attara-Fink SUBSCRIBER 27 minutes ago
How about we need treatment for those who have been vaccinated and get Covid after the
fact???
thomas barloon SUBSCRIBER 1 hour ago
Today I saw a 50 year old man with active pulmonary tuberculosis (TB) . Each time he coughs,
he releases millions of tuberculosis organisms into to the air and fills the rooms he enters
with infectious active bacteria. Should our patient with active tuberculosis be allowed to go
when and where he wants? Would you enter a cafe where he is eating or enter a room where he
is living? Of course, most would hope the man with active TB stays home and takes medication
to treat his active infection. Now, in many states, people with active COVID are allowed to
enter cafes and stores. Who are those with acitive COVID? One does not know until one tests
and traces and isolates. And an effective vaccine is also available and monoclonal antibodies
are available to all. Why do doctors not use HCQ and Invermectin and zinc? Simple. These and
many other medications do not work. Yes, the results are available for all to read for free
in NEJM, JAMA, Nature. Follow facts not fantasy.
William Lamb SUBSCRIBER 1 hour ago
I guessed face mask might not be in this picture, since there are those who claimed it is
ineffective and covered one smile. Beside, it is their constutional rights to infect others
and care less for their fellow American, when they see that it is good to share the same
misery to others.
Dick Motley SUBSCRIBER 56 minutes ago
What an ironic post. You DO realize the vaccines are also categorized as emergency use
because they're also considered experimental right? And you HAVE heard about adverse
reactions to the vaccines, right? And you HAVE heard about "breakthrough" cases (reinfection)
among the vaccinated, right? Jamilla Graves SUBSCRIBER 2 hours ago
It would be irresponsible for the WSJ to spread propaganda about drugs that have been
disproven as treatments against and to prevent COVID-19.
jes merrell SUBSCRIBER 2 hours ago
Agreed. It is equally irresponsible for the layman poster to spread propaganda such as "tens
of thousands" of doctors are doing what? Mikey Metz SUBSCRIBER 3 hours ago
"Fragmented health care" is correct. When will Congress and at least 60 percent of Americans
wake up and realize health care in a capitalized society does not work like Target Corp. or
any business that works in a competitive environment. And to read how little money is spent
in this area is horrible. The world has dealt with terrible viruses forever--and the feet
dragging continues.
Julia Harte SUBSCRIBER 3 hours ago
Here are protocols provided by frontline workers that are having success with preventing and
treating covid 19.https://covid19criticalcare.com/covid-19-protocols/
Claire V SUBSCRIBER 4 hours ago (Edited)
We are not in Russia or China where the state mandates what to do. with your thinking it has
to be difficult for you to be in a country where there is freedom of choice. Richard Dole SUBSCRIBER 6 hours ago
Let's see, all the Science (actual peer reviewed studies) indicate that those who have
recovered from COVID (naturally vaccinated) or been jabbed are good to go, have broad
immunity. So why worry about others if you are protected........
J Domingo SUBSCRIBER 6 hours ago (Edited)
So why worry about others if you are protected........
Because this is not about protecting people.
It is about controlling people.
That is the only explanation for why Covid survivors are put on the BAD list. If they
don't line up and demonstrate their servility, they are in trouble.
T
Thomas
Erb SUBSCRIBER 6 hours ago
Now, a new NIH-supported study shows that the answer to this question will vary based on how
an individual's antibodies against SARS-CoV-2 were generated: over the course of a naturally
acquired infection or from a COVID-19 vaccine. The new evidence shows that protective
antibodies generated in response to an mRNA vaccine will target a broader range of SARS-CoV-2
variants carrying "single letter" changes in a key portion of their spike protein compared to
antibodies acquired from an infection. These results add to evidence that people with
acquired immunity may have differing levels of protection to emerging SARS-CoV-2 variants.
More importantly, the data provide further documentation that those who've had and recovered
from a COVID-19 infection still stand to benefit from getting vaccinated.
J Domingo SUBSCRIBER 5 hours ago (Edited)
Israel is struggling with a fourth wave of infections, and the Israeli Health Ministry
announced at that Pfizer vaccine is only 39% effective against the Delta variant there.
People who have had Covid and recovered are not being reinfected at a high rate.
Now, a new NIH-supported study shows that the answer to this question will vary... Quoting a study that is not yet published provides little useful information,
and cannot be used to conclude vaccination is superior to recovery from natural infection.
Thomas Erb SUBSCRIBER 5 hours ago
you missed a part of the Israeli quote
The two-dose vaccine still works very well in preventing people from getting seriously
sick, demonstrating 88% effectiveness against hospitalization and 91% effectiveness against
severe illness, according to the Israeli data.
David Richardson SUBSCRIBER 5 hours ago
Because I still have about a 20% chance of getting the Delta virus if I am in direct contact
with unvaccinated and unmasked people. I then have a 10% chance of getting seriously ill.
But, the many people who post exactly the same question know this data. It is reported daily
by outlets ranging from the MSM to Fox. You just don't like it . It cuts your argument that
unvaccinated people are not a concern or threat to vaccinated people to shreds Man up. Or, at
least, shut up. If you or others decide not to get vaccinated you are materially raising the
immediate risk to others and--perhaps even worse--the odds that you will bread an even worse
variant.
Hersh Goel SUBSCRIBER 3 hours ago
you do not have a 20% chance of getting Delta virus from unvaccinated pople - dont shake
hands, dont hug or kiss. dont get in crowded places like elevators. wear an eye shield and
mask - your risk is essentially zero. The evidence is the thousands of unvaccinated health
care workers who took care of covid 19 cases for over a year.
But if you want to have 'direct contact' with people, thats a choice you make.
T Swan SUBSCRIBER 5 hours ago
This from India news, July 1, 2021
'Not a long-drawn process': Bharat Biotech expecting WHO approval soon As several European
countries are accepting WHO-listed Covishield, Covaxin too is expected to receive WHO
approval soon.
Stephen Carroll SUBSCRIBER 6 hours ago
The highest rates of unvaccinated people live in the inner cities. In order to get support
from liberals the Democrats have neglected these inner city people so it would not disprove
their narrative that it is suburban conservatives that are failing to get vaccinated.
Nikola Sizgorich SUBSCRIBER 6 hours ago
Time to stop the fear-mongering and hysteria. There is risk to everything in life, and
you can't hide under the bed for the rest of your lives because something might happen. Let's
get back to normal and stop being held prisoner by confused people like Fauci who don't
understand their 15 minutes of fame are long over.
K Baker SUBSCRIBER 4 hours ago
Everybody knows a person can still get covid even if a person is fully vaccinated and spread
it to other people. Except JD. He will Spin that a 1000 different ways to try to confuse
people. He is talking to himself.
J Domingo SUBSCRIBER 1 hour ago
Everybody knows a person can still get covid even if a person is fully vaccinated... That's truly funny.
"You're not going to get COVID if you have these vaccinations." Joe Biden, speaking
at the CNN Town Hall in Cincinnati, OH, July 21, 2021
K Baker, and most D's don't even know what their confused leader believes and is
saying publicly about the vaccine.
Without misinformation, the Left would be bereft of information.
Out of unvaccinated Americans surveyed in a poll by the Associated Press-NORC Center for
Public Affairs Research, 64 percent believe the vaccines are ineffective against variants.
U.S. health officials say the Delta variant has caused 83 percent of new cases in the
country, the AP reported. In comparison to those not confident in the vaccine's protection, 86
percent of vaccinated Americans have some belief in the vaccine's effectiveness in the face of
variants. Out of the unvaccinated Americans surveyed in the poll, 35 percent said they will
probably not get the shots while 45 percent were sure that they never will.
"We always knew some proportion of the population would be difficult to persuade no matter
what the data showed, (and) a lot of people are beyond persuasion," said infectious disease
specialist Dr. Amesh Adalja who works at Johns Hopkins University.
Only 3 percent said they definitely plan to get vaccinated and 16 percent said they probably
will get their doses.
With the highly infectious delta coronavirus variant spreading at an alarming rate, the
World Health
Organization in late June 2021 urged people to again wear masks indoors – even those
who are fully vaccinated.
... ... ...
What's the science behind the WHO recommendation?
There is clear and mounting evidence that – though rare – breakthrough COVID-19
infections can occur, even in the fully vaccinated. This is particularly true with emerging
variants of concern.
The CDC has been following these data closely. By mid-July 2021, nearly 60% of the U.S.
population age 18 or older had been fully vaccinated. Infections in those who are fully
vaccinated are rare, and serious outcomes from COVID-19 in that population are even rarer
– though they do still occur. However, the CDC stopped tracking nonhospitalized cases of
COVID-19 for people with and without symptoms among fully vaccinated individuals on May 1,
2021.
The risk of infection leading to serious illness and death, however, differs starkly between
vaccinated and unvaccinated people.
... ... ...
One recent preliminary report from Israel is sobering, however. Before the delta variant
became widespread, from January to April 2021 , Israel reported
that the Pfizer vaccine was 97% effective in preventing symptomatic disease. However,
since June 6 ,
with the delta variant circulating more widely, the Pfizer vaccine has been 64% effective in
preventing symptomatic disease, according to preliminary data reported by Israel's Ministry of
Health in early July.
And in another new
report that is not yet peer-reviewed , researchers compared blood serum antibodies from
people vaccinated with Pfizer Moderna and Johnson & Johnson vaccines and found that the
J&J vaccine lent much lower
protection against delta, beta and other variants, compared with the mRNA-based
vaccines.
Despite the power of Covid-19 vaccines in cutting the risk of hospitalization and death from
the disease,
fully vaccinated people can get very sick and die from the virus in rare cases. Those
individuals tend to be older than 65 or have weakened immune systems or other severe medical
conditions, an NBC News survey of health officials nationwide found.
"Throughout the pandemic, people who died of Covid-19 were most likely to be older, and that
continues to be true with breakthrough cases," a spokesperson for the Massachusetts Department
of Public Health said in an email.
Full coverage of the
Covid-19 pandemic
In Oregon, about 10 percent of the breakthrough infections reported to the state were in
people living in nursing homes or congregate care facilities, and the majority of deaths were
older people.
By Arun Rath July 19, 2021
All Things Considered SHARE
Shira Doron on All Things Considered | July 19, 2021
COVID-19 cases are trending upwards across the country. In Massachusetts, where vaccination rates are relatively high, cases
are still on the rise" and a cluster in Provincetown among mostly vaccinated individuals caused the town to issue a new mask advisory
Monday. Tufts Medical Center epidemiologist Dr. Shira Doron spoke with Arun Rath on GBH's All Things Considered about where
thing stand in the Commonweath and the nation.
Arun Rath: It probably makes sense to start with today's news out of Provincetown. The town is putting its indoor mask
advisory back in place after more than 100 new COVID cases popped up after the July Fourth holiday. What do you make of that uptick
and the response?
Shira Doron: Well, the outbreak is unexpected. It's not what we've been seeing. There's quite a bit of transmission there
reported between vaccinated individuals. And really, what we've seen so far, has been that, certainly, breakthrough cases occur in
vaccinated individuals" usually they have mild symptoms, which we do believe to be the case here" but usually they don't transmit
to others, so the fact that there are so many cases" 132 reported" that a good proportion of them are vaccinated and that it appears
that there was transmission among them is unusual. And so it makes sense for health authorities there to take some swift and rather
aggressive action, at least for the moment, to try to control the outbreak, and then continue to study what might have happened there,
because there's still so much we don't know.
Rath: Interesting. So that uptick of 100 cases is as unusual as it sounds, that's sort of why the response is what it is.
Doron: Yes, we really haven't seen anything quite like this yet.
Rath: Are you concerned that we will start to see other incidents like this?
Doron: I hope not. I hope that this was, you know, an anomaly that was probably related to the fact that the delta variant
is so very contagious that some people who harbor it have very, very high viral loads in the respiratory tract. The fact that it
was a holiday weekend, very crowded bars and nightclubs, some rain that drove people inside more than usual, and that perhaps all
of those things came together this one time to cause this outbreak...
... ... ...
During a WABC 770 AM radio interview with New York businessman
John Catsimatidis, Paul, a trained ophthalmologist, said that he made his decision based on the
fact that he
already contracted COVID-19 in March 2020.
The Centers for Disease Control and Prevention (CDC) recommends that individuals
who previously had COVID-19 should still get vaccinated because there is no timetable for
natural immunity.
Paul said that until he feels assured that immunity through vaccination is more effective
than natural immunity, he will skip taking any shots.
"Until they show me evidence that people who have already had the infection are dying in
large numbers, or being hospitalized or getting very sick, I just made my own personal decision
that I'm not getting vaccinated because I've already had the disease and I have natural
immunity," Paul emphasized.
In the interview, Paul said that people who had contracted COVID-19 and recovered did not
need to wear masks.
"We have 11 million people in our country who've already had COVID," he said
on Fox News at the time. "We should tell them to celebrate. We should tell them to throw
away their masks, go to restaurants, live again, because these people are now immune."
Paul told WABC 770 that taking the COVID-19 vaccine is a personal decision and should not be
compulsory.
"In a free country you would think people would honor the idea that each individual would
get to make the medical decision, that it wouldn't be a big brother coming to tell me what I
have to do," he said. "Are they also going to tell me I can't have a cheeseburger for lunch?
Are they going to tell me that I have to eat carrots only and cut my calories?"
He added: "All that would probably be good for me, but I don't think big brother ought to
tell me to do it."
According
to the CDC , 61.1 percent of adults have received at least one vaccination shot and 49.2
percent of the adult population is now fully vaccinated.
A new way to fight vaccine hesitancy?
Klobuchar's bill would carve out an exception to Section 230, the 1996 law that protects
internet platforms from liability for content that users post, for health misinformation
proliferating during public health emergencies -- like the misinformation that has been running
rampant about vaccines for Covid-19.
https://www.dianomi.com/smartads.epl?id=3533
"We need a long term solution" that goes beyond removing accounts spreading falsehoods about
the crisis, Klobuchar said. "This legislation will hold online platforms accountable."
Why it matters: Lawmakers on both sides of the aisle have been pushing to amend or
revoke the Section 230 statute -- often for opposite
reasons . Many congressional Democrats argue that social media platforms have leaned on
Section 230 legal protections to flout responsibility for false and potentially dangerous
content on their sites, like the medical misinformation that has undermined the uptake of
Covid-19 vaccines.
The Biden administration is struggling
to fight vaccination misinformation , a problem that has contributed to vaccine hesitancy
and a plateau in inoculation rates at a time when the Delta variant is sweeping the country and
the U.S. appears to be backsliding on recovery.
Klobuchar's Health Misinformation Act of 2021, co-sponsored by Sen. Ben Ray Luján
(D-N.M.), is one attempt to address that, and it would extend beyond just the current crisis.
Under the measure, tech platforms would be on the hook for propagating false or misleading
health content during any public health emergency that has been declared as such by the
secretary of Health and Human Services. The secretary, with input from experts and the leaders
of other federal agencies, would be tasked with defining what qualifies as health
misinformation.
What's missing: Republican support. Political polarization around vaccinations
is
intensifying as some Republican lawmakers and conservative activists attack
the vaccines and the administration's strategy for deploying it. In this climate, without
Republican buy-in, Klobuchar's bill faces an uphill battle.
Via
BBC :
"Researchers estimate that 25 deaths in a population of some 12 million children in
England gives a broad, overall mortality rate of 2 per million children."
Despite the above-cited statistics, 56% of big-D
Democrats supported mandating vaccines for schoolchildren in a July 2021 poll.
That's less in Israel.
4 Details on FBI inquiry into Kavanaugh draw fire from Democrats Democrats' divide on voting
rights widens as Biden faces pressure
Los Angeles County Public Health Director Barbara Ferrer announced on Thursday that 20
percent of new COVID-19 cases identified in Los Angeles County were in vaccinated
individuals.
..."The Delta variant is a game-changer," Ferrer said. With the Delta variant driving
community spread and positive case numbers up in LA County, the percentage of breakthrough
cases in fully-vaccinated people has gone up as well. The daily average case rate was 7.1 per
100,000 people on July 15 and shot up to 12.9 on Thursday.
... about 53 percent of LA County residents are fully vaccinated against coronavirus. About
58 percent of young people between the ages of 18 and 29 are fully vaccinated.
... Vaccinated people are still far more likely to be able to fight off the virus when
exposed. Vaccinated people are also much less likely to advance to serious illness or death,
with 90 percent of nationwide hospitalizations or fatalities occurring in unvaccinated
people.
...
new data shows people infected with the delta strain can carry up to 1,000 times more virus
in their nasal passages than those infected with the original strain.
"I think people are underestimating how bad this is going to get," said Dr. Ashish Jha. "We
are in for a very tough August, probably a very tough September before this really turns
around."
Dr. Rochelle Walensky, director of the Centers for Disease Control and Prevention,
told reporters at a briefing Thursday that the delta variant "is one of the most infectious
respiratory viruses we know of, and that I have seen in my 20 year career."
Jha told CNBC's " The News with Shepard
Smith ," that the infection rate could be worse if it were winter, and predicted the delta
spike could peak within two months.
"It might peak in September, but we are far away from the peak, right now we are doing
40,000 cases a day, it's going to go substantially higher before it peaks," Jha said.
The delta variant has spread rapidly through the U.S., accounting for more than 83% of
sequenced cases in the U.S. right now, up from 50% the week of July 3, according to the
CDC.
At delta variant of Covid-19 spreads across many Western and
Southern U.S. states, its high transmission rate could increase them number of immune to the
virus people from about 50% to 85%" even if vaccination rates continue to plateau, Dr. Scott
Gottlieb, a former chief of the Food and Drug Administration, said.
Gottlieb noted that millions of Americans remain vulnerable and now
have a "choice in terms of how [they] acquire immunity."
Both vaccinated and those who have natural immunity still have
increased risk Gottlieb said, pointing to data showing immunity among individuals naturally
infected with Covid-19" and particularly those who are older" declines after about eight
months. It looks like the decline for vaccinated people is even faster and that's why there are
talks about booster shots
He predicted Covid will effectively act as a "second circulating flu
this winter," though he said its prominence "could be a little worse."
In Mexico, an estimated 84% of cases are delta infections, which may be a warning that this
variant may also be endemic in Latin America.
If the virus continues to mutate as fast as did in 2020 and 2021 herd immunity against this
virus might never be achieved.
CRUCIAL QUOTE
"I wouldn't be declaring mission accomplished. I think this is going to be a long fight,"
Gottlieb said Sunday. "You're seeing a decoupling between cases, hospitalizations and deaths
because there's so much immunity in the population""not just through vaccination""but also
through prior infection... But this is likely to become an endemic virus. We're going to have
to deal with it."
KEY BACKGROUND
Since the start of the pandemic, experts have long said Covid-19's threat would largely
wane once herd immunity is reached,
referring to a large-enough proportion of immunity that effectively makes
person-to-person transmission highly unlikely within a community. If the virus cominutes to
mutated in a ways it did in 202 and 2021 this might not happen all and herd immunity against
this virus might never be achived.
If we assume that 80% of population is vaccinated and 30-40% of vaccinated can be infected and spread the virus, that simply means
that like in case of flu and other coronaviruses herd immunity from COVID-19 will never be achieved as in one year the virus sufficiently
mutates to infect significant percentage of previously vaccinated people. The situation with mass vaccination of children looks pretty
absurd, if not criminal
The news is peppered with anecdotal evidence of breakthrough cases. The headlines are terrifying and the personal stories are
tragic:
Boston Globe : "79 fully vaccinated Massachusetts residents have died, 303 hospitalized in very rare COVID "˜breakthrough'
cases, officials say"
The Guardian : "COVID outbreak among vaccinated Vegas hospital workers underscores Delta risks"
NBC : "Illinois Coronavirus Updates: Breakthrough COVID Cases Are 2% of State's Deaths This Year"
So, why do breakthrough cases happen?
We shouldn't think of vaccine protection as binary (yes or no). It's better to think of protection on a spectrum: On one end the
vaccine will protect people in every situation and on the other end it doesn't protect people at all. And each of us land somewhere
in between.
There are many factors that determine where we land:
There's of course the variants. Depending which variant you come in contact with determines your level of protection. mRNA
vaccines' efficacy is now ~88% against Delta. If 100 people got COVID19, Pfizer/Moderna could have prevented 88 of them. 12 people
would have still gotten some form of the disease. On the other hand, if people came in contact with the original strain, 95 (out
of a 100) would have been prevented.
Some of us just don't have immune systems that can build protection. For example, it looks like
certain drugs for
immunocompromised patients reduce and/or prevent protection. Also, older adults are less protected.
Behaviors, too, can predict your place on this spectrum. If a vaccinated person is exposed to a large enough dose of a virus
OR exposed to enough unvaccinated people where transmission is high, the virus can overcome the vaccine and cause infection, even
among the sturdiest of immune defenses.
And then there's just luck. Even if you compare
twins , the level of protection
can differ. Some people will just create fewer or less strong defense mechanisms (antibodies, T cells, and/or memory B cells).
And we don't really know why.
Nonetheless, should the virus make it through, Dr. Ali Ellebody, an immunologist at Washington University in St. Louis,
said it best:
"It becomes a race [against] time. The pathogen rushes to copy itself, and the immune system recruits more defenders. The longer
the tussle drags on, the more likely the disease is to manifest."
It's important to monitor all breakthrough cases.
If we closely monitor them, we can answer some very critical questions like"¦
Are breakthrough cases happening at the rate in which we expect?
Who's most likely to break through?
What is the rate of a mild breakthrough case vs. severe breakthrough case?
Are variants, like Delta, causing more (or more severe) breakthrough cases than other variants?
A study was published describing breakthrough
cases between January 1-April 30. During this time among 101 million fully vaccinated Americans, 10,262 breakthrough infections were
reported to the CDC. Who were they?
63% female
Median age was 58 years (age range was 40""74 years)
10% were hospitalized
2% died. Median age of patients who died was 82 years (age range was 71""89 years)
Genomic sequence data were available for 5% of breakthrough cases
Beginning May 1, 2021, though, the CDC transitioned from monitoring all breakthrough infections to investigating only those among
patients who are hospitalized or die. The CDC doesn't have the infrastructure to rigorously investigate all breakthrough cases. They
needed to prioritize their operation, so they decided to focus on cases of highest clinical and public health significance.
The CDC continuously publishes the latest count on their
website . As of July
6, there were 5,186 severe breakthrough cases. This includes 988 deaths (although it's important to notice the footnote stating
that 255 of these were not directly related to COVID19).
... ... ...
From February 1 to June 21, 123,620 Delta cases were sequenced in the UK. Among those, 10,834 cases were among fully vaccinated
( i.e. breakthrough cases) and 71,932 cases among the unvaccinated. While this isn't all of the breakthrough cases, this gives
an even closer estimate to the "true" rate of breakthrough cases due to Delta. But even this is among patients who went to the hospital.
We still don't know the asymptomatic and/or mild breakthrough rate.
Anna Stern
Jul 16
It really angers me that the CDC isn't tracking all breakthroughs even if they don't investigate everything, because we are
losing so much information, such as what's going on here.
There have been a couple of Delta breakthrough CLUSTERS in the news lately, so there may be fully vaxxed people who are superspreaders.
I don't think you can attribute these to individual immune system issues.
In this cluster, the sources had a vaccine with lower effectiveness, and they probably stood pretty close together, even though
outdoors. But the other folks had mRNA. All guests were required to be fully vaxxed.
https://www.businessinsider.com/fully-vaccinated-people-got-covid-after-an-outdoor-wedding-2021-7
8 fully vaxxed, 2 partially vaxxed, 1 unvaxxed health care workers were infected at a pool party.
https://www.reviewjournal.com/life/health/covid-case-cluster-hits-vaccinated-las-vegas-hospital-workers-2398382/
Reply
3 replies
GP
Jul 17
Question: Many of the news reports about breakthrough cases show that groups of friends or couples who are all fully vaccinated
but spent time together somehow *all* ended up as breakthrough cases. With the 88% vaccine efficacy rate, how does that work? For
example, if a husband who is fully vaccinated is infected as a breakthrough case, shouldn't it be highly unprobable mathematically
that his fully vaccinated wife also then contracts it from him?
Anna Stern
Jul 16
This is the newest/current NY Yankee cluster.
https://newyork.cbslocal.com/2021/07/15/new-york-yankees-game-postponed/
Jul 16
Thanks for this! Katelyn, you are a gem. As a retired fed health professional, I have kind of an embedded risk vs threat meter
after all those years of working. I am cringing at everyone going back to normal, like the pandemic is over. I over quote Yogi Berra
- it ain't over till it's over.
Reply Rose W.
Jul 18
As a fully vaccinated person, I have continued to mask indoors as my kids are not vaccinated and I do not want to risk spreading
it to them. I am now getting nervous about outdoor interactions i.e school dropoffs, outdoor bday parties, etc. with potentially
unvaccinated individuals. The wedding and Vegas pool party stories have made me a bit nervous. Any thoughts?
Reply Ralt18
Jul 18
I wish I could put an attachment here but in the same vein of all of this, my sister , who is a diehard anti vaxxer sent me a
snip of the Israel Health ministry case reporting from last week which breaks down cases of fully vaccinated and non vaccinated by
age group. The chart shows almost higher percentage of vaccinated individuals with cases and show small case load but overall high
percent . She is running with this information saying this proves that the vaccine makes you more suspepticle to covid and is causing
the current issues. Local, I know you have explained this data reporting misunderstanding before but can you explain again why the
data looks skewed in Israel ? Also check me on my chart
Unvaccinated Americans widely believe that the
COVID-19 vaccine is riskier than the novel coronavirus itself, according to a new
Yahoo News/YouGov poll.
The finding comes as the United States has hit a plateau for COVID-19 vaccinations, even
as the more transmissible delta variant of the virus continues to circulate through the
country.
Per
Yahoo News , the poll result "contradicts all available science and data and underscores
the challenges that the United States will continue to face as it struggles to stop a growing
' pandemic
of the unvaccinated' driven by the hyper-contagious delta variant."
How do people feel about the COVID-19 vaccine?
According to
Yahoo News , the poll found 29% of unvaccinated Americans believe the virus poses a greater
risk than the vaccine. However, 37% feel the vaccine is riskier, while 34% remain unsure.
In total, 93% of unvaccinated people surveyed in the
Yahoo News poll said they would either never get the vaccine or they will wait to see
what happens to others before they do.
Why don't people want to get the vaccination?
The
Yahoo News poll also looked into why people aren't getting vaccinated. It found several
reasons among the survey participants, including:
There isn't easy access to a vaccination site (4%).
People can't get time off from work (3%).
Some already had COVID-19 (9%).
People aren't worried about getting COVID-19 (12%).
Others don't trust the COVID-19 vaccine (45%).
widely believe that the
COVID-19 vaccine is riskier than the novel coronavirus itself, according to a new
Yahoo News/YouGov poll.
The finding comes as the United States has hit a plateau for COVID-19 vaccinations, even
as the more transmissible delta variant of the virus continues to circulate through the
country.
Per
Yahoo News , the poll result "contradicts all available science and data and underscores
the challenges that the United States will continue to face as it struggles to stop a growing
' pandemic
of the unvaccinated' driven by the hyper-contagious delta variant."
How do people feel about the COVID-19 vaccine?
According to
Yahoo News , the poll found 29% of unvaccinated Americans believe the virus poses a greater
risk than the vaccine. However, 37% feel the vaccine is riskier, while 34% remain unsure.
In total, 93% of unvaccinated people surveyed in the
Yahoo News poll said they would either never get the vaccine or they will wait to see
what happens to others before they do.
Why don't people want to get the vaccination?
The
Yahoo News poll also looked into why people aren't getting vaccinated. It found several
reasons among the survey participants, including:
There isn't easy access to a vaccination site (4%).
People can't get time off from work (3%).
Some already had COVID-19 (9%).
People aren't worried about getting COVID-19 (12%).
Others don't trust the COVID-19 vaccine (45%).
... "Like everything in life, this is an ongoing risk assessment," Dr. Inci Yildirim , a Yale
Medicine pediatric infectious diseases specialist and a vaccinologist, told Yale Medicine.
NAV 39 minutes ago remove link
When Dr. Robert Malone who invented the mRNA and DNA vaccine core platform technology
has grave concerns about the lack of transparency of side effects, the censoring of
discussion and the lack of informed consent, one wonders why the conventional media refuses
to share this information and is cooking the data.
Attorney Files Lawsuit Against CDC Based on "Sworn Declaration" from Whistleblower
Claiming 45,000 Deaths Are Reported to VAERS – All Within 3 Days of COVID-19 Shots \
Global Research
Ohio-based Attorney Thomas Renz was one of several speakers this past weekend at a
conference in Anaheim, California, where he announced that with the help of America's Frontline
Doctors , he was filing a federal lawsuit in Alabama based on a "sworn declaration,
under threat of perjury," from an alleged whistleblower who claims to have inside knowledge
of a cover-up of reported deaths filed with the Vaccine Adverse Event Reporting System
(VAERS), which is operated by the CDC.
This whistleblower has allegedly claimed, under oath, that there are at least 45,000
reported deaths that have occurred within 3 days of receiving a COVID-19 "vaccine." Renz
states that this report of 45,000 deaths is just from "one system" that reports to
VAERS.
This would be significantly greater than what the CDC is currently reporting, which is
10,991 deaths, and many of those are beyond 3 days following the shots. See:
CENSORED: CDC Records Almost 12,000 DEATHS in 7 Months Following COVID-19
Injections
Renz also states that he believes Google, Facebook, and Twitter are "complicit with
causing death" due to their censorship, and he stated "I cannot wait to sue you, over and
over again."
https://www.globalresearch.ca/attorney-files-lawsuit-against-cdc-based-sworn-declaration-whistleblower-claiming-45000-deaths-reported-vaers-all-within-3-days-covid-19-shots/5750620
https://www.midlandscbd.com/articles/warning-physician-who-invented-mrna-shot-speaks-out
...breakthrough infections among the vaccinated, which is another reason that there are
increasingly louder questions about whether immunity may be waning among some people who have
been vaccinated and
if boosters are needed to combat declining protection.
The booster debate has also been fueled by preliminary data out of Israel that indicates
BioNTech SE and Pfizer Inc.'s shot is
64% effective against delta -- a significant decline from the
95% efficacy rate reported in clinical trials.
"We have the same data as Israel," Sen. Richard Burr, a North Carolina Republican, said
during Tuesday's Senate HELP committee hearing. "Why aren't we making the same decisions?"
Dr. Anthony Fauci, chief medical adviser to President Joe Biden, later responded, saying:
"Right now we are doing studies to determine whether or not we will need boosters, to increase
the durability of protection. We don't want people to believe that when you're talking about
boosters that means that the vaccines are not effective. They are highly effective. We're
talking about the durability."
It's still unknown how long immunity to SARS-CoV-2 lasts, whether from a previous infection
or from vaccination. Pfizer recently said it believes immunity from its shot begins to wane
between six and 12 months after vaccination. Some countries, including Israel, Canada and the
U.K., are providing or considering booster shots for certain high-risk patient groups.
Fauci said that the CDC is currently tracking 20 groups of people who have been vaccinated
to better understand whether there is or will be a need for boosters. This includes thousands
of healthcare workers and people from long-term-care facilities and nursing homes.
"We're anticipating that this will wane and not plummet," CDC director Dr. Rochelle Walensky
said during the hearing. "As we see that waning, that will be our time for action."
Johnson and Johnson vaccine was ineffective against South African mutation. So why Delta, and
especially Delta Plus variant which has the same mutation as South African variant (Beta in new
classification). Thus like South African variant is has further advantages in infected already
vaccinated people
Delta plus variant of SARS-CoV-2- What do we know so far
The Delta
variant of the COVID-19 virus continues to spread. It now
constitutes 83% of the COVID cases in the U.S.
And now, as CBS2's Dr. Max Gomez reported Wednesday, a preliminary study not yet peer
reviewed suggests that the Johnson & Johnson vaccine may
not be as effective against the Delta variant as the other two authorized vaccines.
... The J&J vaccine has been given to more than 13 million people
Those conclusions differ from smaller clinical results released by J&J earlier this
month that said a single dose of their vaccine did protect against Delta, even eight months
after inoculation.
Those differences could be because the new study looked at antibodies in the lab compared to
real world immunity in people, which would include T-cell immunity. Peer review would help
determine that contribution to protection.
... ... ...
Delta variant dominates vaccine-breakthrough infections
To come to this conclusion, scientists from the Cambridge Institute of Therapeutic
Immunology and Infectious Disease looked at more than 100 health workers at three centres
across India. Titled "Sars-Cov-2 B.1.617.2
Delta Variant Emergence and Vaccine Breakthrough: Collaborative Study". One of the centres
was Sir Ganga Ram Hospital (SGRH) in Delhi. It is yet to be peer reviewed.
Researchers of this study found that the Delta variant, which emerged in India, dominates
vaccine-breakthrough infections with higher respiratory viral loads compared to non-Delta
infections.
They also saw that this variant generates greater transmission among the fully vaccinated
healthcare workers. Moreover, the study found that, in vitro, the Delta variant is around
eight-fold less sensitive to vaccine-elicited antibodies compared to the original
virus.
Hence, they came to the conclusion that Delta variant is both more transmissible and
better able to evade the immunity a patient gets from previous infection as compared to
previously circulating coronaviruses.
DG , Jun 18 2021 10:44 utc |
65
Mandatory vaccination with experimental vaccines is abhorrent and it should have us all
worried.
Unfortunately majorities in many countries have accepted this in the name of protecting
public health.
This is a very tragic situation and should be given our full attention.
And no, no one should be blackmailed to have these vaccines because they work in a
hospital, or a care home. They have the right to refuse at least as long as these vaccines
are in the experimental phase.
In Greece they are already preparing laws to make vaccination mandatory for doctors,
health workers, teachers and firefighters.
This is highly terrifying.
That correlates well with Israel data.
60% of people being admitted to the hospital with Covid-19 in England are fully vaccinated,
Sky News
reported .
According to Sir Patrick Vallance, the government's chief scientific advisor, Covid patients
have received two doses of the Covid vaccine.
"In terms of the number of people in hospital who've been double-vaccinated, we know it's
around 60% of the people being admitted to hospital with COVID," Vallance said.
"We do expect there to be over 1,000 people per day being hospitalized with coronavirus
because of the increase in infections," he added. "But the rates should be lower than they have
been previously because of the protective effects of vaccination."
Update: Now Sir Patrick Vallance is claiming he misspoke during Monday's presser!
"Correcting a statistic I gave at the press conference today, 19 July. About 60% of
hospitalisations from covid are not from double vaccinated people, rather 60% of
hospitalisations from covid are currently from unvaccinated people." Vallance said in a
tweet.
The author totally missed the key point: What are the benefits of mass vaccination campaign
if we can never achieve this mysterious herd immunity. Looks like herd immunity is impossible
with coronaviruses and the virus will become endemic. The first generation of experimental
vaccines proved to be less affective against Delta and probably will be even less effective
against future mutations and as the time from vaccination increases. also using experimental
maccines on the whole US population is not that different from Tesla testing thier limited
self-driveing on the the USA roads. The only difference is there are more victims in vaccines
case.
While Harris rhetoric during campaign was reprehensible, Trump did rushed experimental
vaccines' and this was a very questionable move as the idea of achieving herd immunity now with
Delta variant looks like a fiasco. If we can't achieve herd immunity, why not limit vaccination
to most vulnerable for which risk from vaccination are negligible in comparison with benefits. As
well as inhabitants on big metropolises like NYC, where you use public transport and this
experience additional risks and people over 50 who during their business day are forced to
communicate with a lot of strangers.
Originally from:
Guess who undermined public confidence in vaccines- by Andrew C. McCarthy
Harris had stated that any such effort pushed by then-President Trump was
untrustworthy . This was consistent with the Biden campaign theme that the Trump
administration had been incompetent in responding to the COVID-19 pandemic - a position that
morphed, when President Biden took office, into a claim that the Trump team hadn't even had a
workable plan on vaccine distribution (a claim so patently false that even Anthony Fauci,
director of the Institute of Allergy and Infectious Diseases, denied it).
The vice presidential candidates' debate was Harris's highest-profile appearance of the
campaign. She took the opportunity to explain that she would not get a vaccine pushed by Trump.
That is what got the habitually placid Pence's dander up. He turned to Harris and memorably
admonished , "Stop playing politics with people's lives."
This is a vignette worth keeping in the front of our minds as Biden cynically exploits his
bully pulpit against Facebook. The president and his administration are endeavoring to shift
blame to the social media giant for the predictable effects of their own demagoguery.
The propagandist-in-chief inveighed against Facebook on Friday for " killing
people " by spreading misinformation about the efficacy and potentially damaging side
effects of the vaccines. The claim is nearly as shameful as Biden's recent
portrayal of state election-procedure reforms (e.g., curbs on drive-thru voting) as the
reestablishment of Jim Crow and a threat to democracy on a par with "the Civil War."
Biden's attack on Facebook is reprehensible. Though he won't be called on it by the
Democratic media complex, these are outrageous lies comparable to what the president accuses
his predecessor of routinely spewing.
The administration is upset because, after his campaign discredited the vaccine effort,
Biden over-promised what he could deliver once he took charge of it. He claimed that by
Independence Day 70 percent of adult Americans would have received at least one dose of a
vaccine. In fact, the Mayo Clinic put the July
4 count at about 55 percent. (It has inched up to 56 percent in the two weeks since, and just
under half the eligible population has been fully vaccinated.)
Patently, this is not Facebook's fault. Facebook is a social media platform with
billions of users . As a matter of human inevitability, there will be some misinformation
on it. That is the nature of speech in a large, pluralistic, free society. It is to be expected
of a free-communications medium that is nudged by law to be minimalist in regulating the
exchange of information and to avoid content discrimination.
Even so, Facebook has been tireless in informing users about where and when vaccines are
available, and in disseminating exhortations that Americans avail themselves of them. It also
contends that 85 percent of U.S. Facebook users have been or want to be vaccinated.
There is abundant reason to be skeptical about that claim - really, how would Facebook know?
At the same time, it would not be surprising at all if Facebook, as a user community, does in
fact have a higher vaccination rate than the nation as a whole on Biden's watch. After all,
none of Facebook's principals cavalierly undermined the government's vaccine effort for what
they perceived to be a fleeting political advantage. It was Biden officials who did that.
... ... ...
Former federal prosecutor Andrew C. McCarthy is a senior fellow at National Review Institute , a contributing editor at
National Review and a Fox News contributor. His latest book is "
Ball of Collusion ." Follow him on Twitter @AndrewCMcCarthy
.
KRISTA B
5h
No, it's people wising up.So, what's the advantage to an unproven, unguaranteed non-vaccine? None. So.... Why?
It's not Facebook, or Biden. It's people, finally wising up.
Looks like in the USA Hippocratic oath has been modified: First do no harm to the pharma
profits
Looks like in the USA Hippocratic oath has been modified: First do no harm to the pharma
profits
Daniel Kotzin @danielkotzin · May 28
The American Academy of Pediatrics recommends that
children in diapers wear masks until they are fully vaccinated. Coincidentally, Yvonne
Maldonado is the Chair of the AAP's Committee on Infectious Diseases AND she runs the trial of
the Pfizer vaccine on 2 to 5-year-olds.
Brandon Fisher
(BoulderFish) @boulderfish Replying to @jessicamstone and @danielkotzin
It's literally nauseating. 2 year olds
getting this injection?? WTF is wrong with people!? These poor kids.
Kerry Evans @TomEvan81013762 · May 28
Replying to @boulderfish
@jessicamstone and @danielkotzin
Babies have already died from these. One
nursing baby. One two year old. Two days after the shot! It is criminal.
"This is a dramatic increase, up from 50% [in] the week of 4 July," Rochelle Walensky,
director of the Centers of Disease Control and Prevention (CDC), said in Senate testimony.
Walensky also said Covid fatalities had risen by nearly 48% over the past week to an average
of 239 a day.
"Each death is tragic and even more heartbreaking when we know that the majority of these
deaths could be prevented with a simple, safe available vaccine," she said.
A cluster of midwestern and southern states have emerged as the new hotspots for
Covid-19.
Myocarditis is inflammation of the heart muscle, and pericarditis is inflammation of the
outer lining of the heart. In both cases, the body's immune system causes inflammation in
response to an infection or some other trigger.
There have been more than 1,200 such cases in people who received the Pfizer or Moderna
COVID-19 vaccine, according to the CDC. According to the CDC presentation, men under 30 make up
the bulk of the cases and most cases appear to be mild (79% fully recovered)
The agency said cases in individuals who received two doses were doubled compared to cases in
individuals who only received one dose of the mNRA vaccines
What
You Need to Know
More than 177 million people have received at least one dose of COVID-19 vaccine in the
United States, and CDC continues to monitor the safety of COVID-19 vaccines for any health
problems that happen after vaccination.
Since April 2021, there have been more than a thousand reports to the Vaccine Adverse
Event Reporting System (VAERS) of cases of inflammation of the heart -- called myocarditis
and pericarditis -- happening after mRNA COVID-19 vaccination (i.e., Pfizer-BioNTech,
Moderna) in the United States.
These reports are rare, given the hundreds of millions of vaccine doses administered, and
have been reported after mRNA COVID-19 vaccination, particularly in adolescents and young
adults. View the
latest information .
CDC and its partners are actively monitoring these reports, by reviewing data and medical
records, to learn more about what happened and to understand any relationship to COVID-19
vaccination.
Most patients who received care responded well to treatment and rest and quickly felt
better.
Confirmed cases have occurred:
Mostly in male adolescents and young adults age 16 years or older
More often after getting the second dose than after the first dose of one of these
two mRNA COVID-19 vaccines
Typically within several days after COVID-19 vaccination
... ... ...
What Myocarditis/Pericarditis Symptoms Should I Be on the Lookout for
after mRNA COVID-19 Vaccination?
Be on the lookout for any of the following symptoms:
Chest pain
Shortness of breath
Feelings of having a fast-beating, fluttering, or pounding heart
Seek medical care if you think you or your child have any of these symptoms within a week
after COVID-19 vaccination.
If you have any health problems after vaccination, report them to the Vaccine Adverse Event Reporting System external
icon (VAERS).
That correlates well with Israel data.
60% of people being admitted to the hospital with Covid-19 in England are fully vaccinated,
Sky News
reported .
According to Sir Patrick Vallance, the government's chief scientific advisor, Covid patients
have received two doses of the Covid vaccine.
"In terms of the number of people in hospital who've been double-vaccinated, we know it's
around 60% of the people being admitted to hospital with COVID," Vallance said.
"We do expect there to be over 1,000 people per day being hospitalized with coronavirus
because of the increase in infections," he added. "But the rates should be lower than they have
been previously because of the protective effects of vaccination."
Update: Now Sir Patrick Vallance is claiming he misspoke during Monday's presser!
"Correcting a statistic I gave at the press conference today, 19 July. About 60% of
hospitalisations from covid are not from double vaccinated people, rather 60% of
hospitalisations from covid are currently from unvaccinated people." Vallance said in a
tweet.
"Masks have value, unquestionably. But masks are not going at the root of the problem
– vaccination is. So, we do not intend a mask mandate. We do intend to double down on
vaccinations. We'll be speaking about it through the week and beyond, new approaches to
vaccination. This is where we make the difference," de Blasio said.
So far, the mayor says 4.8 million New Yorkers have received at least one dose of the
vaccine. The mayor says 4.5 million are full vaccinated.
As the Delta variant of COVID-19 makes its way across the globe, a new report from Israeli
website Ynet
First, the good news: Data from the Israel Health Ministry find the vaccine holds up well
against the variant when it comes to hospitalizations and serious illness, with an efficacy
rate of 93 percent according to data from June 6 to July 3, when the Delta variant really began
to take hold,
Bloomberg reports . That's down from 98.2 percent compared to the variants that came
before, but still very good.
The bad news is the data appear to indicate a significant drop in efficacy when it comes to
the Pfizer vaccine preventing infection overall. Between May 2 and June 5, the vaccine had a
94.3 percent efficacy rate at preventing infection,
Bloomberg explains. That rate dropped to 64 percent in the month that
followed.
If the data are correct, it means that even if you're fully vaccinated, you could still
catch and show symptoms of COVID-19. That's always been the case, but the Delta variant makes
it more likely. But the immunization still significantly reduces your chances of landing in the
hospital.
Vaccinated people who have experienced Covid-19 symptoms in the past 10 days, however,
should get tested and isolate themselves from others for 10 days if their test is positive, the
CDC has recommended.
Look like Delta variant is less toxic then previous and led to fewer deaths and
hospitalization, as often happen with later mutations of the virus.
The key here is the rate of infection of already vaccinated, not the fact that
hospitalizations and death stats decoupled from new cases stats. If the significant percentage of
vaccinated can be infected by Delta (say, over 20%) that could well be the last nail into the
coffin of "herd immunity" delusion promoted by Fauci and other high level medical bureaucrats.
There were never herd immunity from coronaviruses as they mutate too quickly to achieve it. That
does not means that vaccination is useless, especially for those who live in big cities and use
public transportation or need to meet customers during each working way. But that makes the idea
of "total vaccination" effort including children over 12 as useless as quarantine efforts before
widespread riots.
Two weeks ago, when markets were merrily melting up without a worry in the world, and
certainly were not paying attention to the recent spike in Delta cases, we showed that unlike
in 2020 when covid hospitalizations and deaths promptly followed - with a slight lag - any move
higher in new covid cases, now that vast swaths of the population have been vaccinated, there
has been a clear decoupling between new cases on one hand, and hospitalizations and fatalities
on the other
... Yet while infections may indeed be rising, Fauci purposefully refused to address the
real elephant in the room: is there a concurrent surge in hospitalizations and/or deaths: after
all, it those that matter - especially if the Delta variant results in a much weaker form of
covid as many have speculated - and not the cases outright.
...
Where we do agree with Kolanovic, however, is where he repeats what we said two weeks ago
with the chart shown at the top of this post, namely that the "Delta variant is a key risk to
the call, but encouragingly the link between the case count and hospitalizations/deaths in the
UK and other countries has weakened meaningfully (Figure 1)." In short cases and
hospitalizations have decoupled... just as we showed they have even if the government's
propaganda spin masters refuse to acknowledge.
As the Delta variant takes hold, some of the first COVID-19 cases among the vaccinated
population are being detected. According to the states data, 74 vaccinated California's have
died, however, the report states it is unknown if the primary cause of death in these cases was
COVID-19 or if there were other alternate causes.
... At Zuckerberg San Francisco General Hospital one of seven COVID patients was vaccinated.
According to the latest
state data, 20.4 million fully vaccinated individuals, 10,430 post-vaccination cases
(0.051%) have been identified.
Bob Wachter @Bob_Wachter If
you're wondering how bad Delta really is, even in highly vaccinated SF (76% of >age 12 fully
vaxxed) & still w/ a lot of masking (most folks in stores), we're seeing a pretty steep
Covid uptick. Daily cases up 4-fold (10->42; Fig L), hospital pts doubled (9->19;
R)(Thread 1/4) 3:41 PM · Jul 15,
2021 · Twitter Web App 2,064
Retweets 285 Quote Tweets 3,874 Likes Bob Wachter @Bob_Wachter · Jul 15 Replying to
@Bob_Wachter Uptick mirrored
@ucsfhospitals : Covid
inpatients (we were at ~3 pts two-wks ago) now 13 (Fig L). Overall test positivity rate was
well below 1%; it's now up to 2.6% (Fig R). Even more worrisome, test positivity rate in
asymptomatic pts was ~0.15%, now up 6-fold to 0.9%. (2/4) 14 93 362 Bob Wachter @Bob_Wachter · Jul 15 I don't have
vaccinated/unvaxxed breakdown for SF & UCSF – I assume most severe cases are in
unvaxxed. But even for vaxxed, w/ more Covid in air expect more breakthru cases. As for me, I'm
back to double-mask in stores. Still indoor dining but might abort if trends continue.(3/4) 88
197 719 Bob Wachter @Bob_Wachter
· Jul 15 The SF # s are still
fairly low, & are cause for caution, not panic. But this kind of uptick in SF (U.S.'s
vaccination leader) shows that Delta is very real – the places w/ much lower vax rates
may well get clobbered. Alas, doesn't seem like there are many persuadables left.(4/4) 67 185
854 Derek Reilly @DerekReilly19
· Jul 15 Replying to
@Bob_Wachter 42 and 19? Come on
Bob seriously. 1 1 8 kenlipartito
@kenlipartito · Jul 15 Really. It's not like
this thing grows exponentially, right? 3 26 Show replies geva kra oz @gevakraoz · Jul 15 Replying to @Bob_Wachter @Meir_Rubin Can't Working
@ArianneM12 · Jul 15 Replying to @Bob_Wachter Was waiting on the post 4th of
July consequences. Hopefully they all live 1 5 Stressedout @TMD666 · Jul 15 Replying to @Bob_Wachter Any advice for @CDCgov ? They missed the window of opportunity.
What can @CDCgov do in addition to
vaccine to bring delta under control? 6 6 Michaela Barnes @mabarnes9 · Jul 15 Replying to
@Bob_Wachter Montgomery County MD
where I live has 81.8% of 12yo and up fully vaccinated per CDC and we're also seeing big %
upticks from very low numbers. 6 10 75 Show replies 𝗚𝗿𝗮𝗵𝗮𝗺
𝗪𝗮𝗹𝗸𝗲𝗿, 𝗠𝗗 @grahamwalker
· Jul 15 Replying to @Bob_Wachter Same Bob; anecdotally have
started seeing COVID again in the ED when previously hadn't seen any in months, thus far only
in unvaccinated patients. It's baaack, despite us being probably the most vaccinated large city
in the US.
In the last month or so, about 20-25% of the cases in Fayette County have been
breakthroughs. Health leaders say it was expected that vaccinated people could still catch the
virus, but the important thing is they are much less likely to get severely ill as a
result.
... "Some of that is likely because of the Delta variant, but also because people who are
vaccinated are likely not taking as many precautions as they did before," spokesperson Kevin
Hall said. "This could be compared to wearing your seatbelt. It does protect you, they still
don't go 120 miles an hour down the interstate. You need to still take precautions."
Hall said they've also seen a few cases where unvaccinated people bring the virus home and
infect vaccinated family members.
He said even though there isn't a mandate, those safety precautions, like wearing a mask
around crowds, are still encouraged.
Neoliberal MSM now are trying to swipe under the carpet the bankruptcy of the idea or achieving "herd immunity"
via mass vaccination campaign. Which was sent to its grave by Delta variant.
The fact that CDC does not track mild cases does not prevent estimate them from other statistics relying of percentage of
hospitalization cases to total cases and deaths to total cases. If we use death state for the USA (624746 death for 34994151
cases), then for 1063 death of vaccinated people we will have around 60K infected. Of we assume that death of vaccinated is
ten time less probable then for non vaccinated the number will 600K. As such cases are concentrated in a few big cities
they probably ensure the spread of the virus even in totally vaccinated population. Then the question arise: was the gain from
this mass campaign ? And high level medical bureaucrats already failed us with the lockdown and quarantine which did not have
any noticeable effect of epidemic and then made all sacrifices a joke by riots in major cities.
As CDC admits : "The findings in this report are subject to at
least two limitations. First, the number of reported COVID-19 vaccine breakthrough cases is likely a substantial undercount of all
SARS-CoV-2 infections among fully vaccinated persons. The national surveillance system relies on passive and voluntary reporting,
and data might not be complete or representative. Many persons with vaccine breakthrough infections, especially those who are
asymptomatic or who experience mild illness, might not seek testing. Second, SARS-CoV-2 sequence data are available for only a small
proportion of the reported cases."
Fauci and other high level medical bureaucrats, who put all eggs into vaccination basket made a very risky move. They knew
that there were no successful vaccine against coronaviruses, because they constantly mutated, and still put them whole country into
questionable path of "total immunization"
Notable quotes:
"... The COVID-19 vaccines are extremely effective, but a few vaccinated people have gotten sick. ..."
"... "Breakthrough" infections are typically mild and might be less contagious than other cases. ..."
"... Out of more than 157 million fully vaccinated Americans, only 733 people had died of COVID-19 as of July 6, according to CDC data . At least 3,554 people had been hospitalized and survived. The CDC is no longer tracking mild breakthrough cases. ..."
Originally from:
Fully vaccinated people who got COVID-19 describe their mild symptoms, and their relief that
they'd gotten a shot
The COVID-19 vaccines are extremely effective, but a few vaccinated people have
gotten sick. "Breakthrough" infections are typically mild and might be less contagious than other
cases.
... ... ...
The COVID-19 vaccines have been extremely successful at preventing serious illnesses that
could lead to hospitalizations and deaths. But no vaccine is 100% effective at preventing
infection, Dr. Lisa V. Adams, an associate dean for global health at Dartmouth College, told
Insider.
"We know there are and will be some breakthrough infections in individuals who are
vaccinated - at least until we get to a point where there is very little virus circulating,"
Adams said. "The good news is that their illness should be very mild."
The vaccines
are designed to prevent hospitalizations and deaths In early July, Dr. Rochelle Walensky, the director of the Centers for Disease Control and
Prevention,
said new data indicated that 99.5% of COVID-19 deaths in the US were in unvaccinated
people.
Out of more than 157 million fully vaccinated
Americans, only 733 people had died of COVID-19 as of July 6, according to CDC
data . At least 3,554 people had been hospitalized and survived. The CDC is no longer
tracking mild breakthrough cases.
About 75% of breakthrough infections occurred in people 65 and older. That included cases in
nursing homes ,
whose residents and staff members were among the first Americans to get vaccinated.
Paul Offit, the director of the Vaccine Education Center at the Children's Hospital of
Philadelphia, told Insider that even with a smattering of breakthrough infections taken into
account, the vaccines had met the goal of protecting most people from severe illness.
"The goal of these vaccines is to keep you out of the hospital and keep you out of the ICU
and keep you from dying. If you have a mild infection where you're PCR positive and have
essentially an asymptomatic infection, that's fine," Offit said, referring to a type of
COVID-19 test.
'Breakthrough' cases might cause some symptoms, but they're usually mild
Emerging data suggests many breakthrough infections are so mild that they might as well be
asymptomatic.
A
recent analysis of breakthrough infections in the UK indicated that the top symptoms of
Delta-variant COVID-19 were a runny nose and a headache, largely because most people mingling
and exposed to the virus were younger or fully vaccinated.
As of Monday, there were 3,200 new COVID-19 cases in California, and now, medical doctors
are noticing some of the first numbers of COVID vaccine breakthrough cases.
...According to the states data, 74 vaccinated California's have died, however, the report
states it is unknown if the primary cause of death in these cases was COVID-19 or if there were
other alternate causes.
... According to the latest
state data, 20.4 million fully vaccinated individuals, 10,430 post-vaccination cases
(0.051%) have been identified.
That's one in almost 2,000 vaccinated Californians reporting a breakthrough case.
Background
Recently, India has seen a significant rise in new COVID-19 cases predominantly caused by
the delta variant (B.1.617.2) of SARS-CoV-2. Similar to the alpha (B.1.1.7), beta (B.1.351),
and gamma (P.1) variants, the delta variant has gained beneficial mutations in the spike
protein , which make it more infectious and pathogenic than previously circulating
variants.
The delta variant belongs to the B.1.617 lineage that is currently circulating in more than
50 countries. Because of its significant threat to public health, the delta variant has been
designated as the Variant of Concern (VOC) by the World Health Organization.
Studies investigating vaccine efficacy against
emerging SARS-CoV-2 variants have indicated that the delta variant is partially resistant to
vaccine-induced antibodies. A study conducted in the UK has indicated that the Pfizer/BioNTech
COVID-19 vaccines is 88% effective in preventing symptomatic disease caused by the delta
variant.
In the current study, the scientists have described the transmission of delta variants among
family members who were attending a wedding ceremony with 92 guests. The wedding events were
held outside in a large open-air tent, and all guests were fully vaccinated.
Important
observations
The scientists identified a total of six individuals at the wedding ceremony who tested
positive for SARS-CoV-2 and were symptomatic. Of them, one developed severe COVID-19 requiring
monoclonal antibody infusion and one died eventually. Based on encounter timings and viral
sequence similarities, the scientists suggested that two persons traveling from India probably
have transmitted the delta variant to other guests during the wedding events.
Related
Stories
Of two guests from India, one was a man without any comorbidities, and one was a woman with
diabetes. They both received the 2 nd dose of Covaxin (BBV152) 10 days before
traveling to the wedding venue. Moreover, they tested negative for SARS-CoV-2 before boarding
the flight.
Soon after developing symptoms including fatigue, cough, and fever, both guests from India
tested positive for SARS-CoV-2 infection. At day 6 post-wedding, the man without comorbidity
was admitted to a hospital because of worsening symptoms. One month after the wedding, he died
due to COVID-19 related complications.
Four other guests who also tested positive for SARS-CoV-2 had confirmed interactions with
the guests from India. Of 4 guests who were fully immunized with the Pfizer/BioNTech or Moderna
COVID-19 vaccine, one developed severe COVID-19 that required infusion of monoclonal
antibodies.
Testing of viral variant
Nasopharyngeal
swab samples were collected from all six guests and analyzed by reverse
transcription-polymerase chain reaction (RT-PCR) to detect viral variants. All samples tested
positive for the original Wuhan strain of SARS-CoV-2 and negative for the alpha variant. All
positive samples were subsequently sequenced by Swift Normalase Amplicon Panels with multiple
overlapping amplicons to identify the causative variant. The findings revealed that all six
guests were infected with the delta variant of SARS-CoV-2 (B.1.617.2).
Study
significance
Six vaccine breakthrough cases identified in the study highlight the notion that
antibodies elicited by Pfizer/BioNTech BNT162b2, Moderna mRNA-1273, and Covaxin BBV152 may not
be sufficient to provide full protection against the delta variant. Although some people fail
to develop adequate immunity in response to vaccination, none of the patients identified in the
study had a history of vaccine failure.
As mentioned by the scientists, mutations in three antigenic regions of the spike
receptor-binding domain (450–469 IDf, 480–499 IDg, and 522–646 IDh) could
potentially reduce the susceptibility of delta variant to antibody-mediated neutralization.
Defining a vaccine breakthrough infection
For the purpose of this surveillance, a vaccine breakthrough infection is defined as the
detection of SARS-CoV-2 RNA or antigen in a respiratory specimen collected from a person ≥14
days after they have completed all recommended doses of a U.S. Food and Drug Administration
(FDA)-authorized COVID-19 vaccine.
Identifying and investigating hospitalized or fatal
vaccine breakthrough cases
As of May 1, 2021, CDC transitioned from monitoring all reported vaccine breakthrough cases
to focus on identifying and investigating only hospitalized or fatal cases due to any cause.
This shift will help maximize the quality of the data collected on cases of greatest clinical
and public health importance.
Previous data on all vaccine breakthrough cases reported to CDC from January–April
2021 are available .
State health departments report vaccine breakthrough cases to CDC. CDC now monitors reported
hospitalized or fatal vaccine breakthrough cases for clustering by patient demographics,
geographic location, time since vaccination, vaccine type, and SARS-CoV-2 lineage. Reported
data include hospitalized or fatal breakthrough cases due to any cause, including causes not
related to COVID-19.
... ... ...
As of July 12, 2021, more than 159 million people in
the United States had been fully vaccinated against COVID-19.
During the same time, CDC received reports from 48 U.S. states and territories of 5,492
patients with COVID-19 vaccine breakthrough infection who were hospitalized or died.
Total number of vaccine breakthrough infections reported to CDC
Hospitalized or fatal vaccine breakthrough cases reported to CDC
5,492
Female
2,680
(49%)
People aged ≥65 years
4,109
(75%)
Asymptomatic infections
1,107
(20%)
Hospitalizations*
5,189
(94%)
Deaths†
1,063
(19%)
Infections and even hospitalizations due to COVID-19 have begun to increase since the Fourth
of July weekend. And it turns out that those vaccinated against the disease aren't completely
immune, as state officials revealed that there have been thousands of breakthrough infections
-- and even dozens of deaths -- among people who have gotten their shots since the rollout
began.
... ... ...
As of July 10, 4,450 vaccinated people in Massachusetts had tested positive for COVID-19
since the rollout began this past winter, according to the state's Department of Public
Health.
That 's just over 0.1 percent -- or one in a thousand -- of the 4,195,844 people in
Massachusetts who were fully vaccinated at the time.
Of that tiny faction, the overwhelming majority of cases weren't severe.
DPH officials say that 303 -- or 6.8 percent -- of the breakthrough infections involved
hospitalization and a total of 79 vaccinated individuals in Massachusetts have died.
... ... ...
Since June 25, the average number of new positive COVID-19 tests in the state has nearly
doubled, from 64 to 122. DPH officials also reported 208 new confirmed COVID-19 cases
Wednesday, the first single-day report over 200
since early June , a time when the state's testing rate was nearly a third higher.
Over the same time period, the state's positivity rate more than doubled from 0.31 percent
to 0.72 percent.
Following a steady decline this spring, hospitalizations have also increased from a low of
80 statewide COVID-19 patients on July 4 to 102 as of Tuesday.
...
According to the CDC, the Delta accounted for 10 percent of new cases in Massachusetts as of
June 22, but that data is now nearly a month old -- and predates the current uptick.
Cassandra Pierre, a Boston Medical Center epidemiologist and Boston University professor,
says the recent uptick in overall cases in "somewhat concerning" given the national rise of the
Delta variant.
"We have some data to show that the delta variant is responsible for more hospitalizations
than the previous dominant variant and while the jury is out on whether it's also more virulent
(capable of causing severe illness) we've begun to see COVID-related death rates rise in some
of the hardest hit states," Pierre told Boston in an email.
... ... ...
While experts have
predicted a mild, seasonal uptick in COVID-19 cases this fall, Pierre says the recent
increase is earlier than anticipated. She noted that the rainy weather over the Fourth of July
weekend may have pushed more gatherings and activities indoors.
DPH guidance says that unvaccinated resident should continue to wear masks when near people
outside their household, especially indoors. While the Delta variant has caused some cities and
organizations to extend that mask guidance to all individuals, regardless of vaccination
status, the still-low case rates have yet to induce such a move in Massachusetts.
... ... ...
State officials say they don't have a breakdown of the recent infections among vaccinated
and unvaccinated individuals, in part because the data on breakthrough cases is reported
separately (while health care providers report all positive tests directly to the state,
breakthrough cases are first reported to the CDC, and then to state officials).
However, earlier data on breakthrough infection
obtained by the Herald through a public records request suggests that there have
been 543 breakthrough cases between June 19 and July 10. That's roughly 30 percent of the 1,809
positive cases reported by the state over the same time period, meaning 70 percent of new cases
were among the minority of residents who were not fully vaccinated.
... over 83 percent of Massachusetts adults have gotten at least one shot
There's quite a bit about COVID-19 and vaccines that we still don't know.
While the vaccines are up to 95 percent effective against COVID-19, there have been
breakthrough cases. That's where those who are vaccinated test positive. The CDC
was monitoring all reported breakthroughs . However, back in May, as more people got
vaccinated, the feds transitioned to focusing on cases where someone went to the hospital or
died. They said that data would have the greatest importance.
"The question is are we getting more cases than we should be seeing as breakthrough cases,"
Dr. Jill Roberts at USF Health said. "That's really hard to determine because there isn't a
good source of data, so there's a lot of people looking at this. They're sequencing this strain
from the people who got breakthrough cases to see if it's really Delta variant or if the thing
has mutated again."
"We're trying to figure out what's going on. Is this really, truly a vaccine failure or is
it expected numbers? And without the data, we can't tell," she added.
Dr. Roberts says she would like to see
more information on variants – like which populations contracted them, if they're
vaccinated, and what they do for living so doctors can have a better idea of infection
control.
As states cut back on their COVID-19 data collection and fail to document
"breakthrough" cases , we are left to guess how often and where people are being infected.
I have said this a few times and now it is becoming real.
Read deeper to let me explain why the phrase "breakthrough" may be a disservice to the
public.
First, consider the case unfolding in Las Vegas, where the
Las Vegas Review-Journal reports :
At least 11 employees of Sunrise Hospital and Medical Center tested positive for COVID-19
after attending a party on June 7, according to Southern Nevada Health District emails
obtained through records requests by the Brown Institute for Media Innovation's Documenting COVID-19
project . The emails, which were shared with the Review-Journal, indicate that eight of
the employees had been fully vaccinated in December and January, meaning that the virus had
"broken through" the protection of inoculation.
Two other employees who were infected had received one dose of a double-dose vaccination.
One was unvaccinated. At least 10 of the 11 had the delta variant, a more easily
transmissible strain of the virus.
One question is whether the vaccines had been properly stored. But the hospital that
administered them said there was no problem with storage. Was there something unique about this
party that made transmission more possible?
Meanwhile, the Centers for Disease Control and Prevention and some states have stopped
gathering as much data as they once did. Again, the Las Vegas Journal-Review:
Beginning May 1, the Centers for Disease Control and Prevention stopped monitoring all
reported vaccine breakthrough cases, focusing instead on those resulting in hospitalization
or death. The state of Nevada and the health district, in turn, stopped reporting totals of
identified cases.
However, in a June 22 email, a health district official told other agency officials there
had been 471 identified breakthrough cases in Clark County, with 53 resulting in
hospitalization and eight in death. In other words, there were nearly 10 times as many
breakthrough cases identified as were publicly disclosed.
Nobody promised that there would be no breakthroughs. As WCVB explains , as with
any vaccine -- especially one protecting against a fast-changing virus -- some fully vaccinated
people will still get sick or become virus carriers. Remember, even in breakthrough cases,
vaccinated patients are far less likely to become seriously ill.
The Atlantic raises the issue of whether using the word "breakthrough" is harmful to the
public's understanding. Because, really, these are expected infections:
The thing to know about the COVID-19 vaccines is that they're flame retardants, not
impenetrable firewalls, when it comes to the coronavirus. Some vaccinated people are still
getting infected, and a small subset of these individuals is still getting sick -- and
this is completely expected .
We're really, really bad at communicating that second point, which is all about
breakthroughs, a concept that has, not entirely accurately, become synonymous with vaccine
failure. It's a problem that goes far beyond semantics: Bungling the messaging around our
shots' astounding success has made it hard to convey the truly minimal risk that the
vaccinated face, and
the enormous gamble taken by those who eschew the jabs .
The CDC has
a definition for "breakthrough cases." And, the CDC says:
As of July 6, 2021, more than 157 million people in
the United States had been fully vaccinated against COVID-19.
During the same time, CDC received reports from 48 U.S. states and territories of 5,186
patients with COVID-19 vaccine breakthrough infection who were hospitalized or died.
(CDC)
Keep in mind that the CDC no longer gathers "breakthrough" data unless the person ends up in
the hospital. This means that it misses a lot of cases since we know from the data that most
breakthrough cases do not result in sickness serious enough to send a person to the hospital.
To get an idea of what the data looks like when all "breakthrough" cases are reported,
look at the
January through April data , before the CDC changed its rules. More than 10,000 cases were
reported in that timeframe.
I like the way The Atlantic put all of this in perspective:
The overwhelming majority of the COVID-19 cases we're seeing are among the unvaccinated.
And when the virus does affect the immunized, it seems to accumulate to lower levels, and
spread less enthusiastically to new hosts; it's causing, on average, milder and more
transient symptoms.
A Covid Vaccine Crossroads - WSJ By The Editorial Board
... ... ...
But resistance has also formed among conservatives who are skeptical of pronouncements by
public-health experts and politicians, many of whom insisted without evidence that school
closures and economic lockdowns were necessary to contain the virus. Many Democrats, including
Kamala Harris and New York Gov. Andrew Cuomo, politicized the vaccines last fall to take down
Donald Trump .
Now some of the same people are disparaging the unvaccinated as backwards or crazy, much as
they do people who hold sincere religious beliefs. Many of them, including Anthony Fauci and
Democratic politicians, have little credibility with half the country.
government health bodies in the U.S. and other countries have analyzed rare adverse side
effects. These include myocarditis in young adults from the Pfizer vaccine, and
Guillain-Barré syndrome from the J&J vaccine. Their conclusion is that the benefits
outweigh the potential risks even in sub-populations.
The calculus for school-age children will be different because their Covid risks are so much
lower, and trial data won't identify 1 in 50,000 events. There's no need for K-12 schools to
mandate vaccines
SUBSCRIBER 2 hours ago Los Angeles just re-instituted its mask mandate for
everyone, vaccinated or not, indoors in a public building. Las Vegas is considering the same.
SUBSCRIBER 3 hours ago According to the CDC as of today:
68% of those over 18 have received at least one dose.
That sounds like mass vaccination has been achieved, and those who are at the highest risk
have almost all be vaccinated.
Given that, why force those who do not want it or those who have close to 0 risk of adverse
effects from covid to get it?
Per the state of TN, your survival rate for a CONFIRMED Covid case is 99.99% if you are
1-10, 100.00% if you are from 10-20, and 99.97% if you are from 20-30. Why are forcing the
folks to get shots they do not really need?
That is what most of us are objecting to. SUBSCRIBER 3 hours ago But an American 15 year
old's probability of dying in the next year is 0.0005, according to actuarial tables at the
Social Security Administration. Catching COVID increases their chance of death by 60 pct.
That is how a lot of families think about it. Like thumb_up 3 Reply reply Share link Report flag
B
Brian Johnson SUBSCRIBER 3 hours ago
And what is the probability they will catch COVID?
What is the probability of dying from the vaccine?
I am not against vaccines. I am fully vaccinated. In my case the risk reward was pretty
clear cut.
However, when the heart issues from the vaccines came to light, I paused about getting my
children vaccinated. What other side effects are their for children?
All summer I heard about the heart issues with athletes and covid. It was used as a
justification for the Big 10 not playing football.
The severity of the heart issues are pretty close between COVID and the vaccine. The
difference is there is a low chance of my child getting COVID but a 100% chance of vaccine
exposure if they get the shot.
So now, am I not supposed to worry about the heart issues?
BTW, I have a 16 year old who is about to get their license. I can't imagine what that
does to the probability of dying in the next year.
richard cheverton SUBSCRIBER 4 hours ago
First, take a deep breath, sit down with a cuppa tea, relax, and think.
Think about the phrase, "... the benefits outweigh the potential risks..." And reflect
that the so-called risks are not potential, but very real and documented with government
figures. Then assume that you are one of the "rare" cases of some complication; you took the
jab and paid the price for herd immunity. Congratulations!
Then contemplate the mutterings about "boosters," on top of the two required shots. How
come, you might wonder. Then look at spikes in infections in the UK and Israel, which are
highly-vaccinated nations. Why?
Then consider that government has offshored the enforcement of vaccine coercion to private
corporations, none of which have any expertise in virology, or epidemiology, and which are
not licensed to practice medicine.
Think about that.
Brian Johnson SUBSCRIBER 3 hours ago
All six Yankees players who have COVID were vaccinated, and they still need to sit out.
40% of COVID hospitalizations in Israel this week were vaccinated. The Pfizer vaccine is
at 60% effectiveness at preventing COVID in Israel and falling.
The vaccines do help, but they will not end COVID. At best, they will limit the damage to
high risk patients.
If you are at low risk of severe symptoms, why do you need the vaccine? Why are you being
forced to take it to go to school?
Robert Houston SUBSCRIBER 1 hour ago
The New York Public Health response to Covid was really ugly. The number of ICU beds per
population, ventilators, masks and lack of public health nursing services were critical to
the disaster. The Gov sent the infected elderly from public hospitals to private nursing
homes unprepared for their new public need (they didn't have refrigerated trucks and the
mortuaries would not take the infected dead). A vaccine will not cure these shortages and
their Public Health poor planning.
MARK VANDERMAUSE SUBSCRIBER 49 minutes ago
We all take risks every day, and consciously and not, weigh the benefit to be gained against
the inherent risk of an activity we participate in. William Cnossen SUBSCRIBER 5 hours ago
"Most Americans believe the personal benefits from vaccination outweigh the potential risks."
And for most people that is true. But for children and young adults with no amplifying
problems it may not be. Also if you have already had the disease the vaccine could do more
harm than good. For teacher's unions and government officials to make any blanket requirement
about mandating vaccine use just won't work.
There is a reason that freedom is such a powerful force in this country. Individuals
assessing their own conditions and risk tolerance is always better than one-size-fits-all
government edicts.
Robert Houston SUBSCRIBER 5 hours ago
The current administration has millions of "last year's" vaccines that they can't give away.
Yes, they ordered all of them because they thought that they would need to vaccinate
everybody: Fauci kept moving the goalposts. Unfortunately, (me being Swedish), the "natural
herd immunity" theory was actively censored as "too dangerous." Well, who is right and who is
wrong?
Look at the Covid death rates on the CDC web site. The pandemic in the USA is over. It
looks like we only needed to vaccinate the "high risk groups." Yes, we may need to get the
2021 updated Covid vaccine this fall (all for that). With the objective success in the USA,
forcing vaccinations with the current vaccines makes as much sense as selling lottery tickets
after the prize winner has received the payout.
richard crane SUBSCRIBER 6 hours ago
... it's pretty clear that Fauci et al destroyed their own credibility by lying and
guessing.
Alan Rigg SUBSCRIBER 6 hours ago
We have already had all the "mass vaccination" we have ever needed to have... of high-risk
individuals. Why should people who have a 99.98% chance of surviving coronavirus (which is
people under 50) and people with natural antibodies (as a result of recovering from
coronavirus) pursue vaccination?
Tom Richard SUBSCRIBER 7 hours ago
1. No mention of natural immunity of those who have had the virus. They are a legitimate part
of the percentage necessary for herd immunity and have no need of a vaccine. Jeffrey P SUBSCRIBER 7 hours ago
Tom
You should update yourself. Past infection isn't enough.
"Covid-19 Immune Response Could Be Long Lasting, but Variants Present Risks"
https://www.wsj.com/articles/covid-19-immune-response-could-be-long-lasting-but-variants-present-risks-11626439371?mod=mhp
Timothy Kenefick SUBSCRIBER 5 hours ago
Incorrect: As a recent article in Nature points out vaccination after infection results in a
much more robust antibody response and likely longer immunity (which can be less than a yr
after natural infection) and better coverage for infections with variants.
350+ children have died of covid far more that from seasonal flu for which we routinely
vaccinate. Covid itself causes myocardial inflammation and inflammatory disease at a rate
much greater that the vaccine.
Tom Richard SUBSCRIBER 5 hours ago
T cell and B cell response also lasts far longer than the initial antibodies that are
produced in response to the initial infection. Natural immunity could last far longer than
that produced by vaccines.https://www.nature.com/articles/s41577-020-00436-4
So now the neoliberal MSM narrative became that people who recovered from COVID-19 need to be
vaccinated as this strengthen their immune response to the new infection. So they are still
pushing "total vaccination of population" agenda, despite obvious fiasco of this agenda after
emergence of Delta variant. This valiant along with South African variant had shown that the
virus remains a threat and can propagate in fully vaccinated population. It is logical to expect
that it will mutate in the direction of of evading the protection provided by the first
generation vaccines and new variants after Delta will be even more efficient in infecting
vaccinated people. Corrupt neoliberal medical establishment does not have the courage to admit
that the virus outplayed them. This is a very questionable assumption indeed.
Most WSJ comments are highly skeptical of the official coverage... How thos medical brass
can't understadn that emergence of Delta variant was the writing on the wall? Why they behaved is
such strange and stupid way? What are their hidden assumption that dictated "there is no tomorrow
without total vaccination" response. Mortality does not justifies such a response and there are a
dozen more dangerious infectional desease in circulation that have higher mortality then
COVID-19. Is this because they suspect that the virus has artificl origin or what?
Also the whole idea of booster shots undermine the idea of "total immunization" and makes
achieving "herd immunity" impossible.
The durability of immune response after Covid-19 infection or vaccination is one of the most
important factors in the trajectory
of the pandemic , health experts say. Exactly how long the immune response might be
protective isn't clear, in part because the earliest known infections and vaccinations stretch
back only some 18 months at most.
The durability of immune response after Covid-19 infection or vaccination is one of the most
important factors in the trajectory
of the pandemic , health experts say. Exactly how long the immune response might be
protective isn't clear, in part because the earliest known infections and vaccinations stretch
back only some 18 months at most.
"We shouldn't get scared when we see the antibody response go down," said Miriam Merad,
director of the Precision Immunology Institute at the Icahn School of Medicine at Mount
Sinai.
Some immunologists have also reported other parts of the immune system adapting to recognize
the virus that causes Covid-19, such as Memory B cells that churn out antibodies and T-cells that can
direct an immune response or kill infected cells.
In a May study in the scientific journal Nature, researchers found Covid-19-specific immune
cells in the bone marrow from 15 of 19 patients who had experienced a mild infection as much as
eight months earlier. That indicates that their bodies were forming a lasting immune memory
against the virus, said Ali Ellebedy, an associate professor of pathology and immunology at the
Washington University School of Medicine in St. Louis and the senior author on the study.
"Those people have some partial protection remaining for a long time," Dr. Ellebedy
said.
Immunologists and health authorities caution that not everyone generates a robust immune
response following a Covid-19 infection, especially people who are older or have weakened
immune systems
... many people who are immunocompromised fail to elicit a strong immune response even after
full vaccination.
Israel has started giving booster shots to people with weaker immune systems as cases
caused by the Delta variant increase in the country.
... ... ...
Both Pfizer Inc.
and BioNTech SE as
well as Moderna Inc.
have demonstrated that their mRNA vaccines are effective for at least six months. A CDC
official earlier this week said the agency hasn't yet seen evidence of waning immunity among
people vaccinated as far back as December and January.
Covid-19 vaccines strengthen the immune response among people who have been previously
infected, immunologists say. In one cohort of 63 previously infected participants, 41% of whom
were subsequently vaccinated, researchers found that people who had been infected but not
vaccinated generated an immune response up to a year later.
me title=
People who were vaccinated after being infected generated more-effective antibody responses
against viral mutations.
"They basically become bulletproof," said Michel Nussenzweig, an immunologist at the
Rockefeller University and senior author on the study. "It's a big difference."
The CDC and many health authorities recommend that people who have previously had Covid-19
still get vaccinated to boost their immune response.
John Pound SUBSCRIBER 55 seconds ago
Man, the non-stop drug pushing in the media is bizarre. Google T and B cells as regards immunology and sleep easier.
Taiwan suffered less than 15 deaths from covid in 2020 and only 749 total to date from
both covid and the Delta variant despite a population of 24M and relatively lax covid
policies.
Why? Blood serology showed massive cross-immunization from SARS 2003 that swept through
Taiwan 18 years ago.
Mother nature was saving human lives long before Pfizer....
Girish Kotwal SUBSCRIBER 2 minutes ago
I am making a strong case for Covid-19 Immune Response being longer lasting, more robust and
broader in terms of emerging variants, than any of the current first generation vaccines
against COVID alone. I am gathering a ton of evidence not just theoretical prediction to
submit to a top journal for Med. Research. But let me summarize my rationale for making a
bold statement.
1) An average vaccinee has no higher antibody level against the surface glycoprotein of
SARSCoronavirus 2/COVID after the first vaccine dose of Pfizer or Moderna or after the single
dose of J&J.
Gregory Gustilo SUBSCRIBER 37 minutes ago
Are none of our health and govt officials going to bring up the possibilities, that, most
likely, after studying and comparing Sars 2 with the other 11 man made virus', it shares the
same unique fingerprint, that maybe, just maybe this is not a mutation at all, but a
completely different man made creation? Asking for a friend. Are we about to be bombarded by
"new" virus', which will create "new" vaccines and an eco system of big Pharma creating a
never ending source of revenue? Asking for a f different friend.
Ken Belcher SUBSCRIBER 5 minutes ago
As it is, marketing has driven the increase in diabetes, and lowered people's opportunities
to acquire immunity to common infections by pushing 'cleaning' products to needlessly
sterilize ones environment.
Even if Covid-19 was man-made, how would that change the rational responses to protect you
and your family from it?
kris thiruvillakkat SUBSCRIBER 46 minutes ago
Speculations, hypothesis, steady streaming by WSJ (and others). Long term? What months,
years? No clinical evidences, only studies; we haven't been on it long enough. Simple known
facts about most (if not all) viruses are known for years. So, in this respect, covid will
not be much different, say, from the flu viruses; it's just another "variant". And, we know
that flu vaccines offer limited immunity (months to a year), as they are mutating (into
different variants, fast- that's how they work). It would help to put this kind of facts in
perspective with covid also. Don't get stressed out or overly hopeful by reading these kinds
of coverage.
Dom Fried SUBSCRIBER 37 minutes ago
It is not a flu. I wish people would stop saying that. The mRNA vaccines are novel. No prior
flu vaccine has been mRNA. Neither the vaccines nor the viruses are the same, so any
conclusions you just drew based on past flu experiences are invalid and pure nonsense.
John C SUBSCRIBER 1 hour ago
Here is some news for you, T Swan. CA hospitals are now seeing a surge in Delta (or Epsilon,
I'm not sure which) cases in previously-vaccinated people. But Gov Gav CAN'T lockdown again
because he has a recall election this fall. So regardless of the science, Gav can't shut down
again because he knows he will be victim-blamed for the upsurge. He won't "follow the
science" because now it's politically inconvenient for him. But there will have to be new
mask mandates shortly in CA and that alone might create enough of a political whirlwind to
recall the governor.
If COVID will become endemic virus how any professional can talk about herd immunity? For
example, how would you rate the following statement ""The higher infectivity of Delta means the
threshold for herd immunity will be higher." He says while a 70% vaccination rate may have been
enough to reach herd immunity against the initial strain of COVID-19, it "likely isn't high
enough against Delta, as shown by case increases in places like the UK and Israel, which have
high vaccination rates." Former NYC Health
Commissioner- Threshold For Herd Immunity Against COVID-19 Will Be Higher
If 80% of a population is immune to a virus, four out of every five people who encounter
someone with the disease won't get sick (and won't spread the disease any further). In this way,
the spread of infectious diseases is kept under control. Depending how contagious an infection
the threshold need to be higher and generally varies from 50 to 95%. Measles, for example,
spreads so easily that an estimated 95% of a population needs to be vaccinated to achieve herd
immunity. For polio, the threshold is about 80%.
If Delta variant infects 30-40% of vaccinated (who then can spread the virus) and threshold
for immunity for COVID-19 is over 80%, it looks like herd immunity in unachievable with the
current generation of vaccines (not sure about natural immunity) It looks like the situation with
COVID-19 vaccines is similar to the situation with vaccines for flu and the idea of creating
efficient multi-year vaccine against coronavirus is on very shaky ground. Taking into account the
amount and severity of adverse effects any vaccine need years of testing before the distribution
to the general population can be approved. Side effects of the current generation of vaccines are
largely unknown but they already include death, paralysis and myocarditis (for Pfizer) and
neurological disorders (For J*J and AstraZenica vaccines)
We do not know how many people have natural immunity to COVID-19. All we have are cruel
natural experiments on cruise ships, especially famous Diamond Princess epidemic (712 out of 3711
tested positive, 14 dead). This shows that natural immunity can be significant. Quarantine!, a
book written by passenger Gay Courter on her experience on board the quarantined vessel, was
released in November 2020. The HBO documentary The Last Cruise tells the story of the voyage.
This is not the firs mass infection on cruise ships: norovirus was the typical epidemic on cruise
ships for a long time...
There is a difference between protecting with vaccination the most venerable (say people from
65 years old, morbidly obese, and some other categories) and the mass vaccination campaign
unleashed without sufficient testing.
... ... ...
"I wouldn't be declaring mission accomplished. I think this is going to be a long fight,"
Gottlieb said Sunday. "You're seeing a decoupling between cases, hospitalizations and deaths
because there's so much immunity in the population" not just through vaccination" but also
through prior infection... But this is likely to become an endemic virus. We're going to
have to deal with it. "
In recent weeks, Israeli media has become a factory for stories that cut against the
'official' 'scientific' narrative about the COVID-19 vaccines. Most visibly, I srael
has made a deal with Pfizer to start doling out "booster" shots for the most vulnerable
Israelis, despite the FDA's insistence that there's "no evidence" that a booster shot is
necessary.
Now, the Israeli Health Ministry has discovered that the number of patients who had been
infected prior to becoming infected again during the latest Delta-driven wave of the pandemic
were less likely to be reinfected than patients who have only been vaccinated. The finding
directly contradicts research spouted by American experts like Dr. Fauci, along with Pfizer and
Moderna, who have previously insisted that the antibodies created by their jabs are more
powerful than antibodies produced by natural infection (which is one reason even the previously
infected have been asked to get vaccinated).
According to Israel National News , more than
7.7K new cases of the virus have been detected during the most recent wave (beginning back in
May). However, just 72 of the confirmed cases were reported in people who were known to have
been previously infected - that is, less than 1% of the new cases.
Roughly 40% of new cases "" involving more than 3K patients "" were infected despite being
fully vaccinated.
By this count, Israelis who had been vaccinated were 6.72x more likely to get infected after
the shot than after natural infection, with more than 3K of the 5,193,499, or 0.0578%, of
Israelis who were vaccinated getting infected in the latest wave. The disparity has confounded
Health Ministry experts, with some saying the data proves the higher level of immunity provided
by natural infection versus vaccination. However, others remain unconvinced.
Israel's Health Ministry previously estimated that the efficacy of Pfizer's COVID jab
was only 64% against the Delta variant , which helped prompt Pfizer and its partner
BioNTech to develop a new jab designed to protect against variants including Delta and Beta
(the variant first discovered in South Africa).
Lord Baltimore 3 hours ago remove link
"Roughly 40% of new cases "" involving more than 3K patients "" were infected despite
being fully vaccinated."
Which implies that it's not really a vaccine.
Plus Size Model 2 hours ago
It was a privilege worth waiting for hours in line a few months ago! Ha
I'll never forget watching some poor guy on CNN suffer while being taunted by a bunch of
newsmen hyping up the juice. The poor guy looked like he was dying from COVID and the
interviewer claimed that, anecdotally, the vaccines can work miracles. He also claimed that
the vaccine can, anecdotally of course, clear up this guy's symptoms that he's been having
for the past year.
The guy was just wrecked. He could hardly sit up without fainting, couldn't sleep, and
often had to cool his feet off in icewater.
At the end of the vaccine advertisement, the interviewer had the audacity to claim that
he wasn't eligible for the vaccine yet and had to suffer for a few more months.
Sadists!!
GreatUncle 1 hour ago remove link
Those participating in the experiment ... the issue is not necessarily the vaccine i t
is what changes it makes to the rest of your immune system . If you had measles ... has
that immunity been wiped people should be asking because NOBODY KNOWS!
This is why people with a poor disposition to vaccines will get an adverse outcome.
Do the test ... let 10000 people be vaxxed and now write down on the persons vaxxed card
this one gets Guinne & Barrie. Get 100% right and no errors or guesses then I would
consider you a real pro.
But then if you were that good you should be pulling that person out and saying no vaxx
for you ... so in effect those vaxxing are no better than murderers and fast approaching
10K kills.
THAT LOGIC TELLS ME THIS MASS VACCINATION IS MORALLY REPREHENSIBLE.
hwinoree 3 hours ago
How mRNA Vaccines
Work
philipat 2 hours ago
By definition, the mRNA and DNA devices are experimental gene therapies, not vaccines.
Their issued patents confirm this.
Even according to the manufacturers, these products do NOT induce immunity and do NOT
prevent transmission.
They are, in fact "leaky" prophylactic therapies which simply claim to reduce the
severity of symptoms. There are risks of using such products in the middle of a pandemic,
as set forth by Dr Geert Vanden Bossche.
HowdyDoody 2 hours ago
"Which implies that it's not really a vaccine."
Pfizer/Moderna/AZ are not. The acceptance criteria for a 'successful vaccine' was never
'reduction of symptoms in some cases of the disease.'
LetThemEatRand 3 hours ago
Funny how the "conspiracy theorists" predicted this months ago. I suppose social media
and other big tech will allow people to post comments and videos about this now that mother
Israel said it's true? Or not. Maybe they will ban the Israeli government for spreading
disinformation for a while before they get a call from the ADL.
serotonindumptruck 3 hours ago
The propaganda is now coming fast and hard.
Not only are "vaccine" passports being suggested (and implemented), but now "booster"
shots are being forced down everyone's throats.
Masking these mandates behind Israel only raises my suspicions.
Are Israelis receiving placebos and vitamin shots in lieu of the genocidal kill
shots?
Plus Size Model 3 hours ago
I'm seeing some goofballs / paid agents / bots requesting a drip line like it's
chemotherapy. It's hilarious making them explain their logic. It's even funnier what they
come up with.
Plus Size Model 2 hours ago
Doesn't look like it. They've got the same drama going on there too. This guy claims the
vaccines killed lots more than the virus itself and got "fact checked" by some whatever
website.
https://healthfeedback.org/claimreview/data-from-israel-showed-that-the-pfizer-biontech-vaccine-reduces-the-likelihood-of-dying-from-covid-19-analysis-in-a-forum-post-claiming-the-opposite-is-flawed/
philipat 2 hours ago (Edited)
With the exception of high risk group (mostly the age cohort > age 70), natural
infection is better protection for everyone against any Covid in terms of the risk/benefit
equation (a/k/a informed consent). The survival rate in this group is 99.95% whereas the
vaccine AE risk is not insignificant. Natural immunity also provides a broader, deeper and
longer-lasting.
But we are still being lied to about :
Naturally immune people still need vaccination. The scientific fact is they don't and
in fact there may be dangers (ADE, or Pathogenic priming) in doing so. Why the
lies?
Herd Immunity can only be achieved through vaccination. The WHO has changed its
definition and M-W dictionary has revised its defintion accordingly. But again the
science does not support this. In fact, the experiences of both Diamond Princess and USS
Theodore Roosevelt both suggest (albeit only anecdotally) that only 20% of the population
will ever become infected. This is consistent with scientific assessments which have
variously estimated that up to 80% may have pre-existing immunity. There is a good
possibility that Herd Immunity had already been reached BEFORE the "vaccine" rollout
started and that the "fall in new cases" was more attributable to the decline in
testing.
So why all the lies and denial of science? Are there other reasons, perhaps, for the
obsession with "vaccinating" everyone, even those who don't need it (the already immune and
children) and pregnant women, where normal medical precaution suggests that it could at
least wait until after delivery?
Kassandra 2 hours ago (Edited) remove link
Unlike some say, it's a real illness. Had it early on, Dec 2019 into Jan 2020. Dry,
brutal cough. Felt like I broke a rib. Fever went to 104.2 after that I can't remember. Too
sick to go to Dr. Sweats to make the sheets wet. I realized if it got any worse, I should
go to ER. Also realized all I had to do was breathe. Lay on my side and had the heating pad
on high on my upside lung area..and concentrated on breathing. And everything tasted like
nothing..cardboard or worse. I'm in my 60s..decent health. But it was no joke. I've
survived a lot of nasty **** including staph pneumonia, twice, as a child. This was worse.
They can't possibly make a vaccine against this. You couldn't pay me any amount of money to
take the vaccine.
CatInTheHat 1 hour ago
The tests were/are a FRAUD..
They were deliberately run at high cycle thresholds (35-42), guaranteeing FALSE
positives.
The American people have beem so dumbed down, that stupid gov slogans like flatten the
curve, social distancing and my personal favorite ASYMPTOMATIC, that convinced a nation of
healthy people that they were sick FOR OVER A YEAR, they no longer recognize truth and
******** out of gov.
THAT is frightening. Honestly stupidity ignorance and flat out NARCISSISM from Dem
voters via this massive hoax they bought into hook line and sinker does NOT bode well for
the future. One wonders what it will take to wake them up. I thought dead and injured
CHILDREN would do it. But NOPE.
Johnny Walker 2 hours ago (Edited) remove link
Explained why you should NOT take the jab:
https://principia-scientific.com/doctor-heart-failure-from-mrna-jabs-will-kill-most-people/
https://www.bitchute.com/video/OUJXK7t9UUaW/
CatInTheHat 1 hour ago
What kills me is that these murderers call myocarditis MILD..
If you get onto Telegram and head over to the MRNA DEATH TOLL group you'll see just how
"mild" this is for CHILDREN
rejectnumbskull 1 hour ago
The bitchute video with the doctor was really good. Very important. EVERYBODY should
watch it.
Sluggo315 2 hours ago remove link
Dr. Kurt Vanden Bossche predicted this would occur. He made videos proclaiming that the
world should not be vaccinating during a pandemic because of exactly this reason. I just
did a Google search and his name never even appeared in the predictive function when typing
his name. Why? The vax should be stopped immediately and anyone associated with Phizer,
BioNTech, Moderna, J and J, Gates Foundation, Schwab Foundation should all be put on trial
somewhere for crimes against humanity!! IMO. Will they? Hell no, the media will just say
this is all a big conspiracy...
Multi 1 hour ago
France (Macron) just made mandatory proof of vaccination to ENTER SHOPS and USE PUBLIC
TRANSPORTATION .
ay_arrow
Jim in MN 1 hour ago
Let's also please keep reminding people of the new UK data on children in which less
than one in FOUR MILLION healthy children actually died from this. Compare that to the risk
of a completely new mRNA serum that actually targets an extremely rare and poorly
understood type of immune cell--and one of the only things we do know about these immune
cells is that altering their function plays a major or even key role in autoimmune
disorders.
Millions of kids. Playing Fauci Roulette with life-long debilitating or fatal side
effects.
Just stop all of this. It's madness, or worse.
fackbankz 1 hour ago
All I hear on the news is how 99% of "cases" in the US are in unvaccinated people.
Somebody's lying, and in this case, I definitely trust Israel's numbers.
JD59 2 hours ago (Edited)
The US Gov., big pharma, and the media have been lying to the world the entire time
about this bug.
trailer park boys 1 hour ago
What am I missing here?
"...less than 1% of the new cases were reported in people who were known to have been
previously infected."
"Roughly 40% of new cases "" involving more than 3K patients "" were infected despite
being fully vaccinated."
"By this count, Israelis who had been vaccinated were 6.72x more likely to get infected
after the shot than after natural infection."
The math doesn't add up - or am I reading this wrong?
LEEPERMAX 3 hours ago
😳Wow
CoronaGate Update :
https://brandnewtube.com/watch/dr-david-martin-dr-reiner-fuellmich-july-9-2021_RlmKScwsMf6ATEG.html
Imxploring 1 hour ago
No doubt the human body is the best machine to produce durable antibodies.... artificial
methods work.... but are limited.
Po0h Bear 1 hour ago
Psaki Slip: "˜Vaccines Can Kill You if You're Under 27'
https://www.infowars.com/posts/psaki-slip-vaccines-can-kill-you-if-youre-under-27/
CheapBastard 2 hours ago (Edited)
Bottom line:
Lots of politicians, doctors and corporations and esp Big Pharma are benefiting greatly
either financially from this or enabling them to exert more CONTROL on people. It comes
down to:
USGrant 1 hour ago (Edited)
If the population of Israel is 9 E6 and the number of delta cases is 7.7 E3 then there
is to date a 7.7E3/9E6 =.000856 or .0856% chance of coming down with it. It may be more
likely you will choke on a mouthful of steak.
5.1E6 have been jabbed or 5.1E6/9E6 or 56.6% jabbed and then 3.9E6/9E6= 43.4% unjabbed.
So getting delta if unjabbed is 3.08E3/3.9E6=.00079 or .079%. So .0856/.079=1.1 times more
likely to come down with delta if jabbed versus unjabbed. So jabbing confers nothing.
Natural immunity confers a large advantage as a minuscule number of 72 is assigned to those
confirmed to have been originally infected.
Captive 34 minutes ago (Edited)
All we can say is that so far, the number of individuals being infected by the delta
variant who had previous infections is small and the number of those infected who were
previously vaccinated is similar to the background rate of infectivity. Which, like you
concluded, likely means that vaccination imparts little added benefit but natural recovery
is likely protective. Quantifying it... I agree, not possible without knowing precisely how
many in Israel had previous infections.
Bob Lidd 2 hours ago remove link
Until an infectious disease crisis is very real, present, and at an
To sustain the funding base beyond the crisis, we need to increase public
A key driver is the media, and the economics follow the hype. We need to use
that hype to our advantage to get to the real issues. Investors will respond if they
see profit at the end of process,
Peter Daszak - President of EcoHealth Alliance
https://www.brighteon.com/a569c7c9-9572-47ed-ba3c-130b0c13aa55
desertboy 2 hours ago remove link
Similar results to the 52,000 participant cohort of the Cleveland Clinic recently
published, showing dramatically better response from naturally-developed immunity than from
the vaccinated.
But Professor Sucharit Bhakdi is a kooky conspiracy theorist,
and Fauci is not a politician.
Po0h Bear 1 hour ago
Italian Neurosurgeon Who Operated on Young Covid Vaccine Victim Says "Never Seen
Anything Like This"
Neurosurgeon interviewed by Italian media says brain of 18-year-old girl swelled to
point that skull was opened to relieve pressure. She passed away days later
'I had never seen a brain that was affected by such an extensive and severe
thrombosis.'
https://www.infowars.com/posts/italian-neurosurgeon-who-operated-on-covid-vaccine-victim-says-never-seen-anything-like-this/
Jim in MN 1 hour ago
Let's just check their math shall we?
Total population = 9,371,370 https://en.wikipedia.org/wiki/Israel
Total new cases = 7,700
'Known recovered' = 835,792 per the article
New cases among recovered = 72 or .00862% infection rate
'Vaccinated' = 5,193,499
New cases among vaccinated = 'over 3,000' but we'll call it 3,000 or .0578% infection
rate
That leaves 4,628 new cases among the rest of the 'status unknown' population of
3,342,079. 0.139% infection rate.
A few observations, first, 7,700 'cases detected' is itself in total less than one tenth
of one percent of the population. Just saying.
The infection rate among the vaccinated is indeed 6.7 times that of the 'recovered'. The
'status unknown' rate is another 2.4 times that.
OutaTime43 22 minutes ago (Edited)
People in their 30's are dying from Covid (delta). Even those without pre conditions.
So, stop listening to this misinformation targeting conservative readers please. It's
probably being done on purpose.
99% of those right now being hospitalized with Covid 19 are unvaccinated.
green_dog 10 minutes ago
Please, provide a link to data supporting your claim about the deaths in the younger age
group with no co-morbidities.
C0rnelius 11 minutes ago
where is your source that 99% of those hospitalized with delta are unvaccinated? The
first delta case in the US was back in March and deaths have continued to trend down. Covid
is clearly becoming less deadly as it mutates.
OutaTime43 7 minutes ago (Edited) remove link
Here you go boss. This is a fact.
https://newsroom.clevelandclinic.org/2021/05/12/most-covid-19-infections-and-hospitalizations-are-in-unvaccinated/
More recent data from Virginia..
https://fredericksburg.com/news/local/99-of-virginians-who-died-from-covid-19-since-january-were-unvaccinated/article_6f4be63e-cc02-54ce-b306-ae82dfa1b406.html
Also, here's the case rate per population. The highest case rates are in the lowest
vaccinated states.
https://covid.cdc.gov/covid-data-tracker/#cases_casesper100klast7days
Moderna's Next Act Is Using mRNA vs. Flu, Zika, HIV, and Cancer
The biotech has reached a $100 billion market cap. But after Covid, the challenges get even bigger.
By Robert Langreth July 14, 2021, 5:00 AM EDT Updated on July 14, 2021, 10:15 AM EDT SHARE THIS ARTICLE
Share Tweet Post Email
A year ago, Moderna Inc. was an unprofitable company with
no marketed products and a promising but totally unproven technology. None of its experimental drugs and vaccines had ever completed
a large-scale trial. Experts were divided on how well the mRNA-based Covid-19 vaccine it was about to enter in a Phase III trial
would stack up against older, more established vaccine technologies.
Listen to this story
This year, Moderna could deliver 1 billion doses of its Covid shot and bring in $19 billion in revenue. It's become the rare biotech
to hit the big time without being gobbled up by, or splitting profits with, a larger, more established company. Its market value""which
hit $100 billion for the first time on July 14th""exceeds that of stalwarts such as
Bayer AG , the German inventor of aspirin, and biotech peers
such as Biogen Inc. , founded three decades prior.
The speed with which Moderna and its primary mRNA competitor, a partnership between
Pfizer Inc. and
BioNTech SE , devised their shots has made a major contribution
to the fight to end the pandemic. With strong efficacy, steady supply, and no show-stopping safety scares (officials are carefully
monitoring rare heart inflammation cases in teenagers and young adults), mRNA shots have become the vaccines of choice, at least
in countries that can get them.
But for Moderna Chief Executive Officer Stéphane Bancel, the Covid vaccine is just the beginning. He's long promised that if
mRNA works, it will lead to a giant
new industry capable of treating most everything from heart disease to cancer to rare genetic conditions. Moderna has drugs in
trials for all three of these categories, and Bancel says his company can also become a dominant vaccine maker, developing shots
for emerging viruses such as Nipah and Zika, as well as better-known, hard-to-target pathogens such as HIV.
In the past 40 years, more than 50 new human viruses have been discovered. Only three have authorized vaccines. Bancel views that
as an opportunity. "We are going to totally disrupt the vaccine market,"� he says during a late May interview at Moderna's Cambridge,
Mass., headquarters, which fills a 10-story building north of the MIT campus. The Swiss drugmaker
Novartis AG occupies labs in an adjacent building, and Pfizer
and Merck & Co. have offices a few blocks away.
Bancel, who's 48, wears a pressed blue shirt, dark blue jeans, and a black Hermès belt. An avid runner, he appears even trimmer
in person than on his frequent virtual conference appearances. He repeatedly jumps to his feet during the interview to graph on a
whiteboard how the Covid outbreak could evolve. One chart forecasts seasonal waves, declining each passing year but still significant.
Another projects the possible decay of vaccine efficacy over time, with mRNA shots like his starting in the best position but gradually
declining. The take-home message coincides neatly with Moderna's business prospects: Countries may want to stockpile
booster shots soon. "My mother is 72, and she has leukemia,"� he says. "I don't want her to go through the fall without a boost."�
The company has vaccines for 10 viruses that are in, or about to be in, human trials. These include three types of Covid-19 boosters
that are in midstage trials, a seasonal flu shot that began its first human study in July, and HIV shots that are slated to begin
studies later this year. The furthest along besides the Covid shots combats cytomegalovirus, a ubiquitous bug that spreads through
bodily fluids and is a common cause of birth defects; it's set to begin a Phase III trial this year in women of childbearing age.
In the long term, Moderna is aiming to develop an annual supershot that could suppress numerous respiratory ailments, including Covid,
the flu, and others. "Our goal is to give you several mRNAs in a single shot at your local CVS or GP every August or September,"�
Bancel says.
Now comes the difficult part: delivering on that promise while keeping ahead of just about every other vaccine company in the
world as they rapidly invest in mRNA. In the future, Moderna won't have the pandemic to highlight mRNA's most obvious advantages
over older technologies""speed and flexibility. Future vaccines and drugs will usually have to go through the U.S. Food and Drug
Administration's normal approval process, meaning longer follow-ups to gather data and 6- to 10-month review timelines. That time
frame will provide space for mRNA-wielding rivals and older technologies to compete.
Pfizer, with its partner BioNTech, has become an mRNA manufacturing juggernaut and
expects to produce 3 billion doses this year; it has also dominated foreign distribution of mRNA vaccines so far. Another vaccine,
from CureVac NV in Germany, which took a different approach
to mRNA, performed tepidly, proving only 48% effective in Phase III trial data released in June, but still another, from China's
Walvax Biotechnology Co. , will soon begin Phase III testing
in seven countries.
More established technologies are reasserting themselves, too. On June 14,
Novavax Inc. said its recombinant protein vaccine was
90% effective in a nearly 30,000-person trial in the U.S. and Mexico, with relatively few side effects""results that more or
less matched those of the best mRNA shots. Vaccine giants Sanofi
and GlaxoSmithKline Plc are in Phase III trials on their
own protein-based Covid vaccine, which could hit the market by yearend.
Mani Foroohar, an analyst at SVB Leerink LLC, calls Moderna's accomplishments with the Covid vaccine "truly breathtaking."� But
he also says it's far from certain whether such vaccines will have clear efficacy advantages with other viral diseases. And how big
a role the technology could play in treating noninfectious diseases such as cancer is unknown. So though public expectations are
boundless, he says, "the revenue opportunity is not."�
The reply, for Bancel and the others pouring money into tiny RNA strands, lies in those two key advantages of speed and adaptability.
At their heart, mRNA vaccines are a modular technology; they deliver the genetic code telling cells how to make the virus proteins
that provoke an immune response, and the cells do the hard work from there. Now that Moderna is profitable and sitting on almost
$8 billion in cash""Bancel's own stake, including options, is worth around $7 billion, according to the Bloomberg Billionaires Index""it
can move quickly and aggressively into numerous new applications simply by changing the genetic code it puts into the mRNA. While
Moderna's shot appears to be holding up well against the currently surging delta variant, for example, it's a straightforward process
for the company to incorporate mutations into the vaccine if needed. "We don't have to introduce new technology or new processes,"�
Bancel says. "It's exactly the same thing."�
When Bancel left the top job at the French diagnostics company BioMérieux SA and became the second employee at Moderna""the name
is a mashup of "modified"� and "RNA"�""a decade ago, the idea that messenger RNA could be medically useful was radical. At the time
the molecule, which evolved to carry protein blueprints from DNA in the cell's nucleus to the compartments that synthesize proteins,
had a reputation among lab scientists as fragile and hard to work with. When mRNA is artificially inserted in the human body, the
immune system identifies it as a threat and attacks it. And because mRNA's function is temporary, enzymes found throughout the body
can break it down. Neither are desirable outcomes for a drug or vaccine.
Starting in 2005, two researchers at the University of Pennsylvania, Katalin Karikó and Drew Weissman, managed to slightly modify
mRNA so it generated less of an immune reaction in the body. The finding drew little recognition at the time, but it turned out to
be a critical advance. (Katalin left Penn to join BioNTech in 2013.) In 2010 a trio of Harvard and MIT scientists funded by venture
firm Flagship Pioneering picked up on the idea and founded Moderna, bringing Bancel on the next year. Moderna and BioNTech later
licensed the Penn technology.
Bancel recalls telling his wife before he changed jobs that there was a 5% chance the mRNA concept would succeed, but if it did,
it would be huge. When Bancel pitched Moderna's now-president, Stephen Hoge, on the company the following year, Hoge says, his reaction
was, "He's either brilliant or crazy."� Hoge was then a McKinsey & Co. partner with a medical degree, and he was interested in doing
something that would have more societal impact. He slowly came around to Bancel's view that mRNA therapy, if it worked, "was really
going to transform medicine."�
"The smart countries are saying, "�I'd rather be two months too early than two months late'"�"�
The concept behind mRNA vaccines is simple. When the shots bring those protein-making instructions to cells, they effectively
turn them into microscopic vaccine factories in their own right. This allows developers to streamline what is normally a messy manufacturing
process. Many flu vaccines, for example, are made inside chicken eggs, and even newer genetically engineered vaccines still require
growing viral proteins inside vats of live cells. Bypassing such steps lets mRNA vaccine manufacturers shift gears fairly quickly.
It also appears to be relatively easy for them to make complicated vaccines involving multiple viral proteins.
"Everything with mRNA is just simpler,"� says Barney Graham, deputy director of the Vaccine Research Center at the National Institute
of Allergy and Infectious Diseases (Niaid), whose lab has been formally collaborating with Moderna since 2017. "For me, making vaccines
that are as simple as possible is the way to go."� Graham says gene-based shots such as mRNA vaccines are particularly well-suited
to fighting viruses, because they seem to be adept at producing the so-called killer T-cells that destroy virus-infected cells.
Before Moderna could create an mRNA-based product, it had to crack the problem of how to protect the molecule from the body's
defense systems. By modifying the RNA, the Penn researchers had figured out how to dampen the hair-trigger immune response it provoked,
but their approach would be useless if it were broken down by enzymes before it could reach cells. The key to solving that problem
turned out to be adding protective lipid nanoparticles to surround the mRNA molecules""essentially creating "balls of fat with little
bits of RNA mixed in there,"� says Kerry Benenato, a chemist who left AstraZeneca Plc to join Moderna in 2014.
When Moderna started working on this approach in 2013, it had been tried mostly on much smaller types of RNA molecules, and there
were concerns about side effects. "People had decided they were toxic,"� Hoge says. Nanoparticles contain synthetic fats, and in
early iterations some of those fats tended to accumulate in cells, building up over time and potentially causing liver damage or
other side effects.
Benenato's assignment was to devise nanoparticles that could safely and efficiently carry the mRNA into cells, release the payload,
and then quickly break down. When she started, the chemistry involved in using nanoparticles with mRNA was so unexplored that there
were few published scientific papers to guide her. She and her team made one tweak after another, pinpointing changes that improved
tolerability without harming their ability to deliver mRNA. By 2015, Moderna had made a breakthrough, finding a series of lipid molecules
that fit the bill. "Then it was off to the races,"� Benenato recalls. They patented the formulas and started deploying them in vaccines.
In its early years, Moderna had focused on therapeutics, including programs for cancer, heart disease, and other lucrative areas.
The company gradually turned to vaccines as Bancel realized they would be the best way to prove mRNA technology worked. You have
to inject only a couple of doses to stimulate a long-lasting immune reaction.
Working with Graham's team at Niaid, Moderna began formulating a Covid vaccine as soon as Chinese scientists released the coronavirus
RNA sequence in early January 2020. Later that month, Bancel asked his manufacturing chief what it would take to make a billion vaccine
doses in 2021. "He looked at me like I was insane,"� Bancel recalls. The Moderna plant had never made more than 100,000 doses of
anything in a year. The U.S. government agreed to pay $955 million for the vaccine trials and initial small-scale production, but
Bancel says he couldn't initially persuade any country to pay for a full scale-up. Moderna instead raised $1.3 billion in a May 2020
stock offering for the purpose. The move allowed the company to take its leap onto the world stage""and laid the groundwork for what
comes next.
Moderna produces its nanoparticles and mRNA in a former Polaroid factory in the Boston suburb of Norwood, 15 miles south of its
headquarters. The plant, which opened in July 2018, has been running around the clock since November. It looks less like a factory
than like a cross between a tech startup and a molecular biology lab. Dozens of operations and quality-control workers dressed in
casual clothing occupy a large warren of open-layout desks in the front of the building. Covid vaccines are produced in clean rooms,
some of which are visible behind glass panels in the back. There are nine of these clean rooms making the shot here, up from three
in December, and six more are scheduled to be running by the end of the year. The suites, which are roughly 1,000 square feet each,
were built for flexibility, with mixing reaction vessels, chromatography instruments, and other equipment on wheels so they can be
easily reconfigured.
The process starts with pieces of DNA called plasmids that Moderna brings in from a contract manufacturer. These plasmids contain
the genetic blueprint for the Covid-19 spike protein. In one set of clean rooms, the spike protein DNA is synthesized into mRNA using
a technique called in vitro transcription. It's basically the laboratory version of a process that normally occurs in cell nuclei.
The mRNA solution can be made in a matter of hours, says Scott Nickerson, a senior vice president who oversees the site. It then
takes several days to purify unreacted enzymes and other extraneous material. From there, the purified mRNA goes to a separate set
of clean rooms, where workers spend another few days formulating it with the lipid nanoparticles. The final product is frozen in
sterile bioprocessing bags, encased in a protective shell, and shipped in temperature-controlled trucks to Catalent Inc.'s plant
in Bloomington, Ind. There the vaccine is diluted, put into vials, labeled, and shipped. When Moderna started making the Covid vaccine
in commercial quantities last year, the process took as long as 19 days to complete. Now it takes only 10 days to prep a batch for
shipping to Catalent.
Last May, Moderna
signed a 10-year deal , since expanded twice, with Lonza Group
AG , which is expected to produce the bulk of its European supply at factories in Switzerland and the Netherlands. Moderna also
made pacts this year with Sanofi, Samsung Biologics, and Thermo Fisher Scientific to bolster the vial-filling capacity that Catalent
and Laboratorios Farmacéuticos Rovi in Spain currently provide. Increasing so-called fill-finish capability will become important
as a greater share of the population is vaccinated and doctors can't find enough patients to use up the larger vials now in use,
which contain between 10 and 15 doses.
Moderna's production this year, 800 million to 1 billion doses, will amount to only about a third of Pfizer and BioNTech's output.
Pfizer had "100 times more people"� at the start of the pandemic, along with existing plants it could retool for vaccine production,
Bancel says. Moderna's head count has almost doubled since last year, to 1,500. Next year, with more capacity and a significant portion
of its output potentially going into booster shots and pediatric formulations that use lower doses, the company and its partners
expect to produce
as many as 3 billion doses , approaching Pfizer and BioNTech's projected 2022 supply of 4 billion. If Novavax meets its production
goals, Sanofi's protein-based vaccine also works, and companies such as Johnson & Johnson and AstraZeneca solve their manufacturing
bottlenecks, at some point next year the world could shift from being desperately short of Covid shots to swimming in them.
As the virus settles down to a more manageable threat over the next few years, Covid vaccine sales may decline""perhaps precipitously.
Morningstar Inc. analyst Karen Andersen says this market could top out at $72 billion worldwide this year, slip to $65 billion in
2022, and plummet to $8 billion a year after that. The extent of the slide will depend on how many people need booster shots, how
often, and whether Moderna, Pfizer, and others will be able to raise prices to compensate for a smaller market. The science on booster
shots is still unsettled""it's not yet clear how often, or even whether, they'll be needed in large numbers.
Moderna has three types of boosters in Phase II trials, including a lower-dose version of its existing vaccine, one booster that's
been customized against the beta variant that was first spotted in South Africa, and a third that combines both. More variants can
be added if necessary. The process for the beta booster went even faster than for the original shot. Design work started on Jan.
22, with Moderna ultimately switching out some of the chemical "letters"� in its original mRNA vaccine, so they correspond to the
spike protein in the beta variant. Manufacturing began three days later, and the first trial dose was administered on March 10""only
47 days in all, compared with the 65 for the main vaccine.
Moderna is already cutting deals that encompass potential booster doses, including a June order from the U.S. for 200 million
additional shots in late 2021 and early 2022. Despite the uncertain need for boosters, Bancel's pitch is that it's best to be prepared
for an evolving virus. At an investor conference in early June, he told everyone that "the smart countries are saying, "�I'd rather
be two months too early than two months late.'"�"�
Beyond Covid, most of Moderna's experimental vaccines remain in early stages of human trials. An exception is the shot for cytomegalovirus.
No vaccine exists for this virus now, and the shot could turn into a multibillion-dollar product if it works. Moderna also plans
human trials this year of a vaccine against another complicated pathogen, Epstein-Barr virus, which causes mononucleosis.
Influenza is an obvious target, and a shot for that could be combined with Covid boosters, locking them into an existing annual
market. With the Pfizer-BioNTech alliance also slated to start trials on a flu shot later this year, researchers say they're hoping
the mRNA vaccines can improve on existing versions, which must sometimes begin production six months in advance based on experts'
assessment of which strains are likely to circulate. The shorter lead times required to make mRNA shots could, in theory, let health
officials more closely match flu strains and improve upon typical 40% to 60% efficacy rates. "The mRNA vaccines have a very high
likelihood of being better than the egg-based vaccines we use now,"� says Andrew Pekosz, a virologist at Johns Hopkins Bloomberg
School of Public Health. He adds that the shorter lead times could "shave off months"� from the process. But he notes that it's an
open question whether there would be a good economic case for mRNA-based flu vaccines if they turn out to be more expensive and only
modestly better than the old ones.
Moderna is also targeting a few nasty respiratory viruses that don't have vaccines. These include metapneumovirus, which can lead
to hospitalization in infants, and respiratory syncytial virus, which causes more than 175,000 U.S. hospitalizations annually in
the elderly and about 50,000 more in young children. In the latter case, Moderna's vaccine will be competing with efforts at GlaxoSmithKline
and Johnson & Johnson that draw on other technologies and are further ahead.
Hoge says Moderna could combine as many as a dozen or more viral strains in one shot. The goal is a seasonal vaccine that "eliminates
the majority of the respiratory viral diseases that we all suffer from,"� he says. "The only way that we're really going to get good,
broad population immunity against these respiratory viruses is if we can make it feel like your flu shot."�
The concept makes sense on paper, according to Tony Moody, a physician-researcher at the Duke Human Vaccine Institute, which is
working on mRNA-based flu vaccines. Combinations are "one of the strengths of the technology,"� he says. He estimates that it would
cost only a few dollars more per shot to add the necessary mRNA for a given viral target. "If you could get a combo shot that gives
you a degree of protection against a lot of respiratory viruses, I think there would be a market for that,"� he says. It won't be
fast or easy. Researchers will first have to show that the individual vaccines work and then perform studies showing that complex
combinations don't compromise efficacy or result in troublesome side effects.
To realize its vision, Moderna will have to move quickly. Competitors are investing heavily to catch up.
Sanofi said in late June it would spend €400 million ($475 million) annually on mRNA research, focusing on stable vaccines
with few side effects. With emergency authorizations unlikely in the future, considerations such as side effects and convenience
will assume new prominence. Moderna is working on eliminating the complicated refrigeration requirements of its Covid shot. Future
products will also have to find ways to reduce the high rates of fatigue, headache, and muscle pain produced by the shot. For the
boosters, the company is testing lower doses, which may help.
How broadly mRNA can expand beyond vaccines into the far larger and more lucrative therapeutics market remains to be seen. There
will be additional technical hurdles to surmount. To treat chronic diseases, for example, companies will have to prove that they
can deliver the therapies to the target organs and that mRNA can be administered safely. And to develop cancer vaccines, mRNA researchers
will have to solve the thorny problem of teaching the immune system to distinguish between specific tumors and healthy cells. Many
previous approaches have failed.
The good news is that mRNA's adaptability also makes it easier to try out many possibilities. Within a few years, Moderna could
have 60 drugs and vaccines either in human trials or nearing them, according to Bancel. If it works out the way he hopes, mRNA will
make inventing vaccines and drugs a bit more like creating software. "We use the same four-letter code"� for every vaccine and drug,
Bancel says. "We can scale the number of products we have in development at a pace that has never been done before."�
Read next:
The World's Best Hope to End the Pandemic Still Needs More Doses
Is not this a fiasco?
Pfizer Outlines Booster Plans While Regulators Signal Caution By
Robert Langreth and
Josh Wingrove July 8, 2021, 5:00 PM EDT
Updated on July 8, 2021, 9:56 PM EDT
Early human data shows third shot raises antibody levels
Federal health agencies say no need for boosters at this time
Pfizer Inc. plans to request U.S. emergency authorization
in August for a third booster dose of its Covid-19 vaccine, based on early data showing that it can sharply increase immune protection
against the coronavirus.
At the same time, however, federal health officials signaled that they would take a cautious approach to potential booster shots,
and underlined that the currently available vaccines are effective at keeping people from being sickened by the coronavirus.
Pfizer has received initial data from an early human study showing that a third dose of its existing coronavirus vaccine is safe
and can raise neutralizing antibody levels by 5 to 10 fold compared with the original vaccine, the company's research head, Mikael
Dolsten, said in an interview.
Once more data is in hand, Pfizer plans to ask the FDA to authorize a booster shot that could be given six to eight months after
the original two doses, Dolsten said. The drugmaker is also talking with regulators in other countries and the European Union about
the new results, he said. Pfizer produces the vaccine in partnership with
BioNTech SE .
Drugmakers' Spending on Stock, Dividends and Executive Pay Exceeds Research, Democrats Say Posted on
July 11, 2021 by Jerri-Lynn Scofield
By Michael McAuliff.
Originally published at Kaiser Health News .
The largest drug companies are far more interested in enriching themselves and investors than in developing new drugs, according
to a House committee report released Thursday that argues the industry can afford to charge Medicare less for prescriptions.
The
report by the House Oversight and Reform Committee says that contrary to pharmaceutical industry arguments that large profits
fund extensive research and innovation, the major drug companies plow more of their billions in earnings back into their own stocks,
dividends and executive compensation.
And they can do it largely because Congress has imposed few restrictions on their pricing in the United States" including in the
Medicare program, which is not permitted to negotiate drug prices, House Democrats say.
"What we have found is shocking," said Oversight Committee Chair Carolyn Maloney (D-N.Y.). "Drug companies are actively and intentionally
targeting the United States for price increases, often while cutting prices in the rest of the world."
According to the data crunched by the committee, the 14 largest drug manufacturers paid themselves and investors $578 billion
from 2016 to 2020 through dividends and stock buybacks, while investing $56 billion less" $522 billion" on research and development.
On top of that, the report says, some of that R&D money is spent researching ways to suppress competition, such as by filing hundreds
of new, minor patents on older drugs that make it harder to produce generics.
"Despite Big Pharma's lip service about innovation, many drug companies are not actually spending significant portions of their
research-and-development budget to discover innovative new treatments," Maloney told reporters in a conference call. "Instead, these
companies are spending their research-and-development dollars on finding ways to game the system."
"How can Pharma say with a straight face "¦ that lower drug prices for Americans will have to come at the expense of research
and development?" House Speaker Nancy Pelosi asked on the call.
The release of the report during a congressional recess seemed aimed at least partly at boosting support for the House Democrats'
Lower Drug
Costs Now Act , which, among other things, would allow Medicare to negotiate drug prices, let Americans with private insurance
pay those same rates and limit U.S. prices to an average price other countries pay.
Pelosi said she would like to see the measure, numbered H.R. 3, included in a massive bill that Democrats are preparing under
what is known as the budget reconciliation process. That process allows taxing and spending bills to be packaged together and get
though the Senate on a simple majority vote exempt from a filibuster. Democrats are expected to use the process for a number of key
initiatives, including possible changes in Medicare eligibility and benefits, outlined by President Joe Biden and congressional leaders
and panned by Republicans.
"With the savings on the lower drug prices, we can invest in transformational improvements in American health care," Pelosi said.
"We have an historic opportunity to do so as we craft the reconciliation bill. We'll see how we proceed there."
Some more moderate Democrats have raised concerns about H.R. 3, in part echoing industry assertions that curbing drugmakers' revenues
might cut their ability to innovate. Pelosi can afford to have only a handful of Democrats defect in the House, and all 50 Democrats
in the Senate are needed to pass a reconciliation measure.
Among the starker examples the report highlights, the company Novo Nordisk spent twice as much on executive pay and buying back
its own stock as on R&D over the five years.
The drugmaker Amgen especially cashed in on the 2017 tax cuts pushed through a Republican Congress, spending five times as much
on buybacks as on research, the report says.
According to the report, if the 14 large companies maintain roughly their current practices, they will pay themselves and investors
$1.15 trillion over the next decade, which the committee notes is double the estimated cost of H.R. 3.
The report also singles out internal documents from the pharmaceutical giant AbbVie as an illustration of "research and development"
being aimed at suppressing cheaper competition, in this case by seeking new minor patent enhancements on the rheumatoid arthritis
drug Humira, which costs $77,000 a year.
"An internal presentation emphasized that one objective of the "˜enhancement' strategy was to "˜raise barriers to competitor ability
to replicate,'" the report says, likely delaying lower-priced biosimilar drugs at least until 2023. It also notes that the company
identified about $5.19 billion in R&D for Humira, about 7.4% of the drug's net U.S. revenue.
In another case, the report highlights an internal presentation from Celgene, which makes the $16,744-a-month cancer drug Revlimid
and has since been bought by Bristol Myers Squibb.
The report says Celgene targeted the United States for its profitable price hikes and admitted in a presentation that it was because
of the country's "highly favorable environment with free-market pricing."
In some other cases, the combined $3.2 billion that the 14 companies' top management earned over the five years was conditioned
on U.S. price hikes.
A spokesperson for Novo Nordisk said its buybacks were entirely justified and included them in what he described as the company's
overall long-term investments.
"These investments have led to the discovery of innovative treatments that have made substantial impacts on peoples' lives," said
Michael Bachner, director of communications for Novo Nordisk.
"Given the complex challenges in the health care system, we remain committed to developing solutions in cooperation with policymakers
and other stakeholders," he said. "We will continue to work towards maintaining a sustainable business that will foster innovation
and provide patients with access to needed new therapies."
Frank Benenati, a spokesperson for AbbVie, took issue with the report's emphasis on Humira's R&D costs. He said the report "is
misleading in that it focuses on the R&D spend for one drug, not the total R&D spend, which was approximately $50 billion since 2013."
Other companies did not immediately answer requests for comment, but a spokesperson for the industry's lobbying arm, the Pharmaceutical
Research and Manufacturers of America, said the release of the report was political and aimed at backing legislation that PhRMA said
would harm Medicare.
"While we can't speak to specific examples cited in the report, this partisan exercise is clearly designed to garner support for
an extreme bill that will erode Medicare protections and access to treatments for seniors," said PhRMA spokesperson Brian Newell.
"Every year, biopharmaceutical research companies invest tens of billions of dollars in the research and development of new cures
and treatments, as well as our significant investments in time and resources creating treatments and vaccines to combat the global
pandemic."
Despite the report, he said, net prices on drugs are coming down, when rebates to customers are included. He added that the greater
problems are with high deductibles charged by insurers and with profits taken by middlemen such as pharmacy benefit managers.
"We are committed to working with policymakers on commonsense, bipartisan solutions that address the real challenges patients
face," Newell said. "Working together we can make sure medicines are affordable and accessible for everyone."
timbers
July 11, 2021 at 7:25 am
It's good Nancy Pelosi said those really mean things about drug companies on the call and Democratic Congresswoman Carolyn
Maloney told us she was shocked SHOCKED the committee found that gambling was going on in the casino and that Dems are pushing
this NOW when they now know for sure they can't pass it because President Machin will veto it.
And kudos to article being fair and balanced by quoting the Pharmaceutical Research and Manufacturers of America without breaking
out into hysterical laughter:
"Despite the report, he said, net prices on drugs are coming down, when rebates to customers are included. He added that the
greater problems are with high deductibles charged by insurers and with profits taken by middlemen such as pharmacy benefit managers.
"
It's all those millionaire pharmacy managers and assorted working class folk that is driving up the cost of drugs.
Nikkikat
July 12, 2021 at 2:54 pm
I also chuckled at Maloney being SHOCKED, shocked I tell you!
jo6pac
July 11, 2021 at 8:11 am
Of course they do they're not the late Dr. Silk.
Arizona Slim
July 11, 2021 at 8:21 am
Dr. Salk was truly one-of-a-kind.
When I was a younger Slim and in the employ of the University of Pittsburgh, I noticed the revered status of Salk Hall. It
was considered to be a very special part of the Pitt campus.
On another note, this part of the post really bopped me over the head:
"[W]ould allow Medicare to negotiate drug prices."
Sounds good, but just how hard of a bargain is Medicare going to drive? IMHO, the harder the better, but won't those Medicare
negotiators eventually want to take jobs in the pharmaceutical industrial complex?
jo6pac
July 11, 2021 at 9:15 am
Thanks for the correct spelling and story
Arizona Slim
July 11, 2021 at 10:03 am
You're welcome!
On a somewhat related note, I also worked on the University of Arizona campus. While there, I knew the man who shot that famous
photo of the little girl taking the oral vaccine with numerous adults looking on. Photographer was George Kew, and darn if I can
find that photo online.
The Rev Kev
July 11, 2021 at 10:11 am
Not this one by any chance, Slim? You have to click the one under "˜Images'-
https://www.britannica.com/biography/Jonas-Salk/images-videos
Arizona Slim
July 11, 2021 at 1:28 pm
No. This was the oral vaccine that was developed by Dr. Sabin. ISTR George telling me that his photo was featured in Life magazine.
Mikel
July 11, 2021 at 8:17 am
"How can Pharma say with a straight face "¦ that lower drug prices for Americans will have to come at the expense of research
and development?" House Speaker Nancy Pelosi asked on the call.
Because they will cut R&D further to maintain their big pay days and perceived status. Not too subtle. That is what they are
saying.
allan
July 11, 2021 at 10:27 am
Throw in the billions that Big Pharma spends on marketing prescription drugs directly to consumers,worse health outcomes, and
you have a real problem:
"¦ For health care that is mediated by a clinician's order or prescription,
Evidence that physicians have been either misled or otherwise persuaded to act based on fraudulent pharmaceutical marketing
in recent decades, however, suggests that professionals may need further education or support to serve as the arbiter of deceptive
marketing.3 Moreover, the expectation that clinicians will prioritize the patient's well-being in making care recommendations
breaks down when the clinician is linked with the manufacturer, as is the case with some advertised products that help patients
to find a physician who can prescribe without ever meeting the patient face to face. Scrutiny of such arrangements to ensure
they do not undermine the intent of existing licensure and regulatory regimes that govern prescribing seems warranted.
"¦ Patients' trust in physicians puts them in a position to help mitigate the harms of DTC advertising. However, trust in
physicians and health care institutions may be at stake if medical marketing by practitioners, health care organizations, and
manufacturers of health care products continues to increase unchecked.
Christopher Horne
July 12, 2021 at 2:40 am
Also, the many perks their salespeople use to get doctors to perscribe
John Zelnicker
July 11, 2021 at 11:12 am
So, PhRMA says negotiating prices with Medicare will harm the program and "erode Medicare protections and access to treatments
for seniors".
Yeah, right! They're going to stop selling drugs that are still insanely profitable if they can't charge even more insanely
profitable prices. /s
Christopher Horne
July 12, 2021 at 2:43 am
"¦.And I gots some fine swampland in Florida for sale for you.
bill dietrich
July 11, 2021 at 11:15 am
Stock-buy-back operations, were illegal until 1982, when Securities and Exchange Commission (SEC) Chairman John Shad, a former
Wall Street CEO, redefined unlawful "stock manipulation" to exclude stock buybacks. Another joke on us by R Reagan.
https://banyanhill.com/buybacks-destroy-corporations/
drumlin woodchuckles
July 11, 2021 at 6:48 pm
If an SEC Chairman can redefine stock buybacks as not unlawful stock manipulation, then another SEC Chairman can un-redefine
stock buybacks back to being unlawful stock manipulation.
Perhaps Congress could make accepting an SEC Chair nominee contingent upon that nominee's willingness to un-redefine stock
buybacks back to being illegal. Perhaps it the confirmed nominee breaks such a promise, Congress can authorize zero funding for
SEC until SEC Chair issues such a ruling.
Hayek's Heelbiter
July 11, 2021 at 11:32 am
And you mustn't forget that a huge amount of the basic research funded by the taxpayers is cherrypicked and then financialized
by Big Pharma.
https://www.pnas.org/content/115/10/2329
This report shows that NIH funding contributed to published research associated with every one of the 210 new drugs approved
by the Food and Drug Administration from 2010""2016. Collectively, this research involved >200,000 years of grant funding totaling
more than $100 billion. The analysis shows that >90% of this funding represents basic research related to the biological targets
for drug action rather than the drugs themselves.
Susan the other
July 11, 2021 at 12:20 pm
Whereas it's a perverse incentive to tax big oil's corporate profits (because they will just invest in capital improvements
for a business that is already operating beyond full capacity "" a business that needs to be restricted to contain CO2 emissions
as well as conserve oil "" it is a very good idea to tax the crap out of pharma's corporate profits because they haven't been
"capitalists" for as long as I can remember. They need to start being actual modern pharmaceutical companies. They should also
be deprived of any government help-at-all-whatsoever until they stop profiteering, and if they do not comply then it's time to
nationalize them too. Good riddance.
Adam Eran
July 11, 2021 at 12:27 pm
This imbalance between C-suite pay and R&D may be new, but Marcia Angell wrote years ago that big pHRMA paid 55% of its gross
for marketing, but only 15% for R&D (in NYRB). Most of that R&D is targeted at extending the patent life of already patented drugs
(think: "Time release viagra").
Mariana Mazzucato's TED talk about government-as-innovator notes that 75% of pharmaceutical innovation comes from government-funded
research.
bill dietrich
July 11, 2021 at 1:51 pm
Stock-buy-back operations, were illegal until 1982, when Securities and Exchange Commission (SEC) Chairman John Shad, a former
Wall Street CEO, redefined unlawful "stock manipulation" to exclude stock buybacks. Another joke on us by R Reagan.
https://banyanhill.com/buybacks-destroy-corporations/
lincoln
July 11, 2021 at 1:53 pm
The Lower Drug Costs Now Act sounds like a very good idea. U.S. consumers have been overcharged for essential medicines for
far too long. And drug manufacturers unfortunately play a big part in this. But drug prices are also high because of an extensive
chain of rebates (aka kickbacks) between drug manufacturers
and insurers. I hope this legislation will address the price manipulating actions of health insurers and Pharmacy Benefit Managers
as well.
John Buell
July 11, 2021 at 2:40 pm
I would like any data on spending for marketing. Just from viewing commercial TV I surmise the ad budget is quite large and
perhaps even greater than when Dr. Angell wrote
KEY FACTS
"Given how transmissible this variant is," Gottlieb told CBS News' This Week it's likely about 85% of the U.S. population
will end up with some level of Covid-19 immunity.
With about 55% of the population at least partly immune due to vaccination and one-third of Americans having been naturally infected,
Gottlieb noted that millions of Americans remain vulnerable and now have a "choice in terms of how [they] acquire immunity."
PROMOTED
me title=
Even those immune through natural infection are at heightened risk, Gottlieb said, pointing to data showing immunity among individuals
naturally infected with Covid-19""and particularly those who are older""declines after about eight months.
The physician predicted Covid will effectively act as a "second circulating flu this winter," though he said its prominence "could
be a little worse." CRUCIAL QUOTE
"I wouldn't be declaring mission accomplished. I think this is going to be a long fight," Gottlieb said Sunday. "You're seeing
a decoupling between cases, hospitalizations and deaths because there's so much immunity in the population""not just through vaccination""but
also through prior infection... But this is likely to become an endemic virus. We're going to have to deal with it."
64% make the idea of herd immunity a joke. Fauci who promoted this idea should go...
In a brief statement issued on Monday, the government said that as of June 6, the vaccine provided 64% protection against infection.
In May -- when the Alpha variant dominated in Israel and the Delta strain had not yet spread widely -- it found that the shot was
95.3% effective against all infections. The government added that the vaccine was now 93% effective in preventing severe disease
and hospitalizations, compared to 97% reported in the medical journal The Lancet in May. The statement cited top line figures, but
did not release underlying data or other details about its analysis. A team at Hebrew University said in a separate statement that
it was too soon to tell how much the
Delta variant was affecting vaccine efficacy.
In another statement Tuesday, Israel's Ministry of Health released some data about illness caused by Covid-19 and offered an expanded
explanation of the vaccine's protectiveness. Despite an apparent decline in the vaccine's ability to prevent all infections during
the spread of the Delta variant, the statement emphasized its continuing benefit in preventing severe cases.
Israel has deployed the Pfizer vaccine to everyone over the age of 12, and its early and quick rollout gave scientists one of
the first real-world snapshots of its efficacy.
The government said the drop in efficacy is likely due to the spread of the Delta variant in Israel. This more infectious strain
of the virus was first identified in India earlier this year and is also known as B.1.617.2.
Dr. Anthony Fauci, the director of the US National Institute of Allergy and Infectious Diseases, told CNN more granular data was
needed to determine the exact reason for the drop in efficacy in Israel. While "the Israelis know what they're doing," the data is
sparse, Fauci said, adding that the circumstances of the reported drop in efficacy are unclear.
Still, Dr. Richard Besser, former director of the US Centers for Disease Control and Prevention, told CNN the data from Israel
is worth paying attention to, because Israel started vaccinating before the US and so "if there's going to be a problem, we'll likely
see it there before we see it here in the United States." "I take this as actually encouraging information, that these vaccines are
still highly effective in terms of preventing hospitalizations, severe illness and death," Besser said.
Fact Check-Claim that vaccinated people are six times more likely to die from the Delta variant than those who are unvaccinated
is misleading
By Reuters Fact Check
6 MIN READ
Social media posts have claimed that those who have received a COVID-19 vaccine are more six times more likely to die from being
infected by variants than those who have not been inoculated. While the data was indeed taken from a Public Health England (PHE)
briefing held in June, it was taken out of context.
Several blogs have spread the claim and screenshots of the blogs are being shared on social media.
The headline of a blog post, published on June 23 by DC Clothesline, reads: "Vaccinated people found to be 600% more likely to
die from covid "variants" than unvaccinated people" ( archive.fo/nF2fM ).
"Death rate from variant COVID virus six times higher for vaccinated than unvaccinated, UK health data show," reads a headline
from a similar blog published in Life Site News on June 18 ( archive.fo/yQAi3
).
Examples of the blogs being shared on social media can be found (
here ), (
here ) and (
here ).
Referring to data compiled by Public Health England (PHE) in a technical briefing released on June 18 regarding the SARS-CoV-2
variants (
here ), the authors of the blogs make several calculations.
On page 12 of the briefing, it shows that 26 people have died since February 1 after testing positive for the Delta variant of
the virus, having also been fully vaccinated for more than two weeks. In total, 4,087 tested positive more than two weeks after their
second dose. Meanwhile, 35,521 people who were unvaccinated tested positive for the Delta variant and 34 people died.
The authors then divide the number of deaths by the total number of people who tested positive for the Delta variant and found
the rate of death to be 0.000957 for unvaccinated individuals and 0.00636 for those who have been inoculated.
In late April Axios
reported
that the United States is expected to run out of adults who want to get vaccinated within the next two to four weeks, citing a recent
Kaiser Family Foundation analysis. According to the authors of the
paper , "It appears we are quite close to the tipping point where demand for rather than supply of vaccines is our primary challenge."¦"
When in July 2021 the belief of vaccine protection at least partially went out of windows after Delta variant baceme the dominant
and Pfizer started talking about booster shots the situation turned to worse.
In early 2020, the scientific community went into hyperdrive to develop not one but several vaccines against COVID-19. In the
US, the government and the medical community worked overtime to set up the infrastructure to get doses into arms around the country.
Clinics and volunteers have jumped into action at a community level to make sure, as of this week, that 58% of adults have gotten
at least one shot and over 70% of those older
than 65 are fully vaccinated.
But all this effort is now hitting up against resistance. Or hesitancy. Or barriers to access. States are cutting back on their
vaccine orders from the federal authorities. Daily vaccination rates have dropped
nearly 20% from last week.
Employers are basically bribing people to get their shots. Millions of
people aren't even bothering to show up for their
second doses.
Yesterday,
the FDA confirmed that the Johnson & Johnson jab may be linked to rare side effects
consistent with a neurological condition known as Guillain-Barré. The news was only the
latest revelation of a rare but potentially life-threatening side effect caused by the
vaccines. Both AstraZeneca and J&J have been linked to cerebral blood clots, while the
Pfizer and Moderna jabs (which use a new technology known as mRNA) have been linked to heart
inflammation in a small number of patients.
Unsurprisingly, the media hasn't devoted much attention to covering these defects.
Authorities like the CDC insist that the benefits of the jabs far outweigh the risks, while Dr.
Fauci took to CNBC Tuesday morning to offer reassurances about J&J's new warning label
while suggesting that private companies do more to coerce Americans to get vaccinated.
me title=
Unmute Fullscreen Pause Up Next
https://imasdk.googleapis.com/js/core/bridge3.471.1_en.html#goog_1291402947 All You Need To
Know About COVID-19 Booster Shots NOW PLAYING One More Thought: Lying Flat The EU Doesn't Treat
All COVID-19 Vaccines Equally When It Comes to Travelers Study: 3rd AstraZeneca shot gives
strong immunity COVID-19 Vaccines Do Not Affect Sperm Count Fans With AstraZeneca Vaccine Can't
Attend Springsteen On Broadway S&P 500, Nasdaq notch record closing highs AstraZeneca's
Executive VP Sees Upside, As China's Government Speeds Up New Drug Approval
Fortunately for the small number of patients who are potentially at risk of developing a
vaccine-induced side effect, the makers of the AstraZeneca and J&J jabs (which both use
adenovirus technology) are working on modifications that could lower - or eliminate - certain
dangerous side effects, according to
WSJ.
Thanks to help from scientists around the world, early stage research has helped to identify
what's causing the blood clots. Fast-developing clues into how the clots form (driven in part
by independent scientists in Europe, the US and Canada) are boosting hopes of identifying the
cause and possibly re-engineering AstraZeneca's shot by next year, according to some of these
people.
Still, it's too early to know whether either shot can be modified, or whether doing so would
make commercial sense, according to WSJ's anonymous sources.
For both AstraZeneca and J&J, eliminating the rare blood-clotting issues and the other
neurological symptoms described above would be major victories for two companies that have lost
their leading positions in the vaccine race. The changes could even help turn the shots into
"moneymakers."
But first scientists say they need to understand whether the problem is one of the
ingredients in the shots, the purification process or something that's embedded in how the
vaccine's work (which would be a bigger problem). Sarah Gilbert, an Oxford vaccinologist and
co-inventor of the vaccine, says her team is focused on figuring out what exactly triggers the
immune response underpinning the clots.
In other news,
Reuters reports that European regulators haven't received key data and other materials from
the creators of Sputnik V, the Russian-developed vaccine that's already being used by a small
number of EU nations, but is seeking approval for use across the EU.
Sources told Reuters that the failures are likely due to the Gamaleya Institute's lack of
experience in dealing with overseas regulators. "They are not used to working with a regulatory
agency like the EMA," the person close to the agency said, referring to Gamaleya and its
scientists.
A J&J spokesman said the company supports "continued research and analysis as we work
with medical experts and global health authorities." AstraZeneca has said it is "actively
working with the regulators and scientific community to understand these extremely rare
blood-clotting events, including information to drive early diagnosis and intervention, and
appropriate treatment."
Unknown 6 hours ago (Edited) remove link
...while the Pfizer and Moderna jabs (which use a new technology known as mRNA) have
been linked to heart inflammation in a small number of patients.
It can't be a small number when there are so many people with major heart complications.
I know one that probably will be disabled for life.
Besides what is a small number or rare? Why they don't report the actual numbers?
Greed is King 5 hours ago (Edited)
Repost: Part of an article I posted in another comment on ZH, together with the link for
the full article.
------------------------------------------------------------------------------------------------
Vaccine adverse reactions to date of this article (late May 2021)
To date, some 822,845 vaccine adverse reactions have been recorded in the United Kingdom
by the Medicines and Healthcare products Regulatory Agency (MHRA), together with 1,180
deaths.
Unlike the deliberately confusing datasets presented by the MHRA, the UK Column dataset
is presented in a clear and easily searchable database. It should be noted that where
minor
https://www.ukcolumn.org/article/greater-manchester-vaccination-centre-and-mhras-yellow-card-adr-scam-part-1
----------------------------------------------------------------------------------------
Interestingly.
According to the BBC`s news tonight, 45,978,017 people in the UK have had their first
jab, combine this figure with the reported 822,845 adverse side effects (above). A little
maths gives us a percentage of 1.78964 people who have reported side effects. That`s
practically 2 in every 100, or 2%.
The reported deaths of 1,180 gives a vaccine fatality percentage of 0.00256.
Yes the deaths from vaccines are rare, but so is the death from the virus, in fact
there`s very little in it fatality wise.
So overall, I don`t think the jab is worth the risk, because, if you have the virus and
recover as the vast majority do, that`s it, you`ve got antibodies, you`re IMMUNE.
If you have the jab, the adverse side effects keep on giving for who knows how long, and
you`re not immune anyway, and you`re going to need booster jabs every 6-12 months.
in_xanadu_did_kubla_khan 5 hours ago
Try telling that to the "scientists" and health care overlords.
Abbie Normal 4 hours ago
This sounds suspiciously like those iphone 6 bending issues. Apple stated that out of
millions of phones, they only received reports of a couple dozen that bent. But when the 6S
came out the next year, Apple proudly announced that they had resolved the bending issue.
Pretty civil of them to fix it for just a couple dozen users out of millions sold.
So we should just wait for the pharms to get it right in V2 of the next jab?
HonestLee 7 hours ago
Overhead in lab -
Rat 1: "Hey, have you gotten your Covid jab yet?"
Rat 2: "Nah, I'm waitin til the human trials are over"
Stranger_in_a_Strange_Land 7 hours ago
I don't understand? Why would they need to work on modifications to reduce deadly
side-effects? That makes no sense, because they told me it was completely safe and
effective. Were they lying then, or lying now?
TacoNasty 7 hours ago
Right? What exactly are they "modifying" to prevent this auto-immune disorder and if
they actually know how to do that safely, why didn't they do it before the vaccine in the
first place?
The lies around this vaccination campaign have gotten so thick and distorted that it
doesn't even sound like they're speaking English, anymore.
And, if these vaccines even work, why do I still have to wear a mask especially when
Morbidly Obese Middle Aged Democrat politican women don't have to?
wizeye 5 hours ago
This is why it take 8-12 years to get a vaccine to the market, even most of them aren't
really safe at all.
But this shot isn't even a vaccine. It is illegally called a vaccine to win public
acceptance, and illegally put on the market, because there ARE safe effective treatments
for covid. The EUA is illegal.
Some New Jersey residents have become infected with COVID-19 even after receiving a first
dose of the two-shot Moderna or Pfizer COVID vaccine, and a tiny number have developed
"breakthrough infections" more than two weeks after their second dose of the vaccine.
The total number of such cases in New Jersey is not known
So it looks like NJ repeats the pattern observed in Israel -- the rise of cases with Delta
variant despite high level of vaccination. . Looks like they try to hide statistics of infections
among vaccinated... With 70% of adult population vaccinated ( NJ COVID Update- 70%
of adult population in state fully vaccinated - ABC7 New York ) NJ is one of the most highly
vaccinated state and Pfizer vaccine is predominant in this state like in Israel.
Japan warns of 'sense of crisis' about China's threat to conquer Taiwan Sen. Cotton
expresses 'real doubts' about US Navy's ability to defeat China in
The Delta variant of COVID-19 is now the predominant strain in New Jersey, according to
Governor Phil Murphy and health officials.
Pause Current Time 2:03 / Duration 2:12 Unmute 0 LQ CaptionsFullscreen Delta variant now
dominant COVID strain in NJ Click to expand The highly contagious strain that originated in
India and is surging around the globe now accounts for 41% of new variant cases in the Garden
State last month, overtaking the Alpha variant that was first documented in the United
Kingdom.
For the week ending June 26, Delta accounted for 70% of identified variant cases.
... ... ...
More than 5.1 million people have been fully vaccinated in New Jersey, Murphy said, which is
about 66% of the eligible population, according to the Centers for Disease Control and
Prevention, compared with about 56% for the country overall.
The seven-day rolling average of daily new cases in New Jersey rose the past two weeks from
235 new cases per day on June 26 to 264 on Sunday.
The seven-day rolling average of daily deaths fell, going from nine deaths a day on June 26
to almost five a day on Sunday, according to data from Johns Hopkins University.
Meanwhile, New Jersey's rate of transmission ticked up above 1 -- to 1.01, for the first
time since late January.
Let me follow up briefly on my post from yesterday on
vaccine hesitancy.
Demeaning people is the first step towards ignoring their interests or even persecuting
them. Jason Brennan urges us to ignore the welfare of the unvaxxed by painting a picture of
them as moral terrorists or extortionists. He holds them responsible for their confusion and
fears. He pretends that everyone is well-informed and knows how to evaluate scientific
evidence, and that everyone has loads of time to keep up on the latest covid news. Then he
blames people who fail to get vaccinated for their poor choices.
These are the key facts, as I see the matter:
Many people are not vaccinated, vaccination rates are slowing, rates of hesitancy are
high.
Most unvaccinated people are not hard-core anti-vaxxers. Many are busy or have difficulty
figuring out how or where to get vaccinated. Some are scared of needles. Some just worry
about the safety of the vaccines. Young people are likely to prove difficult to vaccinate,
because they are at very low risk of dying from covid.
Unvaccinated people are a threat to themselves, to people who for medical reasons cannot
be vaccinated (a small group, apparently), and to people who are vaccinated but have
compromised immune systems. They are also (presumably) a very, very small risk to people who
are relatively healthy and vaccinated.
I got covid in December during a visit to the hospital. While I was in the hospital –
with an active diagnosis of covid, being cared for by doctors and nurses whose job it was to
care for people with active covid – I had several nurses who said they would not get
vaccinated, at least not right away. My sense is they were worried about possible side-effects.
They were not malevolent, they were (relatively) well-informed about the risks of covid and of
the vaccines, and they were not as far as I could tell making a political statement. Their
worries were understandable, but their planned choices were (arguably) terribly misguided given
their high exposure at work.
We owe it to the unvaxxed to at least try to persuade them to get vaccinated. This means
spending money: on education, outreach, transportation. It means doing research to figure out
what works. Maybe we should go further and pressure people to get vaxxed or use positive
incentives (money, beer, pot) to get everyone to vax up. The case for using pressure and/or
incentives is strengthened by third party benefits.
The Biden administration needs to orchestrate a vaccination campaign taking into account our
polarized political situation. That's hard. Polarization means that the government cannot
simply require people to get vaxxed; even pressuring them will be controversial. It means that
people need to hear pro-vax messages from people they trust – their doctors, religious
leaders, family members, etc., not from politicians. This makes communication much more
difficult. President Biden can get lots of free press to spread the word on vaccines, but if
vaccination becomes closely associated with him some Republicans may decline to get their
shots.
Brennan's characterization of the situation is uncharitable, inaccurate, and politically
destructive. May 13, 2021 6:51 am
I can see both sides, but neither in a very good light. It is easy for one to make good
decisions when one has all the relevant information, but it is not a realistic expectation for
most of life's important decisions. Everyone is afraid of something and most people are ruled
by their worst fears. Good judgement seems to be a lost art.
The Claim
Far-right U.S. news outlet The Epoch Times reported on March 6 that 966 people had
died after having the Pfizer or Moderna COVID vaccines.
The report said it had drawn the data from VAERS reports between December 14, 2020 and
February 19, 2021.According to the report, 472 people died after receiving a Moderna vaccine,
while 489 died after receiving a Pfizer vaccine. Additionally, five people died after receiving
a jab from an unknown manufacturer.
The report also included data on age group and gender. It showed the largest proportion of
deaths -- 29 percent -- occurred in people ages 80 to 89. It also showed males accounted for 55
percent of deaths to 43 percent of females. It said the deaths had occurred between 0 and 49
days after vaccination, with 94 unknown.
The article has been shared on Twitter , and users have gained hundreds of
retweets and likes from posting a screenshot of the VAERS data reported by The Epoch
Times .
The Facts
There are hundreds of reports of people having died after getting a COVID vaccine, but that
does
not necessarily mean the vaccine was the cause.
Using WONDER, the CDC's VAERS database search tool, Newsweek gathered adverse report
data specifically on deaths following a COVID vaccine from Moderna or Pfizer. It is important
to note that our data contained VAERS reports processed as of February 26.
Newsweek selected only deaths as an adverse event, and selected the COVID vaccine as
the only vaccine in the dataset. We specified Pfizer and Moderna as the vaccine manufacturers.
We also chose our symptom onset interval as "All days," which ranges from 0 to over 120 days.
We did not specify gender or age in the overall results. Our time frame ran from the earliest
possible dates, "before 1990," to ensure every COVID vaccine was included.
Our VAERS result showed 970 people died after being given a Pfizer or Moderna vaccine shot.
Of those deaths, 495 occurred following a Moderna shot, and 475 occurred following a Pfizer
shot. Newsweek contacted Pfizer and Moderna for comment.
Just a few days ago, researchers
warned people that one specific mild COVID-19 vaccine side effect could appear several
days after the first or second dose, rather than immediately: skin issues, including redness
and rashes. These adverse reactions were observed after the Moderna jabs -- especially after
the first dose. They're not a cause of concern, and they tend to disappear on their own within
a few days.
The CDC made a few changes to its coronavirus vaccine guidelines on Friday, adding three new
side effects to the list. Initially,
the agency described six potential adverse reactions. Two are local (pain and swelling),
and four are systemic (fever, chills, tiredness, and headache), as seen below.
The new guidelines
include nine possible coronavirus vaccine side effects. In addition to pain and swelling on the
arm where the shot is administered, people might also experience redness. As for the systemic
reactions, the CDC added muscle pain and nausea to the list. Muscle pain should not be confused
with pain at the site of injection.
These reactions are an indication that the immune system is responding to the perceived
threat -- the vaccine -- and developing immunity. Coronavirus antibodies should begin to appear
about two weeks after the first jab, and maximum protection is obtained about two weeks after
the second injection.
The guidelines also provide helpful tips for dealing with the side effects. "Talk to your
doctor about taking over-the-counter medicine, such as ibuprofen, acetaminophen, aspirin, or
antihistamines, for any pain and discomfort you may experience after getting vaccinated," the
guidelines read. "You can take these medications to relieve post-vaccination side effects if
you have no other medical reasons that prevent you from taking these medications normally."
The CDC also reminds people that it's not recommended to take these medications before
vaccination in an effort to prevent the side effects.
After vaccination, people can use cool, wet cloths over the vaccine area to reduce pain and
discomfort, and use or exercise the arm. Drinking plenty of fluids and dressing lightly can
help with the general side effects that might appear. The CDC advises people to inform their
doctors if these side effects do not go away after a few days. If the redness or tenderness in
the arm gets worse after 24 hours, people should also consider contacting a doctor.
The CDC's info about coronavirus vaccine side effects is available at this link .
The Food and Drug Administration is planning to warn that Johnson & Johnson's
coronavirus vaccine can lead to an increased risk of a rare neurological condition known as
Guillain–Barré syndrome, another setback for a vaccine that has largely been
sidelined in the United States because of manufacturing problems and a temporary safety pause
earlier this year, according to several people familiar with the plans.
Although regulators have found that the chances of developing the condition are low, they
appear to be three to five times higher among recipients of the Johnson & Johnson vaccine
than among the general population in the United States, according to people familiar with the
decision.
Federal officials have identified roughly 100 suspected cases of Guillain-Barré
disease among recipients of the Johnson & Johnson shot through a federal monitoring system
that relies on patients and health care providers to report adverse effects of vaccines. The
reports are considered preliminary. Most people who develop the condition recover.
... ... ...
Nearly 13 million people in the United States have received Johnson & Johnson's shot,
but 92 percent of Americans who have been fully vaccinated received shots developed by
Pfizer-BioNTech or Moderna. Even though it requires only one dose, Johnson & Johnson's
vaccine has been marginalized by manufacturing delays and a 10-day pause while investigators
studied whether it was linked to a rare but serious blood clotting disorder in women. That
investigation also resulted in a warning added to the fact sheet.
... ... ...
Johnson & Johnson's vaccine has played a minor role in the nation's inoculation campaign
partly because the Baltimore plant that was supposed to supply most of the doses to the United
States has been shut down for three months because of regulatory violations. The factory,
operated by Emergent BioSolutions, a subcontractor, has been forced to throw out the equivalent
of 75 million doses because of suspected contamination, severely delaying deliveries to the
federal government.
... ... ...
The Guillain-Barré cases are expected to be discussed in an upcoming meeting of a
committee of outside experts who advise the C.D.C.
The F.D.A. has also attached a warning to the Pfizer-BioNTech and Moderna vaccines, but some
health officials described that as less serious than the warnings about Johnson & Johnson.
Last month, the agency warned about an increased risk of inflammation of the heart or the
tissue surrounding it -- diseases known as myocarditis and pericarditis -- particularly among
adolescents and young adults who had received Pfizer-BioNTech or Moderna shots. But the C.D.C.
said in most cases, symptoms promptly improved after simple rest or medication.
The Guillian-Barré syndrome is more likely to result in medical intervention,
officials said. It occurs when the immune system damages nerve cells, causing muscle weakness
and occasional paralysis, according to the F.D.A. Several thousand people -- or roughly 10 out
of every one million residents -- develop the condition every year in the United States. Most
fully recover from even the most severe symptoms, but in rare cases patients can suffer
near-total paralysis.
The suspected cases were reported in the Vaccine Adverse Event Reporting System, or VAERS, a
30-year-old federal monitoring system. So far, researchers have not identified any particular
demographic pattern, but the many of the reports in the publicly available database indicate
that the patients were hospitalized.
Guillain-Barré syndrome has also been linked to other vaccines. The Centers for
Disease Control and Prevention has said that flu vaccines, including the 1976 swine flu
vaccine, led to a small increased risk of contracting the syndrome, although some studies
suggested that people are more likely to develop Guillain-Barré from the flu itself than
from flu vaccines. Earlier this year, the F.D.A. warned that GlaxoSmithKline's shingles
vaccine, Shingrix, could also increase the risk of the disease.
If nothing else, this simply demonstrates that "the science" is no longer the priority for
either Big Pharma, nor the federal government, since Big Pharma is now focused on maximizing
profits from its new cash cow, while the federal government is calibrating everything it says
and does with an eye toward encouraging as many American adults as possible to get
vaccinated.
And if people read that they're going to need a booster shot in a few months anyway, why
would they bother getting vaccinated now?
Anyway, having been stymied in the US, Pfizer is trudging ahead with its "booster shot"
plans by striking a deal to expedite resupply to Israel, which is planning to administer a
third "booster" jab to patients with certain high-risk comorbidities starting Aug. 1.
The
Jerusalem Post reports that the next shipment of Pfizer jabs will arrive on Aug. 1 instead
of in September (Israel also has 200K doses of Moderna on hand, but those can only be used on
adult patients).
Israeli PM Naftali Bennett said Sunday: "We have been working on the issue of vaccines for
several weeks," Bennett said. "This morning, I am pleased to announce that after a series of
discussions with Pfizer CEO Albert Bourla, we closed a deal last night to move up the next
vaccination delivery to August 1." "There are vaccines for everyone."
Last week, Israel announced it had agreed on a vaccine-exchange deal with South Korea. Under
the terms of the deal, Israel delivered some 700K doses to South Korea, which it will return
when it receives its next vaccine delivery.
And as we noted earlier, immuno-compromised patients will be able to receive their third
shot starting immediately, said Health Minister Nitzan Horowitz.
In the meantime, Israel continues to register a higher number of daily cases. At the
beginning of June, some 10-20 people were found to be new virus carriers every day. Currently,
several hundred are testing positive on a daily basis. The number of active cases (which had
shrunk to 200 recently) has rebounded to 4,000.
Pfizer will meet with top US health officials on Monday to discuss Pfizer's push to receive
federal authorization for its booster shot, according to
the Associated Press.
"Certainly, immunity decreases over time...the question is how much time," one doctor told
CNBC during an interview Monday morning.
Before Delta arrived in Israel, some believed the country had reached "herd immunity". But
as Dr. Scott Gottlieb and others have pointed out, COVID is now endemic in the human
population, and reaching "COVID zero", a standard that Israel is aiming at, simply might not be
possible. Israeli officials have already acknowledged that with the large percentage of
Israeli's vaccinated, deaths and hospitalizations associated with COVID will likely continue to
decline, even if the number of new cases does rise.
13,313 109
Bacon's Rebellion 1 hour ago (Edited) remove link
/////////////////////////////////////////////////////////////////////////////The
Lancet
Take away....
6,400 total deaths since day 1 of Covid19
1,127,965 people age 65+
138 "vaccinated" deaths = 99.99% survival rate
>> 0.63% greater survival rate in the vaccinated group.
1,764,098 people age 45 to 64
14 "vaccinated" deaths = 99.99% survival rate
>> 0.02% greater survival rate in the vaccinated group.
3,646,848 people age 16 to 44
0 "vaccinated" deaths = 100% survival rate
>> 0.003% greater survival rate in the vaccinated group.
Heart inflammation link to Pfizer and Moderna jabs 7 hrs ago Like |
9
Heart inflammation is a "very rare" side-effect of the Covid vaccines made by Pfizer and
Moderna, according to regulators in Europe.
The European Medicines Agency
said the side-effects were more common in younger men .
The medicines safety body said the benefits of Covid vaccines continue to far outweigh any
risks.
But doctors and patients have been advised to be aware of the symptoms of heart
inflammation.
These include chest pain, a feeling of breathlessness and a pounding or fluttering
heartbeat. Anyone with these symptoms should see a doctor.
Two conditions were linked to the vaccines - inflammation of the heart muscle itself, known
as myocarditis, and inflammation of the fluid-filled sac the heart sits in, known as
pericarditis.
The EMA analysis of cases found:
Pfizer-BioNTech - 145 cases of myocarditis and 138 cases of pericarditis out of 177m
doses given
Moderna - 19 case of myocarditis and 19 cases of pericarditis out of 20 million doses
given
Five people died. The review said they were all either elderly or had other health
conditions.
The UK's Medicines and Healthcare products Regulatory Agency (MHRA) has also been
investigating the link.
It reported: "A consistent pattern of cases occurring more frequently in young males and
shortly after the second dose of the vaccines.
"These reports are extremely rare, and the events are typically mild with individuals
usually recovering within a short time with standard treatment and rest," it added.
Most cases are thought to be within 14 days of vaccination.
While the risk is very rare, it is more likely to develop in young people - who are
currently the focus on the vaccination campaign in the UK.
Concerns about the side-effects have already played into
the UK debate around vaccinating children , who are at lower risk of Covid.
Myocarditis and pericarditis will be officially listed as side-effects in the UK and Europe,
mirroring a
move by the regulators in the US last month .
"The chance of these conditions occurring is very low, but you should be aware of the
symptoms so that you can get prompt medical treatment to help recovery and avoid
complications," the EMA said.
The link with heart inflammation was found only in the vaccines that rely on mRNA technology
to train the immune system.
The was no link found for vaccines such as Oxford-AstraZeneca or Janssen, which use a
genetically modified virus.
However, the EMA has advised anyone with a history of capillary leak syndrome should not be
given the Janssen vaccine. This is a rare but serious syndrome in which fluid leaks from blood
vessels in the body.
So Motley Fool analysts advocate profiteering... Nice. there is some dark neoliberal humor in
stating that the elimation of booster shots is bad..
Keith Speights: Some findings were recently published in Nature magazine that
indicate that the Pfizer-BioNTech and the Moderna vaccines may provide protection for
years.
Many investors are and were hoping for annual recurring revenue from these companies'
vaccines. Brian, how troublesome is this latest data for the prospects for Pfizer, BioNTech,
and Moderna?
Brian Orelli: There's a bit of an extrapolation going on here. The researchers looked at
memory B cells, which tend to provide more long-term protection than, let's say, antibodies.
They looked at those in the lymph nodes and found the cells were there as long as 15 weeks.
Typically, they'd mostly be gone by four to six weeks. So that's the basis of this claim
that it could offer protection for years. If true, that will be a big blow obviously to vaccine
makers, at least for Moderna and BioNTech.
Pfizer would be fine because it's so diversified. It's really hard to make an argument for
the valuations of Moderna and BioNTech right now if these vaccines are one and done over a
couple of years. They really need to have ongoing sales until they can get growth from other
drugs in their pipelines.
Speights: Brian, when I first saw the story, I went to check out to see how the stocks were
performing, and Moderna is up, BioNTech was barely changed, Pfizer barely changed. It seems to
me that investors really aren't making much of this news. Do you think that's the right take at
this point?
Orelli: I think it's still too early to be able to conclude that it's definitely going to
work for years. The other issue is that we're looking at, will those B cells actually protect
against the variants?
If they don't protect against the variants, then it doesn't really matter if you have B
cells in your lymph nodes. If they're not going to protect against the variants then we're
going to have to get a booster shot anyway.
Speights: Right. Obviously, if these vaccines provide immunity for multiple years, these
companies aren't going to make nearly as much money as they expect and a lot of investors
expect. So this is a big story to watch, but like you said, really, really early right now and
too soon to maybe go drawing any conclusions at this point.
The delta variant was estimated by health officials is perhaps twice as contagious as the
original virus and at least 20 percent more contagious than Alpha.. It was first identified in
India a wave of infections there in April and May.
LaCount has lived in Grand Junction, Colo., a city of 64,000, nearly her whole life. As a
hospital pathologist, she knows better than most that her hometown has become one of the
nation's top breeding grounds for the delta variant of COVID-19.
"The delta variant's super scary," LaCount said.
That highly transmissible variant, first detected in India, is now
the dominant COVID-19 strain in the United States. Colorado is among the top
states with the highest proportion of the delta variant, according to the Centers for
Disease Control and Prevention.
Mesa County has the most delta variant cases of any county in Colorado, state health
officials report, making the area a hot spot within a hot spot. A CDC team and the state's
epidemiologist traveled to Grand Junction to investigate how and why cases of the variant were
moving so quickly in Mesa County.
... ... ...
A few yards away from LaCount and her son on the playground, a man fished in a still pond
with his 10-month-old daughter in a backpack. Garrett Whiting, who works in construction, said
he believes COVID is still being "blown out of proportion," especially by the news media.
"They got everybody scared really, really fast," said Whiting, slowly reeling in a sparkly
blue lure from the water. "There's no reason to stop living your life just because you're
scared of something."
Whiting tested positive for COVID about three months earlier. He said he doesn't plan to get
vaccinated, nor does his wife. As for the baby on his back, he said he's not sure whether
they'll have her vaccinated when regulators approve the shot for young children.
Warnings
from around the world
The delta variant is one of four " variants of
concern " circulating in the U.S., according to the CDC, because the delta strain spreads
more easily, might be more resistant to treatment and might be better at infecting vaccinated
people than other variants.
The delta variant has raised alarms around the world. Parts of Australia have
locked down again after health officials said the variant leapfrogged its way from an
American aircrew to a birthday party
where it infected
all unvaccinated guests , and after it also is reported to have jumped between shoppers in
a "
scarily fleeting " moment in which two people walked past each other in a mall.
Israel
reissued an indoor mask requirement after a spate of new cases linked to schoolchildren. A
leading
health official there said about a third of the 125 people who were infected were
vaccinated, and most of the new infections were delta variant.
A rise in delta variant cases delayed the United Kingdom's planned reopening in June. But
public health officials have
concluded after studying about 14,000 cases of the delta variant in that country that full
vaccination with the Pfizer-BioNTech vaccine is 96% effective against hospitalization. Studies
around the
world have made similar findings. There is also evidence the Moderna and Johnson &
Johnson vaccines
are effective against the variant.
Los Angeles
County recently recommended that residents resume wearing masks indoors regardless of
vaccination status, over concern about the delta variant. The World Health Organization is
also urging vaccinated people to wear masks, though the CDC hasn't changed its guidelines
allowing vaccinated people to gather indoors without masks.
After months of data collection, scientists agree: The delta variant is the most contagious
version of the coronavirus worldwide. It spreads about
225% faster than the original version of the virus, and it's currently dominating the
outbreak in the United States.
A new study,
published online Wednesday, sheds light on why. It finds that the variant grows more
rapidly inside people's respiratory tracts and to much higher levels, researchers at the
Guangdong Provincial Center for Disease Control and Prevention reported.
On average, people infected with the delta variant had about 1,000 times more copies of the
virus in their respiratory tracts than those infected with the original strain of the
coronavirus, the study reported.
In addition, after someone catches the delta variant, the person likely becomes infectious
sooner. On average, it took about four days for the delta variant to reach detectable levels
inside a person, compared with six days for the original coronavirus variant.
Article
continues after sponsor message
https://5fa4726d68399a0c53022b32e378f4d8.safeframe.googlesyndication.com/safeframe/1-0-38/html/container.html
GOATS AND
SODA
Is The Variant From India The Most Contagious Coronavirus Mutant On The Planet?
In the study, scientists analyzed COVID-19 patients involved in the first outbreak of the
delta variant in mainland China, which occurred between May 21 and June 18 in Guangzhou, the
capital of Guangdong province. The researchers measured the levels of virus in 62 people
involved in that outbreak and compared them with the levels in 63 patients infected in 2020
with an early version of the virus.
Their findings suggest that people who have contracted the delta variant are likely
spreading the virus earlier in the course of their infection.
GOATS AND
SODA
Coronavirus FAQ: I've Been Vaccinated. Do I Need To Worry About Variants? And the scientists underscore the importance of quarantining immediately for 14 days after
coming into contact with someone diagnosed with COVID-19, as the U.S. Centers for Disease
Control and Prevention recommends.
Or even better, getting fully vaccinated. Preliminary data shows that in some U.S. states,
99.5% of COVID-19 deaths in the past few months were among people who weren't vaccinated, the
CDC's director, Dr. Rochelle Walensky, said Thursday at the White House.
"We know that the delta variant ... is currently surging in pockets of the country with low
vaccination rates," Walensky said. "We also know that our authorized vaccines prevent severe
disease, hospitalization and death from the delta variant."
Los Angeles County is reporting a 165 percent spike in coronavirus infections in a single
week amid the rise of the highly contagious delta variant.
The L.A. County Department of Public Health said in
a statement that 839 new coronavirus infections had been reported as of Thursday. The daily
average case rate is at 3.5 per 100,000 people, up from last week's 1.74 cases per 100,000
people.
The agency said that the delta variant of the coronavirus first identified in India has
become the most commonly sequenced variant in the county since the beginning of June, and now
accounts for the majority of variants identified by labs, "consistent with what other parts of
the U.S. are seeing."
...According to the Centers for Disease Control and Prevention, the variant now makes up the
majority of new cases in the United States, driving spikes in infections in several states.
...The county said that slightly less than 4 million of its residents are still not
vaccinated, while 4.6 million are fully vaccinated.
... There are currently 296 people hospitalized, of which 24 percent are in intensive
care.
8 hours ago (Edited) remove link
The Alpha version of supposed SARS-CoV-2 was supposedly the most transmissible and
infectious pathogen ever. With a transmission rate of at least 3.8 and reported to be perhaps
as high as 9.
Meaning each infected person infects at least 3.8 other people, and perhaps up to nine.
During the year we were told one infected choir singer passed the infection on to at least 220
people in one church. If Delta is 50-60% more infectious than Alpha, then each person will
infect at least six others. Perhaps dozens.
The problem with that, is Delta is from last year in August. That is when it was first
"identified". A pathogen that infectious would have infected over 8 billion people in less than
five weeks.
The supposed Alpha strain would have infected the entire world by the middle of last June.
After a year, the cases would measure in the trillions if the exponential progression
continued. Obviously there aren't trillions of people on the planet.
What that proves is either SARS-CoV-2 isn't as infectious as claimed, or every single person
on the planet has been exposed multiple times and simply didn't even know.
There is a certain definitive fact. Whatever the government tells you is for sure an
absolute lie. lay_arrow
OliverAnd 7 hours ago
Mutations are usually deleterious; one small percentage will mutate into a strain that
may be more or less pathogenic; the purpose of the mutation is so that the virus becomes
less pathogenic so that it can live symbiotically with its host.
We humans are a hilarious bunch; for example we sleep with whores knowing they are
walking STD labs catching herpes, HPV, gonorrhea, etc increasing our chances of cancer
while decreasing our lives by decades, yet we worry about getting vaccinated. We eat
processed foods, junk food, high sugar and salt foods, smoke, speed, drink, etc taking many
years off our lives yet we worry about a jab. Where are all those people not wanting the
vaccine? They are eating at the fast food chains sleeping with that one who has been around
the block stressed out because they are unable to go shopping with their empty pockets.
play_arrow 1
Numerous virologists have said that the vaccine encourages the virus to mutate to bypass the
antibodies produced by the vaccine.
https://www.quantamagazine.org/how-vaccines-can-drive-pathogens-to-evolve-20180510/
You should never trust Goldman, but still
Q. The Delta variant (first identified in India) is estimated to be 50-60% more
transmissible than the Alpha variant (first identified in the UK). How effective are the
Western vaccines against the Delta variant?
A. While the Delta variant weighs on the efficacy of vaccines (and especially single doses)
at preventing infections (especially asymptomatic infections), Pfizer and AstraZeneca full
vaccinations remain highly effective at protecting hospitalizations, and Moderna and J&J
lab results look encouraging
A study from Public Health England estimates elevated Delta-specific efficacies at
preventing hospitalizations of 94%/96% after one/two Pfizer doses and 71%/92% after one/two
AstraZeneca doses. Public Health England estimates lower efficacies at preventing symptomatic
disease after two doses for Pfizer of 88% and 60% for AstraZeneca. Similarly, a new study from
Canada also estimates an 87% efficacy of full Pfizer vaccinations to prevent symptomatic
disease. The symptomatic efficacy, however, is lower after one dose and estimated at one-third
for both Pfizer and AstraZeneca in the English study, and 56%/72% for Pfizer/Moderna in the
Canadian study
Yesterday, Israel's Health Ministry reported a 64% effectiveness of the Pfizer vaccine in
preventing any infections and a 93% effectiveness in preventing hospitalizations. The 64%
estimate likely corresponds to the effectiveness to prevent both asymptomatic and symptomatic
infections while the studies from England and Canada and clinical trials assess symptomatic
infections. Taken at face value, these headline numbers suggest a reduced ability of the Pfizer
vaccine to stop the transmission of Delta infections relative to previously dominant strains,
although the "additional" infections are more likely to be asymptomatic.
Finally, in vitro studies from Moderna and Johnson & Johnson demonstrate their ability
to neutralize the Delta variant with neutralizing titers that were lower compared to the
ancestral strain but higher than for the Beta variant (first identified in South Africa), where
high efficacy against severe disease was clinically demonstrated.
Q. How effective are the Eastern vaccines against the Delta variant?
A. Although data remain very limited, Chinese and Russian expert commentary and clinical
trial results from India's Bharat Biotech suggest that the Sinopharm, Sputnik V, and Bharat
Biotech vaccines provide solid protection against severe disease.
Q. What about Delta's impact on reinfection risk?
A. Although the data are particularly limited, research and experts suggest that prior
infections continue to provide some protection against Delta, especially against severe
disease.
Q. The UK is experiencing a surge in infections although hospitalizations and especially
fatalities remain relatively low (Exhibit 2). What drives this "decoupling" and will it
continue?
A. This mostly reflects the concentration of new infections among younger individuals but
also a stronger vaccine protection against hospitalizations than against infections (especially
for AstraZeneca). We therefore expect this decoupling to continue.
Q. Are infections and hospitalizations/fatalities also "decoupling" outside of the UK?
A. Most other economies with high vaccination rates and Delta outbreaks are also
experiencing this decoupling, although it is particularly pronounced in the UK. We expect
hospitalizations to remain relatively low in high vaccination countries.
Q. Does the virus still matter for activity in North America and Europe if hospitalizations
stay low?
A. Yes. The virus GDP drag should, however, be much diminished and reflects travel
restrictions, consumer risk aversion, and lingering softness in labor supply
... ... ...
Q. The Delta variant has raised the theoretical bar to achieve herd immunity to probably at
least 85% of the population. Does vaccine hesitancy imply that countries will never approach
such high immunity levels?
A. Not necessarily, and many medical experts believe the coronavirus will eventually turn
from a pandemic to an endemic stage. The Delta variant likely implies higher ultimate
vaccination rates (and immunity rates). In fact, further outbreaks appear to be sharply
boosting demand in several countries, including the US, China, Australia, Israel, and
especially Portugal (Exhibit 13).
EatMyAssLibtards 9 hours ago
How anyone can believe this $hit anymore is a question not even God would have an answer
for
Four chan 6 hours ago
ITS GLOBALIST ******** FOLKS.
MaxmaxExtreme 5 hours ago remove link
Wait until the vaccine pushers hear about booster shots until the day they die, or
rather until it kills them.
The Ingenious Gentleman 7 hours ago
The vaccine is the new god. People who get it seem to positively religious about getting
others to do the same. Almost like they have been programmed.
Nona Yobiznes 5 hours ago
Have you seen the reddit community called ChurchOfCOVID? Worth checking out for some
laughs.
HowdyDoody 3 hours ago
What has happened to Goldman Sacks? They are way behind the curve. Delta is yesterday's
news. Lambda is where the action is.
And how about "herd immunity? Is not this a fiaco of the idea?
Jun 26, 2021
The World Health Organization is recommending that everyone, even the fully vaccinated,
continue to wear masks because of the highly transmissible variant.
In an alarming new development, the particularly transmissible delta variant of COVID-19 has infected some
fully vaccinated adults in Israel, officials there have reported.
Of more than 100 daily cases amid an outbreak of the delta variant, half were children
younger than 16.
... Spurred by the new information, the Israeli government has now reimposed an indoor mask
mandate and quickly expanded its vaccination program to include children ages 12 to 15.
The World Health Organization
on Friday also warned everyone, even those fully vaccinated, to
"play it safe" and continue to wear a mask and maintain social distancing in light of the
large numbers of people who remain unvaccinated and the emergence of the delta variant, which
it called the "
most transmissible " form of the coronavirus identified to date.
"People cannot feel safe just because they had the two doses. They still need to protect
themselves," Dr. Mariangela Simao, WHO assistant director-general for access to medicines, said
at a news briefing in Geneva. "Vaccine alone won't stop community transmission."
"People need to continue to use masks consistently, be in ventilated spaces, [use] hand
hygiene ... [practice] physical distance, avoid crowding."
Critique of this finding by Reuters look weak. I think the finding still stands and is an
interesting statistics pointing to the unforeseen danger of vaccination.
Referring to data compiled by Public Health England (PHE) in a technical briefing released
on June 18 regarding the SARS-CoV-2 variants (
here ), the authors of the blogs make several calculations.
On page 12 of the briefing, it shows that 26 people have died since February 1 after testing
positive for the Delta variant of the virus, having also been fully vaccinated for more than
two weeks. In total, 4,087 tested positive more than two weeks after their second dose.
Meanwhile, 35,521 people who were unvaccinated tested positive for the Delta variant and 34
people died.
The authors then divide the number of deaths by the total number of people who tested
positive for the Delta variant and found the rate of death to be 0.000957 for unvaccinated
individuals and 0.00636 for those who have been inoculated.
... ... ...
In England, approximately 85% of the adult population have had one dose of a COVID-19
vaccine and 65% are fully inoculated, Dr Cevik said.
"When most people are vaccinated, most infections and deaths are expected to be among those
vaccinated," she added.
The vaccination program also prioritised "clinically vulnerable" individuals, and thus the
majority of those vaccinated will "disproportionately represent elderly and those with
underlying comorbidities, who are already at significant risk of hospitalisation and death," Dr
Cevik, said.
The posts do not consider the overall higher number of cases due to the Delta variant for
those who are unvaccinated compared to those who are inoculated (
here ).
Highly recommended !That means that 64% of vaccinated can get Delta variant and spread it. This is the last nail
in the coffin of idiotic (in case of coronaviruses) Fauci idea of "herd immunity" and connected
with this fiasco of (1)vaccination of teenagers (and generally people younger then 30), pregnant
women and people who already recovered from COVID-19 and thus has natural immunity
Please note that COVID vaccines are experimental, unproven drugs (or gene therapy in case of
Pfizer and Moderna) and Fauci and other high level medical bureaucrats should be liable for any
negative consequences of this campaign.
The Israeli Ministry of Health announced that an epidemiological analysis had found that
since June 6 there was a "marked decline in the efficacy of the Pfizer vaccine in preventing
infection (64%) and symptomatic illness (64%)."
"This decline has been observed simultaneously with the spread of the Delta variant in
Israel," t he
ministry said in a statement .
At the same time, "The vaccine maintains an efficacy rate of about 93% in preventing serious
illness and hospitalization cases," the officials emphasized.
... Professor Nadav Davidovitch, who sits on the government's expert advisory committee on
the coronavirus, told the Financial Times
the new finding was based on "preliminary" figures gathered by health authorities. "Delta is a
lot more infectious, but appears to not lead to as much serious illness and death, especially
given that we now have the vaccine," he said.
Mina , Jul 4 2021 20:34 utc |
34
Interesting. Swiss team retracted a paper on the little benefit of massive vaccination
https://www.mdpi.com/2076-393X/9/7/729/htm
It included this kind of statement "Thus, we need to accept that around 16 cases will
develop severe adverse reactions from COVID-19 vaccines per 100,000 vaccinations delivered,
and approximately four people will die from the consequences of being vaccinated per 100,000
vaccinations delivered....Adopting the point estimate of NNTV = 16,000 (95% CI,
9000–50,000) to prevent one COVID-19-related death, for every six (95% CI, 2–11)
deaths prevented by vaccinationwe may incur four deaths as a consequence of or associated
with the vaccination.
Simply put: As we prevent three deaths by vaccinating, we incur two deaths."
Another case of Swiss-paid research (as in the time of Tobacco is good?) or do they have a
point? After all, even Cuba, Russia and Iran see the need for vaccinating their
populations.
Jen , Jul 5 2021 11:33 utc |
85
S P Korolev @ 79:
Israel was one of the first countries to get the Pfizer-BioNTech treatment some time last
year after then-PM Netanyahu pushed Israel to the front of the queue using means both fair
and foul (but perhaps more on the foul side).
The Israel People's Committee, comprised of people with medical, legal and epidemiological
expertise,
released a summary report of the country's experience with mass inoculation of the
Pfizer-BioNTech treatment in April this year. It does not make for very comforting reading so
maybe I'll allow Doctors 4 Covid Ethics to take up the narrative:
... The data collected by the group paint a grim picture:
- The overall mortality in the January-February vaccination period was higher in 2021
than in any other year within the preceding decade. In the age group of 20–29 years,
mortality in this time period exceeded that of the previous year by 32%.
- 288 deaths overall, mostly within the first 10 days after vaccination, were reported
to the group. This number is more than six times greater than the 45 deaths officially
admitted to by the Health ministry.
- The group gives the following estimates for the mortality among the vaccinated:
overall, 1:5,000; age 20–49 years, 1:13,000; age 50–69 years, 1:6,000; age 70+,
1:1,600.
- Across lethal and non-lethal adverse events there was a relatively high rate of
cardiac-related injuries, 26% of which occurred in young people below the age of 40, a high
prevalence of massive vaginal bleeding, neurological, skeletal and skin damage, and events
directly or indirectly related to coagulopathy (myocardial infarction, stroke,
miscarriages, disruption of blood flow to the limbs and pulmonary embolism).
According to the authors, the compilation of the report was severely hampered by
obstruction on the part of government authorities, involving in particular the shutting
down of all monitoring and tracking systems for adverse events ...
dustbunny , Jul 5 2021 11:55 utc |
86
Jen | Jul 5 2021 11:33 utc | 85 Founding
signatories .
Mina , Jul 5 2021 12:14 utc |
87
dustbunny,As to the contracts, same opacity for the EUhttps://ec.europa.eu/commission/presscorner/detail/en/ip_21_302 https://www.reuters.com/article/health-coronavirus-eu-pfizer-idUSL1N2ME0Z5 https://www.reuters.com/article/us-health-coronovirus-eu-vaccines-idUSKBN2C10MU
https://www.bloomberg.com/news/articles/2021-05-07/eu-set-to-sign-off-new-pfizer-vaccine-contract-as-soon-as-friday
Lurk , Jul 5 2021 12:31 utc |
89
@dustbunny | Jul 5 2021 11:55 utc | 86
"Confirmed" just how? Because of your unsourced badmouthing? Fool, you are covered
yourself in the mud that you are throwing.
Looking at the list, apart from one psychologist, they all appear to be competent medical
authorities.
S.P. Korolev , Jul 5 2021 12:31 utc |
90
Jen @85
Cheers. I understand part of Israel's sweetheart deal with Pfizer involves keeping most
data collected secret and sharing it only with the company so I'm not surprised data is hard
to come by. The instances of 'coagulopathy' are new to me, likely a different mechanism than
the cause of the AZ/J&J problems. The makers of Sputnik V have identified a possible
cause
of the adenovirus
clotting disorder so hopefully they are looking into the mRNA vaccines also.
Lurk , Jul 5 2021 13:14 utc |
95
@S.P. Korolev | Jul 5 2021 12:31 utc | 90
https://www.biorxiv.org/content/10.1101/2021.06.29.450356v1.full.pdf
Summary paragraphWe show
thatintravenous but not intramuscular injection of ChAdOx1 nCov-19triggers
platelet-adenovirus aggregate formation andplatelet activation. After intravenous
injection, theseaggregates are phagocytosedby macrophagesin the spleenandplatelet remnants
are found in the marginal zone and follicles. This is followed by a pronounced B-cell
response with the emergence of circulating antibodies binding to platelets. Our work
contributes to the understanding of TTS and highlights accidental intravenous injection as
potentialmechanism for post-vaccination TTS. Hence,safe intramuscular injection, with
aspiration prior to injection,could bea potential preventive measurewhen administering
adenovirus-based vaccines.
This is the very recent research that I mentioned
earlier in the thread but without attribution.
Not sure if the reaction as described in the article is triggered by the protein
impurities that Gamaleya claims to have found in the AstraZeneca vaccine.
farm ecologist , Jul 5 2021 13:28 utc |
98
mrna vaccines haven't been promoted as experimental... that is indeed what they
are..
Posted by: james | Jul 4 2021 20:56 utc | 41
The idea for mRNA vaccines has been around for about three decades, but until last year
clinical evidence of their efficacy was minimal. I thus was skeptical about the ones
developed for covid but so far it seems that they do work. Still, it remains to be determined
whether they are as good as traditional vaccines.
You are absolutely correct that all new vaccines and drugs are experimental at first
(whether people realize it or not), but the rules are that clinical trials must show safety
and efficacy before these are licensed for use in the general population. Sometimes things
that are useless or even harmful still manage to get pushed through, which is why postmarket
safety surveillance is so important.
Peter AU1 , Jul 5 2021 6:52 utc |
77
https://www.abc.net.au/news/2021-07-05/australia-covid-astrazeneca-deal-withheld-national-security/100261920
"The total value of Australia's five vaccine deals is more than $5 billion in taxpayer
funds."
Mina , Jul 5 2021 8:31 utc |
78
It does raise questions that the cheap, non-profit, one-shot J&J, which did not need
special storage, got various problems that may also be related to the production of the
vaccines (one case was publicized, https://time.com/5951709/johnson-johnson-covid-19-vaccine-error/).
S.P. Korolev , Jul 5 2021 9:00 utc |
79
re the mRNA vaccines,
What are the most common side effects from the Pfizer vaccine? It's the only one available
in my country as the Govt only accepts vaccines with 90%+ effectiveness and of the four
vaccines we did deals for (Pfizer, AZ, J&J, Novavax) only Pfizer measures up (haven't
heard about results from Novavax, too far down the queue for Moderna and Sputnik V doesn't
exist apparently as we are a 5 eyes country).
Heard of allergic reactions that can be fatal for the very old or very sick, and heart
inflammation issues. The way the heart issues were reported in the media (in the context of
the trials for 12-16 y.o.) made it seem they only effected the young but apparently a problem
for everyone. Doesn't seem as serious as the AZ/J&J clotting issues as it usually clears
up without treatment? My parents are both over 65 and have had their 1st Pfizer doses, no
side effects so far for Dad and a tetanus shot-style sore arm for Mum that lasted a couple of
days.
Mina , Jul 5 2021 9:51 utc |
82
Finally some positive comments on ivm in the Western press
https://news.wttw.com/2021/07/02/covid-19-long-haulers-turning-ivermectin-relief-questions-over-drugs-effectiveness
Jen , Jul 5 2021 11:16 utc |
84
Peter AU 1 @ 77:
That news about Scott Moronson's government doing a deal with Astra Zeneca, the details of
which must be kept hush-hush, does not surprise me.
Look at this from Doctors 4 Covid Ethics:Pfizer
Vaccine Authorised, Data Sight Unseen
A Freedom of Information request to the Australian drugs regulator that approved the
Pfizer vaccine confirms that they have never seen the study data.
A freedom of information request (FOI) request was made by one of our members in
February 2021 to the Australian drugs regulator, the TGA (Therapeutic Good Administration)
to ask what should have been simple questions. The TGA is the Australian equivalent of the
FDA (US), MHRA (UK) and EMA (Europe) and is held in high regard worldwide. Essentially the
FOI questions were:
1/ Did the TGA request the raw data from Pfizer
The rationale of the request relates to concern over the validity and verifiability of
Pfizer's data given its legal history (and expressed by Peter Doshi in the BMJ in February)
as well as the proven concerns over fraudulent data relating to Covid-19 as seen in the
"Lancetgate" scandal of June 2020.
The document ... is a redacted version of the documents that were sent by the TGA in
response to this request. What they show is that the TGA never saw or requested the patient
data from Pfizer and simply accepted their reporting of their study as true. This means
that when the head of the TGA John Skerritt said that "the safety evidence is pretty
thorough" on the 6th February (here) his words would ring hollow to most Australians who
have assumed, rightly or wrongly, that the TGA had actually looked at the patient data
themselves.
A further concerning aspect of the FOI request is the efforts to which the TGA appeared
to go to suppress the request – initially requesting a 6 months extension in view of
a "voluminous request" which eventually yielded only one document of 14 pages, heavily
redacted. This required an instruction from the Office of the Information Commissioner to
the TGA to answer the request by the 26th May, a deadline that the TGA also failed to
meet.
Eventually the only document that was produced from the FOI request was a heavily
redacted single study (not studies, as claimed in the TGA assessment document) showing that
the only investigation into the effects on the fetus was performed on 44 rats with no long
term data on the offspring. It is impossible to assess this study fully because 98% of the
document was removed in order to protect Pfizer's intellectual property (points 32-44 of
the report)...
... Doctors for Covid Ethics remain concerned that the TGA's failure to validate the
Pfizer data has been replicated at other agencies worldwide (FDA, MHRA and EMA). It is
currently not known whether any of the major agencies has independently verified, or
attempted to verify, Pfizer's data, before proceeding with provisional/emergency
authorisation of Pfizer's mRNA therapy vaccine.
Bet this information about how the TGA applied so-called rigour to checking Pfizer's data
before approving the Pfizer-BioNTech treatment sure gladdens your heart, don't it?
Why there is so much social pressure if the idea of "herd immunity" became a fiasco after
emergence of Delta variant, which like South African variant can infect vaccinated people and
thus can spread in vaccinated population (although not as quickly as in unvaccinated population).
What government medical bureaucrats like Fauci are hiding ?
psychohistorian
74
I am retired in the US so I only see some of the working world through others eyes. What I
am seeing more of is pressure to take the vaccine in US even though the infection numbers are
going down in most states.
I have shared before that I have a cousin, my age, that got one of the mRNA vaccines and
now has some sort of blood cancer. I believe this is related to the mRNA vaccines and that
more cases like my cousin will occur and eventually it will effect an "important" someone who
the MSM can't suppress the connection to the vaccines and the flood gates of related cases
like my cousin will open....can you imagine what the blowback will be??.....the jaded in me
says they are planning on that blowback to keep the chaos/fear/manipulation level
high.....its all China's fault/snark
What is the final straw that will bring the barbarian shit show to a halt? Inquiring minds
want to know. What will finally break through the brainwashing?
Biswapriya
Purkayast
80
The state in which I live has made it compulsory for shops to vaaccinate all staff in
order to be permitted to open.
Lurk , Jul 4 2021 21:18 utc |
46
One more post about the new coronavirus, the associated COVID-19 and the "dreaded"
vaccines. Caveat emptor, I am not a medically trained person, just a curious information
hoarder.
While sars-cov-2 primarily targets epithelial cells, the damaging COVID-19 syndrome
appears to be largely related to mast cells. Mast cells are part of the innate immune system
and are the oldest form af immune system. The mast cells are also involved in tissue growth
and regeneration.
I read an interesting article that made a link between secondary dengue syndrome and
covid, suggesting that both are forms of slow-motion anaphylaxis. Classical anaphylaxis
reactions(as eg. peanut allergy) are mediated by mast cells.
It seems that both "long covid" and similar symptoms that arise as complications from
vaccinations are related to an overactivated mast cell system. Check out "mast cell
activation syndrome" for more info. Ivermectin, quercetin and other "maverick" medications
that appear to hold no antiviral efficacy could simply be what quiets the mast cells and
dampens the inflammatory chain reaction.
On another note, there are the reported blood clotting incidents with the Astra Zeneca
vaccine. There is an ongoing discussion that these are caused by improper application of the
vaccine. It has to be injected intramuscularly, and not intravenously. In the former
case, the innate immune system (mast cells) triggers and the reaction is primarily contained
locally in the muscle tissue. From there the larger immune system is informed about the
invader. In case of accidental intravenous application, the vaccine attaches to blood
platelets. This in turn triggers a reaction in the spleen, causing the adaptive immune system
to attack the platelets and white blood cells in an autoimmune type reaction.
So, for the mRNA vaccines (and also COVID itself), it could be important to have a
stabilized mast cell system.
For the Astra Zeneca and (J&J?) vaccine, asking the person applying the vaccine to
draw blood before injecting (in order to test for accidental venous injection) is
important.
Well, at least that's what I understand from what I've picked up lately. Do your own
research and correct me on anything above that I wrote in well-meant ignorance.
Lurk , Jul 4 2021 23:44 utc |
53
@Peter AU1 | Jul 4 2021 22:09 utc | 48
Long covid, and other virus that can take a long tome to recover from I believe trigger
inflammation of the myelin sheath that insulates the nerves.
How interesting that you should mention that. The proverbial affliction featuring
inflammation of myelin sheaths is multiple sclerosis. Mast cells are suspected to play a
major role in the onset of ms.
Guess what serendipitous nugget I found when searching for links between ivermectin and
mast cells?
Common Anti-Parasitic Agent Eases Motor Symptoms, Aids Remyelination in MS Mouse
Model
The actual study that the above article reports on, investigated the effect of ivermectin
on microglia, but as another study puts it: Microglia and mast cells: two tracks on the road
to neuroinflammation . Both cell types are part of the innate immune system.
Another similar find was that palmitoylethanolamide, which is sometimes used to ameliorate
ms progression and symptoms, was proposed for
combating severe lung inflammation in covid-19
On an entirely different track, "antiparasitic" ivermectin was shown to remarkably aid
wound healing and decrease scar tissue formation. As I stated in the previous post, mast
cells are involved also in tissue growth and regeneration, so this could be related. (I have
in the past personally used mimosa hostilis root bark infusion to heal third degree burn
wounds without any scarring, who knows if and what substance in that plant (also known as
tepezcohuite - "skin tree") might have similar effects on mast cells.)
Anyway, to end the speculation here are two medical articles pointing out the relation
between severe covid and mast cell activation:
Covid-19
hyperinflammation and post-Covid-19 illness may be rooted in mast cell activation
syndrome Signatures of mast cell
activation are associated with severe COVID-19
Oh and here's the article (appears to be self-published but no less interesting)
speculating on the parallels between covid and secondary dengue virus infection syndrome:
Immunological mechanisms
explaining the role of IgE, mast cells, histamine, elevating ferritin, IL-6, D-dimer, VEGF
levels in COVID-19 and dengue, potential treatments such as mast cell stabilizers,
antihistamines, Vitamin C, hydroxychloroquine, ivermectin and azithromycin
Mina , Jul 4 2021 21:06 utc |
43
considering the billions of profit made by Pfizer, and the complete politicization of the
authorizations, there is no reason to be optimistic about the West's intentions.https://qz.com/1999082/jj-sold-100-million-worth-of-covid-19-vaccine-shots/
... Watching crowds in football stadiums these latest days and reading about athletes
obliged to get vaxxxed to go to the Olympics in Japan further adds to the dismay. Live
experiment for all or house arrest for the rest of life.
psychohistorian
44
@ Mina, dh-mtl and james about the mRNA vaccines
The axiom of always taking advantage of a crisis, even if you have to sell the crisis, is
at play here. The facts we are seeing come out support this perspective.
Think about how much money Big Pharma saved by foisting their mRNA research costs off on
the brainwashed public. And if it doesn't work out they have immunity from prosecution....its
all legal as Obama has said about the financial rape by the global private finance
cult.....if it does work out then they have a big new income stream instead of using
out-of-patent therapies.....win-win for the wrong side.
The shit show continues until it doesn't....who is "winning" this week?
The U.K. is among the first governments to set out provisional plans for booster shots,
following advice from specialists who are concerned that possible further Covid-19 outbreaks
over the winter could coincide with
a wave of influenza and put pressure on the country's health system.
The government said the actual rollout would depend on further advice from an expert group
known as the Joint Committee on Vaccination and Immunization, based on a host of new data,
including whether protection from the vaccines
weakens after six months .
As of July 2, 2021 out of 4456 total deaths attributed to vaccination (of them 1890 after
vaccination with Pfizer), it looks like there were at least 36 death of people aged less then 30
years after vaccination with Pfizer vaccine (out of 61 total). Around 136 millions were fully
vaccinated,.
Other sources list higher figure (6113)
CDC- 6,113 DEAD Following COVID-19 Injections ("Besides the 6,113 deaths reported, there are
5,172 permanent disabilities, 6,435 life threatening events, and 51,558 emergency room visits."
)so my method of extracting those data from VAERS database might be wrong or not all death are
reported to VAERS.
Another 5 young people were crippled but survived (67 total).
Each year, more than 165 million Americans get the flu shot. There were 85 reported
deaths following influenza vaccination in 2017; 119 deaths in 2018; and 203 deaths in
2019
Between mid-December 2020 and April 23, 2021, at which point between 95 million and 100
million Americans had received their COVID-19 shots, there were 3,544 reported deaths
following COVID vaccination, or about 30 per day
In just four months, the COVID-19 vaccines have killed more people than all available
vaccines combined from mid-1997 until the end of 2013 -- a period of 15.5 years
As of April 23, 2021, VAERS had also received 12,618 reports of serious adverse events.
In total, 118,902 adverse event reports had been filed
In the European Union, the EudraVigilance system had as of April 17, 2021, received
330,218 injury reports after vaccination with one of the four available COVID vaccines,
including 7,766 deaths
In a May 5, 2021, Fox News report, Tucker Carlson asked the question no one is really
allowed to ask: "How many Americans have died after taking the COVID vaccine?"
1
Mefobills says: July 4,
2021 at 1:24 am GMT • 1.8 hours ago • 300 Words ↑ @RoatanBill
Then there's not selling Syria the latest S#00 system to help keep Israel out of Syrian
skies. That tells me he's using Syria for personal / State gain and that is where he's wrong.
That's what makes him just another politician.
I totally get it, there are things that are puzzling to those of us in the audience,
watching the moves from afar.
An advanced S-300 or S-400 system could paint every F-16 as it took off from Israel. This
would be a red line for Israel and would bring in Uncle Shmuel.
Syria (and by extension Russia) has been allowing Israel to overfly her territory and bomb
Hezbollah installations.
It's puzzling – why would you allow a foreign power to bomb your territory, especially
if you have S-300's. The answer must be that Syria and Russia are holding back on purpose for
reasons only known to them. I can speculate, in that they don't want to give away military
capability unless the war goes hot.
Think about the situation now, as opposed to the 90's. Russia's military has been
modernized; Military physical fitness is up by 30% (better nutrition?); Foreign exchange is in
good shape; the economy is modernizing; food production is up – so Russia is no longer
food insecure; oil can be extracted at prices that Saudi cannot compete with; the Artic route
is opening up; national economy is more diversified thanks to the western sanctions; Yamal LNG
will be fueling Asia; Nordstream will be fueling Europe.
The same study says the spike protein is going into blood plasma and traveling all over. I'm
wondering if it can cross the blood brain barrier.
Mustapha Mond
Mefobills July 3, 2021 at 7:39 pm
GMT "¢ 7.5 hours ago
@Mustapha Mond
and if the mRNA vaccines cause the spike proteins to accumulate in the ovaries of women of
childbearing years and younger, this shared concern might play a role.
It's not the spike protein collecting in ovaries. It is the "lipid shell." The lipid is
going to the ovaries and bone marrow according to the Japanese Study. The same study says the
spike protein is going into blood plasma and traveling all over. I'm wondering if it can cross
the blood brain barrier.
Both actions are bad, so your point remains. But, it is possible the body could deal with
the lipid.
So Fauci push toward "herd immunity" was meaningless from the very beginning. In Israel 50%
(which has 85% of adults fully vaccinated with Phizer vaccine) of infected with Delta were
vaccinated.
Both South African variant and the Delta variant (also known as B.1.617.2) changed the
picture of "herd immunity". Official figure is that Two doses of Pfizer's vaccine are still 88
percent effective at preventing symptomatic Delta infections. You can probably cut this figure by
half to get more realistic estimate based on Israel experience with Pfizer vaccine. Israel has
fully vaccinated about 85 percent of adults
Worryingly, a recent study documented several cases during India's spring surge in which
health-care workers who were fully vaccinated with AstraZeneca's vaccine were infected by Delta
and passed it on.
Now there is talk about that vaccinated people
might need booster shots . Which essentally mean re-vaccination with the newer version of
vaccine.
When breakthrough cases do arise, it's not always clear why. The trio of vaccines now
circulating in the United States were all designed around the original coronavirus variant, and
seem to be a bit less effective against some newer versions of the virus. These troublesome
variants have yet to render any of our current vaccines obsolete. But "the more variants there
are, the more concern you have for breakthrough cases," Saad Omer, a vaccine expert at Yale,
told me. The circumstances of exposure to any version of the coronavirus will also make
a difference. If vaccinated people are spending time with groups of unvaccinated people in
places where the virus is running rampant, that still raises their chance of getting sick.
Large doses of the virus can overwhelm the sturdiest of immune defenses, if given the
chance.
The human side of the equation matters, too. Immunity is not a monolith, and the degree of
defense roused by an infection or a vaccine will differ from person to person, even
between identical twins . Some people might have underlying conditions that hamstring their
immune system's response to vaccination; others might simply, by chance, churn out fewer or
less potent antibodies and T cells that can nip a coronavirus infection in the bud.
Read:
You're not fully vaccinated on the day of your last dose
The effects of vaccination are best considered along a spectrum, says Ali Ellebedy, an
immunologist at Washington University in St. Louis. An ideal response to vaccination might
create an arsenal of immune molecules and cells that can instantaneously squelch the virus,
leaving no time for symptoms to appear. But sometimes that front line of fighters is relatively
sparse. Should the virus make it through, "it becomes a race [against] time," Ellebedy told me.
The pathogen rushes to copy itself, and the immune system recruits more defenders. The longer
the tussle drags on, the more likely the disease is to manifest.The range of vaccine
responses "isn't a variation of two- to threefold; it's thousands," Ellebedy told me.
"Being vaccinated doesn't mean you are immune. It means you have a better chance of
protection."
For these reasons and more, Viviana Simon, a virologist at the Icahn School of Medicine at
Mount Sinai, in New York, dislikes the term breakthrough case , which evokes a barrier
walling humans off from disease. "It's very misleading," she told me. "It's like the virus
'punches' through our defenses."
Vaccination is actually more like a single variable in a dynamic playing field -- a
layer of protection, like an umbrella, that might guard better in some situations than
others. It could keep a lucky traveler relatively dry in a light drizzle, but in a windy
maelstrom that's whipping heavy droplets every which way, another person might be overwhelmed.
And under many circumstances, vaccines are still best paired with safeguards such as masks and
distancing -- just as rain boots and jackets would help buffer someone in a storm.
Read: People
are keeping their vaccines secret
In some ways, the shots' staggering success in trials -- where
breakthrough cases were also observed, causing appropriately minimal stir -- may have
papered over the inevitability of post-vaccination infections in more natural settings. "The
vaccines exceeded expectations," Luciana Borio, a former acting chief scientist at the FDA,
told me. Now, as we exit what Borio calls the "honeymoon phase" of our relationship with the
jabs, we need to temper our enthusiasm with the right amount of realism, especially as more
data on the shots' strength and longevity accumulate. Even excellent vaccines aren't foolproof,
and they shouldn't be criticized when they're not. "We can't expect it's going to be perfect,
on day one, always," Borio said.
A team at the CDC is tracking breakthroughs and will soon start reporting case counts, as
well as any patterns related to where, or in whom, these infections are occurring, Martha
Sharan, a CDC spokesperson, told me. Details like those matter. They can help experts figure
out why post-vaccination infections happen, and how they might be stopped. "The reassuring part
is, these cases will not go unnoticed," Omer told me.
Most of the time, vaccines are far more likely to offer some help than none. Serious
disease, hospitalization, and even death
will still occur , as will less well-studied outcomes, such as the long-term symptoms that
often arise from less severe disease. But should post-vaccination infections climb to
unexpectedly high rates, backup plans will quickly kick into gear. Some shot recipients might
get second or third shots to bolster their immune response; others might be administered a
tweaked vaccine recipe to account for a new viral variant.
There's something a touch counterintuitive about breakthrough cases: The more people we
vaccinate, the more such cases there will be, in absolute numbers. But the rate at which they
appear will also decline, as rising levels of population immunity cut the conduits that the
virus needs to travel. People with lackluster responses to vaccines -- as well as those who
can't get their jabs -- will receive protection from the many millions in whom the shots
did work. In a crowd of people holding umbrellas, even those who are empty-handed will
stay more dry.
Katherine J. Wu is a staff writer
at The Atlantic, where she covers science.
Might be uptick might be statistical noise. The differences are stillsmall... in Israel the
Delta variant is infecting vaccinated people, who represent as many as 50% of new cases
If vaccines don't cover everyone, we need to know why and how we can fix it. Fauci is one
trick pony who made all bets of the success of the vaccines, decpite that fact that there were no
any sucessful coronavirus vaccine developered before COVID-19 epidemic.
Notable quotes:
"... Most Covid-19 patients in the Mercy hospital in Springfield are unvaccinated, though there have been a few cases among people who were vaccinated, Dr. Sistrunk said. ..."
The variant, which is about
40% to 60% more contagious than the previous dominant variant, is sending more people to
hospitals in the northern and southwestern parts of the state, health officials say.
In Springfield, Mo., Mercy Hospital had 90 Covid-19 patients on a recent day, up from 10
seven weeks ago, said William Sistrunk, lead infectious-disease doctor for Mercy, a multistate
hospital system with several facilities in Missouri. Almost all had the Delta variant, and most
were unvaccinated, he said. The hospital's caseload peaked at about 120 in late December.
Officials say the patients being admitted are younger, ages 30 to 60, a change from the last
two waves of infection. "It ramped up a lot faster than it did last fall when we had that
wave," Dr. Sistrunk said. "What's happening in Springfield may be an early warning for other
communities. This variant, we need to take this seriously."
The number of people in the hospital with Covid-19 in Missouri has started to climb in
recent weeks. The latest seven-day average is 864, up from 668 a month prior, according to the
state health department. During the winter surge in Covid-19 cases in 2020 and 2021,
hospitalizations topped 2,700 several times. Missouri has a population of 6.1 million.
... In Missouri, 55% of adults have received at least one vaccination shot, 11 percentage
points below the national rate, according to the CDC. Most Covid-19 patients in the Mercy
hospital in Springfield are unvaccinated, though there have been a few cases among people who
were vaccinated, Dr. Sistrunk said.
Defining a vaccine breakthrough infection
For the purpose of this surveillance, a vaccine breakthrough infection is defined as the
detection of SARS-CoV-2 RNA or antigen in a respiratory specimen collected from a person ≥14
days after they have completed all recommended doses of a U.S. Food and Drug Administration
(FDA)-authorized COVID-19 vaccine.
Identifying and investigating hospitalized or fatal
vaccine breakthrough cases
As of May 1, 2021, CDC transitioned from monitoring all reported vaccine breakthrough cases
to focus on identifying and investigating only hospitalized or fatal cases due to any cause.
This shift will help maximize the quality of the data collected on cases of greatest clinical
and public health importance.
Previous data on all vaccine breakthrough cases reported to CDC from January–April
2021 are available .
State health departments report vaccine breakthrough cases to CDC. CDC now monitors reported
hospitalized or fatal vaccine breakthrough cases for clustering by patient demographics,
geographic location, time since vaccination, vaccine type, and SARS-CoV-2 lineage. Reported
data include hospitalized or fatal breakthrough cases due to any cause, including causes not
related to COVID-19.
To the fullest extent possible, respiratory specimens that test positive for SARS-CoV-2 RNA
are collected for genomic sequencing to identify the virus lineage that caused the
infection.
Some health departments may continue to report all vaccine breakthrough cases to the
national database and can continue to submit specimens to CDC for sequencing. However, CDC will
focus its monitoring on reported hospitalized and fatal cases.
Developing a data access
and management system for reporting COVID-19 vaccine breakthrough cases
CDC developed a national COVID-19 vaccine breakthrough REDCap database where designated
state health department investigators can enter, store, and manage data for cases in their
jurisdiction. State health departments have full access to data for cases reported from their
jurisdiction.
Ultimately, CDC will use the National
Notifiable Diseases Surveillance System (NNDSS) to identify vaccine breakthrough cases.
Once CDC has confirmed that a state can report vaccination history data to NNDSS, CDC will
identify vaccine breakthrough cases through that system. At that time, the state health
departments can stop reporting cases directly into the REDCap database. After this change, CDC
will upload the available data reported to NNDSS into REDCap database for further review and
confirmation by the state health department.
Hospitalized or fatal COVID-19 vaccine
breakthrough cases reported to CDC as of June 21, 2021
As of June 21, 2021, more than 150 million people in
the United States had been fully vaccinated against COVID-19.
During the same time, CDC received reports from 47 U.S. states and territories of 4,115
patients with COVID-19 vaccine breakthrough infection who were hospitalized or died.
Total number of vaccine breakthrough infections reported to CDC
Hospitalized or fatal vaccine breakthrough cases reported to CDC
4,115
Female
2,001
(49%)
People aged ≥65 years
3,124
(76%)
Asymptomatic infections
750
(18%)
Hospitalizations*
3,907
(95%)
Deaths†
750
(18%)
*1,004 (26%) of 3,907 hospitalizations reported as asymptomatic or not related to
COVID-19.
Previous data on all vaccine breakthrough cases reported to CDC from January–April
2021 are available .
How to interpret
these data
The number of COVID-19 vaccine breakthrough infections reported to CDC likely are an
undercount of all SARS-CoV-2 infections among fully vaccinated persons. National surveillance
relies on passive and voluntary reporting, and data might not be complete or representative.
These surveillance data are a snapshot and help identify patterns and look for signals among
vaccine breakthrough cases.
Data on patients with vaccine breakthrough infection who were hospitalized or died will be
updated regularly. Studies are being conducted in multiple U.S. sites that will include
information on all vaccine breakthrough infections regardless of clinical status to supplement
the national surveillance.
COVID-19 vaccines are effective
Vaccine breakthrough cases occur in only a small percentage of vaccinated people. To
date, no unexpected patterns have been identified in the case demographics or vaccine
characteristics among people with reported vaccine breakthrough infections.
COVID-19 vaccines are effective. CDC recommends that everyone 12 years of age and older
get a COVID-19 vaccine as soon as they can.
People who have been fully
vaccinated can resume activities that they did prior to the pandemic.
Looks like two doses of Pfizer vaccine are effective against hospitalization (but not from
infection) from the Delta variant, according to UK data.
Roughly 10 per cent of infections in the US are linked to the variant, but that rate is
doubling every two weeks, the former FDA chief told CBS
News on Sunday .
"That doesn't mean that we're going to see a sharp uptick in infections, but it does mean
that this is going to take over," he said. "And I think the risk is really to the fall that
this could spike a new epidemic heading into the fall."
The more-contagious B 1.161.2 variant – a common development as a virus replicates
through transmission – was first discovered in India and has emerged as a dominant
strain in the UK, responsible for roughly 90 per cent of new infections there.
Are those cases false positives or are a testament that new mutation evade vaccine
protection?
A star NBA player, the U.S. Open golf champion and a Ugandan Olympic coach have something in
common that is creating a new headache for sports organizers: they tested positive for the
novel coronavirus after being vaccinated.
Throughout the pandemic, athletes have been the most tested population on the planet,
sometimes providing vivid examples of emerging theories""and sometimes helping prove them.
Now these athletes are showing that while vaccines are exceptionally effective in preventing
death and severe illness from the coronavirus and its known variants, some are far from
foolproof in preventing infection altogether.
Most of the athletes with so-called "breakthrough" infections are asymptomatic. The
infections wouldn't have been noticed except for the fact that people who work in sports are
among the last being tested intensely for the virus.
These surprising positive tests are a problem for the hosts of large events. In the case of
the Olympics, they could trigger an outbreak in the surrounding Japanese population or beyond,
to any of the 200 participating nations""in addition to creating chaos in competitions.
The positive tests also complicate the argument made to athletes that vaccination will spare
them from a positive test that bars them from competition. Now sports leaders have to contend
with questions such as: Are people who are vaccinated but testing positive for the virus
contagious? What does this mean for their close contacts? Who, if anyone, should be removed
from the biggest event of their lives?
... ... ...
Breakthrough infections also hit the New York Yankees, professional golfer Jon Rahm and NBA
star Chris Paul. In Rahm's case, he had only recently had his shot. But in the case of the
Yankees, that wasn't the obvious factor. In May, at least nine Yankees" spanning players,
coaches and staff members" tested positive for the virus. All had been vaccinated in March or
April with the single-dose Johnson & Johnson vaccine ,
which has been found to be 66.1% effective at protecting people from developing moderate
and severe cases of Covid-19 at least 28 days after vaccination.
Rahm, the golfer, got the Johnson & Johnson vaccine in the days leading up to the
Memorial Tournament. As he played his third round, a test he had taken after his second round
came back positive. Rahm found out at the end of his round from the PGA Tour's medical adviser,
on national television""yanking away a near-sure win in the tournament, and a payday of nearly
$1.7 million. Two weeks later, however, he was testing negative and won the U.S. Open.
... ... ...
There have been at least two prominent, apparent breakthrough cases in the NBA. The most
recent involves Paul, the Phoenix Suns' star and the president of the National Basketball
Players Association, who missed the first games of the Western Conference Finals while
sidelined by the league's health and safety protocols. Paul tested positive despite being fully
vaccinated and remained asymptomatic, according to multiple reports.
The more-transmissible delta variant first found in India and now spread widely in the U.K.
is expected to become the dominant strain in the U.S., said Rochelle Walensky, director of the
Centers of Disease Control and Prevention. She added that full vaccination provides good
protection against it.
To coronavirus behaved like expected and partially defeated vaccination efforts.
LA County -Strongly- Recommends Masks For Vaxx'd & Unvaxx'd People Over -Delta- COVID-19
Variant - ZeroHedge
The Los Angeles
County health agency suggested to residents that they wear masks -- regardless of vaccination
status -- due to the so-called " Delta " COVID-19 variant.
... ... ...
The World Health Organization (WHO) has similarly called on people to wear masks due to the
Delta variant, which is believed to have emerged in India. Meanwhile, Hong Kong officials also
announced this week that it will ban travelers from the UK over concerns about the
strain.
Those warnings came after officials in Israel said that half the adults infected in a recent
Delta COVID-19 outbreak fully vaccinated, according to the
Wall Street Journal late last week.
However, some have said that the concerns about the Delta strain are overblown.
"Don't let the fearmongers win," wrote Sen. Rand Paul (R-Ky.) on
Tuesday.
"New public England study of delta variant shows 44 deaths out of 53,822 (.08%) in
unvaccinated group."
Separately, pharmaceutical giant Moderna said that its two-dose mRNA COVID-19 vaccine works
against the Delta strain, which will likely be used in future arguments against new masking or
lockdown mandates.
"These new data are encouraging and reinforce our belief that the Moderna COVID-19 Vaccine
should remain protective against newly detected variants," CEO Stéphane Bancel said in a
press release issued on Tuesday about the findings.
vk
8
US should
ask scientists to investigate itself if it truly cares about origins: epidemiologist
I agree. If the US scientists are so worried about the possibility the SARS-CoV-2 leaked
from a laboratory, why don't they also ask their government to investigate their own
labs?
Charlatans are a plague in modern science.
Grieved , Jun 17 2021 17:55 utc |
28
And also, the corruption of the medical profession, to which he is now speaking (it's
running as I write this). The interviewer is using the words "medical mafia", citing the
later manifestations we've seen this year. But this interview seems that it will do much to
illustrate the long process of corruption that has happened over the years and decades, and
this is very valuable to learn.
Worth spelling the link out, if I may:Swine Flu And Covid:
Pandemic Deja Vu? / With Dr Wolfgang Wodarg 9th June
Many thanks for this.
john , Jun 17 2021 20:20 utc |
38
Grieved @ 28
The interviewer is using the words "medical mafia", citing the later manifestations
we've seen this year
Yes, the circuitous depravity they've engaged, the 'offer you can't refuse' has worked
wonders, as the interviewer attests his young peers who've taken the jab only to
regain their 'freedom', like my youngest daughter, 30, against my spoken preference, and my
silent prayers.
Notable quotes:
"... On Monday, health officials in Los Angeles County followed suit , recommending that "everyone, regardless of vaccination status, wear masks indoors in public places as a precautionary measure." ..."
"... Natural immunity among those already infected has also kept transmission low, she noted, but it is not clear how long natural immunity will last. ..."
But that was before the spread of the Delta
variant . Worried by a global surge in cases, the World Health Organization last week
reiterated its longstanding recommendation that everyone -- including the inoculated -- wear
masks to stem the spread of the virus.
On Monday, health officials in Los Angeles County followed
suit , recommending that "everyone, regardless of vaccination status, wear masks indoors in
public places as a precautionary measure."
Barbara Ferrer, the county's public health director, said the new recommendation was needed
because of upticks in infections, a rise in cases due to the worrisome Delta
variant , and persistently high numbers of unvaccinated residents, particularly children,
Black and Latino residents and essential workers.
Roughly half of Los Angeles County residents are fully
vaccinated , and about 60 percent have had at least one dose. While the number of positive
tests is still below 1 percent in the county, the rate has been inching up, Dr. Ferrer added,
and there has been a rise in the number of reinfections among residents who were infected
before and did not get vaccinated.
To the extent that Los Angeles County has managed to control the pandemic, it has been
because of a multilayered strategy that combined vaccinations with health restrictions aimed at
curbing new infections, Dr. Ferrer said.
Natural immunity among those already infected has also
kept transmission low, she noted, but it is not clear how long natural immunity will last.
Notable quotes:
"... On Monday, health officials in Los Angeles County followed suit , recommending that "everyone, regardless of vaccination status, wear masks indoors in public places as a precautionary measure." ..."
"... Natural immunity among those already infected has also kept transmission low, she noted, but it is not clear how long natural immunity will last. ..."
But that was before the spread of the Delta
variant . Worried by a global surge in cases, the World Health Organization last week
reiterated its longstanding recommendation that everyone -- including the inoculated -- wear
masks to stem the spread of the virus.
On Monday, health officials in Los Angeles County followed
suit , recommending that "everyone, regardless of vaccination status, wear masks indoors in
public places as a precautionary measure."
Barbara Ferrer, the county's public health director, said the new recommendation was needed
because of upticks in infections, a rise in cases due to the worrisome Delta
variant , and persistently high numbers of unvaccinated residents, particularly children,
Black and Latino residents and essential workers.
Roughly half of Los Angeles County residents are fully
vaccinated , and about 60 percent have had at least one dose. While the number of positive
tests is still below 1 percent in the county, the rate has been inching up, Dr. Ferrer added,
and there has been a rise in the number of reinfections among residents who were infected
before and did not get vaccinated.
To the extent that Los Angeles County has managed to control the pandemic, it has been
because of a multilayered strategy that combined vaccinations with health restrictions aimed at
curbing new infections, Dr. Ferrer said.
Natural immunity among those already infected has also
kept transmission low, she noted, but it is not clear how long natural immunity will last.
As the Delta variant of the coronavirus surges through the U.K., almost half of the
country's recent Covid-19 deaths are of people who have been vaccinated.
.... ... ...
The U.K. is a testing ground for how vaccines are coping. Delta is racing through the
country -- with 146,000 identified cases in the past week, 72% up on the week before. The
country is also a world leader in identifying through testing and genetic sequencing which
versions of the virus are prevalent: By mid-June, 97% of cases were Delta infections. And Delta
is spreading among a population that is among the most highly vaccinated in the world: 85% of
adults have had at least one vaccine shot and 63% have had two.
Data from Public Health England show that there were 117 deaths among 92,000 Delta cases
logged through June 21. Fifty of those -- 46% -- had received two shots of vaccine.
First, vaccines aren't 100% effective. Not everyone who is inoculated will respond in the
same way. Those who are elderly or whose immune systems are faulty, damaged or stressed by some
other illness are less likely to mount a robust response than someone younger and fitter.
Covid-19 vaccines are highly effective but some people will still be vulnerable to the virus
even after receiving their shots.
Second, the risk of dying from Covid-19 increases steeply with age. If a vaccine reduces an
80-year-old's risk of death from Covid-19 by 95%, for instance, that 80-year-old's risk of
death might still be greater than the risk faced by an unvaccinated 20-year-old. Some chronic
illnesses such as diabetes, hypertension and lung disease are also associated with a higher
risk of severe illness and death.
Third, as more of the population gets vaccinated, there are fewer unvaccinated people for
the virus to infect. If the pool of vaccinated people is larger than the pool of unvaccinated
people, then it is possible and even likely that breakthrough infections resulting in death in
the older, vaccinated group would match or exceed deaths in the younger, unvaccinated group.
Consider an imaginary country with 100% of people vaccinated, where the virus can still somehow
spread. All Covid-19 deaths would be in vaccinated individuals.
Of those 50 deaths in fully vaccinated people in England, all were in people aged 50 years
and over, the data show. There have been no deaths recorded in double-vaccinated under 50s.
The data show that, overall, the fatality rate for confirmed cases of Covid-19 has been
lower than it was with the Alpha variant, which was first spotted in the U.K.
... Public Health England, using a variety of statistical analyses, has estimated that
vaccination reduces the risk of hospitalization with the Delta variant in people who have
received two doses by between 91% and 98%, with a central estimate of 96%.
Though vaccines offer substantial protection against severe illness and death, there is
growing evidence from lab studies and real-world data that Delta does have some ability to
bypass vaccines to cause milder infection.
Public Health England says that its analysis of Delta cases in England implies protection
against symptomatic Covid-19 caused by Delta of around 79%. That compares with an 89% reduction
in the risk of symptomatic Covid-19 with Alpha.
In Israel, a senior health official said in late June that in a recent outbreak of 200 or so
Delta cases, about half were in children 15 years old and younger and the other half were in
those aged 16 and above, of whom more than 80% are fully vaccinated.
British data shows Delta is even more adept at evading our immune response after just one
dose of vaccine, highlighting the importance, public health officials say, of getting two
shots. A single dose reduces the risk of symptomatic Covid-19 with Alpha by 49%, according
Public Health England, but only by 35% with Delta.
Notable quotes:
"... De Garay explained that after receiving the second coronavirus vaccine dose, her daughter started developing severe abdominal and chest pains. Maddie described the severity of the pain to her mother as "it feels like my heart is being ripped out through my neck." ..."
"... The Ohio mother added her daughter experienced additional symptoms that included gastroparesis, nausea, vomiting, erratic blood pressure, heart rate, and memory loss. "She still cannot digest food. She has a tube to get her nutrition," De Garay said to Carlson. "She also couldn't walk at one point, then she could I don't understand why and [physicians] are not looking into why...now she's back in a wheelchair and she can't hold her neck up. Her neck pulls back." ..."
"... De Garay said she had joined a Facebook support group to help people cope with the unexpected events happening from the coronavirus vaccine trial, and she said it was shut down. "It's just not right," she said. ..."
"... Sen. Ron Johnson , R-Wis., has sent letters to the CEOs of Pfizer and Moderna seeking answers about adverse reactions to the COVID-19 vaccine following a June 28 press conference with affected individuals. The conference in Milwaukee included stories from five people, including De Garay ..."
"... The Wisconsin senator noted that some adverse reactions were detailed in Pfizer's and Moderna's Food and Drug Administration (FDA) emergency use authorization (EUA) memorandums following early clinical trials ..."
"... Those reactions included nervous system disorders and musculoskeletal and connective tissue disorders for the Pfizer EUA memo. The Moderna EUA memo included reactions such as nervous system disorders, vascular disorders and musculoskeletal and connective tissue disorders, according to Johnson's letter. ..."
"... You missed the whole point! The issue is that the government is not acknowledging and and not reporting these side effects of the vaccine. Instead they are lying about the safety. If you are young, you are much more likely to get sick and injured by the vaccine than COVID. ..."
"... anyone under 25 should not get the vaccine because the percentages are about the same or worse having a negative impact from the vaccine versus the actual virus. ..."
"... With the Covid19 mortality rate among the children why even vaccinate? As a Chemist / Biochemist I learned that there is always unintended consequences. ..."
"... Vaccines may have long term effects that are not known today. ..."
"... The CDC's generic guidelines for getting a vaccine for any reason are very restrictive, first being, the disease you're getting vaccinated against has to pose a real, immediate danger. CV-19 poses virtually no danger whatsoever to kids under 14. Of all the deaths of children 14 and under in the last 18 months only .8% of them had a case of CV-19. That's 367 deaths out of over 46,000. (Data from CDC website) Forcing them to take an experimental vaccine that they absolutely don't need is criminal. As a parent, allowing your child to take the vaccine without spending a few hours doing some research is criminally negligent. This is like some terribly warped Kafka novel but it's real. ..."
Mom details 12-year-old daughter's extreme reactions to COVID vaccine, says she's now in
wheelchair Stephanie De Garay shares story with Tucker Carlson By Stephanie Giang-Paunon | Fox
News Facebook Twitter
Flipboard Comments Print Email
https://static.foxnews.com/static/orion/html/video/iframe/vod.html?v=20210701170943#uid=fnc-embed-1
Mom describes daughter's
bad COVID vaccine reaction, says she's now in wheelchair
Mother Stephanie De Garay joins 'Tucker Carlson Tonight' to discuss how her 12-year-old
daughter volunteered for the Pfizer vaccine trial and is now in a wheelchair.
An Ohio mother is speaking out
about her 12-year-old daughter suffering extreme reactions and nearly dying after volunteering
for the Pfizer coronavirus
vaccine trial.
Stephanie De Garay told "Tucker Carlson Tonight" Thursday
that after reaching out to multiple physicians they claimed her daughter, Maddie De Garay,
couldn't have become gravely ill from the vaccine.
"The only diagnosis we've gotten for her is that it's conversion disorder or functional
neurologic symptom disorder, and they are blaming it on anxiety," De Garay told Tucker Carlson.
"Ironically, she did not have anxiety before the vaccine."
De Garay explained that after receiving the second coronavirus vaccine dose, her daughter
started developing severe abdominal and chest pains. Maddie described the severity of the pain
to her mother as "it feels like my heart is being ripped out through my neck."
Video
The Ohio mother added her daughter experienced additional symptoms that included
gastroparesis, nausea, vomiting, erratic blood pressure, heart rate, and memory loss. "She still cannot digest food. She has a tube to get her nutrition," De Garay said to
Carlson. "She also couldn't walk at one point, then she could I don't understand why and
[physicians] are not looking into why...now she's back in a wheelchair and she can't hold her
neck up. Her neck pulls back."
Carlson asked whether any officials from the Biden administration or representatives from
Pfizer company have reached out to the family. "No, they have not," she answered.
"The response with the person that's leading the vaccine trial has been atrocious," she
said. "We wanted to know what symptoms were reported and we couldn't even get an answer on
that. It was just that 'we report to Pfizer and they report to the FDA.' That's all we
got."
After her heartbreaking experience, the Ohio mother said she's still "pro-vaccine, but also
pro-informed consent." De Garay mentioned she's speaking out because she feels like everyone
should be fully aware of this tragic incident and added the situation is being "pushed down and
hidden."
De Garay said she had joined a Facebook support group to help people cope with the
unexpected events happening from the coronavirus vaccine trial, and she said it was shut
down. "It's just not right," she said.
"They need to do research and figure out why this happened, especially to people in the
trial. I thought that was the point of it," De Garay concluded. "They need to come up with
something that's going to treat these people early because all they're going to do is keep
getting worse."
Sen. Ron
Johnson COVID-19 vaccine .
The Wisconsin senator noted that some adverse reactions were detailed in Pfizer's and
Moderna's Food and Drug Administration (FDA) emergency use authorization (EUA) memorandums
following early clinical trials .
Those reactions included nervous system disorders and musculoskeletal and connective tissue
disorders for the Pfizer EUA memo. The Moderna EUA memo included reactions such as nervous
system disorders, vascular disorders and musculoskeletal and connective tissue disorders,
according to Johnson's letter.
Pfizer and Moderna did not immediately respond to inquiries from Fox News about Johnson's
letters.
J jeff5150357 6 hours ago
My daughter had the same thing happen to
her after getting a flu vaccine 9 years ago. Within days of getting it, she went from being as
healthy as an ox to years of awful, unexplained illness. The short version is they concluded
that she had a severe adverse reaction to the vaccine, but from the delivery chemicals, not the
flu content itself. Formaldehyde was the likely major cause. Now she is getting ready to begin
college and is being required to get the Covid vaccine by her university and the NCAA for
athletics. It is causing her, my wife and I horrible anxiety and we feel like we are being
railroaded into something that could be very dangerous for her. Any discussion or concern
expressed on social media is immediately blocked. I know from years of working in the research
grants office at Yale University that the big pharma industry is powerful and will go to great
lengths to control the narrative. What I don't understand is why mainstream media and social
media are so willing to help them these days!
jeff5150357 4 hours ago
While the college experience is great for a young adult. I would look at getting a degree
online. Her future earnings will be based on her merit, not where she went to school. If
someone was telling me what to do with my personal health, and I was uncomfortable with their
prescription, I would follow my instincts.
LoraJane92649 jeff5150357 5
hours ago
If her flu vax is well documented she should be able to get a waiver. Hopefully you
have an able bodied family physician or medical team to advocate on your behalf.
G gunvald 7 hours ago
You know when you take it that there can be adverse
reactions. So, in that sense, you are informed. Any one of us could be the odd person. That
said, I have a problem with any child getting these vaccines, especially when most people
recover from the disease. It's one thing for me as an elderly person to make the decision to
take it as covid affects the elderly person more and I wanted to avoid that ventilator. Most of
my life has been lived and that's how I evaluated it. This will always come down to putting it
in God's hands.
TheTruthAsItIs gunvald 6 hours ago
You missed the whole point! The
issue is that the government is not acknowledging and and not reporting these side effects of the
vaccine. Instead they are lying about the safety. If you are young, you are much more likely to
get sick and injured by the vaccine than COVID.
D DontDestoryUSA
gunvald 4 hours ago
It's not being informed when you are forced to take a vaccination that they
clearly had trouble with past vaccination sounds like a lawsuit for the university is on the
horizon. With a big pay day
Tony5SFG 7 hours ago
"Ohio
mother said she's still "pro-vaccine, but also pro-informed consent." " And as a pediatrician
for over 40 yrs (retired now) and a 10 year member of my medical school's Institutional Review
Board (which had to approve all human research), THAT is a problem I have been bringing up As
far as requiring all young people, such as entering or in college, to get the vaccine Children
are a protected class and the informed consent for research on them is much more strenuous than
for adults And, requiring young people to take these new vaccines is the equivalent of doing
research on them. The issue of myocarditis is quite troubling. And while it has been seen in
natural infections, I have not yet seen an adequate risk - benefit evaluation regarding risking
natural infection versus vaccination And people say that the myocarditis is not severe, no one
can be sure of the long term effects of a young person getting it. The vaccines that we give
children have been used for decades and the risks/benefits have been well established
D DallasAmEmail Tony5SFG 6 hours ago
A friends daughter who just went through internship as
Physicians assistant based on the percentages in age groups believes anyone under 25 should not
get the vaccine because the percentages are about the same or worse having a negative impact
from the vaccine versus the actual virus. Yes, older age groups the percent having negative
impact from the virus is much greater than the vaccine, so yes older age groups should get the
vaccine. What really is bothersome is when Youtube removes Dr. Robert Malone video who helped
create the mrna vaccine express concern that normal testing has not happened and be cautious
about taking it, especially for the young.
marinesfather601 Tony5SFG 5
hours ago
With the Covid19 mortality rate among the children why even vaccinate? As a Chemist /
Biochemist I learned that there is always unintended consequences.
Hilltopper9 7 hours ago
Vaccines may have long term effects that are not known
today. The same could be said of all the chemicals we apply to our body daily through shampoos,
hair dyes, body lotions, and suntan lotions. Life's a gamble. It's up to each individual to
make the best decisions possible given the facts available.
A akbushrat
Hilltopper9 6 hours ago
The CDC's generic guidelines for getting a vaccine for any reason are
very restrictive, first being, the disease you're getting vaccinated against has to pose a
real, immediate danger. CV-19 poses virtually no danger whatsoever to kids under 14. Of all the
deaths of children 14 and under in the last 18 months only .8% of them had a case of CV-19.
That's 367 deaths out of over 46,000. (Data from CDC website) Forcing them to take an
experimental vaccine that they absolutely don't need is criminal. As a parent, allowing your
child to take the vaccine without spending a few hours doing some research is criminally
negligent. This is like some terribly warped Kafka novel but it's real.
F
Fauxguy930 Hilltopper9 5 hours ago
☢️ N-butyl-N-(4-hydroxybutyl)nitrosamine is a
nitrosamine that has butyl and 4-hydroxybutyl substituents. In mice, it causes high-grade,
invasive cancers in the urinary bladder, but not in any other tissues. It has a role as a
carcinogenic agent. Ingredient in all shots. How did a carcinogen get FDA approved, oh it was
an emergency.
R RussellRika 6 hours ago
I have a
twelve year old, and not a chance I'd allow her to volunteer for any vaccine trial, and
especially not this one. She very much wanted to get a vaccine, until she started reading about
some of the adverse reactions. Sorry, but I'm a child, the benefit does not outweigh the risk.
MrEd50 6 hours ago
I took the vaccine because I'm 60 years old and work with special ed kids. My 18 year old child
refuses to take it and I support him on this. COVID shouldn't be an issue for most of us.
At an event hosted by a U.S. senator, a mother cried as she recounted how the Pfizer experimental coronavirus vaccine left her
previously healthy, active 12-year-old daughter in a wheelchair.
On Monday, Sen. Ron Johnson (R-WI) hosted a
news
conference
to discuss adverse reactions related to COVID-19 vaccines. Stephanie de Garay tearfully explained that her
12-year-old daughter, Maddie, is now wheelchair-bound after volunteering to take the Pfizer vaccine as part of the vaccine trial.
Since receiving the injection, Maddie has been to the emergency room nine times and hospitalized three times for two months.
Maddie and her parents were excited for her to participate in the vaccine trial, as they identify as "pro-vaccine and pro-science."
However, after receiving her second dose of the Pfizer vaccine on January 20, Maddie immediately experienced pain in her arm where
she had been vaccinated. Within the next 24 hours, she developed severe abdominal and chest pain.
Maddie told her mother that she felt "like my heart is being ripped out through my neck" as she experienced painful electrical
shocks down her neck and spine, forcing her to hunch over to walk.
At the instruction of the vaccine trial nurse administrator, Maddie's parents took her to the ER, where her labs were taken and she
was tested for appendicitis, given an IV with medicine, and then sent home. She was diagnosed with "adverse effect of vaccine
initial encounter."
Over the next 2 1/2 months, Maddie's mother said her abdominal, muscle, and nerve pain became unbearable. Maddie suffered from
gastroparesis, nausea and vomiting, erratic blood pressure, memory loss, brain fog, headaches, dizziness, fainting, seizures, verbal
and motor tics, menstrual cycle issues, lost feeling from the waist down, lost bowel and bladder control, and she had a nasogastric
tube placed because she lost the ability to eat.
"Why is she not back to normal? She was totally fine before this," said Stephanie de Garay, Maddie's mother. Maddie had volunteered
for the Pfizer vaccine trial "to help everyone else and they're not helping here. Before Maddie got her final dose of the vaccine,
she was healthy, got straight As, had lots of friends and had a life."
Some doctors attempted to attribute her neurological condition to anxiety and tried to send Maddie to a mental hospital. This caused
her parents to seek aid from other sources. They met others suffering from similar adverse vaccine reactions who connected them with
competent medical professionals.
"All we want is for Maddie to be seen, heard, and believed because she has not been. And we want her to get the care that she
desperately needs, so she can go back to normal," said de Garay.
LifeSiteNews has produced an extensive COVID-19 vaccines resources page.
View
it here.
play_arrow
NAV 3 hours ago
And here is one of Fauci's vaccinated - and no one cares except to suggest that this
young girl be put in a facility for mental patients...
Mother weeps as she tells senator how Pfizer shot left her daughter wheelchair-bound
'Before Maddie got her final dose of the vaccine, she was healthy, got straight As, had
lots of friends and had a life.'
https://www.lifesitenews.com/news/mother-weeps-as-she-tells-senator-how-pfizer-shot-left-her-daughter-wheelchair-bound
Realism 2 hours ago
"Maddie and her parents were excited for her to participate in the vaccine trial, as
they identify as "pro-vaccine and pro-science."
If this is true, who in the world would be excited to let their children participate in
a medical experiment, they are the problem and now her child is paying the price
Not Your Father's ZH 2 hours ago
Mom-of-3 'Excited About Getting Vaccine' Dies From Blood Clot in Brain Following
Astrazeneca Jab
She needed some excitement in her life. Now she doesn't.
Brushy 57 minutes ago
"How can Fauci claim you are at considerable risk if not vaccinated"
Its called lying.
Sparehead 1 hour ago
Considerable ~ 0.01% risk
Hipneck911 11 minutes ago
...
NSW Health - Covid PCR tests at 40 cycles, double the ...
https://cairnsnews.org/2021/06/28/nsw-health-covid-pcr-tests-at-40-cycles-double-the-recommended-rate-yielding-80-per-cent-false-positives/
← Craig Kelly MP a true Australian hero warns there could have been 50,000 deaths
from Covid vax. NSW Health - Covid PCR tests at 40 cycles , double the recommended rate
yielding 80 per cent false positives* Jun 28. Posted by Editor, cairnsnews. Letter to the
Editor.
Hipneck911 10 minutes ago
You gutless losers sure do like lying:
https://www.msn.com/en-us/health/medical/experts-us-covid-19-positivity-rate-high-due-to-too-sensitive-tests/ar-BB18wE8B
Up to 90 percent of people tested for COVID-19 in Massachusetts, New York and Nevada in
July carried barely any traces of the virus and it could be because today's tests are 'too
sensitive', experts say.
... PCR tests analyze genetic matter from the virus in cycles and today's tests
typically take 37 or 40 cycles, but experts say this is too high because it detects very
small amounts of the virus that don't pose a risk.
Experts say a reasonable cutoff for the virus would be 30 or 35 cycles, according to
Juliet Morrison, a virologist at the University of California, Riverside.
Mina said he would set the cutoff at 30.
New York's state lab Wadsworth analyzed cycle thresholds values in already processed
COVID-19 PCR tests and found in July that 794 positive tests were based on a threshold of
40 cycles.
With a cutoff of 35, about half of those tests would no longer qualify as positive.
About 70 percent would no longer be judged positive if the cycles were limited to 30.
In Massachusetts, from 85 to 90 percent of people who tested positive in July with a
cycle threshold of 40 would have been considered negative if the threshold were 30 cycles,
Mina said.
Highly recommended !This one big fraud. And Fauci is implicated. the fact that in the USA the results of the test
do not come with the number of amplifications used speaks volumes about the current medical
establishement.
Notable quotes:
"... With a cutoff of 35, about half of those tests would no longer qualify as positive. About 70 percent would no longer be judged positive if the cycles were limited to 30. ..."
"... It's just kind of mind-blowing to me that people are not recording the C.T. values from all these tests -- that they're just returning a positive or a negative,' Angela Rasmussen, a virologist at Columbia University in New York, said. ..."
Marlene Lenthang For Dailymail.com 8/30/2020
Up to 90 percent of people tested for COVID-19 in Massachusetts, New York and Nevada in July
carried barely any traces of the virus and it could be because today's tests are 'too
sensitive', experts say.
... PCR tests analyze genetic matter from the virus in cycles and today's tests typically
take 37 or 40 cycles, but experts say this is too high because it detects very small amounts of
the virus that don't pose a risk.
... ... ...
Experts say a reasonable cutoff for the virus would be 30 or 35 cycles, according to Juliet
Morrison, a virologist at the University of California, Riverside.
Mina said he would set the cutoff at 30.
New York's state lab Wadsworth analyzed cycle thresholds values in already processed
COVID-19 PCR tests and found in July that 794 positive tests were based on a threshold of 40
cycles.
With a cutoff of 35, about half of those tests would no longer qualify as positive.
About 70 percent would no longer be judged positive if the cycles were limited to 30.
In Massachusetts, from 85 to 90 percent of people who tested positive in July with a cycle
threshold of 40 would have been considered negative if the threshold were 30 cycles, Mina
said.
'I would say that none of those people should be contact-traced, not one,' he said.
The Food and Drug Administration said that it does not specify the cycle threshold ranges
used to determine who is positive and 'commercial manufacturers and laboratories set their
own.'
The Centers for Disease Control and Prevention said it is examining the use of cycle
threshold measures for 'policy decision'.
The CDC said its own calculations suggest its extremely hard to detect a live virus in a
sample above a threshold of 33 cycles.
It's just kind of mind-blowing to me that people are not recording the C.T. values from
all these tests -- that they're just returning a positive or a negative,' Angela Rasmussen, a
virologist at Columbia University in New York, said.
Authorities doe not telling truth: people who already have COVID do not need to be
vaccinated. Also if Delta varient can infect vaccineted in conserable quantities how any resobale
person can maintain this goal of "herg immunity". How it can be achieved if a vaccinated person
can be infected and thus spread the disease both amoung vaccinated cohort and among the
unvaccinated cohort. The fact the vaccinated people are infected with Delta changes the game and
here Senator Paul is wrong.
Pushing vaccination on chidren in such curcumstances changes nothing is became a very
questionable move both from scientific an from ethical perspective.
America's favourite Chinese lab funding coronavirus doomonger doctor Anthony Fauci announced
Tuesday that there are now two Americas, a vaccinated America and an unvaccinated America.
As Senator Rand Paul noted
earlier this week , there is a boat load of misinformation on the matter coming from a
government that is indiscriminately pushing vaccinations:
Rand Paul TEARS Into Senate Witness for Indiscriminately Pushing Vaccines
SexyJulian 3 hours ago
There are now two Americas. One that's retarded. And one that wants Fauci on a
lamppost.
liberty2 1 hour ago (Edited)
Note that the officials said there's no such thing as "herd immunity" last year. Now
this year they keep saying that we can reach "herd immunity" if we are 70% vaxxed! Terms
are used if it fits their narrative.
Ride_the_kali_yuga 3 hours ago (Edited)
In the Covidian Cult, there is true believers in one side and heretics on the other
side. Vaxxed and unvaxxed.
Divide and rule strategy, as always. Do not undurestimate the ratio of retarded people
among the population, it has been growing like a cancer for decades. It amazes me how
perfectly coordinated those MSM Covidian propaganda events appears worldwide.
In here France, 2 days ago, most MSM have all simultaneously gone full berserk (without
any reason) blaming the reluctant ones. One of them on TV said something like : "if it was
me, i will use police to drag those who refuse these "vaccines" from their home and force
it on them"
This was priceless, this little man has morbid obesity. We now officialy all live on the
twilight zone on steroids. Land whales dictate how people should consider their own health.
This ride seems to never end.
We now have officialy entered the dehumanization phase of the unvaxxed. The sanitary
gulag is not far from here.
NIRP-BTFD 1 hour ago
There are 2 Americas. The 0.01% (the rulers that own everything) and the serfs.
DemandSider 1 hour ago
Exactly, parasite and host. Fauci would be the former, obviously.
E5 11 hours ago remove link
Uncomfortable Truths democrats don't have in their tool kit:
1) Flu is still down 98% and would normally account for a large percentage of the covid
deaths.
2) 20% more babies were born in 1946 than in 1945. Deaths are increasing but not that
much. This is accounts for the rest of the covid deaths.
3) Coronavirus' are among the highest mutating virus types and can not be eliminated by
vaccine.
4) If the COVID symptoms arise from SARS-CoV-2 which came from bats and pangolins: then
vaccinating Humans will have zero effect in eliminating the virus.
5) COVID is a set of symptoms not a virus. The virus is called SARS. This is a
relationship like how AIDS is the symptom set that arises out of HIV. To talk about a
vaccine for COVID as a medical professional is malpractice.
6) 50% of the people getting the "delta" variant are previously vaccinated. In clinical
terms that means the vaccine experimental trial has failed.
If you still believe in mandating masks and vaccines then you are a fascist or your IQ
is too low and should give up your right to vote.
Bacon's Rebellion 9 hours ago (Edited) remove link
//////////////////////////////////////////////
June 25 th , 2021 - Public Health England
Summary:
Cases:
Overnight Hospitalization required:
Deaths:
Death rate was 9.86 times higher for the vaccinated!
IF - 53,822 "Unvaccinated" cases = 38 deaths
(Link downloads a PDF | SARS-CoV-2 variants of concern)
Public Health England
truth or go home 10 hours ago remove link
These are interesting facts. Some comments:
1. Flu deaths have been greatly exaggerated in recent years in order to push the flu
vaccine. Just like Covid, they changed the definition of flu to count more deaths, so they
could push the vaccine. Most of them are general respiratory deaths that can be/were
reclassified to Covid.
2. There was a baby boom in 1946 and that was 75 years ago, so we should start seeing an
acceleration from that about now, but there also has been massive population growth since
then, so the effect will be muted.
3. I don't claim to understand virology, but if these things mutate so fast, they likely
get less virulent rather than more. It certainly calls into question the entire vaccine
program.
4. Vaxx the bats... I thought many of them died off from their own virus a few years
ago, but I saw millions of them fly out from under a bridge in Austin a couple years
ago.
6. This is logic beyond the understanding level of the idiot media folks - they would
never be able to ask the question.
Nathan Hale PREMIUM 10 hours ago
It was a fungal infection that was/is killing bats in the US, for the record
Bacon's Rebellion 8 hours ago (Edited) remove link
Imagine the clusterphuek in the court system if these vaccines are connected with
miscarriages...lawyers are salivating...your employer coerced you into vaccination...your
baby died inside you...geesh...how anyone could take that chance!
/////////////////////////////////////////////////////////////////
Angela Merkel: All of these vaccines are conditionally approved. In the course of this
conditional approval, we are gaining experience for the first time on what happens if
this vaccine is used on millions of people? ...In the phase of the conditional approval
of such a vaccine is then very closely monitored - that is why everything is monitored so
specifically - what side effects can happen or what cases or what certain things can
occur.
Loads in German - Use Chrome to read in English:
Angela Merkel:
Sigh. 11 hours ago remove link
The Delta Strain is supposedly more fearful and deadly and contagious than the
'original' product, why, exactly?
Where are the studies comparing the relative efficacy and methodology of the vectors?
You recall the diagrams, the sneeze in one aisle of a supermarket, the blue haze covering
three aisles? Is the Delta Strain so contagious it now goes seven aisles?
Instead of the diagram of the beachgoer getting virus'd from the airborne particulates
from someone sneezing on a surfboard, are the viruses now coming in from further offshore,
the oil rig 40 miles out?
Instead of just old people, who are easily infected with everything that comes along,
now we must fear that kids and teens are susceptible? (Perhaps that's because they've worn
masks for so long they aren't getting 'natural' immunological defenses?)
This is just another worldwide scare tactic designed to keep the masks on and the
economy slowed. Look to the "Climate Change" set and the "One World Government" set for
reasons why we're facing these "new" strains.
aegis551 11 hours ago (Edited) remove link
CDC says we have nothing to worry about. Covid will never get here.
CDC says we have the ability to defeat this thing they said would never get here.
CDC says dont worry you dont need to wear masks. Because they wont protect you from the
virus.
CDC says some anti-viral medications may work. CDC corrects itself 24hrs later and says
only a vaccine can save us. Dr Fauci admits he and his family have been taking
hydroxychloroquine since the pandemic began. Even though they dont work.
CDC mandates everyone to wear masks because they will stop the spread.
CDC says we need to lock down for 2 weeks to stop the spread. CDC then mandates
lockdowns in perpetuity.
CDC says, etc, etc...
Why the hell is anyone listening to the CDC?
pods 10 hours ago remove link
Usually for any scam if you look under the cover you will find the hand of
government.
Ex. Pfizer has a vested interest of to keep their shots on the market. Profit motive and
to repay their development costs for their mRNA shots. Clinical trials are not cheap.
Pfizer will use contacts to nudge policy in a direction that benefits them. Doesnt have
to be evil, their job is to make stuff and sell it.
Why is Pfizer (could really be any of them) in this position? Because there was a
government policy to rush a product to market, Operation Warp Speed.
If that policy was never enacted none of these companies would have undertaken the
development of these shots with the resources they did. It would merely be pinheads doing
animal studies still at this point because a typical vaccine takes a decade to develop, and
mRNA has not been proven safe, so it would take longer to prove safety in target
populations, including mutagenic/teratagenic studies.
So really it was a government policy that landed us where we are at now. This is not a
political statement. No left/right BS is intended. Just a deductive theory of how the world
works, at a level above the left/right pigpen.
Brushy 10 hours ago remove link
Rand Paul didnt tweet the most important part of that study;
Delta variant deaths;
117 total deaths
44 unvaccinated
23 single dose
50 fully vaccinated
Thats 73 deaths for those who have been fully or partially vaccinated vs only 44 deaths
for the unvaxxed. Its looking more and more like the "Delta variant" is just code for
vaccine injury.
FrankDrakman 10 hours ago remove link
On the one page of data shown, I calculated the following: (rounded)
Unvaxxed: 35,000/34 deaths ~= 1/1000
One shot < 21 days: 4,000/1 deaths ~= 1/4000
One shot > 21 days: 9,000/10 deaths ~= 1/900
Two shots > 14 days: 4,000/26 deaths = 1/150
The second shot's the killer!
Morse_Code 8 hours ago
The virus is a poor excuse for the "Great Reset" into corporate fascism and to check out
the "Chicken Little" theory of the 'Sky is Falling' social syndrome.
They have already convinced society that white people are bad, men are really women, we
don't need police if they take our guns away and inflation is good, the U.S. is better
because of illegal immigration and that Biden won.
RathdrumGal 10 hours ago
I 100% agree. My career was spent in Critical Care nursing. I have seen people die and I
have seen what torture comes from a fear of death. I am much more afraid of a vancomycin
resistant enterococcus than COVID. Two days ago I was jet boating in Hell's Canyon in 117
degree heat. It was red neck heaven, no one on our boat was masked. We stopped for lunch on
the way home in a college town. So many young healthy looking people wearing masks, with
their young children masked! They can't all be on chemo, and I assume if they are that
afraid of COVID they have been vaccinated. What gives?
The key unanswered question is: what benefits for 12 years old vaccine provides. I do not see
any, while risks are real and unknown. At this point we already know that vaccine cause serious
heart problems in some vaccinated young people (say below 30 yours old)
Fauci bears some responsibility for this indent
link
Twelve year-old Maddie was enrolled in the Pfizer vaccine clinical trial. She's now in a
wheelchair, has an NG tube, and is suffering from severe memory loss, along with many other
issues.
Full video is here
nobody
I am SO sorry for this girl. She relied on her parents, their job, to protect their minor
children. They failed.
The only way I would I "consider" allowing my child to sign up to be a guinea pig in any
clinical trial is if they had a life threating incurable disease and the trial was specific to
their disease & participation was a "chance" to save their life. I worked in a clinical
trial office, you agree to being the guinea pig when you agree that you will never know if
you're injected with
What sort of parent would give their kid an untested, un-needed vaccine? There is NO excuse.
None. Zero. Mother should be in tears. 100% well deserved.
Deplored
" in healthcare" means nothing anymore. I've been in healthcare for 25 years and it blows my
mind how many 500,000$ plus educations lined up for the "vax" AND do not know the simple
definition of a vaccine. I watched 1st hand as practically overnight medicine went from being
science based to political weapon. We used to have to have an evidence based system where
doctors would look at the published studies and make decisions based on the best info
available. That's all gone now. You can't even trust the medical journals anymore that at one
time were the pinnacles of scientific medical discovery. The hospital I've worked in for 25
years is going to mandate the vax as soon as the FDA approves it,which means I'm out. 15% of us
are unvaxed and they have plans to get rid of us. The medical tyranny STARTED w the mandating
of the flu shot years ago for HC workers and now it's covid. It's not going to end ,just wait
til the next shit show released on us. Next time they will have the ballz to say ur locked in
ur home until u comply. Then when u can't pay ur property taxes because u cant leave the house
to work u find out who actually owns ur home. Peetoonya
The US "Healthcare" INDUSTRY ranks 37th in the world. John Hopkins put out a report that the
3rd leading cause of death is going to your doctor and doing what he/she says! I remember in
the 90's they ran off or bought out most of the private practices especially in the rural areas
with malpractice claims if they didn't sell out. But these days you can make up to $50,000 a
year just sending people the bill for your inflicted genocide. Medical Billing Specialist
Salary in the United States https://www.salary.com/research/salary/benchmark/medical-billing-specialist-salary
All the cowardly doctors will do as they are told for fear of losing their license. PS The
profession that has the highest rate of suicide is Doctors! I haven't been to a doctor in 21
years. Riseliberty
This is not a vaccine. Do you understand? It is experimental gene therapy. You cannot
compare this with any FDA approved vaccine you've had in the past. Hehe62
Before watching one clip I suggest you watch the entire press conference. ALL of the
participants explained they are pro science and pro vaccine up front.
As an NP who has been thrust into covid from the get go I now daily see covid 19 vaccine
injuries albeit less than those suffered from these victims; depending on how you see it.
Type 1 diabetes in a perfectly healthy 16 year old athletic boy with healthy family members
now requiring insulin for the rest of his life-happened right after 2nd pfizer. Tons of
shingles and herpes viruses, and regular colds that have taken out staff members for 3-4 weeks
versus 2-3 days in the past.
As an NP that started in the military and has all vaccines and vaccinated all my children
and seeing and living in the medical community throughout this I personally will NEVER get
another vaccine the government suggests or requires ever again. I will NEVER go see a
mainstream medical provider ever again unless I'm taken against my will or knowledge.
Sure, tons of people have gotten the vax without issue, but YOU are the phase III clinical
trial for this thing, it has only been about 6 months. Long term effects who knows. I have a
feeling it isn't going to get better. And the fact that these people have been completely
silenced, questioned, and "debunked" by mainstream media and the public as a whole that
suddenly seems to have 100% confidence in their government???? is EXTREMELY concerning. Ron
God bless Maddie and her family. For context, I'd like to know how many children have had
the Pfizer vaccine without serious side effects. We shouldn't fall into the left wing tactics
of using anecdotal emotional cases to distort reality to make a larger point. The fact is that
vaccines have saved millions of lives and prevented millions of crippling side effects from
polio, smallpox, yellow fever, mumps, measles, hepatitis, HPV . Regretfully, some of the
vaccinated have suffered side effects, but the benefit greatly outweighs the risk.
JedWSmith
For perspective, this "vaccine" has caused more deaths than all the other vaccines given
over the last century. Maybe caution is warranted. This little child had an almost ZERO chance
of any complications from the China virus. There's ZERO reason for someone who's had the China
virus and recovered, having natural antibodies, to get the vaccine. The therapeutics work. They
were demonized only because a sitting president, hated by the fake media, big pharma, and the
DC deep state, promoted them. Dillard
Offering up your child for experiments, was it for $$$$$$$?
Remember the Canadian govt with pop up vaccination sites offering children ice cream if they
got the jab, and they did it WITHOUT PARENTS CONSENT? Think about that one. The govt rolls up
and opens a vaccine tent near your home, your child sees FREE ICE CREAM and goes to get free
ice cream and gets injected without your knowledge. That is some real evil there. William
Walker
I'm terribly sorry for the young girl, but I'm inflamed with anger that the stupid parents
put not one, but THREE children through clinical trials giving them the vaccine–all the
while touting the science (oh, the science!) which completely contradicts the claims that young
people are in any way threatened by Covid as a demographic. This is tragic, this is moronic
liberalism, and this is a direct result of the parents swilling all the false idiocy from CNN
and MSNBC without questioning the actual empirical data and science. PALydia
"Trials" are done to determine outcome. The word "trial" is synonymous with the word
"experiment." I.e. you are playing Russian Roulette when you enroll your child in ANY trial.
That IS science. You should NEVER assume something is safe and harmless when it is still in
"trial" phase .never mind these vaccines bypassed animal trials and all previous mRNA vaccines
failed animal trials. My heart breaks for this child but it's criminal for any parent to
subject their child to this. LiberalsRPinworms
Was waiting for the "but we still think you should vaccinate your kids too "
I find it interesting that all these cult members keep saying they're pro science. However,
scientific experiments are based on hypotheses, not already known facts. Why is she upset? Her
kid wanted to provide data to this experiment and did just that. Too bad she wasn't an outlier
considering, if she were, she could probably still eat food on her own. Thanks for your
contribution to the science folks! navi282
I am very sorry about what has happened to Maddie, but the responsibility lies with the
parents who believe in the false religion of "scientism" and have opted into the con-game that
vaccinations are genuine healing methodologies. As an engineer Maddie's mother should have
studied logic and the philosophy of science and then discerned that the politicization of the
medical field in recent years created confirmation bias, poor SPC (statistical process
control), and question-begging fallacies from those who should have known better. Complicity or
Ignorance -- take your pick. Matt Walters
Being pro-science means you base decisions on data. There is not yet a data set for the
short and long-term risks, benefits, and side effects of this vaccine that would allow a
science-based decision to take it or not. Those who are pro science wait for reliable data
before considering taking an experimental vaccine that is not approved by the FDA. constitution
rules
For USA children ages 5 to 18:
I notice a common trend among these child abuser parents .they go online to complain how
their kids were maimed by the experimental mRNA, but then they always have to preface it by
saying "oh but we're pro vaccine and pro science"
Well, I am anti-vaccine and I'm anti-mRNA. Have some conviction you retard. No wonder you
find yourselves in the position you're in.
I sincerely feel bad for your kids. You stole their lives from them and they will never be
the same and while the fallen man part of me wants to say "just deserts", the Catholic part of
me prays the rosary for you and your kids every single night. solome
' .we are pro-vaccine and pro-science'
.these parents make a great case that academia does not necessarily convey common sense it
can convey a buttload of chutzpah ..we know that because Washington DC is full of it excessive
hubris, too and, in turn, they can make decisions that prove disastrous for the future of We
the People Christina
This is a terrible tragedy for this family. I hope this beautiful young girl will eventualy
recover fully. I hope her parents will recover as well.
As for her parents, however, who are obviously very intelligent, did they miss the reams and
reams of scientific studies, white papers, and patent applications available to the public
before they permitted their child to get this not yet approved, experimental gene therapy
injection?
Did they not watch the hours and hours of video interviews and presentations by doctors,
virologists, epidemiologists, etc., who warned, warned, warned us to NOT TAKE IT?
Even after big tech started censoring and scrubbing most of this information off the net and
everywhere else, even before the massive pro-vax propaganda machine cranked up, millions of
people informed themselves about what it really is and thus decided to not be part of the human
trials.
Most of us had our flu shots and regular real vaccines as well, real vaccines are not the
issue, here.
I'm really sorry to tell you this, Mom, but you either ignored the real science or you, too,
were caught up in the propaganda that caused so many people to automatically reject any thing
people on the other side of the debate had to say.
One more red flag when it comes to politics and propaganda: DID YOU NOT QUESTION WHY SO MANY
MEDICAL PROFESSIONALS WHO TRIED TO WARN US HAD THEIR INFORMATION SCRUBBED, CENSORED, LOST THEIR
JOBS, AND RECEIVED DEATH THREATS SIMPLY FOR DOING DUE DILIGENCE AND ENGAGING IN THE ALWAYS
REQUIRED DEBATES AMONG MEDICAL PROFESSIONALS BEFORE APPROVING VACCINES? AND THEN WARNING THE
PUBLIC BEFORE THE POLITIAL CAMPAIGN BEGAN.
This is a very, very sad day in America. It's a very, very sad day for this family.
But maybe other parents will think twice, now, before they sign their children up for
potentailly horrific experiences related to the gene therapy injections. Maria
So sad. I feel sorry for the girl. But parents are volunteering much young children.
https://www.msn.com/en-us/health/medical/3-siblings-get-pfizers-covid-19-vaccine-as-part-of-global-trials-in-young-children/ar-AALjHd5
President Donald J. Trumper
"Twelve year-old Maddie was enrolled in the Pfizer vaccine clinical trial."
The complete blame belongs on the parents. The tearful mother, an electrical engineer, said
she and her husband were pro-vaccine. If they were so smart, why in the hell would they enroll
their CHILD in a clinical trial for a fast-tracked vaccine, especially when children are not in
a high-risk group, and Covid-19 survival is 99.8 percent? I am furious with these highly
educated people. THEY WERE DUMBER THAN DOORKNOBS TO SACRIFICE THAT GIRL TO THE
GOVERNMENT/PHARMA COMPLEX. Libby ChickenLittle
When I was a 12 year old girl, I didn't even know what a clinical trial was. But then again,
I grew up at time when kids were allowed to be just kids and not political pawns by their
brainwashed parents. Sorry mom – I know comments are going to be harsh – but you
deserve EVERY SINGLE ONE OF THEM. smith. jane smith.
Q. How does a government make a pro-vaccine person turn into an anti-vaccine person?
A. Give them a vaccine that makes them sicker than they were before they got the vaccine,
sicker with the very thing the vaccine was supposed to prevent.
I was told to go get a flu shot by my commander. Being a good USAF airman, I did so. I was
just a kid following orders. Two days later I was in the hospital, so sick with the flu until I
could not take 4 steps without getting so dizzy that I had to stop moving to keep from throwing
up. And it took 5 days before I was able to walk down a hallway without getting dizzy!
That was the last time I ever had a flu shot. Or the flu.
And that was over 35 years ago.
If the vaccine is such a good idea, then why does everybody have to get it in order for it
to work?
How about those who get the vaccine just leave those alone who choose not to get it?
And after what has happened to this lady's kid(s) .
Why the heck is she still PRO‐vaccine ????
I blame the Fauci, Government, and the MSM for brainwashing fear amongst the masses. If you
are repeatedly gaslighted about almost every issue, you begin to believe the lies. You can add
schools also as they indoctrinate instead of teaching critical thinking.
The US Food and Drug Administration added a warning about the risk of myocarditis and
pericarditis to fact sheets for Moderna and Pfizer-BioNTech Covid-19 vaccines Friday.
The warning notes that reports of adverse events following vaccination -- particularly after
the second dose -- suggest increased risks of both types of heart inflammation.
Earlier this week, vaccine advisers to the US Centers for Disease Control and Prevention
heard that the agency had received about 1,200 reports of such heart inflammation after 300
million doses of the two vaccines had been given.
"Patients who had had COVID-19 within the past year and people vaccinated with two doses of
Pfizer retained enough antibodies to be protected against the Indian variant, but three to six
times less antibodies than against the UK variant, Schwartz said. The study shows that "this
variant.. has acquired partial resistance to antibodies," Schwartz said." Pfizer jab
less effective, still protects against Indian strain- study
in people who had been fully vaccinated with two doses of the Pfizer-BioNTech vaccine,
levels of neutralising antibodies were more than five times lower against the B.1.617.2 variant
when compared to the original strain, upon which current vaccines are based.
Importantly, this antibody response was even lower in people who had only received one dose.
After a single dose of Pfizer-BioNTech, 79% of people had a quantifiable neutralising antibody
response against the original strain, but this fell to 50% for B.1.1.7, 32% for B.1.617.2 and
25% for B.1.351.
While antibody
levels decreased with age against all variants, no correlation was observed for sex or
BMI.
More recently, there has been a Delta outbreak at the Foothills Medical Centre in Calgary,
with 16 patients and six staff infected. The majority experienced mild symptoms, though one
required treatment in the intensive care unit. Of the 22, 11 had been fully vaccinated, while
seven had one dose; all were given an mRNA vaccine, communications director Kerry Williamson of
Alberta Health Services told Maclean's . (The province did not disclose whether the one
admitted to ICU had been vaccinated.)
An outbreak of the Delta variant of COVID-19 in Israel has spread to some vaccinated people
-- with about half of the adults infected fully inoculated with the Pfizer shot, a health
official said.
The Delta variant or the B.1.617.2 was first identified in India during late 2020 and is now prevalent in more than 70 countries
across the world.
An outbreak of the Delta variant of COVID-19 in Israel has spread to some vaccinated people -- with about half of the adults infected
fully inoculated with the Pfizer shot, a health official said.
Ran Balicer, who heads a COVID-19 government advisory committee, said that about 90 percent of new infections in the country were
likely caused by the Delta variant, a highly-contagious strain that first emerged in India,
the
Wall Street Journal reported
.
"The entrance of the Delta variant has changed the transmission dynamics," Balicer said.
Children under the age of 16 -- the majority of whom had not received the vaccine -- were responsible for about half of the new cases,
Balicer said.
But about half of adults infected in the outbreak were considered fully-vaccinated -- meaning that it had been at least two weeks
since they received their final dose of the Pfizer shot, he said.
Balicer added that the so-called breakthrough cases were expected because though Pfizer is highly effective against the virus, it's
not 100 percent protective.
Israelis
wear protectives against COVID-19 at a shopping mall in Jerusalem on June 25, 2021.
EMMANUEL
DUNAND/AFP via Getty Images
The spread of the Delta variant comes as daily cases rose to 200 on Thursday from around 10 a day for most of June, the Wall Street
Journal reported.
Though the outbreak is small by global standards, it has prompted the government to reimpose indoor mask mandates, the newspaper
reported.
Health officials in the US have warned that the Delta variant will soon become the dominate strain of COVID-19.
But evidence has shown that the vaccine will prevent severe cases of the bug, as well as hospitalizations.
"Right now, in the United States, [Delta accounts for] about 10 percent of infections. It's
doubling every two weeks," Scott Gottlieb, former commissioner of the Food and Drug
Administration, said Sunday on
Face the Nation . "So it's probably going to become the dominant strain here in the
United States. That doesn't mean that we're going to see a sharp uptick in infections, but it
does mean that this is going to take over. And I think the risk is really to the fall -- that
this could spike a new epidemic heading into the fall."
Adding to the worry is new data that suggests Delta may also cause more severe disease -- in
addition to spreading to more people. Early findings out of Scotland suggest infections with
the Delta variant were associated with nearly double the risk of infected persons ending up
hospitalized compared to infections with the Alpha variant. The data was published
Monday as Correspondence in the Lancet . Experts say they'll need more data to confirm that
risk.
The bright side
The good news in all of this is that being fully vaccinated appears to protect against
Delta. At the end of May, researchers at Public Health England posted data (which had not been
peer-reviewed) indicating that two doses of the Pfizer-BioNTech vaccine were 88 percent
effective at preventing a symptomatic infection with the Delta variant . Meanwhile, the
data said, two doses of the Oxford-AstraZeneca vaccine were 60 percent effective. (Notably,
just one shot of either vaccine was not protective, offering only 33 percent efficacy
against symptomatic Delta infections. Experts emphasized the importance of not skipping the
second dose.)
Data out
of Scotland Monday likewise suggested that two doses of the Pfizer-BioNTech vaccine were 79
percent effective against the Delta variant, while two doses of Oxford-AstraZeneca vaccine were
again 60 percent effective.
Also on Monday, PHE released another analysis (also not peer-reviewed) that finds that two
doses of the Pfizer-BioNTech vaccine were
96 percent effective against hospitalization and two doses of the Oxford-AstraZeneca
vaccine were 92 percent effective against hospitalization.
"So we have the tools to control this and defeat it," Gottlieb noted.
Looming risk
But experts are still concerned. The pace of vaccination has slowed significantly in the US,
and many states -- particularly in the South -- are far behind the goal of getting 70 percent
of adults at least one vaccine. Pockets of low vaccination are fueling fears among experts,
including Gottlieb, that cases could once again spike as Delta continues its spread.
Peter Hotez, director of the Texas Children's Hospital Center for Vaccine Development,
echoed that concern Tuesday. He told CNN that he is " extremely
worried " about the Delta variant. He emphasized that right now is "crunch time" to get
fully vaccinated -- which takes five to six weeks -- before Delta spreads further.
In a press briefing last week, top infectious disease expert Anthony Fauci made a similar
plea, pointing to the rapid spread of the Delta variant in the UK. "
We cannot let that happen in the United States ," he said. This "is such a powerful
argument... to get vaccinated."
This is a fiasco for Fauci "herd immunity" campaign and the US goverment official strategy --
full, if necessary compulsive, vaccination of population with the first generation of vaccines.
It means that people vaccinated with the the first generation vaccines can become infected with
Delta variant and spread the virus much like unvaccinated people.
An Israeli receives a coronavirus vaccine in Tel Aviv, Israel, on January 6. Sebastian
Scheiner/AP As many as half of new COVID-19 cases in Israel are vaccinated people, a health
official suggested. The Delta variant, not as easily beaten by vaccines as other variants, is
driving Israel's surge. The figure is likely an estimate, as the health ministry is still
analyzing the cases. As Israel faces a surge in cases driven by the Delta variant, its health
officials suggested that as many as half of new cases were among people who'd been
vaccinated.
Fully vaccinated people who've come into contact with the Delta variant have no immunity and
have to quarantine, Chezy Levy, the director-general of Israel's health ministry, said on
Wednesday, Haaretz reported. Levy told the state broadcaster Kan Bet that about 40% to 50% of
new cases appeared to be people who had been vaccinated, Haaretz reported.
He did not appear to specify a time frame for the new cases. The figure is likely an
estimate, as the ministry is still analyzing the cases. On Monday, Levy said that a third of
the new daily cases were people who had been vaccinated.
Highly recommended !This is a fiasco for Fauci "herd immunity" campaign. It means that vaccinated people can
become infected and spread the virus much like unvaccinated people.
Cases of the Delta variant of coronavirus have almost doubled in a week
with 73 people now confirmed to have died after testing positive for the variant, 26 of whom
had had both vaccine doses.
Public Health England (PHE) said that as of Monday, the UK has seen 75,953 confirmed cases
of the Delta variant first identified in India, up 33,630 - or 79% - from the previous
week.
While just 26 people died more than two weeks after their second COVID-19 vaccine dose from
the Delta variant, more than 30.6 million in the UK have had both jabs, according to the
latest
government figures .
PHE said a total of 806 people in England have been admitted to hospital with the Delta
variant as of 14 June, a rise of 423 on the previous week.
So we have real problems with vaccines as Delta mutation puts the end of Fauci and company
fake dream about herd immunity -- it infects vaccinated people, but we can't discuss that the US medical establishment is corrupt,
in bed with Big Pharma and failed us.
This "medical bolshevism" should better be stopped.
Notable quotes:
"... Johnson said Sheryl Ruettgers will detail "severe neurological reactions that still inhibit her ability to live a normal life, including muscle pain, numbness, weakness and paresthesia" that she experienced after getting the COVID-19 vaccine earlier this month. ..."
Wisconsin Republican Senator Ron Johnson announced plans to hold a news conference to
discuss adverse reactions related to the COVID-19 vaccine, drawing backlash from health care
experts who view the move as "dangerous" and a way to promote misinformation.
© Anna Moneymaker/Getty Images U.S. Sen. Ron Johnson (R-WI) is facing backlash after he
announced plans to hold a news conference to discuss the negative effects of the COVID-19
vaccine. Here, Johnson listens during a hearing in the Senate Homeland Security and
Governmental Affairs Committee on June 22, 2021 in Washington, DC.
In a statement Friday, Johnson said he plans to give a platform to six people from across
the country who claim to have had negative health reactions after receiving the coronavirus
jab. Johnson said the conference will take place Monday to allow the individuals to tell their
stories and discuss issues that have been "repeatedly ignored" by the medical community,
according to the Milwaukee Journal Sentinel.
The Republican senator, who has been a vocal critic of vaccine mandates and has previously
advocated for alternative and unproven drug treatments to COVID-19, faced immediate backlash
from critics who feel the event will be a platform for spreading misinformation about the
safety of vaccines.
Dr. Jeff Huebner, a doctor in Madison, Wisconsin, said that Johnson was "promoting dangerous
and unfounded claims" about the vaccine that contradict medical research and analysis.
"As a member of the Wisconsin medical community I'm gravely concerned about the impact his
event and remarks will have on our ability to return to normal and protect Wisconsinites from
COVID-19.," Huebner said in a statement, the Journal Sentinel reported .
Joanna Bisgrove, a Wisconsin primary care doctor, told FOX6 that Johnson's statements and
event are "putting people at risk and already hurting people."
Tony Evers, the state's Democratic governor, added Friday that Johnson was being "reckless
and irresponsible" and said the event was "jeopardizing the health and safety" of the state's
vaccine rollout and economic recovery.
.@SenRonJohnson, you're being reckless and irresponsible. The #COVID19 vaccine is safe and
effective and based on years of science and research. Every time you suggest otherwise,
you're jeopardizing the health and safety of the people of our state and our economic
recovery.
-- Governor Tony Evers (@GovEvers) June 25, 2021
In defense, Johnson said Friday that he is "just asking questions" and isn't against the
vaccine.
"We're all supporters of vaccines. As I've repeatedly said, I'm glad that hundreds of
millions of Americans have been vaccinated, but I don't think authorities can ignore and censor
some of the issues," Johnson said in a tweet responding to Evers. "On Monday, we'll bring light
to stories that deserve to be seen, heard & believed."
Monday's event in Milwaukee will include statements from former Green Bay Packers player Ken
Ruettgers and his wife, Sheryl.
Johnson said Sheryl Ruettgers will detail "severe neurological reactions that still inhibit
her ability to live a normal life, including muscle pain, numbness, weakness and paresthesia"
that she experienced after getting the COVID-19 vaccine earlier this month.
Additional testimonies will be heard from individuals from Ohio, Missouri, Utah, Michigan
and Tennessee.
The medical community has long stressed that the benefits of the COVID-19 vaccine far
outweigh the risks of possible side effects. Earlier this week, top U.S. health officials, medical agencies, laboratory and hospital
associations issued a statement reiterating the benefits by stating that getting vaccinated is
the "best way to protect yourself, your loved ones, your community, and to return to a more
normal lifestyle safely and quickly."
Newsweek contacted Johnson for additional comment, but did not hear back in time for
publication.
Newsweek, in partnership with NewsGuard, is dedicated to providing accurate and
verifiable vaccine and health information. With NewsGuard's HealthGuard browser extension,
users can verify if a website is a trustworthy source of health information. Visit the Newsweek
VaxFacts website to learn more and to download the HealthGuard browser extension.
Related Articles
Start your unlimited Newsweek trial
How the Pfizer-BioNTech Vaccine Works
By Jonathan Corum
and Carl Zimmer Updated
May 7, 2021 Leer en
español
The German company BioNTech
partnered with Pfizer to develop and test a coronavirus
vaccine known as BNT162b2 , the generic name tozinameran or the brand name Comirnaty . A
clinical trial demonstrated that the vaccine has an efficacy rate
of
over 90 percent in preventing Covid-19.
Producing a batch of the
Pfizer-BioNTech vaccine currently takes 60 days.
A Piece of the Coronavirus
The SARS-CoV-2 virus is studded with
proteins that it uses to enter human cells. These so-called spike proteins make a tempting
target for potential vaccines
and treatments
.
Spikes
Spike
protein
gene
CORONAVIRUS
Like the Moderna
vaccine , the Pfizer-BioNTech vaccine is based on the virus's
genetic instructions for building the spike protein.
mRNA Inside an Oily Shell
The vaccine uses messenger RNA, genetic material that our cells read to make proteins. The
molecule" called mRNA for short "" is fragile and would be chopped to pieces by our natural
enzymes if it were injected directly into the body. To protect their vaccine, Pfizer and
BioNTech wrap the mRNA in oily bubbles made of lipid nanoparticles.
Lipid nanoparticles
surrounding mRNA
Because of their fragility, the mRNA molecules will quickly fall apart at room temperature.
Pfizer is building special containers with dry ice, thermal sensors and GPS trackers to ensure
the vaccines can be transported at ""94°F (""70°C) to stay
viable.
Entering a Cell
After injection, the vaccine particles bump into cells and fuse to them, releasing mRNA. The
cell's molecules read its sequence and build spike proteins. The mRNA from the vaccine is
eventually destroyed by the cell, leaving no permanent trace.
VACCINE
PARTICLES
VACCINATED
CELL
Spike
protein
mRNA
Translating mRNA
Three spike
proteins combine
Spike
Cell
nucleus
Spikes
and protein
fragments
Displaying
spike protein
fragments
Protruding
spikes
Some of the spike proteins form spikes that migrate to the surface of the cell and stick out
their tips. The vaccinated cells also break up some of the proteins into fragments, which they
present on their surface. These protruding spikes and spike protein fragments can then be
recognized by the immune system.
Spotting the Intruder
When a vaccinated cell dies, the debris will contain many spike proteins and protein
fragments, which can then be taken up by a type of immune cell called an antigen-presenting
cell.
Debris from
a dead cell
Engulfing
a spike
ANTIGEN-
PRESENTING
CELL
Digesting
the proteins
Presenting a
spike protein
fragment
HELPER
T CELL
The cell presents fragments of the spike protein on its surface. When other cells called
helper T cells detect these fragments, the helper T cells can raise the alarm and help marshal
other immune cells to fight the infection.
Making Antibodies
Other immune cells, called B cells, may bump into the coronavirus spikes on the surface of
vaccinated cells, or free-floating spike protein fragments. A few of the B cells may be able to
lock onto the spike proteins. If these B cells are then activated by helper T cells, they will
start to proliferate and pour out antibodies that target the spike protein.
HELPER
T CELL
Activating
the B cell
Matching
surface proteins
VACCINATED
CELL
B CELL
SECRETED
ANTIBODIES Stopping the Virus
The antibodies can latch onto coronavirus spikes, mark the virus for destruction and prevent
infection by blocking the spikes from attaching to other cells.
ANTIBODIES
VIRUS Killing Infected Cells
The antigen-presenting cells can also activate another type of immune cell called a killer T
cell to seek out and destroy any
coronavirus-infected cells that display the spike protein fragments on their
surfaces.
ANTIGEN-
PRESENTING
CELL
Presenting a
spike protein
fragment
ACTIVATED
KILLER
T CELL
INFECTED
CELL
Beginning
to kill the
infected cell Remembering the Virus
The Pfizer-BioNTech vaccine requires two injections, given 21 days apart, to prime the
immune system well enough to fight off the coronavirus. But because the vaccine is so new,
researchers don't know how long its protection might last.
First dose
0.3ml
Second dose
21 days later
A preliminary study found that the vaccine seems to offer strong protection about 10
days after the first dose , compared with people taking a placebo:
Cumulative incidence of Covid-19
among clinical trial participants
2.5%
2.0
People taking
a placebo
1.5
1.0
Second
dose
First
dose
People taking the
Pfizer-BioNTech vaccine
0.5
0
1
2
3
4
8
12
16
Weeks after the first dose
It's possible that in the months after vaccination, the number of antibodies and killer T
cells will drop. But the immune system also contains special cells called memory B cells and
memory T cells that might retain information about the coronavirus for years or even
decades.
For more about the vaccine, see Pfizer's Covid Vaccine: 11 Things
You Need to Know .
Preparation and Injection
Each vial of the vaccine contains 5 doses of 0.3 milliliters. The vaccine must be thawed
before injection and diluted with saline. After dilution the vial must be used within six
hours.
Vaccine Timeline
January, 2020 BioNTech begins work on a
vaccine after Dr. Ugur Sahin, one of the company's founders, becomes convinced that the
coronavirus will spread from China into a pandemic.
March BioNTech and Pfizer agree to collaborate.
May The companies launch a Phase
1/2 trial on two versions of a mRNA vaccine. One version, known as BNT162b2, had fewer side
effects.
July 22 The Trump administration awards a
$1.9 billion contract for 100 million doses to be delivered by December, with an option to
acquire 500 million more doses, if the vaccine is authorized by the Food and Drug
Administration.
July 27 The companies launch a Phase 2/3
trial with 30,000 volunteers in the United States and other countries, including Argentina,
Brazil and Germany.
Sept. 12 Pfizer and BioNTech
announce they will seek to expand their U.S. trial to 44,000 participants.
Nov. 9 Preliminary data indicates the Pfizer vaccine is over 90
percent effective , with no serious side effects. The final data from the trial shows the
efficacy rate is 95 percent.
Nov. 20 Pfizer requests an emergency use
authorization from the F.D.A.
Dec. 2 Britain gives emergency
authorization to Pfizer and BioNTech's vaccine, becoming the first Western country to give
such an approval to a coronavirus vaccine.
Dec. 8 William
Shakespeare , age 81, is among the first people to receive a shot of the vaccine in
Britain, on the first day of vaccinations for at-risk health care workers and people over
80.
Dec. 9 Canada
authorizes the Pfizer-BioNTech vaccine.
Dec. 10 Saudi Arabia approves the
vaccine.
Dec. 11 The F.D.A. grants Pfizer-BioNTech vaccine the first emergency use
authorization for a coronavirus vaccine in the United States.
Mexico also approves the vaccine for emergency use.
Dec. 14
Vaccination begins in the United States.
Dec. 21 The European Union
authorizes the vaccine.
Dec. 31 Pfizer expects to produce up to
50 million doses by the end of the year, and up to 1.3 billion doses in 2021. Each
vaccinated person will require two doses.
January, 2021 Scientists grow concerned about the
emergence of fast-spreading variants that might be able to evade antibodies. Tests on
a variant
called P.1 , first identified in Brazil, show that Comirnaty
will likely work against it as well . However, researchers find that antibodies produced by
Comirnaty are somewhat
less effective against another variant called B.1.351
, first identified in South Africa.
Feb. 15 Pfizer and BioNTech register a trial specifically for
pregnant women.
Feb. 26 The companies
announce a study to develop a B.1.351-specific booster.
April 16 Pfizer says their vaccine may require a third dose within a
year of the initial inoculation, followed by annual vaccinations.
April 20 Some vaccinated people are professing loyalty to the
brand they happened to have received.
April 25 Nearly 8 percent of Americans who got initial Pfizer or Moderna shots have
missed their
second doses .
April 28 Pfizer has delivered more than 150 million
doses of the vaccine to the United States, and expects to double that number by
mid-July.
May 7 Pfizer and BioNTech apply
for full approval from the U.S. Food and Drug Administration.
Tracking t
In the USA Indian mutation probably will be dominant in a month or two.
The comments were made on Sky News by Special Envoy on Covid for the World Health
Organisation (WHO). Dr David Nabarro.
Nabarro suggested that there would be a long list of mutations of the Indian variant which
would in some cases evade the protection offered by vaccines.
"We will go from Delta to Lambda and then on to the other Greek letters, that's inevitable,
and some of these variants will be troublesome," he said.
"I'm basically saying variants are going to go on coming. That's part of life, we need to
pick them up fast, we need to move quickly if we see them in a certain location, we need to
build the management of variants into what we call our Covid-ready strategy, which is going to
be the pattern for the foreseeable future," he added.
According to Nabarro, mask mandates and social distancing need to remain in place for the
foreseeable future "as part of our defence" against COVID , particularly in regions which have
high infection rates.
y_arrow
Roacheforque 2 hours ago
[For those who already had Covid-19] the variants are a nothing burger according to Dr.
Yeadon, who is censored and cancelled , just like ivermectin and HCQ.
Crimes against humanity.
trailer park boys 1 hour ago
I was going to bring up Dr. Mike Yeadon also. As the former VP and respiratory research
head globally for Pfizer, he has the knowledge to call Bullshiit! on this variant crap. He
was on The Highwire a week or so ago and it is the best hour and a half to clue you in on
the Covid scam that you'll ever see.
https://thehighwire.com/videos/pfizer-vp-the-thing-to-be-terrified-of-is-your-government/
BLOTTO 1 hour ago
' the idea of mutations of SARS-CoV-2 is based only on an interpretation of the fact
that all DNA is constantly changing. Or more generally formulated, the idea of the virus
mutation arises only because one still works with completely outdated, long since disproved
scientific hypotheses.
https://projekt-immanuel.de/en/entry-the-virus-mutation/
keeper20 19 seconds ago
Confidential Documents reveal Moderna sent mRNA Coronavirus Vaccine Candidate to
University Researchers weeks before emergence of Covid-19
https://truth11.com/2021/06/22/confidential-documents-reveal-moderna-sent-mrna-coronavirus-vaccine-candidate-to-university-researchers-weeks-before-emergence-of-covid-19/
Confidential Documents reveal Moderna sent mRNA Coronavirus Vaccine Candidate to
University Researchers weeks before emergence of Covid-19
Tap News / Weaver
U.S. Gov't Sent "mRNA Coronavirus Vaccine Candidates" to University Researchers WEEKS
BEFORE "COVID" Outbreak in China
Virgil Krenshaw PREMIUM 2 hours ago remove link
AKA the plan from the beginning.
Permanent lockdown is one way to keep the people from rising up. Or it might cause them
to rise up. Flip a coin, oligarchs. You feel lucky?
HRH of Aquitaine 2.0 2 hours ago
The twisted part is the dumb people that are followers are the ones getting vaxxed and
wearing a mask. Both of which have serious health implications. Oh well. Not my problem if
the dumb ones, as usual, win the Darwin Award.
williambanzai7 PREMIUM 2 hours ago
Your papers please
Rectify77 PREMIUM 2 hours ago
Total mind control. Fear only works until people realize that the bogeyvirus isn't
really dangerous to the 99.8%. Wake up people!
pods 1 hour ago remove link
This guy [who advocates social distancing] needs to be ventilated. You know how many
people will die from lack of socialization? More than from the boogeyman virus.
These psychopaths need to be removed from society. We've lived and died for a long time
with communicable diseases. We aren't going dystopia cyborg life now.
Nope, "2 ropes to stretch his neck".
hegger 2 hours ago (Edited)
The WHO lost its scientific relevance and whatever psychological authority it had left
when it changed its version of "herd immunity" such that herd immunity could now only be
possible through vaccines. (I'm too lazy to provide a link, but look it up; it
happened.)
The WHO and its scientists have betrayed the light of logos for the short-term dopamine
hits provided by power and money. They are quite literally a net negative to the human
species and, hopefully, history will prepare an appropriately excruciating conclusion of
their miserable lives.
GeezerGeek 1 hour ago
I suspect that the narrowly targeted mRNA jabs do a really poor job of developing herd
immunity. They only potentially address one of the many ways -> our immune systems
normally work. Or so I've read.
But what do I know? I'm not a doctor and it's been decades since I last "played doctor"
with anyone.
SuperareDolo 2 hours ago (Edited)
SARS is only 80% identical to Covid, versus 99.99% identical for these stupid variants.
Survivors of SARS have robust T-cell immunity today, including against Covid, 17 years
after having the disease. Antibodies don't do the heavy lifting against viruses, and
surface antigens like spike protein are often not the principal immune targets. So useless
vaccines might indeed allow endless variants to spread. But all those people who've had the
virus now have the gold standard of immunity, and don't need to give another thought to
it.
KittyAW 2 hours ago remove link
The Earth is inundated w/ viruses, bacteria, fungi & other microorganisms. They are
everywhere; the air, soil, oceans - THIS is the environment in which humans evolved. Those
whose immune systems were inadequate early on, died early on; those whose immune systems
degenerated died later.
In the more recent centuries sanitation & improved diets have enabled very many to
overcome infections who would have died in centuries past. Far more recently tho, many ppl
have ruined their immune systems via life-style practices, among them poor eating habits
leading to obesity. Those who have kept themselves truly healthy - or regained good health
- which always includes a strong immune system, should not be penalized (nor penalized
themselves) bc of the many who have let themselves become immune-wise dysfunctional.
These new "variants" are not much different from the original & the prevention
measures of serious illness are the same. But this WHO "Special Envoy on Covid" is NOT
going to say that. The financial backing from the likes of Bill Gates is all promulgated on
Pushing "Vaccines", even tho they will have little to no diminishing effect on anything but
general health over the next few years as data is likely to show..... But a diminished
population is exactly what certain parties want.
trailer park boys 2 hours ago
Dr. Mike Yeadon has given the most insightful explanation of all the nefarious goings on
this past year plus. As the former VP and respiratory research head globally for Pfizer, he
has the knowledge to call Bullshiit! on this variant crap. He was on The Highwire a week or
so ago and it is the best hour and a half to clue you in on the Covid scam that you'll ever
see.
https://thehighwire.com/videos/pfizer-vp-the-thing-to-be-terrified-of-is-your-government/
YouThePeople 2 hours ago
The WHO...We Won't Get Fooled Again!
Able Ape 2 hours ago (Edited)
I think he's a moron... Him and that midget Fauci make quite a pathetic pair...
Schroedingers Cat 2 hours ago
He's not stupid. He either brainwashed, blackmailed or in all likelihood a greedy
genocidal psychopath who puts his career and income before the future of the entire human
race..
WeNamedTheDogIndiana 1 hour ago
mask mandates and social distancing need to remain in place for the foreseeable future
"as part of our defence" against COVID
Just like getting groped at airports by TSA goons, warrantless surveillance, warrant
applications approved almost 100% of the time by a shadowy court, and renewal of the
Patriot Act....all for our safety. Sure.
liberty2day 2 hours ago
the only ugly face that needs a muzzle is faoxi's
dockw 2 hours ago
Could you reference some studies, like in scientific, that demonstrate Masks are
effective in blocking the Covid? -- which virons are smaller than the material in a mask I
didn't think so.https://www.acpjournals.org/doi/10.7326/M20-6817
hoytmonger 1 hour ago
Here's an article written by Yeadon...
https://www.dailymail.co.uk/news/article-8899053/DR-MIKE-YEADON-Three-facts-No-10s-experts-got-wrong.html
Max21c 50 minutes ago remove link
According to Nabarro, mask mandates and social distancing need to remain in place for
the foreseeable future "as part of our defence" against COVID , particularly in regions
which have high infection rates.
Social distancing seems rather silly. If a person remains the required distance away
from another person this does not mean they may not be breathing the same air. The air does
not abide by social distancing. Air moves. People move. If people move through contaminated
air yet keep the proper social distancing space with other persons yet people are still
passing through contaminated air. Even if there is no one around and a person is perfectly
social distanced from the entire human race thus they can still be breathing in
contaminated air that was previously contaminated by an infected person even a few moments
before. I just don't get the whole folly of social distancing thing.
Further, it's a talking virus that is spread by talking. So if one is perfectly socially
distanced from another and yet talking or one is talking on their cell and the other not
talking... well it still comes down to masks and contaminated air.
People should generally tend to wear masks when venturing out especially as to high
pedestrian traffic areas or high traffic sites such as big box stores or grocers or even
neighborhood small stores that receive a lot or constant foot traffic/patronage.
The shots are "safe and effective," the propagandists proclaim.
That's absolutely true. Until some woefully ignorant, or psychopathic imitation of a human
being injects them into someone.
Anyone with two or more brain cells that get along, and has paid the slightest attention
knows that those under 20 are virtually immune to the virus, and those under 40 are no more at
risk than they are from the common cold, and those under 60 with no other serious co-morbidity
are only at slight risk. There is no logical reason to vaccinate ANYONE under 20. Very little
reason regarding those 20-40, and choose your poison if you are 40-whatever. At 67 I've chosen
to take my chances without participating in a medical experiment.
Regarding safety, they are the most dangerous vaccine ever produced, much less deployed,
even by the woefully inadequate results of under reporting to VAERS. By those results, the
COVID vaccines have already killed about 6,000 Americans. More than all other vaccines combined
for the last 10-30 years, and the year is only half over. Some of those other vaccines were
pulled from the market because of as few as 50 deaths. Why do the COVID vaccines get a pass for
6,000? And that's just deaths. There are abundant other side effects, including mounting
evidence of mental disability, and definite reproductive damage.
boyplunger7777 13 hours ago remove link
VAERS data: "5,888 deaths", "19,597 hospitalizations", "43,891 urgent care", "58,800
office visits", "1,459 anaphylaxis", "1,737 Bell's palsy", "2,190 heart attacks" and "652
miscarriages". CDC says data is "unreliable". You choose who to believe.
WarrenLiz 16 hours ago
Over 15,472 dead from Jab in 27 EU countries, about half of Europe's 50 countries.
The EudraVigilance database reports that through June 19, 2021 there are 15,472 deaths
and 1,509,266 injuries reported following injections of four experimental COVID-19
shots:
From the total of injuries recorded, half of them (753,657) are serious injuries.
ALL UNNECESSARY...
https://vaccineimpact.com/2021/15472-dead-1-5-million-injured-50-serious-reported-in-european-unions-database-of-adverse-drug-reactions-for-covid-19-shots/
Globalist Overlord 14 hours ago remove link
So between the EU and US there are a confirmed MINIMUM of 21,000 MURDERED by BigPharma
and their highly-paid apparatchiks like Fauci and Walensky.
And the public does nothing.
pods 16 hours ago
Graphing VAERS numbers alongside the shot numbers should show abnormalities.
They probably saw the numbers and put the brakes on putting them in the database. So a
slope change will be seen in the VAERS data.
They run it so they can do what they want. Public can submit a case, but that doesn't
mean it goes into the database. Crooks.
pmc 17 hours ago (Edited)
Tucker Carlson: How many Americans have died after taking the COVID vaccine?
https://www.foxnews.com/opinion/tucker-carlson-how-many-americans-have-died-after-taking-the-covid-vaccine
The answer to Carlson's question is because.. it's a money grabbing death cult!.
Natural immun system is destroyed... just wait till next flu season or the next virus
they relase and see what death numbers we see!
racing_flowers 17 hours ago
Isn't it curious that the 3 big pharma Corps (think Vacc pushers) and the big 2 MSM
Corps are BOTH controlled by Blackrock Partners Hedge Fund...
Nona Yobiznes 18 hours ago remove link
Them going after the children makes me deeply suspicious. Nobody under 50, unless
they're made of blubber, dies from this. In 2020, there was practically zero excess death
for people younger than 70 years old in Sweden. These are their official statistics. For
the vast majority of people it's basically a flu you get for a couple days and you're over
it. What the **** is all this about? If the vaccine is only really good for preventing
hospitalizations, and doesn't stop you from spreading or from catching variants, what in
the hell are we giving kids vaccines when they are more likely to die from the regular flu?
It's freaky, and it stinks.
Having been caught delivering some fact-base 'science' that does not
jibe with the establishment's message that all kids should be jabbed immediately, The WHO has
rapidly 'adjusted' its science-based recommendations for whether children should get
vaccinated... or not...
Gone is the big headline - "Children should not be vaccinated for the moment."
The new guidance is as follows: (emphasis ours... in case you are confused by their
guidance)
Children and adolescents tend to have milder disease compared to adults, so unless they
are part of a group at higher risk of severe COVID-19, it is less urgent to vaccinate them
than older people, those with chronic health conditions and health workers.
More evidence is needed on the use of the different COVID-19 vaccines in children to be
able to make general recommendations on vaccinating children against COVID-19.
WHO's Strategic Advisory Group of Experts (SAGE) has concluded that the Pfizer/BionTech
vaccine is suitable for use by people aged 12 years and above. Children aged between 12 and
15 who are at high risk may be offered this vaccine alongside other priority groups for
vaccination.
Vaccine trials for children are ongoing and WHO will update its recommendations when the
evidence or epidemiological situation warrants a change in policy.
So to clarify... children aren't really at risk of this virus so no hurry on the jab... more
evidence is needed on its usefulness in kids... oh but the Pfizer vax is suitable?
So is there evidence or not? Is the vaccine worthwhile for kids? If you have to ask, you
aren't following the science.
Here's the new page ( source
)
h/t @AlexBerenson
Color us not entirely surprised at this farce... but one thing we are sure of, this will
simply be dismissed as a coincidence and WHO had planned on adjusting its guidance the whole
time (it was just waiting to get caught in a disagreement with Fauci and friends).
* * *
As The Ron Paul Institute for Peace & Prosperity's Adam Dick noted yesterday, in
America, national, state, and local governments are pulling out all the stops to advance giving
experimental coronavirus shots to children down to the age of 12.
Up next, babies and children up to age 11.
The shots are "safe and effective," the propagandists proclaim.
Meanwhile, the World Health Organization (WHO) has a different approach. The WHO says do not
vaccinate children, at least not yet.
At its website, the WHO offers this advice regarding giving experimental coronavirus
vaccines, some of which are not even vaccines under the normal meaning of the term, to
children:
Children should not be vaccinated for the moment. There is not yet enough evidence on the
use of vaccines against COVID-19 in children to make recommendations for children to be
vaccinated against COVID-19.
Children and adolescents tend to have milder disease compared to adults.
However, children should continue to have the recommended childhood vaccines.
Choose accordingly.
Kugelhagel 18 hours ago
Conspiracy theorist = heretic ... they couldn't use that word anymore, because everyone
would understand that this is about silencing the truth.
Ride_the_kali_yuga 17 hours ago
Nice analogy.
JimmyJones 17 hours ago remove link
Yep, women with their periods messed up, their babies allergic to their breast milk,
young people with heart inflammation, people having partial paralyzed limbs. I know there's
more.
We don't even know what 6-12 months has in-store or 1-2 years.
Alice-the-dog 13 hours ago
I'm always on the look out for new conspiracy theories, because my old ones all turned
out to be accurate.
It was a brilliant psyop by the CIA to invent the term to cover up the murder of JFK.
But if one takes a cursory look at it, how is a conspiracy ever to be exposed without a
theory that there is one? If every time someone proposes a theory regarding this or that
possible conspiracy, they are swept into the kook dust bin, how will any conspiracy ever be
exposed? Hence they aren't, unless iron clad evidence of their existence is encompassed by
the theory.
WarrenLiz 15 hours ago
Over 15,472 dead from Jab in 27 EU countries, about half of Europe's 50 countries.
The EudraVigilance database reports that through June 19, 2021 there are 15,472 deaths
and 1,509,266 injuries reported following injections of four experimental COVID-19
shots:
From the total of injuries recorded, half of them (753,657) are serious injuries.
ALL UNNECESSARY...
https://vaccineimpact.com/2021/15472-dead-1-5-million-injured-50-serious-reported-in-european-unions-database-of-adverse-drug-reactions-for-covid-19-shots/
skizex 13 hours ago remove link
and this on KOMO this morning:
https://komonews.com/news/local/cdc-young-people-least-likely-to-get-vaccinated-allowing-covid-to-spread
Nona Yobiznes 17 hours ago (Edited)
...Too many people are stuck in normalcy bias and are too trusting of the modern elite
class. You don't have to look back very far to see the unspeakable atrocities powerful
people are willing and able to commit.
Ride_the_kali_yuga 17 hours ago (Edited) remove link
My guess was depopulation due to lower EROIE on petroleum. Deathcross of the fossil
energy (oil) available was near to us, maybe we already are behind peak oil. Eolians, solar
panels and EV are an energical leftist joke and will never be an alternative to nuclear/
charchoal power plants and thermic motors.
I was thinking about it for quite some time. Why all this Covidian Cult was necessary
for? What does it produce? Lockdowns was a main response worldwide.
Was it usefull? absolutely not. No more planes in the sky, economic slowdown, a lot less
of enegy used . I guess this sanitary madness was all about cheap energy we can get from
oil. The human population exploded due to the industrial revolution, the machines, their
capacities and -in fine- oil made it possible. If you do not have enough cheap oil and the
EROIE is way to high, then the industrial technology we live in can no longer be.
The Covidian Cult produced what an energy crisis would have made...
The_Dude 16 hours ago
Evil is narcissism run amok...
Rose Marie PREMIUM 15 hours ago
Intelligence without wisdom. Always looking at what, how, when, where, but no interest
in asking why. Running thought processes without examining the meaning.
uncle_duke 18 hours ago remove link
An age of unlimited information, and a population too dumb and lazy to do anything with
it. Reality has become Pythonian.
DAVOS-19 14 hours ago
Not so fast. Remember, they lie, probably also about history.
Now Voyager 14 hours ago
What happens when you stop natural selection and substitute unnatural selection.
Ride_the_kali_yuga 13 hours ago
Yeah, the gene pool is over crowded with genetics defects. See diabetics, i mean
"genetical" ones since a young age. Insuline was a great discovery, it saves a lot of
people at some point. Then without the natural selection they had kids of their own and has
a consequence they spread their genetic defect in the gene pool. Sometimes great inventions
make unintended results.
Diseases are a way for nature to get rid of the olders and the weak. It is not moral,
there is no justice in this, this is just the way nature works. Human tried damn hard to
break nature's law, the thing is, there is consequences playing god.
"Delta is driving surges around the world, and I suspect it's going to be the same here,"
said William Lee, the vice president of science at Helix. Delta is growing more than twice as
fast as gamma, the variant first seen in Brazil, in undervaccinated communities.
Meanwhile, the gamma variant, which appears better at evading vaccines, was found to be more
prevalent in counties with higher inoculation rates.
People who have received the Pfizer/BioNTech vaccine have fewer antibodies targeting the
Indian COVID-19 variant compared to other strains, new data suggests.
Levels of these antibodies are lower with increasing age and decline over time, the analysis
of blood samples from 250 healthy people also suggests.
This provides even more evidence in support for vaccine boosters for the vulnerable come
autumn, researchers believe.
The data, from the Francis Crick Institute and the National Institute for Health Research
(NIHR) UCLH Biomedical Research Centre, also supports current plans to reduce the dose gap
between the jabs.
It found that after just one dose of the Pfizer jab, recipients were less likely to develop
antibody levels against the Indian variant, also known as Delta, as high as those seen against
the UK variant, now known as Alpha.
me height=
But scientists say antibody levels alone do not predict vaccine effectiveness and
prospective studies are also needed.
...researchers at Emory University performed similar studies with antibodies taken from 15
people who have been vaccinated with either the Pfizer or Moderna shots. In these studies, the
antibodies could still neutralize the B.1.617 variant, but the potency of the antibodies
dropped by about sevenfold on average, the authors reported .
"Despite this reduction, all vaccine blood samples ... still maintained the ability to block
the B.1.617 variant," said immunologist Mehul Suthar
at Emory, who led the study.
Together the data suggests the Pfizer and Moderna vaccines will still work well against
B.1.617, just as they do for the variant from South Africa, known as B.1.351. In both cases,
the shots will likely offer high protection from death and severe illness, but they may lose
some ability to stop mild or asymptomatic infections.
European health authorities have more or less confirmed that adenovirus-vector vaccines
produced by AstraZeneca and J&J can, in rare instances, cause potentially deadly cerebral
brain clots in patients with low blood-platelet counts. These findings, which were hinted at
during the late-stage trials for the AstraZeneca vaccine (which saw its US trials halted for a
month over safety issues) have
led to some European governments imposing restrictions on the vaccines.
... ... ...
The FT reports that the CDC
has found a "likely association" between a handful of cases of heart inflammation and the mRNA
COVID-19 vaccines. The reactions were documented in adolescent patients, which might explain
the delay in detection since teenagers have only just become eligible.
There were 323 confirmed cases among people who received the vaccine of certain types of
heart inflammation in the US up to June 11, with 309 people requiring hospital treatment.
Nearly 80% of the people with confirmed cases have fully recovered, according to the CDC's
Vaccine Safety Technical Work Group.
The cases have prompted the agency to start monitoring for new instances of myocarditis and
pericarditis, two different types of heart inflammation, to see if any new cases or potential
links emerge. The demographic group that's most vulnerable so far appears to be men under the
age of 30 (by contrast, the rare side effect for the AstraZeneca jabs mostly impacted young
women). Right now, the cases of heart inflammation have occurred at a rate of 4.4 per million
vaccine doses after the first dose, then rising to 12.6 per million after the second dose,
which is still exceedingly rare.
If an adolescent patient experiences heart inflammation after their first dose, the CDC
recommends deferring the second dose.
"This is an extremely rare side-effect, and only an exceedingly small number of people
will experience it after vaccination," doctors from the US health department, CDC and others
said in a statement following the meeting. "Most cases are mild, and individuals recover
often on their own or with minimal treatment. In addition, we know that myocarditis and
pericarditis are much more common if you get Covid-19 , and the risks to the heart from
Covid-19 infection can be more severe," they added.
In the US and Israel, high vaccination rates have prompted authorities to start vaccinating
younger and younger patients, with Israel now vaccinating patients as young as 12 . Anyone who
objects is quickly reminded of the threat of "variants" like the mutant strain "Delta".
Meanwhile, the developing world is still woefully undersupplied, leaving even the most
vulnerable patients without access.
Stinkbug 1 20 hours ago remove link
He's not being judgmental, just stating the facts as he sees them.
The young men who submit to the shot are cannon fodder for big Pharma. The young men who
went to war for causes that turned out out be lies were also cannon fodder. Part of the
tragedy is that their anger cannot be channeled into healthy change since they are either
disabled or no longer with us.
If you were forced to take this shot, focus your anger on the system, not those who
point out the corruption.
ohm 16 hours ago remove link
Who is being forced to take the shots? Unless they have people holding you down or a
gun at your head, you are not forced.
You are being forced in certain countries like Indonesia and the Philippines. In the
rest of the world your are being coerced. Either way, it is a violation of the Nuremberg
code. Libtards, Fauci, Collins and the rest of the public health authorities prove again
that Mengele was just ahead of his time.
WHO's Swaminathan said that scientists still needed more data on the variant, including its
impact on the efficacy of Covid-19 vaccines. How many are getting infected and of those how many
are getting hospitalized and seriously ill?
Some countries, like the U.S. and U.K., have already signaled that they could
roll out Covid-19 booster shots within a year . Now, pressure is building on governments to
mobilize booster shot programs" no easy task given the ongoing uncertainties surrounding the
pandemic, vaccines and variants.
However, concrete plans for Covid-19 booster shots are lacking. Dr. Peter Marks, director of
the FDA's Center for Biologics Evaluation and Research, last month said it was,
"just something we're gonna have to figure out as we go."
As talk of booster shots grow, here's what we know so far: What?
First of all, there are question marks over whether we actually need a third dose of any
Covid-19 vaccine given that we don't know how long immunity currently lasts.
In the U.S. and U.K. the shots being used are those from Pfizer - BioNTech , Moderna and Johnson & Johnson , with the U.K. also relying
heavily on the AstraZeneca
-Oxford University vaccine.
WATCH NOW VIDEO 01:22 Dr. Scott Gottlieb on whether people will
need Covid booster shots
There are also unknowns regarding whether people should get a booster shot that's the same
as the vaccines they originally had. And also whether the shots need to be tweaked to deal with
variants, much like the flu vaccine, or whether they can remain as they are.
This report claims that people who had been fully vaccinated with two Pfizer doses had
antibodies that were 6 times lower against the B.1.617.2 variant (aka Indian variant, aka Delta
variant). Other reports claim that two doses of the Pfizer vaccine provided about 88% protection.
Analysis from Public Health England released last week showed that two doses of the
Pfizer-BioNTech or Oxford-AstraZeneca Covid-19 vaccines are highly effective against
hospitalization from the delta variant.
This is the most transmissible of all the variants that we've seen. But now a mutation of
that variant has emerged, called "delta plus," which could potentially be more transmissible. The
variant appears to cause alarmingly severe symptoms, scientists say. Stomach pain, nausea,
vomiting, loss of appetite, hearing loss, and joint pain are among the symptoms now being seen in
India, according to six doctors treating patients across India, Bloomberg News reports.
The delta plus variant has three worrying characteristics. These are, it said: increased
transmissibility, stronger binding to receptors of lung cells and the potential reduction in
monoclonal antibody response (which could reduce the efficacy of a lifesaving monoclonal antibody
therapy given to some hospitalized Covid patients).
The Delta variant, as it's now called, has swept across the UK, all but replacing the Alpha
variant first identified there late last year.
As of June 19 20.6% of the cases in the USA are Delta. This number has roughly doubled every
two weeks, he added.
Currently, 62.5% of Americans 12 and up have gotten at least one dose of a vaccine, according
to CDC.
June 4, 2021 -- The Pfizer COVID-19 vaccine produces lower
levels of antibodies against the Delta variant, known as B.1.617.2 and discovered in India,
according to a new
study published Thursday in The Lancet .
The antibody levels also appear to be lower in older people and decline over time, which
could mean that some vaccinated people will need a booster shot this fall.
"This virus will likely be around for some time to come, so we need to remain agile and
vigilant," Emma Wall, PhD, the lead study author and an infectious diseases specialist at the
Francis Crick Institute in London, said
in a statement .
"The most important thing is to ensure that vaccine
protection remains high enough to keep as many people out of hospital as possible," she said.
"And our results suggest that the best way to do this is to quickly deliver second doses and
provide boosters to those whose immunity
may not be high enough against these new variants."
The research team analyzed antibodies in the blood of 250 healthy people, ages
33-52, up to 3 months after receiving their first dose of the Pfizer COVID-19 vaccine . The team looked for
"neutralizing antibodies," or the ability of antibodies to block the virus from entering
cells.
The researchers tested five variants: the original strain discovered in China, the dominant
strain in Europe during the first wave in April 2020, the B.1.1.7 variant discovered in the
U.K., the B.1.351 variant first seen in South Africa, and the newest variant of concern, which
is the B.1.617.2 variant discovered in India.
The team compared the concentrations of the neutralizing antibodies among the variants.
They found that people who had been fully vaccinated with two Pfizer doses had antibodies that
were 6 times lower against the B.1.617.2 variant, 5 times lower against the B.1.351 variant,
and 2.6 times lower against the B.1.1.7 variant when compared to the original strain.
The antibody response was even lower in people who had received only one dose. After a
single Pfizer dose, 79% of people had neutralizing antibodies against the original strain,
which fell to 50% for the B.1.1.7 variant, 32% for the B.1.617.2 variant, and 25% for the
B.1.351 variant.
The study group plans to continue its research on neutralizing antibodies and the variants,
including in people who have been vaccinated with the AstraZeneca vaccine.
"New variants occur naturally, and those that have an advantage will spread. We now have the
ability to quickly adapt our vaccination strategies to maximize protection where we know people
are most vulnerable," David Bauer, PhD, the senior study author and group leader of the Francis
Crick Institute's RNA Virus Replication Laboratory, said in the statement.
"Keeping track of the evolutionary changes is essential for us to retain control over the
pandemic and return to
normality," he said. "This work "¦ can help us to navigate changes in this new phase of
the pandemic."
Bank_sters 12 hours ago remove link
Credit racing flowers:
On Friday, Italy halted the administration of the killer vaccine for those under the age
of 60. The decision followed the death of a perfectly healthy 18-year-old named Camilla
Canepa, who died last week of blood clotting and a brain hemorrhage after receiving the
vaccine shot on the 25th of May.
I think most of us have come to the conclusion that these deaths are the way it was
suppose to work. That makes this the greatest crime against humanity.....ever
fuckyou 12 hours ago remove link
So I looked at your story about Italy and they stopped the AstraZeneca vaccine, all the
others are still available. So partially correct.
Jim in MN 15 hours ago
Not everyone will die. Many more will just be crippled and need expensive medical care
for decades, while being unable to fight or resist the regime.
Jim in MN 15 hours ago
The immune cells that the mRNA targets are well-known as key factors in autoimmune
disorders when their function is disrupted.
This is Wikipedia-level stuff. People should not be in any way ignorant about this.
Jim in MN 15 hours ago (Edited) remove link
https://en.wikipedia.org/wiki/Dendritic_cell
The exact genesis and development of the different types and subsets of dendritic cells
and their interrelationship is only marginally understood at the moment, as dendritic cells
are so rare and difficult to isolate that only in recent years they have become subject of
focused research. Distinct surface antigens that characterize dendritic cells have only
become known from 2000 on.
Altered function of dendritic cells is also known to play a major or even key role in
allergy and autoimmune diseases
....
Sparehead 13 hours ago
Nah, just looks at this massively under-reported VAERS death graph.
https://www.openvaers.com/covid-data/mortality
See, no worries at all. Face diapers, anti-social distancing, and one-way shopping
arrows saved us. Let's just hope there's no "variants" that start dropping the vaxxed like
flies.
Rex Dickerson 15 hours ago
Duh.
Pfizer clinical trial ends April 2023.
Moderna clinical trial ends October 2022.
LeadPipeDreams 15 hours ago
Pfizer human trial ends April 2023.
Moderna human trial ends October 2022.
FIFY
Vaccines typically take 10 - 15 years to prove their safety and efficacy, so even these
human trials are a joke to prove they are "safe and effective".
Esperanza 15 hours ago
Technically, the trials are not trials any more. They have been compromised due to the
control group taking the vaccine.
El_Puerco 15 hours ago
https://www.gospanews.net/en/2021/03/23/mrna-vaccines-cancer-risks-wlo-crimes-against-humanity/
The famous virologist Montagnier
Prompt complaint to the International Criminal Court
And now " The Circus" is open..
WOW!
hooligan2009 13 hours ago
someone ask the CDC why children should be stabbed instead of giving them either nothing
at all, or a small amount of ivermectin
from here:
https://journals.lww.com/americantherapeutics/Abstract/9000/Ivermectin_for_Prevention_and_Treatment_of.98040.aspx
" Low-certainty evidence found that ivermectin prophylaxis reduced COVID-19 infection by
an average 86% (95% confidence interval 79%""91%).
--
Conclusions:
Moderate-certainty evidence finds that large reductions in COVID-19 deaths are possible
using ivermectin. Using ivermectin early in the clinical course may reduce numbers
progressing to severe disease. The apparent safety and low cost suggest that ivermectin is
likely to have a significant impact on the SARS-CoV-2 pandemic globally."
hooligan2009 13 hours ago remove link
not as if the stabs prevent covid anyway!
https://www.thegatewaypundit.com/2021/06/nearly-4000-people-massachusetts-tested-positive-coronavirus-fully-vaccinated/
NAV 14 hours ago
What happens after the concentrations of the vax nanoparticles accumulate in the bone
marrow, which they are doing? Perhaps leukemia? We don't know. But for some, it is more
important to virtual signal that you and your children got the vaccine rather than its
unknown consequences.
Robert Malone, MD, inventor of mRNA vax technology, is dismayed by Pfizer's study for
Japan showing the vax nanoparticles accumulate in the bone marrow, ovaries, spleen, and
lymph nodes.
He says there needs to be monitoring of vaccine recipients for leukemia and lymphomas
because of these concentrations in the bone marrow and lymph nodes. He says these signals
often don't show up for six months to 3-9 years down the road.
Malone says the FDA knew the COVID spike protein was biologically active and could
travel from the injection site and cause adverse events, and that the spike protein is
very dangerous.
He says there should have been 2-3 year trials to monitor for potential autoimmune
consequences of the vaxxes, but of course that didn't happen. He says they also didn't
conduct proper animal studies.
Malone agreed with Vanden Bossche that conducting mass vaxxing in the middle of a
pandemic is insane because of the danger of creating a more virulent wild Covid. -- Nemo
(
https://raypeatforum.com/community/threads/covid-vaccine-adverse-reaction-reports-post-here.39666/page-56
)
Inventor of mRNA Technology: Vaccine Causes Lipid Nanoparticles to Accumulate in 'High
Concentrations' in Ovaries
On the "Dark Horse Podcast," Dr. Robert Malone, creator of mRNA vaccine technology, said
the COVID vaccine lipid nanoparticles -- which tell the body to produce the spike protein
-- leave the injection site and accumulate in organs and tissues (particularly the ovaries
and bone marrow). O6/17/21
https://childrenshealthdefense.org/defender/mrna-technology-covid-vaccine-lipid-nanoparticles-accumulate-ovaries/?utm_source=salsa&eType=EmailBlastContent&eId=1052c4b1-d2be-46fc-875b-a65558e66b73
Pair Of Dimes Shift 14 hours ago remove link
There are suspicions, but nobody knows for sure.
Jim in MN 14 hours ago
See my comments below on dendritic cells. That's what the mRNA is supposed to target,
and even doing that is messing with immune system mechanisms that scientists don't even
understand in the first place , before they mess with it.
Jim in MN 15 hours ago
While a COVID-19 vaccine will prevent serious illness and death, we still don't know the
extent to which it keeps you from being infected and passing the virus on to others.
Sooooooooo.......all the databases and vaccine requirements to do this and that
are........not based on anything?
Anything.........at all?
That's what I thought. Thanks for clearing that up.
Giant Meteor 15 hours ago
" While a COVID-19 vaccine will prevent serious illness and death, it may also create
serious illness and death!"
Hmmm decisions decisions ..
Volga Boat Man 15 hours ago remove link
Only a flaming moron would allow themselves to take the Zombie Jab when both the
Gruberment AND the Manufacturer claim NO liability for anything that happens as a result,
i.e., dying.
Conservative Thought 15 hours ago
WHO and CDC are not on same page...shocker
Some facts that have not changed since 2019 outbreak
It's a bioweapon not a naturally occurring virus - gain of function confirmed
It's a gene modifying cell therapy not a vaccine - first time used on humans
It's only approved an emergency authorization; it's not FDA approved
It's unproven read as potentially unsafe since over 5,500 Americans have died after
getting the jab
It's not effective since Pfizer and Moderna claim it's not stopping transmission
Pfizer former VP Dr. Michael Yeadon warns people not to take the jab
TQRock 16 hours ago
Unclear how an experimental "vaccine" authorized for emergency use only could be
proclaimed "safe and effective."
BAG 18 hours ago remove link
The covid-19 EUA should be changed to make the vaccine manufactures liable for damages
to anyone under the age of 50 years old. Then they can tell us how safe it is.
Goldbugger 12 hours ago remove link
Eric Clapton says COVID VACCINE damaged his Immune system.
https://articles.mercola.com/sites/articles/archive/2021/06/22/eric-clapton-covid-19-vaccine-injury.aspx?ui=19ac65ba714eca3fb361a42233b18ddba12e5c42f1ee5279b189266b75264633&sd=19000101&cid_source=dnl&cid_medium=email&cid_content=art2HL&cid=20210622&mid=DM917124&rid=1189768552&p4=20131022&p5=
Enraged 12 hours ago
My uncle believes everyone should be vaccinated, while I will never accept the lethal
injection. The difference between us is he watches MSM and reads the daily newspaper, while I
cut the cord seven years ago.
COVID/vaccine is psychological warfare by the globalist elite and banksters against the
people using the propaganda media. The MSM viewership will soon be too low to broadcast as
their viewers are the mind controlled vaccine takers.
El_Puerco 15 hours ago remove link
If you understand this...Good for you.
https://www.who.int/emergencies/diseases/novel-coronavirus-2019/covid-19-vaccines/advice
Note:
Children should not be vaccinated for the moment.
There is not yet enough evidence on the use of vaccines against COVID-19 in children to
make recommendations for children to be vaccinated against COVID-19. Children and
adolescents tend to have milder disease compared to adults. However, children should
continue to have the recommended childhood vaccines.
Simpson 19 hours ago
According to Dr. Michael Yeadon kids are 50 times more likely to die from the shot then
they are from the WuFlu.
Parents who give their kids this toxic ****e deserve a shot right between the eyes.
walküre 19 hours ago
"doing their part"
"nobody is safe, until we're all safe"
Hail Stalin, Mao, Hitler, Gates & Fauci!
walküre 19 hours ago (Edited) remove link
About fking time!
HANDS OFF THE KIDS!
There's going to be blood in the streets if they keep pushing us further and
further!
Our kids are not some cannon fodder for the elite's wars! Only despots and tyrants do
this when they're running out of options. Feeding kids into the lines of fire. We have a
Nuremberg code and a Geneva convention for a REASON!
The vax is garbage!
Absolutely NIL benefit for your health, only benefit to your social credit score.
Go ahead, get vaxxed if you feel like it. Know the risks, and inform yourself what the
ridiculous and negligible advantages are of having the synthetic toxins injected into your
system.
The side effects FAR outweigh the risks of potentially getting sick from whatever it is,
circulating out there. If your body is too weak or your system is responding badly to the
"virus", it will also respond negatively to the injections. When your time has come, your
time has come. Life is meant to be lived. Longevity is a God given privilege or curse, but
it is not a competition.
Samual Vimes 19 hours ago
Let them change genders and compete against girls in peace.
PrivetHedge 14 hours ago remove link
Number of verified covid test methods: Zero
Number of children damaged by the vaccine: Hundreds, soon to be Millions.
https://healthimpactnews.com/
Gravel Rash 17 hours ago remove link
Emergency experimental drugs are never given to children, pregnant women or the old with
health issues. Doesn't happen, full stop.
And yet its happening with the covid gene therapy shots, the official name alone
warrants that it would never be given to kids and the pregnant. One can only assume the
greed of Pharma companies and their lackeys at regulatory agencies knows no bounds, they
know there are issues with the drugs. However they have indemnity from being sued, as such
they want to sell as much as they can before the ignorant masses catch on.
You wonder how these killers can sleep at night.
NoPension 17 hours ago
Trump's out. They sleep like babies.
Person familiar with the situation 17 hours ago
It's NOT about money. People keep making that baseless assumption just because most
everything else is about money in their own little world. The criminals here have printing
presses in every country and create money out of thin air.
Yamaoka Tesshu 9 hours ago (Edited)
He is Uncle Warren's longtime lieutenant. Look at AIDS. "If we make up a fake disease we
will get a fortune in funding." And they did. They prescribed lethal drugs that killed
people with the express purpose of creating hysteria. Murder for money.
Man on the Silver Mountain 19 hours ago
A demand that kids shouldn't be injected with this experimental shot is almost a
sideways admission the mRNA potion is detrimental to natural immunity, yet there's an
obsessively urgent need to stab adults? In the US I'd suspect the source of this motivation
is politics and a grasping greed for profit.
UselessEater 6 hours ago
NEW: Former Head Scientist at PFIZER Says Covid Threat is 100% FAKE
https://redpilluniversity.org/former-head-scientist-at-pfizer-says-covid-threat-is-100-fake/
Prior to forming his own biotech company in 2011, Michael Yeadon was the Vice President
and Chief Scientific Officer for Allergy & Respiratory Research at Pfizer
Pharmaceutical.
He is a top scientist in the world of drugs and vaccines in the treatment of respiratory
diseases such as Covid. In this video he declares that the Covid pandemic is a fraud. He
explains why masks are useless, why distancing is absurd, why PCR tests are meaningless,
why quarantining healthy people is stupid, why variants of virus strains are no threat, and
why Covid vaccines should be rejected.
Yeadon says many of his colleagues privately agree with this appraisal but remain silent
to protect their salaries and research grants. It's all about money.
He concludes that, because of the massive number of deaths that will follow within a few
years of vaccination, there clearly is an agenda to deliberately eliminate billions of
people from the Earth and to enslave those who remain ..... plus much more.
[This scientist is such a good, brave man. He loves humanity. His voice is being
silenced on mainstream media and he is putting out this info to the public despite being
smeared and attacked (though they don't address his facts at all). So:
Pse share this video out to at least 5 other people as he gives simple scientific
explanations for all his statements.
archipusz 19 hours ago (Edited)
Giving this gene therapy called a vaccine to kids is worse than shutting down an economy
based on pcr tests run at 45 cycles.
Tao 4 the Show 11 hours ago remove link
I don't do Facebook or twitter, but someone should do an experiment:
Post something condemning vaccination in children and reference the WHO and link.
https://www.who.int/emergencies/diseases/novel-coronavirus-2019/covid-19-vaccines/advice
Let's watch some "fact checker" (that is, thought Gestapo) heads explode.
Straw Dog 12 hours ago (Edited) remove link
COVID-19 mRNA Shots Are Legally Not Vaccines
By Joseph Mercola
Mercola.com
February 11, 2021
Did you know that mRNA COVID-19 vaccines aren't vaccines in the medical and legal
definition of a vaccine? They do not prevent you from getting the infection, nor do they
prevent its spread. They're really experimental gene therapies.
I discussed this troubling fact in a recent
interview with molecular biologist Judy Mikovits , Ph.D. While the Moderna and Pfizer
mRNA shots are labeled as "vaccines," and news agencies and health policy leaders call them
that, the actual patents for Pfizer's and Moderna's injections more truthfully describe
them as "gene therapy," not vaccines.
Picked up this article and pasted it in an MS Word docx. Interestingly you can't find it
by Google search - Censored
Bank_sters 13 hours ago remove link
Ok so Fauci and the cdc telling colleges and schools to push for experimental poison to
be given as a condition for young people to return to school. Now the myocarditis,
reproductive health, blood clotting cases are EXPLODING.
TheABaum 13 hours ago remove link
There are school districts demanding vaccination as a condition to return to live
instruction.
Hello Wilkes Barre, PA
One of the worst in the state.
Sparehead 15 hours ago remove link
Children are not lab rats and CANNOT make their own decisions about potentially
life-altering treatments for various reasons. Children are at essentially ZERO risk unless
they get jabbed.
ToSoft4Truth 15 hours ago
The parents did it.
Sparehead 15 hours ago
That not really the point, and there's many places that are allowing children to get
jabbed without parent consent, even in the US.
https://districtadministration.com/covid-19-vaccination-and-parental-consent/
Things that go bump PREMIUM 14 hours ago remove link
I've read that they are planning to go into schools in the fall and make sure all the
kids get their shots. Parental consent is not required.
almost 16 hours ago
WHO ~ World Health Organization sounds like The Ministry of Love in George Orwell's
novel 1984
It's more like World Death organization nowadays
Enraged 17 hours ago remove link
A 13-year old boy died three days after the 2nd Pfizer injection. The autopsy results
show an enlarged heart and there was some fluid surrounding it. He had no health problems
and was on no medications.
https://citizenfreepress.com/breaking/13-year-old-boy-dies-after-second-pfizer-shot/
Parents, if you allow your children to be injected with the vaccine, then you are an
accessory to murder.
rag_house 6 hours ago
Pfizer continues to have the greatest number of deaths and adverse events yet is
continually touted as the safest.
GoodyGumdrops 6 hours ago
If you want to truly understand how evil these psychopaths are start listening to this
video at 11:55. It's only a few minutes of your time.
https://www.bitchute.com/video/U2i5UzXj3hln/
JOHNLGALT. 11 hours ago remove link
📌📌📌📌For the 9,999th time. TRIALS FOR 'CRIMES AGAINST
HUMANITY' please.
The Nuremberg Code 1947 Permissible Medical Experiments
The great weight of the evidence before us to effect that certain types of medical
experiments on human beings, when kept within reasonably well-defined bounds, conform to
the ethics of the medical profession generally. The protagonists of the practice of human
experimentation justify their views on the basis that such experiments yield results for
the good of society that are unprocurable by other methods or means of study. All agree,
however, that certain basic principles must be observed in order to satisfy moral, ethical
and legal concepts:
1. The voluntary consent of the human subject is absolutely essential. This means that
the person involved should have legal capacity to give consent; should be so situated as to
be able to exercise free power of choice, without the intervention of any element of force,
fraud, deceit, duress, overreaching, or other ulterior form of constraint or coercion; and
should have sufficient knowledge and comprehension of the elements of the subject matter
involved as to enable him to make an understanding and enlightened decision. This latter
element requires that before the acceptance of an affirmative decision by the experimental
subject there should be made known to him the nature, duration, and purpose of the
experiment ; the method and means by which it is to be conducted; all inconveniences and
hazards reasonably to be expected; and the effects upon his health or person which may
possibly come from his participation in the experiment.
2. The duty and responsibility for ascertaining the quality of the consent rests upon
each individual who initiates, directs, or engages in the experiment . It is a personal
duty and responsibility which may not be delegated to another with impunity.
3. The experiment should be such as to yield fruitful results for the good of society,
unprocurable by other methods or means of study, and not random and unnecessary in
nature.
4. The experiment should be so designed and based on the results of animal
experimentation and a knowledge of the natural history of the disease or other problem
under study that the anticipated results justify the performance of the experiment.
5. The e xperiment should be so conducted as to avoid all unnecessary physical and
mental suffering and injury.
6. No experiment should be conducted where there is an a priori reason to believe that
death or disabling injury will occur; except, perhaps, in those experiments where the
experimental physicians also serve as subjects.
7. The degree of risk to be taken should never exceed that determined by the
humanitarian importance of the problem to be solved by the experiment.
8. Proper preparations should be made and adequate facilities provided to protect the
experimental subject against even remote possibilities of injury, disability or death.
9. The experiment should be conducted only by scientifically qualified persons. The
highest degree of skill and care should be required through all stages of the experiment of
those who conduct or engage in the experiment.
10. During the course of the experiment the human subject should be at liberty to bring
the experiment to an end if he has reached the physical or mental state where continuation
of the experiment seems to him to be impossible.
11. During the course of the experiment the scientist in charge must be prepared to
terminate the experiment at any stage, if he has probable cause to believe, in the exercise
of the good faith, superior skill and careful judgment required of him, that a continuation
of the experiment is likely to result in injury, disability, or death to the experimental
subject.
Lou Saynis 12 hours ago
I'd like to see the people responsible for gain of function research, that led to
KNOWINGLY creating a dangerous infectious agent, be publicly held responsible . If they are
not and the masterminds of this doomsday device are allowed to vanish behind a veil of
bureaucracy... then it will result in all global powers engaging in an arms race similar to
nuclear weapons in the 20th century.
The difference is, a significant degree of action is required to fire off a nuke where a
virus can be accidentally or intentionally released with a much larger blast radius and
much more difficult to identify the source. There must be consequences for Covid19.
The reason the vaccine is a different subject is that a large portion of the civilized
world have already been inoculated. The consequences of that will be apparent in all of our
lifetimes and it's too early to start blaming people for it's known faults.
CheapBastard 15 hours ago (Edited)
13-Year-Old Dying Days After COVID Vaccine
13-year old nephew died three days after receiving a second dose of Pfizer's coronavirus
vaccine.
https://www.breitbart.com/tech/2021/06/21/twitter-censors-conservative-news-site-for-story-on-tweet-reporting-coronavirus-vaccine-death/
Probably just coincidental, right?
Things that go bump PREMIUM 14 hours ago remove link
Vaccine companies are always shielded from lawsuits. If your kid dies or is disabled
from the MMR (it does happen), you have to apply to the government for compensation. The
risks are well know and considered acceptable for public health. If your kid is among the
unlucky ones, well, you must bear that burden and thank you for your service to the cause
of public health.
realitybiter 16 hours ago remove link
I'm no lawyer, but I do know that the law protects Big Pharma. The law does not protect
anyone else who has demanded that anyone get the vaccine in order for them to conduct their
lives. -Go to school, go to work,etc. This is a Nuremberg violation:
The voluntary consent of the human subject is absolutely essential. This means that the
person involved should have legal capacity to give consent; should be so situated as to be
able to exercise free power of choice, without the intervention of any element of force,
fraud, deceit, duress, overreaching, or other ulterior form of constraint or coercion; and
should have sufficient knowledge and comprehension of the elements of the subject matter
involved as to enable him to make an understanding and enlightened decision.
Sue them into oblivion.
Start with the BLUE STATE GOVERNORS
"hang em high"
Gunston_Nutbush_Hall 16 hours ago (Edited)
You do realize our founders had no check and balance against the National/State
Government(s) performing eugenic medical/science theory fraud experimentation upon the
people, under criminal false pretenses for private profit and control, except one.
There is no Court or law enforcement/cops coming to halt these crimes against
Americans/humanity.
If the representatives of the people betray their constituents, there is then no
resource left but in the exertion of that original right of self-defense which is
paramount to all positive forms of government , and which against the usurpations of the
national rulers, may be exerted with infinitely better prospect of success than against
those of the rulers of an individual state. In a single state, if the persons intrusted
with supreme power become usurpers, the different parcels, subdivisions, or districts of
which it consists, having no distinct government in each, can take no regular measures
for defense. The citizens must rush tumultuously to arms, without concert, without
system, without resource; except in their courage and despair. The usurpers, clothed with
the forms of legal authority, can too often crush the opposition in embryo- Alexander
Hamilton; The Federalist Papers : No. 28
https://avalon.law.yale.edu/18th_century/fed28.asp
on target 3 hours ago remove link
Incontrovertible "data" was available and known to the WHO/NIH/CDC/NIAID that children
under 14 have a negligible risk of death or serious injury from Covid19 in March 2020. The
risks have actually diminished since then. Given these facts, the original recommendation
to vaccinate the entire population, including the young, amounts to medical malpractice. If
your clueless family doctor or pediatrician is recommending this experimental "vaccine" for
your children, find another medical provider. The politicized agenda driven WHO is playing
both sides, as usual, rather than following the science and common, reasonable, tried and
trusted practices. Remember: The Government can't even get 40 percent of the workers at the
CDC/NIH/FDA to take their "jab" despite enormous pressure. Keep this uppermost in your mind
and decision making.
Son of Loki 18 hours ago
A Doctor Reacts to Bills Receiver Cole Beasley's Refusal to Get the Covid Vaccine
Cole Beasley , wide receiver with the Buffalo Bills, caused a stir on Friday when he
shared a statement on Twitter in which he asserted that he would not be getting the Covid
vaccine. "Hi, I 'm Cole Beasley and I 'm not vaccinated!," he wrote. "I will be outside
doing what I do. I'll be out in the public. If your scared of me then steer clear, or get
vaccinated. Point. Blank. Period. I may die of covid, but I'd rather die actually
living."
"I 'm not going to take meds for a leg that isn't broken, " he continued. "I'd rather
take my chances with Covid and build up my immunity that way. Eat better. Drink water.
Exercise and do what I think is necessary to be a healthy individual. That is MY CHOICE
based on MY experiences and what I think is best ... If I 'm forced into retirement, so be
it."
https://www.msn.com/en-us/health/medical/a-doctor-reacts-to-bills-receiver-cole-beasley-s-refusal-to-get-the-covid-vaccine/ar-AALf9ZL?li=BBnba9O&ocid=mailsignout
walküre 17 hours ago (Edited) remove link
check the picture of Cole Beasley the MSN link is using .. nice framing job there,
propaganda ministry of truth apparatschicks.
put "Dr" Mike Hansen on the list of accused for the Nuremberg trials
"There's really only one valid medical reason why someone shouldn't get the vaccine,"
he added. "If someone has a severe allergy history when it comes to getting a vaccine,
that could be a legit medical reason."
While Beasley has made a personal choice, Hansen explains that when it comes to the
vaccine, the decisions we make about our own health affect outcomes for others.
"What's going to happen is you're going to have other variants of the coronavirus,
like the Delta variant which originated in India and is all across the globe and is in
the United States," he said. "Not only does it spread easier, it's thought to be more
infectious, more dangerous. Over time that has the potential to overcome those who are
vaccinated. It could be that the vaccines work for a little while, but because we don't
reach that herd immunity, that virus never goes away. The other aspect of not getting
herd immunity is, those who can't get the vaccine, like children, then you're making them
more prone to the virus."
His scientific statement is utter garbage. The "virus" isn't likely to effect more
unvaxxed, because of a higher rate of vaxxed. That's the "new normal" logic and it's failed
like so many other arguments they're making.
The vax doesn't provide herd immunity. PERIOD. At best, if the "spike protein" theory is
correct, it will provide marginally better chances to beat the severe symptoms. That's a
big IF. Double vaxxed are now dying in larger numbers, months after they completed the
experiment. That was predictable.
Guys like Mike Hanson need to be paid a visit. At minimum, a proper dead horse's head on
this guy's pillow. If he doesn't stop, he needs to be taken out into the woods.
I'm not joking. Real men need to start doing real God's work.
Highly recommended !IF expressing concerns for kid vaccination is a punishable offence that's 100% pure
Lysenkoism and strongly smells with Stalinism.
Via The Justice Center For Constitutional Freedom,
The Justice Centre for Constitutional
Freedoms represents Dr. Francis Christian, Clinical Professor of General Surgery at the
University of Saskatchewan and a practising surgeon in Saskatoon .
Dr. Christian was called into a meeting today, suspended from all teaching responsibilities
effective immediately, and fired from his position with the University of Saskatchewan as of
September 2021.
There is a recording of Dr.
Christian's meeting today between Dr. Christian and Dr. Preston Smith, the Dean of Medicine
at the University of Saskatchewan, College of Medicine, Dr. Susan Shaw, the Chief Medical
Officer of the Saskatchewan Health Authority, and Dr. Brian Ulmer, Head of the Department of
Surgery at the Saskatchewan College of Medicine.
In addition, the Justice Centre will represent Dr. Christian in his defence of a complaint
that was made against him and an investigation by the College of Physicians and Surgeons of
Saskatchewan. The complaint objects to Dr. Christian having advocated for the informed consent
of Covid vaccines for children.
Dr. Christian has been a surgeon for more than 20 years and began working in Saskatoon in
2007. He was appointed Director of the Surgical Humanities Program and Director of Quality and
Patient Safety in 2018 and co-founded the Surgical Humanities Program. Dr. Christian is also
the Editor of the Journal of The Surgical Humanities.
On June 17, Dr. Christian
released a statement to over 200 doctors which contained his concerns regarding giving the
Covid shots to children. In it he noted that he is pro-vaccine, and that he did not represent
any group, the Saskatchewan Health Authority, or the University of Saskatchewan.
"I speak to you directly as a physician, a surgeon, and a fellow human being."
Dr. Christian noted that the principle of informed consent was sacrosanct and noted that a
patient should always be "fully aware of the risks of the medical intervention, the benefits of
the intervention, and if any alternatives exist to the intervention."
"This should apply particularly to a new vaccine that has never before been tried in
humans"¦ before the vaccine is rolled out to children, both children and parents must
know the risks of m-RNA vaccines," he wrote.
Dr. Christian expressed concern that he had not come across "a single vaccinated child or
parent who has been adequately informed" about Covid vaccines for children.
Among his points, he stated that:
The m-RNA vaccine, is a new, experimental vaccine never used by humans before.
The m-RNA vaccines have not been fully authorized by Health Canada or the US CDC, and
are in fact under "interim authorization" in Canada and "emergency use authorization" in
the US. He noted that "full vaccine approval takes several years and multiple safety
considerations "" this has not happened."
That in order to qualify for "emergency use authorization" there must be an emergency.
While he said there is a strong case for vaccinating the elderly, the vulnerable and health
care workers, he said, "Covid does not pose a threat to our kids. The risk of them dying of
Covid is less than 0.003% "" this is even less than the risk of them dying of the flu.
There is no emergency in children."
Children do not readily transmit the Covid virus to adults.
M-RNA vaccines have been "associated with several thousand deaths" in the Vaccine
Adverse Reporting System in the US. "These appear to be unusual, compared to the total
number of vaccines administered." He called it a "strong signal that should not be
ignored."
He noted that vaccines have already caused "serious medical problems for kids"
worldwide, including "a real and significantly increased risk" of myocarditis, inflammation
of the heart. Dr. Christian notes the
German national vaccine agency and the UK vaccine agency are not recommending the
vaccine for healthy children and teenagers.
The Saskatchewan Health Authority/College of Medicine wrote a letter to Dr. Christian on
June 21, 2021, alleging that they had "received information that you are engaging in activities
designed to discourage and prevent children and adolescents from receiving Covid-19 vaccination
contrary to the recommendations and pandemic-response efforts of Saskatchewan and Canadian
public health authorities."
Dr. Christian's concerns regarding underage Covid vaccinations are not isolated to him. The
US Centre for Disease Control had an "emergency meeting" today to discuss the growing cases of
myocarditis (heart inflammation) in younger males after receiving the Covid-19 vaccines.
The CDC released
new data today that the risk of myocarditis after the Pfizer vaccine is at least 10 times
the expected rate in 12 "" 17 year old males and females. The German government has issued
public guidance against vaccinating those under the age of 18.
The World Health Organization posted an update to its website on Monday, June 21, which
contained the statement in respect of advice for Covid-19 vaccination that " Children should not be
vaccinated for the moment ." Within 24 hours, this guidance was withdrawn and new
guidance was posted which stated that "Covid vaccines are safe for those over 18 years of
age."
Dr. Christian says there is a large, growing "network of ethical, moral physicians and
scientists" who are urging caution in recommending vaccines for all children without informed
consent. He said, physicians must "always put their patients and humanity first."
Dr. Byram Bridle, a prominent immunologist at the University of Guelph with a sub-speciality
in vaccinology, recently participated in a Press Conference on Parliament Hill on CPAC organized by MP
Derek Sloan, where he discussed the censorship of scientists and physicians. Dr. Bridle
expressed his safety concerns with vaccinating children with experimental MRNA vaccines.
Justice Centre Litigation Director Jay Cameron also has concern over the growing censorship
of medical professionals when it comes to questioning the government narrative on Covid.
"We are seeing a clear pattern of highly competent and skilled medical doctors in very
esteemed positions being taken down and censored or even fired, for practicing proper science
and medicine," says Mr. Cameron.
The Justice Centre
represented Dr. Chris Milburn in Nova Scotia, who faced professional disciplinary
proceedings last year after a group of activists took exception to an opinion column he wrote
in a local paper. The Justice Centre provided
submissions to the College on Dr. Milburn's behalf, defending the right of physicians to
express their opinions on matters of policy in the public square and arguing that everyone is
entitled to freedom of thought, belief, opinion and expression, as guaranteed by the Canadian
Charter of Rights and Freedoms "" including doctors. The Justice Centre noted that attempting
to have a doctor professionally disciplined for his opinions and commentary on matters of
public interest amounts to bullying and intimidation for speaking out against the
government.
Last week, Dr. Milburn also faced punishment for speaking out with his concerns about public
health policies, as he was removed from his
position as the Head of Emergency for the eastern zone with the Nova Scotia Health
Authority. In an unusual twist, a petition has been started to have Dr. Milburn replace Dr.
Strang as the province's Chief Medical Officer.
"Censoring and punishing scientists and doctors for freely voicing their concerns is
arrogant, oppressive and profoundly unscientific", states Mr. Cameron.
"Both the western world and the idea of scientific inquiry itself is built to a large extent
on the principles of freedom of thought and speech. Medicine and patient safety can only
regress when dogma and an elitist orthodoxy, such as that imposed by the Saskatchewan College
of Medicine, punishes doctors for voicing concerns," Mr. Cameron concludes.
Mr. Apotheosis 4 hours ago
These mother f'ers are seriously evil. To the bone evil.
high5mail 3 hours ago
I'm Canadian and the sooner they throw Trudeau and Manitoba's Pallister out of office
won't be too soon.
It is effen ridiculous what this country turned into. Makes California appear to be a
free place compared to here and that is saying something.
I am jealous of people living in Florida, Texas and South Dakota. They don't know how
lucky they are that some people in power there are not only intelligent but have
cajones...
No_Pretzel_Logic 2 hours ago
The Davos crowd is clutching most of the Western countries by the short hairs.
Yank....how does that feel, plebe?
Delta Variant Outbreak in Israel Infects Some Vaccinated Adults
Government reimposes indoor mask requirement in light of preliminary findings
The government of Israeli Prime Minister Naftali Bennett moved to reimpose some coronavirus restrictions on
Friday.
PHOTO:
KOBI WOLF/BLOOMBERG NEWS
By
Dov Lieber
Updated June 25, 2021 11:39 am ET
Listen to Article
4
minutes
00:00 / 04:25
1x
Queue
This article is in your queue.
Open Queue
TEL AVIV -- About half of adults infected in an outbreak of the Delta variant of Covid-19 in Israel were fully
inoculated with the
Pfizer
Inc.
vaccine,
prompting the government to reimpose an indoor mask requirement and other measures to contain the highly
transmissible strain.
Preliminary findings by Israeli health officials suggest about 90% of new infections were likely caused by the Delta
variant, according to Ran Balicer, who leads an expert advisory panel on Covid-19 for the government. Children under
16, most of whom haven't been vaccinated, accounted for about half of those infected, he said.
The government this week expanded its vaccination campaign to include all 12- to 15-year-olds after a jump in
infections among schoolchildren in a town in central Israel. It has since quickly spread geographically and to
other groups of the population.
Israel is now reassessing its Covid-19 regulations after moving to open up its society and economy following
multiple lockdowns last year.
"The entrance of the Delta variant has changed the transmission dynamics," said Prof. Balicer, who is also the
chief innovation officer for Israel's largest health-management organization, Clalit.
The Delta variant,
which
first emerged in India in late 2020
and is also known as B.1.617.2, has now been detected in more than 70
countries.
In
the U.S.
, public-health experts expect it to soon become the dominant strain.
DELTA VARIANT
These so-called breakthrough cases -- defined as positive Covid-19 test results received at least two weeks after
patients receive their final vaccine dose -- are broadly expected as the Pfizer vaccine is highly effective but not
100% foolproof, according to Mr. Balicer.
Israeli health officials are optimistic that even if the variant does spread, evidence from countries such as the
U.K. indicate the vaccine will prevent a large increase in severe illness and hospitalizations that plagued the
country's health system in previous outbreaks. Israel has only recorded five severe cases in the past 10 days,
Prof. Balicer said, but whether more will emerge is too early to tell.
The number of cases in Israel is relatively low by global standards. New cases of Covid-19 rose to over 200 on
Thursday from around 10 a day for most of June.
https://tpc.googlesyndication.com/safeframe/1-0-38/html/container.html
Those exempt from the mask requirement included children under seven, people with disabilities that prevent them
from wearing a mask or two workers who work regularly together. The government had canceled the indoor mask
requirement 10 days ago and dropped most other preventive measures after running one of the world's fastest
vaccination campaigns. About 80% of Israelis of age 16 and above have received two doses of the vaccine that was
developed by Pfizer and German partner
BioNTech
SE
.
The Israeli government earlier this week recommended that all 12- to 15-year-olds be vaccinated to protect
against the Delta variant.
PHOTO:
NIR ALON/ZUMA PRESS
Israel was an early
test
case for the effectiveness
of the vaccine after outbreaks last year at one point gave it one of the world's
highest per-capita infection rates. Since the start of the pandemic, 840,522 of the country's 9.3 millions
citizens have been infected, of which 6,429 died.
Israeli health officials said the highly contagious strain had likely entered the country through its main
international airport, near Tel Aviv, where a system meant to vet every new arrival through testing was overloaded
in recent days amid a surge in foreign travel.
On Wednesday, the government delayed allowing foreign nationals to enter into the country for tourism from July 1
to Aug. 1 and reimposed a mask requirement inside airports.
"Our goal at the moment, first and foremost, is to safeguard the citizens of Israel from the Delta variant that is
running amok in the world," Israeli Prime Minister Naftali Bennett said Wednesday.
Related Video
Delta Variant Likely to Spread World-Wide
YOU MAY ALSO LIKE
UP NEXT
0:00
/
1:46
1:23
Delta Variant Likely to Spread World-Wide
The Covid-19 strain known as Delta is in at least 60 countries including the U.S. and likely to spread
world-wide, Covid-19 Genomics UK Chair Dr. Sharon Peacock tells WSJ's Betsy McKay at the WSJ Tech Health event.
(Video from 6/9/21)
Corrections & Amplifications
An independent panel of experts advised the CDC and FDA to add a warning to the Pfizer and
Moderna vaccines after over 300 cases of Myocarditis have been reported and linked to the
shots. Plus, there is no evidence for the need of booster shots to defend against the virus,
NBC's Erika Edwards has the story.
Highly recommended !Notable quotes:
"... Noorchashm also called on Pfizer and Modern to institute "clear recommendations to clinicians that they delay immunization in anyone recently recovering from COVID, as well as any known symptomatic or asymptomatic carriers -- and to actively screen as many patients with high cardiovascular risk as is reasonably possible, in order to detect the presence of SARS-CoV-2, prior to vaccinating them." ..."
"... 'It's a colossal error to vaccinate people who have had prior infections, and this is totally avoidable harm we are causing. Why are we rushing to vaccinate people who we know are immune and don't stand to gain any benefit? If I do anything medically unnecessary to someone as a doctor, I'm opening them up to potential harm. If you've had a recent infection and you have viral antigens in your tissues, you can literally and immunologically cause tissue damage." ..."
"... "We know that natural SARS CoV-2 virus can affect the heart. It can cause blood clots that can lead to heart attacks and strokes and myocarditis. The virus can trigger an immune response or inflammation to the heart. Anywhere the virus goes the immune system will target that tissue and cause problems. If you've had a prior infection and you have antigens in the tissues where the virus goes, like the heart, and you activate the immune response [with a vaccine], you're going to activate damage." ..."
In an interview with The Defender, Marie Follmer said no one warned her that her 19-year-old son -- a healthy, elite athlete
who had recovered from COVID -- shouldn't get the Pfizer vaccine because it would put him at greater risk of developing myocarditis.
The Defender is experiencing censorship on many social channels. Be sure to stay in touch with the news that matters
by
subscribing to our top news of the day . It's free .
Greyson Follmer, an Ohio State University (OSU) student, was an elite athlete and member of the university's chapter of the Reserve
Officers' Training Corps (ROTC).
But, according to his mother, the 19-year-old from Ohio is looking at a very different future now, after he developed severe
heart complications following his second dose of Pfizer's COVID vaccine.
In an exclusive interview with The Defender , Marie
Follmer said nobody warned her about the potential for increased risks of COVID vaccine-related adverse events for people like her
son, who already had COVID and had acquired
natural immunity.
Greyson has played sports since he was 4 years old. He was an athlete who played in the state soccer championship in high school
and then went on to OSU and started college during the COVID pandemic. He also joined ROTC his freshman year and was very active
-- running several miles every day with heavy packs on his back.
Greyson was perfectly healthy and had no underlying conditions except for asthma -- which didn't affect his athletic abilities
-- and food allergies.
Like most students early on in the year, Greyson and his friends got COVID.
Though most had no symptoms, Greyson experienced mild flu symptoms -- though they were nothing like his post-vaccine symptoms,
Follmer explained.
The university required students who had COVID to quarantine. It also required them to get a heart MRI before they could return
to school. Follmer thought that was strange, but she made sure her son got one.
When the cardiac MRI came back it showed Greyson's heart was enlarged with slight inflammation. The cardiologist thought it could
be related to being an elite athlete, and signed a release for Greyson to return to school.
"He wasn't 100%, but he was recovering. He was able to go skiing, return to ROTC and went on spring break," Follmer said.
Follmer and her husband got vaccinated first with
Moderna . When a friend of Follmer secured appointments for the kids to be vaccinated, she drove to OSU, picked up Greyson and
told him he was going to get vaccinated.
Greyson received his first dose of
Pfizer
on April 16, and a second dose on May 7. After the first dose Greyson experienced minor symptoms, but his mother didn't connect them
to the COVID vaccine.
It was after his second dose that things really changed, Follmer said.
Greyson experienced significant symptoms shortly after his second dose. Three times he was taken to
Nationwide Children's Emergency Hospital
.
'My son feels like he's having a heart attack 24/7," Follmer said. "He now has high blood pressure, severe chest pains, back pain,
elevated kidney levels, hypothyroidism, inflamed lymph nodes in different areas of his body, and he can't work or exercise."
Follmer said Greyson feels like he's dying and has to sleep all the time. He likely won't be able to go back to ROTC and doesn't
know if he will be able to return to school in August. Greyson experienced broken feet from soccer and said nothing compares to the
chest pain he feels now.
'A perfectly healthy kid has gone downhill," his mom said.
Doctors initially attributed the heart problems Greyson experienced in May, after the vaccine, to the COVID he had in September
2020. Believing he was a "long-hauler," they referred her son to the Ohio COVID Clinic.
According to the
Harvard
Gazette , "COVID long-haulers" is a term used to describe those who continue to feel symptoms of COVID long after the expected
recovery time. Patients tend to be younger, and in some cases, initially experienced only mild symptoms.
On June 15, Greyson was taken by emergency medicine services to Ohio Health
. Follmer said she knew her son's symptoms were connected to the Pfizer vaccine, but nobody knew how to help him.
Greyson has seen numerous doctors and specialists. His family has spent more than $12,000 in one month. Lab work is covered by
insurance but his other treatments are not. Greyson is doing stem cell treatments, taking Ivermectin and numerous supplements to
support his condition.
Doctors project it will take him two years to fully recover, though there's no research or information on how to treat
myocarditis
brought on by a COVID vaccine.
In the meantime, Greyson can't mow the grass, work or go to school. He walks around holding his chest and is in counseling to
cope with the effects this has had on his life, his mother said.
Follmer said she's not an
anti-vaccine
person, especially because she has a young daughter who could get sick. None of her children had ever had reactions to vaccines.
Follmer's 11-year-old daughter is immunocompromised. Even though all of her children had been exposed to COVID, she thought she
was protecting her daughter by having her son vaccinated.
Follmer explained:
'I think what's frustrating to me right now is that nobody told me that if you have an enlarged heart or heart inflammation, don't
get the shot. Not one person ever told us this. I never would have thought in a million years my kid would get sick.
'I was ready to give my daughter the vaccine -- she is going to be 12 in August and has one lung and a reconstructive airway.
There is no way on this planet I would give her the vaccine now. Greyson's twin brother will also not be getting the vaccine after
seeing what his brother has gone through."
Follmer said no one told her about reporting her son's
adverse reaction to the Centers for Disease Control and Prevention's (CDC) Vaccine
Adverse Events Reporting System (VAERS). "If I hadn't put it on Facebook and someone hadn't told me to put it in VAERS, I would
have never known to do it."
Follmer said she has since reported her son's
adverse reaction to VAERS (ID1395886), but no one has followed up on her son's case nor has the report been added to the system.
She also tried calling the CDC to see if someone there could help them.
'I just want him better. That's the bottom line," Follmer said. I just want everyone to know -- don't be naive like I was and
think that this can't happen to your kids."
Cardiothoracic surgeon warns against vaccinating people who've already had COVID
Dr. Hooman Noorchashm, a surgeon , immunologist
and patient safety advocate, wrote
several letters to the U.S. Food and Drug Administration (FDA) shortly after the agency granted Pfizer and Moderna
Emergency Use Authorization for their COVID vaccines.
In his letters, Noorchashm urged the FDA to require pre-screening for SARS-CoV-2 viral proteins in order to reduce COVID vaccine
injuries and deaths.
Noorchashm also
called on Pfizer and Modern to institute "clear recommendations to clinicians that they delay immunization in anyone recently
recovering from COVID, as well as any known symptomatic or asymptomatic carriers -- and to actively screen as many patients with
high cardiovascular risk as is reasonably possible, in order to detect the presence of SARS-CoV-2, prior to vaccinating them."
According
to Noorchashm , it is scientifically established that once a person is naturally infected by a virus, antigens from that virus
persist in the body for a long time after viral replication has stopped and clinical signs of infection have resolved.
When a vaccine reactivates an immune response in a recently infected person, the tissues harboring the persisting viral antigen
are targeted, inflamed and damaged by the immune response.
"In the case of SARS-CoV-2, we know the virus naturally infects the heart, the inner lining of blood vessels, the lungs and the
brain,"
explained Noorchashm . "So these are likely to be some of the critical organs that will contain persistent viral antigens in
the recently infected. Following reactivation of the immune system by a vaccine, these tissues can be expected to be targeted and
damaged."
In an interview with The Defender , Noorchashm said
Greyson's case reminded him of
Everest Romney -- the all-American basketball player who was hospitalized after his second dose of Pfizer for blood clots in
his brain.
According to Noorchasm, both Romney and Greyson had acquired natural immunity because they'd been infected with COVID, and they
likely did not stand to
gain any benefit from a COVID vaccine.
Noorchashm explained:
'It's a colossal error to vaccinate people who have had prior infections, and this is totally avoidable harm we are causing. Why
are we rushing to vaccinate people who we know are immune and don't stand to gain any benefit? If I do anything medically unnecessary
to someone as a doctor, I'm opening them up to potential harm. If you've had a recent infection and you have viral antigens in your
tissues, you can literally and immunologically cause tissue damage."
Medical necessity is on the ground floor of everything doctors do in regards to safety, Noorchasm said. "If you want to be a safe
hospital, doctor, practitioner or health agency you would not do anything that's not necessary to people or fundamentally not beneficial.
There's only a probability of harm if there's no medical necessity," he said.
When asked specifically about myocarditis, Noorchashm said this is the original prediction and prognostication he made to the
FDA.
Noorchashm said:
"We know that natural SARS CoV-2 virus can affect the heart. It can cause blood clots that can lead to heart attacks and strokes
and myocarditis. The virus can trigger an immune response or inflammation to the heart. Anywhere the virus goes the immune system
will target that tissue and cause problems. If you've had a prior infection and you have antigens in the tissues where the virus
goes, like the heart, and you activate the immune response [with a vaccine], you're going to activate damage."
Noorchashm, who is pro-vaccine, said shots need to be spread out for people who are not immune and want to be vaccinated, and
the FDA and CDC should think carefully about limiting the shot to one dose, especially in young people, or increasing the duration
between first and second doses.
In his
letter to the FDA , Noorchashm recommended actively screening as many patients with high cardiovascular risk as is reasonably
possible, in order to detect the presence of SARS-CoV-2, prior to vaccinating them.
"If someone has a known history of COVID, there should not be any rush to get them vaccinated," Noorchashm said. "That should
be our national policy.
If you've either had COVID, or you have laboratory evidence of immunity, you shouldn't rush into getting vaccinated ."
On Covid, Israel, which used Pfizer vaccines, and had only last week removed indoor mask
mandates, has now reinstituted them, and is asking its citizens not to go abroad over concerns
the Delta variant is surging
A Centers for Disease Control and Prevention (CDC) safety panel said there is a "likely
association" of mild heart inflammation in adolescents and young adults after they were
vaccinated with an mRNA COVID-19 vaccine.
The
initial cases of myocarditis, inflammation of the heart muscle, and pericarditis, inflammation
of the membrane surrounding the heart, reported on the federal government's tracking system
were generally mild, especially compared to traditional myocarditis, scientists said.
Most cases have been mild, with symptoms like fatigue, chest pain and disturbances in heart
rhythm that quickly clear up within a day or so. CDC scientists said they will need to follow
up with patients in the months ahead in order to get a complete picture of the impact.
"Clinical presentation of myocarditis cases following vaccination has been distinct,
occurring most often within one week after dose two, with chest pain as the most common
presentation," said Grace Lee, chairwoman of the CDC's vaccine safety committee.
Officials said they are tracking about 1,200 initial reports of the rare heart inflammation
following doses of mRNA coronavirus vaccines have been filed with the federal government's
Vaccine Adverse Event Reporting System (VAERS), though they have not yet been definitively
linked to the vaccines.
Most reports came from people in their late teens and early 20s, and many more occurred
after the second dose than the first.
...There were more cases in males than females, and the cases essentially disappeared in
older age groups.
The agency said there have been 267 cases of myocarditis or pericarditis reported after
receiving one dose of the mRNA vaccines and 827 reported cases after two doses through June
11.
But the reports are preliminary, and do not mean the health issues have been linked to the
vaccine. The database is meant as a repository of all events observed after vaccination.
There were 323 confirmed reports of myocarditis and pericarditis for people under the age of
29, which is the group CDC is investigating. Among those confirmed, 218 people have fully
recovered. Nine people were hospitalized, with two in intensive care as of June 11, according
to the CDC.
There have been about 300 million vaccine doses administered nationwide.
Scientists have emphasized this occurrence is rate - for both mRNA vaccines combined, there
were 12.6 heart inflammation cases per million doses.
The highest confirmed rate of myocarditis and pericarditis was about 20 cases per 1 million
doses with Moderna's vaccine, compared to 8 cases per million for Pfizer's.
Officials emphasized that the benefits of vaccines outweigh the risks, and noted that for
every million doses of mRNA vaccine given, there are far more COVID-19 cases and
hospitalizations prevented compared to the number of potential myocarditis cases.
ghost of
q.mensch
June 17, 2021 at 1:37 pm GMT • 5.3 days ago
Eric Clapton shares his feelings candidly about the past year of Covid lockdown, in
this 25 min YT (06/14/21):
He talks about the flip-flops in policies and actions of British political and public
health officials throughout the the entire pandemic that frequently set off his "bullshit
radar", and:
-How he has been surprised to have been attacked/labeled a Trump supporter (within England
?!) for his public statements during the the pandemic.
-Talks about his own frightening symptoms after receiving the two-jab, AstraZeneca spike
protein-coding DNA-adenovector type experimental gene therapy vaccine agent.
It's YT, so the video may not be up for long .
Robert Dolan
June 17, 2021 at 6:13 pm GMT • 5.2 days ago
@ghost of q.mensch
Love Eric Clapton ..disturbing about his reaction to the jab.
He once gave a fabulous slightly drunken rant regarding the foreign invasion of England,
and of course he was labeled a "racist."
Fauci pushing vaccines is borderline with criminality.
TheMoon
June 16, 2021 at 3:06 pm GMT • 6.3 days ago
@Peripatetic Itch pregnant the first time, my obgyn hands me a list of common foods and
drinks to avoid, and now the government wants to inject an experimental drug into me? No
thanks. You don't even need to go to conspiracies and shadowy research for that one. I have
to avoid caffeine, but untested drug is OK?
I don't even want the J&J one (when I'm done with babymaking) even though it seems
closer to a traditional vaccine. I read it was something already existing from efforts to
develop an HIV shot, but they seem to have a recurring issues with contamination where they
manufacture it. Too many diversity hires, maybe.
On the other hand, the MSM seems to downplay the mRNA complications and overplay the
J&J ones, which is curious.
Craig Morris
June 16, 2021 at 5:44 pm GMT • 6.2 days ago
@TheMoon
J&J also creates spike proteins, it just does it with a viral vector instead of mRNA.
Sputnik and Sinovac are traditional vaccines if you can get them.
Does WHO try to fearmonger the importance of vaccination using Delta (Indian) mutation as the
"eminent threat". While that real problem is that vaccines are much less effective against this
train (although probably not to the extent South African mutation wiped out the credibility of
the first generation vaccines from the USA, especially Moderna and Johnson & Johnson (
Moderna Developing Vaccine Booster Shot for Virus Strain Identified in South Africa - WSJ
"Moderna said its vaccine induced production of neutralizing antibodies against the strain first
identified in the U.K., known as B.1.1.7, at levels comparable to prior variants. Yet
neutralization decreased sharply in the case of the strain in South Africa, known as
B.1.351,"
A weak protection against the South Africa variant suggests the flow of "total vaccination"
propaganda and clear deficiencies of several first generation vaccines.
As the mutant COVID-19 strain known as "Delta" picks up steam across Europe and the US, one
of the WHO's leading doctors has just expressed concern about recent research published in the
Lancet showing that the first generation of COVID-19 vaccines aren't as effective at protecting
against "Delta".
Answering a question from a reporter during the organization's regular Monday briefing in
Geneva, Dr. Maria Van Kerkhove said that there is data "showing a reduction in neutralization"
for the Delta variant, but not as much as the "Beta" variant - better known as the mutant
strain that was first discovered in South Africa.
play_arrow
Johnny Walker 1 minute ago
"Asking the CDC to look into vaccine safety is like asking the fox to guard the chicken
coop."-- Dr Rimland Ph.D.
Unbelievabubble 40 seconds ago
Less WHO doctor, more WITCH doctor.
Mike Rotsch 2 minutes ago
It's kinda like a never-ending Henry Kissinger interview. On one hand, we're told that
he's some kind of a genius and master of political science. On the other hand, he has
absolutely nothing but a lifetime of consistent and predictable failure to show for it.
It is not clear if Ivermectin is effective. But were are government studies on this important
topic. Where is out "vaccines zealot" Fauci and his institute results ?
Authored by Matt Taibbi
via TK News ,
On December 8, 2020, when most of America was consumed with what The Guardian called Donald
Trump's "desperate, mendacious, frenzied and sometimes farcical" attempt to remain president,
the Senate's Homeland Security and Governmental Affairs Committee held a hearing on the "
Medical Response to
Covid-19 ." One of the witnesses, a pulmonologist named Dr. Pierre Kory, insisted he had
great news.
"We have a solution to this crisis," he said unequivocally.
"There is a drug that is proving to have a miraculous impact."
Kory was referring to an FDA-approved medicine called ivermectin. A genuine wonder drug in
other realms, ivermectin has all but eliminated parasitic diseases like river blindness and
elephantiasis, helping discoverer Satoshi OÌ„mura win the Nobel Prize in 2015 . As far
as its uses in the pandemic went, however, research was still scant. Could it really be a magic
Covid-19 bullet?
Kory had been trying to make such a case, but complained to the Senate that public efforts
had been stifled, because "every time we mention ivermectin, we get put in Facebook jail." A
Catch-22 seemed to be ensnaring science. With the world desperate for news about an
unprecedented disaster, Silicon Valley had essentially decided to disallow discussion of a
potential solution" disallow calls for more research and more study" because not enough
research and study had been done. Once, people weren't allowed to take drugs before they got
FDA approval. Now, they can't talk about them.
Subscribe and read the rest of the post
here .
play_arrow
Dabooda 6 hours ago
If Ivermectin is ever recognized as effective against the Wu-flu, all the "vaccines"
will become illegal. They are ONLY authorized for emergency use because no other safe and
recognized treatment is available. So the pharmaceutical companies will pull out all the
stops to prevent that happening. Expect a new article in The Lancet any day now, "proving"
that it doesn't work.
chumlee 5 hours ago
Exactly!!
Pinto Currency 3 hours ago
Breakthrough: Ivermectin Inhibits Covid Spike Protein Binding
https://principia-scientific.com/breakthrough-ivermectin-inhibits-covid-spike-protein-binding/
" Ivermectin... has shown great efficacy in the fight against covid-19. For the first
time, medical researchers have documented how ivermectin docks to the SARS-CoV-2 spike
receptor-binding domain that is attached to the ACE2 receptor."
ClimbingTheLog 5 hours ago remove link
the Lancet may well do that but c19ivermectin.com has a hundred studies now showing the
Lancet as being part of the coverup.
Demologos 4 hours ago
Great video discussing several treatments including Ivermectin. Of course, it's already
pulled from YouTube, after nearly 600K views, but it can be found on odysee.com .
Dr. Bret Weinstein ( Dark Horse Podcast) is the moderator with Dr. Robert Malone (one of
the inventors of mRNA vaccine technology) and Steve Kirsch. Search "how to save the world
in three easy steps". Video is 3 hours but well worth your time.
h/t to a ZH commenter a few days ago.
Demologos 4 hours ago
Ivermectin peer-reviewed meta study released today. Dr. Tess Lawrie.
https://www.researchgate.net/publication/348297284_Ivermectin_reduces_the_risk_of_death_from_COVID-19_-a_rapid_review_and_meta-analysis_in_support_of_the_recommendation_of_the_Front_Line_COVID-19_Critical_Care_Alliance_Latest_version_v12_-_6_Jan_2021
philipat 3 hours ago (Edited)
More importantly, had Ivermectin and HCQ (As well as prophylactic Vitamnin-D
supplementation in the Northern Hemisphere) been approved as (effective, cheap and AE-free)
treatments for "Covid" under the laws of many countries, especially the US, it would not
have been possible to approve the experimental gene therapies under the EUA mechanism.
Which would, of course, have scuttled the entire profitable psyop.
LetThemEatRand 6 hours ago
Your answer is clearly the correct one (vaccine would not be allowed if there are
effective treatments). Guys like Taibbi can't accept that obvious and correct explanation
for the question in his article, because doing so means admitting that there is a vast
conspiracy going on regarding COVID. So he will only entertain stupid answers like "well,
Trump said it was effective, therefore people said it wasn't." This is already what we're
hearing with regard to the Wuhan lab.
RedDog1 7 hours ago
Big tech = Ministry of Truth.
paranoid.dragon 7 hours ago
Big Tech = created by Pentagon
Not Your Father's ZH 7 hours ago (Edited) remove link
The Real Anthony Fauci: Bill Gates, Big Pharma, and the Global War on Democracy and Public
Health
Dr. "Follow The Science" Fauci controls a $7 billion budget that uses vaccines as
weaponry. Kennedy Jr. discloses that the chronic disease rate in the US in 1968 when Fauci
became director of the Institute of Infectious Disease was 6% and now is 54%. Fauci turned
his agency into an incubator of prescription drugs and vaccines. His agency has a financial
conflict of interest in vaccine patents.
Fauci runs a medical dictatorship, says Kennedy. Fauci gives away 13 times more money
than billionaire Gates.
edotabin 5 hours ago remove link
The EUA cannot be given if there are alternatives. Of course they knew. How do I
know?
1. World famous French scientist (Raoult) notices hydroxychloroquine works and starts
speaking about it. Lancet publishes false study stating the opposite. They eventually are
forced to retract study. They continue to give the medication to very late- stage patients
and gave wrong doses so as to purposely continue to discredit its effectiveness. Sales of
drug banned in Europe and Dr. Raoult goes from being world-renowned to invisible. Many
pharmacists in the US refuse to fill prescriptions.
2. Ivermectin shows fantastic results in India and elsewhere. Numbers start dropping
like a rock. The situation is stabilized. What happens? Ivermectin is bad-mouthed and in
some areas of India it is banned. As a matter of fact, read this:
https://www.thedesertreview.com/opinion/columnists/indian-bar-association-sues-who-scientist-over-ivermectin/article_f90599f8-c7be-11eb-a8dc-0b3cbb3b4dfa.html
In 1954, annual births first topped four million and did not drop below that figure until
1965, when four out of ten Americans were under the age of 20. Mid-20th century baby boom -
Wikipedia
E5 6 hours ago
20% more babies were born in 1946 than in 1945.
State for the record which two years you believe there will be 20% more dead boomers
than the year before.
Then contemplate the truth about that.
Trade accordingly... and factor in what the government will do with that crisis. Truth?
or Control?
Actually heard about lung transplant for a young woman during waping epidemic.
As scientists start to assess the impact that COVID-19 has had on patients and the American
medical system more broadly,
Bloomberg reports that hospitals across the US have seen a surge in patients receiving
single- and double-lung transplants.
Transplants are necessary for only the most serious COVID-19 cases. In these patients -
pretty much always patients with comorbidities - COVID-19 ravages the lung tissue, leaving
nodules in the lungs incapable of absorbing oxygen from the air and transmitting it to the
blood stream. For many patients, the grueling procedure may be the only solution after
experiencing the worst lung damage caused by the virus - when the body fails to properly
respond to, and heal from, the hyper-inflammatory response provoked by COVID-19.
... ... ...
Fortunately, COVID-19 vaccines supposedly offer "100% protection" against "severe" COVID-19
symptoms. Though patients with comorbiditis may still be at risk as variants like the "delta"
strain continue to spread.
DanishViking 7 hours ago (Edited)
Fear mongering article sourced from Bloomberg (surprised?), pushing the jab
narrative
ohm 4 hours ago
If your dumb enough to believe the vaccines are 95% or 100% effective against anything,
I have a bridge in Brooklyn to sell you.
https://www.thelancet.com/action/showPdf?pii=S2666-5247%2821%2900069-0
Although the RRR considers only participants who could benefit from the vaccine, the
absolute risk reduction (ARR), which is the difference between attack rates with and
without a vaccine, considers the whole population. ARRs tend to be ignored because they
give a much less impressive effect size than RRRs: 1·3% for the
AstraZeneca–Oxford, 1·2% for the Moderna–NIH, 1·2% for the
J&J, 0·93% for the Gamaleya, and 0·84% for the Pfizer–BioNTech
vaccines.
bigjim 2 hours ago remove link
Fortunately, COVID-19 vaccines supposedly offer "100% protection" against "severe"
COVID-19 symptoms.
Really? Last I heard, some 30% of the people who have been dying here in the UK had
received both jabs.
Dr. Know 3 hours ago (Edited)
"...severe lung damage that did not improve despite prolonged mechanical
ventilation"
A number of RNs and MDs have stated that the ventilators cause this damage, especially
when turned up too high.
krda 1 hour ago
Bingo. 85% of Covid patients put on ventilators in China died. Something like 50% of
people put on ventilators for any cause die.
The damage was caused by the rush to 'ventilators! ventilators! ventilators!' rather
than using other treatments which wouldn't have killed them.
Countrygirl1411 2 hours ago
Seems they left out what has happened to one young person because of the covid
injection
19-Year-Old College Freshman Dies From Heart Problem One Month After Second Dose of
Moderna Vaccine
https://childrenshealthdefense.org/defender/19-year-old-dies-heart-problem-moderna-vaccine/
kjm 1 hour ago remove link
Agreed, watch Dr. (cardiologist) Peter McCullough testifying to the Texas Senate.
Essentially he said 85% didn't have to die if treated early and properly. Lung damage would
have been avoided as well. I would add massive (30-50 grams, initially and repeated daily
until symptoms alleviated) doses of IV vitamin C to the protocol. IV C has been used
successfully for more than 70 years on Polio and other viruses. Look up Dr. Klenner.
As I have described before for
Forbes
,
your myocardium is a term for your heart muscles because "myo"� stands for "muscle"� and "cardium"� stands for "heart."� Your
pericardium is the thin membranous sac that surrounds your heart. The suffix "-itis"� stands for being "inflamed."� Therefore,
myocarditis means that your heart muscles are inflamed. Pericarditis means that your sac is inflamed, the sac around your heart that
is.
Typically, you don't want any parts of your heart to be inflamed, unless it is just some kind of metaphor for love. Inflammation can
interfere with your heart's ability to pump blood to the rest of your body and lead to abnormal heart rhythms as well. While milder
cases can resolve without longer-lasting problems, such conditions could lead to more severe, long-lasting, and even
life-threatening consequences. So myocarditis or pericarditis shouldn't be like a mild case of indigestion. You shouldn't say during
a date, "oh, it's nothing. Just my myocarditis acting up. What do you want to do after we've finished this pile of oysters?"�
In June 10 presentation to a U.S. Food and Drug Administration (FDA) advisory committee
, Tom Shimabukuro, MD, MPH Deputy
Director of the CDC's Immunization Safety Office, summarized reports of these conditions from the Vaccine Adverse Event Reporting
System (VAERS) as of the end of May. Maintained by the U.S. Department of Health and Human Services, the VAERS allows anyone to
enter a report of a problem after getting a vaccine, any vaccine. Note that this vaccine safety system accepts all reports from
anyone. So in theory, you could report that you became a pink unicorn after receiving the Covid-19 vaccine. That's why all reports
ultimately need to be reviewed and vetted by medical experts before being taken seriously. For example, you'd have to prove that you
are indeed a pink unicorn and that there isn't some other obvious reason for your transformation.
As of May 31, 2021, the VAERS had 789 reported cases of myocarditis or pericarditis in people after they've received doses of either
the Pfizer/BioNTech or the Moderna Covid-19 vaccine. Most (573) of these reports were from after the second dose. The median times
to first noticing symptoms was three days after the first dose and two doses after the second dose, meaning that half of the time
symptoms started within a few days of vaccination. Although there were reports of symptoms starting as far as 33 days after the
first dose and 80 days after the second dose.
Over half (475) of the 789 reported cases have been among those 30 years and younger. However, so far, only 226 of the 475 cases
have met the CDC working case definition, meaning that they indeed seemed to be legitimate cases of myocarditis or pericarditis
after the vaccination event. Most (81%) of these cases have had a documented full recovery. The rest either have ongoing symptoms or
currently lack follow-up information to determine what's happened.
Of course, this still doesn't mean that all 226 cases were caused by the vaccines. But the 226 is higher than the number of cases
that you'd expect among this age group if you just account for other possible causes of myocarditis and pericarditis. As Paul A.
Offit, MD,
the
Director of the Vaccine Education Center and a Professor at Children's Hospital of Philadelphia
, explained in the following
video, a number of different viruses can cause myocarditis and many of these tend to circulate during the Spring:
https://embedly.forbes.com/widgets/media.html?src=https%3A%2F%2Fwww.youtube.com%2Fembed%2Ffh3zTC9o6y8&display_name=YouTube&url=https%3A%2F%2Fwww.youtube.com%2Fwatch%3Fv%3Dfh3zTC9o6y8&image=http%3A%2F%2Fi.ytimg.com%2Fvi%2Ffh3zTC9o6y8%2Fhqdefault.jpg&key=3ce26dc7e3454db5820ba084d28b4935&type=text%2Fhtml&schema=youtube
In fact, as mentioned earlier, one of the viruses that could cause myocarditis or pericarditis is the Covid-19 coronavirus.
As
described by a recent publication in
JAMA
Cardiology
, a study used cardiac testing to screen competitive athletes in the Big 10 conference who had Covid-19 for any
evidence of myocarditis. When just checking for symptoms and not using cardiac magnetic resonance imaging (MRI), 0.31% ended up
being diagnosed with myocarditis. Adding cardiac MRIs bumped this number up to 2.3%, meaning that many athletes had myocarditis
without having noticeable symptoms.
So keep these numbers in mind when looking at the myocarditis cases after vaccination against Covid-19. A total of 226 cases after
vaccination would still make such events very rare and lower than the numbers that might be expected after a Covid-19 coronavirus
infection. After all, over 4.85 million doses of the Pfizer/BioNTech vaccine and over 4.03 million doses of the Moderna vaccine had
already been administered by May 29. Using your abacus and finger and toes to make the appropriate calculates would yield rates of
about 2.8 cases of myocarditis or pericarditis per one million first doses administered and 16.1 cases per million second doses
administered. Again this is like beef cooked at 120 to 130º F, still quite rare.
Still, though, this situation merits further investigation. Again, myocarditis or pericaditis are not just "dust yourself off and
walk it off"� conditions. If you have symptoms of either condition such as chest pain, rapid or abnormal heart rhythms, shortness of
breath, or swelling of your legs, ankles and feet, contact your doctor as soon as possible. Of course, these should be unexplained
symptoms. So momentary heart palpitations after seeing BTS or a bowl of mac-n-cheese may not count.
For the upcoming ACIP meeting
, you do have the opportunity to submit written comments by June 18, 2021, or submit a request to
make an oral comment at the meeting no later than 11:59 p.m., EST, on June 16, 2021
.
Of
course, just because you submit a request doesn't mean that you be allotted the up to three minutes to speak at the meeting. The CDC
will have to determine how many of the requests are legitimate versus the "how do I order a hamburger"� or "keys seem to stick to my
head after vaccination, what are you going to do about it"� comments that are unverifiable and not related to the topic at hand. Of
the requests that seem to fall within the scope of the meeting, CDC will conduct a lottery to determine who will be able to speak.
After all, time will be limited.
At this point, just because the CDC is investigating these cases doesn't mean that you should not get vaccinated. Again myocarditis
and pericarditis have been rare occurrences. No one has established cause and effect yet. It remains to be seen whether there were
other possible reasons behind the myocarditis and pericarditis cases.
Nevertheless, once again, the CDC and FDA must take all potential serious adverse events seriously. Otherwise, the risk is losing
the public's trust.
The Pfizer and BioNTech
SE shot is 96% effective against hospitalization after two doses, while the AstraZeneca and
University of Oxford Covid inoculation is 92% effective, according to an analysis announced
Monday by Public Health England. Those results are comparable with the protection offered
against the alpha variant, which first emerged in Britain, the data show.
...
Findings in May showed the effectiveness of both vaccines against symptomatic disease from
the delta variant was 33% three weeks after the first dose.
That study found the Pfizer shot was 88% effective two weeks after the second dose, and
that two doses of the AstraZeneca vaccine were 60% effective.
Mulga
Mumblebrain June 13, 2021 at 10:10 pm GMT
• 8.3 hours ago
@SteveK9
Japanese research showed that the Pfizer lipid nano-particle package, presumably with its
mRNA cargo intact, did NOT remain in situ in the deltoid muscle, but within hours had spread
via the circulation to most of the body, including bone marrow, and, most markedly, the
ovaries.
Diversity
Heretic June 10, 2021 at 12:01 pm GMT
• 3.8 days ago
My understanding is that Sputnik is an adenovirus vector vaccine, not really a
"traditional" vaccine. The Chinese vaccine is a traditional attenuated virus vaccine and
there is a SANOFI protein fragment vaccine in Phase III trials, which I think also uses a
proven technology. While I think that Sputnik is better than the messenger RNA genetic
treatments, which creep me out, I still prefer to wait for more traditional vaccines to be
approved, if I have to be vaccinated at all.
But why design a biological weapon that works best against the elderly and already
infirm?
Stephane June
10, 2021 at 12:59 pm GMT • 3.7 days ago
Sputnik V is a traditional vaccine
Actually, no.
It is an adenovirus viral vector vaccine – a "neutered" adenovirus is used as a
vector to inject DNA coding for viral proteins in the cells and make them produce/present
them to the immune system. In fact it's somewhat similar to what Pfizer or Moderna do with
lipidic nanoparticules as vector and mRNA as "source code" for protein synthesis.
This vaccine technology is fairly recent and IIRC only used in four CODID-19 (Suptnik V,
AstraZenecca, J&J and one of the Chinese vaccines – maybe two) and two Ebola
vaccines.
If you want "traditional", you should look into the sub-unit – for the moment it's
Russian EpiVacCorona and CoviVac – or inactivated virus based vaccines, IIRC chinese
only for the moment.
SteveK9 June
10, 2021 at 1:29 pm GMT • 3.7 days ago
The primary goal of the response to SARS-Cov-2 was to have everyone in the World forced to
have a vaccine on a regular basis. The lies reached mountainous proportions.
I am no more interested in Russia's vaccine than anyone else's. Perhaps it will prove to
be somewhat safer, although it also directs the patients cells to produce the spike protein.
Perhaps it is not as likely to go everywhere, including the circulatory system, which may
make it safer.
But, I see no reason for vaccines for anyone under 70, and for those over 70 and everyone
else there are effective treatments, like HCQ and Ivermectin the ban on these will probably
end someday, just like the ban on discussing the origins of SARS-Cov-2.
Ultrafart the
Brave Website June
10, 2021 at 2:56 pm GMT • 3.6 days ago
@SteveK9 n the Corona
Chan bug.
Corona Chan "Vaccines" Kill Lots & Lots of People
( https://www.bitchute.com/video/bSxEe9RS0P29/
]https://seed163.bitchute.com/2dPYYSnBMwXp/bSxEe9RS0P29.mp4
]
(
https://freenations.net/record-vaccine-deaths-risk-greater-than-covid-governments-manipulate-data-illegal-tracking-of-vaccinated-illegal-propaganda-covid-fascists-revealed/
]
Levtraro June
13, 2021 at 7:08 pm GMT • 11.3 hours ago
@Ultrafart the Brave he
"spike protein", they actually inject it directly, encapsulated in said adenovirus envelope.
You may be misunderstanding how adenovirus vector vaccines work. You are right that these
vaccines do not instruct human cells to synthesize the protein (as mRNA vaccines do) but they
are not delivering the protein directly, what they do is to carry the gene that synthesizes the
protein, the gene is carried in the genetic make up of the adenovirus. The foreign gene is
inserted into the adenovirus. Usually a crucial gene for replication of the adenovirus is
replaced (gene swapping) with the foreign gene that synthesizes the protein of interest
rendering the adenovirus impotent.
Lung scarring (
Score: 1 , Informative)defovil901 ( 7969846 ) on Thursday June 10, 2021
@05:28PM ( #61474844 ) Covid
causes lung scarring and heart and organ failure. Wear a mask and get vaccinated!b!bb
Reply to This Share Flag as Inappropriate 2 hidden comments Re:Lung scarring (
Score: 5 , Interesting)clovis ( 4684 ) on Thursday June 10, 2021 @07:02PM (
#61475072 )
Covid-19 also causes pericarditis in a small number of the people infected.
The problem with the data is that we have no ways of knowing how many of those people had been
exposed to coronavirus in the weeks before getting the vaccine, or were people who had the
long-term covid-19 problem.
Here is a case of someone for whom pericarditis was the only symptom of infection.
https://casereports.bmj.com/co...
[bmj.com]
Reply to This Parent Share Flag as Inappropriate Re:Lung scarring (
Score: 5 , Interesting)im_thatoneguy ( 819432 ) on Thursday June 10, 2021
@07:57PM ( #61475206 )
Pericarditis or worse. I have a friend who had to have open heart surgery and then died
almost a year later. Covid ate his heart. He was young too.
Reply to This Parent Share Flag as Inappropriate Re:
Definitely false, at least for COVID, can't comment about the vaccine but I strongly suspect
it doesn't apply there. There are multiple cases of people who were perfectly healthy that
ended up with severe pulmonary fibrosis, requiring a lung transplant, solely because of COVID.
If the patient wasn't otherwise healthy before getting COVID, odds are super high that they
wouldn't have even been eligible for transplant anyways as they likely would not even survive
the surgery.
Here's a case of a firefighter in p Re:
https://mediabiasfactcheck.com...
[mediabiasfactcheck.com]
seems to like them
Azfamily.com is the joint website for KTVK and KPHO television stations based in Phoenix,
Arizona. The website covers local news, sports, weather, entertainment, crime and TV
programming information.
Factual Reporting: HIGH
Overall, we rate azfamily.com Least Biased based on balanced story selection and minimal
editorializing. We also rate them High for factual reporting due to proper sourcing and a clean
Re:
Anecdotes aren't scientific proof of anything. There are super-healthy firefighters and
special ops soldiers falling dead of coronary and lung disease all the time. I had a family
member like that, died at the age of 30 due to an unknown and underlying heart condition,
super-fit, was just sitting in the sun one afternoon and dropped dead. You don't need an
underlying heart condition...
Any serious disturbance of the immune system homeostasis may result with a secondary
streptococcal infection of the heart muscle - i.e. inflammation of the heart muscle.
I've had that twice.
Once due to influenza resulting in a high fever, as a teenager.
The night of the fever I could barely catch my breath to speak and in the morning mom had to
take me by the hand to the local health center which was literally down the road from us.
Ended up in the hospital for couple of weeks as doctors kept Did they cut
corners? (
Score: 1 , Troll)klipclop
( 6724090 ) on Thursday June 10, 2021 @05:29PM ( #61474852 ) I'm
noticing the "rare" cases of side effects are due to lack of data. Then once they actually
review, it becomes less rare. I always thought drug approval processes were because large drug
companies cut corners and lie in order to get drug approval. This pandemic was a once in a
lifetime occurrence and drug reviews should go back to the original process.
Reply to This Share Flag as Inappropriate Re: Did they cut
corners? (
Score: 3 , Informative)KamikazeSquid ( 3611985 ) on Thursday June 10, 2021
@05:32PM ( #61474856 ) Drug
and vaccine review processes are only ever tested on otherwise healthy people who aren't taking
other medications or have other pre-existing health conditions. They don't really know if the
latest drug or vaccine is going to cause negative side effects in certain subgroups of people
until they actually roll it out.
Reply to This Parent Share Flag as Inappropriate
2 hidden comments Re: Did they cut
corners? (
Score: 5 , Informative)dirk (
87083 ) < [email protected] #61475608 )
Homepage
I can't speak to the vaccine review process, but this is completely false for the drug
review process. I would in the drug research sphere (I'm in IT, but I have been in it for over
20 years so I know how it works) and you are 100% incorrect. Phase 1 trials are conducted on
healthy people. These are usually first in man studies looking for any side effects from the
drug, so they want healthy people who are not on other medication. It then goes on to phase 2
trials, which are designed to see if the drug works. So if it is a high blood pressure drug, it
is given to people with high blood pressure to see if the drug actually works and does what
they want it to. These people are often on other medications. There is not a requirement they
not be on other medications unless they know of negative interactions or the other drugs also
may do something similar to the drug they are testing (which means the results could be
skewed). Then the drug goes onto phase 3 trials which compare the drug to other drugs used for
the same thing to see if the new drug performs better.
So as you can see, no, drugs are not "only ever tested on otherwise healthy people who
aren't taking other medications or have other pre-existing health conditions". It is true they
cannot test the interaction witha ll other drugs or conditions, since that would be practically
impossible, but the idea that drugs are not tested on people with any other conditions is
completely wrong.
Reply to This Parent Share Flag as Inappropriate Re:
Actually, no. But for rare side-effects, there is only "phase 4" testing, i.e. you vaccinate
the target population and check what happens. The numbers from the article are too low to be
found in any systematic test, simple statistics already gives you that. Nobody can run a drug
test on about 10M people and that is what you would need here. Re:Did they cut
corners? (
Score: 5 , Insightful)Xest (
935314 ) on Thursday June 10, 2021 @05:47PM ( #61474896 )
I don't think so; typically medicines are always updated post approval when they're in the
open market and new side effects are found because realistically if you're talking about a 1 in
500,000 issue the ability to even get 500,000 test subjects for most medicines is flat out
impossible because a lot of the time you're talking about medicines for conditions that there
just aren't even that many people suffering from it at any given time. The only reason it's
making headlines this time is because we're talking about medicines that everyone is getting,
so those rare case are, in absolute numbers, more obvious.
If you have a vaccine for something that isn't given as broadly, it's possible you'd simply
never see such rare outcomes even though they're theoretically possible. So this isn't really a
function of lack of testing prior to release as it is business as usual making headlines
because it's relevant to everyone. If for example rabies, or Japanese encephalitis vaccines had
side effects like this you wouldn't expect the UK's medicines regulator to even notice because
the rarity with which those vaccines are given out in the UK is small, but that doesn't mean
that rare side effects not found during testing like this aren't a possibility.
IMO it's only really an issue when for example as with the AZ vaccine the British government
tried to bury it out of nationalist pride - first by saying it wasn't a real issue and Europe
as just bitter about Brexit, then lying and saying it's only a 1 in 1 million chance, before
finally admitting a few weeks back it's a 1 in 60,000 chance of getting a blood clot and
effectively, in real terms, phasing out the AZ vaccine in the UK because no one else after that
point is now getting it in the UK other than for second doses.
So all we're really doing here is seeing everything happen at high speed - whereas with many
vaccines or medicines it might take many years before millions of people are treated with them
for enough cases of a rare side effect to be noticed, here we're just seeing it in a much
shorter time frame - that's not because rushing it has made things less safe, it's just made
issues that are typically noticed over years or even decades in classically vetted medicines
get noticed within months instead because of the sheer numbers involved.
Reply to This Parent Share Flag as Inappropriate
2 hidden comments Re:
> Sure but that's a function of what people like Trump have done to politics
Wait, now we're blaming Trump for making politics political?
Time to close up shop... I've literally seen it all. Re:Did they cut
corners? (
Score: 5 , Insightful)The Wily Coyote ( 7406626 ) on Thursday June 10,
2021 @07:30PM ( #61475140 )
The parent isn't blaming Trump and those of his ilk for making politics "political". He/She
is blaming them for making politics a completely toxic winner take all game where those you
disagree with are enemies. Trump didn't start this trend (arguably it goes back to the 1960s),
but he did accelerate it.
Politics can be about thoughtful compromise, but that requires a certain kind of politician,
one who is in very short supply in the current political climate in the US.
Reply to This Parent Share Flag as Inappropriate Re:
It's really not our ex-president (who lost .. and lost and lost.. he's really one of
the biggets losers ever).
It started with Mitch McConnell and the republican senate in 2007 when they told
incoming VP Biden, the republicans intended to vote "no" to everything Obama proposed- even if
they had proposed it themselves under bush.
McConnell and what's left of the republican party (most the sane conservatives have
left now) are a real threat to our democratic republic.
Re:Did they cut
corners? (
Score: 4 , Interesting)Bongo
( 13261 ) on Friday June 11, 2021 @07:43AM ( #61476292
)
Simply, if you test by giving it to 10,000 but the adverse event happens in 1 in
12,000, you probably won't see it. And if adverse events just end up sporadically reported,
maybe or maybe not, and just go undiagnosed, who knows when you'll see it.
This is why, regardless of politics, beliefs, pro/anti-vax, etc., the only real test
of what will happen to 100,000,000 people is when you give it to 100,000,000 people (and then
pay very close attention). We're not firing projectiles which follow precise mathematical laws,
these are living systems.
Vaccine companies are like, you want to give this to hundreds of millions of people?
Fine, we want complete absence of liability. You want to advise the public that it is safe?
Fine, say what you want, make sure we can never be sued, because we can't humanly know what
will actually happen when you roll it out en masse. We can't and it would be irrational and
unreasonable to expect that we could.
This is pure empiricism--safe vaccines are known safe because they're been out there
for may years, decades even, and been given to hundreds of millions. Safe because we know from
experience, not because we extrapolated from small tests and principles. Actually a lot of the
scares around vaccines are from theoretical ideas, i.e. still science, just difference of
opinions. ("anti-vax" plays on the notion that they're all quacks, but it is easy to pay
attention and find all the ones which have impressive credentials -- it is intellectually
honest to try to find the best and most qualified people on the opposing side, rather than just
point to the worst).
The technology is amazing. mRNA as a platform is an amazing technology. Imagine you go
to the doctor, and they diagnose something, and they just tap a few keys on the PC, and a
machine prints some molecules into a solution, and they inject you right there and
then--replacing pills, chemo, radiation, you name it. Totally customised health treatments
which your body can manufacture itself. As they say on their website, it is an operating system
with many potential apps to run on it.
But there's no magic crystal ball to substitute for real world, give it to a billion
people, and wait 100 years to study the long term effects. Unless you think you're god. If you
want to play god, you can say, well let's just give it to everyone--we think it'll probably be
ok, based on data so far, and we can fix the bugs later.
Reply to This Parent Share Flag as Inappropriate Re:Did they cut
corners? (
Score: 5 , Insightful)UnknowingFool ( 672806 ) on Thursday June 10, 2021
@05:51PM ( #61474904 ) There
have been 226 cases of these side effects out of 140M+ persons vaccinated in the US. Your
explanation for rare occurrences of side effects: "Those drug companies must have cut corners
or lied!" How about the 0.00016% chance of the side effect is by definition of the word "rare"?
Reply to This Parent Share Flag as Inappropriate Very possible many are
not reported Re: Re:
Just wait until they find out the fatality rate of Aspirin. ›
Re: Did
they cut corners? (
Score: 3 , Insightful)Trailer Trash ( 60756 ) on Thursday June 10, 2021
@11:24PM ( #61475662 )
Homepage
Imagine if he found out about car accidents or lightning strikes. Get the vaccine,
people.
Reply to This Parent Share Flag as Inappropriate Re:Did they cut
corners? (
Score: 5 , Informative)im_thatoneguy ( 819432 ) on Thursday June 10, 2021
@08:06PM ( #61475220
)
Wildtype Covid has an overall Infection Fatality Rate of about 0.8% in the US (based
on our age/demographics).
With the latest variants such as Delta (Indian) you're needing about 80-90% immunity
to stop the spread. And that's assuming it wouldn't mutate further with that high of levels of
infection.
0.008 IFR * 140 million Americans have now been fully vaccinated * 0.8 herd immunity
factor * 0.9 vaccine effectiveness. = 800,000 deaths have been prevented by the
vaccines.
3 people of those 140 million vaccinated Americans have gone into the ICU for
treatment. 0 have died.
Even if all 3 die... even if those 3 are 1% of the actual number who developed
problems in died. Even if you wildly inflated the assumptions about how many will die you're
looking at 300 deaths vs 800,000 deaths.
What they're going to do is review the data and confirm that everybody receiving a
vaccination is still less likely to die from the vaccine than Covid or if there are any groups
they should carve out to not be recommended to receive vaccine. If it's only a problematic side
effect in people with families who have a history of severe heart disease and if you're under
18 and have no risk factors for severe covid side effects they might say "Ok this 1% of the
population should take the vaccine, but they should carefully monitor their
condition."
U.S. public health advisers will meet to discuss a potential link between Covid-19 shots
that use messenger RNA technology and heart inflammation after hundreds of vaccinated people
experienced a condition called myocarditis.
The Centers for Disease Control and Prevention's Advisory Committee on Immunization
Practices will gather on June 18 to discuss an increase in reported cases of the condition,
particularly among adolescents and young adults. Covid vaccines made by Moderna Inc. and
partners Pfizer Inc. and BioNTech SE's use mRNA technology.
KEEP READING
Rural Philippines pays price for ignoring COVID warnings The politics of Japan's Taiwan vaccine
donation Biden announces "˜no strings attached' global vaccine donation US government
workers can return to office without COVID jab
Since April, the CDC has seen a spike in reports of myocarditis along with pericarditis, an
inflammation of the membrane around the heart. The cases, while rare, have occurred mostly in
male teens and young adults.
The CDC has identified a total of 216 cases of heart inflammation after the first dose of an
mRNA shot, and another 573 cases after the second dose. The median age of people with
myocarditis or pericarditis following the first dose was 30, and 24 among the second-dose
cases. There were 475 cases identified among those under the age of 30.
Most patients have responded well to treatment and rest, according to the agency, and more
than 8 in 10 have had full relief from their symptoms. The agency is further examining the
cases by age.
About 130 million Americans have received the full two-dose regimen of one of the two
authorized mRNA vaccines. Many teenagers have now received their first dose of the
Pfizer-BioNTech vaccine, which was cleared for adolescents 12 and older on May 10.
"We're still learning about the rates of myocarditis and pericarditis," Tom Shimabukuro, a
safety expert of CDC's National Center for Emerging and Zoonotic Infectious Diseases, said
Thursday in a Food and Drug Administration panel meeting. "As we gather more information we'll
begin to get a better idea of the post-vaccination rates and hopefully be able to get more
detailed information by age group."
Shimabukuro said the U.S. data is consistent with findings from Israel's vaccinated
population.
"It's hard to deny that there's some event that seems to be occurring," said Cody Meissner,
head of the Pediatric Infectious Disease Division at Tufts Medical Center, at the FDA's
advisory committee meeting on Thursday.
\
Notable quotes:
"... one in 10 current cases had caught the variant of the virus now spreading in Victoria from a stranger. ..."
Genome sequencing has confirmed the cases in Victoria are from the variant that was first
detected in India.
Merlino said in a separate statement on Wednesday that authorities had discerned that
one in 10 current cases had caught the variant of the virus now spreading in Victoria from
a stranger.
Can't wait for Fauci's next round of explanations.
You_Cant_Quit_Me 21 minutes ago
Will insurance companies charge higher life insurance premiums to those who were
vaccinated?
Kelley 28 minutes ago (Edited)
It's the CDC's version of the Plunge Protection Team.
If anyone assumes the 'emergency' is about protecting the public, this is my message to
you: harharharharhar!
Divide_And_Conquer 38 minutes ago remove link
Satanists must be eliminated at all costs
Just a Little Froth in the Market 6 minutes ago
"Another 1,260 were reported in people 65 or older through claims data from Medicare
claims data. Neither number raised safety signals, Steve Anderson, director of the FDA's
Office of Biostatistics and Epidemiology said."
Of course there were no safety signals. Nothing's more important than Joetard reaching
his July 4th goal
on target 34 minutes ago
Why is the CDC even recommending this vaccine for the young, the immune, and those with
antibodies. Unethical. Unscientific. No bang for buck. Why wait a week. Why not meet
tomorrow. Answer--it takes a week to get their cover stories together. Zero confidence now
in the CDC and anything they say. It is all political Science.
Notable quotes:
"... Dr. Makary is a professor at the Johns Hopkins School of Medicine, Bloomberg School of Public Health and Carey Business School. He is author of "The Price We Pay: What Broke American Health Care""and How to Fix It," just out in paperback. ..."
The news about the U.S. Covid pandemic is even better than you've heard. Some 80% to 85% of
American adults are immune to the virus: More than 64% have received at least one vaccine dose
and, of those who haven't, roughly half have natural immunity from prior infection. There's
ample scientific evidence that natural immunity is effective and durable, and public-health
leaders should pay it heed.
Only around 10% of Americans have had confirmed positive Covid tests, but four to six times
as many have likely had the infection. A February study in Nature used antibody
screenings in late summer 2020 to estimate there had been seven times as many actual cases as
confirmed cases. A similar study , by the University of Albany and New
York State Department of Health, revealed that by the end of March 2020""the first month of New
York's pandemic""23% of the city's population had antibodies. That share necessarily increased
as the pandemic spread.
The contribution of natural immunity should speed up the timeline for returning fully to
normal. With more than 8 in 10 adults protected from either contracting or transmitting the
virus, it can't readily propagate by jumping around in the population. In public health, we
call that herd immunity, defined broadly on the Johns Hopkins Covid information webpage as
"when most of a population is immune." It's not eradication, but it's powerful.
Without accounting for natural immunity, we are far from Anthony Fauci's stated target of
70% to 85% of the population becoming immune through full vaccination. But the effect of
natural immunity is all around us. The plummeting case numbers in late April and May weren't
the result of vaccination alone, and they came amid a loosening of both restrictions and
behavior.
In Los Angeles, 45% of city residents were found to have antibodies in February. Once
vaccines were introduced, the seven-day average of daily Covid cases fell from a peak of more
than 15,000 on Jan. 11 to 253 four months later, even as people became more mobile. That sharp
decline, which came far faster than health officials expected, can't be accounted for by
vaccination rates, which were below 50% during that time.
Natural immunity is durable. Researchers from Washington University in St. Louis reported last month that
11 months after a mild infection immune cells were still capable of producing protective
antibodies. The authors concluded that prior Covid infection induces a "robust" and "long-lived
humoral immune response," leading some scientists to suggest that natural immunity is probably
lifelong. Because infection began months earlier than vaccination, we have more follow-up data
on the duration of natural immunity than on vaccinated immunity.
Washington University's lab findings are consistent with physicians' bedside observations.
After treating Covid for 16 months, we haven't seen significance incidence of re-infection. In
Italy no re-infection clusters have been observed . In a
large study
from Denmark, less than 0.7% of people who tested positive for Covid, including those who were
asymptomatic, ever tested positive again""a "breakthrough infection" rate similar to that of
vaccines. These numbers are especially low considering the sensitivity of Covid PCR tests,
which can sometimes detect a single viral particle in a blood sample. It often takes thousands
to make you sick.
Skeptics of natural immunity point to Manaus, capital of the Brazilian state of Amazonas,
where reports in January suggested a wave of re-infections despite herd immunity. But the
initial estimate of those infected was incorrect because
it was based on antibody testing among those who donated convalescent plasma""an
unrepresentative subgroup of the population. A follow-up study
debunked the re-infection hypothesis and found only three confirmed re-infections in the entire
state, whose population exceeds four million. Other studies have confirmed that re-infections
are rare and usually asymptomatic or mild.
Some health officials warn of possible variants resistant to natural immunity. But none of
the hundreds of variants observed so far have evaded either natural or vaccinated immunity with
the three vaccines authorized in the U.S.
Should the previously infected be vaccinated? My clinical advice to healthy patients with
natural immunity is that one shot is sufficient, and maybe not even necessary, although it
could increase the long-term durability of immunity. A University of Pennsylvania
study of people previously infected with Covid found that a single vaccine dose triggered a
strong immune response, with no increase in that response after a second dose. A separate
study from New York's Mount
Sinai School of Medicine concluded that "the antibody response to the first vaccine dose in
individuals with pre-existing immunity is equal to or even exceeds the titers found in
naïve"""never-infected"""individuals after the second dose."
Researchers from the Cleveland Clinic published a study this week of 1,359
people previously infected with Covid who were unvaccinated. None of the subjects subsequently
became infected, leading the researchers to conclude that "individuals who have had SARS-CoV-2
infection are unlikely to benefit from COVID-19 vaccination."
What's the harm of underestimating or disregarding the protection afforded by natural
immunity? It almost certainly cost American lives by misallocating vaccine doses earlier this
year, and is still doing so in countries where Covid is prevalent and shots are scarce. It
continues to delay full reopening and prolongs the state of fear that has many people wearing
masks even when there's no mandate, or reason, to do so.
Dr. Fauci said last Aug. 13 that when you have fewer than 10 cases per 100,000, "you should
be able to open up safely and clearly." The U.S. reached that point in mid-May. It's time to
stop the fear mongering and level with the public about the incredible capabilities of both
modern medical research and the human body's immune system.
Dr. Makary is a professor at the Johns Hopkins School of Medicine, Bloomberg School of
Public Health and Carey Business School. He is author of "The Price We Pay: What Broke American
Health Care""and How to Fix It," just out in paperback.
Merck & Co Inc (NYSE: MRK
)
has entered into a procurement agreement with the U.S. government for molnupiravir
(MK-4482), an antiviral candidate for mild to moderate COVID-19.
Molnupiravir is currently being evaluated in Phase 3 MOVe-OUT study to treat
non-hospitalized patients with laboratory-confirmed COVID-19 and at least one risk factor
associated with poor disease outcomes.
Through the agreement, if molnupiravir receives FDA Emergency Use Authorization (EUA) or
approval, Merck will receive approximately $1.2 billion to supply about 1.7 million courses of
molnupiravir to the government.
Merck has been investing to scale up the production of molnupiravir and expects to have more
than 10 million courses of therapy available by the end of 2021.
The company is also planning to submit applications for emergency use or approval to
regulatory bodies outside the U.S. It is currently in discussions with other countries
interested in advance purchase agreements for molnupiravir.
Merck is developing molnupiravir in collaboration with Ridgeback Biotherapeutics .
Price Action: MRK shares are up 0.55% at $72.80 during the premarket session on the last
check Wednesday.
Is this a study or an unethical medical experiment?
On of they main question here is "Why?" as children have an extremely low risk of complications from COVID-19. For them it is
nothing more then a flu.
New study to enroll thousands of children below 12 years at dozens of sites across the US, Finland, Poland and Spain.
The
Pfizer-BioNTech vaccine has already been approved for adolescents in the EU [Andreea Alexandru/AP Photo]
8 Jun 2021
Pfizer has said it will begin testing its COVID-19 vaccine in a larger group of children below 12 years of age after selecting a
lower dose of the shot in an earlier stage of the trial.
The study will enrol up to 4,500 children at more than 90 clinical sites in the United States, Finland, Poland and Spain, the
pharma company said.
The vaccine made by Pfizer and its German partner BioNTech is already authorised for emergency use in anyone 12 and older in the US,
Canada and the European Union. They receive the same dose as adults: 30 micrograms.
Enrolment of five- to 11-year-olds for the new study began this week. Based on safety, tolerability and the immune response
generated by 144 children in a phase I study of the two-dose shot, Pfizer said it will test a dose of 10 micrograms in children
between five and 11 years of age, and 3 micrograms for the age group of six months to five years.
A Pfizer spokesperson said the company expects data from five-to-11-year-olds in September and would likely ask regulators for
emergency use authorisation later that month. Data for children two to five years old could arrive soon after that, he said.
Pfizer expects to have data from the six-month to two-year-old age group sometime in October or November.
Nearly seven million teens have received at least one dose of the vaccine in the US, according to the US Centers for Disease Control
and Prevention (CDC).
Inoculating children and young people is considered a critical step towards reaching "herd immunity"� and taming the COVID-19
pandemic.
Still, scientists in the US and elsewhere are studying the possibility of a link between heart inflammation and mRNA vaccines,
particularly in young men. Both Pfizer and Moderna Inc's vaccines are mRNA shots.
Israel's Health Ministry said last week it had found the small number of myocarditis cases observed mainly in young men who received
the Pfizer vaccine there were probably linked to their vaccination. The cases were generally mild and did not last long.
Pfizer has said it is aware of the Israeli observations of myocarditis and that no causal link to its vaccine has been established.
Separately on Tuesday, the European Union's drug regulator said it expects to give a verdict on the use of Moderna's COVID-19
vaccine in 12- to 17-year-olds next month, following an application by the drugmaker.
The two-dose vaccine is already being used in the EU for people above 18 years of age in several countries. The company has also
sought approval in Canada for use in adolescents and plans for a US application.
If approved, Moderna's vaccine would become the second shot cleared for use in teenagers in the EU after Pfizer and BioNTech's
vaccine was given the green light last month.
A European Medicines Agency (EMA) committee would speed up the assessment of data submitted with the application, the regulator
said, adding that a delay would happen if the EMA required any additional information.
Emergency meeting in eight more days.. ??? An emergency meeting would be something held
tonight; an emergency meeting that can wait days needs to call it differently --"out of schedule
meeting" or something like that.
What happens when you have inflammation and damage? You get scar tissue. Do you really think
that this doesn't have lasting effect? These guys will have problems ater in life with their
hearts and it won't because of McDonalds....
The Centers for Disease Control and Prevention announced Thursday that it will convene an
"emergency meeting"
of its advisers on June 18th to discuss rare but higher-than-expected reports of heart
inflammation following doses of the mRNA-based Pfizer and Moderna COVID-19 vaccines.
The new details about myocarditis and pericarditis emerged first in presentations to a
panel of independent advisers for the Food and Drug Administration, who are meeting
Thursday to discuss how the regulator should approach emergency use authorization for using
COVID-19 vaccines in younger children.
As CBS reports, the CDC previously
disclosed that reports of heart inflammation were detected mostly in younger men and
teenage boys following their second dose, and that there
was a "higher number of observed than expected" cases in 16- to 24-year-olds. Last month,
the CDC urged providers to "ask about prior COVID-19 vaccination" in patients with symptoms of
heart inflammation.
me title=
Play Video
https://imasdk.googleapis.com/js/core/bridge3.464.0_en.html#goog_772135364
https://imasdk.googleapis.com/js/core/bridge3.464.0_en.html#goog_595720652 Wall Street
Bounces, After Selloff Fed Boosts Liquidity NOW PLAYING SoftBank Said to Plan $14 Billion Sale
of Alibaba Shares China's Companies Have Worst Quarter on Record, Beige Book Says U.S.-Saudi
Oil Alliance Under Consideration, Brouillette Says ETF Volumes Surge in Current Market
Environment Investors Have Given Up on a V-Shaped Recovery, BNY's Young Cautions
We'll leave the judgment up to someone far more qualified...
https://platform.twitter.com/embed/Tweet.html?dnt=false&embedId=twitter-widget-0&features=eyJ0ZndfZXhwZXJpbWVudHNfY29va2llX2V4cGlyYXRpb24iOnsiYnVja2V0IjoxMjA5NjAwLCJ2ZXJzaW9uIjpudWxsfSwidGZ3X2hvcml6b25fdHdlZXRfZW1iZWRfOTU1NSI6eyJidWNrZXQiOiJodGUiLCJ2ZXJzaW9uIjpudWxsfSwidGZ3X3R3ZWV0X2VtYmVkX2NsaWNrYWJpbGl0eV8xMjEwMiI6eyJidWNrZXQiOiJjb250cm9sIiwidmVyc2lvbiI6bnVsbH19&frame=false&hideCard=false&hideThread=false&id=1403113666120138752&lang=en&origin=https%3A%2F%2Fwww.zerohedge.com%2Fcovid-19%2Fcdc-hold-emergency-meeting-after-100s-suffer-heart-inflammation-following-covid-vaccines&sessionId=6b0992400c58b46ba331c397cfcb0155add8e5a1&siteScreenName=zerohedge&theme=light&widgetsVersion=82e1070%3A1619632193066&width=550px
https://platform.twitter.com/embed/Tweet.html?dnt=false&embedId=twitter-widget-1&features=eyJ0ZndfZXhwZXJpbWVudHNfY29va2llX2V4cGlyYXRpb24iOnsiYnVja2V0IjoxMjA5NjAwLCJ2ZXJzaW9uIjpudWxsfSwidGZ3X2hvcml6b25fdHdlZXRfZW1iZWRfOTU1NSI6eyJidWNrZXQiOiJodGUiLCJ2ZXJzaW9uIjpudWxsfSwidGZ3X3R3ZWV0X2VtYmVkX2NsaWNrYWJpbGl0eV8xMjEwMiI6eyJidWNrZXQiOiJjb250cm9sIiwidmVyc2lvbiI6bnVsbH19&frame=false&hideCard=false&hideThread=false&id=1403116038770864129&lang=en&origin=https%3A%2F%2Fwww.zerohedge.com%2Fcovid-19%2Fcdc-hold-emergency-meeting-after-100s-suffer-heart-inflammation-following-covid-vaccines&sessionId=6b0992400c58b46ba331c397cfcb0155add8e5a1&siteScreenName=zerohedge&theme=light&widgetsVersion=82e1070%3A1619632193066&width=550px
Does anyone else not find it odd that after discovering 800 cases in the VAERS database the
"emergency" meeting is in 7 days ? ... and in the meantime, every public health authority
figure is encouraging parents to get their young children vaccinated ?
* * *
As The Epoch Times' Zachary Stieber detailed earlier , Federal authorities have received
over 800 reports of heart inflammation in people who received a COVID-19 vaccine, a health
official said Thursday.
The reports of myocarditis or pericarditis were submitted to the Vaccine Adverse Event Reporting System, a passive
reporting system run jointly by the Centers for Disease Control and Prevention (CDC) and the
Food and Drug Administration, through May 31.
The bulk of the reports described heart inflammation appearing after the second of two doses
of either the Pfizer of Moderna vaccines, both of which utilize messenger RNA technology.
Authorities stress that anybody can submit reports through the reporting system but
authorities have already verified that 226 of the reports meet the CDC's working case
definition, Dr. Tom Shimabukuro, a deputy director at the agency, said during a presentation of
the data. Followup and review are in progress for the rest.
Of the 285 case reports for which the disposition was known at the time of the review, 270
patients had been discharged and 15 were still hospitalized, officials said. Myocarditis
typically requires hospital care. No deaths were reported.
A slide on myocarditis reports post-COVID-19 vaccination is shown during the Food and Drug
Administration's Vaccines and Related Biological Products Advisory Committee meeting on June
10, 2021. (FDA/Screenshot via The Epoch Times)
The CDC
announced last month that it was investigating reports of heart inflammation in teenagers
and young adults who received a COVID-19 vaccine, though it took no definitive action besides
saying it would continue reviewing case data.
An advisory committee to the agency, the Advisory Committee on Immunization Practices, said
in a little-noticed update published dated May 24 and published on June
1 that data from VAERS showed that in the 30 days following the second dose of mRNA
vaccinations, "there was a higher number of observed than expected myocarditis/pericarditis
cases in 16""24-year-olds."
Data from the Vaccine Safety Datalink, an active reporting system that relies on nine
healthcare organizations in seven states, did not show higher than expected cases, it
added.
"However, analyses suggest that these data need to be carefully followed as more persons
in younger age groups are vaccinated," the advisory committee's vaccine safety workgroup said
in its report.
Israel's Health Ministry
said that same day that it found 275 cases of heart inflammation among the more than 5
million people in the country who received a vaccine between December 2020 and May. An Israeli
study found "a probable link" between receiving the second dose of the Pfizer jab "and the
appearance of myocarditis among men aged 16 to 30," the ministry said.
Shimabukuro said the U.S. passive surveillance data "are consistent with the surveillance
data that emerged from Israel."
The figures are also consistent with other case reports and data from the Department of
Defense.
The vast majority of the U.S. reports deal with male patients. Approximately 300 preliminary
reports indicated the patients suffered chest pain, with nearly as many having elevated cardiac
enzymes.
Family members watch as a 12-year-old is inoculated with Pfizer's vaccine against COVID-19
at Dekalb Pediatric Center in Decatur, Ga., on May 11, 2021. (Chris Aluka Berry/Reuters)
A case report
examining myocarditis in seven adolescents following vaccination with Pfizer's jab,
published in Pediatrics, the journal of the American Academy of Pediatrics, this month, said
all seven developed the inflammation within 4 days of receiving the second dose, did not have
evidence of COVID-19 infection, and did not meet the criteria for MIS-C, a rare disease.
The seven males, between the ages of 14 and 19, all required hospital care but each was
eventually discharged.
Authors, who did not respond to requests for comment, said no link has been established
between the vaccines and myocarditis and that the benefits of the vaccines outweigh the risks.
But they also urged healthcare workers "to consider myocarditis in the evaluation of
adolescents and young adults who develop chest pain after COVID-19 vaccination."
A
commentary on the study published in the same journal, said "there are some concerns
regarding this case series that might suggest a causal relationship and therefore warrant
further analysis through established surveillance systems."
"First, the consistent timing of symptoms in these seven cases after the second
vaccination suggests a uniform biological process. Second, the similarities in clinical
findings and laboratory characteristics in this series suggest a common etiology. Finally,
these cases occurred in the context of a dearth of circulation of common respiratory viruses
known to be associated with myocarditis, and thorough diagnostic evaluations did not identify
infectious etiologies," they added.
The expected number of myocarditis/pericarditis cases in those aged 16 or 17, based on
background incidence rates and the number of doses administered to that population through May
31, is between two and 19. But based on the VAERS reports, the number is 79.
Likewise, the expected number for cases among young adults between the ages of 18 and 24 is
eight to 83. The number based on the reports is 196.
"In the 16- to 17 year-olds and the 18- to 24-year-olds, the observed reports are exceeding
the expected based on the known background rates that are published in literature," Shimabukuro
told members of a Food and Drug Administration vaccine advisory committee in the meeting on
Thursday, though he cautioned that not all the reports will "turn out to be true
myocarditis/pericarditis reports."
" Of note, of these 528 reports after second dose with symptom onset within 30 days, over
half of them were in these younger age groups, 12""24 years old , whereas roughly 9 percent of
total doses administered were in those age groups, so we "clearly have an imbalance there," he
added later.
A slide on myocarditis reports post-COVID-19 vaccination is shown during the Food and Drug
Administration's Vaccines and Related Biological Products Advisory Committee meeting on June
10, 2021. (FDA/Screenshot via The Epoch Times)
Data from the Vaccine Safety Datalink, which comes from nine healthcare groups that have
collectively administered over 8.8 million doses""only some 284,000 of those have been given to
12- to 17-year-olds""did not indicate safety concerns, with just 60 myocarditis or pericarditis
events reported through May 29, the doctor continued.
A Food and Drug Administration surveillance system, the Biologics Effectiveness and Safety
Initiative, which utilizes claims data from CVS and two other partners, has detected 99 cases
of myocarditis/pericarditis in the 42 days following vaccination among some 3.1 million shots
given to people between the ages of 12 and 64, the panel was told earlier by an official from
the drug regulating agency.
Another 1,260 were reported in people 65 or older through claims data from Medicare claims
data.
Neither number raised safety signals, Steve Anderson, director of the FDA's Office of
Biostatistics and Epidemiology said.
Dr. Cody Meissner, chief of the Division of Pediatric Infectious Disease at the Tufts
Children's Hospital, and a member of the panel that heard from Shimabukuro and others, said
after the presentations that he was "struck by the fact" that myocarditis "occurs more commonly
after the second dose."
"It's a pretty specific interval of time, it's primarily after the mRNA vaccines as far as
we know, we know that the consistent age, there's a lack of alternative explanations even
though these patients have been pretty well worked up, and it's a widespread occurrence
because, as you said, Israel has found a pretty similar situation," he said during the
meeting.
He asked Shimabukuro about the rates of blood clots seen in women between the ages of 30 and
49 after vaccination""most of the clots appeared in that population after getting a Johnson
& Johnson shot, though officials ultimately lifted a pause,
saying the benefits outweighed the risks ""and to restate the rate of incidence of
myocarditis in adolescents after a jab.
Shimabukuro said that in contrast with the clotting situation, when data showed "strong
evidence of a causal relationship fairly early on," further study is needed on heart
inflammation.
"At this point, I think we're still learning about the rates of myocarditis and
pericarditis. We continue to collect more information both in VAERS and continue to get more
information in VSD, and I think as gather more information we'll begin to get a better idea of
the post-vaccination rates and hopefully will be able to get more detailed information by age
group," he said.
"It's still early," he added, noting that authorization for a vaccine for 12- to
-15-year-olds didn't come
until mid-May while immunization of older adolescents largely came later than shots for
adults.
"I believe that we will ultimately have sufficient information to answer those questions,"
he said.
A general view of the Centers for Disease Control and Prevention (CDC) headquarters in
Atlanta, Ga., on Sept. 30, 2014. (Tami Chappell/Reuters)
Another panel member, Dr. Jay Portnoy, director of the Division of Allergy, Asthma, &
Immunology at Children's Mercy Hospitals & Clinics, asked for a comparison between the
adverse events in vaccinated versus unvaccinated persons, saying if the adverse event rate was
lower in those who are vaccinated, then it would still be worth getting a jab.
Shimabukuro said a risk-benefit assessment would be provided by the CDC's advisory panel,
known as ACIP, on vaccines during a meeting next week.
A CDC spokeswoman also referenced the upcoming meeting, which will take place on June 18,
after saying reports of myocarditis remain rare, given that over 300 million doses have been
administered in the United States.
"Given the number of COVID-19 vaccine doses administered, these reports are rare. More
than 18 million people between ages 12-24 have received at least one dose of COVID-19 vaccine
in the United States," she told The Epoch Times via email.
"CDC continues to recommend COVID-19 vaccination for everyone 12 years and older. Getting
vaccinated is the best way to help protect yourself and your family from COVID-19."
A Pfizer spokesperson told The Epoch Times in an email that the company is aware of federal
data indicating "rare reports of myocarditis and pericarditis, predominantly in male
adolescents and young adults, after mRNA COVID-19 vaccination." It noted that federal officials
have not concluded that mRNA COVID-19 vaccines cause either condition, before expressing
support for an assessment of suspected adverse events.
"With a vast number of people vaccinated to date, the benefit risk profile of our vaccine
remains positive," the spokesperson added.
Moderna did not return an inquiry.
Dr. Monica Gandhi, professor of medicine and associate chief at the University of
California, San Francisco, told The Epoch Times in an email that in light of the increased risk
of myocarditis above expected rates among young people, especially after the second dose,
parents should keep a close eye out for when guidance is issued by federal authorities.
"Possibilities include only vaccinating children without prior infection as there is an
association between prior COVID and this adverse effect; giving 1 dose instead of 2 below the
age of 20; addressing the dosage of the vaccine (currently at 30 micrograms down to the age
of 12, which is the same dose as in adults); and extending the duration between doses 1 and 2
for younger people," she said.
"I look forward to ACIP guidance on this over the next few weeks."
BugMan 13 minutes ago
"The infamous spike protein of the coronavirus gets into the blood where it circulates
for several days post-vaccination and then accumulated in organs and tissues including the
spleen, bone marrow, the liver, adrenal glands, and in quite high concentrations in the
ovaries"; "a large number of studies has shown that the most severe effects of SARS-CoV-2,
the virus that causes COVID-19, such as blood clotting and bleeding, are due to the effects
of the spike protein of the virus itself."
Top Immunologist and "˜Pro-Vaccine' Doctor Byram Bidle Issues Warning"¦ ""
CITIZEN FREE PRESS
GregBurton 3 minutes ago
I don't see how the CDC, Fauci, Wuhan (CCP), Fort Detrick, Ralph Baric, Peter Daszak and
the WHO are going to get out of this: the 'vaccine' mRNA spike protein is toxic, it is a
pathogenic protein that causes clotting, heart problems and may be associated with
infertility...
bringonthebigone 1 hour ago
The heart has almost no repair capability. Even mild damage at that age likely takes
years or decades off life expectancy. Seems likely the number of undiscovered cases far far
exceed the number reported.
I Write Code 1 hour ago
"Possibilities include only vaccinating children without prior infection as there is
an association between prior COVID and this adverse effect; giving 1 dose instead of 2
below the age of 20; addressing the dosage of the vaccine (currently at 30 micrograms
down to the age of 12, which is the same dose as in adults); and extending the duration
between doses 1 and 2 for younger people," she said
No kidding Doctor Obvious.
BUT extending the duration is probably the wrong move, or if you do, cut the second dose
by 90%.
Hear me now, believe me later.
MRob 5 minutes ago remove link
Watching latest Brett Weinstein interview, Dark Horse, guest claimed the numbers of
complications from the vaccine could be anything up to 100x the official figures. Unlikely,
but emphasises that the error bar is massive. Above reporting system is voluntary, and
people have been censored from knowing what to even look for, and propagandised from
considering their issues could be due to the vaccine. Vaccine complication groups of fb
were deleted, with 70k or 120k people in them. Such a screwed up situation. With the
suppression of ivermectin etc, this is nuremberg trials level for sure.
https://ivmmeta.com spread the
word
GreatUncle 23 minutes ago
The problem is 2 part.
1. The vaccine is not tailored to the individual and therefore never 100% safe it is not
possible when working with statistics and probability as your guide.
2. The reporting system is next to non-existent even under vaers because that is the
measure of liability for those making people take gene therapies / vaccines.
Therein lies your two fundamental problems ... too fix it though you have too destroy
the whole system it should never have been put in place that way.
hoytmonger 36 minutes ago
In Idaho, the Idaho National Guard is "assisting" vaccination of students at their
middle school...
https://www.lewrockwell.com/2021/06/gary-d-barnett/public-political-school-madness-military-supported-vaccination-of-students-in-idaho/
Fat Beaver 54 minutes ago (Edited)
So the commenter on here, vasilievich mentioned he and his wife got the vax and his wife
went into cardiac arrest shortly after (4 days ago)...they are in their 80's...(God help
them)...several others have noted they knew people that went into cardiac arrest after the
vax...seems to be much, much more common than they are letting on...
Seabass120 36 minutes ago
My wife got her second Pfizer vacc and now cannot go into the sun without breaking out
into hives. Prior to the jab, she was outside daily.
JoKe Biden 27 minutes ago
Yep so predictable, some of the statements will read something like this.
The FDA and CDC have confidence that the vaccine is safe and effective in preventing
COVID-19.
The FDA has determined that the available data show that the vaccine's known and
potential benefits outweigh its known and potential risks in individuals 18 years of age
and older.
At this time, the available data suggest that the chance of heart inflammation
occurring is very low, but the FDA and CDC will remain vigilant in continuing to
investigate this risk.
_Rorschach 25 minutes ago
its not a vaccine
its gene therapy
ebworthen 38 minutes ago
An untested genetic experiment and not a "vaccine" in any sense of the word.
toady 19 minutes ago
"Just say no"
-Nancy Reagan
RawDrum 20 minutes ago
Imagine being a parent who got their teenage child injected with an experiment jab for
something they are at trivial risk of any impact from, that has no-one liable should it go
wrong, in an American for profit health insurance system, doing zero research and
outsourcing critical thinking to media, big tech and pharma corporations engaged in obvious
censorship and obfuscation, and that resulted in your child having an enlarged heart
impacting the rest of their shortened life.
YOLO!
LetThemEatRand 1 hour ago
"The chances of dying from COVID for the young are almost impossible to measure they are
so small" - doesn't matter. Any risk is too much. You must wear a mask and stay home and be
vaccinated when we're ready for that.
"The chances of dying from the COVID vaccine are unknown and documented cases of serious
side effects are growing." - it's a tiny risk, doesn't outweigh the benefit of the
vaccine.
RedSeaPedestrian 43 minutes ago
From Pfizer: "With a vast number of people vaccinated to date, the benefit risk profile
of our vaccine remains positive," the spokesperson added.
Tell that to the families that have had a loved one die from the "jab".
Farmer Dave 24 minutes ago
My dad has been fighting this for a month. He got the jab and ended up in the hospital
with blood clots and the heart inflammation. He is a tough old man and seems to be getting
better. I told him if he would have heeded my warnings about the jab he wouldn't be sick.
Anyone who gives this jab to a child is an idiot.
fackbankz 44 minutes ago (Edited)
If any other product killed 5000 people and injured 200,000, it would be pulled, not
pushed.
There is no such thing as "mild" myocarditis, especially in juveniles. If they live,
they will have a lifetime of heart problems and will likely never be able to enjoy fun
activities like sports or sex. I'm only saying this to inoculate you against the incoming
PR blitz of, "Oh, it's just a few mild cases of heart inflammation."
We must avenge this crime against humanity. My hope is that it is done through courts
and due process, but if ends up just being heads on pikes, so be it.
Dr. Gonzo 47 minutes ago
Biden is giving away 500,000 of these serums to our lucky Vassals. Eh hem. I mean
Allies. For a special thank you from the Empire.
nowhereman 19 minutes ago remove link
After asking yourself a couple more questions like that, and you begin to understand
that it's never been about a "virus" it's about the jab.
hoytmonger 16 minutes ago (Edited)
There's an article to that effect...
https://www.lewrockwell.com/2021/06/joseph-mercola/was-the-whole-pandemic-about-the-vaccine/
absalom_hicks 41 minutes ago remove link
"Population decimated by rare blood clots", "Extremely rare side effects devastate
many", "Benefits far outweigh risks as die off causes labor shortages", "Scientists explain
how lab created viruses evolve naturally", "New variants cause only mild symptoms in
vaccinated travelers", "Annual vaccination necessary for return to new normal, CEO of
CALPERS says."
Headlines in a mentally ill society.
TieOneOn 47 minutes ago
Looks like 'Gain of Function' is full steam ahead......
Befits 10 minutes ago (Edited) remove link
They are not panicked. They will do a farce meeting and declare " the benefits of the
Covid 19 vax outweigh the risks". Even for the young men who " in very small number of
cases where there is no clear causal link between the Covid vax and myocarditis". Then when
the microphone is off and the transcription is ended they will laugh their asses off "
these fools will buy it
🤣🤣🤣🤣
". Cha Ching...
boyplunger7777 10 minutes ago
By late summer, should the general public begin to experience serious side effects, the
nation will go into full blown panic...
You_Cant_Quit_Me 9 minutes ago
They'll just say it's a variant of COVID-19 and blame that
Cabreado 38 minutes ago (Edited)
The CDC has been sufficiently exposed, and they're trying to save face with the
masses.
Good luck finding any non-corrupt oversight to resolve this situation... that of a rogue
CDC.
Rubicon727 1 hour ago
What the CDC refuses to admit is the EU system, that keeps far more accurate deaths,
severe illnesses can be looked at any time of the day. Link to EUdraVigilance.com . They've shown many examples of severe
repercussions from the different kinds of Covid vaccines that have harmed, or killed people
for weeks now.
Now you tell us, how is it this is just NOW emerging from the CDC? Explain that.
Lt. Shicekopf 4 minutes ago
Why are kids getting jabbed? In the off chance they contract this virus there is a 99.8%
chance of recovery. I just do not get it.
AriusArmenian 3 minutes ago
Money.
allfactsmatter 21 minutes ago
The mrNA technology is a new technique for vaccine development.
Despite this, the Pfizer and Modern "vaccines" have been tested LESS than traditional
vaccines. Yet the FDA and CDC says the risks from these shots are acceptable.
Keep in mind that healthy young men have almost NO mortality risk from COVID, and
receive no benefit from these shots as a direct consequence.
Big Government and Big Pharma are gambling with people's lives with these Frankenvirus
vaccines.
liberty2 27 minutes ago
Not a vaccine, they label it as a vaccine to have immunity to lawsuits, no pun intended.
They also call it a vaccine to get emergency authorization. It's not APPROVED, only
authorized, there's a difference. There's NO law mandating the vax, NONE. Your employer can
be sued for discrimination or you can claim Workman's Comp if you should suffer side
effects.
Danoc 29 minutes ago
Can't wait for Fauci's next round of explanation.
opaopaopa 26 minutes ago
all rounds are the same:
"it's the Science"
fackbankz 10 minutes ago
"A few minor cases of heart inflammation, nothing to worry about. Benefits outweigh the
risks."
You know the drill.
Any other product that caused 800 cases of lifelong heart problems in young people would
have been pulled, not pushed, and it's probably a lot more than 800.
TonTon 58 minutes ago
Looks like they are hardly even checking for Myocarditis in the 50+ age bracket and
especially in the 65+ age bracket given it's less than the normal rate for this age group.
I'm sure they are just putting it down to some of the many coincidences happening after
people get the 'jab.' Given that the rate is less than normal though you could be forgiven
for thinking that they are ACTIVELY SUPPRESSING information on side effects. We are
experiencing and epidemic of coincidences these days.
Notable quotes:
"... Singapore found that the mutation accounted for 95% of the local Covid samples linked to variants of concern. ..."
"... Higher rates of transmission and a reduction in the effectiveness of vaccines have made understanding the strain's effects especially critical. ..."
"... Some patients develop micro thrombi , or small blood clots, so severe that they led affected tissue to die and develop gangrene , said Ganesh Manudhane , a Mumbai cardiologist ..."
"... Doctors are also finding instances of clots forming in blood vessels that supply the intestines , causing patients to experience stomach pain -- their only symptom, local media have reported. ..."
"... But with emerging evidence delta and at least one other variant may be adept at evading vaccine-induced antibodies, pharmaceutical companies are under pressure to tweak existing shots or develop new ones. ..."
The coronavirus variant driving India's devastating Covid-19 second wave is the most
infectious to emerge so far. Doctors now want to know if it's also more severe.
Hearing impairment, severe gastric upsets and blood clots leading to gangrene, symptoms not
typically seen in Covid patients, have been linked by doctors in India to the so-called delta
variant. In England and Scotland, early evidence suggests the strain -- which is also now
dominant there -- carries a higher risk of
hospitalization .
Delta, also known as B.1.617.2, has spread to more than 60 countries over the past six
months and triggered travel curbs from Australia to the
U.S . A spike in infections, fueled by the variant, has forced U.K. to
reconsider its plans for reopening later this month, with a local report saying it may be
pushed back
by two weeks. Singapore found that the mutation accounted for 95% of the local Covid
samples linked to variants of concern.
Higher rates of transmission and a reduction in the effectiveness of vaccines have made
understanding the strain's effects especially critical.
... ... ...
"˜New Enemy'
"Last year, we thought we had learned about our new enemy, but it changed," Ghafur said.
"This virus has become so, so unpredictable."
Stomach pain, nausea, vomiting, loss of appetite, hearing loss and joint pain are among the
ailments Covid patients are experiencing, according to six doctors treating patients across
India. The beta and gamma variants -- first detected in South Africa and Brazil respectively --
have shown little or no evidence of triggering unusual clinical signs, according to a
study
by researchers from the University of New South Wales last month.
Some patients develop
micro thrombi , or small blood clots, so severe that they led affected tissue to die and
develop
gangrene , said Ganesh Manudhane , a
Mumbai cardiologist , who has treated eight patients for thrombotic complications at the
Seven Hills Hospital during the past two months. Two required amputations of fingers or a
foot.
"I saw three-to-four cases the whole of last year, and now it's one patient a week,"
Manudhane said.
India has reported 18.6 million Covid cases thus far in 2021, compared with 10.3 million
last year. The delta variant was the "primary cause" behind the country's deadlier second wave
and is 50% more contagious than the alpha strain that was first spotted in the U.K., according
to a
recent study by an Indian government panel.
The surge in cases may have driven an increase in the frequency with which rare Covid
complications are being observed. Even still, Manudhane said he is baffled by the blood clots
he's seeing in patients across age groups with no past history of coagulation-related
problems.
"We suspect it could be because of the new virus variant," he said. Manudhane is collecting
data to study why some people develop the clots and others don't.
Doctors are also finding instances of clots forming in blood vessels that supply the
intestines , causing patients to experience stomach pain -- their only symptom, local media
have reported.
Some Covid patients are also seeking medical care for hearing loss, swelling around the neck
and severe tonsillitis, said Hetal Marfatia, an ear nose and throat surgeon at Mumbai's King
Edward Memorial Hospital.
The unusual presentations for delta and a closely related variant known as kappa, whose
spread led to a fourth lockdown in the Australian city of Melbourne, are still being confirmed,
said Raina MacIntyre, a professor of global biosecurity at the University of New South Wales in
Sydney. "In the meanwhile, it is important to take note of this and be aware of possible
atypical presentations," she said.
Delta Variant
From India Begins to Show Its True Ugly Colors
The most alarming aspect of the current outbreak in India is the rapidity with which the
virus is spreading, including to children, said Chetan Mundada, a pediatrician with the
Yashoda group
of hospitals in Hyderabad.
... But with emerging evidence delta and at least one other variant may be adept at
evading vaccine-induced antibodies, pharmaceutical companies are under pressure to tweak
existing shots or develop new ones.
Bacon's Rebellion 4 hours ago (Edited)
/////////////////////////////////////////////////////////////////////////////
Israel Vaccination Statistics from The
Lancet
Take away....
1,127.965 people age 65+
138 "vaccinated" deaths = 0.0136% of the group died
So, looking at the entire group, you had a 0.62% greater chance of dying if not
vaccinated.
1,764,098 people age 45 to 64
14 "vaccinated" deaths = 0.001% of the group died
You had a 0.034% greater chance of dying if not vaccinated.
3,646,848 people age 16 to 44
0 "vaccinated" deaths = 0.0% of the group died
You had a 0.0027% greater chance of dying if not vaccinated.
Emergency authorization of an untested drug to reduce your chance of death by less than
1%?
GTFO!
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(21)00947-8/fulltext
Farmer Tink 1 hour ago
@Bacon's Rebellion We'll see soon enough. The India/Delta variant is in the US and the
British say that it's more infectious than the British variant. If it's here, it will spread
fast and that means that a lot of people who have taken the vaccine will be exposed.
Highly recommended !Notable quotes:
"... In today's world, brimful as it is with opinion and falsehoods masquerading as facts, you'd think the one place you can depend on for verifiable facts is science. You'd be wrong. Many billions of dollars' worth of wrong. ..."
"... A few years ago, scientists at the Thousand Oaks biotech firm Amgen set out to double-check the results of 53 landmark papers in their fields of cancer research and blood biology. The idea was to make sure that research on which Amgen was spending millions of development dollars still held up. They figured that a few of the studies would fail the test -- that the original results couldn't be reproduced because the findings were especially novel or described fresh therapeutic approaches. But what they found was startling: Of the 53 landmark papers, only six could be proved valid. ..."
"... "Even knowing the limitations of preclinical research," observed C. Glenn Begley, then Amgen's head of global cancer research, "this was a shocking result." ..."
"... A group at Bayer HealthCare in Germany similarly found that only 25% of published papers on which it was basing R&D; projects could be validated, suggesting that projects in which the firm had sunk huge resources should be abandoned. ..."
"... "The thing that should scare people is that so many of these important published studies turn out to be wrong when they're investigated further," ..."
"... Eisen says the more important flaw in the publication model is that the drive to land a paper in a top journal -- Nature and Science lead the list -- encourages researchers to hype their results, especially in the life sciences. Peer review, in which a paper is checked out by eminent scientists before publication, isn't a safeguard. Eisen says the unpaid reviewers seldom have the time or inclination to examine a study enough to unearth errors or flaws. ..."
"... Eisen is a pioneer in open-access scientific publishing, which aims to overturn the traditional model in which leading journals pay nothing for papers often based on publicly funded research, then charge enormous subscription fees to universities and researchers to read them. ..."
"... But concern about what is emerging as a crisis in science extends beyond the open-access movement. It's reached the National Institutes of Health, which last week launched a project to remake its researchers' approach to publication. ..."
"... PubMed Commons is an effort to counteract the "perverse incentives" in scientific research and publishing, says David J. Lipman, director of NIH's National Center for Biotechnology Information, which is sponsoring the venture. ..."
"... The demand for sexy results, combined with indifferent follow-up, means that billions of dollars in worldwide resources devoted to finding and developing remedies for the diseases that afflict us all is being thrown down a rathole. NIH and the rest of the scientific community are just now waking up to the realization that science has lost its way, and it may take years to get back on the right path. ..."
In today's world, brimful as it is with opinion and falsehoods masquerading as facts, you'd think the one place you can depend
on for verifiable facts is science. You'd be wrong. Many billions of dollars' worth of wrong.
A few years ago, scientists at the Thousand Oaks biotech firm Amgen set out to double-check the results of 53 landmark
papers in their fields of cancer research and blood biology. The idea was to make sure that research on which Amgen was spending
millions of development dollars still held up. They figured that a few of the studies would fail the test -- that the original
results couldn't be reproduced because the findings were especially novel or described fresh therapeutic approaches. But what
they found was startling: Of the 53 landmark papers, only six could be proved valid.
"Even knowing the limitations of preclinical research," observed C. Glenn Begley, then Amgen's head of global cancer research,
"this was a shocking result."
Unfortunately, it wasn't unique. A group at Bayer HealthCare in Germany similarly found that only 25% of published
papers on which it was basing R&D; projects could be validated, suggesting that projects in which the firm had sunk huge
resources should be abandoned. Whole fields of research, including some in which patients were already participating in clinical trials, are based
on science that hasn't been, and possibly can't be, validated.
"The thing that should scare people is that so many of these important published studies turn out to be wrong when they're investigated
further,"
says Michael Eisen, a biologist at UC Berkeley and the
Howard Hughes Medical Institute. The Economist recently estimated spending on biomedical R&D; in industrialized countries at $59
billion a year. That's how much could be at risk from faulty fundamental research.
Eisen says the more important flaw in the publication model is that the drive to land a paper in a top journal -- Nature
and Science lead the list -- encourages researchers to hype their results, especially in the life sciences. Peer review, in which
a paper is checked out by eminent scientists before publication, isn't a safeguard. Eisen says the unpaid reviewers seldom have
the time or inclination to examine a study enough to unearth errors or flaws.
"The journals want the papers that make the sexiest claims," he says. "And scientists believe that the way you succeed is having
splashy papers in Science or Nature -- it's not bad for them if a paper turns out to be wrong, if it's gotten a lot of attention."
Eisen is a pioneer in open-access scientific publishing, which aims to overturn the traditional model in which leading journals
pay nothing for papers often based on publicly funded research, then charge enormous subscription fees to universities and researchers
to read them.
But concern about what is emerging as a crisis in science extends beyond the open-access movement. It's reached the
National Institutes of Health, which last week launched a project to remake its researchers' approach to publication. Its new
PubMed Commons system allows qualified scientists to post
ongoing comments about published papers. The goal is to wean scientists from the idea that a cursory, one-time peer review is enough
to validate a research study, and substitute a process of continuing scrutiny, so that poor research can be identified quickly and
good research can be picked out of the crowd and find a wider audience.
PubMed Commons is an effort to counteract the "perverse incentives" in scientific research and publishing, says David J. Lipman,
director of NIH's National Center for Biotechnology Information, which is sponsoring the venture.
The Commons is currently in its pilot phase, during which only registered users among the cadre of researchers whose work appears
in PubMed -- NCBI's clearinghouse for citations from biomedical journals and online sources -- can post comments and read them.
Once the full system is launched, possibly within weeks, commenters still will have to be members of that select group, but the
comments will be public.
Science and Nature both acknowledge that peer review is imperfect. Science's executive editor, Monica Bradford, told me by email
that her journal, which is published by the American Assn. for the Advancement of Science, understands that for papers based on
large volumes of statistical data -- where cherry-picking or flawed interpretation can contribute to erroneous conclusions -- "increased
vigilance is required." Nature says that it now commissions expert statisticians to examine data in some papers.
But they both defend pre-publication peer review as an essential element in the scientific process -- a "reasonable and fair"
process, Bradford says.
Yet there's been some push-back by the prestige journals against the idea that they're encouraging flawed work -- and that their
business model amounts to profiteering. Earlier this month, Science published a piece by journalist John Bohannon about what happened
when he sent a spoof paper with flaws that could have been noticed by a high school chemistry student to 304 open-access chemistry
journals (those that charge researchers to publish their papers, but make them available for free). It was accepted by
more than half of them.
One that didn't bite was PloS One, an online open-access journal sponsored
by the Public Library of Science, which Eisen co-founded. In fact, PloS One was among the few journals that identified the fake
paper's methodological and ethical flaws.
What was curious, however, was that although Bohannon asserted that his sting showed how the open-access movement was part of
"an emerging Wild West in academic publishing," it was the traditionalist Science that published the most dubious recent academic
paper of all.
This was a 2010 paper by then-NASA biochemist Felisa Wolfe-Simon
and colleagues claiming that they had found bacteria growing in Mono Lake that were uniquely able to subsist on arsenic and even
used arsenic to build the backbone of their DNA.
The publication in Science was accompanied by a breathless press release and press conference sponsored by NASA, which had an
institutional interest in promoting the idea of alternative life forms. But almost immediately it was debunked by other scientists
for spectacularly poor methodology and an invalid conclusion. Wolfe-Simon, who didn't respond to a request for comment last week,
has defended her interpretation
of her results as "viable." She hasn't withdrawn the paper, nor has Science, which has published numerous
critiques of the work . Wolfe-Simon is now
associated with the prestigious Lawrence Berkeley National Laboratory.
To Eisen, the Wolfe-Simon affair represents the "perfect storm of scientists obsessed with making a big splash and issuing press
releases" -- the natural outcome of a system in which there's no career gain in trying to replicate and validate previous work,
as important as that process is for the advancement of science.
"A paper that actually shows a previous paper is true would never get published in an important journal," he says, "and it would
be almost impossible to get that work funded."
However, the real threat to research and development doesn't come from one-time events like the arsenic study, but from the dissemination
of findings that look plausible on the surface but don't stand up to scrutiny, as Begley and his Amgen colleagues found.
The demand for sexy results, combined with indifferent follow-up, means that billions of dollars in worldwide resources
devoted to finding and developing remedies for the diseases that afflict us all is being thrown down a rathole. NIH and the rest
of the scientific community are just now waking up to the realization that science has lost its way, and it may take years to
get back on the right path.
Michael Hiltzik's column appears Sundays and Wednesdays. Read his new blog, The Economy Hub, at
latimes.com/business/hiltzik, reach him at
[email protected] facebook.com/hiltzik and follow
@hiltzikm on Twitter.
GEORGE SCANGOS: Well, a strong message is, I think it's a really important day in the fight
against COVID-19. We have an antibody drug that we have developed, brought through a phase
three trial. The initial analysis of that showed that we had an 85% reduction in reducing
hospitalization or death and on patients who had taken it. So that's quite an impressive
number.
COVID cases are going down in the US now, but they're not going away. We're going to
continue to need good therapies for the foreseeable future, and we're really quite excited
about what we can do now, for not only patients in the US but around the world.
ADAM SHAPIRO: George, congratulations. Help us understand what the drug actually does. It's
not an antiviral. Or is it an antiviral? Or does it prevent the issues that wind up making
people seriously ill and then eventually, perhaps, dying?
GEORGE SCANGOS: No, it is an antiviral. The antibody recognizes the virus, it binds to the
virus, and it does two things, actually, which distinguishes it from some of the other drugs
that are on the market. First, it prevents the virus from infecting cells. And secondly, when
people are already infected, there are a number of cells that are already infected, and they're
making even more viral particles. So this particular antibody is capable of blocking the
infection of new cells and killing those cells that are already infected with the virus to
prevent making even more viral particles.
... ... ...
ADAM SHAPIRO: Is it a pill? Is it like-- Regeneron, I think, is administered via IV. Is a
simpler way to administer this drug?
GEORGE SCANGOS: No, this is also intravenous, so you administer just like the other
antibodies. We are quickly working on just a normal injection-- intramuscular injection-- so it
would be similar to what you get with the vaccine or a flu shot. And that's in clinical trials
right now, but the medicine for which we had the EUA is administered IV.
... ... ...
ADAM SHAPIRO: The biotechnology that makes this an effective drug, does it have applications
for viral issues other than COVID-19? Could you be growing this for other remedies?
GEORGE SCANGOS: Well, that's a very interesting question. This particular antibody, as
opposed to all of the other COVID antibodies, is able to protect against other coronaviruses in
addition to the COVID coronavirus-- this coronavirus. Doesn't protect against all
coronaviruses, but, for example it would protect against SARS, we believe, and a whole family
of coronaviruses.
So we do believe that it's important to bring forward drugs that can not only treat this
pandemic but have the potential to be effective in future pandemics. And we're taking that
approach with not only COVID but flu and other diseases as well. Yeah.
JULIE LA ROCHE: Well, George Scangos, president and CEO of Vir Biotechnology, I thank you so
much for joining us. And congratulations, again, on the latest as it relates to your treatment
and this, of course, important fight against COVID-19.
Can't sit still 12 hours ago Can't sit still 12 hours ago
Here is a fantastic vid showing that our widespread lack of vitamin D is the root cause of
so many problems.
https://www.youtube.com/watch?v=tgCL4abBFzc
Ivermectin, an anti-parasitic drug placed the same radioactive category as
Hydroxychloroquine (HCQ) for the treatment of COVID-19, has reemerged as a promising treatment
in the battle to extinguish the pandemic.
New York Times best-selling author
Michael Capuzzo has called it the "
drug that cracked Covid ," writing that there are "hundreds of thousands, actually
millions, of people around the world, from Uttar Pradesh in India to Peru to Brazil, who are
living and not dying."
Doctors in India are
big fans .
To that end Dr. Justus R. Hope, MD asks in
The Desert Review : Is Ivermectin the new Penicillin?
MeLurkLongtime 5 hours ago
Have to have a surgery, met with surgeon today. Second question after how are you was have you had your covid shot? I said
no. He said why not? I said I was waiting until it was approved by FDA. He said that would be 5 years and Covid would be over
by then. I said OK. He said he refused to do surgery on anyone not vaxed for Covid. I said Ok, and left. So....now looking for
another surgeon. So there is that. Pretty dismayed, actually.
RedSeaPedestrian 4 hours ago
He violated your HIPAA protections. If you want a bit of revenge, turn him in.
The fines can be quite hefty.
HIPAA violations are taken very seriously. Anyone other than a licensed health care professional asking a private person about
their health conditions, including vaccinations, is against HIPAA regulations. NONE OF THE HIPAA LAWS WERE REPEALED OR RESCINDED
DUE TO COVID.
The minimum penalty for a criminal HIPAA violation is $50,000 per instance and can rise to $250k.
A private individual breaking HIPAA regulations can be fined $100, the company they work for if broken within a work environment
will be fined $50k.
So if I am not wearing a mask, and you ask for proof of vaccination, you just got your business a $50k fine.
https://www.hipaajournal.com/what-happens-if-you-break-hipaa-rules/
MeLurkLongtime 4 hours ago
Red Sea- He is a Surgeon that specializes in the surgery I need, no HIPAA violation. But thank you.
RedSeaPedestrian 4 hours ago
Did the surgeon tell you that? Read the link.
Quia Possum 4 hours ago (Edited)
Anyone other than a licensed health care professional asking a private person about their health conditions, including vaccinations,
is against HIPAA regulations.
BS. HIPAA only applies to medical record holders, not random people, and violations are by the record holder divulging information
that they should not. Asking prying questions is rude but not a HIPAA violation.
The USA vaccination efforts were badly thought out and badly implemented, resulting in dramatic economic losses for non-existent
public health gains. Looks like governments suspected that "the genie is out of the bottle" -- pathogen escaped from biolab in
the USA or China and badly overreacted, creating unnecessary economic losses and mass unemployment comparable with the Great
Depression.
There is no need to vaccinate people who already have had COVID-19. Natural immunity is much better than a vaccine that was rushed through the FDA.
Also many people are naturally immune to COVID-19 due tot he fact that they have previous coronavirus infection. This issue is
completely ignored in neoliberal MSM/
Notable quotes:
"... Obviously, you not only got immune to the Wuhan virus, but also to the globalist/collectivist and state propaganda. Those of us who lived in Soviet socialist "paradise" get it back in the USSR while protecting our mind and soul from state propaganda and government statistics. ..."
"... So more of the lies are being exposed, the lies that some who want to be in control have told are so bad, and yet some believe them. Why was SARS not a continuing pandemic, if it is the same base virus ..."
"... This is too funny. So at some point is anyone going to ask why this report is being featured on yahoo FINANCE? The answer is in the reference to the publicly-traded, pharmaceutical companies named in the Dr.'s interview. ..."
Dr. Adrian Burrowes, Family Medicine Physician &CFP Physicians Group CEO, joined Yahoo Finance to discuss the latest on covid-19.
Thomas 2 hours ago
I had Covid twice. Once in 2020 and once this year. The first time I had it I coughed for two whole months. I had a fever off
and on and I had to sleep with an extra pillow. I was miserable but I thought it was the flu because we didn't know the virus
was here yet. It was only after I was tested for antibodies several months later did I learn that I had it.
This past January, I got it again after some co-workers came down with it and we all were tested. I was quarantined for 10
days. During this 10 day period, I was only sick for 1 day with a slight stomach ache and diarrhea.
The rest of the time I was out doing yard work and cutting dead limbs out of my trees.
I told my wife that if my T-Cells had that good of memory to protect me that well, I probably won't get the shot. After all,
what can the shot do for me that the virus hasn't already.
Mike -> Thomas 38 minutes ago
Obviously, you not only got immune to the Wuhan virus, but also to the globalist/collectivist and state propaganda. Those of
us who lived in Soviet socialist "paradise" get it back in the USSR while protecting our mind and soul from state propaganda and
government statistics.
With the time, I hope enough Americans will develop the same herd immunity to propaganda masquerading as news, unhealthy "guidance"
from government health agencies and corrupt intelligent agencies' deceptions that serve self-centered bureaucrats and political
operatives, not the country. G-d Bless!
Ed 3 hours ago
So more of the lies are being exposed, the lies that some who want to be in control have told are so bad, and yet some believe
them. Why was SARS not a continuing pandemic, if it is the same base virus , and did not have a vaccine. and yet you hear nothing
about it, could it be that people gained immunity and so it is not a horrible thing as this engineered virus. and remember that
SARS started in the same area of the world as this covid 19.
AB 3 hours ago
This is too funny. So at some point is anyone going to ask why this report is being featured on yahoo FINANCE? The answer
is in the reference to the publicly-traded, pharmaceutical companies named in the Dr.'s interview.
The USA vaccination efforts were badly thought out and badly implemented, resulting in dramatic economic losses for non-existent
public health gains. Looks like governments suspected that "the genie is out of the bottle" -- pathogen escaped from biolab in
the USA or China and badly overreacted, creating unnecessary economic losses and mass unemployment comparable with the Great
Depression.
There is no need to vaccinate people who already have had COVID-19. Natural immunity is much better than a vaccine that was rushed through the FDA.
Also many people are naturally immune to COVID-19 due tot he fact that they have previous coronavirus infection. This issue is
completely ignored in neoliberal MSM/
Notable quotes:
"... Obviously, you not only got immune to the Wuhan virus, but also to the globalist/collectivist and state propaganda. Those of us who lived in Soviet socialist "paradise" get it back in the USSR while protecting our mind and soul from state propaganda and government statistics. ..."
"... So more of the lies are being exposed, the lies that some who want to be in control have told are so bad, and yet some believe them. Why was SARS not a continuing pandemic, if it is the same base virus ..."
"... This is too funny. So at some point is anyone going to ask why this report is being featured on yahoo FINANCE? The answer is in the reference to the publicly-traded, pharmaceutical companies named in the Dr.'s interview. ..."
Dr. Adrian Burrowes, Family Medicine Physician &CFP Physicians Group CEO, joined Yahoo Finance to discuss the latest on covid-19.
Thomas 2 hours ago
I had Covid twice. Once in 2020 and once this year. The first time I had it I coughed for two whole months. I had a fever off
and on and I had to sleep with an extra pillow. I was miserable but I thought it was the flu because we didn't know the virus
was here yet. It was only after I was tested for antibodies several months later did I learn that I had it.
This past January, I got it again after some co-workers came down with it and we all were tested. I was quarantined for 10
days. During this 10 day period, I was only sick for 1 day with a slight stomach ache and diarrhea.
The rest of the time I was out doing yard work and cutting dead limbs out of my trees.
I told my wife that if my T-Cells had that good of memory to protect me that well, I probably won't get the shot. After all,
what can the shot do for me that the virus hasn't already.
Mike -> Thomas 38 minutes ago
Obviously, you not only got immune to the Wuhan virus, but also to the globalist/collectivist and state propaganda. Those of
us who lived in Soviet socialist "paradise" get it back in the USSR while protecting our mind and soul from state propaganda and
government statistics.
With the time, I hope enough Americans will develop the same herd immunity to propaganda masquerading as news, unhealthy "guidance"
from government health agencies and corrupt intelligent agencies' deceptions that serve self-centered bureaucrats and political
operatives, not the country. G-d Bless!
Ed 3 hours ago
So more of the lies are being exposed, the lies that some who want to be in control have told are so bad, and yet some believe
them. Why was SARS not a continuing pandemic, if it is the same base virus , and did not have a vaccine. and yet you hear nothing
about it, could it be that people gained immunity and so it is not a horrible thing as this engineered virus. and remember that
SARS started in the same area of the world as this covid 19.
AB 3 hours ago
This is too funny. So at some point is anyone going to ask why this report is being featured on yahoo FINANCE? The answer
is in the reference to the publicly-traded, pharmaceutical companies named in the Dr.'s interview.
Last week,
we reported that several increasingly desperate communities across India have been embracing a controversial (at least, in the
US) strategy for trying to mitigate the fallout from the crisis. Communities have been doling out inexpensive anti-malaria drugs
as a prophylactic against COVID-19, citing scant data showing it could help lower mortality and hospitalization rates - which is
critical given India's nationwide shortage of hospital beds and oxygen to sustain seriously ill patients.
The drug in question, ivermectin, is in some ways similar to hydroxychloroquine, which also showed some evidence of being an effective
prophylactic to protect the most vulnerable against COVID-19 (President Trump memorably informed the press that he was taking it
daily at one point). But since India is mostly cut off from adequate supplies of vaccines and therapeutics like Gilead's remdesivir
(which studies have shown isn't all that effective anyway), public health officials have been forced to improvise.
The
Times of India published an editorial this week signed by Dr. Vikas Sukhatme and Vidula Sukhatme, two American academics and
medical professionals, suggesting a handful of cheap, commonplace drugs that could be taken as prophylactics by the most vulnerable
patients in India. The drugs aren't approved to treat COVID, but nevertheless have shown "remarkable promise in preventing or treating
the new coronavirus." Deploying them would likely reduce mortality and hospitalizations. While some of the drugs are currently being
tested in large-scale randomized trials, there's no time to wait for the outcome.
Instead, Indian health authorities should issue guidelines recommending use of the most promising drugs for each stage of COVID-19.
By so doing, physicians will be encouraged to prescribe them as interventions. The resulting data should of course be tracked for
any insights it might show.
The two main drugs cited by the doctors, ivermectin and fluvoxamine, have proven effective, and anecdotal unpublished data from
more than 400 acutely ill COVID-19 patients suggests that prescribing fluvoxamine and ivermectin together may be even more efficacious.
While daily case numbers have retreated from the peak in India, hospitalizations and mortality remain near all-time highs. Of
course, as developing nations fight to waive IP protections for COVID vaccines, the notion that cheap existing drugs might be effective
at combating COVID would represent yet another threat to Big Pharma's bottom line.
Read the full editorial below:
The COVID-19 humanitarian calamity unfolding in India is on a scale not seen in this pandemic. This is an extraordinary situation
"" and it may benefit from an extraordinary response.
There exist affordable, readily available and minimally toxic drugs approved for non-COVID-19 use which show remarkable promise
in preventing or treating the new coronavirus. Deploying these drugs in India is likely to rapidly reduce the number of COVID-19
patients, reduce the number requiring hospitalization, supplemental oxygen and intensive care and improve outcomes in hospitalized
patients.
Some of these drugs are being tested in large-scale randomized clinical trials in the US and abroad but in most cases, definitive
efficacy data is pending. With the current COVID-19 situation in India, we do not have time to wait for results of these studies.
Importantly, currently available safety and outcomes data on these drugs is strong enough that it is time to incorporate them into
national practice guidelines. Indian authorities should issue such guidelines on the most promising drugs for each stage of COVID-19.
By so doing, physicians will be encouraged to use these interventions. The resulting real world data from a few healthcare settings
in select cities should be tracked in real time and guidelines suitably revised. If such measures were adopted, we could see effects
in 3-4 weeks. This strategy might be unusual but it is not unheard of: France has the Temporary Recommendation for Use, a "regulatory
instrument which aims to allow, on a temporary basis, the use of a medicinal product to allow its effectiveness to be evaluated on
the basis of its use."
The choice of drugs is critical. We have worked closely with personnel at the Food and Drug Administration and have connected
with the World Health Organization and the National Institutes of Health to evaluate the merits of repurposed drugs. Based on a mechanistic
rationale, data in animal models, human retrospective analyses, clinical trials (some randomized, others not) and anecdotal human
data, we created a prioritized list of interventions that hold the greatest promise and that could be deployed at scale. For instance,
there is strong data from a randomized trial and a real-world study that administering fluvoxamine sharply reduces the need for hospitalization
in COVID-19 outpatients. Moreover, anecdotal unpublished data in over 400 acutely ill COVID-19 patients from several community practitioners
suggests that administering fluvoxamine and ivermectin together may be even more efficacious.
Intervention as early as possible after symptom onset is key. Ivermectin is already listed as a "MAY DO" on the ICMR and Indian
government guidelines for treatment of acute mild COVID-19 and we suggest that fluvoxamine be added in this category. Also, ivermectin
in the prophylactic setting merits serious consideration. For the hospitalized, there are treatments currently used for other conditions
that might reduce the need for ventilator support and lower the risk of death. These include inhaled adenosine, cyproheptadine and
dipyridamole. For ideas for which there is rather limited human data, the government should offer pre-approved pilot protocols and
funding for rapid implementation in select centers rather than issue a recommendation for use.
To be clear, it would be ideal to pursue large clinical trials to test the efficacy of all promising interventions. A randomized
adaptive design could efficiently sift through the many possibilities. It may be possible to rapidly set up parallel protocols in
India if government authorities can expedite the regulatory process and offer funding. US trial investigators can be persuaded to
provide protocols and web-based data collection tools.
We hope that the Indian government will take advantage of repurposed drug research and use temporary use authorizations or guidelines
to rapidly promote the most promising therapies at a national level while in parallel aggressively encourage pilot studies and large-scale
clinical trials with shovel-ready protocols and funding. Given the current situation, India has little to lose in piloting these
approaches: the potential gains could benefit not just the country but the world.
Is this because PCR test with high level of amplifications is junk or there are more serious problem with vaccination?
KYLE , May 19 2021 23:59 utc |
47
Well, it's official. One of my friends in the USSA who was fully vaccinated (Phizer I
think) within the past 3 months just got a positive COVID test. Teenage son brought it back
home and they all have it now.
uncle tungsten @40 - It looks like that bogus quote is used often, including by academics
and the paper I found was basically hidden, so it's an easy mistake to make by Strategic
Culture (whoever wrote that article). I had never seen/heard of that one so I looked it up
due to the non-contemporaneous looking language. Surprised to learn that "under-cover" is
actually a more recent term than "un-American" which I would have thought originated in the
1920s or 30s - or even 40s (WWII). According to that paper I found, it was first coined/used
just two years after Rush's passing. Go figure. Seems that several more of Rush's quotes as
told in the present day seem to be bogus as well.
Authored by Isabel van Brugen and Jan Jekielek via The Epoch Times,
The lockdowns implemented to curb the transmission of COVID-19 in the United States and
across the globe have not only been a "heinous abuse of power," but they have also failed to
protect the elderly and vulnerable, according to former White House COVID-19 adviser Dr.
Scott Atlas .
In an interview for Epoch TV's "
American Thought Leaders ," Atlas, a public health policy expert, suggested that the
consequences of lockdowns, which he believes have been largely fear-driven, will be felt in the
country for decades to come.
"We will have a massive price to pay for what was done in the United States," said
Atlas.
"The consequences of the lockdowns have been enormously harmful and they will last for
decades after this pandemic is completely finished."
In November 2020 Atlas resigned as former President Donald Trump's special adviser on the
White House pandemic task force. He is a senior fellow for the Hoover Institution at Stanford
University.
A large failure on the part of public health experts, Atlas said, has been the approach to
stop COVID-19, the disease caused by the
CCP (Chinese Communist Party) virus , at all costs, disregarding the consequences of the
policies that were implemented in an attempt to do so.
And while he believes that imposing initial lockdowns during the onset of the pandemic last
spring was an "appropriate" response, that was only because the world was reacting to extremely
"imperfect knowledge," including an estimated fatality rate that was higher than what the world
knows now.
Further, the restriction of movement orders implemented last year as the virus began to
spread across the country were initially pushed as short-term measures to prevent the
overcrowding of hospitals and health care facilities, he said.
Fear
Soon, Atlas said, rational thinking and critical thinking disappeared, and lockdown measures were driven by
fear. No longer was the goal to prevent the overcrowding of hospitals, but it gradually shifted
to stopping COVID-19 cases altogether.
"Fear is very powerful, and it was really shown how powerful fear is during this pandemic.
They [Americans] bought into it because it was temporary, because [people] thought that would
be a very small price to pay to get things sort of under control, and have some handle on how
to proceed," Atlas said.
The public health policy expert suggested that a "frenzy" took over out of fear, out of a
lack of leadership by the faces of public health to put things into context and perspective,
and to recognize immediately what the consequences of these lockdowns would be.
"There's a big reason why lockdowns were never recommended in prior pandemics," Atlas
added.
"And those rules, those simple rational logical assessments, were thrown out the
window."
Protecting the Elderly, Vulnerable
Lockdowns have ultimately failed, Atlas said, as they failed to protect the elderly and
high-risk individuals in the early months of the pandemic last year. Meanwhile, countless
others have suffered due to diversions of medical resources.
"We saw even in March, April, May [2020], the lockdown policies were number one, failing
to protect the high risk people""people were dying, they were elderly. The nursing home
deaths made up 40 to 50 percent of all deaths," Atlas explained.
"And it was through many of our states; at one point in Minnesota, 80 percent of the
deaths were [in] nursing homes."
Americans were also skipping chemotherapy treatments, while people who had suffered acute
strokes and heart attacks were too afraid to call an ambulance as they didn't want to be in a
medical setting, and the majority of live organ transplants weren't conducted during the onset
of the pandemic, Atlas said.
Meanwhile, child abuse and domestic abuse skyrocketed, opioid deaths and suicides surged,
and there has been a dramatic rise in young people suffering from depression and anxiety, he
added.
"I think that it is still somehow held by many people that OK, the lockdowns are an economic
harm, but we're saving lives. No, you're destroying families, you're destroying lives, and
you're literally killing people with the lockdowns," Atlas said.
Citing
June 2020 data from the U.S. Centers for Disease Control and Prevention, Atlas said that
one in four young adults contemplated suicide.
"The lockdowns failed, they still failed to protect the people who are high risk, and the
lockdowns destroyed and killed," Atlas said.
"Many other people destroyed families, sacrificed our children out of fear for
adults""even though the children do not have significant risk. And we didn't care as a
country. We kept them out of school."
He added: "It's a disgrace. It's a heinous abuse of the power of public health experts to do
what was done."
play_arrow
yerfej 4 hours ago
Funny how 78% of those who were hospitalized or died of "covid" were obese, and everyone
else was old or comorbid. BUT the progressive lunatics in government demanded schools be
shutdown...
NIRP-BTFD 4 hours ago
He added: "It's a disgrace. It's a heinous abuse of the power of public health experts
to do what was done."
Atlas should replace Fauci asap!
Dabooda 47 minutes ago
Actually, keeping the kids out of government schools is probably the best thing that you
could do for them, unless you really WANT them to turn into brain-dead propagandized drones
of indeterminate sex. Homeschool them for about
$200 (for a full 12 year curriculum.
chunga 3 hours ago
The facility where my wife works as an RN has not seen much of a pandemic materialize
over the last year and a half. Dystopia Virus was not the leading cause of death or
sickness but the staff spends a huge amount of time (almost all) on that at the expense of
everyone else. She tells me just as many died from extreme "treatment" for Dystopia Virus
and that they are not doing that anymore. One was a last ditch cancer treatment.
Of all the science not followed, the medical community has earned a great share of
this.
TightLiner 3 hours ago remove link
Guy I know is an ICU nurse. They quit using ventilators when 80% of people on them died.
He said, once you're on a ventilator you're not coming off alive.
chunga 3 hours ago remove link
All the ingredients for a pandemic are there, except the pandemic itself. Where my wife
works they are still occupying themselves largely with meetings and filling out Dystopia
forms. Corporate management is trying to bribe the staff to get the experimental injections
with bonuses and perks. That figure is right around 50/50 who've refused.
https://gab.com/LaurenWitzkeDE/posts/106233406197285394
Pernicious Gold Phallusy 3 hours ago
The reptilian viciousness of hospital administrators is on full display for all staff to
see. Nobody would forget opening their front door and finding a saltwater crocodile.
Al Jolson 4 hours ago
https://www.americasfrontlinedoctors.org/legal/tro
Motion for Temporary Restraining Order Against Use of COVID Vaccine in Children
The case will challenge the EUAs for the injections on several counts, based on the law
and scientific evidence that the EUAs should never have been granted, the EUAs should be
revoked immediately, the injections are dangerous biological agents that have the potential
to cause substantially greater harm than the COVID-19 disease itself, and that numerous
laws have been broken in the process of granting these EUAs and foisting these injections
on the American people.
Portal 4 hours ago remove link
Covid is a Trojan horse that brought Fascism to the western world. Just like Hitler,
"emergency powers" become permanent fascism.
When the Saints start getting dragged to jail you know your country is turning fascist.
"3rd Canadian pastor arrested for holding worship services violating COVID-19 orders"
jammyjo 3 hours ago
Atlas was pilloried, but he was the man we needed instead of Fauci. Atlas had a more
balance perspective. Fauci was scared of his own shadow, and maybe even corrupt since he
was a life long government hack.
strych10 2 hours ago remove link
The only reason such power was granted is because the country is chock-full of obese,
poorly educated morons who were easily frightened into ludicrously unworkable "solutions"
by a profit driven media and idiotic, power hungry politicians.
NoPension 2 hours ago remove link
Still the best.....
Local TV reporter addressing a group of Amish leaders..." Why hasn't covid seemed to
affect the Amish?"
Amish leader... " the Amish don't have tv"
Notable quotes:
"... may have contained downstream effects of some endothelial changes that would give rise to the hypercoagulable state that is characteristic of the disease ..."
"... We suggest that, in part, the presence of spike protein in circulation may contribute to the hypercoagulation in COVID-19 positive patients and may cause severe impairment of fibrinolysis. Such lytic impairment may be the direct cause of the large microclots we have noted here ..."
Amyloid deposits in response to spike protein
The researchers examined the fluorescent amyloid signals in abnormal clots and in healthy
platelet-poor plasma (PPP) with or without spike protein.
This showed a marked increase in dense abnormal amyloid clots, called amyloid deposits, in
PPP to which spike was added, with or without thrombin. Thrombin alone also created an
extensive fibrin clot. However, there was a significant increase in the percentage area of
amyloid deposits.
Related Stories
The greatest change followed the addition of both spike and thrombin.
Platelet
activation
When whole blood was exposed to spike protein even at low concentrations, the erythrocytes
showed agglutination, hyperactivated platelets were seen, with membrane spreading and the
formation of platelet-derived microparticles.
In all samples, spontaneous amyloid deposits formed after exposure to the spike protein
without the need for thrombin exposure.
Clotting in microfluidics channels
Microfluidics systems were set up to simulate extensive endothelial damage, with resulting
hypercoagulability. This showed that COVID-19 produced changes in the clotting profile of the
PPP.
Clot formation in healthy PPP occurred slowly and gradually, to a moderate size, and with
orderly clot layers that allowed blood flow to occur through the channel's center. These clots
were easily removed by flushing the channel at 1 mL/min.
The PPP from COVID-19 patients showed large disorderly clots that often projected into the
channel's center and obstructed the flow. These clots were impossible to dislodge at the
earlier flow rate or even at a higher flow.
Again, large clots formed in PPP from COVID-19 patients when it was exposed to thrombin in
about 90 seconds. However, most of the clotting happened in one burst, with not much
propagation of the clot thereafter, indicating rapid consumption of the thrombin.
This was not the case with PPP exposed to spike protein, where a fibrous laminar clot was
combined with a chaotic clot. Moderate flow disruption was also observed. These clots could
also be removed with similar ease. This intermediate state could be due to the absence of
multiple other biological factors that may have hindered the formation of the characteristic
clots seen in COVID-19 patients.
Mass spectrometry
The results of mass spectrometry of the healthy PPP with spike protein showed changes in the
structure of the beta and gamma fibrin(ogen) proteins, together with complement 3 and
prothrombin. These proteins showed resistance to degradation by trypsin, a powerful proteolytic
enzyme, in the presence of spike protein.
What are the implications?
The researchers show that the spike S1 not only interacts directly with both platelets and
with the key clotting protein fibrinogen and its activated form, fibrin, causing changes in the
protein that, in turn, alter the way blood clots.
In PPP, the addition of thrombin was found to induce fibrinogen's polymerization into a
fibrin mesh. Exposure to spike protein was shown to precipitate dense clots.
When spikes and thrombin were added to healthy PPP, the formation of abnormal amyloid
deposits was increased. These also showed significant changes in the blood cells'
ultrastructure, including the red cells and platelets.
The presence of extensive spontaneous fibrin networks following the addition of the spike
protein to whole blood matches the ultrastructural appearance seen on COVID-19-positive blood
smears. Here again, the primary features were anomalous clotting, amyloid in the clots, and
spontaneous fibrin network formation.
The study also shows that it may alter blood flow in COVID-19. The microfluidics simulation
showed that the PPP from COVID-19 patients, which is almost pure fibrinogen, formed large
obstructing clots. The PPP " may have contained downstream effects of some endothelial
changes that would give rise to the hypercoagulable state that is characteristic of the
disease ."
" We suggest that, in part, the presence of spike protein in circulation may
contribute to the hypercoagulation in COVID-19 positive patients and may cause severe
impairment of fibrinolysis. Such lytic impairment may be the direct cause of the large
microclots we have noted here ."
Thus, the free S1 subunit has harmful effects on the host even without direct infection of
the cells themselves. This strengthens the case for targeting the spike protein via antibodies
and vaccines.
*Important Notice
medRxiv publishes preliminary scientific reports that are not peer-reviewed and,
therefore, should not be regarded as conclusive, guide clinical practice/health-related
behavior, or treated as established information.
Journal reference:
Notable quotes:
"... Neutralization of B.1.617 and B.1.618 spike protein variants by REGN10933 and REGN10987. Image Credit: https://www.biorxiv.org/content/10.1101/2021.05.14.444076v1.full.pdf ..."
India's surge in SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2) infections are
linked to the new variants B.1.617 and B.1.618, with mutated spike proteins . In
recent months, it has caused a devastating second wave of the coronavirus disease 2019
(COVID-19) pandemic. According to the World Health Organization (WHO), it is reported that from
3 January 2020 to 17 May 2021, there have been over 25 million confirmed cases of COVID-19 with
over 274 thousand deaths.
Neutralization of B.1.617 and B.1.618 spike protein variants by REGN10933 and REGN10987.
Image Credit: https://www.biorxiv.org/content/10.1101/2021.05.14.444076v1.full.pdf
The mutations in these variants may contribute to the increased transmissibility of the
virus, and could potentially result in re-infection or resistance to the vaccine-elicited
antibodies. The mutations are driven by selective pressure for increased affinity for its
receptor, ACE2 (angiotensin-converting enzyme), and escape from neutralizing
antibodies . This raises concern over the fitness of the Indian SARS-CoV-2 variants and
their ability to escape the vaccine-elicited immune response.
In this context, researchers from the NYU Grossman School of Medicine, New York, USA, tested
the neutralization of B.1.617 and B.1.618 SARS-CoV-2 variant spike proteins and determined
their resistance to neutralization by convalescent sera, vaccine-elicited antibodies, and
therapeutic monoclonal antibodies.
To achieve this they generated lentiviruses pseudotyped by the variant proteins. They found
that these viruses with B.1.617 and B.1.618 spike proteins were neutralized with a 2-5-fold
decrease in titer by convalescent
sera and vaccine-elicited antibodies.
They observed a modest neutralization resistance to the vaccine-elicited antibodies. This is
good news as it suggests that the current vaccines will protect against the B.1.617 and B.1.618
42 variants. This study, led by Professor Nathaniel R. Landau, is recently posted on the
bioRxiv *
Our results lend confidence that current vaccines will provide protection against variants
identified to date."
The researchers also found that the resistance was caused by the L452R, E484Q, and E484K
mutations. Further, they reported that the variants were partially resistant to REGN10933,
which is one of the two mAbs constituting the Regeneron COV2 therapy (casirivimab (REGN10933)
with imdevimab (REGN10987), for the treatment of mild-to-moderate COVID-19).
The B.1.617 encodes a spike protein with the mutations L452R, E484Q, D614G, and P681R while
the B.1.618 spike has mutations Î"145-146, E484K, and D614G. The B.1.617 variant spike
protein contains L452R and E484Q mutations in the RBD in addition to D614G and the P681R
mutation near the proteolytic processing site and the B.1.618 spike has E484K in the RBD in
addition to D614G and the N-terminal deletion Î"145-146.
Related Stories
The researchers generated the lentiviral virions, expressing the spike proteins at a level
similar to that of wild-type D614G. They also tested the infectivity of the virus, reporting
that the B.1.617 spike protein (L452R/E484Q/P681R) was >2-fold increase in infectivity while
B.1.618 was similar to wild-type D614G.
Significantly, they found that the increased infectivity of the B.1.617 spike was attributed
to L452R mutation, which caused a 3.5-fold increase in infectivity and, in combination with
E484Q caused a 3-fold increase. Other point mutations had an insignificant effect on the
infectivity.
Both variants B.1.617 and B.1.618 have increased affinity for ACE2 and the researchers found
that both are partially resistant to the monoclonal antibodies. They discussed the mutations,
the expressed proteins, and the subsequent effect on binding and infection.
In this study, the researchers reported that the virus variants B.1.617 and B.1.618 spike
were partially resistant to neutralization, with an average 3.9-fold and 2.7-fold decrease in
IC50 for convalescent sera and antibodies elicited by Pfizer and Moderna mRNA vaccines,
respectively. The neutralization resistance was mediated by the L452R, E484Q, and E484K
mutations. The resistance of these variants is similar to the previous variants.
Even with the 3-4-fold decrease in neutralization titer of vaccine-elicited antibodies,
average titers were around 1:500, a titer well above that found in the sera of individuals
who have recovered from infection with earlier unmutated viruses."
Significantly, this study reassures that the vaccinated individuals will remain protected
against the B.1.617 and B.1.618 variants.
Commenting on the other vaccines, the researchers said, "The analyses in this study were
restricted to the mRNA-based vaccines but there is no reason to believe that vector-based
vaccines such as that of Johnson and Johnson that express a stabilized, native, full-length
spike protein would be different with regarding antibody neutralization of virus
variants."
*Important Notice
bioRxiv publishes preliminary scientific reports that are not peer-reviewed and,
therefore, should not be regarded as conclusive, guide clinical practice/health-related
behavior, or treated as established information.
H ere is link to Dr. Makary interview. This may
not be the Video mentioned in the article above but it is a similar gist of his critizisms of the CDC.
Dr. Marty Makary made the comments during a recent interview, noting that "natural immunity works" and it is wrong to vilify those
who don't want the vaccine because they have already recovered from the virus.
Makary criticised "the most slow, reactionary, political CDC in American history" for not clearly communicating the scientific
facts about natural immunity compared to the kind of immunity developed through vaccines.
" There is more data on natural immunity than there is on vaccinated immunity, because natural immunity has been around longer,"
Makary emphasised.
"We are not seeing reinfections, and when they do happen, they're rare. Their symptoms are mild or are asymptomatic," the professor
added.
"Please, ignore the CDC guidance," he urged, adding "Live a normal life, unless you are unvaccinated and did not have the infection,
in which case you need to be careful."
"We've got to start respecting people who choose not to get the vaccine instead of demonizing them," Makary further asserted.
The professor's comments come amid a plethora of
media generated propaganda suggesting that natural immunity isn't enough, and that those who do not choose to take the vaccine
should be socially ostracised Justus D. Barnes 4 hours ago (Edited) remove link
I would not call it a hoax as some people do get sick and die.
However. Some people are allergic to peanuts. So lets force everyone to get vaccinated against peanuts?
I think of this whole thing as $#IT politicians shoving their $#IT policies down stupid peoples throats. In a free America
any thoughtful person would asses the danger that corona or a peanut would present to them personally and then take the action
they thought best. IMHO If your state does not let you make the choice for yourself then you join a class action lawsuit against
your state or move.
FurnitureFireSale 4 hours ago remove link
And that's the problem in that what America has become: a bunch of thoughtless sheep that do what their idols tell them to
do; what the commercials tell them to do; what the brainwashing convinces them to do. There are many, many of them and a good
amount of thoughtful ones (us)too. It is the latter having these discussions about these therapies, no matter how much the MSM
and FAANG's try to supress it. Many highly intelligent people I know have gone ahead and gotten their shots. Several in my circle
have not- never will. The have nots understand just what is going on. The liberal states that are pushing this agenda need to
be reeled in via a class action. One should not be forced to move based upon their vaccination status. It's as arbitrary as saying
"move to a state where they don't serve peanuts". You're exactly right.
sun tzu 3 hours ago (Edited) remove link
Deaths from purely from covid was probably in the 25,000 range in the past 14 months, which is less than half of 5 months of
flu deaths each year. Some died due to pneumonia or cytokine storm. Others died when the spike proteins got into their blood and
caused clots. The vast majority died with covid, either real or thru a false positives. Probably 25-50K were murdered on ventilators.
philipat 1 hour ago remove link
As I have written about previously, the CDC/WHO are playing (political) games with science and their actions only discredit
themselves and raise other obvious questions which challenge the official explanation(s) of events, in summary as follows:
The definition of Herd Immunity has been changed (including in the Merriam-Webster Dictionary) to EXCLUDE natural immunity
as a contributing factor. This is scientifically false because naturally acquired immunity is the best type of immunity because
it is a complete immune response which conveys long-lasting immunity and prevents transmission of any virus. This is NOT true
for the "vaccines" whose manufacturers only claim a reduction in the severity of any symptoms. The obvious conclusion based
on the science is that naturally immune people have a stronger claim on "Vaccine Passports" than the vaccinated.
Not only is it unnecessary for naturally immune people to be vaccinated, there are potential dangers in doing so. Based
again on scientific knowledge from earlier attempts to develop vaccines for CoVs, there is a very real risk of ADE (Antibody
Dependent Enhancement), also described as Pathogenic Priming from occurring when people with non-neutralizing antibodies are
exposed to further challenge from either a live virus or high concentrations of viral antigen. This can potentially occur in
both vaccinated people (we will know during the next "Flu" season) and in naturally immune people exposed to high concentrations
of viral antigen which triggers non-neutralizing antibodies. The subsequent autoimmune reaction can result from a triggered
"cytokine storm" which can result in the shutdown of vital organs and death,The only possible reason for the above denials 1-2) of the science is so as to comply with the official narrative that everyone
needs vaccination "" presumably for reasons other than science and public health.
The CDC still recommends the RT-qPCR test to diagnose "new cases" at a cycle threshold (Ct) of >35 cycles, typically run
at 35-45 or even 50 cycles. This despite the fact they fully understand that at these high cycle counts, the numbers of "false
positives" are high (up to 95% in some labs). However, in coming to terms with "a few breakthrough cases" of disease in vaccinated
people, CDC has been running trials to sequence the virus (in the hope of blaming new variants) obtained from such people.
However, to be included, only samples from patients confirmed positive with a PCR test run at a Ct of <28 cycles are allowed.
Why the difference?
The dilemma for CDC here is obvious. If they recommend that for reasons of accuracy, ALL PCR tests are run at a Ct of <28,
they will not be able to find many "new cases" (a/k/a false positives) to inflate the case numbers and have ample material
to blame "Covid deaths" on. If they run the trials on "breakthrough infections" at a Ct of >35 (as recommended for general
use) they will "confirm" (by their own definition) thousands of such " extremely rare breakthrough cases". This clearly demonstrates
duplicity on the part of CDC and destroys their credibility, which has been built on science not politics.
The Virus origin dilemma. The Overton window has allowed two, and only two, "explanations" for the origin of the virus.
Setting aside the fact that whenever the Establishment presents a limited number of explanations for anything, they are always
all wrong (and in this case there are other explanations surrounding the Military Games, held in Wuhan at around the time the
first patients were recorded) it is now obvious that the desired conclusion is a "leak" at the Wuhan Institute of Virology
(WIV). That means we must also set aside the fact that Bio Safety Level 4 labs don't just "leak" "" I can attest to this from
personal experience of BSL training.
The dilemma for the Authorities with this explanation, not yet widely recognised, is that if indeed this is the explanation,
it means that wild SARS-CoV-2 virus (and other man made variants in the "gain of function" research, was being experimented
with in WIV so as to infect the respiratory system of those "infected". Other bodily contamination transported out of the lab
is entirely impossible due to the security features built-in at BSL-4 facilities (Pressure gradients, UV exit lighting, 3 changes
of clothing involving showers with various chemical components etc. "" these are SERIOUS safety precautions)
That being the case, why then has it not been possible to isolate and purify said virus (and its variants) for the purposes
of confirming its existence and for use in more accurate tests and diagnostics plus for use in making natural (real) vaccines?
konputa 4 hours ago
The CDC are vaccine pushers and owners of numerous vaccine patents. It seems to me they are doing their job as intended, it's
just that the public misunderstands their purpose. Their mission isn't public health.
CheapBastard 5 hours ago (Edited)
That's exactly what my doc told me. Stay healthy and take the relevant supplements like Vitamin D. Most likely have immunity
from previous Flu infections with cross-over protection.
Problem is for the CDC and Big Pharma is their Fear **** can't be promoted and they can't make mind-numbing profits from natural
immunity.
What a mess_man 4 hours ago
We knew this last spring with the Diamond Princess.
Notable quotes:
"... They always have these congressional investigations, yet nothing ever happens. ..."
Kentucky Republican discusses why he questioned the top health official over funding of the controversial Wuhan Institute of Virology
on 'Fox News Primetime.' #FoxNews #FoxNewsPrimetime
Tim E 1 day ago
They always have these congressional investigations, yet nothing ever happens.
GwenEcho Taylor 1 day ago
"Medical science has made such tremendous progress that there is hardly a healthy human left." - Aldous Huxley
1 day
ago
Thank you for exposing Fauci for who he really is, the truth is being revealed.
1 day
ago
" It came from wet markets " I remember when they pushed that narrative so hard when they really manufactured it 🤣🤣
Hemiola , May 16 2021 18:16 utc |
33
"Based on the lack of a rational explanation for the actions of the WHO, Merck, FDA and Unitaid, we conclude that they result
from an active disinformation campaign ... "
FLCCC Alliance statement on the irregular actions of Public Health Agencies and the widespread disinformation campaign against
Ivermectin
Nice South African summary:
Don't mention Ivermectin; It'll
Affect the Vaccine Rollout
The Virus and the Parasite
Grieved , May 17 2021 3:06 utc |
95
@33 Hemiola
Thank you for the latest release from FLCCC. When you find the time to comment, you always supply powerful material - I am
extraordinarily grateful for this.
I just spent the time to read the release, and I was absorbed from beginning to end. Of course, there's some unavoidable scientific
terminology, but very little, and most of the document stands as a revolutionary manifesto, a call to action, a call to resist
the misinformation and the disinformation permeating the COVID-19 pandemic.
The document illustrates in a verifiable and succinct charge how the WHO has loaded the dice against the use of ivermectin
as both a prophylactic and a treatment for COVID-19, in order to argue against its adoption - and this, in a world that is increasingly
adopting its use because it quite simply works.
It works, and the results from all over the world are recorded by doctors, showing that it works up to a 90% effectiveness
in the main and close to 100% in some cases, and it does this with negligible collateral harm demonstrated across billions of
doses and many decades - and the WHO, despite that in 2018 it formally lauded its safety, now says that it doesn't work and that
it may be dangerous.
~~
So what is the Why of the WHO?
This release from FLCCC explains why and describes the underlying, systemic rottenness in the western medical system, how it
has been tainted for decades by corporations and large funding sources - and how the common doctors, fighting to do no harm and
to save lives, are up against a wall of opposition during this pandemic that is breathtakingly huge.
The FLCCC press release goes beyond the medical science and explains also the corporate tactics that have demolished scientific
method. It presents a call to action, and sketches the only tools we have to resist. It says much that we already know - but these
are doctors and awarded researchers telling us all the things that are so obviously fishy in the institutional responses
to the pandemic.
Big Pharma, Big Science, Big Media, Big Tech, Big Government, Big Foundations - all in collusion, all following the trail originally
blazed by Big Tobacco.
See, we know how it works because we've watched it for decades. The FLCCC release does us the service of reminding us and enumerating
the instances when corporate venality (my word, not theirs) has destroyed the truth simply to make money.
I recommend it:
FLCCC Alliance Statement on the Irregular Actions of Public Health Agencies and the Widespread Disinformation Campaign Against
Ivermectin
What CDC knows what we do know to issue such draconian guidelines? This looks like is a
concentration camp not summer camp...
Notable quotes:
"... Two-layer masks should be worn at all times "" indoors and out ""except for eating, drinking and swimming ..."
"... Don't allow close-contact games and sports ..."
"... Avoid sharing of objects such as toys, games and art supplies ..."
"... Separate children on buses by skipping rows ..."
"... Divide children into "cohorts" and then keep them away from other cohorts ..."
"... Children should stay three feet away from kids in their cohort and six feet away from those outside their cohort; campers and staff should stay six feet from each other, as should fellow staff members ..."
"... While eating and drinking, stay six feet away from everybody, even your own cohort ..."
CDC Trapped in March 2020 Mindset
In April, the CDC published guidance
for operating youth camps that was the latest eye-rolling example of CDC maximalism that
conflicts with what we've learned about Covid-19.
Before we examine the CDC guidance, let's review some of the key things that we now know
about Covid-19 that we didn't in March 2020:
Covid-19 presents little risk at all to children. According to CDC data, only
295 children age 0-17 have died with Covid-19. Compare that to the CDC's estimation
that 600
died of the flu during the 2017-18 season.
Outdoor transmission pretty much never happens. An Irish
study of more than 232,000 Covid-19 cases found only 0.1% of cases were transmitted
outside.
Surface transmission isn't a material source of spread. The CDC has
declared the risk of contracting the virus by touching surfaces or objects is low, and
that rather than cleaning with disinfectant, "soap and water is enough to reduce risk"
(unless there's a known or suspected Covid-19 case in a community setting).
Vaccines are abundantly available. According to the CDC's vaccination data , 60.5% of U.S.
adults have have received at least one vaccine dose, and 48.4% are fully vaccinated. Gone
are the days when finding the vaccine was a challenge; today, anyone who wants the vaccine
can readily find it.
Covid-19 cases and deaths are in a free fall. The 7-day averages for cases and deaths
have respectively fallen 89% and 83% from
their peaks. On Sunday, the entire state of Texas
reported not a single death from the virus. Today, San Francisco General Hospital has
no Covid-19 patients for the first time
since March 2020.
With that knowledge in mind, here are some key ingredients in the CDC's recipe
for dystopian summer fun:
Two-layer masks should be worn at all times "" indoors and out ""except for eating,
drinking and swimming
Don't allow close-contact games and sports
Avoid sharing of objects such as toys, games and art supplies
Separate children on buses by skipping rows
Divide children into "cohorts" and then keep them away from other cohorts
Children should stay three feet away from kids in their cohort and six feet away
from those outside their cohort; campers and staff should stay six feet from each other, as
should fellow staff members
While eating and drinking, stay six feet away from everybody, even your own
cohort
Who exactly are these draconian, fun-killing guidelines meant to protect? The children
aren't in any meaningful danger"" the number of children who typically drown in a given
year is more than double the number of child Covid deaths we've observed in 15 months .
Meanwhile, against a backdrop of rapidly-vanishing Covid-19 infections across the country,
camp staff will have had more than ample opportunity to be fully vaccinated against Covid-19
before the first kids arrive.
We're told to "follow the science," but what is the CDC following? The agency's guidelines
read like they were written during the early dark ages of the Covid outbreak, when the peril
was still filled with overwhelming mystery, and "erring on the side of caution" still had a
trace of credibility.
As Columbia University pediatric immunologist Mark Gorelik told
New York Magazine , " We know that the risk of outdoor infection is very low. We know risks
of children becoming seriously ill or even ill at all is vanishingly small. And most of the
vulnerable population is already vaccinated. I am supportive of effective measures to restrain
the spread of illness. However, the CDC's recommendations cross the line into excess and are,
frankly, senseless. Children cannot be running around outside in 90-degree weather wearing a
mask. Period. "
Read more and subscribe at https://starkrealities.substack.com/
4 hours ago
Who cares what the CDC says? They have ZERO credibility and should be charged with fraud and
"Crimes Against Humanity"
UpTo11 4 hours ago remove link
Just went to a high school graduation ceremony in Texas. 1 student had a mask. No one else
in the stadium of 400. Not sure who wears masks anymore at all.
ChargingHandle 3 hours ago remove link
Come to oregon and you will see all species of sheeple wearing masks even when completely
by themselves.
GunnerySgtHartman 2 hours ago
I still see people wearing masks while driving their cars ... with nobody else in the cars
... talk about sheeple.
Snakerockhiker 3 hours ago
The CDC guidance has nothing to do with Covid-19 and everything to do with maintaining and
increasing fear, breaking down societal relationships, and ensuring people are following
operant conditioning protocols like Pavlov's dogs. A gang of criminals are running America's
medical heirarchy. We need to eliminate them.
Looks like the chance to win a million bucks can give vaccination rates a real shot in the
arm.
Ohio saw its COVID-19 vaccination rate jump 45% between May 14-19 as compared to the
previous week, thanks in part to the state's Vax-A-Million lottery,
Gov. Mike DeWine told reporters on Wednesday . Last week, the state said it recorded a 28%
spike in vaccinations in the days following the lottery announcement.
An
Associated Press analysis found that the number of Ohio residents ages 16 and up who got
their first COVID shot spiked 33% in the week after
DeWine announced the state would be giving away $1 million prizes and in-state public college
scholarships as incentives to get more residents inoculated.
Each week, adult Ohioans who have received at least one COVID-19 vaccine dose will enter a
random drawing to win a million dollars. And younger vaccinated Ohio residents between the ages
of 12 and 17 will be part of a weekly random drawing to get a four-year scholarship to an Ohio
public university, which will include tuition, room, board and books. There will be five
winners for each prize selected over the next five weeks.Wednesday night, the Ohio lottery
announced the first two winners: Abbigail Bugenske of Silverton, near Cincinnati, won $1
million, while Joseph Costello of Englewood, near Dayton, won the college scholarship. Each
Wednesday moving forward, another adult and another teen winner will be revealed at 7:29 p.m.
through June 23.
More than 2.7 million adults registered for the cash prizes, and more than 100,000 teens are
vying for the scholarships.
psychohistorian
104
I continue to be troubled by the Western Covid response of new vaccines.
Unless you haven't read Big Pharma bragging, they are projecting revenues of $100 billion
this year with $20+ projected by Pfizer alone. Given my jaded economics view of the industry
and Western governments owned by the financial elite, it is not beyond my belief that this
controlled taking advantage of a health care crisis is conscious war criminal behavior just
like the ongoing (since at least 2008) loading of the US Treasury with debt while the profits
go to private finance elite.
Back to further financialization of the Health Care world. I never saw the 1973 movie
Soylent Green but below is the last Wiki line about the movie that resonates with my
perspective of the Western brainwashed becoming a new income stream for Big Health just like
wars are income streams for the MIC
"
When you go to a poker game, look around and can't see who the sucker of the evening is,
take a hint, its you
Its time to shoot the TV folks and end other brainwashing inputs that make it so you can't
see how the world really works.....private finance barbarism which is currently in a
civilization war with China's not barbarism/public finance approach.
With Grieved's friendly update.....
Hell-bent of vaccines?
Five people between D.C., Maryland and Virginia have been tested for the
new strain of coronavirus. There are no confirmed cases in the DMV. https://imasdk.googleapis.com/js/core/bridge3.460.0_en.html#goog_322948139 Author: Nick
Boykin (WUSA9), Jordan Fischer Published: 10:47 PM EST January 27, 2020 Updated: 3:33 PM EST
January 28, 2020
WASHINGTON -- With worries about the coronavirus spreading nationally, the National
Institute of Health's National Institute of Allergy and Infectious Diseases (NIAID) is working
on a vaccine to help combat the virus.
At its Bethesda headquarters, NIAID will be working with a company called Moderna, who
received a grant from the Coalition for Epidemic Preparedness Innovations. Their mission is to
accelerate the development of vaccines against emerging infectious diseases during an outbreak,
according to the Coalition for Epidemic Preparedness Innovations (CEPI) . CEPI is helping
fund the grant money being used.
https://5e8b0d7b0c3a879ded0a413bf89113bc.safeframe.googlesyndication.com/safeframe/1-0-38/html/container.html
https://cdn.embedly.com/widgets/media.html?src=https%3A%2F%2Fwww.youtube.com%2Fembed%2FTYG3EGWUk1U%3Ffeature%3Doembed&display_name=YouTube&url=https%3A%2F%2Fwww.youtube.com%2Fwatch%3Fv%3DTYG3EGWUk1U&image=https%3A%2F%2Fi.ytimg.com%2Fvi%2FTYG3EGWUk1U%2Fhqdefault.jpg&key=0350728de3d54ab7950f978fc80d4a70&type=text%2Fhtml&schema=youtube
Two other organizations, Inovia Pharmaceuticals and The University of Queensland, also
received grants, according to CEPI.
"NIAID has mobilized a research response to 2019-nCoV that builds on experience with
SARS-CoV, MERS-CoV and other emerging pathogens," NIAID said in a statement about the grant.
"NIAID has begun early stage development of an mRNA (messenger RNA) vaccine for 2019-nCoV. mRNA
vaccines direct the body's cells to express a protein to elicit a broad immune response
including high levels of neutralizing antibodies. The expressed protein is designed based on
knowledge of the virus structure, but the platform does not contain live or inactivated virus.
The mRNA platform can be quickly adapted and manufactured efficiently."
https://platform.twitter.com/embed/Tweet.html?dnt=false&embedId=twitter-widget-0&features=eyJ0ZndfZXhwZXJpbWVudHNfY29va2llX2V4cGlyYXRpb24iOnsiYnVja2V0IjoxMjA5NjAwLCJ2ZXJzaW9uIjpudWxsfSwidGZ3X2hvcml6b25fdHdlZXRfZW1iZWRfOTU1NSI6eyJidWNrZXQiOiJodGUiLCJ2ZXJzaW9uIjpudWxsfSwidGZ3X3R3ZWV0X2VtYmVkX2NsaWNrYWJpbGl0eV8xMjEwMiI6eyJidWNrZXQiOiJjb250cm9sIiwidmVyc2lvbiI6bnVsbH19&frame=false&hideCard=false&hideThread=false&id=1220838637547319297&lang=en&origin=http%3A%2F%2Fwww.wusa9.com%2Farticle%2Fnews%2Flocal%2Fmaryland%2Fnih-working-on-coronavirus-vaccine-in-maryland%2F65-7bb9062f-de57-49a5-9470-d7c3a19b97f0&sessionId=f13b8d1a366000bf767e00a00bfc99fe56dfb878&siteScreenName=WUSA9&theme=light&widgetsVersion=82e1070%3A1619632193066&width=550px
While Moderna will develop the vaccine, NIAID will provide IND-enabling studies and a Phase
1 clinical study in the U.S.
NIAID has said that while it has started its work towards helping establish a vaccine, its
availability in the coming months is not likely.
a very small number of teenagers and young adults vaccinated against the coronavirus may
have experienced heart problems, according to the
agency's vaccine safety group .
... The condition, called myocarditis, is an inflammation of the heart muscle, and can occur
following certain infections.
... The cases seem to have occurred predominantly in adolescents and young adults about four
days after their second dose of one of the mRNA vaccines, made by Moderna and Pfizer-BioNTech.
And the cases were more common in males than in females.
... In the general population, about 10 to 20 of every 100,000 people each year develop myocarditis ,
experiencing symptoms from fatigue and chest pain to arrhythmias and cardiac arrest. Many
others likely have mild symptoms and are never diagnosed, according to researchers.
.. The agency did not specify the ages of the patients involved. The Pfizer-BioNTech vaccine
has been authorized for ages 16 and above since December.
... On May 14, the C.D.C. alerted clinicians to the possible link between myocarditis and
vaccines. And on May 17, the working group reviewed data on myocarditis from the Department of
Defense, reports filed with the Vaccine Adverse Event Reporting System and others.
Notable quotes:
"... was vaccinated before it was available to any of us peasants. About 3 weeks ago she was home sick with Covid. He husband got it too, and he was also vaccinated as well. ..."
Just_do_what_they_tellya 3 hours ago
My 29 year old niece that is as skinny as a broom stick is an RN in a pedes unit, and was vaccinated before it was available to
any of us peasants. About 3 weeks ago she was home sick with Covid. He husband got it too, and he was also vaccinated as well.
PHE figures show Covid outbreak is STILL flat despite rapid spread of Indian variant as
expert says it won't stop lockdown easing plans but SAGE adviser warns third wave has begun and
all 10 areas with biggest outbreaks are mutant strain hotspots
Some 95 out of 149 local authorities in England saw Covid cases dip last week. Dr Yvonne
Doyle said the latest data was 'hugely encouraging' but that there was still concern over the
Indian variant.
Last December, Yeadon, a British national,
filed
a petition
with the European Medicines Agency (EMA) to immediately suspend testing on these experimental vaccines due to many
safety concerns, including pathogenic priming, which involves "
an exaggerated immune reaction,
especially when the test person is confronted with the real, 'wild' virus after vaccination
."
In their
white
paper
on the topic, AFLDS warned that such reactions, which can be fatal, "
are difficult to
prove
," as they are often interpreted as infection with "
a worse virus
," or, perhaps, a
more dangerous variant.
Having maintained that there is "
no
need of vaccines
" for COVID-19, Yeadon emphasizes below, "
PLEASE warn every person not to go
near top up vaccines. There is absolutely no need to them
."
At the outset, Dr. Yeadon said:
"
I'm well
aware of the global crimes against humanity being perpetrated against a large proportion of the world's population. I feel great
fear, but I'm not deterred from giving expert testimony to multiple groups of able lawyers like Rocco Galati in Canada and
Reiner
Fuellmich
in Germany. I have absolutely no doubt that we are in the presence of evil (not a determination I've ever
made before in a 40-year research career) and dangerous products."
"
In the U.K., it's abundantly clear that the authorities are bent
on a course which will result in administering 'vaccines' to as many of the population as they can. This is madness, because even
if these agents were legitimate, protection is needed only by those at notably elevated risk of death from the virus. In those
people, there might even be an argument that the risks are worth bearing. And there definitely are risks which are what I call
'mechanistic': inbuilt in the way they work.
"
"
But all the other people, those in good health and younger than
60 years, perhaps a little older, they don't perish from the virus. In this large group, it's wholly unethical to administer
something novel and for which the potential for unwanted effects after a few months is completely uncharacterized. In no other
era would it be wise to do what is stated as the intention. Since I know this with certainty, and I know those driving it know
this too, we have to enquire: What is their motive?
"
"
While I don't know, I have strong theoretical answers, only one
of which relates to money and that motive doesn't work, because the same quantum can be arrived at by doubling the unit cost and
giving the agent to half as many people. Dilemma solved. So it's something else. Appreciating that, by entire population, it is
also intended that minor children and eventually babies are to be included in the net, and that's what I interpret to be an evil
act."
"There is no medical rationale for it. Knowing as I do that the
design of these 'vaccines' results, in the expression in the bodies of recipients, expression of the spike protein, which has
adverse biological effects of its own which, in some people, are harmful (initiating blood coagulation and activating the immune
'complement system'), I'm determined to point out that those not at risk from this virus should not be exposed to the risk of
unwanted effects from these agents.
"
INTERVIEWER: In a
talk
you
gave four months ago, you said:
The most
likely duration of immunity to a respiratory virus like SARS CoV-2 is multiple years. Why do I say that? We actually have the
data for a virus that swept through parts of the world seventeen years ago called SARS, and remember SARS CoV-2 is 80 percent
similar to SARS, so I think that's the best comparison that anyone can provide.
The evidence is clear: These very clever cellular immunologists
studied all the people they could get hold of who had survived SARS 17 years ago. They took a blood sample, and they tested
whether they responded or not to the original SARS and they all did; they all had perfectly normal, robust T cell memory. They
were actually also protected against SARS CoV-2, because they're so similar; it's cross immunity.
So, I would say the best data that exists is that immunity should
be robust for at least 17 years. I think it's entirely possible that it is lifelong. The style of the responses of these people's
T cells were the same as if you've been vaccinated and then you come back years later to see if that immunity has been retained.
So I think the evidence is really strong that the duration of immunity will be multiple years, and possibly lifelong.
In other words, previous exposure to SARS � that is, a variant similar to SARS CoV-2 � bestowed SARS CoV-2 immunity.
The Israel government cites new variants to justify lockdowns, flight closures, restrictions, and Green Passport issuance. Given the
Supreme Court verdict, do you think it may be possible to preempt future government measures with accurate information about
variants, immunity, herd immunity, etc. that could be provided to the
lawyers
who
will be challenging those future measures?
DR. YEADON:
"What I
outlined in relation to immunity to SARS is precisely what we're seeing with SARS-CoV-2. The study is from one of the best labs
in their field.
"So, theoretically, people could test their T-cell
immunity
by
measuring the responses of cells in a small sample of their blood. There are such tests, they are not 'high throughout' and they
are likely to cost a few hundred USD each on scale. But not thousands. The test I'm aware of is not yet commercially available,
but research only in U.K.
"However, I expect the company could be induced to provide
test
kits
"for research" on scale, subject to an agreement. If you were to arrange to test a few thousand non-vaccinated Israelis,
it may be a double edged sword. Based on other countries experiences, 30-50percent of people had prior immunity & additionally
around 25percent have been infected & are now immune.
"Personally, I wouldn't want to deal with the authorities on their
own terms: that you're suspected as a source of infection until proven otherwise. You shouldn't need to be proving you're not a
health risk to others. Those without symptoms are never a health threat to others. And in any case, once those who are concerned
about the virus are vaccinated, there is just no argument for anyone else needing to be vaccinated."
INTERVIEWER: My understanding of a "
leaky
vaccine
" is that it only lessens symptoms in the vaccinated, but does not stop
transmission; it therefore allows the spread of what then becomes a more deadly virus.
For example, in China they deliberately use leaky Avian Flu vaccines to quickly cull flocks of
chicken, because the unvaccinated die within three days. In Marek's Disease, from which they needed to save all the chickens, the
only solution was to vaccinate 100% of the flock, because all unvaccinated were at high risk of death. So how a leaky vax is
utilized is intention-driven, that is, it is possible that the intent can be to cause great harm to the unvaccinated.
Stronger strains usually would not propagate through a population because they kill the host too
rapidly, but if the vaccinated experience only less-serious disease, then they spread these strains to the unvaccinated who contract
serious disease and die.
Do you agree with this assessment? Furthermore, do you agree that if the unvaccinated become the
susceptible ones, the only way forward is HCQ prophylaxis for those who haven't already had COVID-19?
Would the Zelenko Protocol work against these stronger strains if this is the case?
And if many already have the aforementioned previous "17-year SARS immunity", would that then
not protect from any super-variant?
DR. YEADON: "I think the Gerrt Vanden Bossche story is highly suspect. There is no evidence at all that vaccination is leading or
will lead to 'dangerous variants'. I am worried that it's some kind of trick.
"As a general rule, variants form very often, routinely, and tend to become less dangerous & more infectious over time, as it comes
into equilibrium with its human host. Variants generally don't become more dangerous.
"No variant differs from the original sequence by more than 0.3%. In other words, all variants are at least 99.7% identical to the
Wuhan sequence.
"It's a fiction, and an evil one at that, that variants are likely to "escape immunity".
"Not only is it intrinsically unlikely � because this degree of similarity of variants means zero chance that an immune person
(whether from natural infection or from vaccination) will be made ill by a variant � but it's empirically supported by high-quality
research.
"The
research
I
refer to shows that people recovering from infection or who have been vaccinated ALL have a wide range of immune cells which
recognize ALL the variants.
"
This
paper
shows WHY the extensive molecular recognition by the immune system makes the tiny changes in variants irrelevant.
"I cannot say strongly enough: The stories around variants and need for top up vaccines are FALSE. I am concerned there is a very
malign reason behind all this. It is certainly not backed by the best ways to look at immunity. The claims always lack substance
when examined, and utilize various tricks, like manipulating conditions for testing the effectiveness of antibodies. Antibodies are
probably rather unimportant in host protection against this virus. There have been a few 'natural experiments', people who
unfortunately cannot make antibodies, yet are able quite successfully to repel this virus. They definitely are better off with
antibodies than without. I mention these rare patients because they show that antibodies are not essential to host immunity, so some
contrived test in a lab of antibodies and engineered variant viruses do NOT justify need for top up vaccines.
"The only people who might remain vulnerable and need prophylaxis or treatment are those who are elderly and/or ill and do not wish
to receive a vaccine (as is their right).
"The good news is that there are multiple choices available: hydroxychloroquine, ivermectin, budesonide (inhaled steroid used in
asthmatics), and of course oral Vitamin D, zinc, azithromycin etc. These reduce the severity to such an extent that this virus did
not need to become a public health crisis."
INTERVIEWER: Do you feel the FDA does a good job regulating big pharma? In what ways does big
pharma get around the regulator? Do you feel they did so for the mRNA injection?
DR. YEADON: "Until recently, I had high regard for global medicines regulators. When I was in Pfizer, and later CEO of a biotech I
founded (Ziarco, later acquired by Novartis), we interacted respectfully with FDA, EMA, and the U.K. MHRA. Always good quality
interactions.
"Recently, I noticed that the Bill & Melinda Gates Foundation (BMGF) had made a grant to the Medicines and Healthcare products
Regulatory Agency (MHRA)! Can that ever be appropriate? They're funded by public money. They should never accept money from a
private body.
"So here is an example where the U.K. regulator has a conflict of interest.
"The European Medicines Agency failed to require certain things as disclosed in the 'hack' of their files while reviewing the Pfizer
vaccine.
"You can find examples on
Reiner
Fuellmich
's 'Corona Committee' online.
"So I no longer believe the regulators are capable of protecting us.
'Approval'
is therefore meaningless
.
"Dr. Wolfgang Wodarg and I petitioned the EMA Dec 1, 2020 on the genetic vaccines. They ignored us.
"Recently, we wrote privately to them, warning of blood clots, they ignored us. When we
went
public
with our letter, we were completely censored. Days later, more than ten countries paused use of a vaccine citing blood
clots.
"I think the big money of pharma plus cash from BMGF creates the environment where saying no just isn't an option for the regulator.
"I must return to the issue of 'top up vaccines' (booster shots) and it is this whole narrative which I fear will he exploited and
used to gain unparalleled power over us.
"PLEASE warn every person not to go near top up vaccines. There is absolutely no need to them.
"As there's no need for them, yet they're being made in pharma, and regulators have stood aside (no safety testing), I can only
deduce they will be used for nefarious purposes.
"For example, if someone wished to harm or kill a significant proportion of the world's population over the next few years, the
systems being put in place right now will enable it.
"It's my considered view that it is entirely possible that this will be used for massive-scale depopulation."
Reprinted with permission from
America's
Frontline Doctors.
Brian Sandle
April 14, 2021 at 12:57 am
|
#
Not sure of Yeadon's claim disputing Bossche's suggestion of new strains arising from vaccination. We are
early on with the program but also seeing need to check that problem in Israel:
https://www.channelnewsasia.com/news/world/south-african-covid-19-variant-break-through-pfizer-vaccine-14598714
Michael Yeadon, wasn't just any scientist. The 60-year-old is a former vice president of Pfizer, where he spent 16 years as an
allergy and respiratory researcher. He later co-founded a biotech firm that the Swiss drugmaker Novartis purchased for at least $325
million.
In recent months, Yeadon (pronounced Yee-don) has emerged as an unlikely hero of the so-called anti-vaxxers, whose adherents
question the safety of many vaccines, including for the coronavirus. The anti-vaxxer movement has amplified Yeadon's skeptical views
about COVID-19 vaccines and tests, government-mandated lockdowns and the arc of the pandemic. Yeadon has said he personally doesn't
oppose the use of all vaccines. But many health experts and government officials worry that opinions like his fuel vaccine hesitancy
� a reluctance or refusal to be vaccinated � that could prolong the pandemic. COVID-19 has already killed more than 2.6 million
people worldwide.
"These claims are false, dangerous and deeply irresponsible," said a spokesman for Britain's Department of Health & Social Care,
when asked about Yeadon's views. "COVID-19 vaccines are the best way to protect people from coronavirus and will save thousands of
lives."
Recent reports of blood clots and abnormal bleeding in a small number of recipients of AstraZeneca's COVID-19 vaccine have cast
doubt on that shot's safety, leading several European countries to suspend its use.
The developments are likely to fuel vaccine
hesitancy further, although there is no evidence of a causative link between the AstraZeneca product and the affected patients'
conditions.
... ... ...
Robert F. Kennedy Jr., pictured in 2016, was recently banned on Instagram because of his COVID-19 vaccine posts. REUTERS/Stephanie
Keith
The visage and views of Yeadon, widely identified as an "Ex-VP of Pfizer,'' can be seen on social media in languages including
German, Portuguese, Danish and Czech. A Facebook post carries a video from November in which Yeadon claimed that the pandemic
"fundamentally is over." The post has been viewed more than a million times.
In October, Yeadon wrote a column for the United Kingdom's Daily Mail newspaper that also appeared on MailOnline, one of the world's
most-visited news websites. It declared that deaths caused by COVID-19, which then totaled about 45,000 in Britain, will soon
"fizzle out" and Britons "should immediately be allowed to resume normal life." Since then, the disease has killed about another
80,000 people in the UK.
Yeadon isn't the only respected scientist to have challenged the scientific consensus on COVID-19 and expressed controversial views.
Michael Levitt, a winner of the Nobel Prize for chemistry, told the Stanford Daily last summer that he expected the pandemic
would end in the United States in 2020 and kill no more than 175,000 Americans � a third of the [overinflated, so probably right
estimate --NNB] current total
� and "when we come to look back, we're going to say that wasn't such a terrible disease."
And
Luc Montagnier, another Nobel Prize winner, said last year that he believed the coronavirus was created in a Chinese lab
.
Many experts doubt that, but so far there is no way to prove or disprove it.
Levitt told Reuters that his projections about the pandemic in the United States were wrong, but he still believes COVID-19
eventually won't be seen as "a terrible disease" and that lockdowns "caused a great deal of collateral damage and may not have been
needed." Montagnier didn't respond to a request for comment.
...
... ...
Clare Craig, a British pathologist, compared Yeadon's treatment on Twitter � where some users derided his views as nonsense and
dangerous � to medieval societies burning heretics at the stake.
"There is no other way to see it than the burning of the witches," said Craig, who has criticized lockdowns and COVID-19 tests.
"Science is always a series of questions and the testing of those questions and when we are not allowed to ask those questions, then
science is lost."
18 May 2021
You need understand that thing can go wrong. Sometimes badly wrong
JERUSALEM: The coronavirus variant discovered in South Africa can "break through"
Pfizer-BioNTech's COVID-19 vaccine to some extent, a real-world data study in Israel found,
though its prevalence in the country is low and the research has not been peer reviewed.
The study, released on Saturday (Apr 10), compared almost 400 people who had tested positive
for COVID-19, 14 days or more after they received one or two doses of the vaccine, against the
same number of unvaccinated patients with the disease. It matched age and gender, among other
characteristics.
The South African variant, B1351, was found to make up about 1 per cent of all the COVID-19
cases across all the people studied, according to the study by Tel Aviv University and Israel's
largest healthcare provider, Clalit.
But among patients who had received two doses of the vaccine, the variant's prevalence rate
was eight times higher than those unvaccinated - 5.4 per cent versus 0.7 per
cent.
COMMENTARY:
Those new coronavirus variants sure are worrisome This suggests the vaccine is less effective against the South African variant, compared with
the original coronavirus and a variant first identified in Britain that has come to comprise
nearly all COVID-19 cases in Israel, the researchers said.
"We found a disproportionately higher rate of the South African variant among people
vaccinated with a second dose, compared to the unvaccinated group. This means that the South
African variant is able, to some extent, to break through the vaccine's protection," said Tel
Aviv University's Adi Stern.
The researchers cautioned, though, that the study only had a small sample size of people
infected with the South African variant because of its rarity in Israel.
They also said the research was not intended to deduce overall vaccine effectiveness against
any variant, since it only looked at people who had already tested positive for COVID-19, not
at overall infection rates.
Pfizer and BioNTech could not be immediately reached for comment outside business hours.
The companies said on Apr 1 that their vaccine was around 91 per cent effective at
preventing COVID-19, citing updated trial data that included participants inoculated for up to
six months.
In respect to the South African variant, they said that among a group of 800 study
volunteers in South Africa, where B1351 is widespread, there were nine cases of COVID-19, all
of which occurred among participants who got the placebo. Of those nine cases, six were among
individuals infected with the South African variant.
READ: COVID-19 lockdowns around the
world as vaccine efforts stumble
Some previous studies have indicated that the Pfizer-BioNTech shot was less potent against
the B1351 variant than against other variants of the coronavirus, but still offered a robust
defence.
While the results of the study may cause concern, the low prevalence of the South African
strain was encouraging, according to Stern.
"Even if the South African variant does break through the vaccine's protection, it has not
spread widely through the population," said Stern, adding that the British variant may be
"blocking" the spread of the South African strain.
Almost 53 per cent of Israel's 9.3 million population has received both Pfizer doses. Israel
has largely reopened its economy in recent weeks while the pandemic appears to be receding,
with infection rates, severe illness and hospitalisations dropping sharply. About a third of
Israelis are below the age of 16, which means they are still not eligible for the shot.
Highly recommended !Money quote: "I think the PCR test at present is throwing up so many false positives that in
fact we're misdiagnosing the cause of the deaths that are being reported. The number of deaths at
the moment is normal for the time of year. So if I'm right and the pandemic is fundamentally
over, what's going on? And I think quite simply it's not over because SAGE says it's not!"
Notable quotes:
"... You also don't set about planning to vaccinate millions of fit and healthy people with a vaccine that hasn't been extensively tested on human subjects." ..."
Michael Yeadon has voiced [his concerns about government policies regarding COVID-19] and it
has left everyone shocked. As Pfizer pharmaceuticals breaks news for
bringing corona virus vaccine , a former vice president and chief scientists of the company
Michael Yeadon said that there is no need for any vaccine to end the ongoing pandemic.
According to a report published in the Lockdown Sceptics, Yeadon wrote: "There is absolutely
no need for vaccines to extinguish the pandemic. You do not vaccinate people who aren't at risk
from the disease. You also don't set about
planning to vaccinate millions of fit and healthy people with a vaccine that hasn't been
extensively tested on human subjects." Yeadon made the comment on the vaccine development
while criticizing the role played by the Scientific Advisory
Group for Emergencies (SAGE), a government agency of the UK.
SAGE is tasked with a role to determine public lockdown policies; in the UK, as a response
to the COVID-19 virus. He added, "SAGE says everyone was susceptible and only 7 per cent have
been infected. They have ignored all precedent in the field of immunology memory against
respiratory viruses. They have either not seen or disregarded excellent quality work from
numerous world-leading clinical immunologists; which show that around 30 per cent of the
population had prior immunity."
Michael Yeadon wrote "They should also have excluded from 'susceptible' a large subset; of
the youngest children, who appear not to become infected biology; means their cells express
less of the spike protein receptor, called ACE2. I have not assumed all young children don't
participate in transmission, but believe a two-thirds value is very conservative. It's not
material anyway. So SAGE is demonstrably wrong in one really crucial variable, they assumed no
prior immunity, whereas the evidence clearly points; to a value of around 30 per cent (and
nearly 40 per cent if you include some young children, who technically are 'resistant' rather
than 'immune')."
He concluded that the pandemic is effectively over and; can easily be handled by a properly
functioning NHS (National Health Service).
1.6K Mordechai Sones
America's Frontline Doctors ( AFLDS ) today filed a motion in the U.S.
District Court for the Northern District of Alabama requesting a temporary restraining
order against the emergency use authorization (EUA) permitting using the COVID-19 vaccines
in children under the age of 16, and that no further expansion of the EUAs to children under
the age of 16 be granted prior to the resolution of these issues at trial.
The case will challenge the EUAs for the injections on several counts, based on the law and
scientific evidence that the EUAs should never have been granted, the EUAs should be revoked
immediately, the injections are dangerous biological agents that have the potential to cause
substantially greater harm than the COVID-19 disease itself, and that numerous laws have been
broken in the process of granting these EUAs and foisting these injections on the American
people.
AFLDS Founder Dr. Simone Gold spoke about the
reasons for filing the motion: "We doctors are pro-vaccine, but this is not a vaccine," she
said. "This is an experimental biological agent whose harms are well-documented (although
suppressed and censored) and growing rapidly, and we will not support using America's children
as guinea pigs."
She continued: "We insist that the EUA not be relinquished prematurely; certainly not before
trials are complete - October 31, 2022 for Moderna and April 27, 2023 for Pfizer. We are
shocked at the mere discussion of this, and will not be silent while Americans are used as
guinea pigs for a virus with survivability of 99.8% globally and 99.97% under age 70.
"Under age 20 it is 99.997% - 'statistical zero'.
"There are 104 children age 0-17 who died from COVID-19 and 287 from COVID + Influenza - out
of ~72 million. This equals zero risk. And we doctors won't stand for children being offered
something they do not need and of whom some unknown percentage will suffer."
AFLDS Pediatric Director Dr. Angie
Farella explained: "My greatest concerns with the vaccination of children under the age of
18 is the fact that there is no prior study of these individuals before December of 2020."
She went on to say: "Children were not included in the trials, and the adult trials do not
have any long-term safety data currently available."
AFLDS Legal Director Ali Shultz commented on AFLDS' filing:
"Not many people could have taken this on. Dr. Simone Gold is a doctor, and a lawyer, and a
fierce warrior who will stop at nothing to protect humanity.
"She has a certain finesse in developing the right team to see this medical/legal mission
through."
To read the motion and all supporting documents, click here .
New notion: criminal pharma... The big pharma companies know that the chances of you dying of
COVID if you are NOT obese, aged or have 3-4 co-morbidites are close to ZERO. Heads they win,
tails you lose.
glenlloyd 16 hours ago (Edited)
It's a policy designed to reinforce the CDC "get vaccinated" propaganda machine.
I stopped listening to these bozos a long time ago. When the commercials come on the radio
I turn it off, I'm tired of being nagged about something as ridiculous as this.
CDC wants medicine as the savior when in fact the human body is the best source of remedy
for anything like this.
Sick of this BS
paranoid.dragon 7 hours ago (Edited) remove link
if Covid-19 is actually so deadly to be classified as a "pandemic", what happened to a
patients' "right to try" medicines that are not "approved" by the CDC and FDA?
Why cannot a Primary Care Physician call in a prescription to a local pharmacy for a
patient with covid-like symptoms, like Ivermectin, Hydroxychloroquine, dexamethasone, blood
thinners, etc.
And a covid test not even needed.
Who has given the health agencies at the state and federal level the god-like powers to
threaten family doctors with jail, loss of license to practice medicine, and lawsuits for
prescribing a medicine that should be a decision between doctor and patient????
That should be the biggest red flag, at least in America...
Especially against the covid vaccine...
Doctors are not allowed to prescribe medications to treat covid. And the government
agencies and officials have essentially become big pharma reps peddling an experimental
genetic covid vaccine.
the US military has been turned into package boys for big pharma. Your family doctor's
research on covid goes no further than reading emails sent by the government and their big
pharma reps.
... ... ...
PharmaCoin.
Pfizer is already demanding military bases as collateral for their covid
vaccines...
lay_arrow
crazzziecanuck 11 hours ago (Edited)
They answer to a bunch of clueless elected officials, who respond to the fearmongering and
shrill hysterics created by the MSM. All of which starts with Pfizer.
Pfizer doesn't just bribe elected officials and, functionally making the "regulated"
Pfizer able to regulate it's regulators. Pfizer also bribes the MSM with advertising
dollars.
Like Deep Throat instructed: follow the money.
sgpbulion 7 hours ago
Cycle testing - running the same test over and over unitl you get the results you want and
then stopping.
Believe it or not this is the same foolishness that goes into radiometric dating of how
old rocks are. It's why you can take a warm chunk of lava and send it in to the dating lab
and get a result of over 25 million years old.
Trust the science folks - resistance is futile
By the way if the test shows negative after 30 cycles - it means that there is not enough
virus in your system for it be dangerous and that your body can deal with it on its own. By
the time you get to 35 cycles it is amplified so much that it will show any virus fragment in
your system - and at such miniscule amounts that the body does not even know its there - and
its not a problem. When you get 40 cycles and above the test will have to be positive because
there is always some virus fragments in your system. The single fact that they can run +40
cycles and get a negative result shows that this test is actually garbage from the start.
Dr Phuckit 16 hours ago remove link
My own interpretation of Government Data, tells me anything above 25 cycles is
fraudulent.
It looks like the CDC has come to their senses, but still bordering towards fraudulent
data.
At 30 cycles it's 50/50 chance of being right. But right for what exactly because it still
can't detect a virus, can't determine if it was a new infection or an old infection not even
active. Above 40+ even a rock will test positive.
What all this has accomplished though, is Corporations now have DNA samples of most of
worlds population , and these F'wits that weren't sick couldn't opt-in fast enough. Imagine
if these Corporations had said, we want your DNA for our Database, how many would have
volunteered ?
These Corporations now have the capability to target specific people with DNA for any evil
purpose they might have in the future. Perhaps this was the plan all along, DNA
collection.
Dr Phuckit 15 hours ago
The CDC can't stop the flood of lawsuits about to unfold, they are now trying to minimize
the damage to it's control and bank account. And the CDC is nothing but an interface between
All Pharmaceutical Companies and Government. They have no real power to mandate anything, all
they can do is recommend because it's about as Federal as the Federal Reserve.
shakypudding 16 hours ago remove link
The rt-CPR tests were sanctioned per emergency use authorizations (EUA) which means no
prior certification of efficacy. This rendered the lab results useless except for
propaganda.
The vaccines were also issued per emergency use authorization (EUA) which means no prior
certification of efficacy. How and why can this happen? Emergency use authorizations are
permitted when alternative treatments are not officially recognized, such as HCQ, Ivermectin
and vitamin D.
Had the government sanctioned alternative treatments such as HCQ, Ivermectin and vitamin D
millions of drug company profits and government kickbacks would have been forfeited.
Additionally, the opportunity for extending social programs of conditioning and control
would have been forgone by your overlords.
InfiniteIntellRules 10 hours ago remove link
WHO sued over fake PCR test...
https://rightsfreedoms.wordpress.com/2021/05/12/covid-fraud-lawyers-medical-experts-start-legal-proceedings-against-w-h-o-and-world-leaders-for-crimes-against-humanity/
Authored by Kit Knightly via Off-Guardian.org,
New policies will artificially deflate "breakthrough infections" in the vaccinated, while
the old rules continue to inflate case numbers in the unvaccinated.
The US Center for Disease Control (CDC) is altering its practices of data logging and
testing for "Covid19" in order to make it seem the experimental gene-therapy "vaccines" are
effective at preventing the alleged disease.
They made no secret of this, announcing the policy changes on their website in late
April/early May, (though naturally without admitting the fairly obvious motivation behind the
change).
The trick is in their reporting of what they call "breakthrough infections" – that is
people who are fully "vaccinated" against Sars-Cov-2 infection, but get infected anyway.
Essentially, Covid19 has long been shown – to those willing to pay attention –
to be an entirely created pandemic narrative built on two key factors:
False-positive tests. The unreliable
PCR test can be manipulated into reporting a
high number of false-positives by altering the cycle threshold (CT value)
Inflated Case-count. The incredibly broad definition
of "Covid case", used all over the world, lists anyone who receives a positive test as a
"Covid19 case", even if they never experienced any symptoms .
Without these two policies, there would never have been an appreciable pandemic at all , and
now the CDC has enacted two policy changes which means they no longer apply to vaccinated
people.
Firstly, they are lowering their CT value when testing samples from suspected "breakthrough
infections".
From the CDC's instructions for state health authorities on handling "possible breakthrough
infections" (uploaded to their website in late April):
For cases with a known RT-PCR cycle threshold (Ct) value, submit only specimens with Ct
value ≤28 to CDC for sequencing. (Sequencing is not feasible with higher Ct values.)
Throughout the pandemic, CT values in excess of 35 have been the norm, with labs around the
world going into the 40s.
Essentially labs were running as many cycles as necessary to achieve a positive result,
despite experts warning that this was pointless ( even Fauci himself said anything over 35 cycles is meaningless ).
But NOW, and only for fully vaccinated people, the CDC will only accept samples achieved
from 28 cycles or fewer. That can only be a deliberate decision in order to decrease the number
of "breakthrough infections" being officially recorded.
Secondly, asymptomatic or mild infections will no longer be recorded as "covid cases".
That's right. Even if a sample collected at the low CT value of 28 can be sequenced into the
virus alleged to cause Covid19, the CDC will no longer be keeping records of breakthrough
infections that don't result in hospitalisation or death .
From their website
:
As of May 1, 2021, CDC transitioned from monitoring all reported vaccine breakthrough
cases to focus on identifying and investigating only hospitalized or fatal cases due to any
cause. This shift will help maximize the quality of the data collected on cases of greatest
clinical and public health importance. Previous case counts, which were last updated on April
26, 2021, are available for reference only and will not be updated moving forward.
Just like that, being asymptomatic – or having only minor symptoms – will no
longer count as a "Covid case" but only if you've been vaccinated.
The CDC has put new policies in place which effectively created a tiered system of
diagnosis. Meaning, from now on, unvaccinated people will find it much easier to be diagnosed
with Covid19 than vaccinated people.
Consider
Person A has not been vaccinated. They test positive for Covid using a PCR test at 40
cycles and, despite having no symptoms, they are officially a "covid case".
Person B has been vaccinated. They test positive at 28 cycles, and spend six weeks
bedridden with a high fever. Because they never went into a hospital and didn't die they are
NOT a Covid case.
Person C , who was also vaccinated, did die. After weeks in hospital with a high fever and
respiratory problems. Only their positive PCR test was 29 cycles, so they're not officially a
Covid case either.
The CDC is demonstrating the beauty of having a "disease" that can appear or disappear
depending on how you measure it.
To be clear: If these new policies had been the global approach to "Covid" since December
2019, there would never have been a pandemic at all.
If you apply them only to the vaccinated, but keep the old rules for the unvaccinated, the
only possible result can be that the official records show "Covid" is much more prevalent among
the latter than the former.
This is a policy designed to continuously inflate one number, and systematically minimise
the other.
What is that if not an obvious and deliberate act of deception? play_arrow
ArkansasAngie 7 hours ago remove link
Reminds me of money supply numbers. And inflation numbers. And GDP numbers. And
unemployment numbers. Oh ... and votes
JakeIsNotFake 14 hours ago remove link
What is that if not an obvious and deliberate act of deception?
Well, before 3/20, this would have been a FELONY. Each time a lab provided a patient with
KNOWINGLY FALSE test results, the lab and the doctor would have been subject to a 16 month
term in the state penitentiary. For each instance.
Can you imagine getting a positive, terminal prognosis, committing a well deserved murder,
and then not dying?
Oopsie! My bad.
Highly recommended !Michael Yeadon, wasn't just any scientist. The 60-year-old is a former vice president of Pfizer, where he spent 16 years as an
allergy and respiratory researcher. He later co-founded a biotech firm that the Swiss drugmaker Novartis purchased for at least $325
million.
This is amazing interview for a scientist who really knows his staff... His warning is
essentially a very powerful warning against Lysenkoism in science.
I disagree with him on some minor points like wearing masks in closed spaces as well as the spectrum of applicability of
vaccines (I think that healthcare workers, teachers and other people who systematically interact with a lot of (possibly infected)
people might benefit from vaccination, which should in any case be strocly voluntary. But I agree that vaccinating people who
already have had COVID-19 and children s very questionable and probably indefensible practice -- flavor of Lysenkoism which is
called Fauchism. Also stress of vaccines and downgrading therapy is also Faucism, or worse.
I also disagree with his statement that vaccine should be effective against all strains. Now we know that htis not the case. For
exampe South afrecan mutation successfully infects people vaccinated wit the the first generation vaccines.
He is against medicines which are used with violation of safety protocols. He is anti unsafe
medicines, no matter what they are.
We never have such an absurd attribution of death to COVID, when that fact the diseased is
false positive serve as the key reason of death
Lockdowns were political hysteria. Witch hunt against witches which never arrived. They were
unscientific and fradulent. Lockdown were never used before because they are ineffective. Instead
in the past guaranteed the sick. Mass testing of people without symptoms is Lysenkoism and defies
common sense.
Non-symptomatic people will not infect you. That's faucism and new flavor of Lysenkoism.
Asymptomatic transmission is bunk. It can happen but this never exceed fraction of one
percent.
It is all about increasing of the level of fear and increasing political control as in famous
quote. The only open question to what end this control will used for.
PCR technology is similar to technology used in forensic investigation using genetic
material. They just ignore false positives. Nobody in the world releases the percentage of false
positive of PcR test and dependence of the number of false positive on the number of
amplification.
I never expected to be writing something like this. I am an ordinary person, recently semi-retired from a career in the
pharmaceutical industry and biotech, where I spent over 30 years trying to solve problems of disease understanding and seek new
treatments for allergic and inflammatory disorders of lung and skin. I've always been interested in problem solving, so when
anything biological comes along, my attention is drawn to it. Come 2020, came SARS-CoV-2. I've written
about the pandemic as objectively as I could. The scientific method never leaves a person who trained and worked as a
professional scientist. Please do read that piece. My co-authors & I will submit it to the normal rigours of peer review, but that
process is slow and many pieces of new science this year have come to attention through pre-print servers and other less
conventional outlets.
While paying close attention to data, we all initially focused on the sad matter of deaths. I found it remarkable that, in
discussing the COVID-19 related deaths, most people I spoke to had no idea of large numbers. Asked approximately how many people a
year die in the UK in the ordinary course of events, each a personal tragedy, They usually didn't know. I had to inform them it is
around 620,000, sometimes less if we had a mild winter, sometimes quite a bit higher if we had a severe 'flu season. I mention this
number because we know that around 42,000 people have died with or of COVID-19. While it's a huge number of people, its 'only' 0.06%
of the UK population. Its not a coincidence that this is almost the same proportion who have died with or of COVID-19 in each of the
heavily infected European countries � for example, Sweden. The annual all-causes mortality of 620,000 amounts to 1,700 per day,
lower in summer and higher in winter. That has always been the lot of humans in the temperate zones. So for context, 42,000 is about
~24 days worth of normal mortality. Please know I am not minimising it, just trying to get some perspective on it. Deaths of this
magnitude are not uncommon, and can occur in the more severe flu seasons. Flu vaccines help a little, but on only three occasions in
the last decade did vaccination reach 50% effectiveness. They're good, but they've never been magic bullets for respiratory viruses.
Instead, we have learned to live with such viruses, ranging from numerous common colds all the way to pneumonias which can kill.
Medicines and human caring do their best.
So, to this article. Its about the testing we do with something called PCR, an amplification technique, better known to biologists
as a research tool used in our labs, when trying to unpick mechanisms of disease. I was frankly astonished to realise they're
sometimes used in population screening for diseases � astonished because it is a very exacting technique, prone to invisible errors
and it's quite a tall order to get reliable information out of it, especially because of the prodigious amounts of amplification
involved in attempting to pick up a strand of viral genetic code. The test cannot distinguish between a living virus and a short
strand of RNA from a virus which broke into pieces weeks or months ago.
I believe I have identified a serious, really a fatal flaw in the PCR test used in what is called by the UK Government the Pillar 2
screening � that is, testing many people out in their communities. I'm going to go through this with care and in detail because I'm
a scientist and dislike where this investigation takes me. I'm not particularly political and my preference is for competent, honest
administration over the actual policies chosen. We're a reasonable lot in UK and not much given to extremes. What I'm particularly
reluctant about is that, by following the evidence, I have no choice but to show that the Health Secretary, Matt Hancock, misled the
House of Commons and also made misleading statements in a radio interview. Those are serious accusations. I know that. I'm not a
ruthless person. But I'm writing this anyway, because what I have uncovered is of monumental importance to the health and wellbeing
of all the people living in the nation I have always called home.
Back to the story, and then to the evidence. When the first (and I think, only) wave of COVID-19 hit the UK, I was with almost
everyone else in being very afraid. I'm 60 and in reasonable health, but on learning that I had about a 1% additional risk of
perishing if I caught the virus, I discovered I was far from ready to go. So, I wasn't surprised or angry when the first lockdown
arrived. It must have been a very difficult thing to decide. However, before the first three-week period was over, I'd begun to
develop an understanding of what was happening. The rate of infection, which has been calculated to have infected well over 100,000
new people every day around the peak, began to fall, and was declining before lockdown. Infection continued to spread out, at an
ever-reducing rate and we saw this in the turning point of daily deaths, at a grim press conference each afternoon. We now know that
lockdown made no difference at all to the spread of the virus. We can tell this because the interval between catching the virus and,
in those who don't make it, their death is longer than the interval between lockdown and peak daily deaths. There isn't any
controversy about this fact, easily demonstrated, but I'm aware some people like to pretend it was lockdown that turned the
pandemic, perhaps to justify the extraordinary price we have all paid to do it. That price wasn't just economic. It involved
avoidable deaths from diseases other than COVID-19, as medical services were restricted, in order to focus on the virus. Some say
that lockdown, directly and indirectly, killed as many as the virus. I don't know. Its not something I've sought to learn. But I
mention because interventions in all our lives should not be made lightly. Its not only inconvenience, but real suffering, loss of
livelihoods, friendships, anchors of huge importance to us all, that are severed by such acts. We need to be certain that the prize
is worth the price. While it is uncertain it was, even for the first lockdown, I too supported it, because we did not know what we
faced, and frankly, almost everyone else did it, except Sweden. I am now resolutely against further interventions in what I have
become convinced is a fruitless attempt to 'control the virus'. We are, in my opinion � shared by others, some of whom are well
placed to assess the situation � closer to the end of the pandemic in terms of deaths, than we are to its middle. I believe we
should provide the best protection we can for any vulnerable people, and otherwise cautiously get on with our lives. I think we are
all going to get a little more Swedish over time.
In recent weeks, though, it cannot have escaped anyone's attention that there has been a drum beat which feels for all the world
like a prelude to yet more fruitless and damaging restrictions. Think back to mid-summer. We were newly out of lockdown and despite
concerns for crowded beaches, large demonstrations, opening of shops and pubs, the main item on the news in relation to COVID-19 was
the reassuring and relentless fall in daily deaths. I noticed that, as compared to the slopes of the declining death tolls in many
nearby countries, that our slope was too flat. I even mentioned to scientist friends that inferred the presence of some fixed signal
that was being mixed up with genuine COVID-19 deaths. Imagine how gratifying it was when the definition of a COVID-19 death was
changed to line up with that in other countries and in a heartbeat our declining death toll line became matched with that elsewhere.
I was sure it would: what we have experienced and witnessed is a terrible kind of equilibrium. A virus that kills few, then leaves
survivors who are almost certainly immune � a virus to which perhaps 30-50% were already immune because it has relatives and some of
us have already encountered them � accounts for the whole terrible but also fascinating biological process. There was a very interesting
piece in the BMJ in
recent days that offers potential support for this contention.
Now we have learned some of the unusual characteristics of the new virus, better treatments (anti-inflammatory steroids,
anti-coagulants and in particular, oxygen masks and not ventilators in the main) the 'case fatality rate' even for the most hard-hit
individuals is far lower now than it was six months ago.interviewed
recently by Julia Hartley-Brewer on her talkRADIO show and on that occasion I called on the Government to disclose to us the
evidence upon which they were relying to predict this second wave. Surely they have some evidence? I don't think they do. I searched
and am very qualified to do so, drawing on academic friends, and we were all surprised to find that there is nothing at all. The
last two novel coronaviruses, Sar (2003) and MERS (2012), were of one wave each. Even the WW1 flu 'waves' were almost certainly a
series of single waves involving more than one virus. I believe any second wave talk is pure speculation. Or perhaps it is in a
model somewhere, disconnected from the world of evidence to me? It would be reasonable to expect some limited 'resurgence' of a
virus given we don't mix like cordial in a glass of water, but in a more lumpy, human fashion. You're most in contact with family,
friends and workmates and they are the people with whom you generally exchange colds.
A long period of imposed restrictions, in addition to those of our ordinary lives did prevent the final few percent of virus mixing
with the population. With the movements of holidays, new jobs, visiting distant relatives, starting new terms at universities and
schools, that final mixing is under way. It should not be a terrifying process. It happens with every new virus, flu included. It's
just that we've never before in our history chased it around the countryside with a technique more suited to the biology lab than to
a supermarket car park.
A very long prelude, but necessary. Part of the 'project fear' that is rather too obvious, involving second waves, has been the
daily count of 'cases'. Its important to understand that, according to the infectious disease specialists I've spoken to, the word
'case' has to mean more than merely the presence of some foreign organism. It must present signs (things medics notice) and symptoms
(things you notice). And in most so-called cases, those testing positive had no signs or symptoms of illness at all. There was much
talk of asymptomatic spreading, and as a biologist this surprised me. In almost every case, a person is symptomatic because they
have a high viral load and either it is attacking their body or their immune system is fighting it, generally a mix. I don't doubt
there have been some cases of asymptomatic transmission, but I'm confident it is not important.
That all said, Government decided to call a person a 'case' if their swab sample was positive for viral RNA, which is what is
measured in PCR. A person's sample can be positive if they have the virus, and so it should. They can also be positive if they've
had the virus some weeks or months ago and recovered. It's faintly possible that high loads of related, but different coronaviruses,
which can cause some of the common colds we get, might also react in the PCR test, though it's unclear to me if it does.
But there's a final setting in which a person can be positive and that's a random process. This may have multiple causes, such as
the amplification technique not being perfect and so amplifying the 'bait' sequences placed in with the sample, with the aim of
marrying up with related SARS-CoV-2 viral RNA. There will be many other contributions to such positives. These are what are called
false positives.
Think of any diagnostic test a doctor might use on you. The ideal diagnostic test correctly confirms all who have the disease and
never wrongly indicates that healthy people have the disease. There is no such test. All tests have some degree of weakness in
generating false positives. The important thing is to know how often this happens, and this is called the false positive rate. If 1
in 100 disease-free samples are wrongly coming up positive, the disease is not present, we call that a 1% false positive rate. The
actual or operational false positive rate differs, sometimes substantially, under different settings, technical operators, detection
methods and equipment. I'm focusing solely on the false positive rate in Pillar 2, because most people do not have the virus
(recently around 1 in 1000 people and earlier in summer it was around 1 in 2000 people). It is when the amount of disease, its
so-called prevalence, is low that any amount of a false positive rate can be a major problem. This problem can be so severe that
unless changes are made, the test is hopelessly unsuitable to the job asked of it. In this case, the test in Pillar 2 was and
remains charged with the job of identifying people with the virus, yet as I will show, it is unable to do so.
Because of the high false positive rate and the low prevalence, almost every positive test, a so-called case, identified by Pillar 2
since May of this year has been a FALSE POSITIVE. Not just a few percent. Not a quarter or even a half of the positives are FALSE,
but around 90% of them. Put simply, the number of people Mr Hancock sombrely tells us about is an overestimate by a factor of about
ten-fold. Earlier in the summer, it was an overestimate by about 20-fold.
Let me take you through this, though if you're able to read Prof Carl Heneghan's clearly
written piece first, I'm more confident that I'll be successful in explaining this dramatic conclusion to you. (Here is a link to
the record of numbers of tests, combining Pillar 1 (hospital) and Pillar 2 (community).)
Imagine 10,000 people getting tested using those swabs you see on TV. We have a good estimate of the general prevalence of the virus
from the ONS, who are wholly independent (from Pillar 2 testing) and are testing only a few people a day, around one per cent of the
numbers recently tested in Pillar 2. It is reasonable to assume that most of the time, those being tested do not have symptoms.
People were asked to only seek a test if they have symptoms. However, we know from TV news and stories on social media from sampling
staff, from stern guidance from the Health Minister and the surprising fact that in numerous locations around the country, the local
council is leafleting people's houses, street by street to come and get tested.
The bottom line is that it is reasonable to expect the prevalence of the virus to be close to the number found by ONS, because they
sample randomly, and would pick up symptomatic and asymptomatic people in proportion to their presence in the community. As of the
most recent ONS survey, to a first approximation, the virus was found in 1 in every 1000 people. This can also be written as 0.1%.
So when all these 10,000 people are tested in Pillar 2, you'd expect 10 true positives to be found (false negatives can be an issue
when the virus is very common, but in this community setting, it is statistically unimportant and so I have chosen to ignore it,
better to focus only on false positives).
So, what is the false positive rate of testing in Pillar 2? For months, this has been a concern. It appears that it isn't known,
even though as I've mentioned, you absolutely need to know it in order to work out whether the diagnostic test has any value! What
do we know about the false positive rate? Well, we do know that the Government's own scientists were very concerned about it, and a report on
this problem was sent to SAGE dated June 3rd 2020. I quote: "Unless we understand the operational false positive rate of the UK's
RT-PCR testing system, we risk over-estimating the COVID-19 incidence, the demand on track and trace and the extent of asymptomatic
infection". In that same report, the authors helpfully listed the lowest to highest false positive rate of dozens of tests using the
same technology. The lowest value for false positive rate was 0.8%.
Allow me to explain the impact of a false positive rate of 0.8% on Pillar 2. We return to our 10,000 people who've volunteered to
get tested, and the expected ten with virus (0.1% prevalence or 1:1000) have been identified by the PCR test. But now we've to
calculate how many false positives are to accompanying them. The shocking answer is 80. 80 is 0.8% of 10,000. That's how many false
positives you'd get every time you were to use a Pillar 2 test on a group of that size.
The effect of this is, in this example, where 10,000 people have been tested in Pillar 2, could be summarised in a headline like
this: "90 new cases were identified today" (10 real positive cases and 80 false positives). But we know this is wildly incorrect.
Unknown to the poor technician, there were in this example, only 10 real cases. 80 did not even have a piece of viral RNA in their
sample. They are really false positives.
I'm going to explain how bad this is another way, back to diagnostics. If you'd submitted to a test and it was positive, you'd
expect the doctor to tell you that you had a disease, whatever it was testing for. Usually, though, they'll answer a slightly
different question: "If the patient is positive in this test, what is the probability they have the disease?" Typically, for a good
diagnostic test, the doctor will be able to say something like 95% and you and they can live with that. You might take a different,
confirmatory test, if the result was very serious, like cancer. But in our Pillar 2 example, what is the probability a person
testing positive in Pillar 2 actually has COVID-19? The awful answer is 11% (10 divided by 80 + 10). The test exaggerates the number
of covid-19 cases by almost ten-fold (90 divided by 10). Scared yet? That daily picture they show you, with the 'cases' climbing up
on the right-hand side? Its horribly exaggerated. Its not a mistake, as I shall show.
Earlier in the summer, the ONS showed the virus prevalence was a little lower, 1 in 2000 or 0.05%. That doesn't sound much of a
difference, but it is. Now the Pillar 2 test will find half as many real cases from our notional 10,000 volunteers, so 5 real cases.
But the flaw in the test means it will still find 80 false positives (0.8% of 10,000). So its even worse. The headline would be "85
new cases identified today". But now the probability a person testing positive has the virus is an absurdly low 6% (5 divided by 80
+ 5). Earlier in the summer, this same test exaggerated the number of COVID-19 cases by 17-fold (85 divided by 5). Its so easy to
generate an apparently large epidemic this way. Just ignore the problem of false positives. Pretend its zero. But it is never zero.
This test is fatally flawed and MUST immediately be withdrawn and never used again in this setting unless shown to be fixed. The
examples I gave are very close to what is actually happening every day as you read this.
I'm bound to ask, did Mr Hancock know of this fatal flaw? Did he know of the effect it would inevitably have, and is still having,
not only on the reported case load, but the nation's state of anxiety. I'd love to believe it is all an innocent mistake. If it was,
though, he'd have to resign over sheer incompetence. But is it? We know that internal scientists wrote to SAGE, in terms, and,
surely, this short but shocking warning document would have been drawn to the Health Secretary's attention? If that was the only bit
of evidence, you might be inclined to give him the benefit of the doubt. But the evidence grows more damning.
Recently, I published with my co-authors a short Position Paper. I don't think by then, a month ago or so, the penny had quite
dropped with me. And I'm an experienced biomedical research scientist, used to dealing with complex datasets and probabilities.
On September 11th 2020, I was a guest on Julia Hartley-Brewer's talkRADIO
show . Among other things, I called upon Mr Hancock to release the evidence underscoring his confidence in and planning for 'the
second wave'. This evidence has not yet been shown to the public by anyone. I also demanded he disclose the operational false
positive rate in Pillar 2 testing.
On September 16th, I was back on Julia's show and this time focused on the false positive rate issue (1m 45s � 2min 30s). I had read
Carl Heneghan's analysis showing that even if the false positive rate was as low as 0.1%, 8 times lower than any similar test, it
still yields a majority of false positives. So, my critique doesn't fall if the actual false positive rate is lower than my assumed
0.8%.
On September 18th, Mr Hancock again appeared, as often he does, on Julia Hartley-Brewer's show. Julia asked
him directly (1min 50s � on) what the false positive rate in Pillar 2 is. Mr Hancock said "It's under 1%". Julia again asked him
exactly what it was, and did he even know it? He didn't answer that, but then said "it means that, for all the positive cases, the
likelihood of one being a false positive is very small".
That is a seriously misleading statement as it is incorrect. The likelihood of an apparently positive case being a false positive is
between 89-94%, or near-certainty. Of note, even when ONS was recording its lowest-ever prevalence, the positive rate in Pillar 2
testing never fell below 0.8%.
It gets worse for the Health Secretary. On September the 17th, I believe, Mr Hancock took a question from
Sir Desmond Swayne about false positives. It is clear that Sir Desmond is asking about Pillar 2.
Mr Hancock replied: "I like my right honourable friend very much and I wish it were true. The reason we have surveillance testing,
done by ONS, is to ensure that we're constantly looking at a nationally representative sample at what the case rate is. The latest
ONS survey, published on Friday, does show a rise consummate (sic) with the increased number of tests that have come back positive."
He did not answer Sir Desmond's question, but instead answered a question of his choosing. Did the Health Secretary knowingly
mislead the House? By referring only to ONS and not even mentioning the false positive rate of the test in Pillar 2 he was, as it
were, stealing the garb of ONS's more careful work which has a lower false positive rate, in order to smuggle through the hidden and
very much higher, false positive rate in Pillar 2. The reader will have to decide for themselves.
Pillar 2 testing has been ongoing since May but it's only in recent weeks that it has reached several hundreds of thousands of tests
per day. The effect of the day by day climb in the number of people that are being described as 'cases' cannot be overstated. I know
it is inducing fear, anxiety and concern for the possibility of new and unjustified restrictions, including lockdowns. I have no
idea what Mr Hancock's motivations are. But he has and continues to use the hugely inflated output from a fatally flawed Pillar 2
test and appears often on media, gravely intoning the need for additional interventions (none of which, I repeat, are proven to be
effective).
You will be very familiar with the cases plot which is shown on most TV broadcasts at the moment. It purports to show the numbers of
cases which rose then fell in the spring, and the recent rise in cases. This graph is always accompanied by the headline that "so
many thousands of new cases were detected in the last 24 hours".
You should know that there are two major deceptions, in that picture, which combined are very likely both to mislead and to induce
anxiety. Its ubiquity indicates that it is a deliberate choice.
Firstly, it is very misleading in relation to the spring peak of cases. This is because we had no community screening capacity at
that time. A colleague has adjusted the plot to show the number of cases we would have detected, had there been a well-behaved
community test capability available. The effect is to greatly increase the size of the spring cases peak, because there are very
many cases for each hospitalisation and many hospitalisations for every death.
Secondly, as I hope I have shown and persuaded you, the cases in summer and at present, generated by seriously flawed Pillar 2
tests, should be corrected downwards by around ten-fold.
I do believe genuine cases are rising somewhat. This is, however, also true for flu, which we neither measure daily nor report on
every news bulletin. If we did, you would appreciate that, going forward, it is quite likely that flu is a greater risk to public
health than COVID-19. The corrected cases plot (above) does, I believe, put the recent rises in incidence of COVID-19 in a much more
reasonable context. I thought you should see that difference before arriving at your own verdict on this sorry tale.
There are very serious consequences arising from grotesque over-estimation of so-called cases in Pillar 2 community testing, which I
believe was put in place knowingly. Perhaps Mr Hancock believes his own copy about the level of risk now faced by the general
public? Its not for me to deduce. What this huge over-estimation has done is to have slowed the normalisation of the NHS. We are all
aware that access to medical services is, to varying degrees, restricted. Many specialities were greatly curtailed in spring and
after some recovery, some are still between a third and a half below their normal capacities. This has led both to continuing delays
and growth of waiting lists for numerous operations and treatments. I am not qualified to assess the damage to the nation's and
individuals' health as a direct consequence of this extended wait for a second wave. Going into winter with this configuration will,
on top of the already restricted access for six months, lead inevitably to a large number of avoidable, non-Covid deaths. That is
already a serious enough charge. Less obvious but, in aggregate, additional impacts arise from fear of the virus, inappropriately
heightened in my view, which include: damage to or even destruction of large numbers of businesses, especially small businesses,
with attendant loss of livelihoods, loss of educational opportunities, strains on family relationships, eating disorders, increasing
alcoholism and domestic abuse and even suicides, to name but a few.
In closing, I wish to note that in the last 40 years alone the UK has had seven official epidemics/pandemics; AIDS, Swine flu, CJD,
SARS, MERS, Bird flu as well as annual, seasonal flu. All were very worrying but schools remained open and the NHS treated everybody
and most of the population were unaffected. The country would rarely have been open if it had been shut down every time.
I have explained how a hopelessly-performing diagnostic test has been, and continues to be used, not for diagnosis of disease but,
it seems, solely to create fear.
This misuse of power must cease. All the above costs are on the ledger, too, when weighing up the residual risks to society from
COVID-19 and the appropriate actions to take, if any. Whatever else happens, the test used in Pillar 2 must be immediately withdrawn
as it provides no useful information. In the absence of vastly inflated case numbers arising from this test, the pandemic would be
seen and felt to be almost over.
Dr Mike Yeadon is the former CSO and VP, Allergy and Respiratory Research Head with Pfizer Global R&D and co-Founder of Ziarco
Pharma Ltd.
chris/irish Bob
•
3 days ago
so they say. i doubt that seriously. sounds as if the " watch out " that vaccinated can
kill you is another ploy to keep fear porn alive.
Tom Clark
chris/irish •
3 days ago
Its both...its fear porn and also shedding...according to researchers.
The National Vaccine Information Center published an important document relevant to this
topic titled "The Emerging Risks of Live Virus & Virus Vectored Vaccines: Vaccine Strain
Virus Infection, Shedding & Transmission." Pages 34-36 in the section on "Measles, Mumps,
Rubella Viruses and Live Attenuated Measles, Mumps, Rubella Viruses" discuss evidence that
the MMR vaccine can lead to measles infection and transmission.
Studies Show that Vaccinated Individuals Spread Disease
https://www.globenewswire.c...
The Vaccinated Spreading Measles: WHO, Merck, CDC Documents Confirm
https://www.greenmedinfo.co...
shedding vaccines studies
https://scholar.google.com/...
Authored by Kit Knightly via Off-Guardian.org,
New policies will artificially deflate "breakthrough infections" in the vaccinated, while
the old rules continue to inflate case numbers in the unvaccinated.
The US Center for Disease Control (CDC) is altering its practices of data logging and
testing for "Covid19" in order to make it seem the experimental gene-therapy "vaccines" are
effective at preventing the alleged disease.
They made no secret of this, announcing the policy changes on their website in late
April/early May, (though naturally without admitting the fairly obvious motivation behind the
change).
The trick is in their reporting of what they call "breakthrough infections" – that is
people who are fully "vaccinated" against Sars-Cov-2 infection, but get infected anyway.
Essentially, Covid19 has long been shown – to those willing to pay attention –
to be an entirely created pandemic narrative built on two key factors:
False-positive tests. The unreliable
PCR test can be manipulated into reporting a
high number of false-positives by altering the cycle threshold (CT value)
Inflated Case-count. The incredibly broad definition
of "Covid case", used all over the world, lists anyone who receives a positive test as a
"Covid19 case", even if they never experienced any symptoms .
Without these two policies, there would never have been an appreciable pandemic at all , and
now the CDC has enacted two policy changes which means they no longer apply to vaccinated
people.
Firstly, they are lowering their CT value when testing samples from suspected "breakthrough
infections".
From the CDC's instructions for state health authorities on handling "possible breakthrough
infections" (uploaded to their website in late April):
For cases with a known RT-PCR cycle threshold (Ct) value, submit only specimens with Ct
value ≤28 to CDC for sequencing. (Sequencing is not feasible with higher Ct values.)
Throughout the pandemic, CT values in excess of 35 have been the norm, with labs around the
world going into the 40s.
Just a Little Froth in the Market 15 hours ago
They are manipulating the numbers to make it look like only the unvaxxed get infected.
That is fraud, and this rogue agency needs to be stopped.
Enraged 1 hour ago remove link
The CDC is not an independent government agency, but is actually a subsidiary of Big
Pharma.
The CDC owns patents on at least 57 different vaccines, and profits $4.1 billion per year
in vaccination sales.
There are CDC patents applicable to vaccines for Flu, Rotavirus, Hepatitis A, HIV,
Anthrax, Rabies, Dengue fever, West Nile virus, Group A Strep, Pneumococcal disease,
Meningococcal disease, RSV, Gastroenteritis, Japanese encephalitis, SARS, Rift Valley Fever,
and chlamydophila pneumoniae.
https://goldenageofgaia.com/2018/12/07/robert-kennedy-jr-cdc-is-a-privately-owned-vaccine-company/
yerfej 7 hours ago
People might be starting to get the impression that the federal regime, which owns the
media, judiciary, academia, bureaucracy, and big tech, are attempting to manipulate
information to increase their power and wealth. The elites have confiscated almost ALL the
commoners wealth and now they want the rest of the money and complete and total control. Mao
or Stalin would be proud of these fascists.
LetThemEatRand 17 hours ago
Imagine living under the rule of a globalist oligarchy that controls the Press. That.
JakeIsNotFake 14 hours ago remove link
What is that if not an obvious and deliberate act of deception?
Well, before 3/20, this would have been a FELONY. Each time a lab provided a patient with
KNOWINGLY FALSE test results, the lab and the doctor would have been subject to a 16 month
term in the state penitentiary. For each instance.
Can you imagine getting a positive, terminal prognosis, committing a well deserved murder,
and then not dying?
Oopsie! My bad.
gregga777 14 hours ago
Government, and that especially includes the so-called "Scientists" in government service,
are Corrupt, Incompetent, Unaccountable and Untrustworthy. The Government's so-called
"Scientists," including those funded by Government contracts, are no more trustworthy than
politicians.
PeterLong 14 hours ago
Sometimes you have no choice. We had to undergo surgical procedures in a hospital and had
to get tested a few days before. Whether they use the same parameters for these type cases as
for others I don't know. Perhaps they are reluctant to turn away or delay surgical cases for
BS reasons and therefore possibly use more realistic standards , but my opinion of the entire
medical industry has become so low that I could believe anything. I still wonder about
hospital and other medical practices finances concenring this scam. Have they continued to
profit somehow despite being shut down in some ways?
Beebee 1 hour ago (Edited) remove link
Same here, Peter. Hubby's mother broke her elbow last year. And we had to bring her to
tests to do surgery. She was negative. But, afterwards, suddenly, developed lymphoma. Now, I
wonder about these tests! The cancer chemo was delayed due to all this stuff. She had so many
Covid tests, all negative, and just now completed the chemo rounds. It's not necessary and
they do make a profit. She is the only reason we stay here, otherwise we would moved from NY.
She's a mess, and I resent the fact the hold-ups are due to testing.
fewer 36 minutes ago
Hospitals made tons of money on this. Uncle Sugar pays so much, and the administrators
always slice & dice the budget/reports so they seem on the edge of bankruptcy no matter
what. Naturally all of this is "debunked" by (((the usual sources))).
Here's one fact that the "debunkers" deliberately ignore: the feds pay for all the
treatment of uninsured C19 patients... including illegals . Normally if an illegal comes to
the ED and needs to be admitted, the hospital can't refuse to do that and instead has to eat
the cost (well, they pass the cost on to hardworking, insurance having people like you and
me, but bear with me).
If they admit the person for a reason *other* than C19, then the hospital still eats the
cost. Now, tell me, what's the incentive here if an illegal comes in with a bunch of
comorbidities and needs admission to manage those? What should be recorded as the admitting
diagnosis/problem if they can get swabbed for a high Ct PCR test (a meaningless positive
result)?
lasvegaspersona 7 hours ago
After more than 50 years in medicine, I tell friends and family, 'stay away from us if you
can'. Modern medicine is a rats nest of false positive testing and chasing trivial
abnormalities on imaging studies.
The sad part is patients feel relieved when they are told 'nothing was finally
found'....this after great expense of time and money.
spiff 54 minutes ago
Caught Red-Handed
Yes, define "Caught". I have a feeling life will continue without consequences for the
perpetrator of this fraud, or even your average person knowing about it.
_triplesix_ 14 hours ago
CDC, FBI, CIA, DHS, NIH, EPA, DOE...shall I go on?
Drater 6 hours ago
FAA, TSA, SEC, FCC, NHTSA, DOJ
JakeIsNotFake 13 hours ago
CDC is .gov. As an NGO, (funded by 99% .gov and 1% phony donations), the CDC can legally,
(not honestly), claim they are just an advisory body.
While noteing the distinction, please pay attention to the language: Mask mandate,
guidelines, advisories are NOT laws. Just like travel advisories, protocols, and best
practice. These are all weasel words. And totally unenforceable.
snatchpounder PREMIUM 9 hours ago
Everything is rigged, this plandemic, elections, markets you name it because when there's
currency to be made you'll always have someone more than willing to do it. Big pharma is
making a killing literally in this case and tax slaves paid for the gene therapy shots
creation. And all the rubes who took the shot will pay much more than just currency for their
naivety.
archipusz 11 hours ago
We can speculate all we want about what the agenda is of the CDC.
But what we know is that it has nothing to do with the truth or our health.
Enraged 1 hour ago remove link
The CDC is not an independent government agency, but is actually a subsidiary of Big
Pharma.
The CDC owns patents on at least 57 different vaccines, and profits $4.1 billion per year
in vaccination sales.
There are CDC patents applicable to vaccines for Flu, Rotavirus, Hepatitis A, HIV,
Anthrax, Rabies, Dengue fever, West Nile virus, Group A Strep, Pneumococcal disease,
Meningococcal disease, RSV, Gastroenteritis, Japanese encephalitis, SARS, Rift Valley Fever,
and chlamydophila pneumoniae.
https://goldenageofgaia.com/2018/12/07/robert-kennedy-jr-cdc-is-a-privately-owned-vaccine-company/
paranoid.dragon 8 hours ago
amazing they do not even try to hide the deception.
but reporting on such deception will have one labeled a "conspiracy theorist", and the FBI
classifies "conspiracy theorists" as "domestic terrorists".
That's right, re-stating publicly available comments and policies of government agencies
and officials will have you branded as a domestic terrorist.
And the "intellectuals" in the media, academia, and "think-tanks" have abandoned all logic
and common sense to serve their masters in the government and big pharma.
history will not forget.
smacker 12 hours ago
Very good article which rightly exposes the CDC and all those around it for being utterly
corrupt and are perpetrating a fake pandemic with sinister objectives.
crazzziecanuck 11 hours ago
You realize, it's Putin's fault. Putin can rig a presidential election, it's child's play
for him to manipulate the CDC to do his evil bidding.
Everything is Putin's fault: Trump, COVID, 737 Max crashes, slavery, crucifixion of
Christ, the end of the dinosaurs, and so on.
archipusz 13 hours ago
Notice how Rand Paul will argue with Fauci about policy over when we should wear a mask,
BUT WILL NOT DARE ASK THEM WHY THEY HAVE, AND ARE, COMMITTING CRIMINAL FRAUD WITH THE PCR
TESTING?
Demystified 2 hours ago
It's a rigged game, a scam. These people are so dishonest, and intent on falsifying Covid
test results by applying different standards for vaccinated and unvaccinated people? They are
perpetuating a fraud on the people.
You have to be brain dead to not see what they are doing.
Robert De Zero 3 hours ago remove link
This is so evil. Medicalized dictatorship, supported by propaganda media, is here.
Alien 851 4 hours ago
This is NEWS??? Are you kidding?
It was March 2020 when they changed the rules on reporting of Covid deaths to run the
count as high as possible. It is still used in fear headlines today! How about wildly
fluctuation "new cases" that seem to totally respect state borders...?
For God's sake, wake the hell up!!!!
In March, the CDC redefined what is to be reported by Medical Examiners in the US. One
of them gave examples of Covid Death cases reporting criteria:
"The case definition is very simplistic," Dr. Ngozi Ezike, director of Illinois
Department of Public Health, explains. "It means, at the time of death, it was a COVID
positive diagnosis. That means, that if you were in hospice and had already been given a
few weeks to live, and then you also were found to have COVID, that would be counted as a
COVID death. It means, technically even if you died of clear alternative cause, but you had
COVID at the same time, it's still listed as a COVID death."
Sweden presently offers 3 different COVID-19 jabs: Moderna, Pfizer and AstraZeneca, with the
latter being the most widely available (while other European states like Germany have sought to
offer substitutes to younger patients, who are more vulnerable to dangerous cerebral blood
clots, which are a rare - but not unheard of - side effect).
The number of suspected adverse reactions from the two shots seems relatively small when
compared to the 19,961 reports linked to AstraZeneca's Vaxzevria, while the AstraZeneca shot
only accounts for about 26% of the roughly 2.7MM vaccines that have been administered so far in
Sweden, but makes up around 63% of the side effects reports.
Ebba Hallberg, an official with the Medical Products Agency, told Swedish media that it was
unusual to receive so many reports of side effects. She added that the tally was likely higher
because of public focus on the new vaccines.To head off complaints that many of the incidences
of side effects were minor, she said healthcare providers are likely only reporting the more
"serious" side effects.
One Swedish media outlet said the number of complaints filed in just a few months exceeded
the number typically filed over 4 years, which underscores the public anxieties about the COVID
vaccines.
In March, Sweden was one of several nations to temporarily suspend the use of the
AstraZeneca jab, following reports of abnormal blood clotting in recipients. AstraZeneca, as
well as the European Medicines Agency, have insisted that the vaccine is safe after it came
under scrutiny.
4 hours ago remove link
I honestly don't understand how anyone could inject this toxic shot into someone's arm, see
with their own eyes someone having a severe adverse reaction, and then continue to get back to
work injecting more people. What the hell is wrong with these people? play_arrow 51 play_arrow
2
Friedrich not Salma 4 hours ago
It's the teevee. I asked a 75 year old man today "Do you think the nightly news would ever
lie to you?" His answer: "No, I would certainly hope not, or at least not intentionally."
I walked him through how the news is full of Pharma ads and how there was no chance Pharma
would put up with a pharma investigative segment. He at least gave it some thought. His son
wouldn't budge on the idea that the teevee would ever lie.
Billy the Poet 4 hours ago
Ask them to show you the Weapons of Mass Destruction. Then point out that both the TV and
the government lie.
zvzzt 2 hours ago
Even worse (IMHO), if they make a mistake, they'll turn and twist in every way to avoid
any blame, making things worse along the way. Promote the 'fvcker-ups" so they don't rock any
boats.
Zero skin in the game, zero accountability ("you can always vote them away if you dont
like them", right.... ) and thus zero credibility.
And than the endless comment "It's all part of the political game/theatre"... Destroying
lives, destroying value, killing people accross the globe and depressing people for no other
reason than a "game"? Lowest form of life. MSM is just a willing toothless prostitute.
Pie rre 56 minutes ago (Edited)
I used to search the Web for anecdotal experiences with meds my doctor advises me to take.
I Used to be successful but not any longer so I imagine the pharm industry now has bots that
search for and bury them.
PrivetHedge 3 hours ago
Nuremberg Code: Informed Consent.
Deliberate misinformation and witholding of valid information = people doom
themselves.
But we are way beyond laws and democracy now, this is a sustained onslaught: a slaughter
of the naive and careless. Leaving a core population who know exactly what they did: and who
did it. This is probably the biggest flaw in their plan. Plenty of powerful people who don't
want this plan.
As more and more see it, we could see some pushback. Already Gates is becoming a liability
for Technocracy, some in the Trilateral Commision will want him gone. Same with Fauci, the
poison dwarf's credibility is shot and they need a new puppet.
theWHTMANN 4 hours ago
I heard today that the number of vax deaths in the US is 4,191 - more than the combined
vax deaths for all vaccinations in 20 years. In 1976, 25 people died of swine flu vax and
they stopped it in its tracks. Hmmm.
aspnaz again 4 hours ago
FDA worked for the people in the 70s, it now rubber stamps for corporations trying to rip
you off for evermore useless and more dangerous drugs.
Billy the Poet 3 hours ago
From the 5/7/2021 release of VAERS data:
Found 4,057 cases where Vaccine is COVID19 and Patient Died
https://medalerts.org/vaersdb/findfield.php?TABLE=ON&GROUP1=AGE&EVENTS=ON&VAX=COVID19&DIED=Yes
triedandtried 1 hour ago remove link
Apparently side-effect reports make it to VAERS only if the adverse reaction or death
occurs within 1-2 days of the administration of the vaccine. So if someone's skin falls off
on day 3, too bad, not counted .
PrivetHedge 3 hours ago remove link
Yes, CDC is hiding the numbers, most deaths we see are from January.
https://healthimpactnews.com/2021/the-cdcs-crimes-against-humanity-for-allowing-12-to-15-year-olds-to-be-injected-with-covid-bioweapon-shots/
(CNN) A Colorado mass vaccination site paused operations this week after 11
people experienced adverse reactions to the Covid-19 vaccine
. More than 1,700 people received the Johnson & Johnson vaccine on Wednesday at Dick's
Sporting Goods Park, a soccer stadium where the state of Colorado and health care provider
Centura Health operate a mass
vaccination site . The 11 people reported feeling nauseous and dizzy after they were
vaccinated, Colorado health officials said. Two of the patients were transported to a hospital
"out of an abundance of caution," while the other nine were given juice and water to recover,
according to a statement from the Colorado State Joint Information Center. Don't freak out
if you get these side effects from a Covid-19 vaccine. They can actually be a good sign
Officials didn't elaborate on the two hospital patients' conditions. "The state has no reason
to believe that people who were vaccinated today at Dick's Sporting Goods Park should be
concerned," state health officials said. The site closed early on Wednesday afternoon, before
another 640 people were scheduled to receive their vaccine. Their appointments have been
rescheduled to Sunday, Centura Health said. Enter your email to subscribe to the CNN Five
Things Newsletter. "close Email Capture Inline
Zone"
privacy policy. Severe side effects from Covid-19 vaccines are rare It's relatively
common to experience side effects from any of the three vaccines available in the US -- about
10% to 15% of volunteers in vaccine trials developed "quite noticeable side effects," former
Operation Warp Speed Chief Scientific Adviser Moncef Slaoui said late last year. The most
common side effects are arm soreness, fatigue, body aches and, in some cases, a low-grade
fever. Nausea, like the 11 patients in Colorado experienced, headaches and swelling at the
injection site may occur, too, according to the US Centers for Disease
Control and Prevention. Severe side effects, like an allergic reaction, are far less
common, occurring around every two to five per million people, Baylor College of Medicine dean
Dr. Peter Hotez told CNN earlier
this month . Johnson & Johnson vaccine is effective Health officials continue to
combat the stigma that Johnson & Johnson is a lesser vaccine than the Moderna and Pfizer
two-shot offerings, which a
recent CDC study found are 90% effective at preventing Covid-19. Johnson & Johnson's
vaccine was
found to be 66% effective in preventing moderate to severe illness. It's difficult to draw
comparisons between Johnson & Johnson and the two-shot alternatives, though, because the
Johnson & Johnson vaccine was studied after highly contagious variants of coronavirus were
discovered, said
Dr. Leana Wen , a CNN medical analyst. The vaccine was found to be effective in preventing
severe disease in South Africa, where a contagious variant became dominant, and no patients who
received the vaccine were hospitalized or died. "Having a vaccine that is clearly effective
against this type of mutation is a distinct advantage," she told CNN in March.
CNN's Holly Yan and Katia Hetter contributed to this report.
MAY 15, 2021
Authored
by Ryan McMaken via The Mises Institute,
In any given year during the past decade in the United States, more than 2.5 million
Americans have died - from all causes.
The number has grown in recent years, climbing from 2.59 million in 2013 to 2.85 million in
2019. This has been due partially to the US's aging population, and also due to rising obesity
levels and drug overdoses . In fact, since 2010, growth rates in total deaths has exceeded
population growth in every year.
In 2020, preliminary numbers suggest a jump of more than 17 percent in all-cause total
deaths, rising from 2.85 million in 2019 to 3.35 million in 2020.
The increase was not all due to covid. At least one-quarter to
one-third appear to be from other causes. In some cases, more than half of "excess deaths"
were attributed to "underlying causes " other than covid. But whether due to untreated
medical conditions (thanks to covid lockdowns), or drug overdoses, or homicides, total death
increased in 2020. In other words, total excess mortality is a partial proxy for covid deaths.
Whatever proportion of total deaths covid cases may comprise, it stands to reason that if total
deaths decline, then covid deaths are declining also. Moreover, looking at total deaths helps
cut through any controversies over whether or not deaths are properly attributed to covid.
What has been the trend with these "excess deaths" in recent months?
Well, according
to data through mid-March reported by Our World in Data and by the Human Mortality
Database, excess mortality began to plummet in early January and is now back to levels below
the 2015-2019 average:
Excess mortality peaked the week of January 3 and then it began to collapse, dropping back
to summer 2020 levels by mid February. By March 14, excess mortality was at 1 percent above the
2015-2019 average. All this occurred even as very few Americans were vaccinated. When excess
deaths began to drop, less than one percent of
Americans had been fully vaccinated . At the end of January, less than tw o percent of
Americans had been fully vaccinated. By the end of March, when excess mortality returned to
2019 levels, 15 percent of the population had been fully vaccinated.
As of May 11, only one-third of Americans had been fully vaccinated, although "experts"
insist 60 to 70 percent of the population must be vaccinated before we can expect to see a
drop-off in deaths like that which occurred earlier this year.
Yet, as of the week of March 22 -- excess mortality was below both the 2015-2019 average and
below the total for the last year before the official beginning of the covid pandemic
(2019).
It's likely these facts won't stop "public health" bureaucrats from continuing to insist
that another "wave" of covid deaths and cases is right around the corner. These activists have
many strategies for pushing vaccine passports, mask mandates, and even continual precautionary
business closures. They'll tell us that new covid variants are sweeping the globe. This is what
they were saying in January, for instance, when Vox
was telling us it was too dangerous to even visit the grocery store . At least one expert
in late January warned us that the coming weeks would be "
the darkest weeks of the pandemic ."
It's now clear such predictions were spectacularly wrong. By late January, totals deaths
were already in precipitous decline.
But what about the lag in data? We're only looking at data up to mid-March because it tends
to take several weeks for estimates of total deaths to become reasonably reliable. Yes, that
data shows a big drop off. But what about the numbers for April and May? Should we expect those
death totals to surge again with a promised "fourth wave" of new covid death?
If we consider the more recent case and death totals attributed to covid, we see few signs
of a new surge.
Although Anthony Fauci and other government employed technocrats
have been unable to provide any explanation at all for it , the fact remains that months
after Texas and Florida and Georgia have either abolished or greatly scaled back all
social-distancing and mask mandates, cases and deaths are generally declining, and total deaths
per million (attributed to covid) remain below what we've seen in states with severe
lockdowns.
The trend in the United States overall is similar. Indeed, it appears that nearly all states
have seen sizable drops in both cases and deaths, regardless of the mask or
social-distancing policies in place.
Notably, it's only in recent weeks that "CDC guidelines" are beginning to admit the reality.
It wasn't until April 26 that the CDC
declared that fully vaccinated Americans are allowed to venture outside without masks on .
The CDC states these "recommendations" unironically as if it weren't the case that most
Americans -- outside of true-believer hotspots like San Francisco and Chicago -- stopped
wearing masks outside a long time ago. The hermetically sealed world of government employees
and corporate journalists appears unaware that at least half the country pretty much went back
to normal last fall.
So now what?
The technocrats know that they need to keep pressing hard for more de facto vaccine mandates
-- pushed mostly by corporate America for low-risk younger populations. Most Americans can
already see that covid numbers are already in decline in spite of months of Americans flouting
mask mandates and social distancing guidelines. People can see that children -- an increasing
number of whom are returning to schools -- aren't a significant factor in the spread of
disease. So it will be important for the regime to push vaccines for children more aggressively
before people stop listening to the "experts" completely.
Don't expect the regime to admit it has been wrong about anything. If anything, it will
double down on the usual narrative. It's worked pretty well so far.
man_hammer 2 minutes ago (Edited) remove link
What excess death rate ?
2020 8.9 1.19 %
2019 8.8 1.29 %
2018 8.7 1.35 %
2017 8.6 1.37 %
2016 8.5 1.31 %
2015 8.4 1.21 %
2014 8.3 1.02 %
2013 8.2 0.82 %
2012 8.1 0.54 %
Net increase of deaths is zero
alexcojones 1 hour ago remove link
Covidiots (noun)
So-called experts, pseudo scientists, and fake media pundits were on TV, comparing
Covid-19 to the Spanish Flu of 1918 when the lockdowns began. Compare:
If we adjusted for the world population increase and for Covid-19 to be as deadly as the
Spanish Flu, C-19 would have killed roughly 216 million people (50 million x 4.3 to offset
for the increase of population = 216 million).
Plandemic or Scamdemic, you choose
JaxPavan 1 hour ago
Take a look at the CDC total death figures for 2020. It's the only year they publish CDC
"predictions" instead of what the states actually reported. That's right, CDC is "predicting"
the past in 2020. Fact is the real overall mortality probably didn't budge much in 2020.
Lying sacks of excrement.
2thelastman 8 minutes ago
I wouldn't believe anything "science" tells us any longer. Throw all the charts at me you
want to, you've lied so often about so much so completely that you have zero credibility
left. None, nada, nicto.
The communists have accomplished that much.
In Germany, one researcher thinks he has found what is triggering the clots. Andreas Greinacher, a blood expert, and his team at the
University of Greifswald believe so-called viral vector vaccines -- which use modified harmless cold viruses, known as adenoviruses, to
convey genetic material into vaccine recipients to fight the coronavirus -- could cause an autoimmune response that leads to blood
clots. According to Prof. Greinacher, that reaction could be tied to stray proteins and a preservative he has found in the
AstraZeneca vaccine.
Prof. Greinacher and his team has just begun examining Johnson & Johnson's vaccine but has identified more than 1,000 proteins in
AstraZeneca's vaccine derived from human cells, as well as a preservative known as ethylenediaminetetraacetic acid, or EDTA. Their
hypothesis is that EDTA, which is common to drugs and other products, helps those proteins stray into the bloodstream, where they
bind to a blood component called platelet factor 4, or PF4, forming complexes that activate the production of antibodies.
The inflammation caused by the vaccines, combined with the PF4 complexes, could trick the immune system into believing the body had
been infected by bacteria, triggering an archaic defense mechanism that then runs out of control and causes clotting and bleeding.
Prof. Andreas Greinacher is looking at the possible cause of an autoimmune response that leads to blood clots.
PHOTO:
MANUELA JANKE/UMG
Prof. Greinacher has compared the activation of the dormant response -- which has been supplanted in the evolution of the human immune
system, but still lurks in its foundations -- to "awakening a sleeping dragon."
Prof. John Kelton of McMaster University in Canada, whose outfit runs Canada's reference lab for testing patients with
blood-clotting symptoms after vaccination, said the lab replicated some of Prof. Greinacher's research and confirmed his findings.
... ... ...
One reason vaccine-induced clotting might not have been reported in the past is because shots using viral vector technology haven't
been administered at scale. The Russian vaccine Sputnik V and the shot by CanSino Biologics from China use the same technology as
AstraZeneca and Johnson & Johnson, but haven't been linked to the condition so far.
The only similar shot widely administered before the pandemic is one against Ebola by Johnson & Johnson, which was given to at least
60,000 people as of last July.
Clotting occurs between one in 28,000 and one in 100,000, according to European data -- extremely rare amid the hundreds of millions of
doses administered so far, yet higher than one in 150,000 previously assumed by some medical authorities, Prof. Greinacher said.
Most of the hundreds of people who have been diagnosed recover, but between a fifth and a third have died, and others could suffer
permanent consequences.
Data from U.S. and European regulators so far suggest young women are primarily affected by the condition. But several
scientists, including Sabine Eichinger, a senior Austrian hematologist who treated one of the first-known patients, have said the
correlation could reflect that medical workers and teachers were among the first to get the vaccines in Europe, and the majority of
them are younger women
.
Anton Potteg�rd, a professor of pharmacoepidemiology at the University of Southern Denmark, co-wrote a study of more than 280,000
people in Denmark and Norway who received the AstraZeneca vaccine. The study, which was published in the British Medical Journal on
May 5, found the incidence of rare but severe blood clots among vaccine recipients was 2.5 in 100,000.
One
recent study among healthcare workers in Israel estimated that the Pfizer-BioNTech vaccine
is 97% effective against symptomatic infection and 86% effective against asymptomatic
infection.
Serg
14
Germany introduces surveillance of "Covid deniers" and "anti-Vaxxers"
https://politnew.com/world/4874-germany-introduces-surveillance-of-covid-deniers-and-anti-vaxxers.html
For such a large country it is reasonable to expect the new mutations will emerge or already
emerged: " India is sequencing far less than 1% of daily positive samples. An early goal was to
aim for 5% of cases, but that became unrealistic once cases ballooned. The world leader, the
U.K., has been
sequencing up to 10% of samples at points in the pandemic."
... the B.1.617 variant is outpacing other variants, including the variant first identified
in the U.K.
... B.1.617 is the fourth to be classified by the WHO as a variant of concern. The U.N.
agency has also given the same designation to the B.1.1.7 variant, the B.1.35 variant found in
South Africa and the P.1 variant discovered by researchers in Brazil.
Recent research on the B.1.617 variant -- not yet peer-reviewed and published -- has shown
that it broke through to infect fully vaccinated staff at a hospital in New Delhi, though none
of them got seriously ill. A separate paper, also available before publication, found that the
variant showed evasion against a drug cocktail often used on Covid-19 patients and that it had
better entry into some cell lines, mainly in the lungs and gut. The paper also found the
variant "evaded antibodies induced by infection or vaccination, although with moderate
efficiency."
MAY 11, 2021
Authored by Andrew Chen via The Epoch Times (emphasis ours),
Economics professor Doug Allen wanted to know why so many early models used to create
COVID-19 lockdown policies turned out to be highly incorrect. What he found was that a great
majority were based on false assumptions and "tended to over-estimate the benefits and
under-estimate the costs." He found it troubling that policies such as total lockdowns were
based on those models.
" They were built on a set of assumptions . Those assumptions turned out to be really
important, and the models are very sensitive to them, and they turn out to be false ," said
Allen, the Burnaby Mountain Professor of Economics at Simon Fraser University, in an
interview.
People
walk past empty patios in Jacques Cartier Square in Montreal on May 7, 2021. (The Canadian
Press/Ryan Remiorz)
Allen says most of the early cost-benefit studies that he reviewed didn't try to distinguish
between mandated and voluntary changes in people's behaviour in the face of a pandemic .
Rather, they just assumed an exponential growth of cases of infection day after day until herd
immunity is reached.
In a
paper he published in April, in which he compiled his findings based on a review of over 80
papers on the effects of lockdowns around the world, Allen concluded that lockdowns may be one
of "the greatest peacetime policy failures in Canada's history."
He says many of the studies early in the pandemic assumed that human behaviour changes only
as a result of state-mandated intervention, such as the closing of schools and non-essential
businesses, mask and social distancing orders, and restrictions on private social
gatherings.
However, they didn't take into consideration people's voluntary behavioural changes in
response to the virus threat, which have a major impact on evaluating the merits of a lockdown
policy.
"Human beings make choices, and we respond to the environment that we're in, [but] these
early models did not take this into account," Allen said. " If there's a virus around, I don't
go to stores often. If I go to a store, I go to a store that doesn't have me meeting so many
people. If I do meet people, I tend to still stand my distance from them. You don't need
lockdowns to induce people to behave that way ."
Allen's own cost-benefit analysis is based on the calculation of "life-years saved," which
determines "how many years of lost life will have been caused by the various harms of lockdowns
versus how many years of lost life were saved by lockdowns."
Based on his lost-life calculation, lockdown measures have caused 282 times more harm than
benefit to Canadian society over the long term, or 282 times more life years lost than
saved.
Furthermore, " The limited effectiveness of lockdowns explains why, after one year, the
unconditional cumulative deaths per million, and the pattern of daily deaths per million, is
not negatively correlated with the stringency of lockdown across countries ," writes Allen. In
other words, in his assessment, heavy lockdowns do not meaningfully reduce the number of deaths
in the areas where they are implemented, when compared to areas where lockdowns were not
implemented or as stringent.
Today, some 14 months into the pandemic, many jurisdictions across Canada are still
following the same policy trajectory outlined at the beginning of the pandemic. Allen
attributes this to politics.
He says that politicians often take credit for having achieved a reduction in case numbers
through their lockdown measures.
"I think it makes perfect sense why they do exactly what they did last year," Allen
said.
"If you were a politician, would you say, 'We're not going to lock down because it doesn't
make a difference, and we actually did the equivalent of killing 600,000 people this last
year.'"
You wouldn't, he said, because "the alternative is they [politicians] have to admit that
they made a mistake, and they caused multiple more loss of life years than they saved."
Allen laments that media for the most part have carried only one side of the debate on
COVID-19 restrictions and haven't examined the other side . Adding to the concern, he says, is
that views contrary to the official government response are often pulled from social media
platforms.
He says he has heard that even his own published study has been censored by some social
media sites.
"In some sense these are private platforms. They can do what they want. But on the other
hand, I feel kind of sad that we live in the kind of a world where posing opposing opinions is
either dismissed, ignored, or name-called, [and] in some ways cancelled," Allen said.
Notable quotes:
"... Why is healthy 24-year-old Jennifer Gates jumping the line to get the vaccination when older at-risk Americans can't get an appointment? You may not have inherited your father's genius as you claim, but you certainly have his sense of entitlement. ..."
BeaglesForTrump @nice1959 ·
Feb 14
Why is healthy 24-year-old Jennifer Gates jumping the line to get the vaccination when older at-risk Americans can't
get an appointment? You may not have inherited your father's genius as you claim, but you certainly have his sense of
entitlement.
Show this thread Daniel Kotzin @danielkotzin
· 7h
Why do so many people who are fully
vaccinated care whether I have been vaccinated or not? They seem to think that vaccines only "work" if everyone is vaccinated.
Roar Still Not Restored @DETROlTLions313 ·
22h
I am getting vax shamed by my family
for not getting the vaccine yet, especially from my brother who is a surgeon. What's wrong with waiting until there is more data
if you're young and healthy with no underlying conditions?
Pfizer Inc. and
BioNTech SE 's Covid-19
vaccine was cleared for use in children age 12 to 15 in the U.S., paving the way for the mass
vaccination of middle- and high-school students before the next school year.
The Food and Drug Administration said in a statement Monday that it had expanded the shot's
original emergency use authorization to include adolescents 12 through 15 years of age.
(cnbc.com) 408
booster dose of a Covid-19 vaccine within 12 months of getting fully vaccinated . His
comments were made public Thursday but were taped April 1. From a report: Bourla said it's
possible people will need to get vaccinated against the coronavirus annually. "A likely
scenario is that there will be likely a need for a third dose, somewhere between six and 12
months and then from there, there will be an annual revaccination, but all of that needs to be
confirmed. And again, the variants will play a key role," he told CNBC's Bertha Coombs during
an event with CVS Health. "It is extremely important to suppress the pool of people that can be
susceptible to the virus," Bourla said. The comment comes after Johnson & Johnson CEO Alex
Gorsky told CNBC in February that people may need to get vaccinated against Covid-19 annually,
just like seasonal flu shots. Researchers still don't know how long protection against the
virus lasts once someone has been fully vaccinated.
CHINA /
DIPLOMACY
Death of fully vaccinated US expert in India sparks worry over Pfizer's efficacy against COVID-19 double mutant By Fan Anqi and
Lou Kang Published: May 05, 2021 08:48 PM
Medical workers prepare an oxygen parlor for COVID-19 patients in Kolkata, India, May 3, 2021. Photo: Xinhua
Pfizer COVID-19 vaccines have been dragged into the spotlight over efficacy concerns against the new double mutant variant first
found in India after an infectious disease specialist from the US, who had received two Pfizer shots prior to his arrival in India,
passed away after testing positive for coronavirus at the age of 81, local media reported on Wednesday.
Although there is no direct evidence showing reduced efficacy of Pfizer vaccines against the new mutated strain, previous studies
suggest a reduced protection rate against other variants, health experts reached by the Global Times said.
Dr Rajendra Kapila, a professor at Rutgers University in Newark, New Jersey specializing in infectious diseases, arrived in India
in late March and was scheduled to fly back to the US in mid-April, but he found he was infected with COVID-19 on April 8 and was
later admitted to Delhi's Shanti Mukund Hospital, local media the Hindustan Times reported on Wednesday.
He died at the hospital on April 28, the report said, but no details on the cause of his death have been disclosed, nor has it
been specified if Kapila was infected with the double mutated virus.
"For the last one year I have been working at a COVID-19 lab in New Jersey and had ensured a safe environment at home," said Dr
Deepti, Kapila's wife who traveled with him to India. "It is ironic that we came to India for two weeks and he contracted it here,"
she said, Hindustan Times reported.
Mainstream Western media have stayed silent on Kapila's death, and the Shanti Mukund Hospital did not reply to the Global Times'
inquiry as of press time.
However, reports have been circulating on social media such as Reddit since May, which said that Kapila had died from undisclosed
complications of COVID-19. A Facebook user named Neha Majmudar, who claimed he had been given consent from a family friend of Kapila,
replied under a post that "Kapila had history of diabetes and CAD S/P stents… and passed away following a massive heart attack
in the early morning hours." But this information cannot be verified so far.
People wait to receive COVID-19 vaccination at a government school in Delhi, India, on May 3, 2021. (Xinhua/Partha Sarkar)
India's National Institute of Virology shared limited data on the double mutant virus strain in April, which showed that of the
361 genome-sequenced samples collected between January and March this year, 220 of them - almost 61 percent - had carried the double
mutation, Indian Express reported.
In another article, the Indian Express said that the strain, also known as the B.1.617 variant, is fast replacing the previous
variant in south India and is becoming dominant, according to scientists at a local Indian research center on Tuesday.
Tao Lina, a Shanghai-based vaccine expert, told the Global Times on Wednesday there is no direct evidence showing whether the
Pfizer vaccine is effective on this variant or not, while noting that China-developed inactivated vaccines might be more effective
against the double mutant than mRNA ones.
"Technically, Pfizer vaccine uses human cells to synthesize S protein in the human body to produce antibodies, whereas China-developed
vaccines, including Sinovac and Sinopharm, use inactivated viruses as antibodies, which may cover more variants than Pfizer does,"
Tao said.
Tao added that while the efficacy of Pfizer against the new double mutant remains unknown, previous medical studies suggested
a reduced efficacy rate of Pfizer shots against other COVID-19 variants.
"The human body develops resistance to vaccines, and the variants may need even five or six doses of vaccine instead of merely
two to produce enough protection," he noted.
Chinese experts also warned that seniors, people who are obese and those with chronic diseases may have a reduced response to
vaccines, while urging India to conduct further research on Kapila's case.
According to the World Health Organization on Wednesday, over the past week India accounted for nearly half, or 46 percent, of
the world's total COVID-19 infections, and a quarter of global death toll.
According to a press release on its official website, Pfizer said its vaccines show a 95.3 percent efficacy rate against severe
COVID-19 cases, which has been defined by the US Food and Drug Administration.
(nytimes.com) 64
Posted by EditorDavid on Sunday April 11, 2021 @03:34PM from the big-thank-you dept. Long-time
Slashdot reader destinyland writes: The New York Times tells
the story of Hungarian-born Dr. Kariko, whose father was a butcher and who growing up had never
met a scientist â€" but knew they wanted to be
one . Despite earning a Ph.D. at Hungary's University of Szeged and working as a
postdoctoral fellow at its Biological Research Center, Kariko never found a permanent position
after moving to the U.S., "instead clinging to the fringes of academia."
Now 66 years old,
Dr. Kariko is suddenly being hailed as "one of the heroes of Covid-19 vaccine development,"
after spending an entire career focused on mRNA, "convinced mRNA could be used to instruct
cells to make their own medicines, including vaccines." For many years her career at the University of Pennsylvania was fragile.
She migrated from lab to lab, relying on one senior scientist after another to take her in. She
never made more than $60,000 a year... She needed grants to pursue ideas that seemed wild and
fanciful. She did not get them, even as more mundane research was rewarded. "When your idea is
against the conventional wisdom that makes sense to the star chamber, it is very hard to break
out," said Dr. David Langer, a neurosurgeon who has worked with Dr. Kariko... Kariko's husband,
Bela Francia, manager of an apartment complex, once calculated that her endless workdays meant
she was earning about a dollar an hour. One fateful day, the two scientists hovered over a dot-matrix printer in a narrow room at
the end of a long hall. A gamma counter, needed to track the radioactive molecule, was attached
to a printer. It began to spew data.
Their detector had found new proteins produced by cells that were never supposed to make
them â€" suggesting that mRNA could be used to direct any cell to make any protein,
at will.
"I felt like a god," Dr. Kariko recalled. "We both started writing grants," Dr. Weissman said. "We didn't get most of
them. People were not interested in mRNA. The people who reviewed the grants said mRNA will not
be a good therapeutic, so don't bother.'" Leading scientific journals rejected their work. When
the research finally was published , in
Immunity , it got little attention... "We talked to pharmaceutical companies and venture
capitalists. No one cared," Dr. Weissman said. "We were screaming a lot, but no one would
listen."
Eventually, though, two biotech companies took notice of the work: Moderna, in the United
States, and BioNTech, in Germany. Pfizer partnered with BioNTech, and the two now help fund Dr.
Weissman's lab.
The question is why the vaccine needed for teen, not if they are protected or not. If not natural immunity better then
immunity from Pfizer vaccine and teenagers not in danger of getting virus pneumonia in any case -- the main rational for the
development of Pfizer vaccine.
(arstechnica.com) 91
Posted by BeauHD on Wednesday March
31, 2021 @06:40PM from the vaccinated-adolescents dept. An anonymous reader quotes a report
from Ars Technica:
Adolescents ages 12 to 15 were
completely protected from symptomatic COVID-19 after being vaccinated with the
Pfizer/BioNTech mRNA vaccine in a small Phase III clinical trial, Pfizer reported in a
press release Wednesday.
The company also said that the vaccine was well-tolerated in the
age group, spurring only the standard side effects seen in people ages 16 to 25. The vaccine is
already authorized for use in people age 16 and over.
The vaccine appeared more effective at spurring defensive immune responses in adolescents
ages 12 to 15 than in the 16- to 25-year-old group, producing even higher levels of antibodies
that were able to neutralize SARS-CoV-2. In a measure of neutralizing antibodies, vaccinated
youths in the new trial had geometric mean titers (GMTs) of 1,239.5, compared with the GMTs of
705.1 previously seen in those ages 16 to 25, Pfizer noted.
The trial involved 2,260
adolescents ages 12 to 15, of which 1,131 were vaccinated and 1,129 received a placebo.
There
were 18 cases of symptomatic COVID-19 in the trial, all of which were in the placebo group.
In
today's press release, the company trumpeted that the vaccine demonstrated "100 percent
efficacy." The trial was not primarily designed to assess efficacy, however. It was primarily
assessing relative immune responses, so it will require more data to fully evaluate efficacy.
Additionally, Pfizer and BioNTech have only released top-line trial results, not the full data
from the trial, which has not been peer-reviewed.
(www.cbc.ca
The scientist who won the race to deliver
the first widely used coronavirus vaccine says people can rest assured the shots are safe, and
that the technology behind it will soon be used to
fight another global scourge -- cancer . Ozlem Tureci, who founded the German company
BioNTech with her husband, Ugur Sahin, was working on a way to harness the body's immune system
to tackle tumors when they learned last year of an unknown virus infecting people in China.
Over breakfast, the couple decided to apply the technology they'd been researching for two
decades to the new threat.
Britain authorized BioNTech's mRNA vaccine for use in December, followed a week later by
Canada. Dozens of other countries, including the U.S., have followed suit and tens of millions
of people worldwide have since received the shot developed together with U.S. pharmaceutical
giant Pfizer. [...] As BioNTech's profile has grown during the pandemic, so has its value,
adding much-needed funds the company will be able to use to pursue its original goal of
developing a new tool against cancer. The vaccine made by BioNTech-Pfizer and U.S. rival
Moderna uses messenger RNA, or mRNA, to carry instructions into the human body for making
proteins that prime it to attack a specific virus. The same principle can be applied to get the
immune system to take on tumors.
"We have several different cancer vaccines based on mRNA," said Tureci. Asked when such a
therapy might be available, Tureci said "that's very difficult to predict in innovative
development. But we expect that within only a couple of years, we will also have our vaccines
[against] cancer at a place where we can offer them to people." For now, Tureci and Sahin are
trying to ensure the vaccines governments have ordered are delivered and that the shots respond
effectively to any new mutation in the virus.
(cnbc.com) 131
Posted by msmash on Friday March 19, 2021 @03:25PM from the closer-look dept.
The highly
contagious variant first identified in the U.K. likely accounts for
up to 30% of Covid-19 infections in the United States , White House Chief Medical Advisor
Dr. Anthony Fauci said Friday. From a report:
The variant, called B.1.1.7, has also been
reported in at least 94 countries and detected in 50 jurisdictions in the U.S., Fauci said
during a White House news briefing on the pandemic, adding that the numbers are likely growing.
The U.K. first identified the B.1.1.7 strain, which appears to spread more easily and quickly
than other variants, last fall. It has since spread across the world, including the U.S., Fauci
said. U.S. researchers have identified 5,567 cases through genetic sequencing as of Thursday,
according to the Centers for Disease Control and Prevention. U.S. health officials say the
variant could become the dominant strain in the U.S. by the end of this month or in early
April. New variants are especially a concern for public health officials as they could become
more resistant to antibody treatments and vaccines. Top health officials, including Fauci, have
urged Americans to get vaccinated as quickly as possible, saying the virus can't mutate if it
can't infect hosts and replicate.
(wtxl.com) 368
Posted by BeauHD on Friday April 02,
2021 @05:20PM from the freedom-vs-safety dept. New submitter v1 writes:
"Governor Ron DeSantis issued an executive
order Friday
forbidding local governments and businesses from requiring proof of a COVID-19 vaccine ,"
reports WTXL-TV. In addition to local businesses and governments, this move is certain to rub the restarting cruise ship
businesses the wrong way. Let the lawsuits begin!
The executive
order reads, in part: "No Florida government entity, or its subdivisions, agents, or assigns,
shall be permitted to issue vaccine passports, vaccine passes, or other standardized
documentation for the purpose of certifying an individual's COVID-19 vaccination status to a
third party, or otherwise publish or share any individual's COVID-19 vaccination record or
similar health information."
The full executive order can be found here (PDF)
(nytimes.com)
505
Posted by msmash on Monday May 03, 2021 @12:07PM from the closer-look dept. Widely circulating
coronavirus variants and persistent hesitancy about vaccines will keep the goal out of reach.
The virus is here to stay, but vaccinating the most vulnerable may be enough to restore
normalcy. From a report :
Early in the pandemic, when vaccines for the coronavirus were still just a glimmer on
the horizon, the term "herd immunity" came to signify the endgame: the point when enough
Americans would be protected from the virus so we could be rid of the pathogen and reclaim
our lives. Now, more than half of adults in the United States have been inoculated with at
least one dose of a vaccine. But daily vaccination rates are slipping, and there is
widespread consensus among scientists and public health experts that the herd immunity
threshold is not attainable -- at least not in the foreseeable future, and perhaps not ever.
Instead, they are coming to the conclusion that rather than making a long-promised exit, the
virus will most likely become a manageable threat that will continue to circulate in the
United States for years to come, still causing hospitalizations and deaths but in much
smaller numbers.
How much smaller is uncertain and depends in part on how much of the nation, and the
world, becomes vaccinated and how the coronavirus evolves. It is already clear, however, that
the virus is changing too quickly, new variants are spreading too easily and vaccination is
proceeding too slowly for herd immunity to be within reach anytime soon. Continued
immunizations, especially for people at highest risk because of age, exposure or health
status, will be crucial to limiting the severity of outbreaks, if not their frequency,
experts believe. "The virus is unlikely to go away," said Rustom Antia, an evolutionary
biologist at Emory University in Atlanta.
"But we want to do all we can to check that it's likely to become a mild infection."
The shift in outlook presents a new challenge for public health authorities. The drive for
herd immunity -- by the summer, some experts once thought possible -- captured the
imagination of large segments of the public. To say the goal will not be attained adds
another "why bother" to the list of reasons that vaccine skeptics use to avoid being
inoculated.
Yet vaccinations remain the key to transforming the virus into a controllable threat,
experts said. Dr. Anthony S. Fauci, the Biden administration's top adviser on Covid-19,
acknowledged the shift in experts' thinking. "People were getting confused and thinking
you're never going to get the infections down until you reach this mystical level of herd
immunity, whatever that number is," he said.
There is no or very little (depending of type of vaccine) immunity from South African mutation in the USA for people who
already were vaccinated.
From comments: "Herd Immunity or Heard on the Street immunity? COVID was way over-played in order to get Biden in the WH. Now
the shoes on the other foot and the Herd Concept is eroding pretty darn fast"... "Here in the US, it's undeniable that the quantity
of covid cases were intentionally over counted -- likely for political reasons."
"If the re-infection rate is near zero and those who are the most vulnerable are 95% inoculated why should the remaining
unvaccinated (mostly youth) be needed to reach herd immunity? Their reaction to COVID-19 is either undetectable or no worse than a
mild cold. Some people, journalists, just do not want to think and/or act logically."
Notable quotes:
"... For example, there is no herd immunity from South African mutation in the USA for those who were immunized with the Moderna vaccine and Johnson and Johnson vaccine ..."
"... And more mutations will follow this and the next year. So the concept of "herd immunity" when applied to coronaviruses looks to me fuzzy; in this sense this is the goal that the nation probably can't achieve. Remember the "flattering of the curve" fiasco in NYC. Quarantine measures were completely decimated by Floyd-gate riots and authorities were forced to swallow the bitter pill. Measures they advocated proved to be useless and economically damaging. ..."
"... Coronaviruses like C19 are a moving target. Moreover, there are large swats of the US population that have weakened immune system (including some seniors) who that does not respond to vaccination, creating no protection. In large cities like NYC they will serve as the reservoir of virus mutations vaccination, or no vaccination. ..."
"... We have Fauci making unfounded statements that confuse everyone and now economists are going to tell us when herd immunity will become operative. Can't do any worse than the 'media docs'. ..."
Some view herd immunity -- the point at which a critical mass of a population become immune to a disease-causing virus or bacteria -- as a
key factor in determining when Covid-19 will be conquered and economies will return to normal. Until herd immunity is reached, some
say, governments will restrict activities to prevent the disease's spread, resulting in fewer goods and services being produced and
consumed.
Other economists say businesses can reopen and economic activity can rebound without full herd immunity, and likely will.
Part of the challenge for economists is that it is hard to know exactly when a given place will achieve herd immunity, if ever.
For
Covid-19
, epidemiologists generally believe it will require having at least 60% to 80% of a population develop antibodies,
curbing the virus's ability to spread.
... ... ...
Economists at
Goldman
Sachs Group
Inc.
have
tried to incorporate immunity estimates into their forecasts by looking at daily vaccination progress around the world and take
account of estimates of how many people have already been infected.
According to their calculations, 60% of the population in the U.S. and U.K. are already immune to Covid-19; the biggest economies
of Europe will get there by August.
Serg Bezrukov
I agree with Umesh Patil.
For example, there is no herd immunity from South African mutation in the USA for those who were immunized with the Moderna
vaccine and Johnson and Johnson vaccine
.
And more mutations will follow this and the next year. So the concept of "herd immunity" when applied to coronaviruses looks
to me fuzzy; in this sense this is the goal that the nation probably can't achieve. Remember the "flattering of the curve"
fiasco in NYC. Quarantine measures were completely decimated by Floyd-gate riots and authorities were forced to swallow the
bitter pill. Measures they advocated proved to be useless and economically damaging.
Coronaviruses like C19 are a moving target. Moreover, there are large swats of the US population that have
weakened
immune system
(including
some seniors) who that does not respond to vaccination, creating no protection. In large cities like NYC they will serve as the
reservoir of virus mutations vaccination, or no vaccination.
Rick Schaler
SUBSCRIBER
3 hours ago
We have Fauci making unfounded statements that confuse everyone and now economists are going to tell us when herd
immunity will become operative. Can't do any worse than the 'media docs'.
Umesh Patil
SUBSCRIBER
dltravers , Apr 11 2020 1:18 utc |
100
Another doctor comes forward...FROM NYC ICU: DOES
COVID-19 REALLY CAUSE ARDS??!!
I thought it might be some guy making a fake video but I guess not...
Ventilator settings wrong
Greed is King 1 hour ago
Dr. Henry Ealy and his team started looking at CDC data on COVID-19 cases and
fatalities in mid-March 2020, quickly realizing the agency was vastly exaggerating
fatalities
Over-reporting of fatalities was enabled by a March 2020 change in how cause of death
is reported on death certificates. Rather than listing COVID-19 as a contributing cause in
cases where people died from other underlying conditions, it was to be listed as the
primary cause
As of August 23, 2020, the CDC reported 161,392 fatalities caused by COVID-19. Had the
long-standing, original guidelines for death reporting been used, there would have only
been 9,684 total fatalities due to COVID-19
The CDC violated federal law, as the Paperwork Reduction Act requires data collection
and publication to be overseen by the Office of Management and Budget. Proposed changes
must be published in the Federal Register and be open to public comment. None of these
transparency rules were followed
We don't yet know who was responsible for altering the reporting rules in violation of
federal law. To identify the culprits, formal grand jury investigation petitions have been
sent to all U.S. attorneys and the U.S. Department of Justice, requesting a thorough,
independent and transparent investigation; a direct public effort to gather signatures also
commenced on the one-year anniversary of the CDC reporting change
https://articles.mercola.com/sites/articles/archive/2021/04/18/cdc-violated-law-to-inflate-covid-cases-and-fatalities
In April, the CDC reported that an
unvaccinated health-care worker set off an outbreak in a mostly vaccinated Kentucky nursing
home.
Several vaccinated seniors got sick and one vaccinated resident died.
*
To be absolutely clear: The vaccines worked to protect most residents. But no vaccine is
perfect, and the
COVID-19 vaccines won't stop all infections , especially for some people with weak immune
systems.
MAY 3, 2021
Many people I spoke with said they trusted their immune system to protect them. "Nobody ever looks at it from the perspective of a
guy who's like me," Bradley Baca, a 39-year-old truck driver in Colorado, told me. "As an essential worker, my life was never going
to change in the pandemic, and I knew I was going to get COVID no matter what. Now I think I've got the antibodies, so why would I
take a risk on the vaccine?"
Some had already recovered from COVID-19 and considered the vaccine unnecessary. "In December 2020 I tested positive and experienced
many symptoms," said Derek Perrin, a 31-year-old service technician in Connecticut. "Since I have already survived one recorded bout
with this virus, I see no reason to take a vaccine that has only been approved for emergency use. I trust my immune system more than
this current experiment."
Others were worried that the vaccines might have long-term side effects. "As a Black American descendant of slavery, I am bottom
caste, in terms of finances," Georgette Russell, a 40-year-old resident of New Jersey, told me. "The fact that there is no way to
sue the government or the pharmaceutical company if I have any adverse reactions is highly problematic to me."
Many people said they had read up on the risk of COVID-19 to people under 50 and felt that the pandemic didn't pose a particularly
grave threat. "The chances of me dying from a car accident are higher than my dying of COVID," said Michael Searle, a 36-year-old
who owns a consulting firm in Austin, Texas. "But it's not like I don't get in my car."
And many others said that perceived liberal overreach had pushed them to the right. "Before March 2020, I was a solid progressive
Democrat," Jenin Younes, a 37-year-old attorney, said. "I am so disturbed by the Democrats' failure to recognize the importance of
civil liberties. I'll vote for anyone who takes a strong stand for civil liberties and doesn't permit the erosion of our fundamental
rights that we are seeing now." Baca, the Colorado truck driver, also told me he didn't vote much before the pandemic, but the
perception of liberal overreach had a strong politicizing effect. "When COVID hit, I saw rights being taken away. So in 2020, I
voted for the first time in my life, and I voted all the way Republican down the ballot."
...
the no-vaxxers I spoke with just don't care. They've
traveled, eaten in restaurants, gathered with friends inside, gotten COVID-19 or not gotten COVID-19, survived, and decided it
was no big deal. What's more, they've survived while flouting the advice of the CDC, the WHO, Anthony Fauci, Democratic
lawmakers, and liberals, whom they don't trust to give them straight answers on anything virus-related.
The no-vaxxers' reasoning is motivated too. Specifically,
they're motivated to distrust public-health authorities who they've decided are a bunch of phony neurotics, and they're
motivated to see the vaccines as a risky pharmaceutical experiment, rather than as a clear breakthrough that might restore
normal life (which, again, they barely stopped living). This is the no-vaxxer deep story in a nutshell:
I
trust my own cells more than I trust pharmaceutical goop; I trust my own mind more than I trust liberal elites
.
DEREK THOMPSON
is
a staff writer at
The
Atlantic,
where
he writes about economics, technology, and the media. He is the author of
Hit
Makers
and
the host of the podcast
Crazy/Genius
.
Ignacio
May 7, 2021 at 4:41 am
Colonel, thanks a lot for your reporting.
I think that we are collectively failing to understand what can we expect from a campaign
of massive vaccination against a respiratory virus and more particularly against a
respiratory virus that is transmitted with relative ease amongst humans.
I think I have written about this here more than once, twice, etc. Talking about
'immunity' doesn't make much sense in a case like this. There is not a barrier (except some
difficulties the mucosae impose) to virus entry into the upper respiratory tract and as long
as viable particles enter in numbers high enough we will be infected even if we have a
humoral response (antibodies). It is only that the load will have to be increased if you have
some antibodies spread into the URT mucosae. Instead of taking about 'immunity' or a barrier
we should think about vaccination as inducing quantitative protection. The level of
protection will very much depend on the levels of neutralizing antibodies on the
nasopharyngeal mucosae compared with the entry load. So, if you have high enough levels of
antibodies you can be deemed as 'fairly immune'. The levels of antibodies in the mucosae
depend very much on the levels in blood since these cross the circulatory system to spread
around the epithelial tissues of the mucosae.
Unfortunately, to maintain high levels there, where it matters, would require high level
antibody production and sustained in time, something our body cannot afford (particularly
keeping in mind the many virus serotypes that can enter through our respiratory system). In
the best cases you will be fairly immune for some time after the second shot. Sinovac does
not distinguish herself by inducing particularly high levels of neutralizing antibodies
compared with other vaccines so it may well be the case that one is 'fairly immune' just for
a short time, let's say for instance, a few weeks.
But this not the whole story, fortunately. Whether you are fairly, moderately or barely
immune to virus entry in the URT when you have been infected or vaccinated before, not
totally naive to the Coronavirus, for instance with the Sinovac vaccine your chances to fight
the new infection are much better now and there is a range of immune tools that might prevent
further progression of the disease into the worst outcomes: you have memory cells that will
wake up fast, and with the chance of producing new antibodies against new variants that are
somehow different, and you indeed will have a faster cellular response that will help against
progression.
I think it would be very important to have a follow up of these new infections in
Seychelles and compare the development of severe respiratory syndrome between those
vaccinated and infected with those that weren't vaccinated. IMO, there will lie the real
efficiency of the Sinovac vaccine and my guess is that the incidence of severe or fatal
outcomes will be very much reduced within those vaccinated.
ambrit
May 6, 2021 at 12:59 pm
First, most, if not all commercial passenger carrying airliners have fully enclosed cabins
with heavily recycled air. I'd imagine that airliners would have efficient air filtration
systems, considering the exudations and miasmas Terran humans emit. On extended flights, the
degree of inter-personal air mixing probably approaches 100%. There have been several
graphical presentations of the transmission paths for viruses in enclosed spaces here over
the past year. So, the airliner itself, perhaps not so much a factor in virus
transmission.
The airports are where the major viral mixing would happen. International airports are
huge places, usually enclosed with 'tempered' air. The theme of the insufficiencies of the
air filtration systems in public spaces has come up here before.
I would compare giant enclosed public spaces to petri dishes. Mix your 'ingredients' and
see what grows.
Of interest to the 'curious' personality type, a long PDF from NASA outlining the computed
requirements and ancillary items for a space station. From 1982. Atmospheric considerations
are part of section 10.0.
What the NASA document shows me is that we can do the "right thing," when motivated and
funded. At least, we could do so forty years ago.
I am reminded forcefully of the follies of the PMC/Meritocrat politico class when I
consider that both the Space Shuttle Challenger and Space Shuttle Colombia disasters could
have been avoided if the relevant 'expert's' warnings had been heeded. Both disasters were
the result of politically motivated decisions by NASA middle managers, aided and abetted by
NASA upper management's craven careerism.
The 'national' response to the Pandemic is of a piece with the Space Shuttle disasters.
The Laws of Institutions 'select' for cowards and conformists.
See: https://ntrs.nasa.gov/api/citations/19820012330/downloads/19820012330.pdf
TimmyB
May 6, 2021 at 10:10 pm
This article explains the problems with passenger jet cabin air. https://www.cntraveler.com/story/how-clean-and-safe-is-a-planes-cabin-air
fresno dan
May 6, 2021 at 9:24 am
As a microbiologist, humans may be facing a reality that is inescapable. For eons, humans
had no defense against infectious diseases except what evolution provided. Pasteur published
his germ theory around 1860. Success in developing effective vaccines against scourges to
humanity followed and was truly amazing. And as is wont with humans, taken for granted. Look
at mortality tables of the 19th century and it is startling to modern sensibilities.
I think we have reached the point that the truth of the matter is that microbes ability to
evolve will exceed our ability to mount defenses. The fact that measures against microbial
pathogens succeeded so well for so long does not mean that they will continue to succeed.
I am vaccinated, and I have a long list of co-morbidities that put me at great peril. I
hope measures can be implemented that will be effective – I like living. But I think
the truth of the matter is that humans ability to control the environment is much less than
humans suppose. And that is if a significant majority of humans do the rational thing –
which considering that the proposition that a significant majority of humans are rational, is
a dubious proposition.
flora
May 6, 2021 at 12:58 pm
I think we have reached the point that the truth of the matter is that microbes ability
to evolve will exceed our ability to mount defenses.
Especially with a little help from human scientists doing gain-of-function experiments. /
;) (paging Dr. Frankensteen)
Maritimer
May 6, 2021 at 4:31 pm
For, GOF, look no further than Fauci.
https://www.newsweek.com/dr-fauci-backed-controversial-wuhan-lab-millions-us-dollars-risky-coronavirus-research-1500741
Also, let's not forget the mining of US and global health by the 'food' scientists who
design unnutritious food that tastes good. And the behavioural scientists who are more than
willing for a $ to research and design methods to sell that "food". Human health is under
attack by science.
All this while the esteemed Epidemiologists, Virologists, etc. stand obliviously and
silently by.
Pedro
May 6, 2021 at 5:36 pm
There is no herd immunity for COVID19. Period. As there never was herd immunity to the
cold or to the flu.
Raymond Sim
May 6, 2021 at 8:08 pm
I would quibble: There is currently no prospect of lasting herd immunity of the sort that
could prevent further epidemics absent competent public health measures to monitor for and
suppress the outbreaks that will inevitably occur.
TimmyB
May 6, 2021 at 10:32 pm
Monitoring and suppressing future outbreaks isn't "herd immunity." Not even close.
Instead, it's using the tried and true methods of disease control that Vietnam, New
Zealand and other countries that placed saving lives over economic activity used.
Pedro is right. There is no herd immunity.
fresno dan
May 6, 2021 at 2:31 pm
The Rev Kev
https://www.amazon.com/Body-Hero-MD-Ronald-Glasser/dp/0394400135 we believe medicine cures disease. The truth of the matter is, if your
own body's restorative functions are impaired, you will not get better. If your immune system
is impaired or diminished due to age or health condition, the vaccine is going to be
significantly less effective than when provided to a younger person in good health.https://www.mayoclinic.org/diseases-conditions/flu/in-depth/flu-shots/art-20048000
Governments and companies may find that soft bribery is the best way to get the no-vaxxers
to the clinics. Michigan Governor Gretchen Whitmer, for example,
has linked her state reopening policies to progress in shots, letting restaurants and bars
increase their occupancy once 60 percent of the state has been vaccinated, and promising to
lift mask orders when 70 percent of Michiganders have received both doses.
... the cultural backlash against domestic restrictions could be prodigious. If blue-state
governors and sports stadiums deny economic activities to the unvaccinated while red-state
stadiums allow anybody to sit at a bar or in the bleachers, it will deepen the culture-war
tensions between scolding liberals and accommodating conservatives in a way that might not be
good for Democrats politically, even if they have the upper hand in the public-health
argument.
y_arrow
GoodyGumdrops 15 hours ago (Edited)
"Our Operating System
Recognizing the broad potential of mRNA science, we set out to create an mRNA technology
platform that functions very much like an operating system on a computer. It is designed so
that it can plug and play interchangeably with different programs. In our case, the "program"
or "app" is our mRNA drug - the unique mRNA sequence that codes for a protein."
https://www.modernatx.com/mrna-technology/mrna-platform-enabling-drug-discovery-development
strych10 13 hours ago (Edited)
Not really. The author of this piece makes some mistakes and, I'd say, take things a touch
far but in the bigger scheme of things the author isn't very far off base.
I do wish that people would stop making technical errors in the way they talk about this
but that's probably not possible since this is so far over most people's heads that literally
98% of people can't understand it without a genetics course along with a couple (at least)
modern cellular biology courses to boot.
The thing about all of this, IMHO, is that what you're seeing is a massive CYA operation
here. I've covered that here before. You combine that with an ignorant media out to make
money, the general ignorance of the public, the ignorance of some well-meaning but
misinformed pundits and you're going to get a ****show.
For example "gene therapy" (I'm picking on this term and Moderna because I'm not typing
out 30+ pages here).
Yeah, Moderna played a bit loose with how they talked about their mRNA-1273 therapy. The
company referred to it as a "gene-based delivery" at least twice in the last paper that I
read from them. Now, that might be technically true in some regards depending on how they
made mRNA-1273 in terms of a template. In that case the "basis" would be the DNA they used as
either the template or the coding strand to create mRNA-1273. But that's kind of a stretch,
like saying that the basis of good batting in baseball is a solid foundation in forestry.
For all practical purposes what they're saying is not true and Moderna is adding to the
confusion by using this term. It could technically be true that they derived mRNA-1273 from a
template (or coding) strand of DNA that they created to store that information. That would,
technically, make mRNA-1273 a "gene product" (product of a gene) and you could then say that
the ultimate root basis for the Moderna jab is the template (or coding) DNA sequence that can
be transcribed into mRNA-1273. I would however point out to say that mRNA-1273 is a
"gene-based delivery" is a stretch in technical terminology and not likely to be understood
by anyone outside the biology world.
A "gene" is defined as "The fundamental physical unit of heredity, whose existence can be
confirmed by allelic variants and which occupies a specific chromosomal locus. A DNA sequence
coding for a single polypeptide or an RNA molecule" . (Essentials of Genetics, 11th ed. Klug
et al essentially the go-to text on undergraduate genetics at this point in time) Genes are
DNA and are heritable . That definition has nothing to do with mRNA-1273. mRNA is not
heritable. It's a intracellular messaging system that instructs cellular machinery to do or
produce something. It will then be degraded by proteases once its function has been
served.
Now, could this be a gene therapy? Erm, "no" but define your terms, please. The same book
defines "gene therapy" as "A therapeutic approach for providing a normal copy of a gene,
replaces a defective gene or supplementing a gene for treating or curing a genetic disorder"
. Now, with regards to any of these jabs, by design they do none of that. In fact, it would
be quite hard (though admittedly not entirely impossible) for it to happen by accident. Ergo,
this is not a gene therapy (At least not one that's intentional. Or shall we call smoking a
gene therapy?).
Now, here's the point. What I've said here are not really very reasonable objections to
these "jabs" (or whatever you'd prefer to call them) in terms of actual science. However,
they're not unexpected given the nature of what's going on, particularly if one considers the
FDA's stance on this right up until about nine months ago.
That said, rational objections to what's going on do, in fact, exist and are actually not
all that uncommon within the biological sciences community. They're simply things that most
people couldn't understand and which the media doesn't want to cover for various reasons.
The exact objection will depend on who you may talk to and what their specialty is. But
concerns about how the immune system might interpret this kind of mRNA modification over the
longer term are rational. This could produce autoimmune disorders of a huge variety of types.
It could also produce blood, specifically serum, problems that might not be survivable. Some
of the people initially reported as having had "allergic reactions" were NOT treated for
allergic reactions. They were, in essence, treated for serum sickness.
That's somewhat disturbing because no one on the planet really understands blood serum.
Modern methods for treating severe cases are going to be a combination of dialysis and
transfusion over time to remove and replace the problematic serum. And just looking at the
physical nature of the protein produced by mRNA-1273 raises some significant questions as to
if this might be a problem following apoptosis or an unexpected lysing of the cells that
express the new spike glycoprotein.
ShutUpSlave 9 hours ago remove link
I prefer to call it Gene Hacking
Maghreb2 16 hours ago
Those interested should read what Strategic Culture and
Mathew Ehret were talking about when they did their globalists in literature series a few
months back on Zero Hedge. The Huxley article was incredibly informative and deserves to be
disseminated online regardless of how you feel about Strategic Culture.
In my opinion Aldous was giving a warning but was aware of the blue print and mechanisms
due to being from a family who were twisiting science into an ideological tool of the British
establishment. His borther Julian Huxley was profoundly influential at the U.N and UNESCO.
All this was 19th century and early 20th century eugenics at play. Now the danger has been
magnified ten fold by the scientific advances that in some ways make parts of the human
condition obsolete.
In their defense the current generation are more against the conservatives than they are
the general population but its considered by some simply a strategy in the same game.
We'll see how it
plays out.....
No_Pretzel_Logic 15 hours ago
Good comment. Yep, so much of this stuff was initiated many moons ago and by people who
are long dead. I'm sort-of pissed I'm still alive to have to face this crap.
Many of us loved that song when it came out, it was fascinating to ponder the message back
then.
Now, I could only hear less than a minute and started to feel sick.
paranoid.dragon 5 hours ago
Brilliant Article!!
i think the New World Order has now firmly been in place for 50 years.
The Western Liberal Elites(which includes both Democrats and Republicans) have been living
lives of luxury at the expense of everyone else, including their own fellow citizens.
They especially hate those citizens who are true Patriots, Christians, Nationalist who
want a self-reliant country, which decides its own destiny and is not at the mercy of
foreigners, those against foreign interventionism by way of military force and economic
sanctions, those against endless money printing by the FED that is given to the seriously
corrupted wall street, those against the globalism defined by the multinational corporations
of sharehoder capitalism that suck nations dry of resources like parasites.
The Empire built by the Liberal Elites is in serious danger, not by physical force, but by
ideas.
The ideas of conspiracy theorists based on the questioning of the Liberal Elites' true
intentions that challenges their moral authority.
Conspiracy theories that map out the possible next moves of the Liberal Elites. The more
theories the better, as it closes the avenues of possible secret plots of the Liberal
Elites.
Conspiracy theories based on what-if scenarios, referencing history, challenging the
validity of history written by the "victors".
Conspiracy theories that acknowledge Marxist playbooks written in the past, but also the
constant never ending planning and plotting of new schemes.
Conspiracy theories that connect the dots between current events, true science and
mathematics, and try to fill in the blanks of obvious voids of the hidden secret knowledge
deficits the Liberal Elites are hoarding for themselves.
Conspiracy theories that are posited as questions, never accusatorial, pointing out
obvious peculiarities, so they may never be proven as false, because they were claimed to be
true in the first place.
Conspiracy theories that frustrate the Liberal Elites', obvious as they must constantly
demonize Conspiracy Theorists and refute their ideas.
Perhaps this is why the deep state FBI classified conspiracy theorists as potential
"domestic terrorists" back in 2018. Possibility a classic case of projection. As there are
far too many apparent false flag events the FBI has been allegedly been all too eager to go
along with and whitewash and sweep under the rug.
Never stop forming theories of the possible conspiracies these demonic maniacal Liberal
Elites have been scheming
rosiescenario 3 hours ago remove link
"Today's conspiracy is tomorrow's news"
This is starting to look really like staging of "Brave new world..." Today's society is
closer to Huxley's "Brave New World" than to Orwell's "1984". But there are clear elements of
both. If you will, the worst of both worlds has come true today.
Authored by Patricia McCarthy via AmericanThinker.com,
In 1949, sometime after the publication of George Orwell's Nineteen Eighty-Four , Aldous
Huxley, the author of Brave New World (1931), who was then living in California, wrote to
Orwell. Huxley had briefly taught French to Orwell as a student in high school at Eton.
Huxley generally praises Orwell's novel, which to many seemed very similar to Brave New
World in its dystopian view of a possible future. Huxley politely voices his opinion that his
own version of what might come to pass would be truer than Orwell's. Huxley observed that the
philosophy of the ruling minority in Nineteen Eighty-Four is sadism, whereas his own version is
more likely, that controlling an ignorant and unsuspecting public would be less arduous, less
wasteful by other means. Huxley's masses are seduced by a mind-numbing drug, Orwell's with
sadism and fear.
The most powerful quote In Huxley's letter to Orwell is this:
Within the next generation I believe that the world's rulers will discover that infant
conditioning and narco-hypnosis are more efficient, as instruments of government, than clubs
and prisons, and that the lust for power can be just as completely satisfied by suggesting
people into loving their servitude as by flogging and kicking them into obedience.
Could Huxley have more prescient? What do we see around us?
Masses of people dependent upon drugs, legal and illegal. The majority of advertisements
that air on television seem to be for prescription drugs, some of them miraculous but most of
them unnecessary. Then comes COVID, a quite possibly weaponized virus from the
Fauci-funded-with-taxpayer-dollars lab in Wuhan, China. The powers that be tragically deferred
to the malevolent Fauci who had long been hoping for just such an opportunity. Suddenly, there
was an opportunity to test the mRNA vaccines that had been in the works for nearly twenty
years. They could be authorized as an emergency measure but were still highly experimental.
These jabs are not really vaccines at all, but a form of gene therapy . There
are potential
disastrous consequences down the road. Government experiments on the public are
nothing new .
Since there have been no actual, long-term trials, no one who contributed to this massive
drug experiment knows what the long-term consequences might be. There have been countless
adverse injuries and deaths already for which the government-funded vaccine producers will
suffer no liability. With each passing day, new side-effects have begun to appear: blood clots,
seizures, heart failure.
As new adverse reactions become known despite the censorship employed by most media outlets,
the more the Biden administration is pushing the vaccine, urging private corporations to make
it mandatory for all employees. Colleges are making them mandatory for all students returning
to campus.
The leftmedia are advocating the "shunning" of the unvaccinated. The self-appointed
virtue-signaling Democrats are furious at anyone and everyone who declines the jab. Why? If
they are protected, why do they care? That is the question. Same goes for the ridiculous mask
requirements . They protect no one but for those in operating rooms with their insides
exposed, yet even the vaccinated are supposed to wear them!
Months ago, herd immunity was near. Now Fauci and the CDC say it will never be achieved? Now
the Pfizer shot will necessitate yearly booster shots. Pfizer
expects to make $21B this year from its COVID vaccine! Anyone who thinks this isn't about
money is a fool. It is all about money, which is why Fauci, Gates, et al. were so determined to
convince the public that HCQ and ivermectin, both of which are effective, prophylactically and
as treatment, were not only useless, but dangerous. Both of those drugs are tried, true, and
inexpensive. Many of those thousands of N.Y. nursing home fatalities might have been prevented
with the use of one or both of those drugs. Those deaths are on the hands of Cuomo and his
like-minded tyrants drunk on power.
Months ago, Fauci, et al. agreed that children were at little or no risk of getting COVID,
of transmitting it, least of all dying from it. Now Fauci is demanding that all teens be
vaccinated by the end of the year! Why? They are no more in danger of contracting it now than
they were a year ago. Why are parents around this country not standing up to prevent their kids
from being guinea pigs in this monstrous medical experiment? And now they are " experimenting
" on infants. Needless to say, some have died. There is no reason on Earth for teens, children,
and infants to be vaccinated. Not one.
Huxley also wrote this:
"The surest way to work up a crusade in favor of some good cause is to promise people they
will have a chance of maltreating someone. To be able to destroy with good conscience, to be
able to behave badly and call your bad behavior 'righteous indignation' -- this is the height
of psychological luxury, the most delicious of moral treats ."
- Crome
Yellow
Perhaps this explains the left's hysterical impulse to force these untested shots on those
of us who have made the decision to go without it. If they've decided that it is the thing to
do, then all of us must submit to their whims. If we decide otherwise, it gives them the
righteous right to smear all of us whom they already deplore.
As C.J. Hopkins has
written , the left means to criminalize dissent. Those of us who are vaccine-resistant are
soon to be outcasts, deprived of jobs and entry into everyday businesses. This kind of
discrimination should remind everyone of ...oh, Germany three quarters of a century ago. Huxley
also wrote, "The propagandist's purpose is to make one set of people forget that certain other
sets of people are human." That is precisely what the left is up to, what BLM is planning, what
Critical Race Theory is all about.
Tal Zaks, Moderna's chief medical officer, said these new vaccines are "hacking the
software of life." Vaccine-promoters claim he never said this, but he did. Bill Gates called
the vaccines " an operating
system " to the horror of those promoting it, a Kinsley gaffe. Whether it is or isn't
hardly matters at this point, but these statements by those behind the vaccines are a clue to
what they have in mind.
There will be in the next generation or so a pharmacological method of making people love
their servitude and producing dictatorship without tears , so to speak, producing a kind of
painless concentration camp for entire societies so that people will in fact have their
liberties taken away from them but will rather enjoy it.
This is exactly what the left is working so hard to effect: a pharmacologically compromised
population happy to be taken care of by a massive state machine. And while millions of people
around the world have surrendered to the vaccine and mask hysteria, millions more, about 1.3
billion, want no part of this government vaccine mania.
In his letter to Orwell, Huxley ended with the quote cited above and again here because it
is so profound:
Within the next generation I believe that the world's rulers will discover that infant
conditioning and narco-hypnosis are more efficient, as instruments of government, than clubs
and prisons, and that the lust for power can be just as completely satisfied by suggesting
people into loving their servitude as by flogging and kicking them into obedience.
Huxley nailed the left more than seventy years ago, perhaps because leftists have never
changed throughout the ages. 61,497 173
Fat Beaver 14 hours ago (Edited)
If i am to be treated as an outcast or an undesirable because i refuse the vax, i will
immediately become someone that has zero reverence for the law, and i can only imagine 10's
of millions will be right there with me.
strych10 14 hours ago
Welcome to the club.
We have coffee in the corner and occasional meetings at various bars.
Dr. Chihuahua-González 13 hours ago
I'm a doctor, you could contact me anytime and receive your injection.
Fat Beaver 13 hours ago (Edited)
I've gotta feeling the normie world you think you live in is about to change drastically
for the worse...
sparky139 PREMIUM 10 hours ago
You mean you'll sign papers that you injected us *wink *wink? And toss it away?
bothneither 2 hours ago
Oh geez how uncommon, another useless doctor with no Scruples who sold out to big Pharma.
Please have my Gates sponsored secret sauce.
Unknown 6 hours ago (Edited)
Both Huxley and Orwell are wrong. Neoliberalism (the use of once office for personal
gains) is by far the most powerful force that subjugates the inept population. Neoliberalism
demolished the mighty USSR, now destroying the USA, and will do the same to China. And this
poison dribbles from the top to bottom creating self-centered population that is unable to
unite, much less resist.
Deathrips 15 hours ago (Edited) remove link
Tylers.
https://www.youtube.com/watch?v=LIJQuk-qK2o
19331510 14 hours ago (Edited)
https://www.openvaers.com/covid-data/death-stats
AGE Deaths
0-24 23
25-50 184
51-65 506
66-80 1164
81-100 1346
U 321
R.I.P.
Joe Joe Depends 13 hours ago
India up in arms about mere 1%
spanish flu was 3%
JimmyJones 9 hours ago
Is the population of india up in arms or is the MSM?
Nelbev 10 hours ago
Facebook just flagged/censored it, must sign into see vid, Tuck also failed to mention
mRNA and adenovirus vaxes were experimental and not FDA approved nor gone through stage III
trials. Beside deaths, have blood clot issues. Good he mentioned how naturally immune if get
covid and recovered, better than vaccine, but not covered for bogus passports. Me personally,
I would rather catch covid and get natural immunity than be vaccinated with an untested
experimental vaccine.
19331510 14 hours ago
Covid19 links.
Websites:
https://www.americasfrontlinedocs.com/media/
https://covid19criticalcare.com/
https://childrenshealthdefense.org/
https://childrenshealthdefense.org/defender/
https://www.constitutionalrightscentre.ca/category/news/
https://doctors4covidethics.medium.com/
https://www.flemingmethod.com/
https://gbdeclaration.org/
https://www.lifesitenews.com/
https://healthimpactnews.com/
https://www.mercola.com/
https://drleemerritt.com/
https://www.drtenpenny.com/
https://principia-scientific.com/
https://standupcanada.solutions/canadian-doctors-speak
https://thehighwire.com/
https://vaccinechoicecanada.com/
https://vaccinechoicecanada.com/links/general-links/
Video Sharing : https://www.bitchute.com/ ; https://brandnewtube.com/ ; https://odysee.com/ ; https://rumble.com/ https://superu.net
Healthcare Professionals :
Dr. Jayanta Bhattacharya; Dr. Geert Vanden Bossche; Dr. Ron Brown; Dr. Ryan Cole; Dr.
Richard Fleming; Dr. Simone Gold; Dr. Sunetra Gupta; Dr. Carl Heneghan; Dr. Martin Kulldorff;
Dr. Paul Marik; Dr. Peter McCullough; Dr. Joseph Mercola; Dr. Lee Merritt; Dr. Judy Mikovits;
Dr. Dennis Modry; Dr. Hooman Noorchashm; Dr. Harvey Risch; Dr. Sherri Tenpenny; Dr. Richard
Urso; Dr. Michael Yeadon;
A list of Canadian doctors: https://standupcanada.solutions/canadian-doctors-speak
Lawyers : Dr. Reiner Fuellmich; Rocco Galati;
Drug Adverse Reaction Databases:
http://www.adrreports.eu/en/index.html (Search;
Suspected Drug Reactions Reports for Substances) COVID-19 MRNA VACCINE MODERNA (CX-024414);
COVID-19 MRNA VACCINE PFIZER-BIONTECH; COVID-19 VACCINE ASTRAZENECA (CHADOX1 NCOV-19);
COVID-19 VACCINE JANSSEN (AD26.COV2.S)
https://vaers.hhs.gov/data.html
Research papers :
https://cormandrostenreview.com/report/ (pcr
tests)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7680614/
(face masks)
https://onlinelibrary.wiley.com/doi/epdf/10.1111/eci.13484
(lock downs)
https://www.nejm.org/doi/full/10.1056/NEJMc2026670
(child/teacher morbidity)
https://www.medrxiv.org/content/10.1101/2020.11.01.20222315v1
(transmission by children)
https://www.cdc.gov/mmwr/volumes/70/wr/mm7010e3.htm
(masks/restaurants)
https://www.mdpi.com/1648-9144/57/3/199 (biased
trial reporting)
Covid19 links.
Websites:
https://www.americasfrontlinedocs.com/media/
https://covid19criticalcare.com/
https://childrenshealthdefense.org/
https://childrenshealthdefense.org/defender/
https://www.constitutionalrightscentre.ca/category/news/
https://doctors4covidethics.medium.com/
https://www.flemingmethod.com/
https://gbdeclaration.org/
https://www.lifesitenews.com/
https://healthimpactnews.com/
https://www.mercola.com/
https://drleemerritt.com/
https://www.drtenpenny.com/
https://principia-scientific.com/
https://standupcanada.solutions/canadian-doctors-speak
https://thehighwire.com/
https://vaccinechoicecanada.com/
https://vaccinechoicecanada.com/links/general-links/
Video Sharing : https://www.bitchute.com/ ; https://brandnewtube.com/ ; https://odysee.com/ ; https://rumble.com/ https://superu.net
Healthcare Professionals :
Dr. Jayanta Bhattacharya; Dr. Geert Vanden Bossche; Dr. Ron Brown; Dr. Ryan Cole; Dr.
Richard Fleming; Dr. Simone Gold; Dr. Sunetra Gupta; Dr. Carl Heneghan; Dr. Martin Kulldorff;
Dr. Paul Marik; Dr. Peter McCullough; Dr. Joseph Mercola; Dr. Lee Merritt; Dr. Judy Mikovits;
Dr. Dennis Modry; Dr. Hooman Noorchashm; Dr. Harvey Risch; Dr. Sherri Tenpenny; Dr. Richard
Urso; Dr. Michael Yeadon;
A list of Canadian doctors: https://standupcanada.solutions/canadian-doctors-speak
Lawyers : Dr. Reiner Fuellmich; Rocco Galati;
Drug Adverse Reaction Databases:
http://www.adrreports.eu/en/index.html (Search;
Suspected Drug Reactions Reports for Substances) COVID-19 MRNA VACCINE MODERNA (CX-024414);
COVID-19 MRNA VACCINE PFIZER-BIONTECH; COVID-19 VACCINE ASTRAZENECA (CHADOX1 NCOV-19);
COVID-19 VACCINE JANSSEN (AD26.COV2.S)
https://www.openvaers.com/
Research papers :
https://cormandrostenreview.com/report/ (pcr
tests)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7680614/
(face masks)
https://onlinelibrary.wiley.com/doi/epdf/10.1111/eci.13484
(lock downs)
https://www.nejm.org/doi/full/10.1056/NEJMc2026670
(child/teacher morbidity)
https://www.medrxiv.org/content/10.1101/2020.11.01.20222315v1
(transmission by children)
https://www.cdc.gov/mmwr/volumes/70/wr/mm7010e3.htm
(masks/restaurants)
https://www.mdpi.com/1648-9144/57/3/199 (biased
trial reporting)
Ultramarines 15 hours ago (Edited)
His making of the gamma and delta workforce was quite prescient. We are seeing it play out
now, we all know gammas and delta. There was a really good ABC tv movie made in 1980 Brave
New World. Excellent show, it shows the Alphas and names them Rothchild and so on. Shows what
these people specifically want to do to the world. I wonder if the ruling psychopaths
actually wait for science fiction authors to plan the future and then follow their
script.
Mineshaft Gap 10 hours ago
If Huxley were starting out today no major publisher would touch him.
They'd tell him Brave New World doesn't have a diverse enough of cast. Even the mostly
likable totalitarian guy named Mustapha turns out to be white! A white Mustapha. It's soooo
triggering. Also, what's wrong with a little electronic fun and drug taking, anyway? Lighten
up , Aldous.
Meanwhile his portrait of shrieking medieval Catholic nuns who think they're possessed in
The Devils of Loudun might remind the leftist editors too uncomfortably of their own recent
bleating performances at "White Fragility" struggle sessions.
Sorry, Aldous. Just...too...problematic.
Fact check- Pfizer CEO Albert Bourla has received COVID-19 vaccine "That report is categorically false," Pfizer spokeswoman
Sharon Castillo told USA TODAY via email. "Dr. Bourla has been fully vaccinated with the Pfizer-BioNTech vaccine."
Notable quotes:
"... Not a single resource on the Pfizer Executive team or Board of Directors has been injected with the Pfizer (experimental poison yet) vaccine yet. - C Weissman. Excuses allegedly provided offering the less fortunate an opportunity to go first. Don't laugh. True story. Some real humanitarians. ..."
End Times Prophecy
Not a single resource on the Pfizer Executive team or Board of Directors has been injected
with the Pfizer (experimental poison yet) vaccine yet. - C Weissman. Excuses allegedly provided offering the less fortunate an opportunity to go first. Don't
laugh. True story. Some real humanitarians.
... ... ...
single dose of the Pfizer-BioNTech vaccine protects against two of the most concerning
coronavirus variants, but perhaps only in people who have
overcome the infection naturally, research suggests.
An effective immunisation programme has long been hailed as a route out of the pandemic, however, the emergence of new variants
in Kent, South Africa and India has left many concerned the virus may no longer respond to the UK's three approved jabs.
With most confident the vaccines will be at least somewhat effective,
scientists from Imperial College
London analysed the immune response of healthcare workers at London's Barts and Royal Free hospitals after one Pfizer-BioNTech dose.
Results suggest the workers who had overcome a mild or asymptomatic infection with the original coronavirus variant experienced
"significantly enhanced protection" against the so-called Kent and South Africa variants post-jab.
The workers who had not fought off the coronavirus had a weaker immune response after the vaccine, potentially leaving them at
risk of the variants.
Read more: Everything
we know about India's coronavirus variant
A person's immune system may be "primed" after overcoming the coronavirus naturally, raising the potency of its response following
the first vaccine dose.
The results may highlight the importance of getting the second jab when called up, with the first dose similarly priming the immune
system.
The coronavirus can acquire new mutations as it replicates, some of which may enable variants to spread more easily, evade vaccines
or cause more severe disease. (Stock, Getty Images)
"Our findings show people who have had their first dose of vaccine, and who have not previously been infected with SARS-CoV-2
[the coronavirus], are not fully protected against the circulating variants of concern," said lead author Professor Rosemary Boyton.
TEL AVIV: The Pfizer vaccine is effective against the Indian variant of Covid-19, albeit at
a reduced efficacy level, Israeli authorities have said, say reports.
Israel, which has been touted as one of the world’s vaccination success
stories due to its sweeping inoculation campaign against Covid-19, has identified eight cases
of the so-called “Indian†variant of the novel coronavirus, just
days after the country ended its outdoors mask mandate
... ... ...
The Indian variant has been identified in both the UK and in Ireland.
“The impression is that the Pfizer vaccine has efficacy against it,
albeit a reduced efficacy,†the Israel’s health ministry
director-general, Hezi Levy, told Kan public radio, saying the number of cases of the variant
in Israel now stood at eight.
Israel has already vaccinated 81 per cent of its 9.3 million population, all residents above
the age of 16.
Double mutant variant
Indian authorities had in January detected a “double mutantâ€
variant of the virus, with changes to the SARS-nCov-2 virus spike protein similar to those in
both UK and South Africa at once.
While the UK variant was known to be more infectious, the South African variant was believed
to be deadlier â€" and triggered reduced efficacy rates in existing vaccines.
AstraZeneca had announced plans to develop a modification to its vaccine to better tackle
the threat of new variants, aiming to prepare this by the end of the year.
Pfizer, meanwhile, has said those who had already taken its vaccine may require a third dose
within 6-12 months, as their immunity to the virus starts to wane.
(Reuters) - A laboratory study suggests that the South African variant of the coronavirus
may reduce protective antibodies elicited by the Pfizer Inc/BioNTech SE vaccine by two-thirds,
and it is not clear if the shot will be effective against the mutation, the companies said on
Wednesday.
The study found the vaccine was still able to neutralize the virus and there is not yet
evidence from trials in people that the variant reduces vaccine protection, the companies
said.
Still, they are making investments and talking to regulators about developing an updated
version of their mRNA vaccine or a booster shot, if needed.
For the study, scientists from the companies and the University of Texas Medical Branch
(UTMB) developed an engineered virus that contained the same mutations carried on the spike
portion of the highly contagious coronavirus variant first discovered in South Africa, known as
B.1.351. The spike, used by the virus to enter human cells, is the primary target of many
COVID-19 vaccines.
Researchers tested the engineered virus against blood taken from people who had been given
the vaccine, and found a two- thirds reduction in the level of neutralizing antibodies compared
with its effect on the most common version of the virus prevalent in U.S. trials.
Their findings were published in the New England Journal of Medicine (NEJM).
Because there is no established benchmark yet to determine what level of antibodies are
needed to protect against the virus, it is unclear whether that two-thirds reduction will
render the vaccine ineffective against the variant spreading around the world.
However, UTMB professor and study co-author Pei-Yong Shi said he believes the Pfizer vaccine
will likely be protective against the variant.
“We don’t know what the minimum neutralizing number
is. We don’t have that cutoff line,†he said, adding that he
suspects the immune response observed is likely to be significantly above where it needs to be
to provide protection.
That is because in clinical trials, both the Pfizer/BioNTech vaccine and a similar shot from
Moderna Inc conferred some protection after a single dose with an antibody response lower than
the reduced levels caused by the South African variant in the laboratory study.
Even if the concerning variant significantly reduces effectiveness, the vaccine should still
help protect against severe disease and death, he noted. Health experts have said that is the
most important factor in keeping stretched healthcare systems from becoming overwhelmed.
More work is needed to understand whether the vaccine works against the South African
variant, Shi said, including clinical trials and the development of correlates of protection -
the benchmarks to determine what antibody levels are protective.
Pfizer and BioNTech said they were doing similar lab work to understand whether their
vaccine is effective against another variant first found in Brazil.
Moderna published a correspondence in NEJM on Wednesday with similar data previously
disclosed elsewhere that showed a sixfold drop antibody levels versus the South African
variant.
Moderna also said the actual efficacy of its vaccine against the South African variant is
yet to be determined. The company has previously said it believes the vaccine will work against
the variant.
The Pfizer vaccine was able to neutralize a coronavirus variant first identified in Brazil
in a new lab study, a positive sign for the vaccine's effectiveness.
...
The study also found strong neutralization of the B.1.1.7 variant, first identified in the
U.K., though that was already expected.
... The study authors cautioned that their results are based on a study in a lab and must
ultimately be validated by real-world evidence.
The coronavirus variant discovered in South Africa can “break
through†Pfizer-BioNTech’s COVID-19 vaccine to some extent, a
study in Israel found.
The South African coronavirus variant managed to penetrate the protection offered by two
doses of the Pfizer-BioNTech vaccine to some degree, though it remains unclear just how much
efficacy is lost, it said.
... ... ...
The research, released on Saturday, compared nearly 400 people who tested positive for
COVID-19 two weeks or more after they received one or two doses of the vaccine, against the
same number of unvaccinated patients with the disease.
It matched age and gender, among other characteristics.
The South African variant, B.1.351, was found to make up about 1 percent of all the
COVID-19 cases across all the people studied, according to the study by Tel Aviv University and
Israel’s largest healthcare provider, Clalit. But among patients who had
received two doses of the vaccine, the variant’s prevalence rate was eight
times higher than those unvaccinated â€" 5.4 percent versus 0.7 percent.
This suggests the vaccine is less effective against the South African variant, compared with
the original coronavirus and a variant first identified in Britain that has come to comprise
nearly all COVID-19 cases in Israel, the researchers said.
“ We found a disproportionately higher rate of the South African
variant among people vaccinated with a second dose, compared with the unvaccinated group. This
means that the South African variant is able, to some extent, to break through the
vaccine’s protection,†said Tel Aviv
University’s Adi Stern who led the study.
However, the researchers cautioned that the study only had a small sample size of people
infected with the South African variant because of its rarity in Israel.
They also said the research was not intended to deduce overall vaccine effectiveness against
any variant, since it only looked at people who had already tested positive for COVID-19, not
at overall infection rates.
Pfizer and BioNTech could not be immediately reached for comment outside business hours.
... ... ...
Almost 53 percent of Israel’s 9.3 million population has received both
doses of the Pfizer-BioNTech vaccine.
Israel has largely reopened its economy in recent weeks as the pandemic appeared to recede,
with infection rates, severe illness and hospitalisations dropping sharply.
About one-third of Israelis are below the age of 16, which means they are still not eligible
for the shot.
March 9, 2021 -- The Pfizer/ and Moderna vaccines
don’t work as well against the coronavirus variant first discovered in South
Africa as they do against the dominant virus strain first seen in United Kingdom, a new study
says.
In the study, 10 blood samples were taken from people who received the Pfizer vaccine, 28
days after the second dose, and 12 samples from those who received the Moderna vaccine , 43 days after the
second dose, Business Insider reported, citing a study published in Nature .
The goal was to find out how well the blood sample antibodies
“neutralized†the original coronavirus, the variant from South
Africa (called B.1.351), and the variant found in the U.K. (B.1.1.7).
The key finding: The percentage of positive antibodies that neutralized the South African
variant was 12.4 fold lower for the Moderna vaccine than against the original coronavirus and
10.3 fold lower for the Pfizer vaccine
, the study says.
The researchers found that the two vaccines still appear to work well against the variant
first found in the U.K.
“Overall, the neutralizing activity against B.1.1.7 was essentially
unchanged, but significantly lower against B.1.351,†the study said.
Both Pfizer and Moderna have previously said their vaccines work better against the U.K.
variant than the South African variant.
The new lab study differed from previous studies because it used real forms of the variant
taken from people who’d been infected with the virus. Earlier studies used
manufactured forms of the South African variant and showed a higher level of effectiveness for
the vaccines.
The variant first detected last fall in South Africa has now been reported in several
countries. The CDC says that in the United States, 81 cases have been found in 20 states.
More than 3,000 cases of the UK variant have been found in the U.S., with every state except
Vermont, South Dakota, and Oklahoma reporting cases as of March 8, the CDC says. Health experts
say it may soon become the dominant coronavirus strain in the country.
Researchers acknowledged the sample size was small and it’s not fully
known how the Pfizer and Moderna vaccines will work in real life against the South African
variant. Both companies have said they’re developing booster shots targeted
for the South African variant.
"I Just Wanted A Little More Time" - Texas Nurse Was Fired For Refusing COVID Vaccine
BY TYLER DURDEN SUNDAY, MAY 02, 2021 - 02:55 PM
Many hospital systems around the country have
been surprised by the number of nurses who have passed on being vaccinated (either because
they had already been infected, or simply because they didn't want the vaccine). But as federal
public health officials crank up the pressure on Americans to submit to the vaccine as unused
jabs pile up, one nurse in Texas complained to local journalists that she was fired simply
because she refused the jab.
Nurse Michelle Fuentes told Dallas-Fort
Worth CBS affiliate KRIV-TV that she had been terminated after working for 10 years at
Houston Methodist Hospital, allegedly because she refused to accept the COVID-19 vaccine.
"I knew that the date was looming over my head of me to get the vaccine and we were
constantly being pressured and pressured," Michelle Fuentes said.
According to their report, at the start of April, Houston Methodist announced it would
require all employees to get the COVID-19 vaccine by June 7. However, the hospital system asked
employees who refused to get the vaccine to submit documentation for consideration for a
medical or religious exemption. The paperwork was reportedly due by May 3.
Michelle Fuentes
Fuentes said she told her employer that she needed more time to make a decision to do more
"research" on her own, but instead wound up turning in her two weeks notice.
"I just needed a little bit more time and little bit more research to be
done,†Fuentes said.
A spokesperson for the hospital system said 90% of its employees are vaccinated, and that
only two have resigned so far. Fuentes said when she didn't agree to stay quiet about the
reason for her departure, she was not allowed to complete her final two weeks and was
immediately escorted out of the hospital by security.
Finally, Fuentes told the press that she wants to wait until all clinical trials are
completed before she decides to get the vaccine or not. She stressed she is not against
vaccines and gets the flu vaccine every year. Fuentes even volunteered to work in the COVID
unit. Despite reassurances that vaccines are safe, and that their vast public benefit outweighs
any risks, recent concerns about vaccine side effects have included
incidents of rare but deadly cerebral blood clots , and also an impact on the menstrual
cycle.
Trials of the
Novavax , Janssen/Johnson & Johnson , and AstraZeneca
vaccines in South Africa, where the B.1.351 variant of concern represents virtually all of the
circulating SARS-CoV-2, seemed to justify those concerns. The South Africa trials found lower
vaccine efficacy compared with trials in other countries where B.1.351
wasn’t dominant.
The pivotal trials of the
Pfizer-BioNTech and
Moderna vaccines, the first 2 authorized by the FDA, were conducted mainly in the US before
any cases of infection by B.1.351 or other variants of concern had been detected in the
country.
Much of the current data on the messenger RNA (mRNA) vaccines’ efficacy
against SARS-CoV-2 variants has come from laboratory studies in which researchers exposed serum
samples from immunized individuals to genetically engineered versions of concerning variants
and then measured neutralizing antibody titers. Such studies repeatedly have shown the vaccines
elicit lower levels of neutralizing antibodies against SARS-CoV-2 variants than against older,
more common isolates.
For example, in a February 17 letter to the editor in The New England Journal
of Medicine , scientists described testing serum samples from individuals immunized with 2
doses of the Pfizer-BioNTech vaccine against recombinant viruses containing some or all of the
spike protein mutations found in the B.1.351 variant. Neutralization of B.1.351 was
approximately two-thirds lower than that of USA-WA1/2020, an early SARS-CoV-2 isolate.
In another letter
published the same day, researchers reported measuring neutralizing antibody activity in serum
samples from participants in the phase 1 trial of the Moderna COVID-19 vaccine. One week after
the participants received the second dose, neutralizing antibody titers induced by a
recombinant virus bearing the B.1.351 spike protein were 6-fold lower than those induced by a
recombinant virus bearing the original Wuhan-Hu-1 spike protein.
However, that still might be sufficient to protect against COVID-19, or at least severe
COVID-19.
“Fortunately, neutralization titers induced by vaccination are high, and
even with a 6-fold decrease, serum can still effectively neutralize the virus,â€
Fauci and 2 NIAID colleagues wrote in a JAMA ï"¿ editorial posted February 11. And, they noted,
lower vaccine efficacy in the South African clinical trials could be related to geographic or
population differences.
... ... ...
Without immune correlates of protection, only real-world experience can provide answers
about COVID-19 vaccines’ efficacy against illness and death from SARS-CoV-2
variants.
“For right now, you know that a line is crossed if you see people fully
immunized with the vaccines [who], nonetheless, when infected with the variants, are being
hospitalized,†Offit said at a February 4 COVID-19 Vaccine Analysis Team press briefing.
At first glance, findings from a phase 2 trial of the Oxford-AstraZeneca vaccine in South
Africa seemed quite discouraging, spurring that country to
suspend its planned rollout of the vaccine. The trial found that the vaccine did not
protect against mild to moderate COVID-19 caused by the B.1.351 variant. The findings , posted February 12, had not
been peer reviewed.
However, “the study was not really designed to determine whether the
vaccine could protect against severe COVID or not,†principal investigator Shabir
Madhi, MBBCH, PhD, a vaccinologist at the University of the Witwatersrand, Johannesburg, and
cofounder and codirector of the African Leadership Initiative for Vaccinology Expertise, said
in a February 7 briefing about the results. Participants, who
numbered only about 2000, were youngâ€"average age 31 yearsâ€"and
healthy, so their risk of severe disease was low, vaccinated or not, explained Madhi, who also
led Novavax’s vaccine trial in South Africa.
Novavax
and
Janssen conducted larger trials in South Africa than Oxford and AstraZeneca. Although both
of their vaccines had lower efficacy rates in South Africa than in trials in other countries,
vaccinated participants who received the Janssen vaccine were still less likely to require
hospitalization for COVID-19 than those who received placebo shots, and Madhi recently
told Nature he
expected that to be the case with the Novavax vaccine as well.
.. ... ...
Pfizer and BioNTech
announced February 25 that they had begun evaluating the safety and immunogenicity of a
third dose of their vaccine to see whether it would boost immunity to SARS-CoV-2 variants. In
addition, the companies said they are discussing with regulatory agencies, including the FDA, a
clinical study to evaluate a modified vaccine based on the B.1.351 variant.
“The companies are hoping to pursue the validation of future modified mRNA
vaccines with a regulatory pathway similar to what is currently in place for flu
vaccines,†according to a press release.
Moderna
announced February 24 that it had shipped a booster vaccine candidate based on B.1.351 to
the NIAID for a phase 1 trial. And Novavax, whose first-generation vaccine
hasn’t been authorized yet in the US, announced January 28 it was working on
developing a booster, a combination bivalent vaccine, or both to protect against variants. The
company said it expected to begin clinical trials in the second quarter of 2021.
Modifying vaccines to target variants isn’t difficult. For example, with
Pfizer-BioNTech’s and Moderna’s mRNA vaccines,
“it’s very convenient, because, basically, all you do is
change a computer program and the synthetic for the synthesizing portion of this and you can
change the vaccine,†Peter Marks, MD, PhD, director of the FDA’s
Center for Biologics Evaluation and Research, which regulates vaccines, said during a January
29 American Medical Association (AMA)
webinar . “But the question is, what do we need from the FDA perspective
to feel comfortable having that deployed.â€
On February 22, the FDA updated its nonbinding
guidance for vaccine manufacturers to include information about what the agency would like
to see when evaluating vaccines that have been modified to address emerging SARS-CoV-2
variants.
The updated guidance advises manufacturers to conduct studies comparing neutralizing
antibody responses to SARS-CoV-2 induced by the modified vaccine with those induced by the
prototype vaccine. One such study should use serum samples from people who
hadn’t been previously vaccinated or infected with SARS-CoV-2, while another
study would use serum samples from people previously vaccinated with a prototype vaccine who
then received an experimental booster against variants of concern.
The Hard Part
Modifying COVID-19 vaccines would probably be the most straightforward step in dealing with
SARS-CoV-2 variants. “For vaccines and biologics, it’s
the manufacturing process that defines the product, and the manufacturing process
isn’t changing,†Baylor explained.
More challenging will be deciding when and how to deploy COVID-19 vaccines 2.0. The
influenza model, in which surveillance during the Southern Hemisphere’s flu
season identifies the circulating strains to target with vaccines in the Northern
Hemisphere’s coming flu season, doesn’t work for
SARS-CoV-2, Baylor noted.
“The challenge for COVID is what variant do you pick†when
modifying a vaccine, he said. “How often does it change?â€
Once that’s decided, would people who’ve already
received the original COVID-19 vaccine get a booster shot to protect against variants of
concern while vaccine-naive individuals receive the original vaccine and the booster rolled
into one? “Do we have the capacity to make both?†Baylor
asked.
Plus, the need to deploy vaccines or boosters targeting new variants would complicate the
already rocky rollout of COVID-19 vaccines, in part due to inexperience in vaccinating US
adults en masse.
“How do we deploy this?†Baylor said of next-generation
COVID-19 vaccines. “When do we pull the trigger to actually do
this?â€
Israeli research finds those vaccinated are at far greater risk of infection by emerging strains than those who are unvaccinated.
Talia Kustin , Noam Harel , Uriah Finkel , Shay Perchik , Sheri Harari , Maayan Tahor , Itamar Caspi , Rachel Levy , Michael Leschinsky
, Shifra Ken Dror , Galit Bergerzon , Hala Gadban , Faten Gadban , Eti Eliassian , Orit Shimron , Loulou Saleh , Haim Ben-Zvi , Doron
Amichay , Anat Ben-Dor , Dana Sagas , Merav Strauss , Yonat Shemer Avni , Amit Huppert , Eldad Kepten , Ran D. Balicer , Doron Nezer
, Shay Ben-Shachar , View ORCID Profile Adi Stern doi: https://doi.org/10.1101/2021.04.06.21254882
This article is a preprint and has not been peer-reviewed
[what does this mean?]. It reports new medical research that has yet to be evaluated and so should not be used to guide
clinical practice.
Summary
The SARS-CoV-2 pandemic has been raging for over a year, creating global detrimental impact. The BNT162b2 mRNA vaccine has demonstrated
high protection levels, yet apprehension exists that several variants of concerns (VOCs) can surmount the immune defenses generated
by the vaccines. Neutralization assays have revealed some reduction in neutralization of VOCs B.1.1.7 and B.1.351, but the relevance
of these assays in real life remains unclear. We performed a case-control study that examined the distribution of SARS-CoV-2 variants
observed in infections of vaccinated individuals (“breakthrough cases�) and matched infections of unvaccinated individuals. We
hypothesized that if there is lower vaccine effectiveness against one of the VOCs, its proportion among the breakthrough cases should
be higher than among unvaccinated cases. Our results show that vaccinees that tested positive at least a week after the second dose
were indeed disproportionally infected with B.1.351, as compared with unvaccinated individuals (odds ratio of 8:1). Those who tested
positive between two weeks after the first dose and one week after the second dose, were disproportionally infected by B.1.1.7 (odds
ratio of 26:10), suggesting reduced vaccine effectiveness against both VOCs at particular time windows following vaccination. Nevertheless,
the B.1.351 incidence in Israel to-date remains low and vaccine effectiveness remains high among those fully vaccinated. These results
overall suggest that vaccine breakthrough infection may be more frequent with both VOCs, yet a combination of mass-vaccination with
two doses coupled with non-pharmaceutical interventions control and contain their spread. Competing Interest Statement
The authors have declared no competing interest.
Funding Statement
This study was supported by an ERC starting grant 852223 (RNAVirFitness), by an Israeli Science Foundation grant 3963/19, and
by kind donations from the Millner and AppFlyer foundations. This study was supported in part by fellowships to TK, NH, and SH from
the Edmond J. Safra Center for Bioinformatics at Tel-Aviv University.
Author Declarations
I confirm all relevant ethical guidelines have been followed, and any necessary IRB and/or ethics committee approvals have been
obtained.
Yes
The details of the IRB/oversight body that provided approval or exemption for the research described are given below:
The study was approved by the CHS institutional review board (IRB #0016-21-COM2) and was exempt from the requirement for informed
consent. The study was further approved by the Tel-Aviv University ethics committee (0002706-1).
All necessary patient/participant consent has been obtained and the appropriate institutional forms have been archived.
Yes
I understand that all clinical trials and any other prospective interventional studies must be registered with an ICMJE-approved
registry, such as ClinicalTrials.gov. I confirm that any such study reported in the manuscript has been registered and the trial
registration ID is provided (note: if posting a prospective study registered retrospectively, please provide a statement in the trial
ID field explaining why the study was not registered in advance).
Yes
I have followed all appropriate research reporting guidelines and uploaded the relevant EQUATOR Network research reporting checklist(s)
and other pertinent material as supplementary files, if applicable.
Yes
Notable quotes:
"... What remains to be seen is how long the mRNA stays viable, how it is down regulated and let us hope it is stable and not prone to telling the cell about something else to build. ..."
45North1 6 hours ago (Edited) 45North1 6 hours ago (Edited)
mRNA based vaccines are mis-named, they are a gene therapy, triggering the manufacture of
antigens to work on virus.
What remains to be seen is how long the mRNA stays viable, how it is down regulated and let
us hope it is stable and not prone to telling the cell about something else to build.
They could push this as an annual thing.
I would prefer the Sputnik V which is made to make the immune system do the work, and maybe
retain that memory for years (?).
https://sputnikvaccine.com/
Faeriedust 3 hours ago
It's true that most common cold coronaviruses only provide immunity for a year or two.
HOWEVER, there is significant cross-immunity between coronaviruses.
Meaning that if we can just get the PTB to drop this ridiculous charade of mandated masks,
blanket testing and partial shutdowns of everything from restaurants to government offices to
baseball games, we can get back to a NORMAL situation in which everyone gets exposed to some
kind of coronavirus disease several times a year, expanding and extending the cross-immunities
that made eighty percent of the population IMMUNE to Covid-19 when it first arrived.
Before this hysteria hit, medical science had begun to take its first baby-steps towards
admitting that humans are biological creatures that exist in a biological environment, in which
our relationships with many microbes are not merely harmless, but essential . To cut ourselves
off from the living world is to die. Sterility kills. Isolating ourselves from all potential
sources of infection inevitably destroys our ability to resist infection when we are finally
exposed . The last thing we need is a world of germ-free "bubbles". If we are to lead healthy
and wholesome lives, we need to reject the fundamental principles on which the worldwide
covid-19 response has been based. Look at Africa. They did nothing. They are healthy and
happy.
Bay Area Guy 4 hours ago remove link
These things are described as vaccines, but they aren’t. The not so fine
print says that they supposedly prevent recipients from getting serious cases of CoVid. (Tell
that to the 74 who died.). That shots will be needed every year was a foregone conclusion.
Anyone who thought differently was naive. There are enormous dollars to be made with a virus
that’s endemic. And with countries jumping on the vaccine passport
bandwagon, not just for travel, but for doing everyday things, Big Pharma is going to rake in
trillions from this.
Some scientists have used the term vaccine resistance haven't been
vaccinated.
When viruses replicate, Penn State biologist David Kennedy, PhD, explained in an interview,
the cycle is like a classic childhood game. "Viruses copying themselves, it's almost like a
game of telephone," said Kennedy, who studies pathogen evolution. "They repeat what they
thought they heard, so they make mistakes all the time."
Despite those many mistakes, Kennedy noted, he's unaware of any vaccines against viral
diseases other than seasonal flu that have had to be updated because of changes in the virus.
Hepatitis B virus developed " vaccine escape mutations ," but they posed
no health risks, he said.
Actually all vaccines carry a risk. The question is the risk is justified by the severity of the deases in question and prevalent
mortality.
Kartoschka , Apr 27 2021 12:33 utc |
24
Maschine translation from:https://www.anti-spiegel.ru/2021/die-profite-der-pharmakonzerne-sind-wichtiger-als-ein-schnelles-ende-des-lockdown/
Mao Cheng Ji , Apr 27 2021 15:33 utc |
31
There's a growing controversy in Hungary, where the government -- Hungarian government -- published stats for all the vaccines
they've been using.
Sputnik V shows the highest effectiveness and least side effects. Sinopharm -- the second best. Pfizer -- the worst.
https://hungarytoday.hu/hungary-vaccines-vaccine-effectiveness-inoculation-vaccine-effectiveness-comparison-pfizer-sputnik-sinopharm/
(I see hungarytoday.hu has already censored the government table out of the article.)
Immediately, a scandal ensued, with herds of righteous grant-eaters explaining why the government stats are not to be believed.
All in all, funny slapstick, I like it.
In a basic sense, there are two types of pressures that lead to mutations that allow the
virus to proliferate at a rate greater than its predecessor. Sometimes these advantages lead to
the emergence of a new dominant strain throughout a population.
The first one is the pressure to infect. A mutation occurs that allows the virus to more
reliably enter a host cell. In other words, the outer protein structure has changed to better
attach and go through a channel in the cell membrane. This type of mutation may be the
predominant mechanism that allows certain strains to spread more easily.
The second is the pressure to evade. A mutation occurs that allows the virus to dodge the
host immune system, a person’s own immune system fighting the virus. This
type of mutation gives rise to strains that can make the person more sick and a vaccine less
effective.
Mutations in the new coronavirus could reduce the effectiveness of vaccines against it. But
vaccines themselves can also drive viral mutations, depending on exactly how the shots are
deployed and how effective they are.
So far, vaccines still appear to work against the new strains â€" though
scientists are warily watching a variant that first appeared in South Africa since it seems to
reduce vaccine effectiveness. And evolution isn't standing still, so scientists realize they
may need to update vaccines to keep them working reliably.
What's going on here is somewhat similar to a larger, and more concerning problem in
medicine: Many bacteria have gradually evolved the ability to survive even when walloped by a
large dose of antibiotics. That problem has created new strains of deadly, drug-resistant
germs.
Viruses also evolve, but the process is different and the result is usually much less severe
when it comes to vaccines. When a virus such as the coronavirus infects someone, that
person's immune system mounts a response. Viruses produce slight variations when they multiply,
and if any of these variants can evade a person's immune response, those variants are more
likely to survive and possibly to spread to other people
Electro Static 6 hours ago
Snyder is not even close to understanding what is going on, but I will give him credit for
at least noticing how insane the mRNA experiments are - and bringing up money and big
pharma.
Here is a well-documented dose of reality for anyone interested in the truth -
https://childrenshealthdefense.org/defender/reasons-not-getting-covid-vaccine/?utm_source=salsa&eType=EmailBlastContent&eId=c2658670-8814-4b16-bf20-22cc0f01ddac
Good luck!
Notable quotes:
"... Remember how Oxford-AZ was going to offer the vaccine pro-bono and Billy Baphomet said they had to charge for it? Pfizer (with a big Black Rock stake) has tried repeatedly to take over AZ (similar BlackRock stake of around 8%) but has been rebuffed. I wouldn't be surprised if AZ is about to be humbled. ..."
"... Oligarchical collectivism is equally happy with fascism, communism or any other variety of state corporatism. Is this why the socialist/communist left has disappeared (it's redundant)? ..."
George Mc
This is gearing up to a money circus indeed. From the Graud:
"EU starts legal action against AstraZeneca over vaccine shortfalls
There will be the usual Left/ Right theatre with interminable wrangling over accusations of incompetence, corruption and a
more responsible system for allocating funds . all over a totally unnecessary and potentially lethal vax for a hyped up flu variant.
Moneycircus Corarden
Remember how Oxford-AZ was going to offer the vaccine pro-bono and Billy Baphomet said they had to charge for it? Pfizer
(with a big Black Rock stake) has tried repeatedly to take over AZ (similar BlackRock stake of around 8%) but has been
rebuffed. I wouldn't be surprised if AZ is about to be humbled.
There is no Department of Commerce, Securities and Exchange Commission, or Competition Commission -- effectively they've disappeared.
Monopoly is the order of the day.
Oligarchical collectivism is equally happy with fascism, communism or any other variety of state corporatism. Is this why
the socialist/communist left has disappeared (it's redundant)?
The recreation of IG Farben (including Bayer-Monsanto) which was a longstanding Rockefeller partner the green light to Amazon
dominance in retail the inevitably centralized nature of subsidized "Green" energy the social credit system implied by replacing
money with digital store credits the attempt to abolish individual self-determination in the interest of "keeping everybody safe"
the intention is clear as day.
acheron2016 10 hours ago
IF vaccines worked it shouldn't matter to a vaccinated person whether you have a
vaccination or not.
The entire "what about the poor wretch that is so ill he cannot survive a vaccine" is just
virtue signaling tripe. FIRST no person has a claim on your life. Period, the only exception
being your own children. And even that has finite limits.
The more truthful complaint is "I KNOW it is a scientific fact that flu vaccines are at
BEST 70%, and often closer to 40% effective. So I am afraid of my own shadow." This exposes a
risk aversion that has long since crossed over into the mental illness of full on
uncontrollable paranoia.
Let the person that is so sick they cannot be around other people self isolate. Let the
person that is so terrified they cannot function in society self isolate too!
The fake outrage and virtue signaling sociopaths have well and truly outlived the patience
of everyone on the planet that doesn't require psychotropic drugs to make it through the
day.
Highly recommended !Notable quotes:
"... "teachers abusing kids" ..."
"... " Pfizer and Moderna are both running clinical trials for their experimental mRNA shots on 11,000 children as young as six months old . Both trials began in mid-March. Moderna calls its study KidCOVE . Johnson & Johnson and AstraZeneca are also using children as guinea pigs . These companies have no moral fiber and are driven solely by profits. That is a given. But the parents are something beyond surreal." ..."
Jacques
"teachers abusing kids"
No shit. Yesterday, as I was driving from my hideaway up on the hill in the woods, I
caught a glimpse of a group of preschoolers coming out of the forest. I thought that they had
facemasks on, which I found preposterous, so I stopped, checked the rear-view mirror and
waited for them to come closer. Sure enough, they did have the fucking things on. Mind you,
it was a nice sunny day, the air fresh, the perfect April weather.
I went full postal and yelled at the teachers with just about all my might. They didn't
seem to give a shit. Maybe they're too afraid, like of "losing their job". Damn, in
retrospect, I should have addressed the kids and told them to tell the teachers to wipe their
ass with the stupid masks.
This is truly horrible, and I know what I'm talking about. I started school in 1970, a
short while after the Soviet invasion of Czechoslovakia in 1968. At a time when all hope was
crushed, when the purges started. When people were afraid of "losing their job", if not
worse. The teachers took out their fear, or perhaps anger, on us kids. Save for some, they
came hard on us children and passed on us the oppression inflicted on them by the regime. I,
as other kids, saw them as enemies and fought against them throughout my younger years. I was
only able to come out of that in university (on the other side of the world).
What the teachers are doing today is much worse. It's not just mindfuck, it physical
terror. They're taking party in asphyxiating the kids.
Disgusting
Corarden
Jacques
Very interesting observation born from real experience Jacques – that the oppressed
adults took it out on the children, focused it through their own lens onto their helpless
captives in a mirror image of the larger version of the cruelty and dehumanising process.
Horrible. Undeniable based on current events.
Arby
Corarden
"VAERS: Two-year-old baby in Virginia dead six days after second experimental Pfizer mRNA
shot"
" Pfizer and Moderna are both running clinical trials for their experimental mRNA
shots
on 11,000 children as young as six months old . Both trials began in mid-March. Moderna
calls its study KidCOVE . Johnson & Johnson and AstraZeneca are also
using children as guinea pigs . These companies have no moral fiber and are driven solely
by profits. That is a given. But the parents are something beyond surreal."
Peter
Arby
Sickening. Evil.
Corarden
NickM
Judge Christian Dettmar
" the children are not only endangered in their mental, physical and spiritual well-being
by the obligation to wear face masks during school hours and to keep their distance from each
other and from other persons, but, in addition, they are already being harmed. At the same
time, this violates numerous rights of the children and their parents under the law, the
constitution and international conventions. This applies in particular to the right to free
development of the personality and to physical integrity from Article 2 of the Basic Law as
well as to the right from Article 6 of the Basic Law to upbringing and care by the parents
(also with regard to measures for preventive health care and 'objects' to be carried by
children) "
As Reiner Fuellmich stated recently – 'They are coming after the children.'
opaopaopa 15 hours ago
15-Year-Old Boy Dies Of Heart Attack Two Days After Taking Pfizer Vaccine, Had No History Of
Allergic Reactions
https://nationalfile.com/15-year-old-boy-dies-of-heart-attack-two-days-after-taking-pfizer-vaccine-had-no-history-of-allergic-reactions/
Notable quotes:
"... If anyone had listened to Dr. Fauci or any of the mainstream press, they would think the vaccine is totally 100% safe. ..."
"... the Vaccine Adverse Event Reporting System, VAERS, would disagree with Dr. Fauci and the mainstream media. ..."
"... According to the most recent data from VAERS found on the CDC website , 3.018 people have been reported died after taking the COVID-19 Vaccine. These deaths constitute 64.45% of all vaccine deaths. So, not only have the COVID vaccines killed 3,018 people, but 6 in 10 recorded deaths from vaccines were from a COVID vaccine alone ..."
"... ABC News reports that 189.4 million flu vaccines were distributed in the 2020-2021 season. Of that, VAERS reports a grand total of 598 people have died from the vaccines. ..."
chubbar 5 hours ago
https://www.thewashingtongazette.com/2021/05/breaking-cdc-data-3018-people-reported.html?utm_source=greatawakening&utm_medium=social&utm_campaign=socialshare
If anyone had listened to Dr. Fauci or any of the mainstream press, they would think the vaccine is totally 100% safe. They
would think that anyone who says differently is a conspiracy theorist with enough tinfoil to build a radio antenna that would
reach the Andromeda Galaxy.
However, the Vaccine Adverse Event Reporting System, VAERS, would disagree with Dr. Fauci and the
mainstream media.
According to the most recent data from VAERS found on the CDC website
, 3.018 people have been reported died after taking the COVID-19 Vaccine. These deaths constitute 64.45% of all vaccine deaths.
So, not only have the COVID vaccines killed 3,018 people, but 6 in 10 recorded deaths from vaccines were from a COVID vaccine
alone :
But, some may say, that mortality rate is completely inline with any other vaccine. Well, not exactly. Right now,
roughly 1 in 2 people older
than 6 months of age have likely received a flu vaccine . However, according to the latest data,
43% of adults have received the first
COVID vaccine dose .
Breaking this down by data, ABC News reports that
189.4
million flu vaccines were distributed in the 2020-2021 season. Of that, VAERS reports a grand total of 598 people have died
from the vaccines.
So, considering more people have taken the Flu vaccine than a COVID vaccine, and far fewer people have died with a flu vaccine
than a COVID vaccine, it is not at all accurate to suggest the Coronavirus vaccine is as safe as a flu vaccine. The VAERS reporting
system says completely differently.
Granted, just because a report goes into VAERS, it doesn't mean that it has been fully investigated and confirmed, but the
CDC's webpage for VAERS says that it is a useful tool to provide
an early warning of safety problems with vaccines:
The strengths of VAERS are that it is national in scope and can quickly provide an early warning of a safety problem with a
vaccine. As part of CDC and FDA's multi-system approach to post-licensure vaccine safety monitoring, VAERS is designed to rapidly
detect unusual or unexpected patterns of adverse events, also known as "safety signals."
If a safety signal is found in VAERS,
further studies can be done in safety systems such as the CDC's Vaccine Safety Datalink (VSD) or the Clinical Immunization
Safety Assessment (CISA) project.
These systems do not have the same limitations as VAERS, and can better assess health risks
and possible connections between adverse events and a vaccine.
This is particularly alarming to say the least, since the COVID vaccine alone has been responsible for
120,000 adverse reactions in general, it would be a good idea to discuss getting the vaccine with your doctor to see if it
is the right choice for you."
QuiteShocking 5 hours ago remove link
We've probably already have herd immunity in many places..
Pfizer and BioNTech said they have asked European regulators to authorise their Covid-19
vaccine for those aged 12-15, a move seen as a crucial step towards achieving herd
immunity.
The companies already filed a similar request with US authorities earlier this month. Their
vaccine is currently only approved for use in people aged 16 and over.
In a joint statement released yesterday, Pfizer and BioNTech said they had submitted a
request with the Amsterdam-based European Medicines Agency (EMA) to expand the use of their jab
to include "adolescents 12 to 15 years of age".
Mr Ugur Sahin, co-founder and CEO of Germany's BioNTech, on Thursday said the jab could be
available for those age groups from next month if EU approval is granted.
The move comes after Phase 3 trial data showed the vaccine provided "robust antibody
responses" and was 100 per cent effective in warding off the disease among those aged 12 to 15.
"The vaccine also was generally well tolerated," the statement added.
In an interview with Der Spiegel weekly, Mr Sahin said he expected regulators' evaluation of
the data to take four to six weeks.
If approved, the green light would apply to all 27 European Union member states.
No coronavirus vaccines are currently authorised for use on children.
While children and teenagers are less likely to develop severe Covid-19 symptoms, they make
up a large part of the population and inoculating them is considered key to ending the
pandemic.
The prospect of getting older children jabbed before the next school year begins would also
ease the strain on parents who are juggling the demands of homeschooling while keeping up with
jobs.
"It's very important to enable children a return to their normal school lives and allow them
to meet with family and friends," Mr Sahin told Spiegel.
BioNTech and Pfizer are also racing to get their jab approved for younger kids, from six
months upwards.
"In July, the first results for five- to 12-year-olds could be available, and those for
younger children in September," Mr Sahin said.
Ongoing trials so far are "very encouraging", he added, suggesting that "children are very
well protected by the vaccine".
The BioNTech/Pfizer shot is based on mRNA technology and was the first Covid-19 jab to be
approved in the West late last year
MORE ON THIS TOPIC
Inoculating children is a
key step toward herd immunity , health officials say.
The Pfizer
-BioNTech vaccine is currently authorized in the U.S. for people 16 years and older. The
companies have asked U.S. health regulators to authorize the vaccine for people 12 years and
older. Mr. Zients said if the FDA authorizes Pfizer's vaccine for adolescents, the
administration will have "both a robust plan and sufficient supply" to administer those
shots.
Shots from Moderna
Inc. and Johnson &
Johnson are authorized in the U.S. for people 18 years and older. Both companies are
testing their vaccines in adolescents.
Mr. Biden's senior Covid-19 advisers say they are reaching out to pediatricians, citing them
as "an important point of trust" who can help encourage parents to vaccinate their children
once shots are approved. The administration hopes children in high school will be vaccinated
going into the fall school year.
Many school districts are still providing hybrid in-person and remote learning, though some
of the largest districts across the country plan to fully reopen in the fall for in-person
instruction.
Estimates have differed on how much of the population would need to be vaccinated to stop
the virus from circulating, but many health experts are using
70% to 80% as a goal . As of Thursday, 52% of adults in the U.S. had gotten at least one
dose of a vaccine, according to the Centers for Disease Control and Prevention. That proportion
ranged from 72% in New Hampshire to 39% in Mississippi.
Podcaster Joe Rogan has become a target of critics on social media after saying he believes
young and healthy people likely don't need Covid-19 vaccines and even opined that inoculating
children is "crazy."
Rogan quickly began trending on social media on Tuesday after a recent clip from his
podcast, 'The Joe Rogan Experience,' prompted critics to accuse him of spreading Covid-19
disinformation and feeding into vaccine hesitancy.
In fact, Rogan said on his show that he believes getting vaccinated is "safe" for
most people – before he argued that not everyone has to get a jab.
ALSO ON RT.COM
Trans MMA fighter Fallon Fox wants 'transphobic' Joe Rogan podcast canceled
"I think for the most part, it's safe to get vaccinated. I do. But if you're like
21-years-old and you say to me, 'should I get vaccinated?' I'll go no," Rogan said in the
clip, first posted by a journalist for the left-wing Media Matters.
The podcaster went on to argue that a healthy person who exercises regularly, eats well, and
has no health conditions that weaken their immune system likely "don't need to worry about
this."
The group Rogan believes should not be subjected to vaccines at all is children, revealing
his own two kids both got Covid-19 and claiming that in the end, "it was nothing."
Adding that he is not "diminishing" that children have died from the virus, Rogan
blasted people who are pushing for children to be vaccinated when most are far less vulnerable
to the virus than adults.
"You should be vaccinated if you're vulnerable," Rogan said.
https://platform.twitter.com/embed/Tweet.html?creatorScreenName=RT_com&dnt=false&embedId=twitter-widget-0&features=eyJ0ZndfZXhwZXJpbWVudHNfY29va2llX2V4cGlyYXRpb24iOnsiYnVja2V0IjoxMjA5NjAwLCJ2ZXJzaW9uIjpudWxsfSwidGZ3X2hvcml6b25fdHdlZXRfZW1iZWRfOTU1NSI6eyJidWNrZXQiOiJodGUiLCJ2ZXJzaW9uIjpudWxsfX0%3D&frame=false&hideCard=false&hideThread=false&id=1387077145156063234&lang=en&origin=https%3A%2F%2Fwww.rt.com%2Fusa%2F522299-joe-rogan-covid-vaccine-young%2F&sessionId=cfb7f43994ff371ba15ad73758c93b12674bf41a&siteScreenName=RT_com&theme=light&widgetsVersion=82e1070%3A1619632193066&width=550px
Rogan's vaccine opinion has gotten him once again on the firing line against liberal
critics. The former 'Fear Factor' host has become a frequent target since his podcast
exclusively moved to Spotify and quickly became the network's most popular show. He's been
criticized for everything from his views on trans women in sports to his openness to interviews
with controversial figures such as Alex Jones.
https://platform.twitter.com/embed/Tweet.html?creatorScreenName=RT_com&dnt=false&embedId=twitter-widget-1&features=eyJ0ZndfZXhwZXJpbWVudHNfY29va2llX2V4cGlyYXRpb24iOnsiYnVja2V0IjoxMjA5NjAwLCJ2ZXJzaW9uIjpudWxsfSwidGZ3X2hvcml6b25fdHdlZXRfZW1iZWRfOTU1NSI6eyJidWNrZXQiOiJodGUiLCJ2ZXJzaW9uIjpudWxsfX0%3D&frame=false&hideCard=true&hideThread=false&id=1387077952588992513&lang=en&origin=https%3A%2F%2Fwww.rt.com%2Fusa%2F522299-joe-rogan-covid-vaccine-young%2F&sessionId=cfb7f43994ff371ba15ad73758c93b12674bf41a&siteScreenName=RT_com&theme=light&widgetsVersion=82e1070%3A1619632193066&width=550px
https://platform.twitter.com/embed/Tweet.html?creatorScreenName=RT_com&dnt=false&embedId=twitter-widget-2&features=eyJ0ZndfZXhwZXJpbWVudHNfY29va2llX2V4cGlyYXRpb24iOnsiYnVja2V0IjoxMjA5NjAwLCJ2ZXJzaW9uIjpudWxsfSwidGZ3X2hvcml6b25fdHdlZXRfZW1iZWRfOTU1NSI6eyJidWNrZXQiOiJodGUiLCJ2ZXJzaW9uIjpudWxsfX0%3D&frame=false&hideCard=true&hideThread=false&id=1387103977016217600&lang=en&origin=https%3A%2F%2Fwww.rt.com%2Fusa%2F522299-joe-rogan-covid-vaccine-young%2F&sessionId=cfb7f43994ff371ba15ad73758c93b12674bf41a&siteScreenName=RT_com&theme=light&widgetsVersion=82e1070%3A1619632193066&width=550px
https://platform.twitter.com/embed/Tweet.html?creatorScreenName=RT_com&dnt=false&embedId=twitter-widget-3&features=eyJ0ZndfZXhwZXJpbWVudHNfY29va2llX2V4cGlyYXRpb24iOnsiYnVja2V0IjoxMjA5NjAwLCJ2ZXJzaW9uIjpudWxsfSwidGZ3X2hvcml6b25fdHdlZXRfZW1iZWRfOTU1NSI6eyJidWNrZXQiOiJodGUiLCJ2ZXJzaW9uIjpudWxsfX0%3D&frame=false&hideCard=false&hideThread=false&id=1387109100366884867&lang=en&origin=https%3A%2F%2Fwww.rt.com%2Fusa%2F522299-joe-rogan-covid-vaccine-young%2F&sessionId=cfb7f43994ff371ba15ad73758c93b12674bf41a&siteScreenName=RT_com&theme=light&widgetsVersion=82e1070%3A1619632193066&width=550px
Others also criticized Spotify, which has even seen employees protest the hiring of Rogan
since the platform went into business with him in what was reportedly a $100 million
contract.
https://platform.twitter.com/embed/Tweet.html?creatorScreenName=RT_com&dnt=false&embedId=twitter-widget-4&features=eyJ0ZndfZXhwZXJpbWVudHNfY29va2llX2V4cGlyYXRpb24iOnsiYnVja2V0IjoxMjA5NjAwLCJ2ZXJzaW9uIjpudWxsfSwidGZ3X2hvcml6b25fdHdlZXRfZW1iZWRfOTU1NSI6eyJidWNrZXQiOiJodGUiLCJ2ZXJzaW9uIjpudWxsfX0%3D&frame=false&hideCard=false&hideThread=false&id=1387113274932617222&lang=en&origin=https%3A%2F%2Fwww.rt.com%2Fusa%2F522299-joe-rogan-covid-vaccine-young%2F&sessionId=cfb7f43994ff371ba15ad73758c93b12674bf41a&siteScreenName=RT_com&theme=light&widgetsVersion=82e1070%3A1619632193066&width=550px
https://platform.twitter.com/embed/Tweet.html?creatorScreenName=RT_com&dnt=false&embedId=twitter-widget-5&features=eyJ0ZndfZXhwZXJpbWVudHNfY29va2llX2V4cGlyYXRpb24iOnsiYnVja2V0IjoxMjA5NjAwLCJ2ZXJzaW9uIjpudWxsfSwidGZ3X2hvcml6b25fdHdlZXRfZW1iZWRfOTU1NSI6eyJidWNrZXQiOiJodGUiLCJ2ZXJzaW9uIjpudWxsfX0%3D&frame=false&hideCard=false&hideThread=false&id=1387112626128293892&lang=en&origin=https%3A%2F%2Fwww.rt.com%2Fusa%2F522299-joe-rogan-covid-vaccine-young%2F&sessionId=cfb7f43994ff371ba15ad73758c93b12674bf41a&siteScreenName=RT_com&theme=light&widgetsVersion=82e1070%3A1619632193066&width=550px
While Rogan cited his own experience with his children when criticizing mass vaccinations,
kids and even younger adults are also statistically far less vulnerable to the virus than older
people. According to data from the Centers for Disease
Control and Prevention (CDC), people under 45 account for less than 3% of the Covid-19 deaths
in the US. The highest is 65 and older, which covers over 80%.
Comorbidities – underlying conditions that weaken the immune system, such as diabetes
and hypertension – are also frequent among the hundreds of thousands of patients who have
died from the virus.
There are currently no vaccines on the market authorized for anyone under 16 to take.
Pfizer's vaccine is approved for patients 16 and older, while Moderna has been approved for
people 18 and over.
ALSO ON RT.COM West
Virginia governor says he'll pay young people $100 savings bonds for getting Covid vaccine,
gets bribery accusations
During another episode of his podcast this year, Rogan revealed he is not planning on
getting a vaccine himself. Asked whether he would get the vaccine when available, he replied,
"no. I mean I would if I felt like I needed it."
Like this story? Share it with a friend!
The Pfizer vaccine could cause
severe neurodegenerative
diseases caused by brain prions created by the mRNA-style vaccine. National File reported, "'The current RNA based SARSCoV-2
vaccines were approved in the US using an emergency order without extensive long term safety testing,' the report declares. 'In this
paper the Pfizer COVID-19 vaccine was evaluated for the potential to induce prion-based disease in vaccine recipients.' Prion-based
diseases are, according to the CDC, a form of neurodegenerative diseases, meaning that the Pfizer vaccine is potentially likely to
cause long term damage and negative health effects with regards to the brain."
In a shocking new
report on the COVID-19 vaccines, it has been discovered that the Pfizer coronavirus vaccine
may have long term health effects not previously disclosed, including “ALS,
Alzheimer's, and other neurological degenerative diseases.â€
“The current RNA based SARSCoV-2 vaccines were approved in the US using an
emergency order without extensive long term safety testing,†the report declares.
“In this paper the Pfizer COVID-19 vaccine was evaluated for the potential to
induce prion-based disease in vaccine recipients.†Prion-based diseases are,
according to the CDC, a form of neurodegenerative diseases, meaning that the Pfizer vaccine is
potentially likely to cause long term damage and negative health effects with regards to the
brain.
This is especially concerning since the Pfizer vaccine is an mRNA vaccine, an untested type
of vaccine which creates new proteins and can actually integrate into the human genome , according to
a report from the National Library of Medicine. In other words, degenerative brain conditions
may appear at any time in your life after receiving the vaccine.
“The RNA sequence of the vaccine as well as the spike protein target
interaction were analyzed for the potential to convert intracellular RNA binding proteins TAR
DNA binding protein (TDP-43) and Fused in Sarcoma (FUS) into their pathologic prion
conformations,†explains the report. TDP-43 is a protein known to cause dementia,
ALS and even Alzheimer's, according to Alzpedia . Similarly, the FUS protein is known
to cause ALS and Hereditary Essential Tremors, according to the Human Genome Database .
The experiment done for the report was to determine whether or not these two harmful
proteins embed themselves into our DNA, as an mRNA vaccine is expected to do. The report
determined that “the vaccine RNA has specific sequences that may induce
TDP-43 and FUS to fold into their pathologic prion confirmations,†meaning that
both proteins have the potential to embed themselves into our DNA and cause harmful
neurological diseases.
The report's abstract summary concludes that “The
enclosed finding as well as additional potential risks leads the author to believe that
regulatory approval of the RNA based vaccines for SARS-CoV-2 was premature and that the vaccine
may cause much more harm than benefit.†The report itself ends with this warning:
“The vaccine could be a bioweapon and even more dangerous than the original
infection.â€
National File actually reached out to the CDC to inquire as to why the Pfizer vaccine is
still being distributed despite these credible allegations. No response was received prior to
publication.
Pfizer CEO Albert Bourla said people will “likely†need a
third dose of a Covid-19 vaccine within 12 months of getting fully vaccinated. His comments
were made public Thursday but were taped April 1.
Bourla said it’s possible people will need to get vaccinated against the
coronavirus annually.
From the very beginning of this crisis, I have been warning my readers that any immunity would
be very temporary.
Natural COVID immunity is very temporary, and immunity conferred by the vaccines is very
temporary too.
The CEO of Pfizer is comparing the COVID vaccines to flu shots. Every year millions of
Americans rush out to get their flu shots, and the CEO of Pfizer is admitting that it looks like
the COVID vaccines will be on a similar schedule
…
“There are vaccines that’s like polio that one dose is
enough, there are vaccines like pneumococcal vaccine that one dose is enough for adults and
there are vaccines like flu that you need every year,†Bourla said.
“The Covid virus looks more like the influenza virus than the polio
virus.â€
If people are going to need a new shot every year, that means that COVID will be with us for a
very long time to come.
This is essentially an admission that the COVID pandemic will not be ending any time soon.
Needless to say, Pfizer stands to make giant mountains of money if COVID vaccines become a
yearly thing, and we need to keep that in mind.
A lot of people that I know are going to be extremely upset when they finally realize that the
two shots that they got only provide temporary immunity.
And of course lots of people are still getting sick after being fully vaccinated. According to
the CDC, so far there have been almost 6,000 documented cases of people being infected after
getting two shots, and dozens of them
have died …
The Centers for Disease Control (CDC) has reported that roughly 5,800 people who received a
coronavirus vaccine still ultimately came down with the disease anyway, according to CNN.
Of those 5,800, 396 of them (roughly 7 percent) were hospitalized; 74 of the vaccinated
people ultimately died. The report proves that the vaccines, though frequently touted by the
government and the media, are not guaranteed to prevent everyone from contracting the
virus.
That wasn’t supposed to happen.
But it is happening.
Meanwhile, there is a lot of uncertainty about how the current vaccines will fare against
variants that have already developed and variants that will develop in the future.
At this point we just don’t know how effective the vaccines will be, but
the New York Times
is assuring us that we don’t have anything to be concerned
about…
“I use the term
‘scariants,’†said Dr. Eric Topol, professor
of molecular medicine at Scripps Research in La Jolla, Calif., referring to much of the media
coverage of the variants.
“Even my wife was saying, ‘What about this double
mutant?’ It drives me nuts. People are scared unnecessarily. If
you’re fully vaccinated, two weeks post dose, you
shouldn’t have to worry about variants at all.â€
Really?
I have a feeling that Dr. Eric Topol will end up eating those words.
The reason why a new flu vaccine comes out every year is because the flu is constantly
changing and mutating.
The same thing is happening to COVID, and there are already dozens of mutant variations
spreading around the globe.
To me, Dr. Eric Topol’s statement was exceedingly irresponsible, especially
considering some of the studies that have come out lately. Here is just one example
…
Two doses of the AstraZeneca Covid-19 vaccine were found to have only a 10.4% efficacy
against mild-to-moderate infections caused by the B.1.351 South Africa variant, according to a
phase 1b-2 clinical trial published
on Tuesday in the New England Journal of Medicine . This is a cause for grave concern as the
South African variants share similar mutations to the other variants leaving those vaccinated
with the AstraZeneca vaccine potentially exposed to multiple variants.
In this article, I haven’t even discussed all of the side effects that we
have been witnessing. A few days ago, the FDA issued an unprecedented order regarding the Johnson
and Johnson vaccine because it was
causing blood clots in a number of cases…
This week, the Food and Drug Administration called for a halt in the administration of the
single dose vaccine for COVID-19 manufactured by Johnson and Johnson. The halt was ascribed to
the rare incidence of blood clots that could potentially be related to the vaccine.
I am glad that the FDA decided to step in, but the order came too late
for this guy …
When the news broke about the pause of the Johnson & Johnson vaccine Tuesday, one Coast
family was already living with a tragedy they believe was caused by the vaccine.
It started out as a normal day for 43-year-old Brad Malagarie of St. Martin. This busy
father of seven spent the morning at his D’Iberville office before heading
to get a Johnson & Johnson vaccine a little after noon.
He returned to work, and within three hours coworkers noticed he was unresponsive at his
desk.
It shouldn’t be controversial to say that rushing experimental vaccines
through the testing process was a really bad idea.
We should be putting the safety of the American people first, and nobody knows for sure what
the long-term effects of these experimental treatments will be.
In this day and age, we all need to do our own research and we all need to think for
ourselves, because the big pharmaceutical companies are more concerned with profits than anything
else.
If you are harmed by their experimental therapies, the big pharmaceutical companies
won’t be there to pick up the pieces for you if something goes horribly
wrong.
* * *
Michael’s new book entitled “Lost Prophecies Of The
Future Of America†is now available in paperback and for the
Kindle on Amazon.
So...
Requiring Vaccine IDs or passports violates medical privacy - Right?
Unvaccinated are NOT a threat because the vaccinated are protected - Right?
Preventing unvaccinated from participating in society is discrimination - Right?
_arrow
The Antisoiler 5 hours ago remove link
It appears they are moving in the direction of mandating a vaccine subscription, where you
will pay monthly or yearly.
Trends indicate subscription based revenue generation is a win-win for both producer,
consumer, and eugenicist.
Remember, you will own nothing and be happy about it. You will be free from the burden of
asset management. And, you'll essentially be a slave, working till you drop into a grave or
incinerator.
Fed Supporter 6 hours ago remove link
Sorry Michael Snyder, you are flat out wrong about natural immunity not lasting very
long.
A corona virus from 17 years ago, every year those who were infected get tested for
immunity, and guess what every year for 17 year those previously infected individuals still
have immunity.
Further, the current corona virus , Covid, is 80% similiar to the one from 17 years ago.
Some virologits estimate that 30% of the world has cross immunity and can not get Covid.
Sorry to burst your bubble, but you need to do more research. You are parroting the MSM
outlets who were selling fear and citing quacks from stanford, etc that said "we just don't
know", No they do know they just wanted to ramp fear sky high. Memory T cells are a thing.
see
Antibody that inhibits the new coronavirus discovered in ...
https://www.livescience.com ›
sars-antibody-inhibits-ne...
May 18, 2020 â€" Blood samples from the patient, who had SARS in 2003, contained
an ... Antibody that inhibits the new coronavirus discovered in patient who had SARS 17 years
ago ... Antibodies form part of the body's immune response to pathogens. ... But Vir
Biotechnology has fast-tracked the antibody for development ...
https://www.nature.com/articles/s41586-020-2550-z
Here we studied T cell responses against the structural (nucleocapsid (N) protein) and
non-structural (NSP7 and NSP13 of ORF1 ) regions of SARS-CoV-2 in individuals convalescing from
coronavirus disease 2019 (COVID-19) ( n = 36). In all of these individuals, we found CD4 and
CD8 T cells that recognized multiple regions of the N protein. Next, we showed that patients (
n = 23) who recovered from SARS (the disease associated with SARS-CoV infection) possess
long-lasting memory T cells that are reactive to the N protein of SARS-CoV 17 years after the
outbreak of SARS in 2003; these T cells displayed robust cross-reactivity to the N protein of
SARS-CoV-2. We also detected SARS-CoV-2-specific T cells in individuals with no history of
SARS, COVID-19 or contact with individuals who had SARS and/or COVID-19 ( n = 37).
SARS-CoV-2-specific T cells in uninfected donors exhibited a, etc.
Fed Supporter 6 hours ago
BTW natural immunity is way better than Mrna vaccines, which are narrowly tailored to target
proteins on the spike protein. Once it mutates, like the South Africa and UK mutations, the
pfizer vaccine will need modified to target the new mutations hence yearly boosters at $180 a
pop. We will be chasing this thing forever, always behind on catching the mutated viruses.
Invest in Pfizer their stock will go so high, they are going to make a ton of money off the
sheep.
Also, some doctors, said it is not wise to get vaccinated for corvid if you already had
it.
Also isn't peculiar the mutations all occurred in countries that ran human trials, Brazil,
UK, SA, Israel. These countries were the first to have humans vaccinated and they are the first
to have mutations.
Bacon's Rebellion 4 hours ago
"Just look at the number of medicines pulled from pharmacies in the last 20 years that the
FDC originally said were perfectly safe"
Think for yourself 4 hours ago (Edited) remove link
also, the mRNA vaccine 'targets' the s-proteins by genetically hijacking your cell to
construct biochemical factories to create these s-proteins. Not only is it a fixed overhead (no
off switch, it's in your genes now) but that overhead is spent building parts that are designed
to inflame your immune system. Even after so-called 'immunity' is acquired, those biochemical
factories will keep working to produce, the immune system will keep working against the
low-level inflammation, so the cells will not only be spending fuel on negative output, but the
spare viral proteins floating around it's creating are just begging to be assimilated into even
more mutant strains.
I am convinced that the mRNA 'vaccine' is exponentially increasing the mutation potential of
covid-19.
Libertarian777 5 hours ago
THIS GUY GETS IT. Lack of antibodies does not mean immunity disappears.
Pazuzu 4 hours ago
Upvoted for clever use of term 'virologits'. If ever there were a bunch of gits the virology
bunch fits the bill.
Josey Yahoo 6 hours ago remove link
Is anybody else stating to feel like they are being played?
For a year now I have been saying that this is a flu, just another flu, being blown into a
major issue to literally destroy our nation.
First the lockdowns, to destroy small business, as the large companies will gladly assist in
the elimination of cash. NOTE, the immediate calls for cash not to be used as it would transmit
the virus, then all of a sudden a coin shortage, when was the last time that happened, oh,
that's right, NEVER!
....
freedommusic 4 hours ago (Edited)
> Huh? Unvaccinated are a threat to other Unvaccinated people who want to get vaccinated
and don't want to die.
No problem that's what your double mask, self isolating, and social distancing is for. Since
it is SO EFFECTIVE , it will provide the necessary protection until all the smart people get
vaccinated.
Then all the unwashed, ignorant, unvaccinated fools will die off as a result of natural
selection.
Everyone wins here and nature wins.
RIGHT?
taketheredpill 6 hours ago
Or maybe the vaccine is 99.9925% Effective (6000 sick out of 80 Million with full dose) and
Pharma guys rounded up?
Bacon's Rebellion 6 hours ago (Edited) remove link
ummm.
Assuming 100% accuracy of the "cause of death" being Covid19:
Covid19 survival rates for all age groups:
Covid19 survival rates over the age of 75:
Covid19 survival rates under the age of 55:
Covid19 survival rates under the age of 25:
Explain to us why in the world we need to vaccinate the 16 to 25 folks? Vaccination DOES NOT
MEAN you can't catch it or spread it...
"" We don't know yet whether or not it prevents you from getting infected where you're not
with symptoms...but you have virus in your nasopharynx that you could then infect an
unvaccinated person who might be vulnerable, and you will inadvertently and innocently get them
sick," Fauci explained."
The whole vaccine jive talk is packed with "Could", "Maybe", "Possibly", "Likely",
"Unknown"...ect.
https://www.cdc.gov/nchs/covid19/index.htm
Bacon's Rebellion 5 hours ago (Edited)
"UNLESS....you get people to lock down, wash hands, wear masks etc."
Yeah, we did that, and we have 31,000,000 confirmed cases.
How many people contracted Covid19 but were never tested?
Estimating the Fraction of Unreported COVID-19
So, at 6 unreported for every reported, more than half of the US population has been
exposed...your masks and lockdowns have been a huge failure....
186,000,000 infections and 563,000 dead = .3% death rate.
University of Chicago
Fed Supporter 5 hours ago remove link
Bacon, don't confuse taketheredpill with facts, his mind is already made. I'll bet he is a
paid sock puppet or just some sick liberal trolling one of the few places post comments that
make sense, and that aren't a bunch of collectivist mindless sheep.
russellthetreeman PREMIUM 6 hours ago
It's not a vaccine. It doesn't even come close to halfway meeting the definition of a
vaccine.
It's not a pandemic. It doesn't even come close to halfway meeting the definition of a
pandemic.
The sars cov 2 virus has a known survival rate of WELL over 99+%.
sun tzu 6 hours ago remove link
The average sheep thinks over 30 million Americans died of covid-19 last year. Idiocy
rules
A Lunatic 6 hours ago (Edited)
That still pales in comparison to the 150 million gun deaths we had last year, according to
Joe.
Bacon's Rebellion 5 hours ago
"It's not a vaccine"...correct, it's a drug that forces your immune system to do something
it doesn't want to do.
The original mRNA researcher when it actually, sorta, worked "I felt like God!"
NYTimes
baja canada 6 hours ago remove link
All BS. My wife and I are unvaccinated and have travelled half the country, always maskless,
over the past year. Not sick, haven’t been sick. Our dog is fine, too.
sun tzu 6 hours ago
Same here. I've been to Mexico 3 times too. Nobody around me, family and co-workers, has
gotten sick or died.
Lead Engineer PREMIUM 6 hours ago
And the CDC estimates that over 30% of the population has been infected. So if we assume
that another 20% had previous natural immunity and another 50% of the susceptible have been
vaccinated, then you can see that this pandemic is rapidly going extinct.
Captive1 6 hours ago (Edited) remove link
" From the very beginning of this crisis, I have been warning my readers that any immunity
would be very temporary. Natural COVID immunity is very temporary, and immunity conferred by
the vaccines is very temporary too."
Disqualifying statement. There is no data to support this statement. Antibody surveillance
studies have shown durability and case studies have demonstrated no reinfections to those who
had an initial antibody response on the first infection. Not to mention T Cell memory. He
doesn't know what he's talking about. Immune memory to COV2 is long lived and protective across
multiple strains. I would link the papers but I'm not helping people not be retarded anymore.
Big pharma wants you to believe that immunity is temporary to drive profit. It's not.
Huxley's Ghost 6 hours ago remove link
We know so little about the immune system (really the entire human body); basic concepts,
yes but effect of environment, innate experience, stressors, diet, etc..not a clue. Individual
immune systems because of all these factors are more like fingerprints--vastly unique to each
unit. The endocrine and immune systems are black boxes to the medical community but they act
like are doing more than spit-balling.
Huxley's Ghost 5 hours ago remove link
In theory, they (vaccine companies) annually analyze what strains are prevalent in the world
and predicted to have the greatest impact. Those strains get selected for production of the
annual flu shot; it could be the case that the same strain(s) prevailed. Or not. These days you
can't believe anything anymore.
Last time I had the flu shot was over 30 years ago. I had flu once since then and took
Tamiflu, which was miraculous in its speed (identify and dose early while viral load is low) of
effect, minimal/no side effects, and efficacy. I was back on my feet in about 36 hours--fully.
I have heard people report horrible abdominal/GI issues (temporary). I was lucky.
strych10 3 hours ago remove link
OK, I've said this before but I will repeat it, ultra basic here:
Natural immunity tends to be both "deeper" and "broader" than what one of these mRNA
(straight up or adeno vector, doesn't matter) can provide.
When a virus infects you there are a lot of different things that happen. The two that
matter the most for the purposes of this discussion are as follows:
1) Your body sees a wide array of viral surface proteins and gets a look at the actual
capsid and lipid envelope too. Particularly after you immune system shreds up some of the
buggers and looks at the pieces.
2) Your body gets to see millions of variations on this, including the most statistically
common variations in surface protein structure.
This means that your body develops a set of antibodies that is much wider than a single
introduced protein can provide.
With the vax you get one structure, lab controlled QC, a single "image" of the target if you
will. In the wild you get a bunch of various proteins and a ton of variation in their physical
shape, hundreds or thousands of images from various angles.
The result is that you get a relatively wide array of antibodies and a hugely wider picture
of what is "not self". This makes it easier for your body to recognize the same or similar
infectious agent/infection next time. You also now have a set of antibodies with variable
structure making it more likely that they can neutralize a mutant strain of the same virus (or
something substantially similar) or at least blunt the next virus' attack long enough to buy
time for your immune system to learn about it without you getting a serious illness.
duck_fur 2 hours ago
You seem to have a background in virology. What of the issue of coding errors - either
during or after manufacture - within the mRNA payload? What of the possibility of the expressed
protein exhibiting a fold due to the error(s)?
strych10 1 hour ago
I'm not a virologist. I'm a cell biologist.
So, trying not to make this a full on basic genetics class...
Yes, what you're asking is possible. It's also statistically rare. The root of misformed
proteins tends to be genetic code error or a mistake in copying that code into mRNA.
Ribosomes, which translate mRNA into a protein, tend to be very good at their job and if
they make an error can often detect it, back up and fix it and then begin sequencing again.
Errors do occur but they're rare. At this stage more common is an issue of improper folding of
the protein resulting in an improper tertiary structure and the inability to form a quaternary
structure due to this. (A quaternary structure is an overall structure formed by multiple
proteins folded to fit together into a larger unit which serves a purpose. For example,
hemoglobin is formed from four separate proteins that fold up and then can fit together to form
hemoglobin.)
So, assuming that the QC is good, which I have no reason to believe that it is not, coding
errors are not really a problem. It's the fact that the QC is too good.
But then you have to step back and ask if this matters. Yes and no, and I'll give you a
quick explanation of each.
An antibody is, essentially, like a Y of gum you're sticking on the key to a lock. The virus
has a key that unlocks the cell, the antibody prevents these two things from coming into
physical contact so the key can never open the lock. Once bound this antibody also marks
whatever it has bound to for destruction by other parts of the immune system. That in
mind...
Yes: If CoV-2 were to mutate to the point that the spike proteins in question changed enough
that an antibody couldn't bind to the virion then the virus could evade the antibodies that
neutralize the virion and mark it for destruction.
No: In order to do this, generally, you need quite a bit of mutation to change the physical
structure of the spike. In a lot of cases this would make the virion non-operational because
the same change that allows it to avoid the antibodies also means it can no longer fit that key
into the desired lock.
So, does it really matter? Again, yes and no. If the virus can "figure out" a key that still
opens the desired lock (or another one) and doesn't fit the antibody it will avoid the immune
system until the immune system figures out what's going on. This takes some time. Infected
cells have to signal that they're infected, inspection has to be done, antibodies synthesized
etc.
So, IMHO, and it's just my opinion: the fear of "breakthrough" is rather overblown. However,
it is still real. In a natural infection there is less chance of this kind of "breakthrough"
because your body has more data on the invader meaning that the invader usually needs to change
a lot more in order to evade the immune system hence "broader" and "deeper". That said, there
are viruses that are pretty good at this. Influenza A is one of them.
This is the root of what you may have heard last year about "T-cell immunity". People had
previously encountered a disease substantially similar to CoV-2 and it was similar enough that
they produced an antibody that neutralized CoV-2.
Quasimodo. 48 minutes ago remove link
If you have breakthrough, you have a new virus. A mutation, not just a variant. Most
variants have only slight changes in protein. A variant is more likely to spread and be more
virulant if it is less deadly since the host survives long enough to spread the virus further,
while a deadlier form (although could happen) will die out quickly as more hosts will die
strych10 15 minutes ago
I actually had to ask my wife about the technical definition about this.
For CoV-2 to change enough to be "not CoV-2" it would require significantly more alteration
than you're stating here.
The things that would change the classification are things like capsid shape, nucleic acid
type, mechanism of infiltration or exfiltration.
You need far more than simply the ability to evade current immune response. Hence why
Influenza A can jump species, come back and still be Influenza A.
Codery 1 hour ago
Ya but that’s just like science, can you explain how any of that helps
get rid of Trump?
strych10 1 hour ago remove link
Yes, in three letters. CNN.
sun tzu 6 hours ago remove link
Stay away from big hospitals. They are contract killers for big pharma
Sluggo315 3 hours ago
My older brother that has three or four co-morbidities (weight, BP, asthma, one more I
think) was rushed to the hospital for a bowel blockage. He spent the night in the emergency
room, and was admitted into the hospital for tests. They put him on the COVID floor. Tell me
these hospitals are not in on it too!!!?
TheTruthisSomewhere 5 hours ago remove link
The article unfortunately is going from the erroneous position that this is worse than the
flu. It is not the statistics are cooked and it is a testdemic. Variants are always less potent
and yes people have natural immunity to this. It is almost a Gaslighting article based on quasi
facts and hearsay.
Joe Rogan: "I think it's safe to get vaccinated, but if you're 21 years old ... if you're a
healthy person and you're exercising all of the time and you're young and you're eating well, I
don't think you need to worry about this." https://twitter.com/i/status/1387077145156063234
And Fauci response: "You have to put a little bit of societal responsibility in your choices,
and that's where I disagree with Mr. Rogan." https://twitter.com/i/status/1387414298432000000
It is unclear how Fauci response correlates with the fact that existing vaccines are less
effective or (in case of Pfizer and South African strain) ineffective against new mutations. Does
he acts as Big Pharma lobbyist, or what ?
Also, you have to be skeptical of pharmaceutical companies and the fact that they cannot be
sued if something goes wrong with the vaccine.
White House
health adviser Dr. Anthony Fauci and communications director Kate Bedingfield have made a point
of belittling and attacking podcaster Joe Rogan for daring to have a mixed opinion on Covid-19
vaccines.
As Rogan has skyrocketed over the years to arguably the most influential and successful
podcaster around, he has also turned into an intensely controversial figure, mainly for
liberals who fear his willingness to give a platform to right-wing figures like Alex Jones and
his less-than-PC takes on everything from transgender athletes to Covid-19 vaccines.
The latter is what landed the former 'Fear Factor' host in the hot seat this week as a clip
from a recent episode of 'The Joe Rogan Experience' made its way across social media and
critics painted Rogan as an anti-vaxxer spreading disinformation.
The controversy stems from Rogan saying, during a conversation with fellow comic Dave
Smith, he would not recommend that a healthy person in their early 20s get a Covid-19 vaccine
as they are not as vulnerable to the virus as older generations (who account for the majority of Covid
deaths in the US) and people with preexisting medical conditions.
The Spotify podcaster also said pushing for kids to be vaccinated is "crazy," citing his
own childrens' history with getting Covid-19, as both recovered relatively quickly.
Critics painted Rogan's comments as an angry anti-vaxx rant, urging his millions of
listeners to avoid getting inoculated against Covid-19. However, they ignored the fact that
Rogan says in the clip (and has said in the past) that getting vaccinated seems mostly safe
and is indeed "important" for certain people.
Criticism of Rogan reached a bizarre new level on Wednesday when the White House appeared to
launch a coordinated effort to disparage and belittle the podcaster, completely dismissing his
opinions.
In multiple interviews, Fauci blasted Rogan for ignoring "societal responsibilities,"
arguing even young and healthy people should get vaccinated as asymptomatic individuals can
still spread the virus.
The infectious disease expert also believes "kids of all ages" will be vaccinated by the
end of the year – there are no vaccines on the market in the US approved for anyone under
16 – and everyone should "absolutely" get inoculated.
ALSO ON RT.COM Rose McGowan tells
Democrats they are in a cult, and their whining, defensive responses prove her right
Bedingfield also dismissed Rogan's opinion in a CNN interview where she said Rogan not being
a doctor basically strips his words of any merit.
"I guess my first question would be, did Joe Rogan become a medical doctor while we
weren't looking?" she asked. "I'm not sure that taking scientific and medical advice
from Joe Rogan is perhaps the most productive way for people to get their information."
Initial social media criticism of Rogan is one thing, but the White House pitting themselves
against a private citizen having an open and frank discussion on a podcast is concerning. It's
alarming enough that White House officials busy with vaccination efforts and a still-fresh
administration would take the time to debate Rogan on the subject, but the responses to his
discussion also show that administration officials are fearful of open debate and conversations
about the vaccines. If one even strays from the belief that vaccines are 100% safe and every
single person, regardless of age or health, should take them, they are attacked, at least if
you have the following that Rogan has.
Rogan's discussions on Covid-19 vaccines do not boil down to a debate on whether getting
inoculated against the virus is good for everyone or not. The recent viral clip even opens with
the podcaster saying vaccines are safe, and he acknowledges that what he says about children
and young, healthy people is not true across the board. He merely expresses concerns as a
father and gives a personal opinion that in no way discourages everyone from getting a
vaccine.
Looking at Fauci and Bedingfield's responses, it appears they aren't even debating what
Rogan actually said.
Fauci, who has been a controversial figure himself and
accused of flip-flopping multiple positions during the pandemic, argues that it is the
potential transmission of the virus from one person to another that is the reason everyone
should be vaccinated. Rogan never talks about the risk of transmission though. He simply makes
the argument that a healthy individual who is younger may not need a vaccination to protect
themselves from the deadlier aspects of Covid.
Bedingfield's argument is even lamer as she says without a "Dr." title, Rogan simply
can't have concerns about vaccinations for children and others. She argues no one should take
"medical advice" from a podcaster, setting Rogan up as a man who presented himself as
some kind of expert on vaccines, dishing out advice to his listeners, who apparently aren't
intelligent enough to make up their own minds, according to these critics.
Fauci and Bedingfield and any other White House official who decides to paint Rogan as the
face of anti-vaxxers should be ashamed of themselves. Their personal attacks are an
opportunistic way to take a shot at someone who has somehow become a near-pariah on the left,
and to discourage open and frank discussions about vaccines. Their swift dismissal of a
comedian who is not quite waving the flag for every single person to be vaccinated shows that
they don't want discussion from citizens they want compliance and for people to keep nodding
their heads at their ever-changing talking points and guidelines.
It really doesn't matter who is right in the White House versus Joe Rogan debate because
there shouldn't be a White House versus Joe Rogan debate. Ironically, Fauci and Bedingfield
have probably made more people aware of Rogan's comments by addressing them. They and other
officials have taken questionable criticism of a fairly harmless conversation and used it to
create a false narrative about one man to strike fear into anyone who would dare consider what
he or anyone else would say above what they do.
If you like this story, share it with a friend!
Notable quotes:
"... CEO of Pfizer, Albert Bourla is a veterinarian! ..."
"... CEO runs a business, not scientific R&D! Pfizer has thousands of employees to do the R&D work. ..."
heehaw2 2 hours ago
CEO of Pfizer, Albert Bourla is a veterinarian! Ha ha ha. Franci depends on this guy to give
out experiment mRNA treatments to humans...what a total joke
AGuy 2 hours ago
CEO runs a business, not scientific R&D! Pfizer has thousands of employees to do the
R&D work.
That's said, I don't have much faith in the vaccines. I think efficiency will drop over time
requiring frequent booster shots as well as virus strains that render the current vaccine
useless. Time will tell.
Notable quotes:
"... In the hard-hit state of Maharashtra, the double mutant has already become the dominant strain, according to Dr. Anurag Agrawal, director of the CSIR Institute of Genomics and Integrative Biology. In samples collected in the state from January to March, over 60% were of the double-mutant variant, according to a study by the National Institute of Virology in Pune ..."
"... That research could inform future vaccine development, especially booster shots that will target particular variants of Covid-19, Dr. Pinsky said. ..."
...The Indian variant has 13 mutations, but gets its name from two mutations similar to those seen separately in other variants.
In other variants, one mutation is associated with making the virus more infectious and appears better at evading antibodies, while
the other is similar to one that has shown signs of being able to sidestep some of the body’s immune responses.
It was first discovered in India in a sample collected in October, said Dr. Rakesh Mishra, director of the CSIR Centre for Cellular
and Molecular Biology, which operates one of the 10 state-run labs charged with genomic sequencing of the virus. Recent data points
to its rapid spread through some regions of India.
In the hard-hit state of Maharashtra, the double mutant has already become the dominant strain, according to Dr. Anurag Agrawal,
director of the CSIR Institute of Genomics and Integrative Biology. In samples collected in the state from January to March, over
60% were of the double-mutant variant, according to a study by the National Institute of Virology in Pune
For the country overall, this variant made up 70.4% of the samples collected during the week ended March 25, compared with 16.1%
just three weeks earlier, according to Covid CG, a tracking tool from the Broad Institute of MIT and Harvard. The tool uses data
from the GISAID Initiative, a global database for coronavirus genomes.
... The virus has already hopped to at least 21 countries, according to researchers at four universities that track viral lineages.
Genetic sequencing has turned up cases in the U.S., Germany, Turkey and Nigeria, among others. In the U.K, genome sequencers have
found the variant among people who haven’t traveled, suggesting it has spread within the community.
... In California, at least 20 confirmed or presumptive cases of the double mutant have been discovered since late March, according
to Dr. Benjamin Pinsky, director of Clinical Virology Laboratory at Stanford University. Dr. Pinsky said samples have already been
sent to collaborators at other laboratories, where research is under way to test how the virus reacts to monoclonal antibodies and
plasmas from infected or vaccinated people.
That research could inform future vaccine development, especially booster shots that will target particular variants of Covid-19,
Dr. Pinsky said.
Many young people are now falling ill and showing up at hospitals with severe symptoms, doctors and public-health experts said.
In this surge, people age 26 to 44 account for about 40% of total cases and 10% of deaths, Dr. Kant said, compared with the previous
wave, when almost all of the deaths were those aged 60 and above.
norecovery , Apr 23 2021 16:19 utc |
12
It's no wonder there's "hesitancy" among the public about vaccination. Sputnik News has a revealing article on Pfizer's push
to compete while downplaying the safety of their experimental treatment --
https://sputniknews.com/world/202104231082693859-is-pfizer-quietly-targeting-other-vaccines-while-holding-back-on-its-own-safety-record-/
Note one of the qualifiers in the death stats: "(3) No clear link between vaccinations and deaths has been found to date" --
it appears these public health agencies have set a high bar for causation in order to obfuscate the truth.
Mina , Apr 23 2021 16:40 utc |
13
Another lie used by the Western governments is the claim about the need for 'herd immunity' via vaccination and the aim of
70% of a population.
Mina , Apr 23 2021 16:53 utc |
15
https://www.youtube.com/watch?v=pyPjAfNNA-U
oldhippie , Apr 23 2021 18:11 utc |
17
Mina @ 13
When smallpox was extincted the WHO goal was 80% vaccination. Not achieved anywhere. Smallpox is gone.
The ‘vaccine’ does not make anyone immune. It creates antibodies that circulate in bloodstream. It is an airborne respiratory
disease. Inside surface of lungs is principal locus of infection. There is no blood on inner surface of lung and thus no antibodies.
The blood is close enough to the lung surface for exchange of O2 and CO2, the larger antibody molecule remains in the capillary.
The epithelial cells lining the lung become infected with no resistance from any ‘vaccine’ related antibody. If the antibody
is useful it will be much later in course of disease.
This is why vaccines for airborne diseases have always been difficult, unreliable. Suddenly, under political pressure, all
sorts of non-possible things are claimed. Or inferred and suggested.
We have no idea how far along herd immunity might be. No one is looking. Anyone who wants to investigate herd immunity is a
political enemy. The sort of testing that would be required Is possible, can be done, has been done, is relatively slow and difficult.
Would need big grants from political bodies. When this all started survivors of SARS-COVID One (from 2003-2005) were asked to
give blood. When that blood was exposed to samples of SARS-COVID2 t-cells remembered just what to do, immediately identified the
2 virus as a familiar antigen and ripped it apart. After fifteen years the t-cells still knew what to do. The One virus is only
80% similar to the 2 virus. Herd immunity will happen. Nothing is being done that will make that come any sooner.
lizzie dw , Apr 23 2021 18:53 utc |
18
I have read enough articles about the side effects of these "vaccines" to think that the countries denied the opportunity to
be injected should almost be thanking their lucky stars. What is even more remiss, IMO, is that no one anywhere is being apprised
of the NEEd for adequate Vit. D levels to combat the virus, nor of at least 2 of the relatively cheap and available therapeutics
that can be given in a protocol including other medications/vitamins (hydroxchloroquine and ivermectin).
john swinburne , Apr 23 2021 19:12 utc |
20
The Ugly Truth About The Covid-19 Lockdowns: https://www.pandata.org/time-to-reopen-society/
Christian J. Chuba says:
April
16, 2021 at 2:35 pm
"Putin critics cite Sputnik V vaccine debacle as attempt to further divide Europe"
This is one of those stories where it is a good mental exercise to try to extract the facts scattered in the layers of BS.
It was just incredible. So here is my summary.
Part 1: the facts
Russia delivered 200,000 doses of Sputnik V gratis to Slovakia with a contract to deliver 2M more doses. The US/NATO agents
busted a gasket, replaced the prime minister and prevented Slovakia from using any of the vaccines. They even refused to return
the 200,000 doses so that Russia could use them somewhere else.
Part 2: the hysterical wailing
Evil Putin is using a divide and conquer strategy to try to destroy Europe but NATO vigilance prevented the Slovakians from
being poisoned by this defective product and foiled the local Russian collaborators. Russia is eagerly peddling Sputnik V because
it is the first new export item they have developed since the end of the Cold War [I don't know I thought Novichok was pretty
good]. India is reconsidering their purchase because the Russians are also selling it to Pakistan (??????? wtf is that supposed
to mean?????)
I can't believe an article like this got past any editor, is there a point where people in the U.S. will catch onto the
fact that they are reading complete nonsense?
Yeah, Right says:
April
17, 2021 at 8:01 am
Novichok is a Soviet-era family of (apparently) non-lethal super-lethal supremely-dangerous nerve agents that you can safely
carry around in a perfume bottle even though it is applied as a gel on a door-nob.
Or in a water bottle. Whatever. I've lost track. Was it sprinkled on someone's underpants, or was that last week's explanation?
But definitely not developed for the post-cold war export market.
I do like the "fact" that the Slovakians are complaining that the State Institute for Drug Control doesn't know the details
of the contract signed with Russia.
Ahem. There is now a new government.
So the institutions of state can solve that particular puzzle by opening the filing cabinet in the Prime Ministers Office and
having a sticky-beak inside.
Perhaps Matovic took the key with him when he vacated the office?
Notable quotes:
"... Science now means refusing to know anything but the narrative. There is just no way we shall know how bad a problem the vaccine is. My supposition that the son-in-law's problems are connected to vaccine could be pure ex post facto rubbish. We shall never know because we refuse to look. ..."
Oldhippie , Apr 25 2021 14:40 utc |
12
Covid-19 Vaccine Thrombosis:
Regarding the three articles posted on covid and thrombosis.
The first article, the NEJM article, reports six younger patients died of thrombosis,
presumably cerebral venous thrombosis. Although the article is so poorly written it is hard
to even know. Patients were in "Germany and Austria" but past that all we have is lab test
reports. Not even clear if the authors ever saw the patients. Cerebral venous thrombosis is
extremely rare in younger patients. The article does make the Astra Zeneca jab the cause of
death, obscuring that by referring to it as ChAdOx1 -Covid-19
Second article is basically "nothing to see here" plus "Look! -- - A squirrel!!!" And
would be entirely dismissed but for the third article, from Gamaleya Center which basically
says "You filthy swine! You inject your citizens with raw sewage and then act surprised you
have problems."
The son-in-law has had a series of cardiac problems. Following his vaccination. Doctors
tell him the vaccination is entirely safe, absolutely no reported cardiac or circulatory
problems reported anywhere. And any who say otherwise are conspiracy theorists he should quit
listening to. Making NEJM conspiracy theorists.
Science now means refusing to know anything
but the narrative. There is just no way we shall know how bad a problem the vaccine is. My
supposition that the son-in-law's problems are connected to vaccine could be pure ex post
facto rubbish. We shall never know because we refuse to look.
Notable quotes:
"... Also registered in Israel, Pfizer vaccine caused more deaths only in Israel than even AstraZeneca in whole Europe.. ..."
Lelush , Apr 25 2021 13:24 utc |
5
On the Pandemic front and vaccines...
Yesterday there was a multitudinary demonstration in London against pandemic measures and mainly against implementation of
"vaccination passports" not reported by the media, not even the alt-media...
Also there were these past days huge demonstrations in Germany agsint Special Pandemic Powers Laws, currently being signed
thorughout the whole EU without people´s knowledge nor escrutiny...
Increasingly are appearing unknown vaccines side effects, as cardiologic ones and effects on menstrual cycle...
Also registered in Israel, Pfizer vaccine caused more deaths only in Israel than even AstraZeneca in whole Europe..
Then this is the vaccine currently monopolizing EU strategy of vaccination through lobbyist like Thierry breton, responsible
for EU internal market, The European Council of Foreign Relations ( which labels the Russian vaccine as a risk on EU health security,
and pressures coming from the US DoS...
Anyway, the risk of suffering a blood clot with AstraZeneca has doubled in 15 days...and Boris Johnson has already announced
that Covid-19 vaccines will not end the pandemic and that "new" meds will be needed to counter next highly likely next fall coming
waves...in spite of alleged British succes with vaccines...
https://www.dailymail.co.uk/news/article-9491869/Coronavirus-Britain-pills-treat-Covid-autumn.html
It is a matter of time that the EU citizenry becomes aware that there are spurious interests in blocking EU acess to safe,
efficient and cheap vaccines while promoting dangerous ones as a single possiblity which not only offer more risk thatn benefits
but also will not provide any kind of immunity, in the best case they prived a slight protection against serious Covid-19 infection.
Lelush , Apr 25 2021 13:41 utc |
6
Who are those profitting from the vaccines...and why there is a war on vaccines, as this is a mutibillion business with no
end in sight, as the pandemic will be eternal by design..
Taking into account who are the main shareholders, one is prone to think that this is the way some countries have decided they
will capitalize their accute debt crisis, by looting from others, as always...
https://mundo.sputniknews.com/20210423/quienes-son-los-duenos-de-las-vacunas-privadas-y-como-se-estan-enriqueciendo-1111506444.html
Also, how is that Moderna registered the patent of its vaccine already in September, past year, when the pandemic was not even
declared yet, not even in China...????
https://twitter.com/aaronyokheved/status/1386015618009272329
Lelush , Apr 25 2021 13:58 utc |
7
A resistance movement against the "new pandemic fascist world order" in surging in Europe.
Images of yesterday greatest in recent history demonstration so far in UK against lockdowns, masks, "vaccine passports" and
authoritarian measures on this pandemic alibi..
https://twitter.com/InfoNewsABC/status/1385979583791501318
Also, a resistance movement has surged in France on initiative of artists, philosophers, intellectuals and fed up people who
usually think on the arbitrariness and absurdity of certain pandemic measures especially outdoors...with a song "Danser Encore"
rising a new resistance hymn...
https://www.youtube.com/watch?v=SyBEMRyt6Qg&ab_channel=HKsaltimbank
It is going viral...
https://www.youtube.com/watch?v=PIQvsOja_30&ab_channel=Journall%27Humanit%C3%A9
German version by Die Box....
https://www.youtube.com/watch?v=phrCiosJB-Q&ab_channel=DIEBOX
Spanish version...
https://www.youtube.com/watch?v=HlT-vwnIAEk&ab_channel=ElenadelValle
Italian version...
https://www.youtube.com/watch?v=L_b_PLfxugM&ab_channel=StefanManderioli
jared , Apr 25 2021 14:17 utc |
8
Regarding the virus and vaccine -- On z/h was a posting claiming that in US, there is poor correlation between states enforcing
stricter measures and states having better outcomes. Difficult to assess because they play very loose with the died of covid assessment.
I suspect this is valid as I dont see the pandaphiles pointing finger at florida texas with any effect.
- It has been noted that the promoters of the pandemic seem to have very low confidence in performance of the vacine as they
propose to continue strict control measures.
- Institutions are requiring vacination and signing of release - requiring people to accept medical treatment with a vaccine
which is not approved by FDA. Frightening on many levels.
Very troubling.
Notable quotes:
"... Science Mag ..."
Covid-19 Vaccine Thrombosis:
THE GAMALEYA CENTER STATEMENT
A comprehensive analysis of adverse events during clinical trials and over the course of
mass vaccinations with the Sputnik V vaccine showed that there were no cases of cerebral venous
sinus thrombosis (CVST).
All vaccines based on adenoviral vector platform are different and not directly comparable.
In particular, AstraZeneca’s ChAdOx1-S vaccine uses chimpanzee adenovirus to
deliver the antigen, consisting of S-protein combined with leader sequence of tissue-type
plasminogen activator. The vaccine from Johnson&Johnson uses human adenovirus serotype Ad26
and full-length S-protein stabilized by mutations. In addition, it is produced using the PER.C6
cell line (embryonic retinal cells), which is not widely represented among other registered
products.
Sputnik V is a two-component vaccine in which adenovirus serotypes 5 and 26 are used. A
fragment of tissue-type plasminogen activator is not used, and the antigen insert is an
unmodified full-length S-protein. Sputnik V vaccine is produced with the HEK293 cell line,
which has long been safely used for the production of biotechnological products.
Thus, all of the above vaccines based on adenoviral vectors have significant differences in
their structure and production technology. Therefore, there is no reason and no justification
to extrapolate safety data from one vaccine to safety data from other vaccines.
The quality and safety of Sputnik V are, among other things, assured by the fact that,
unlike other vaccines, it uses a 4-stage purification technology that includes two stages of
chromatography and two stages of tangential flow filtration. This purification technology helps
to obtain a highly purified product that goes through mandatory control including the analysis
of free DNA presence. In addition, the volume of nucleic acid is several dozen times lower in
adenoviral vectors compared to Pfizer and Moderna vaccines (1 to 2 mcg vs 50 to 100 mcg,
correspondingly).
A study published in The New England Journal of Medicine on April 9, 2021, discusses that
the cause of the thrombosis in some patients vaccinated with other vaccines could be
insufficient purification that leads to the emergence of significant quantities of free DNA.
Insufficient purification or use of very high doses of target DNA/RNA can result in adverse
interaction of a patient’s antibodies that activate thrombocytes with
elements of the vaccine itself and/or free DNA/RNA, which can form a complex with the PF4
factor.
Link to the study:
https://www.nejm.org/doi/full/10.1056/NEJMoa2104840?query=featured_home
The Gamaleya Center is ready to share its purification technology with other vaccine
producers in order to help them minimize the risk of adverse effects during
vaccination.
Highly recommended !Notable quotes:
"... He had a total loss of his platelets -- the little blood cells that stop bleeding. In spite of being treated by a team of physicians, he died two weeks later from a brain hemorrhage, and was reported to have had zero platelets . ..."
"... What happened to this physician and the others seems to be a new previously unseen problem related to vaccination -- despite the manufacturers' claims. ..."
"... Increasingly, vaccine manufacturers and government officials are following the sarcastic maxim from Samuel Shem's novel of medical residency entitled The House of God that "if you don't take a temperature you can't find a fever." In other words, if we don't critically look at the actual recorded patient damage, we won't find our products to be defective. ..."
"... Moreover, a vaccine is supposed to prevent disease. By that definition, these agents are not even vaccines. They are more properly termed "experimental unapproved genetic agents." By admission of the manufacturers themselves, both the Pfizer and Moderna products only lessen the symptoms of COVID; they don't prevent transmission. ..."
Many Americans have heard the news account of Dr. Gregory Michael, a 56-year-old Florida physician who, after receiving his first
dose of a Pfizer COVID vaccine on December 18 of last year, was hospitalized three days later. He had a total loss of his platelets
-- the little blood cells that stop bleeding. In spite of being treated by a team of physicians, he died two weeks later from a brain
hemorrhage, and was reported to have had zero platelets .
By February 10, 2021, 36 other similar cases were reported in the mainstream media. Pfizer, which along with its partner BioNTech
made the vaccine the doctor received, said in a statement that it was aware of the death. Typically, they concluded, "We are actively
investigating this case, but we don't believe at this time that there is any direct connection to the vaccine."
Pfizer made this "finding" despite several unusual circumstances of the case. First, low-platelet disorders, known as idiopathic
thrombocytopenic purpura (ITP), most commonly affect children, and generally follow a viral illness. Only 10 percent of ITP cases
occur in adults, who usually present with a slow onset form of the disorder, referred to as chronic ITP. The disorder usually starts
by someone noticing easy bleeding, such as slow oozing from gums or the nose, or bruises showing up without trauma. Rarely do platelets
drop below 20,000, and generally treatment either reverses the disease or prolongs life for years in spite of the problem.
What happened to this physician and the others seems to be a new previously unseen problem related to vaccination -- despite
the manufacturers' claims.
Increasingly, vaccine manufacturers and government officials are following the sarcastic maxim from Samuel Shem's novel of
medical residency entitled The House of God that "if you don't take a temperature you can't find a fever." In other words,
if we don't critically look at the actual recorded patient damage, we won't find our products to be defective. Now, major media
are increasingly getting on board, condemning "vaccine hesitancy" and pushing everyone to get vaccinated for COVID, discounting any
dangers. But in the practice of medicine, we are supposed to employ the "precautionary principle" -- above all do no harm.
Moderna and Pfizer COVID-19 "vaccines" are experimental, employing a genetic technology never before used on humans. Ironically,
many people who wouldn't purchase the first edition of a new car line are lining up to take an injection they know nothing about,
that has never successfully passed animal trials, that could never meet the required "safety level" for a "drug," and is unapproved
for the prevention of COVID except as an emergency experiment .
Legally, those who get the vaccine are unnamed participants in a Stage IV FDA trial.
Moreover, a vaccine is supposed to prevent disease. By that definition, these agents are not even vaccines. They are more
properly termed "experimental unapproved genetic agents." By admission of the manufacturers themselves, both the Pfizer and Moderna
products only lessen the symptoms of COVID; they don't prevent transmission.
Vaccination was first invented to treat smallpox, which had a a fatality rate of up to 60 percent. Then other diseases such as
typhoid and polio were similarly addressed. But vaccination is not used when effective safe treatment is available. Although censorship
has confused the public understanding, overwhelming evidence dating back to the 1970s shows that viruses can be treated with "lysosomotropic
agents." The truth is, hundreds of papers have shown that chloroquine, and its later version hydroxychloroquine, are very effective
in treating this virus if given early. A worldwide open architecture online review of COVID survival (hcqtrial.com) showed that death
rate was 78.7-percent lower in those countries where hydroxychloroquine was used early and often:
Multiple large studies done in outpatient settings show very excellent prevention and cure with these and other drugs such as
Ivermectin. In Mumbai, India, a study was done of the city police force of 10,000 officers. No deaths were recorded in the 4,600
officers taking a small dose of hydroxychloroquine each week. All the deaths were in the untreated group. Using Worldometer statistics,
COVID deaths per capita in New York State are 2,656 per million population; in New Jersey they are 2,821 per million population.
In India the rate is 126 per million and in Uganda it is only seven per million. Neither India nor Uganda used social distancing
in any real way. But they do use hydroxychloroquine. New York (except for Dr. Zev Zelenko and a few others) does not use the drug.
As to the claims of the efficacy of the drugs, the declaration of 95-percent effectiveness of the Pfizer product was shown to
be bunkum by Dr. Peter Doshi, the associate editor of the British Medical Journal , writing in that publication. After doing
an independent review of the data submitted to the FDA, Dr. Doshi reported that only 30 percent of test subjects, at best, experienced
even the slightest benefit (symptom reduction). Absolute risk reduction -- in other words stopping transmission -- he estimated at
less than one percent.
The limited benefit of taking the drugs is made worse by the relatively high death tolls from the new mRNA therapy. During the
first two months of the rollout of Pfizer and Moderna "vaccines" in 2021, 95 percent of deaths from vaccines recorded in the Vaccine
Adverse Event Reporting System (VAERS) were for those agents, meaning only five percent of reported deaths involved all the other
vaccines put together. Compared to 2019, deaths in VAERS are up 6,000 percent. Thirty-six deaths were recorded in the first quarter
of 2020 versus 1,754 in the first quarter of 2021.
In Israel, where the Pfizer mRNA product is being used exclusively and a major push is on to vaccinate the whole population, an
independent review of government data after two months of the vaccine program was done by the Aix-Marseille University Faculty of
Medicine Emerging Infectious and Tropical Diseases Unit's Dr. Herv� Seligmann and engineer Haim Yativ. They showed that when 12.5
percent of Israelis were vaccinated, 51 percent of the deaths from COVID were in the vaccinated group. Additionally, in the
over 65-year-olds, vaccination resulted in death from COVID 40 times more than in unvaccinated people. In other words, this
is not protecting people from COVID but increasing fatalities from the disease -- and this neglects the number of other side effects.
If the truth were known, most sane, thinking people would not likely take part in such an experiment. With the truth hidden and
with threats of travel bans and an unwarranted fear of COVID, and with pressure from employers and the politicization of COVID in
general, Americans have been throwing caution to the wind.
The Unknowns
To understand what is actually happening to people after receiving the mRNA agents, I reviewed data in VAERS -- an open-source
searchable database of possible vaccine side effects reported by both providers and patients. According to the CDC website:
VAERS is used to detect possible safety problems -- called "signals" -- that may be related to vaccination. If a vaccine safety
signal is identified through VAERS, scientists may conduct further studies to find out if the signal represents an actual risk.
The main goals of VAERS are to:
� Detect new, unusual, or rare adverse events that happen after vaccination.
� Monitor increases in known side effects, like arm soreness where a shot was given
� Identify potential patient risk factors for particular types of health problems related to vaccines
� Assess the safety of newly licensed vaccines
� Watch for unexpected or unusual patterns in adverse event reports
� Serve as a monitoring system in public health emergencies
The CDC acknowledges limitations of the system, including:
� Reports submitted to VAERS often lack details and sometimes contain errors.
◦ Serious adverse events are more likely to be reported than mild side effects.
◦ It is generally not possible to find out from VAERS data if a vaccine caused the adverse event.
I searched the VAERS database using keywords that would identify bleeding problems and thrombocytopenia (low or absent platelets).
Entries are defined by age groups and sex with a narrative account of the injury.
In a two-and-a-half-month period from December 15, 2020 to March 12, 2021, 358 cases of unusual clotting or bleeding were identified,
and it makes grim reading. There were 104 cases of frank thrombocytopenia (low platelets) -- some including young people. However,
the numbers alone do not adequately convey the problems. In one case about an 18-29 year-old female, the physician wrote this: "Patient
was seen in in my office on 1/19/21 with complaint of heavy vaginal bleeding. A CBC was obtained which revealed an H/H of 12.2/36.1
and a platelet count of 1 (not 1K, but 1 platelet!) This was confirmed on smear review." The surprise and horror the doctor experienced
upon seeing the absence of platelets is clear when reading the report.
But the platelet problem may just be the most severe expression of a physical derangement that is producing bleeding of all sorts.
As seen in the table below, there were 49 people with brain hemorrhages -- nine fatal at the time of reporting. A number of other
people arrived at Emergency Departments with bleeding from multiple sites, or internally, so massive that they could not be stabilized
even to clearly define the sources of the bleeding.
Severe Thrombocytopenia
94
Various Spontaneous Skin bleeding
10
Mild Thrombocytopenia
11
Vein bleeding from temple
1
Thrombocytopenic Petechial rash/bruising
5
Prolonged surgical site bleeding
3
Severe Pancytopenia
2
Severe multifocal bleeding
5
Unknown Hematologic Problem
1
Severe internal bleeding
5
Multifocal or "massive" brain hemorrhage
20
Severe uncharacterized bleeding
3
Focal brain hemorrhage
29
Bleeding from cancer site liver
1
GI Bleed
34
Renal dialysis shunt
1
Severe Vaginal Bleeding
7
Hematuria
2
Vaginal Bleeding
21
Renal bleed
1
Bleeding in Pregnancy
6
Tonsillar bleed
1
Bleeding with Miscarriage
12
Acute Uterine Fibroid hemorrhage
1
Irreg Menses
4
Nosebleed
32
Oral bleeding
8
Spontaneous Splenic hemorrhage
1
Subconjunctival Hemorrhage
11
Injection Site Bleeding
21
Intraocular bleed
4
Arm Bruising
1
Most cases of severe problems were in people over the age of 50 years. But there were many younger people involved, especially
in the less severe-but-unusual bleeding problems. Of the 36 reported nosebleeds, six were either unable to be stopped with usual
measures, were recurrent, or were recorded as having significant blood loss or dubbed "profuse." Many were associated with other
symptoms: photophobia (eye sensitivity to light), headache, hives, "sick in bed," brain fog, and face swelling. The youngest patient
with a nosebleed was, sadly, a toddler requiring emergency care. Unusual skin bleeding was also reported. Four 65-plus-year-old males
reported blood spontaneously oozing through the skin: one from the legs, one from the scalp, one from an old biopsy site, and one
from an old healed "boil" site. Frank bleeding at the time of the inoculation occurred 14 times. Some bleeding was momentary, but
often the bleeding was difficult to stop, recurrent, and/or persisted after the patient returned home. (How many times have you had
an injection and bled at all, let alone bled off and on for hours?)
Perhaps the saddest were the bleeding episodes that preceded spontaneous miscarriages. Here are some direct entries in VAERS:
40-49 y.o. Female: The evening of my vaccination I began to feel feverish, weak and achy. During the night I woke with heavy
bleeding and found out the following morning I had miscarried my otherwise healthy pregnancy.
39 y.o. Female: Internal brain bleeding 10 days after 1st dose Covid vaccine; brain damage, confused, suffering memory loss;
This is a spontaneous report from a contactable physician (patient).
30-39 y.o. Female: 48 hours after injection developed micro-hemorrhages in her right eye. Symptoms resolved and 12/29 recurrence
of bleeding to right eye slightly worse than before
65+ y.o. Male: Patient developed significant nose bleed after receiving vaccine. Required emergency department visits x 2 and
hospitalization.
65+ y.o. Female: Vaccine administered 02/02/2021. By Thursday 2/11/2021 patient almost nonverbal, by Monday 2/15/2021 patient
went to the hospital with bruising, sores on her stomach and clots reported as thrombocytopenia. Deceased by Friday, 2/19/20201.
40-49 y.o. Female: Bleeding, myalgia, tingling in the fingers of the right hand; fatigue immediately upon vaccination -- bleeding
at the injection site which the employee reports as filling the Band-Aid over the site. When she got home in the evening and took
it off blood ran.
65+ y.o. Female: Within 15 min of the injection, the individual became aphasic and stroke like symptoms. She was taken to the
ER where she was later diagnosed with a cerebral hemorrhage and passed away.
When such facts are presented, the standard retort from vaccine advocates is, "We have given millions of vaccines, so a few deaths
are to be expected." Besides the fact that a willingness to sacrifice individuals for the nebulous good of the masses represents
a bankrupt moral order, simply calculating the numbers of deaths is inadequate. "Experts" need to take the time to read the narrative
to open their eyes -- and their hearts -- to the suffering happening. There are over 25 pages of such stories printed from VAERS
entries, and we must consider, "How many of these people are now dead, and how many are going to die?"
A second-year medical student armed with the facts should recognize looming disaster -- where are the experts?
In truth, neither recipients nor their doctors know what is in these "vaccines." Only a few people at the top of the Moderna,
Pfizer, Johnson & Johnson, and AstraZeneca research groups really understand them. These mRNA injections produce a potentially deadly
pathogen -- the spike protein -- in your cells.
The Emergency Use Authorization for the Pfizer product says that it contains "a nucleoside-modified messenger RNA (modRNA) encoding
the viral spike glycoprotein (S) of SARS-CoV-2." If your immune system is strong enough to withstand this onslaught and create some
immunity, you may survive the first onslaught. But even if you don't die in the short term, mRNA is an epigenetic controller of
DNA . Though this foreign synthetic mRNA doesn't actually become part of your DNA to make you a "GMO human," as some people have
been worrying about, it can control DNA in ways we have yet to completely understand . We literally have no idea whether this
bodily additive is going to have a side effect of expressing cancer genes, or of repressing cancer protective genes, or thousands
of other potentially deadly unknowns.
Additionally, the Pfizer vaccine includes all types of ingredients that may by themselves create ailments. The Pfizer shot
contains "lipids ((4-hydroxybutyl)azanediyl)bis(hexane-6,1-diyl)bis(2- hexyldecanoate), 2-[(polyethylene glycol)-2000]-N,N-ditetradecylacetamide,
1,2-distearoyl-snglycero-3-phosphocholine, and cholesterol), potassium chloride, monobasic potassium phosphate, sodium chloride,
dibasic sodium phosphate dihydrate, and sucrose."
I insert this list just for completeness -- don't expect to make sense of it. Your doctor can't either. I understand "sucrose"
(sugar) and sodium chloride (salt), but who doesn't get lost in the "hydroxybutyl" and "distearoyl" lipid list?
After doing some sleuthing and having some inside knowledge to start from, I discovered that this lipid particle is an adjuvant
called "Matrix M." As described in scientific literature, "Adjuvant Matrix-M� is comprised of 40 nm nanoparticles composed of
Quillaja saponins , cholesterol and phospholipid."
Matrix-M essentially wraps the mRNA in a lipid coating that allows it to move through cell walls and to linger in your system.
Matrix-M is derived from plant chemicals called saponins, which have poorly understood properties in plant biology. They can be toxic
to humans in some cases, and have been traditionally used by aboriginal tribesmen to poison fish. Should we consider that comforting?
The pharmacology industry has a long history of removing bad drugs from the market. Thalidomide is perhaps the most famous example
of a pharmacologic disaster. The drug was released in 1957 for its sedative effects and was touted as being safe for everyone including
"pregnant women and children." In 1961, Dr. William McBride, an obstetrician, discovered that thalidomide was useful for "morning
sickness" in pregnant women. Later he began to see unusual and devastating birth defects in babies born to women for whom he had
prescribed the drug. Independently, Dr. Widuking Lenz, a pediatrician in Germany, also associated thalidomide with severe and unusual
birth defects, such as the absence of limbs or parts of limbs. Sometimes an infants' hands were attached at the shoulders, there
being no connecting long bones at all. By 1962 the drug was taken off the market.
But unlike with our new, experimental agents, recognition of the thalidomide problem was made relatively easy by several factors.
First among these was the uniqueness of the deformities. These were both profound and obvious, which stand in stark contrast to the
current bleeding problems, which appear on the surface to be normal problems in clinical medicine -- such as nosebleeds. Even now,
doctors continue to call the loss of platelets "ITP" -- even though what we are seeing is not the same as what we would expect to
see under that diagnosis. ITP simply does not kill adult males in a few days.
Second, with thalidomide, the physician who first began using the drug for nausea in pregnancy was also the doctor who delivered
the affected babies, so he could readily put two and two together. In the case of our COVID drugs, when your doctor tells you to
get a vaccine, he doesn't administer it, doesn't witness the injection, and usually doesn't follow up to see how you fared. And if
you were to suddenly develop a vision problem or bleeding from the bowel, you wouldn't be seen by your PCP; you would be in an Emergency
Department -- and they don't usually ask about your recent vaccine history.
Third, Dr. Lenz presciently recognized that, in the case of thalidomide, many less-severe deformities, when put into perspective,
revealed "gradations of the defect." Unfortunately in the present case, lesser degrees of clotting problems are indistinguishable
from bleeding issues frequently encountered in an Emergency Room or doctor's office. For example, if a 75-year-old hypertensive male
-- who has gotten a COVID shot -- suffers a brain hemorrhage and dies, it would not likely be deemed unusual, and the relationship
to vaccination may not even be explored.
Keeping that in mind, we should assume the worst when it comes to these new COVID shots. When any new drug problem starts, it
begins slowly and unrecognized -- like a snowball beginning to roll down a mountain. By the time the problem is generally acknowledged,
the avalanche is well on its way. In the case of thalidomide, over 100,000 children were severely damaged before the drug was removed
from use. Though VAERS has the potential to shorten recognition time of drug problems by trying to spot the "unusual patterns," this
requires that physicians be aware of the system, and take the time to enter any suspected side effects -- not just the worst
cases. It also requires that researchers care enough to look. This is not happening. A report previously submitted to the Agency
for Healthcare Research and Quality revealed that fewer than one percent of adverse events get reported to VAERS.
In the past, testing done on mRNA technology revealed problems specifically involving the clotting system. Antibody-mediated platelet
damage has been suspected. Yet today when these exact problems arise, the researchers are mum. Do the experts not study or know their
own vaccine research history?
For those who are concerned about the risks, we need to advocate for ourselves, either through contacting legislators or simply
refusing to take the shots. It's obvious that the pharmaceutical industry is willing to release untried technology upon the entire
world population, and not be deterred by any inconvenience such as unexplained death.
We need to stop being a gullible population that forces our children to get vaccinated for trivial, non-fatal diseases such as
mumps. We need to stop believing in the god-like status of medical technocrats who claim to be making the world safer. We need to
reject the idea that vaccine deniers are anti-scientific troglodytes. We must reject the unspoken premise under which pharmaceutical
companies and doctors operate -- that all vaccines are always safe in all people all the time. It should not be considered unreasonable
to require scientific transparency, honesty by drug manufacturers, and safety from vaccines.
Vaccines are only indicated for diseases with a high risk of death or morbidity, and for which there is no cure. After
seeing the esteemed leaders in medicine denigrate hydroxychloroquine (even though it was a recognized treatment used successfully
elsewhere for SARS, and mentioned favorably by Dr. Fauci for MERS), after watching three plants used in the production of hydroxychloroquine
burn down in a year -- two on the same day -- after watching doctors lose their jobs and be censored for speaking truth and saving
lives with old safe drugs that work, and now, after seeing experimental genetic agents being rolled out for use globally that have
never passed animal testing and have only a few months human trials, perhaps it is time to address the 800-pound gorilla in the room
and ask, "Are they trying to kill us?"
Dr. Lee Merritt has been in the private practice of Orthopaedic and Spinal Surgery since 1995, has served on the Board of
the Arizona Medical Association, and is past president of the Association of American Physicians and Surgeons. She is a lifelong
advocate for a patient's right to choose their own medical care without government intervention.
OhSoGood tex52 �
4 days ago
Please point to a vaccine that didn't have such a tiny fraction of issues.
Start with Polio... are you going to say that was a bad idea?
Pauper Jim j b �
4 days ago
Try this:
https://archive.org/details...
I think the scale of deployment of Pfizer vaccine is tremendously greater then all other combined. For example in NJ it
is almost the only game in town now. That's might explain this statistic.
Notable quotes:
"... During the first two months of the rollout of Pfizer and Moderna "vaccines" in 2021, 95 percent of deaths from vaccines recorded in the Vaccine Adverse Event Reporting System (VAERS) were for those agents ..."
Goldbugger 2 hours ago remove link
During the first two months of the rollout of Pfizer and Moderna "vaccines" in 2021, 95
percent of deaths from vaccines recorded in the Vaccine Adverse Event Reporting System
(VAERS) were for those agents , meaning only five percent of reported deaths involved all the
other vaccines put together.
Compared to 2019, deaths in VAERS are up 6,000 percent.
Thirty-six deaths were recorded in the first quarter of 2020 versus 1,754 in the first
quarter of 2021.
https://vaers.hhs.gov/data/datasets.html ?
Statements in this site are substantiated with facts that will stand in a court of law. Informed Consent requires a flow of information.
Click on the hyperlinked sections to direct you to primary sources such as CDC, WHO, FDA documents.
Anyone trying to take down this site will be named as codefendant in Nuremberg 2.0 for being an accomplice to crimes against humanity.
That includes social media. Lawyers are standing by.
Did you know?
1. The FDA did not approve
Moderna or Pfizer mRNA gene therapeutics they dubbed "vaccines".
It simply authorized them. Fauci
confirms. 19 doctors warned
the world of the dangers. AstraZeneca is being dropped by 24
countries . Johnson & Johnson
is a
Viral Vector (1) vaccine that was given
Emergency Use Authorization on Feb. 27, 2021. Several States have halted its distribution due to
formation of blood clots . The CDC confirms.
It also confirms (2)
the Pfizer & Moderna jabs are the
deadliest of all "vaccines"
2. The clinical trials will be completed in 2023,
and there are
12
vaccine companies working on profiting from vaccine sales
3. The FDA & CDC have not revealed to the public over 20 adverse effects, including Death, related to Covid19 vaccines, which
were discussed in an
October 2020 meeting
. 3,186 deaths from Covid19 vaccines are reported by the
National Vaccine Information Center as at 4/16/2021, and
one-third of the deaths occurred within 48 hours. For clarification purposes in this article, Covid19 is regarded as an influenza
variant. Some will argue that it was developed in a
Gain-of-Function lab. That is moot. The primary
consideration is whether an experimental vaccine is warranted for a disease with a 99.9% survival rate. I am for tried, true and
tested (safe) vaccines. I am NOT for experimental vaccines backed by disastrous animal studies
4. The mRNA jab delivers a synthetic, inorganic molecule (medical device) that programs your cells to
synthesize pathogens in the form of the spike
protein that your immune system will constantly have to fight off for the rest of your life. Molecular Biologist & Immunologist,
Professor Dolores Cahill explains .
NCGI article elaborates. Fauci
confirms . Dr. Lee Merritt
reconfirms
.
Others call it
Information
Therapy that hacks the software of life, according to Moderna's [Mode RNA] chief scientist. You essentially become a GMO.
Dr. Sherri Tenpenny has mapped out eight mechanisms
of how the Covid jab is going to kill people
5. The mRNA jab does
not prevent you from contracting Covid19 or from transmitting it. Dr. Steve Hotze
elaborates .
Fauci confirms . The
CDC
graph underscores that reality, proving vaccines are ineffective and vaccine passports are totally useless. 87 million Americans
have been vaccinated as at 4/20/21, of which 7,157 have contracted Covid after being
vaccinated , resulting
in 88 deaths
Did you also know?
6. The CDC inflated the death rate for Covid19 - that was not isolated - by instructing medical practitioners in its
March 24, 2020 directive to ascribe the cause of death as Covid19 for all deaths, irrespective if patients were tested positive
for Covid19 or if they had other comorbidities, so as to ramp up the fear, and doctors have publicly stated they are being pressured
to mark Covid19 on death certificates, here is a list:
Dr.
Dan Erickson
Dr.
Scott Jensen
Infectious Disease Director Kris Ehresmann
and that 60,000
Americans have been dying weekly, consistently, before and after the covid scare - more
data - while
deaths by influenza and other diseases have plummeted
7. The CDC later admitted that
94% of deaths had underlying conditions. That means that of the 527,000 deaths reported as Covid19 - the influenza variant
- only 6% were caused directly by Covid19, or 31,620. That brings the true case fatality rate to 0.12% out of the 27 million cases
8. The survival rate for Covid19 is, therefore, roughly 99.9%. When using the state population as the denominator, the death
rate is even lower, ranging from 36 to 247 deaths per
100,000 . As at March 19, 2021, even with the doctored numbers and faulty tests, the CDC arrived at the following
survival rates :
Ages 0-17 99.998%
Ages 18-49 99.95%
Ages 50-64 99.4%
Ages 65+ 91%
9. The CDC lumped
pneumonia, influenza, and Covid19 into a new epidemic it called PIC in order to inflate Covid19 deaths. The
CDC
stats for week of July 3, 2020 confirm that pneumonia and influenza combine with Covid to inflate the death rate. The Feb.
5, 2021
report
does the same. The duplicity is underscored in the
search results page , where only "(P&I)" is mentioned, but PIC graphs appear upon clicking the links. Deaths by influenza
have dropped from 61,000
in 2018 to 22,000 in 2020, while
medical
malpractice is the third leading cause of deaths in the US
10.
Hospitals are paid $13,000 for every Covid19 admission, and $39,000 for every patient that is put on a ventilator, on average.
More proof
Are you aware that...
11. The PCR tests do not detect SARS-CoV-2 particles, but particles from any number of viruses you might have contracted in
the past, and that a lawsuit for crimes against humanity
is being launched by a German attorney for this fraud. Even
Fauci admits PCR
tests don't work. The WHO
backs him up . In this CDC document , testing guidelines
state that false negatives and positives are possible - page 39. The PCR test cannot rule out diseases caused by other bacterial
or viral pathogens - page 40. But most importantly, on page 42, SARS-CoV-2 was never isolated in the first instance: "Since no
quantified virus isolates of the 2019-nCoV were available for CDC use at the time the test was developed and this study conducted,
assays designed for detection of the 2019-nCoV RNA were tested with characterized stocks of in vitro transcribed full length RNA".
Neither the CDC can provide samples of SARS-CoV-2, nor can
Stanford and Cornell
labs , and in a CNN interview
Fauci said he was not getting tested and there is no need to test asymptomatic people. He
reiterates that asymptomatic people have never been the driving force
of a pandemic. Again, the
WHO backs him up
12. There are
class action lawsuits in the works, naming Anthony Fauci as defendant, amongst others. Here's a partial list :
- a lawsuit against the
CDC was filed for illegally withholding information under FOIA
- the WHO has a lawsuit brought against
it by German lawyer, Dr. Reiner Fuellmich, for crimes against humanity. Here is an
update
- nurses are suing a hospital CEO for covering up
the Covid fraud
- California teachers are
suing for being pressured to get an experimental vaccine, the
press release
- the Government of Norway is facing a crimes against humanity
lawsuit
- the UK Goverment will be facing a
lawsuit for crimes against humanity
- Israelis are launching a
crimes against humanity lawsuit against their own Government
- the Canadian Government is facing a legal battle from the best
Constitutional attorney, Rocco Galati, who wants to see
Bill Gates jailed
- Florida is suing the
Federal Government and the CDC
- doctors plead guilty to biotest
fraud
- Human Rights attorney, Leigh Dundas , is going after California
for trying to vaccinate children without parental consent
- a British law firm is fighting
against 'No Jab, No Pay, No Job'
And we're just getting warmed up
13. Therapeutics and prophylactics for coronaviruses, like Hydroxychloroquine, have been approved in
WHO ,
CDC and NIH websites, but were intentionally kept
out of the public eye in order to fast track vaccines. Now, some
doctors are pleading that Ivermectin be used as a sure
cure
14. Front Line Doctors
who try to explain the benefits of proven therapeutics are being silenced, and some have had their license
suspended . A concise summary by Dr. Simone Gold, who is also an attorney and founder of
America's Front Line Doctors , is a
must watch . As well, the
British Medical Journal has broken rank and is citing
corruption and suppression of science
15. Fauci and the CDC
has flip-flopped on masks ,
contaminated surfaces ,
asymptomatic spread ,
testing ,
and has only recently acknowledged that
herd immunity is achieved
when antibodies are spread by those who beat the disease (the 99.9%), but still recommends social distancing, only now from
6 feet to 3 feet , resulting in this lockdown
map . Speaking of
herd immunity, the WHO changed its
June 7, 2020 definition "Herd immunity is the indirect protection from an infectious disease that happens when a population
is immune either through vaccination or immunity developed through previous infection" to "Herd immunity', also known as 'population
immunity', is a concept used for vaccination, in which a population can be protected from a certain virus if a threshold of vaccination
is reached. Herd immunity is achieved by protecting people from a virus, not by exposing them to it" in
Nov. 13, 2020
... and that
16. Injuries
and deaths by mRNA jabs keep rising.
VAERS reports 10,152 serious injuries as at 4/16/21. In the first quarter of 2021 there has been a 6000% increase in vaccine
deaths from the same period a
year ago
17. The CDC at one time recommended DDT for in home use, and used
the same fear tactics to sell vaccines for
H1N1
18. Documents prove that the media was to be the
key player in creating the
hype leading up to the promotion of vaccines, that a VACCINATE WITH CONFIDENCE
paper by the
CDC exists, along with its
British equivalent
, and that lockdowns are used as a
carrot .
19. Politicians are caught on camera talking about the
theater of wearing masks, and the NCBI,
a division of the NIH, published a paper on
the complete ineffectiveness of masks. Even the
CDC warns of the dangers of masks
20. The CDC owns the patent for the coronavirus that is transmitted
to humans; a patent for a
Covid19 test was filed in 2015, and Covid19 test kits were being shipped
around the world in 2018
... or that
Finally, did you know?
26. Covid variant vaccines are to be marketed without
safety trials
, Fauci confirmed it
, and that antibodies/antigens to SARS-CoV-2 are found in
saliva , making the use of masks counterproductive
in achieving herd immunity
27. The CDC, that props itself up with statements like:
"The Centers for Disease Control and Prevention (CDC) is the agency Americans trust with their lives. As a global leader in
public health, CDC is the nation's premier health promotion, prevention, and preparedness agency. Whether we are protecting the
American people from public health threats, researching emerging diseases, or mobilizing public health programs with our domestic
and international partners, we rely on our employees to make a real difference in the health and well-being of people here and
around the world."
buys and resells vaccines at a markup, about $4.6 Billion worth every year, and owns over 20 vaccine patents - according to
Robert F. Kennedy Jr. - and is listed on
Dun & Bradstreet
28. The consent forms in hospitals
disguise vaccines as "biogenics", and
blood brokers have paid up to $1,000 for blood samples of recovered Covid19 people
29. It's against the Nuremberg code to force vaccinations
on a person, and informed consent overrides public
policy. Federal law prohibits employers and others from using vaccines under EUA as a
condition of employment. A Nevada attorney is ready to do battle
30. Donald Trump glories in the fact that he pushed
Warp Speed and Biden gloats that he
ordered 100 million doses
... or that
31. Time ,
again and
again the
WHO has discouraged the wearing of masks by healthy individuals, let alone
children
32. Several "simulations" of a pandemic were held in:
- May 2018 Clade X
by Johns Hopkins University
- September 2019. The WHO's Global Preparedness Monitoring Board established as one of its progress indicators the release
of two lethal pathogens by September 2020.
See pg 39
- 2018. Bill Gates' INSTITUTE FOR DISEASE MODELING released a video modeling a pandemic starting at
Wuhan,
China
- October 2019. Bill Gates sponsored a Global Pandemic Exercise
Event 201 ,
video , and Fauci sits in the
Leadership Council of the
Bill & Melinda Gates Foundation
, which has contributed over $3.5 million to Fauci's
NIH
33. The Pfizer, Moderna and J&J jabs were developed using fetal cell lines, that is, cells grown in labs originally obtained
from aborted fetuses
decades ago . The argument used by pro-vaxers is that these are not the original cells, but descendants or duplicates of the
originals. The medical term is MRC-5 . You have a right
to decline any vaccine that was developed with or contains MRC-5. Furthermore, there are people who cannot take vaccines because
of medical contraindications. A vaccine passport would discriminate against these people as they attempt to live life in American
society. A vaccine passport violates The Americans
with Disabilities Act of 1990 (42 U.S.C. Section 12101) .
34. Lockdowns have had no effect on the
death rate . Here's
another
report . And here we can
see how Covid
respects borders
35. On March 2020, the British Government discussed tactics it would use to ensure citizens complied with the loss of their
rights and freedoms and these have included –
Using media to increase the sense of personal threat
Using media to increase the sense of responsibility to others
Using and promoting social approval for desired behaviors
Using social disapproval for those who do not comply
Here is the document
If ten percent of vaccinated people still get the virus it is hoax not vaccine. The argument
that it prevents serious illness is moot as serious illness is probably less then 1% of COVID-19
infections and happens most to people at risk (over 70, with several other serious medical
conditions, morbidly obese, with compromised immune system, etc)
SaCalobra 3 hours ago (Edited)
The jab is great. Except now you need THREE of them. And except from the fact that you can
still get covid. And that you are still adviced to keep distance. And to wear a mask. And a
vaccine passport. And all the side effects. Like death. Great! I want it!!!
get nothing and like it 3 hours ago (Edited)
But for gods sake you must get the jab. Otherwise you "could" get the virus 50/50 chance,
which would kill you .01% of you are under 60 and healthy, or put you in the hospital maybe
.1%, or make you really sick like the flu 25% chance and the jab does that with 50% of people
or you don't even know you have it 30%. And if you do by chance get it, you have natural
immunity. So yes get the jab for sure ...
3rd Dose Of Pfizer's COVID Vaccine "Likely" Needed To Combat Mutant COVID Strains, CEO Says
BY TYLER DURDEN
THURSDAY, APR 15, 2021 - 03:33 PM
As American waits for the CDC to finish a review of blood-clotting risks associated with Johnson & Johnson's COVID-19 vaccine,
Pfizer CEO Albert Bourlas has warned reporters that recipients of the Pfizer vaccine - the most widely distributed jab in the
US - will "likely" need to receive a third "booster" shot within 12 months of being vaccinated, and possibly as early as six
months after receiving their second dose.
The news is hardly a surprise. Comments and rumors about the need for booster shots have been reported by the US media
since
late last year
. But on Thursday, Bourlas said a booster shout would likely be necessary, and that patients may need to be
vaccinated against COVID annually, similar to the way that flu vaccines are developed and distributed.
"It is extremely important to suppress the pool of people that can be susceptible to the virus," he told CNBC's Bertha Coombs
during an event with CVS Health. Bourlas added that vaccines will need to be used to combat not just COVID, but the evolving
mutant strains - or "variants" - like B.1.1.7, known as the "Kent" strain, which has been blamed for some of the botched
rollout in the US.
Bourlas isn't the only major public health official warning about the need for booster shots. On Thursday, the Biden
administration's Covid response chief science officer David Kessler said Americans should expect to receive booster shots to
protect against coronavirus variants. He noted that while the current crop of COVID jabs is highly effective, they could be
"challenged" by the new variants.
New data released earlier this month by Pfizer said that updated data from its clinical trial showed its vaccine to be highly
effective six months after the second dose. The data was based on more than 12K vaccinated participants. More data is still
needed to determine whether protections last after six months, however. Pfizer and German partner BioNTech began studying a
third dose of their vaccine in late February.
The booster shot is aimed at protecting against future variants, which may be better at evading antibodies from vaccine than
earlier strains of the virus. About 144 volunteers will be given the third dose, mostly those who participated in the
vaccine's early-stage U.S. testing last year.
"We don't know everything at this moment," he told House Select Subcommittee on the Coronavirus Response. "We are studying the
durability of the antibody response," he said. "It seems strong but there is some waning of that and no doubt the variants
challenge...they make these vaccines work harder. So I think for planning purposes, planning purposes only, I think we should
expect that we may have to boost."
Bourla said the company would likely try out the third doses first on a select group of individuals who participated in the
original studies.
In other news, Pfizer has been focusing on trials of its
COVID
jab in children as it aims to become the first to be approved for use in minors
. Currently, the pharma giant is testing
the jab on children and babies younger than one year old.
y_arrow
prom queen
43 minutes ago
Can I
hear a 4, what about a 5??
SERReal1
42 minutes ago
Just used to getting a jab every year
Stalefarts
33 minutes ago
This
is just the calm before the cytokine storm.
CleeTorres
31 minutes ago
He's
not dumb...
1 shot
= I'm making lots of money
2
shots = I'm making lots more money
3
shots = Heck, I need another mansion or two
Yearly
Shot = Damn people are stupid. Maybe I can make it monthly
S. Archer
37 minutes ago
It
won't end with a 3rd shot. This crap is going to become annual. Every year we'll be harassed about whether
we have had our covid shots or not. I for one will not be participating. GTFO with that crap.
Around 20 years ago, the work of two researchers -- Drew Weissman and Katalin Karik� -- helped overcome two primary barriers that had
been standing in the way of utilizing mRNA technology: an inflammatory effect on the body that made test animals ill, and the
fragile nature of the molecule itself, both of which hindered its utility.
Despite those advancements, and the wealth of research that's been carried out since, the fact remains that the two mRNA vaccines in
use today are the first of their kind. That may be in part because it's difficult to generate interest and funding to support
pursuing "non-mainstream" science outside of a crisis, Duprex said -- what he characterized as "a shortsighted way to think about
biology."
Only now, amid a devastating pandemic, has this technology reached mainstream prominence. "Given the choice, I would have rather
avoided this past year," Weissman said. "But we didn't, and now RNA is going to be our future."
Here's a look at how, exactly, these vaccines manage to pull off this feat and some of the key research breakthroughs that made this
moment possible.
How messenger RNA vaccines work
In order to develop these vaccines, researchers took the RNA-based genetic sequence of the coronavirus and turned it into DNA. This
crucial step allowed them to identify the "instructions" necessary to create the spike protein, engineer corresponding synthetic
mRNA and package that into their vaccines.
mRNA, as its moniker implies, is a messenger. This particular type of RNA is tasked with delivering messages to microscopic cellular
machines called ribosomes, located in the cytoplasm of our cells, which are responsible for synthesizing proteins. Those ribosomes
then interpret that message to make proteins and start executing its instructions, explained Phillip Sharp, a molecular biologist
and MIT professor who shared the 1993 Nobel Prize in physiology or medicine for his contribution to our understanding of RNA.
Dendritic cells, the watchdogs of the immune system, play an essential role in responding to pathogens. They patrol the body in
search of foreign invaders and, when they find one, start stimulating an immune response. When these cells encounter mRNA that's
been injected via vaccination, their ribosomes decode the message and allow the cells to temporarily display spike proteins
identical to the ones found on the coronavirus's exterior, Weissman said.
"Dendritic cells make the spike protein and then they present it to other immune cells and activate them to start the immune
response," he added.
An
animated visual of the coronavirus. Megan McGrew/PBS NewsHour
What does the coronavirus look like?
Like the other members of its viral family, SARS-CoV-2 -- the official name for the coronavirus -- is an RNA virus. Simply put,
each individual virus is composed of single strands of genetic material protected by a fatty outer layer that's coated in
spike proteins. Those "spikes" are what the virus uses to hijack our cells and use our molecular machinery to make more copies
of itself.
The proteins allow the dendritic cells to alert two more key players in the immune system -- T cells and B cells -- that if they see
those same spikes on any other cell, they should recognize them as a foreign invaders and either destroy them or generate antibodies
to neutralize them immediately.
"There's a memory component of those cell populations, and that stays in your body over a long period of time," Sharp said. "If a
similar virus infects you, those memory cells are ready to go. They are all perfected to go out and kill that virus."
mRNA naturally degrades rapidly over time, so once it has served its purpose, it simply breaks down. The dendritic cells that
expressed the spike protein eventually die and are replaced by new ones that continue to pick up that vaccine-delivered mRNA and
repeat the process all over again in the course of about two weeks following immunization.
Some members of the public have expressed concern over unfounded speculation that these vaccines could negatively affect the body.
But it is impossible for an mRNA vaccine to alter your DNA because synthetic mRNA operates only in the cytoplasm and is incapable of
entering any other parts of our cells, such as the nucleus.
Like virtually all vaccines, those that use mRNA can trigger temporary symptoms like a fever, fatigue and soreness at the injection
site that dissipate within a few days. But clinical trials that took place before the vaccines were authorized, as well as those
that have followed, all suggest that these vaccines are both safe and effective at preventing serious illness and death.
"It's always, always much more risky to get the disease than it is to get the vaccine," Duprex said.
How did we get here?
mRNA was first
injected
into the muscles of mice in 1990
with the intention to deliver therapeutic proteins. But that effort "didn't go very far,"
according to Weissman, in large part due to the strong inflammatory response it induced, which severely sickened the animals
involved.
That's because in both animals and humans, cells feature a number of different receptors that can recognize mRNA as a foreign
substance that must be destroyed. Those receptors help these cells distinguish their fellow cells from invaders like viruses,
bacteria or even tumor cells.
Both RNA and DNA are composed of four nucleotides. More than a decade after that first injection in mice, Weissman and Karik�, who
now serves as senior vice president at BioNTech, which partnered with Pfizer to manufacture their joint vaccine, figured out a way
to
insert
an modified nucleotide
that allows the synthetic mRNA to masquerade as a normal cell and circumvent those receptors, no longer
triggering extreme inflammation. It also made the mRNA-spurred protein production more efficient.
"Our big discovery was that we could modify the RNA to make it non-inflammatory. And that had a couple of important features to it,
but the first was that it greatly increased the amount of protein made off of the RNA," which increased potency, Weissman said.
With the inflammation problem solved, Weissman and Karik� then turned to tweaking how mRNA is delivered so it could actually do its
job once injected into the body. mRNA is an inherently "labile," or unstable, material that can degrade rapidly to the point of
being rendered ineffective.
After testing around 40 different types of delivery systems, the researchers found their golden ticket: lipid nanoparticles. These
"droplets of fat" coat the mRNA and allow it to successfully enter our cells, which are also encapsulated in an oily substance.
Traditional vaccines are typically formulated with adjuvants that are designed to stimulate the immune response in their recipients.
In what Weissman described as a lucky development, lipid nanoparticles happened to act as an adjuvant that stimulated a specific
type of "helper cell" that promotes antibody responses.
"We use the lipid nanoparticles to get over a lot of the fragility [problems] because that protected the [mRNA] after you injected
it into people, and it promoted these cells to take up the [mRNA] and start the vaccine process," Weissman said.
Where mRNA stands today
In the years since Weissman and Karik� made these breakthroughs, mRNA research has continued to march on. Weissman and his current
colleagues have worked on a variety of mRNA vaccines, including a "universal" flu shot that could cover
a
majority of influenza viruses
and has so far proven to be effective in animal trials.
Compared to traditional vaccine platforms that require a series of complex steps, like growing mammalian cells in massive quantities
and a viral purification process that looks different depending on the pathogen you're working with, mRNA is now easy to manufacture
at a fairly large scale.
Instead of needing "to reinvent the wheel every time you make a new vaccine," Weissman said, "with [mRNA,] it's the same reaction,
and the only thing you have to do is plug in the new sequence for any virus, so that makes it very easy to produce a new vaccine."
Both Moderna and Pfizer's vaccines generated above 90 percent protection after two doses during clinical trials that played out
before new variants of the virus marginally reduced their efficacy. Even so, the two give recipients remarkably high levels of
protection, particularly
against
severe disease and death
.
The CDC recently released new research that found these vaccines reduce a fully vaccinated person's chance of
getting
infected with the coronavirus
by 90 percent in "real-world" settings like the workplace.
Given that no vaccines have ever been approved to immunize people against any kind of coronavirus, and that the FDA's original hope
was to secure one with
at
least 50 percent efficacy
to curb the pandemic, these results represent yet another significant milestone in annals of RNA
technology.
Much more research lies ahead for these vaccines, both of which have been rolled out in the United States and in some other
countries over the past few months. In addition to continuing to track safety and efficacy data, researchers need to know how well
these vaccines
prevent
recipients from transmitting COVID-19
and how long the protection they offer lasts. Until we know the answers to those
questions, recipients should keep following pandemic precautions like wearing a mask, even after they've gotten their two doses,
experts say.
READ MORE: How to stay safe from COVID this summer, according to experts
Johnson & Johnson's vaccine, a one dose shot that uses a
different
yet similarly innovative platform
to deliver immunity compared to mRNA, has also been authorized for use in the United States.
Its strong efficacy and ability to be stored at a less strict temperature range makes experts hopeful that the rollout of this
vaccine will help
close
some gaps in vaccine access
both in this country and abroad.
In tackling COVID-19, Pfizer and Moderna's vaccines have "paved the way," Duprex said, when it comes to illustrating the utility of
synthetic mRNA. And yet, while he anticipates that researchers will "only get better" at making tweaks that allow for better
delivery and stability of this technology, he notes that we're still in the early days of harnessing its utility -- we also can't
assume that mRNA is "the next big panacea" that will solve all of our problems.
But, Duprex said, "the beautiful thing about this is this just gives us another brush for the palette of novel therapeutics [and]
novel ideas that somebody in the next generation of scientists are going to be able to [use to] paint."
SYDNEY, Aug 20 - Triple therapy specialist Professor Thomas Borody, famous for curing peptic
ulcers using a Triple Antibiotic Therapy saving millions of lives, has released the Triple
Therapy Protocol for COVID-19 to Australian GPs, who can legally prescribe it to COVID-19
positive patients, or prescribe it as a preventative medication. Borody says this could be the
fastest and safest way to end the pandemic in Australia within 6-8 weeks.
Professor Thomas Borody MB, BS, BSc(Med), MD, PhD, DSc, FRACP, FACP, FACG, AGAF, FRS(N)
said:[email protected]
"GPs can legally prescribe the therapy today as an "off label" treatment according to
Australian Guidelines - a standard practice in medicine. In fact more than 60% of prescriptions
in Australia are "off-label". It's not a new concept. It's happening every day to manage
diseases and save lives."
Professor Borody continued:
"We have a therapy that can fight COVID-19. The medications have been around for 50 years,
they are cheap, FDA and TGA approved, and have an outstanding safety profile. Why are we just
waiting around for a vaccine? To save lives we should be using whatever is safe and available
right now. We could lead the world in this fight.
"Australia has some of the best medical and science people in the world - indeed the
Ivermectin connection was first discovered by Dr Kylie Wagstaff's team at Monash University in
April. How long do we need to wait before Australian politicians get behind Australian medical
science and use 'war room' tactics with safe and approved medications."
Any test with a cycle threshold above 35 is too sensitive, agreed Juliet Morrison, a
virologist at the University of California , Riverside. "I'm
shocked that people would think that 40 could represent a positive," she said.
A more reasonable cutoff would be 30 to 35, she added. Dr. Mina said he would set the figure
at 30, or even less.
ISITZEN -- What
number of Amplification Cycles being used in the PCR tests?
Moderna Inc.'s vaccine remained more than 90% effective after six months, according to a new
analysis of data from the company's final-stage trial.
Beginning two weeks after the second dose, the shot was more than 90% effective overall, and
more than 95% effective at preventing severe cases, according to a statement. The company
didn't release further details and said the follow-up results were preliminary as the study is
continuing.
If we assume that 10% of vaccinated who get infected (the vaccine does not prevent infection but does prevent development of
virus pneumonia) will get virus pneumonia and if the effectiveness will drop further in 12 month this means that this particular
vaccine is a grandiose failure. Notable quotes:
"... Actual death count means the number of death where CODID-19 is primary cause means deaths from virus pneumonia only. All other needs to be excluded, IMHO. As money are involved, I think the statistics is grossly exaggerated. ..."
"... If we assume that 10% of vaccinated who get infected (the vaccine does not prevent infection but does prevent development of virus pneumonia) will get virus pneumonia and if the effectiveness will drop further in 12 month this means that this particular vaccine is a grandiose failure. ..."
Scientists at the VA's Office of Research and Development in White River Junction, Vermont, have found that the vaccines can provide
immunity for at least seven to nine months, a time frame similar to the immune response generated in people who have had COVID-19.
The study examined antibodies in some of the 240,000 veterans who have contracted COVID-19, Dr. Richard Stone, VA's acting under
secretary for health, said Friday.
Speaking to reporters during a news conference Friday with VA Secretary Denis McDonough, Dr. Richard Stone:
"The evidence is that between seven and nine months, we can feel comfortable that you are still protected. We think it will
be longer than that. That is not a limitation,"
While several studies have shown that immunity following a COVID-19 infection can last at least six months, and perhaps as many
as eight months, research on the lasting impact of COVID-19 vaccines is ongoing, and scientists have been hesitant to discuss the
time frame before all the data is compiled.
But the VA's findings, Stone said, could "extend" the Centers for Disease Control and Prevention's message that immunity from
a vaccine lasts at least six months. Dr. Richard Stone:
"Right now it appears we will be able to publish in the next few weeks."
The belief right now in Covid-19 like the flu is an endemic disease just like influenza. The issue then is how to reduce mortality
and hospitalizations going forward
Likbez ,
> The issue then is how to reduce mortality and hospitalizations going forward
In order to reduce mortality it is important to have valid statistical data of the number of infections (not positive PcR tests
without specifying the number of amplifications )
This number of amplification cycles needed to find the virus, called the cycle threshold, is never included in
the results sent to doctors and coronavirus patients, although it could tell them how infectious the patients are.
[why?]
The C.D.C.'s own calculations suggest that it is extremely difficult to detect any live virus in a sample
above a threshold
of 33 cycles . Officials at some state labs said the C.D.C. had not asked them to note threshold values or to share
them with contact-tracing organizations. [why?]
Any test with a cycle threshold above 35 is too sensitive, agreed Juliet Morrison, a virologist at the University of
California , Riverside. "I'm shocked
that people would think that 40 could represent a positive," she said.
A more reasonable cutoff would be 30 to 35, she added. Dr. Mina said he would set the figure at 30, or even less.
ISITZEN - What number of Amplification Cycles
being used in the PCR tests?
Actual death count means the number of death where CODID-19 is primary cause means deaths from virus pneumonia only.
All other needs to be excluded, IMHO. As money are involved, I think the statistics is grossly exaggerated.
In this respect, one effect that does need a valid explanation is almost total elimination of deaths from influenza this season.
How this could be?
Development of direct methods of treating COVID-19 is also important and can help to reduce "real" mortality. This policy of
putting all money on a single method - vaccination - looks pretty questionable to me, taking into account that coronaviruses mutate
rapidly which limits the duration of vaccination, and the possibility of discovering long term side effects.
What about effective antibody treatment and new medications that supposedly can prevent the development of virus pneumonia?
Which means that death from COVID-19 can be eliminated without vaccination as only pneumonia is deadly in this case.
Traditionally pneumonia is the main cause of deaths among elderly so the fact that now this is the COVID-19 pneumonia changes
very little in statistics of death for the elderly. Post-influenza bacterial pneumonia is dangerous enough for this category of
people, so COVID-19 pneumonia changes almost nothing here.
This wide-scale biological experiment with vaccination for age groups below, say, 50, does not look too promising if the effectiveness
of the vaccine is limited to a single virus season. Which is what the CEO of Pfizer hinted recently.
Bloomberg triumphantly reported that Moderna effectiveness is 90% after six months. But what 90% effectiveness means is anybody
guess.
https://www.bloomberg.com/news/articles/2021-04-12/india-has-2nd-most-cases-u-k-hits-vaccine-target-virus-update?srnd=premium
If we assume that 10% of vaccinated who get infected (the vaccine does not prevent infection but does prevent development of
virus pneumonia) will get virus pneumonia and if the effectiveness will drop further in 12 month this means that this particular
vaccine is a grandiose failure.
Also constant vaccine cheerleading in neoliberal MSM became a little bit annoying as for age groups below, say 50, this virus
does not represent serious, statistically significant danger.
And what if we discover serious side effects of Pfizer or Moderna vaccine a year or two from now ? Then what?
IMHO attempt to immunize people below 25 or 30 years old without serious health problems would be highly questionable and possible
harmful. And, unfortunately, I saw many such people in lines.
Also, one size does not fit all here. There areas with high density of population like NYC and vicinity (NY metropolitan
area). Where the risk is highest and the virus represent serious and immanent threat due to the specifics of this env. Which
is unhealthy env to start with.
And there are rural areas ( like in PA ) where so far there were no cases of COVID-19. At all.
It is wrong to treat them identically.
Also the value of vaccination depends on occupation, along with the age and general health. People who need to contact
many other people can benefit more from the vaccination.
For them the small risk of complications from the vaccine is far less than the risk of being infected and develop COVID-19
pneumonia. For people living more or less isolated life, and, especially, people paranoid about this virus - not so much.
ee-to-read link
Don't show me this again
Covid-19 Drug Prevents Symptomatic Disease in Study, Regeneron Says
Drugmaker says it will ask federal health regulators to clear use among people who haven't been vaccinated
Regeneron said Monday it would ask the U.S. Food and Drug Administration to expand the drug's authorization.
PHOTO:
/ASSOCIATED PRESS
By
Joseph Walker
Updated April 12, 2021 1:32 am ET
Listen to this article
4 minutes
00:00 / 04:25
1x
An antibody drug from
Regeneron
Pharmaceuticals
Inc.
REGN
0.13%
reduced
the risk of developing symptomatic
Covid-19
infection
by 81% compared with a placebo in people living with someone infected by the new coronavirus, a study found.
The results point to potential new preventive applications for the drug, which is already in use to treat earlier
Covid-19 cases.
Regeneron said Monday it would ask the U.S. Food and Drug Administration to expand the drug's authorization among
people exposed to the virus who haven't yet been vaccinated, which could provide temporary stopgap protection as
people
await vaccines
.
So far, 21.3% of the U.S. population has been fully vaccinated, and 35.3% has received at least one shot
...
REGEN-COV
is currently authorized to treat people infected with Covid-19 who have mild to moderate symptoms and are at high
risk of developing severe disease because of factors including age or underlying conditions such as obesity.
Opinion: Morning Editorial Report
All the day's Opinion headlines.
PREVIEW
SUBSCRIBE
Drs. Gottlieb and McClellan say therapeutic antibodies and drugs like remdesivir and dexamethasone have been the
only options. We disagree and have published detailed reviews of successful early treatment.
Thousands of lives have been saved.
Two drugs used, ivermectin and hydroxychloroquine, have two of the best safety records on the market, with
billions of doses safely prescribed.
The former commissioners suggest judging drugs on whether they "shorten the duration of symptoms or reduce viral
load" -- poorly measured and unimportant outcomes compared with hospitalization and mortality. We already have
evidence for generics reducing Covid death rates. Agencies should devote their efforts to confirming these results
instead of chasing new, more expensive drugs.
Sen. Ron Johnson (R., Wis.)
Oshkosh, Wis.
Prof. Harvey Risch, M.D., Ph.D.
Yale School of Public Health
New Haven, Conn.
Highly recommended !Notable quotes:
"... Dr. Kaplan is a faculty member at the Stanford School of Medicine Clinical Excellence Research Center and the UCLA Fielding School of Public Health. He has served as associate director of the National Institutes of Health and chief science officer at the U.S. Agency for Healthcare Research and Quality. ..."
Originally from:
Stop Taking Shots at Those Who Fear Them - WSJ By Robert M. Kaplan April 8, 2021 6:21 pm
ET
Distrust of the establishment plays a role in vaccine hesitancy, but it's probably time to
back off on the prevailing commentary suggesting that those avoiding vaccines are
irresponsible, uninformed or politically manipulated. Achieving herd immunity requires that
about 70% of Americans are vaccinated or contract Covid and develop natural immunity, which
official numbers place around 10% of the population. Polls consistently show that 21% say they
will definitely not get the vaccine and about a third rate their chances of taking the vaccine
as less than 50%. It's better to address common fears and concerns respectfully and
informatively than with hectoring and condescension.
Dr. Kaplan is a faculty member at the Stanford School of Medicine Clinical Excellence
Research Center and the UCLA Fielding School of Public Health. He has served as associate
director of the National Institutes of Health and chief science officer at the U.S. Agency for
Healthcare Research and Quality.
tyberious 20 hours
I just checked the CDC Covid vaccine tracker and most states are under 30%.
I think they may get 5% more to take the jab, but thats about it!
Txjac 20 hours ago
At the hospital where my sister works they have had to ask them to stop shipping the
vaccine. Not many are lining up to take it. Seems like we have an overabundance of it here in
Houston
Though the whole world relies on RT-PCR to "diagnose" Sars-Cov-2 infection,
the science is clear: they are not fit for purpose
Moreover, it is worth mentioning that the PCR tests used to identify so-called COVID-19
patients presumably infected by what is called SARS-CoV-2 do not have a valid gold standard to
compare them with.
This is a fundamental point. Tests need to be evaluated to determine their preciseness --
strictly speaking their "sensitivity"[
1 ] and "specificity" -- by comparison with a "gold standard," meaning the most accurate
method available.
As an example, for a pregnancy test the gold standard would be the pregnancy itself. But as
Australian infectious diseases specialist Sanjaya Senanayake, for example, stated in an
ABC TV interview in an answer to the
question "How accurate is the [COVID-19] testing?" :
If we had a new test for picking up [the bacterium] golden staph in blood, we've already
got blood cultures, that's our gold standard we've been using for decades, and we could match
this new test against that. But for COVID-19 we don't have a gold standard test."
Jessica C. Watson from Bristol University confirms this. In her paper "Interpreting a COVID-19 test result" The British Medical Journal , she writes that there is a
"lack of such a clear-cut 'gold-standard' for COVID-19 testing."
But instead of classifying the tests as unsuitable for SARS-CoV-2 detection and COVID-19
diagnosis, or instead of pointing out that only a virus, proven through isolation and
purification, can be a solid gold standard, Watson claims in all seriousness that,
"pragmatically" COVID-19 diagnosis itself, remarkably including PCR testing itself, "may be
the best available 'gold standard'." But this is not scientifically sound.
Apart from the fact that it is downright absurd to take the PCR test itself as part of the
gold standard to evaluate the PCR test, there are no distinctive specific symptoms for
COVID-19, as even people such as Thomas Löscher, former head of the Department of
Infection and Tropical Medicine at the University of Munich and member of the Federal
Association of German Internists, conceded to us[
2 ].
And if there are no distinctive specific symptoms for COVID-19, COVID-19 diagnosis --
contrary to Watson's statement -- cannot be suitable for serving as a valid gold standard.
In addition, "experts" such as Watson overlook the fact that only virus isolation, i.e. an
unequivocal virus proof, can be the gold standard.
That is why I asked Watson how COVID-19 diagnosis "may be the best available gold standard,"
if there are no distinctive specific symptoms for COVID-19, and also whether the virus itself,
that is virus isolation, wouldn't be the best available/possible gold standard. But she hasn't
answered these questions yet – despite multiple requests. And she has not yet responded
to our rapid response post on her article in which we address exactly the same points, either,
though she wrote us
on June 2nd : "I will try to post a reply later this week when I have a
chance."
NO PROOF FOR THE RNA BEING OF VIRAL ORIGIN
Now the question is: What is required first for virus isolation/proof? We need to know where
the RNA for which the PCR tests are calibrated comes from.
As textbooks (e.g., White/Fenner. Medical Virology, 1986, p. 9) as well as leading virus
researchers such as Luc Montagnier
or Dominic Dwyer state , particle purification -- i.e. the separation of an object from
everything else that is not that object, as for instance Nobel laureate Marie Curie purified
100 mg of radium chloride in 1898 by extracting it from tons of pitchblende -- is an essential
pre-requisite for proving the existence of a virus, and thus to prove that the RNA from the
particle in question comes from a new virus.
The reason for this is that PCR is extremely sensitive, which means it can detect even the
smallest pieces of DNA or RNA -- but it cannot determine where these particles came from
. That has to be determined beforehand.
And because the PCR tests are calibrated for gene sequences (in this case RNA sequences
because SARS-CoV-2 is believed to be a RNA virus), we have to know that these gene snippets are
part of the looked-for virus. And to know that, correct isolation and purification of the
presumed virus has to be executed.
Hence, we have asked the science teams of the relevant papers which are referred to in the
context of SARS-CoV-2 for proof whether the electron-microscopic shots depicted in their in
vitro experiments show purified viruses.
But not a single team could answer that question with "yes" -- and NB., nobody said
purification was not a necessary step. We only got answers like "No, we did not obtain an
electron micrograph showing the degree of purification" (see below).
We asked several study authors "Do your electron micrographs show the purified virus?", they
gave the following responses:
Study 1: Leo L. M. Poon; Malik Peiris. "Emergence of a novel human coronavirus threatening
human health" Nature Medicine , March 2020"The image is the virus budding from an infected cell. It is not purified
virus."
Study 2: Myung-Guk Han et al. "Identification of Coronavirus Isolated from a Patient in
Korea with COVID-19", Osong Public Health and Research Perspectives , February 2020"We could not estimate the degree of purification because we do not purify and
concentrate the virus cultured in cells."
Study 3: Wan Beom Park et al. "Virus Isolation from the First Patient with SARS-CoV-2 in
Korea", Journal of Korean Medical Science , February 24, 2020"We did not obtain an electron micrograph showing the degree of
purification."
Study 4: Na Zhu et al., "A Novel Coronavirus from Patients with Pneumonia in China", 2019,
New England Journal of Medicine , February 20, 2020"[We show] an image of sedimented virus particles, not purified ones."
Regarding the mentioned papers it is clear that what is shown in the electron micrographs
(EMs) is the end result of the experiment, meaning there is no other result that they could
have made EMs from.
That is to say, if the authors of these studies concede that their published EMs do not show
purified particles, then they definitely do not possess purified particles claimed to be viral.
(In this context, it has to be remarked that some researchers use the term "isolation" in their
papers, but the procedures described therein do not represent a proper isolation (purification)
process. Consequently, in this context the term "isolation" is misused).
Thus, the authors of four of the principal, early 2020 papers claiming discovery of a new
coronavirus concede they had no proof that the origin of the virus genome was viral-like
particles or cellular debris, pure or impure, or particles of any kind. In other words, the
existence of SARS-CoV-2 RNA is based on faith, not fact.
We have also contacted Dr Charles Calisher, who is a seasoned virologist. In 2001,
Science published an "impassioned plea to the younger generation" from several
veteran virologists, among them Calisher, saying that:
[modern virus detection methods like] sleek polymerase chain reaction [ ] tell little or
nothing about how a virus multiplies, which animals carry it, [or] how it makes people sick.
[It is] like trying to say whether somebody has bad breath by looking at his fingerprint."[
3 ]
And that's why we asked Dr Calisher whether he knows one single paper in which SARS-CoV-2
has been isolated and finally really purified. His answer:
I know of no such a publication. I have kept an eye out for one."[
4 ]
This actually means that one cannot conclude that the RNA gene sequences, which the
scientists took from the tissue samples prepared in the mentioned in vitro trials and for which
the PCR tests are finally being "calibrated," belong to a specific virus -- in this case
SARS-CoV-2.
In addition, there is no scientific proof that those RNA sequences are the causative agent
of what is called COVID-19.
In order to establish a causal connection, one way or the other, i.e. beyond virus isolation
and purification, it would have been absolutely necessary to carry out an experiment that
satisfies the four Koch's postulates. But there is no such experiment, as Amory Devereux and
Rosemary Frei
recently revealed for OffGuardian .
The necessity to fulfill these postulates regarding SARS-CoV-2 is demonstrated not least by
the fact that attempts have been made to fulfill them. But even researchers claiming they have
done it, in reality, did not succeed.
One example is a study published in Nature on
May 7 . This trial, besides other procedures which render the study invalid, did not meet
any of the postulates.
For instance, the alleged "infected" laboratory mice did not show any relevant clinical
symptoms clearly attributable to pneumonia, which according to the third postulate should
actually occur if a dangerous and potentially deadly virus was really at work there. And the
slight bristles and weight loss, which were observed temporarily in the animals are negligible,
not only because they could have been caused by the procedure itself, but also because the
weight went back to normal again.
Also, no animal died except those they killed to perform the autopsies . And let's not
forget: These experiments should have been done before developing a test, which is not
the case.
Revealingly, none of the leading German representatives of the official theory about
SARS-Cov-2/COVID-19 -- the Robert Koch-Institute (RKI), Alexander S. Kekulé (University
of Halle), Hartmut Hengel and Ralf Bartenschlager (German Society for Virology), the
aforementioned Thomas Löscher, Ulrich Dirnagl (Charité Berlin) or Georg Bornkamm
(virologist and professor emeritus at the Helmholtz-Zentrum Munich) -- could answer the
following question I have sent them:
If the particles that are claimed to be to be SARS-CoV-2 have not been purified, how do
you want to be sure that the RNA gene sequences of these particles belong to a specific new
virus?
Particularly, if there are studies showing that substances such as antibiotics that are
added to the test tubes in the in vitro experiments carried out for virus detection can
"stress" the cell culture in a way that new gene sequences are being formed that were
not
previously detectable -- an aspect that Nobel laureate Barbara McClintock already drew
attention to in her Nobel Lecture back in
1983 .
It should not go unmentioned that we finally got the Charité – the employer of
Christian Drosten, Germany's most influential virologist in respect of COVID-19, advisor to the
German government and co-developer of the PCR test which was the first to be "accepted" (
not validated! ) by the WHO worldwide – to answer questions on the topic.
But we didn't get answers until June 18, 2020, after months of non-response. In the end, we
achieved it only with the help of Berlin lawyer Viviane Fischer.
Regarding our question "Has the Charité convinced itself that appropriate particle
purification was carried out?," the Charité concedes that they didn't use purified
particles.
And although they claim "virologists at the Charité are sure that they are testing
for the virus," in their paper ( Corman et
al. ) they state:
RNA was extracted from clinical samples with the MagNA Pure 96 system (Roche, Penzberg,
Germany) and from cell culture supernatants with the viral RNA mini kit (QIAGEN, Hilden,
Germany),"
Which means they just assumed the RNA was viral .
Incidentally, the Corman et al. paper, published on January 23, 2020 didn't even go through
a proper peer review process , nor were the procedures outlined therein accompanied by controls
-- although it is only through these two things that scientific work becomes really
solid.
IRRATIONAL TEST RESULTS
It is also certain that we cannot know the false positive rate of the PCR tests without
widespread testing of people who certainly do not have the virus, proven by a method which is
independent of the test (having a solid gold standard).
Therefore, it is hardly surprising that there are several papers illustrating irrational
test results.
For example, already in February the health authority in China's Guangdong province reported
that people have fully recovered from illness blamed on COVID-19, started to test "negative,"
and then tested
"positive" again .
A month later, a paper published in the Journal of Medical Virology showed that 29
out of 610 patients at a hospital in Wuhan had 3 to 6 test results that flipped between
"negative", "positive" and
"dubious" .
A third example is a study from Singapore in which tests were carried out almost daily on 18
patients and the majority went from "positive" to "negative" back to "positive" at least once,
and up to
five times in one patient .
Even Wang Chen, president of the Chinese Academy of Medical Sciences, conceded in February
that the PCR tests are
"only 30 to 50 per cent accurate"
etter to the WHO's coronavirus response team and to Anthony S. Fauci on March 22, 2020,
saying that:
It has been widely reported in the social media that the RT-qPCR [Reverse Transcriptase
quantitative PCR] test kits used to detect SARSCoV-2 RNA in human specimens are generating
many false positive results and are not sensitive enough to detect some real positive
cases."
In other words, even if we theoretically assume that these PCR tests can really detect a
viral infection, the tests would be practically worthless, and would only cause an unfounded
scare among the "positive" people tested.
This becomes also evident considering the positive predictive value (PPV).
The PPV indicates the probability that a person with a positive test result is truly
"positive" (ie. has the supposed virus), and it depends on two factors: the prevalence of the
virus in the general population and the specificity of the test, that is the percentage of
people without disease in whom the test is correctly "negative" (a test with a specificity of
95% incorrectly gives a positive result in 5 out of 100 non-infected people).
With the same specificity, the higher the prevalence, the higher the PPV.
In this context, on June 12 2020, the journal Deutsches Ärzteblatt published an
article in which the PPV has been calculated with
three different prevalence scenarios .
The results must, of course, be viewed very critically, first because it is not possible to
calculate the specificity without a solid gold standard, as outlined, and second because the
calculations in the article are based on the specificity determined in the study by Jessica
Watson, which is potentially worthless, as also mentioned.
But if you abstract from it, assuming that the underlying specificity of 95% is correct and
that we know the prevalence, even the mainstream medical journal Deutsches Ärzteblatt
reports that the so-called SARS-CoV-2 RT-PCR tests may have "a shockingly low" PPV.
In one of the three scenarios, figuring with an assumed prevalence of 3%, the PPV was only
30 percent, which means that 70 percent of the people tested "positive" are not "positive" at
all . Yet "they are prescribed quarantine," as even the Ärzteblatt notes critically.
In a second scenario of the journal's article, a prevalence of rate of 20 percent is
assumed. In this case they generate a PPV of 78 percent, meaning that 22 percent of the
"positive" tests are false "positives."
That would mean: If we take the around 9 million people who are currently considered
"positive" worldwide -- supposing that the true "positives" really have a viral infection -- we
would get almost 2 million false "positives."
All this fits with the fact that the CDC and the FDA, for instance, concede in their files
that the so-called "SARS-CoV-2 RT-PCR tests" are not suitable for SARS-CoV-2 diagnosis.
In the "CDC 2019-Novel
Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel" file from March 30, 2020, for
example, it says:
Detection of viral RNA may not indicate the presence of infectious virus or that 2019-nCoV
is the causative agent for clinical symptoms"
And:
This test cannot rule out diseases caused by other bacterial or viral pathogens."
And the FDA admits
that :
positive results [ ] do not rule out bacterial infection or co-infection with other
viruses. The agent detected may not be the definite cause of disease."
Remarkably, in the instruction manuals of PCR tests we can also read that they are not
intended as a diagnostic test, as for instance in those by
Altona Diagnostics and Creative Diagnostics[
5 ].
To quote another one, in the product announcement of the LightMix Modular Assays produced by
TIB Molbiol -- which were developed using the Corman et al. protocol -- and
distributed by Roche we can read:
These assays are not intended for use as an aid in the diagnosis of coronavirus
infection"
And:
For research use only. Not for use in diagnostic procedures."
WHERE IS THE EVIDENCE THAT THE TESTS CAN MEASURE THE "VIRAL LOAD"?
There is also reason to conclude that the PCR test from Roche and others cannot even detect
the targeted
genes .
Moreover, in the product
descriptions of the RT-qPCR tests for SARS-COV-2 it says they are
"qualitative" tests , contrary to the fact that the "q" in "qPCR" stands for
"quantitative." And if these tests are not "quantitative" tests, they don't show how many
viral particles are in the body .
That is crucial because, in order to even begin talking about actual illness in the real
world not only in a laboratory, the patient would need to have millions and millions of viral
particles actively replicating in their body.
That is to say, the CDC, the WHO, the FDA or the RKI may assert that the tests can measure
the so-called
"viral load," i.e. how many viral particles are in the body. "But this has never been
proven. That is an enormous scandal," as the journalist
Jon Rappoport points out .
This is not only because the term "viral load" is deception. If you put the question "what
is viral load?" at a dinner party, people take it to mean viruses circulating in the
bloodstream. They're surprised to learn it's actually RNA molecules.
Also, to prove beyond any doubt that the PCR can measure how much a person is "burdened"
with a disease-causing virus, the following experiment would have had to be carried out (which
has not yet happened):
You take, let's say, a few hundred or even thousand people and remove tissue samples from
them. Make sure the people who take the samples do not perform the test.The testers will never
know who the patients are and what condition they're in. The testers run their PCR on the
tissue samples. In each case, they say which virus they found and how much of it they found.
Then, for example, in patients 29, 86, 199, 272, and 293 they found a great deal of what they
claim is a virus. Now we un-blind those patients. They should all be sick, because they have so
much virus replicating in their bodies. But are they really sick -- or are they fit as a
fiddle?
With the help of the aforementioned lawyer Viviane Fischer, I finally got the Charité
to also answer the question of whether the test developed by Corman et al. -- the so-called
"Drosten PCR test"
-- is a quantitative test.
But the Charité was not willing to answer this question "yes". Instead, the
Charité wrote:
If real-time RT-PCR is involved, to the knowledge of the Charité in most cases
these are [ ] limited to qualitative detection."
Furthermore, the "Drosten PCR test" uses the unspecific E-gene assay as preliminary
assay , while the Institut Pasteur uses the same assay as
confirmatory assay .
According to
Corman et al ., the E-gene assay is likely to detect all Asian viruses , while the other
assays in both tests are supposed to be more specific for sequences labelled "SARS-CoV-2".
Besides the questionable purpose of having either a preliminary or a confirmatory test that
is likely to detect all Asian viruses, at the beginning of April the WHO changed the algorithm,
recommending that from then on a test can be regarded as "positive" even if just the E-gene
assay (which is likely to detect all Asian viruses! )
gives a "positive" result .
This means that a confirmed unspecific test result is officially sold as
specific .
That change of algorithm increased the "case" numbers. Tests using the E-gene assay are
produced for example by Roche
,
TIB Molbiol and
R-Biopharm .
HIGH CQ VALUES MAKE THE TEST RESULTS EVEN MORE MEANINGLESS
Another essential problem is that many PCR tests have a "cycle quantification" (Cq) value of
over 35, and some, including the "Drosten PCR test", even have a Cq of 45.
The Cq value specifies how many cycles of DNA replication are required to detect a real
signal from biological samples.
"Cq values higher than 40 are suspect because of the implied low efficiency and generally
should not be reported," as it says in the MIQE guidelines
.
MIQE stands for "Minimum Information for Publication of Quantitative Real-Time PCR
Experiments", a set of guidelines that describe the minimum information necessary for
evaluating publications on Real-Time PCR, also called quantitative PCR, or qPCR.
The inventor himself, Kary Mullis, agreed,
when he stated :
If you have to go more than 40 cycles to amplify a single-copy gene, there is something
seriously wrong with your PCR."
The MIQE guidelines have been developed under the aegis of Stephen A. Bustin , Professor of Molecular
Medicine, a world-renowned expert on quantitative PCR and author of the book A-Z of
Quantitative PCR which has been called "the bible of qPCR."
In a recent podcast interview Bustin points out that "the use of such arbitrary Cq
cut-offs is not ideal, because they may be either too low (eliminating valid results) or too
high (increasing false "positive" results)."
https://www.podbean.com/media/player/znrvk-d932a7?from=usersite&vjs=1&skin=1&fonts=Helvetica&auto=0&download=1
And, according to him, a Cq in the 20s to 30s should be aimed at and there is concern
regarding the reliability of the results for any Cq over 35.
If the Cq value gets too high, it becomes difficult to distinguish real signal from
background, for example due to reactions of primers and fluorescent probes, and hence there is
a higher probability of false positives.
Moreover, among other factors that can alter the result, before starting with the actual
PCR, in case you are looking for presumed RNA viruses such as SARS-CoV-2, the RNA must be
converted to complementary DNA (cDNA) with the enzyme Reverse Transcriptase -- hence the "RT"
at the beginning of "PCR" or "qPCR."
But this transformation process is "widely recognized as inefficient and variable,"
as Jessica Schwaber from the Centre for Commercialization of Regenerative Medicine in Toronto
and two research colleagues pointed out in a 2019
paper .
Stephen A. Bustin acknowledges problems with PCR in a comparable way.
For example, he pointed to the problem that in the course of the conversion process (RNA to
cDNA) the amount of DNA obtained with the same RNA base material can vary widely, even by a
factor of 10 (see above interview).
Considering that the DNA sequences get doubled at every cycle, even a slight variation
becomes magnified and can thus alter the result, annihilating the test's reliable informative
value.
So how can it be that those who claim the PCR tests are highly meaningful for so-called
COVID-19 diagnosis blind out the fundamental inadequacies of these tests -- even if they are
confronted with questions regarding their validity?
Certainly, the apologists of the novel coronavirus hypothesis should have dealt with these
questions before throwing the tests on the market and putting basically the whole world under
lockdown, not least because these are questions that come to mind immediately for anyone with
even a spark of scientific understanding.
Thus, the thought inevitably emerges that financial and political interests play a decisive
role for this ignorance about scientific obligations. NB, the WHO, for example has financial
ties with drug companies, as the British Medical Journal
showed in 2010 .
And
experts criticize "that the notorious corruption and conflicts of interest at WHO have
continued, even grown" since then. The CDC as well, to take another big player, is
obviously no better
off .
Finally, the reasons and possible motives remain speculative, and many involved surely act
in good faith; but the science is clear: The numbers generated by these RT-PCR tests do not in
the least justify frightening people who have been tested "positive" and imposing lockdown
measures that plunge countless people into poverty and despair or even drive them to
suicide.
And a "positive" result may have serious consequences for the patients as well, because then
all non-viral factors are excluded from the diagnosis and the patients are treated with highly
toxic drugs and invasive intubations. Especially for elderly people and patients with
pre-existing conditions such a treatment can be fatal, as we have outlined in the article
"Fatal
Therapie."
Without doubt eventual excess mortality rates are caused by the therapy and by the lockdown
measures, while the "COVID-19" death statistics comprise also patients who died of a variety of
diseases, redefined as COVID-19 only because of a "positive" test result whose value could not
be more doubtful.
...But an analysis of various studies of how different types of UV light interacts with SARS-CoV-2 found that COVID should
disintegrate even more quickly when exposed to summer sunlight, which features more short-wave radiation,
one
reason risk of contracting the virus outdoors during the summer is much, much lower than being indoors in the winter.
In practice, the team found that "inactivation" of virus particles rendered in
simulated saliva was more than 8x faster than scientists believed in conditions similar to summer sunlight.
A July 2020 experimental study tested the power of UV light on SARS-CoV-2, contained in simulated saliva, and found the
virus was inactivated in under 20 minutes.
However, a theory published a month later suggested sunlight could achieve the same effect, which didn't quite add up. This
second study concluded that SARS-CoV-2 was three times more sensitive to UV radiation in sunlight than the influenza A
virus.
The vast majority of coronavirus particles were rendered inactive within 30 minutes
of exposure to midday summer sunlight,
whereas the virus could survive for days under winter sunlight.
"The experimentally observed inactivation in simulated saliva is over eight times
faster than would have been expected from the theory,"
Luzzatto-Feigiz and his team said. "So, scientists don't
yet know what's going on."
The UC Santa Barbara team hypothesized that the process that destroys the virus is similar to a process seen in wastewater
treatment plants.
The team suspects that, as the UVC doesn't reach the Earth, instead of directly attacking the RNA, the long-wave UVA in
sunlight interacts with molecules in the virus' environment, such as saliva, which speeds up the inactivation, in a process
witnessed previously in wastewater treatment.
Their research suggests that an air filtration system equipped with certain types of UVA-emitters
could
dramatically reduce the spread of viral particles indoors.
For some reason, all this research about the effects of sunlight on the virus has been ignored by governments like the Spanish
government, which recently ordered masks to be worn outdoors, something the country's hospitality industry fears will destroy
more already-embattled businesses while contributing nothing to the public safety effort. But maybe soon that will change.
Doom Porn Star
20 hours ago
It was
intentional.
UV and
Vit D were established months ago.
There
are companies that even rolled out airplane sterilizing devices that merely bombard the cabin with intense
UV.
Fools
locked themselves and their children in their homes, Zoomed those meetings instead of meeting in the sun,
watched Netflix and CNN in stead of hiking or going to beach an such, doing what they were told and waiting
for a miracle pill or shot to solve all those lousy lifestyle choices..
HC-CZ
20 hours ago
UV
and vitamin D has been known for centuries, our grandmothers were adamant about getting us out into the
sun.
edotabin
19 hours ago
Lefties are dangerously stupid and gullible people.
Chlorine Dioxide is not bleach. It is an alternative treatment that many people praise and should be very
thoroughly studied by scientists. However, there's no $$$ in it
The
heat will not kill anything off anything if everyone is stuck in their home. Florida, in contrast to other
places, had the worst numbers in the summer. This was probably because everyone there goes inside (AC)
during the summer. If you remember Florida was doing quite well in the winter and spring because everyone is
outside. It is a climate issue that drives behaviors that , in turn, affects transmission.
TBT or not TBT
19 hours ago
Public transport was and remains a big problem. In America proper, unlike in NYC for example, we have
cars, and ample parking. We fixed stupid here.
McStain
17 hours ago
FL has
a very geriatric population. FL deaths should have been off the lying charts.
But
they weren't.
The
northern blue zoo cities had the deaths, generally obese and/or very old.
This
entire fiasco is a scam.
this_circus_is_no_fun
19 hours ago
I was
never crazy about Trump. However, objectively, many of his statements on CV were completely correct,
especially the ones for which he received harsh criticisms.
It's like the flu = CORRECT
We should have opened up last Easter = CORRECT
Hydroxychloroquine is an effective treatment =
CORRECT
Sunlight destroys the virus = CORRECT
Part
of his problem was that he didn't use precise scientific language when he made these statements. Also, since
his enemies would have attacked him anyway, he should have let real experts speak on his behalf and should
never had allowed Faux-chi anywhere near a microphone.
Walter Melon
19 hours ago
He did
let the "experts" speak, including opposing views like Fauci. You may recall Trump was having daily news
conferences for a while there, surrounded by his advisors.
Your
main stream news outlets, though, didn't show that. They just showed the (apparent but not real) gaffes.
How's that make you feel, that critical data was
hidden from you on purpose?
RiverRoad
15 hours ago
How
about that video of Fauci giving the "thumbs-up" to Acosta as he, Fauci, hung back and made sure he was the
last to leave the room. I almost threw up when I saw that.
RiverRoad
15 hours ago
Trump
should have kicked Fauci upstairs to a broom closet somewhere.
Billy the Poet
19 hours ago
Association of American
Physicians and Surgeons -- Why Are Some Governors Blocking Physicians' Attempts to Save Lives in Coronavirus
Pandemic?
While
governors have been handing down orders, doctors in the U.S. and overseas have been reporting remarkable
success in treating COVID-19 patients: reductions in hospitalization, less need for scarce ventilators, less
need for ICU and intubations, and significantly lower death rates.
Several Governors jumped on this
restriction bandwagon soon after President Trump announced at a recent Corona Task Force briefing that
chloroquine and hydroxychloroquine showed hope in treating COVID-19,
based on several small clinical
studies from Johns Hopkins, France, and (at last count) eight other countries. He did not say he recommended
these medicines, as some media have falsely stated.
https://aapsonline.org/why-are-some-governors-blocking-physicians-attempts-to-save-lives-in-coronavirus-pandemic/
philipat
15 hours ago
Rhetorical question Billy?
If
they acknowledge that there are effective cheap generic treatments available for a "disease" with an
overall 99.7% survival rate (99.95% below age 70) there would be no justification for experimental
vaccines with a high incidence of severe AEs and unknown longer-term effects.
And, of course, no vaccines = no "Vaccine Passports" to start the 24/7 surveillance/ID Card regime, the
precursor to the social credit score implementation.
GemJedi
20 hours ago
BS,
the media smacked down anything Trump suggested. If he talked about vitamins and sunlight, the New York
Times would write about Trump trying to kill people because of vitamin toxicity (at absurd levels) and skin
cancer.
Omega Point
20 hours ago
This
has been known for a looong time. Our public officials have been lying. The best defense against any virus
is a healthy immune system.
Don't be Vitamin D deficient
Don't be obese
Where
has this message been? Why haven't our public health officials been promoting this message?
Follow
these rules and a large % of the deaths "attributed" to Covid could have been prevented. But people have
made lifestyle choices to stuff their faces with junk food and not get out in the sun for Vitamin D or take
Vitamin D supplements. Don't force me to wear a mask because you choose to make yourself fat and not go
outside.
Omni Consumer Product
19 hours ago
Because your advice is 100% unprofitable for the pharma-industrial complex
kickasso
17 hours ago
Bingo.
Vaccine production => Big profits.
Vitamin D production => Small profits.
Sign Felled
19 hours ago
(Edited)
So...isolating people indoors, closing fitness centers, limiting their access to "elective" medical care and
restricting their breathing isn't healthy for them? Gosh, who could have imagined that!
Agent Smith
19 hours ago
No but
it is highly profitable
Mr. Magniloquent
19 hours ago
remove
link
My
oldest daughter would have fun helping me tear down the "caution" tape on the playgrounds. My pocket knife
would make quick work of the ***-ties on swings too. Having those shut down for "covid" was one insult too
far. The silver lining, was that stay-at-home orders allowed us to meet a lot of great people. The sheeple
cowered at home obediently, and polite society had a nice times at the park.
Lt. Shicekopf
19 hours ago
Imagine the mindset of locking down playgrounds. Then, imagine a world where the outlaw is the one
unlocking a playground for kids to play and be kids.
HC-CZ
20 hours ago
That
sunlight and UV rays kills virus and bacteria has been known for centuries. The first use of UV lighting for
disinfection was in 1910. It is a technology that has been well established for a very long time.
The
trick that the news used to insinuate that UV light was ineffective was by claiming that UV did not kill
COVID. Technically true, as noted, it doesn't kill it. It just renders it ineffective.
Trump
proven right, again.
12Doberman
20 hours ago
(Edited)
There
is debate as to whether viruses are even "alive."
TBT or not TBT
18 hours ago
Irrelevant, if ionizing radiation wrecks the instructions encoded in the virus. UV damages the bonds in
genetic molecules. UV photon energy well exceeds that needed to break such bonds.
Wayoutwilly
16 hours ago
remove
link
Yeah,
all these fvckers are liars.
I am a
believer on the sunlight though. I've worked outdoors all my life and had one case of seasonal flu in my 35
+ years of adulthood.
never
had a flu shot and never will.
Boris Badenov
15 hours ago
This
explains why the LOCKDOWNS seemed to target natural Vitamin D : Its the SUNLIGHT
ITSELF
stupid:
1)
Close BEACHES, ban OUTDOOR Sports, close PLAYGROUNDS
2)
Cover your FACE, stay INDOORS, No Walking around in Los Angeles
3)
Explains why The SUNSHINE STATE is doing so well.
How
could the CDC and Fauci be EXACTLY
PRECISELY
180
degrees wrong?
insanityantidote
17 hours ago
UV
light and vitamin D in sunlight. By all means stop the lockdowns and let people live.
Faeriedust
16 hours ago
Problem being that that only works in rural areas where people actually
go
outside
for prolonged periods of time. In cities, access to limited green space is subtly limited to
those in the upper middle class and above, and people spend 10 months out of the year and 9 hours out of
the day in small, cramped indoor spaces with low-level lighting. They become so used to this that they
complain when entering my own house or office, where I attempt to keep the lighting at a level of at
least 1/3 that typical outdoors. They say it's
too
bright
and happily fill their light fixtures with fraudulently-sold "60-watt
equivalent
"
lightbulbs that provide only 77% of the light of the old 60-watt bulbs they're sold to replace. The only
exposure to ultraviolet radiation that they get is those with enough money to bake themselves in "tanning
beds". Because, you know,
real natural (free)
world BAD
,
fake world (manufactured and sold
to you) GOOD
.
Let
the idiots die and good riddance. Evolution has to be good for
something
.
Confining people in badly ventilated apartments during the quarantine was a serious misstep.
If apartment has a patio (on the first floor) or balcony that somewhat can be compensated, but if
not that is clearly harmful for the health of people, especially children and was a blunder.
Another Fauci blunder so to speak.
Tall_Tom 19 hours ago
Based on CDC data on sterilization of corona viruses in general, I calculated a half life
of about 12-15 seconds in full sun exposure last spring. To reduce virus to 1 part in a
million, which is roughly 2^20, would take 4-5 minutes. This is the level generally
recommended as sterile for viruses. Obviously this is only for item in full sun. Your car is
basically sterile for this reason after a few minutes, and doesn't need disinfection...ever.
And high temperatures help this as well.
And yet Spain bleached a beach. I guess they don't understand that the beach gets sun
exposure.
el_buffer 17 hours ago
Well friggin duh.
It's RADIATION.
You think those UV generators in hospitals are there for a TikTok black-light
dance-party?
UV light smashes nucleotide chains into pieces faster than an Antifa near a glass
window.
Oh...and in doing so...causes CANCER.
curiousweb 17 hours ago
Not Far-UVC. Apparently kills airborne viruses very fast at low energy dosages within a
wavelength harmless to humans. Can be used continuously.
https://www.nature.com/articles/s41598-020-67211-2
Faeriedust 16 hours ago
Ever heard of an ancient saying, "Moderation in all things"? Works for most health
treatments, too.
19331510 19 hours ago
The study helps explain the seasonality of the corona virus and which also begs the
question, why are we vaccinating at the end of the flu season?
Notable quotes:
"... Should Merck succeed in demonstrating that molnupiravir is effective and free of serious side effects, it could be a boon to the company, and to society, for many years to come. ..."
"... Viruses are uniquely difficult to attack with drugs. They hijack human cells and set up machinery to churn out copies of themselves, creating a challenge: destroying the virus without harming the cells. Success, when it comes, can be fleeting, because viruses mutate to survive. ..."
"... It interferes in replication, preventing a threat from causing severe infection. Molnupiravir doesn't stop the virus from replicating, though; instead, the drug introduces errors into the virus's RNA that are then replicated until it's defunct. ..."
"... With antivirals such as this, "basically you're going to put a piece of sand in the gears and hope it stops the impact of the virus," says Gomez, the former Niaid scientist. ..."
The antiviral drug molnupiravir, still in clinical trials, would give doctors an important new treatment and a weapon against coronaviruses and future pandemics
Drugmakers see an opportunity to add to the arsenal of potential therapies. There are 246 antivirals in development, according to the
Biotechnology Innovation Organization
, an industry trade group. And companies as big as
Pfizer Inc.
and as little-known as
Veru Inc.
are testing them in pill form. Merck's molnupiravir is among the furthest along. Its developers hope the pills can be
prescribed widely to anyone who gets sick. Think Tamiflu for Covid.
The hurdle, beyond ensuring the drug works, is making sure it's safe. Developers of antivirals have been dealing with the thorny issues
they pose for decades. Should Merck succeed in demonstrating that molnupiravir is effective and free of serious side effects, it could
be a boon to the company, and to society, for many years to come.
Viruses are uniquely difficult to attack with drugs. They hijack human cells and set up machinery to churn out copies of themselves,
creating a challenge: destroying the virus without harming the cells. Success, when it comes, can be fleeting, because viruses mutate
to survive.
The first antiviral approved in the U.S. was idoxuridine, a herpes treatment regulators green-lit in 1963, generations after the discovery
of antibiotics. It's among a widely used class of drugs called nucleoside analogues -- synthetic versions of nucleosides, critical building
blocks of DNA and its counterpart, RNA, the messenger molecule that delivers instructions to a cell's protein-making factories. Nucleoside
analogues prevent viruses from replicating, or from replicating effectively, inside cells.
Concerns that idoxuridine was toxic to the heart led it to be recommended only for topical use -- the sort of hurdle that kept antiviral
drug development slow. The AIDS crisis of the 1980s invigorated the field. "Until HIV came along, there were precious few antivirals,"
says Saye Khoo, a professor of pharmacology and therapeutics at the University of Liverpool. Rising death rates and the public outcry
about the virus prompted companies and governments to pour millions of dollars into an area that hadn't seen that kind of investment
before.
The breakthroughs were meaningful. Khoo says scientists discovered that some people appeared to have a
natural resistance
to getting HIV -- they lacked a receptor allowing the virus to enter cells -- leading to a new class of drugs. They
also realized that antivirals would need to be adaptable enough to deal with mutations, and that potent combination therapies involving
multiple drugs could prevent the evolution and spread of drug resistance. At the same time, some of the new treatments had serious side
effects, including anemia and liver problems, pushing drugmakers to continually improve upon their treatments.
During this era, the U.S. government also started to boost its pandemic preparedness, with an emphasis on guarding against bioterrorism.
President Bill Clinton, alarmed after reading the Richard Preston novel
The Cobra Event
, in which a terrorist unleashes a virus that causes a fictional ailment called brainpox, convened a group of
cabinet members and scientists in April 1998 to assess such threats. That led to the formation of what's now called the
Strategic National Stockpile
, whose objective was to have enough emergency medicines and materials to deploy within 12 hours of
an official request in times of crisis.
Following the Sept. 11 and anthrax attacks of 2001, the Bush administration directed the stockpile
to procure products such as smallpox vaccines. Then, in 2006, Congress authorized the formation of the Biomedical Advanced Research
and Development Authority, or
Barda
, to help develop treatments and vaccines for public-health threats.
Pharma's next major advance in antivirals came in 2013, a $1,000-per-pill hepatitis C cure produced by Gilead. The company was
roundly criticized
for setting so high a price for such a widely used drug...
... ... ...
The chemical compound on which molnupiravir is based -- C9H13N3O6, or N4-hydroxycytidine -- has been known for decades. Like idoxuridine,
the herpes drug, it's a nucleoside analogue. It interferes in replication, preventing a threat from causing severe infection. Molnupiravir
doesn't stop the virus from replicating, though; instead, the drug introduces errors into the virus's RNA that are then replicated until
it's defunct.
With antivirals such as this, "basically you're going to put a piece of sand in the gears and hope it stops the impact of the virus,"
says Gomez, the former Niaid scientist. But, he adds, stopping the virus by creating errors in the genetic code or through other means
can come with unintended consequences. "You don't know where the sand might end up in the other parts of the body." A company called
Pharmasset Inc.
(a hepatitis C drugmaker Gilead bought in 2011) investigated molnupiravir's main ingredient around the turn of the
century, but it abandoned development over concerns that it was mutagenic, meaning it could lead to birth defects.
Painter dusted off the chemical structure of molnupiravir years ago. Prompted by a concern raised by the
Defense Threat Reduction Agency
, a unit of the U.S. Department of Defense, he was looking for a countermeasure against weaponized
Venezuelan equine encephalitis, the stuff of
Cobra Event
-level nightmares. A chemist who holds 45 patents, some for hepatitis B and HIV antiviral drugs in use today, Painter
has made a career of bridging the gap between academic drug discovery and the biotech and pharma industries that get treatments across
the finish line. He took the chemical structure that Pharmasset had once studied and screened it against a wide range of viruses, including
SARS and MERS. In late 2016 he made it possible to use in pill form by modifying that chemical structure into a "prodrug," which meant
the compound would break down in the body, allowing the part that interferes with viral replication to be properly absorbed into the
bloodstream.
After his initial research, Painter settled on influenza, an ever-present threat, as molnupiravir's first target and prepared to launch
an NIH-funded safety trial in early 2020. He also applied for funding from Barda but didn't get it. Rick Bright, then the agency's director,
later noted in a
whistleblower complaint
about the Trump administration's pandemic response that, though his supervisor at the
Department of Health and Human Services
was excited about molnupiravir and wanted to fund it, Bright had been reluctant to invest
when it was first presented to him in the fall of 2019. Other nucleoside analogues had caused birth defects in animals, and he wanted
more safety data before signing off.
... ... ...
uncle tungsten , Apr 1 2021 21:20 utc |
44
Fnord13 #13
Have you ever heard the saying "Science advances one funeral at a time"?
Yes, it was Max Planck Science progresses funeral by funeral.
I like that saying. Perhaps it is equally applied as:
Pharmaceutical approvals advance one funeral at a time
Raytheon advances funeral by funeral
Peace in Yemen advances funeral by funeral
Usastan advances funeral by funeral
enough! bleak moment.
Orage , Apr 1 2021 18:26 utc |
3
The EU handling of the vaccine supply has also caused splits within the EU. Many countries
including Austria, Hungary and Czech republic are going to be using the Sputnik vaccine
despite it not being approved by the EMA. This is a definite ite deplomatic win for Russia
and further shows that these countries will no longer sacrifice national interest when
ordered to do so.
ian , Apr 1 2021 18:35 utc |
6
"Most scientists agree ..."
Science is not about consensus. It is about what can be proved with a repeatable
experiment.
Norwegian , Apr 1 2021 18:36 utc |
7
@ian | Apr 1 2021 18:35 utc | 6
Thank you, you are exactly right. Science is not determined by voting.
cirsium , Apr 2 2021 20:58 utc |
95
@Arius Armenian, 71
The experimental mRNA injections are not vaccines. They do not give immunity or prevent
transmission. Their purpose is to mitigate symptoms so that the sick person does not get sick
enough to require hospitalisation and emergency approval was given on that basis.
Typically vaccines, such as the one for measles, provide lifelong immunity. It is unclear how
coronavirus vaccines fair against mutations of COVID-19. The question is can vaccinated people
provide for COVID-19 the new platform for mutations.
Efficiency is probably aroun 80% ( if calculated as (850-77)/(850+77) ) not 91% as the
article claims.
The Covid-19 vaccine from Pfizer Inc. and BioNTech SE remains highly effective six months
after its second dose, an indication that protection could last for an even longer period.
The findings, released on Thursday, emerged from a continuing review of how volunteers in
the shot's late-stage trial were faring and whether they contracted Covid-19 with symptoms.
... Of the 927 cases of symptomatic Covid-19 observed through March 13, 850 were in people
who received a placebo and 77 in people who were vaccinated, according to the companies.
That corresponds to a vaccine efficacy of 91.3% up to six months after getting the second
dose, Pfizer and BioNTech said.
The protection remained generally consistent across age, gender, race and ethnicity, as well
as among individuals with underlying health conditions, the companies said.
The vaccine was also 95% to 100% effective against severe disease, with the precise figure
depending on whether researchers used a definition of severe disease from the U.S. Centers for
Disease Control and Prevention or one from the U.S. Food and Drug Administration.
Some 800 trial subjects were enrolled in South Africa, where a more contagious variant of
the virus was first identified. Among those volunteers, there were nine cases of Covid-19, all
in people who got a placebo. Sequencing confirmed six of the nine cases were of the variant.
...the vaccine generated a slightly lower immune response against the variant than the more
common strain circulating in the U.S., but was
still effective at neutralizing the variant virus .
Of the 697 cases of symptomatic Covid-19 among study subjects in the U.S., 647 were in
people who received a placebo, with the rest in vaccinated subjects, indicating 92.6% efficacy,
according to the companies.
...They are also in discussions with regulators about studying a tweaked version of their
vaccine that researchers designed to protect against the variant found in South Africa.
Pfizer has previously said it anticipates producing the Covid-19 shots for at least several
years on the expectation that booster shots will be needed annually or every few years to
maintain protection.
There are a lot of issues with vaccine rollout. One issue is that they do not check if a person has immunity to
the virus or not.
Another issue is how long vaccine will be effective is the next year we might face yet another strain of the virus.
Coronaviruses are mutating viruses and that's why previous attempts to create vaccine failed.
Are those people who demonstrate a severe reaction to the vaccine the same people who would get severe case of COVID-19 if
infected ?
Yes another issue is "emergency use". Long time effects are not known. We do not know why immunity for some people do not emerge
and they became ill even after being immunized. We do not know how long immunization status hold. Will it weaken in six months
to the level when infection became possible again or. and how effective it is against new strains.
So this rush with vaccine rollout is a large scale biological experiment with uncertain consequences.
In this sense any skeptic is valuable.
Notable quotes:
"... and then that test came back negative. ..."
"... suspected but unconfirmed ..."
Alex Berenson- The Pandemic's
Wrongest Man - The Atlantic
Derek Thompson, Staff writer at The Atlantic
For the past few weeks on Twitter, Berenson has mischaracterized just about every detail regarding the vaccines
to make the dubious case that most people would be better off avoiding them. As his conspiratorial nonsense accelerates
toward the pandemic's finish line, he has proved himself
the
Secretariat of being wrong
:
Usually, I would refrain from lavishing attention on
someone so blatantly incorrect. But with vaccine resistance
hovering
around 30 percent of the general population, and with 40 percent
of Republicans saying they won't get a shot, debunking
vaccine skepticism, particularly in right-wing circles, is a matter of life and death.
Jon D. Lee: The utter familiarity of even the strangest vaccine conspiracy theories
Berenson's TV appearances are more misdirection than
outright fiction, and his Twitter feed blends internet-y irony and scientific jargon in a way that may obscure what he's
actually saying. To pin him down, I emailed several questions to him last week. Below, I will lay out, as clearly and
fairly as I can, his claims about the vaccines and how dangerously, unflaggingly, and superlatively wrong they are.
Before I go point by point through his wrong
positions, let me be exquisitely clear about
what is true
. The vaccines work. They
worked in the clinical trials, and they're working around the world. The vaccines from Pfizer-BioNTech, Moderna, and
Johnson & Johnson seem to provide
stronger
and more lasting protection
against SARS-CoV-2 and its variants than natural infection. They are
excellent
at reducing symptomatic infection
. Even better, they are extraordinarily
successful
at
preventing severe illness from COVID-19. Countries that have vaccinated large percentages of their population quickly, such
as the U.S., the United Kingdom, and Israel, have all seen sharp and sustained declines in hospitalizations among the
elderly. Meanwhile, countries that have lagged in the vaccination effort -- including the U.K.'s neighbors France and Italy,
and Israel's neighbor Jordan -- have struggled to contain the virus. The authorized vaccines are marvels, and the case against
them relies on half-truths, untruths, and obfuscations.
me title=
me title=
Berenson's claim:
In country after country, "cases rise after vaccination campaigns begin," he wrote in an
email.
The reality:
In
country after country, cases decline after vaccination campaigns begin.
One of Berenson's themes is that the mRNA vaccines
are badly underperforming outside the clinical trials and are possibly even causing a spike in cases after the first shot.
But just this week, CDC researchers studying real-world conditions came to the opposite
conclusion
:
The mRNA vaccines by Moderna and Pfizer are 90 percent effective two weeks after the second dose, in line with the trial
data. "COVID-19 vaccination is recommended for all eligible persons," they concluded.
Still, Berenson pushes the argument that the vaccines
are causing suspicious illness and death. On
Twitter
and
in his email to me, Berenson claimed that
an
"excellent" Denmark study
showed a 40 percent rise in infections immediately after nursing-home residents received
their first vaccine shot.
I reached out to
that
study's lead author
, Ida Rask Moustsen-Helms at the Statens Serum Institut, who said that Berenson had mischaracterized
her findings. She explained to me that the Danish nursing homes in question were already experiencing a significant
COVID-19 outbreak when vaccinations began. Many people in the long-term-care facilities were likely already sick before
their vaccine was administered, and "these people would technically count as vaccinated with confirmed COVID-19, even if
the infection happened prior to the vaccination or its immune response," she said. With limited vaccines, countries ought
to give the first vaccines to the groups most likely to get COVID-19. That's exactly what seems to have happened here.
Berenson is scaremongering about the vaccines by essentially criticizing their wise distribution.
In our emails, Berenson further argued that many of
the perceived benefits of the vaccines are illusory. "It is very hard to distinguish the course of the epidemic this winter
in countries that have vaccinated heavily, such as Israel and the UK, and those that have not, such as Canada and Germany,"
he wrote.
This is hogwash. In the U.K. and Israel,
hospitalizations have fallen by at least 70 percent since mid-January, and they remain low. In
Canada
,
hospitalizations fell by significantly less, and in Germany, the seven-day average of COVID-19 cases has more than
doubled
since
mid-February; its government has
debated
a new lockdown
.
This stage of the pandemic is a race between the
variants and the vaccines. In many states, such as Michigan and New York, normalizing behavior combined with more
contagious strains of the virus are pushing up cases again. This is not evidence that America's vaccination campaign isn't
working. Quite the opposite: It highlights the urgency of moving faster to deliver vaccines, which are our best chance to
control the spread of contagious variants.
Berenson's claim:
Pfizer-BioNTech's clinical-trial data prove that the companies are being shady about vaccine
efficacy.
The reality:
His
"proof" is a total mischaracterization of trial data.
Berenson seems to enjoy spelunking through research to
find esoteric statistics that he then dresses up with spooky language to make confusing points that sow doubt about the
vaccines. Arguing that COVID-19 cases spike after the first dose, he
directs
people
to the
Pfizer-BioNTech
FDA briefing document
, which reports hundreds of "suspected but unconfirmed" COVID-19 cases in the trial's vaccine
group that aren't counted as positive cases in the final efficacy analysis.
me title=
me title=
But "suspected but unconfirmed" doesn't refer to
participants who were probably sick with COVID-19. On the contrary, it refers to participants who reported various
symptoms, such as a cough or a sore throat, and then took a PCR test --
and then that test
came back negative.
"His point is absolutely stupid, and I would know
because I enrolled participants in the Pfizer-BioNTech trial," Kawsar Talaat, an assistant professor at Johns Hopkins
University, told me. "He's talking about people who call in and say, 'I have a runny nose.' So we mark them as 'suspected.'
Then we ask them to take a PCR test, and we test their swab, and if the test comes back negative, the FDA says it's
'unconfirmed.' That's what
suspected but unconfirmed
means."
Read: Coronavirus reinfection will soon become our reality
When I emailed Pfizer and BioNTech representatives
about Berenson's claim, they struggled to even understand what I was talking about. Someone was taking a group of several
thousand people who had tested negative for COVID-19 and, from afar, diagnosing all of them with COVID-19? "Does not make
sense," a BioNTech spokesperson responded curtly.
If you were enrolled in Berenson's vaccine trial for
SARS-CoV-2 and never contracted the virus, but one day you told a clinician that you had a bit of a cough, Berenson would
mark you down as "infected with COVID-19" and blame the vaccine. That's the logic here, and, as you can tell, it's not
really logic; it just seems like an attempt to find something -- anything -- wrong with the vaccines.
Berenson's claim:
The mRNA vaccines dangerously suppress your immune system, possibly causing severe illness
and even death.
The reality:
His
claim is based on a total misunderstanding of how the immune system works.
Berenson wrote in an email that "the first dose of
the mRNA vaccine temporarily suppresses the immune system." He has claimed on
Twitter
that
the mRNA vaccines "transiently suppress lymphocytes," or our white blood cells, and suggested that this might lead to
"post-vaccination deaths."
Scientists tore this one to shreds. "The claim he is
making is simply fearmongering, connecting a simple physiological event with bogus claims of deaths," Shane Crotty, a
researcher at the Center for Infectious Disease and Vaccine Research at the La Jolla Institute for Immunology, told me.
"The observation of lymphocyte numbers temporarily dropping in blood is actually a common phenomenon in immune responses."
Renee DiResta: Anti-vaxxers think this is their moment
A little background is useful here: White blood cells
are the immune system's scouts. After an effective vaccination, some of them leave the blood and go to the site of
inflammation, such as the arm that received the shot. "The cells are not gone," Crotty said. "They come back to the blood
in a few days. It is generally a good sign of an immune response, not the opposite." To demonstrate that the vaccines are
counterproductive, then, Berenson is pointing to the very biological mechanism that strongly suggests they're working just
as scientists expected.
me title=
me title=
Readers are surely familiar with other biological
events that sound bad in the short term but are part of a normal, healthy process. When you lift weights at the gym, your
muscles experience small tears that recover and then strengthen over time. Imagine if some loudmouth started screaming in
the middle of the weight room, "You all think you're building your muscles, but actually you're tearing them to shreds, and
it could kill you!" You would probably carry on calmly, assuming that this guy just got a little overexcited after finding
a Yahoo Answers article about muscle formation and stopped reading after the first paragraph. Berenson's claim is basically
a version of that, but for your immune system.
"Actually," Talaat said, "his argument is even worse
than your analogy. Muscles really do tear at the gym. But lymphocytes don't go away. They just move. What he's describing
as dangerous in these tweets is just the regular functioning of our immune system."
Berenson's claim:
In Israel, the shots are causing a scary number of deaths and hospitalizations.
The reality:
Israel
is a sensational vaccine success story: a nearly open economy where COVID-19 rates are plunging.
See
for yourself!
On February 11, Berenson
warned
his
followers that early data from Israel proved that vaccine advocates "need to start ratcheting down expectations." This was
a strange claim to make at the time: An Israeli health-care provider had
reported
no
deaths and four severe cases among its first 523,000 fully vaccinated people. But the claim seems even more ridiculous now,
in light of Israel's incredible success since then. New positive cases in Israel are down
roughly
95 percent
since January. Deaths have plunged, even though the economy is
almost
fully open
.
When I asked Berenson to explain his beef with
Israel's vaccine record, he sent
a
link to a news story in Hebrew
that, he said, reported "several hundred deaths and hospitalizations and thousands of
infections in people who have received both doses." I can't read Hebrew, so I reached out to someone who can, Eran Segal, a
computational biologist at the Weizmann Institute of Science, in Rehovot, Israel. He replied by email: "This link actually
shows that the vast majority of those who died were NOT vaccinated." By Segal's calculations, the vaccines have reduced the
risk of death by more than 90 percent in the Israeli population. Segal also said that "numbers of infections only went
down, and even more so among the age groups who were first to vaccinate."
Berenson is wrong about all sorts of little things
when it comes to Israel, but I want to emphasize how straightforward and obvious the big picture is here. Israel is
a
world leader in vaccinations
. Its COVID-19 cases have plunged, and its economy is roaring back to life.
Berenson's claim:
Healthy people under 70 shouldn't get a vaccine.
The reality:
Outside
of extremely rare cases, every adult should get a vaccine -- and if it's authorized for children, children should get it
too.
I wanted to know where Berenson stood on the most
important question: Who does he think should get a vaccine, and who does he think shouldn't? This was the core of his
answer:
For most healthy people under 50 -- and certainly under 35 -- the side effects
from the shots are likely to be worse than a case of Covid. Over 70, sure. The grey zone is somewhere in the middle and
probably depends on personal risk factors.
This response has two huge problems. First, although
the disease clearly gets more severe with age, drawing a line at 70 is nonsensical. Those in their 50s and early 60s are
three times more likely to die from this disease than a 40-something, and
400 times
more
likely to die than a teenager, according to the CDC.
Vax-r-us March 29, 2021 at
6:02 pm GMT • 2.3 days ago
According to virologist and vaccine expert, Geert Vanden Bossche, this experimental
procedure causes the recipients body to start producing antibodies specific for Covid but
practically eliminates a bodies natural ability to produce antibodies capable of eliminating
Covid variants or any other diseases.
In other words, taking the jab ruins our natural immune system. Those who have been
"vaccinated" and travel around freely become super-spreaders of the variant mutations. Notice
the recent news reports indicating a rising number cases involving covid variants.
An interview with Mr. Bossche:
https://centipedenation.com/first-column/virologist-and-vaccine-expert-geert-vanden-bossche-risks-reputation-and-career-by-speaking-out-against-administration-of-covid19-vaccines/
Brian Reilly March 29, 2021 at
6:43 pm GMT • 2.3 days ago
Very well put, but the window is closed. We are all going to have to pass through the
totalitarian crucible (maybe gauntlet is a better term) unless we die along the way. Too many
people have bought into this nonsense for sense to prevail without a brutal systemic failure.
And it will be a while, so make a point of putting some relevant time capsules together so
that the people of the future will have some real hard copy to study, as the electronic files
will not survive.
Wade March
29, 2021 at 7:59 pm GMT • 2.2 days ago
@Vax-r-us
I listened to this interview but why does this jab do that but others (flu, measles, hpv,
etc ) do not do the same thing?
I get that part of his argument is that this vaccine is "leaky", that is to say it doesn't
stop the virus but accelerates its evolution/mutation rate. However, I still didn't grok the
way this vaccine is different in terms of compromising our natural immunity compared to other
vaccines which apparently don't (Bossche is not complete anti-vax).
guttersnipe March 29, 2021 at
10:28 pm GMT • 2.1 days ago
@Wade
previous vaccines primed the immune system by using offensive dead or attenuated virus
combined with other junk designed to piss off your system.
mRNA vaccines actually create the offending particles by burrowing into your cells and
using them as partial Covid spike protein factories. this REALLY pisses off your immune
system. and it is feared it could cause cytokine storms (dangerous excessive immune response)
upon exposure to the wild virus.
among other things.
Adam Smith March 30, 2021 at
4:01 am GMT • 1.9 days ago
@Wade hat
should have conferred immunity.
WHO
and UNICEF said in a joint statement the polio outbreak in the Philippines is concerning
because it is caused by vaccine-derived poliovirus type 2.
Nearly
all the cases of polio in the modern world are caused by polio vaccines.
michael888 March 30, 2021 at
12:39 pm GMT • 1.5 days ago
@Vax-r-us ts
rid of the plasma cells making them within a few months.
Our authorities have rejected the use of pharmacological treatments (such as
glucocorticoids in serious cases to dampen cytokine storm, published by Chinese for treating
Covid-19 in March, 2020) and aspirin, to minimize clotting from Covid-19. There are a host of
well-understood approved drugs that in combination may be effective prophylactically. As most
of the censored dissident scientists have noted, just keeping healthy and avoiding vitamin/
nutrient deficiencies (a major problem in the elderly) may be enough to avoid serious case of
Covid-19 without vaccines.
The European Union
's drugs regulator said a link between AstraZeneca Plc 's Covid-19 vaccine and a rare
type of blood clot is possible, identifying at least 62 cases of the condition while insisting
the shot's benefits still outweigh its risks.
The comments further cloud the picture around the vaccine after Germany restricted it to
older people this week amid growing concerns about side effects. That could slow Europe's
already lagging immunization program as virus cases surge anew.
The European Medicines
Agency said its safety committee will probably issue an updated recommendation next week.
If the panel concludes there's a connection between the clots and Astra's vaccine, the EMA will
change its recommendations to patients and health-care officials, Executive Director Emer Cooke
said.
"At the moment, at this stage of our investigations, the link is possible, and we cannot say
any more than that at this point," Cooke said in a press conference. For now, there's no
evidence to support restricting use of the vaccine in any population of people, she said.
... .... ....
Concerns surrounding the Astra shot have focused on an unusual type of blood clot known as
cerebral venous sinus thrombosis. It's associated with a low number of blood platelets and
occurs most commonly in women between the ages of 30 and 45 -- a group that, in the EU, has
been disproportionately vaccinated with Astra's shot, EMA officials said.In individuals under
the age of 60, health authorities are seeing more cases of the rare clots in people who
recently got the Astra vaccine than would be normally expected, said Peter Arlett, EMA's head
of pharmacovigilance and epidemiology. The agency has identified about one report per 100,000
people under the age of 60 who got the vaccine in the European economic area. It hasn't yet
been able to identify specific risk factors, however, such as age, gender or previous medical
history of clotting disorders.
The figure of 62 cases of the rare clots includes all side effects reported in the EMA's
EudraVigilance system, which includes cases both in and outside Europe, the agency said.
The count dates to March 22, and additional cases have occurred since then.
Looking beyond the rare clots, most of the adverse reactions reported in patients who had
received Astra's vaccine occurred in the U.K., where it has been used most and where the
government has defended the homegrown shot. A March 8 review identified 246 reactions
involving various types of artery blockages or blood clots in Britain, including a range of
conditions. That's out of 269 instances in a dozen countries, which included about 40 deaths,
the regulator
said . Just because the reactions were reported after vaccination doesn't mean they're
linked to the vaccine.
So, the New Normals are discussing the Unvaccinated Question. What is to be done with us?
No, not those who haven't been "vaccinated" yet. Us. The "Covidiots." The "Covid
deniers." The "science deniers." The "reality deniers." Those who refuse to get "vaccinated,"
ever.
There is no place for us in New Normal society. The New Normals know this and so do we. To
them, we are a suspicious, alien tribe of people. We do not share their ideological beliefs. We
do not perform their loyalty rituals, or we do so only grudgingly, because they force us to do
so. We traffic in arcane "conspiracy theories," like "pre-March-2020 science," "natural herd
immunity," "population-adjusted death rates," "Sweden," "Florida," and other heresies.
They do not trust us. We are strangers among them. They suspect we feel superior to them.
They believe we are conspiring against them, that we want to deceive them, confuse them, cheat
them, pervert their culture, abuse their children, contaminate their precious bodily fluids,
and perpetrate God knows what other horrors.
So they are discussing the need to segregate us, how to segregate us, when to segregate us,
in order to protect society from us. In their eyes, we are no more than
criminals , or, worse, a plague , an infestation. In the
words of someone (I can't quite recall who), "getting rid of the Unvaccinated is not a question
of ideology. It is a question of cleanliness," or something like that. (I'll have to hunt down
and fact-check that quote. I might have taken it out of context.)
In Israel
,
Estonia , Denmark
,
Germany , the
USA , and other New Normal countries, they have already begun the segregation process. In
the UK , it's just a matter
of time. The WEF, WHO, EU, and other transnational entities are helping to streamline the new
segregation system, which, according to the WEF, "
will need to be harmonized by a normative body, such as the WHO, to ensure that is ethical
."
Cowboy March 29, 2021 at
4:26 pm GMT • 2.4 days ago
@follyofwar
Nice thoughts but the high priests of the new secular cult of scientism are playing a zero
sum game. It's an either/or for them; slavery or scalp. The rituals of the cult reinforce the
dogma. The continual washing of hands as an act of purification. The mask as an act of
penance for your defiling breath. Forced solitude to keep you in front of the 24 hour Cult
broadcasts on tv. Social distancing as a way to inculcate insular thinking. Any resistors to
the new rituals will be brought to a tribunal of neo torquemadas. Perhaps a better way to be
thinking of the resistance is in terms of knighthood.
Auntie
Analogue March 29, 2021 at
5:25 pm GMT • 2.3 days ago
A black market trade in forged been-vaccinated-passports should be expected to debut and
thrive.
,
Sollipsist March 30, 2021 at 4:04
am GMT • 1.9 days ago
The pawpaw and the goat are both listed in stable condition for now.
The sheep, of course, tested negative and has since received 8 marriage proposals from
relieved Tanazanian suitors.
Ilya G
Poimandres
March 26, 2021 at 5:51 am GMT • 4.4 days ago
Some Ape: "you are not vaccinated, don't come near me!".
Me: "but you are, so you are immune from the virus – whaddayou care about me?!".
Ape: "this vaccine does not provide full immunity".
Me: "then it's not a vaccine, is it!".
Ape: "heretic!!!".
RegretLeft
March 26, 2021 at 2:43 pm GMT • 4.0 days ago
Kansas City Council Woman DEAD Hours After Receiving Experimental COVID Injection
https://vaccineimpact.com/2021/kansas-city-council-woman-dead-hours-after-receiving-experimental-covid-injection/
" immediately suffered anaphylaxis, a severe allergic reaction, during the 15-minute
waiting period after the experimental shot. She was transported to Stormont Vail Health in
Topeka, where she was pronounced dead "
she was 68 – sounds like she was dead in about 15 min.
Why nobody answer the question how long vaccine will be effective for this mutating
coronavirus. Pfizer CEO has had the audacity to suggest that people should be vaccinated each
year. Bit as we know "Ye cannot serve God and mammon"; so any such CEO pronouncement should be
taken with a grain of salt. He is a corporate crook first and foremost trying to maximize the
profits at the expense of people. In 2009 Pfizer was assessed the largest fine in history for
deliberate medical fraud
https://www.justice.gov/opa/pr/justice-department-announces-largest-health-care-fraud-settlement-its-history
but after lengthy appeals their attorneys managed to get the judgment reduced by almost two
billion dollars.
In the study of efficiency of Pfizer vaccines out of 36,000 participants split into two
groups (one greo got real vaccine, the other placebo), nine vaccinated participants became
infected with the virus, compared with 169 individuals injected with the placebo. But one
individual in the vaccinated group had a sever case of COVID-19 which raises a lot questions. Why
this could ever happen?
So the vaccine in not 100% protective even against the strain of the virus it was developed
for. But there is a difference both in the number of infected and the outcomes in two groups. We
cannot presume that the experiences of 19,000 vaccinated individuals will extrapolate to millions
of people. For example, it's impossible to detect less common side-effects. It is clear that the
efficiency of the vaccine in real world will be lower than in controlled groups study and side
effects might be more pronounced.
The open question is whether it will provide any protection in one year. It's almost certain
that the immune response initially generated will wane over time. If not, this is a very
questionable initiative: taking substantial risk for very little temporary benefit. It is also
unclear whether it will be effective against new strains, or vaccinated people will serve as a
catalysts for the development of new strains.
That's why previously there were no vaccines against the coronaviruses at all. The second
question is whether vaccinated people can curry and spread the virus beciang a danger to all
other people. And the last is whether vaccinated people will became a platform for development of
the new strains of the virus. And we now know that it is possible to became infected aeven after
being vaccinated, so vaccinated people can serve as the platform for development of new strains
of the virus.
my intention is not to criticize the vaccines themselves, but the manner by which they are
being shoved down our throats. That, I object to strongly because it violates the people's
right to informed consent. A lopsided, nationwide public relations blitz that relentlessly
glorifies vaccines while deliberately excluding even the slightest criticism from respected
professionals, does not respect the rights of the people. It's brainwashing, pure and
simple.
And why have behavioral psychologists been employed by the government to promote the
vaccination campaign? Why have they concocted a strategy designed "to change people's beliefs
and feelings about vaccination" to inform "people about the prosocial benefits of vaccination",
and to "intervene on behavior directly", which means that you're given an appointment, and told
that you will be getting your vaccination at the end of the session." Psychologists call this a
"presumptive recommendation" which effectively eliminates the element of personal choice by
creating a scenario in which getting vaccinated is a fait accompli. How is this not
coercion?
It is coercion, subconscious coercion. The doctor is strong-arming the patient into getting
vaccinated by making it look like its standard procedure. That puts pressure on the patient to
follow the path of least resistance, which is compliance. It's a clever tactic, but it is also
transparently manipulative.
The behavioral psychologists who have helped to shape the government's policy, believe that
the emphasis should be placed on the "safety and effectiveness" of the vaccines. That's the
cornerstone for building public support. At the same time, they show no interest in providing
evidence that would support their claims, which suggests that "safe and effective" is nothing
more than a meaningless bromide that is invoked to dupe the sheeple into getting
inoculated.
You might have also heard the term "vaccine hesitancy" used to describe the people who have
decided not to get vaccinated. The moniker is clearly intended to denigrate vaccine skeptics by
suggesting that they have a mental condition, like paranoid schizophrenia. This is an effective
way to discredit one's enemies, but it also shows the glaring weakness of the pro-vaccine
position. If the proponents of vaccination had something of substance to offer, they would rely
on facts and data rather than ad hominin attacks. As it happens, the facts do not support their
position. Besides, "vaccine hesitancy" is not a character flaw or a mental condition, it's the
sign of someone who has taken responsibility for his own health and welfare. Ask yourself this:
Why would a normal, rational person be eager to have an experimental cocktail injected into his
bloodstream potentially triggering all manner of long-term ailments or death? Is that the
choice a normal person would make?
As far as I can see, behavioral psychologists are playing a critical role in this mass
vaccination campaign. According to a report put out by the National Institutes of Health, it
appears that a rapid response team has been formed to attack the opinions of people who
challenge the "official narrative". Check out this blurb from the report titled "COVID-19
Vaccination: Communication: Applying Behavioral and Social Science to Address Vaccine Hesitancy
and Foster Vaccine Confidence":
Mitigate the impact of COVID-19-related misinformation
The spread of health-related misinformation was a significant public health concern well
before the COVID-19 pandemic. During the last decade, vaccine-related discourse online and
in the media has been plagued by misinformation. Anti-vaccine groups have leveraged political
and social divisions to diminish trust in vaccines, pushed false narratives questioning the
safety and effectiveness of vaccines, spread false claims about adverse outcomes, and
downplayed the risks of the disease's vaccines protect against. .
COVID-19 vaccine communication efforts cannot ignore misinformation and must take
actions, informed by behavioral and communication research, to identify emerging rumors and
respond in a way that is informed by behavioral science. Real-time, agile, and scalable
monitoring of discourse concerning COVID 19 vaccination -- including conspiracy theories,
rumors, and myths -- can support a swiftly developed and implemented response.
"Misinformation surveillance" efforts should identify the most prominent sources of
misinformation, the tactics being used, and the groups most at risk of being exposed to and
influenced by the rumors. This information, in addition to data regarding the dynamics and
patterns of misinformation spread, could help inform the appropriate response and best
targets for intervention efforts .
Correcting the false claim contained in the message, exposing the tactics used by
disinformation agents , and inducing skepticism by highlighting the ulterior
motives of these actors are all potentially effective strategies for mitigating the
impact of misinformation " ( "COVID-19
Vaccination* Communication: Applying Behavioral and Social Science to Address Vaccine
Hesitancy and Foster Vaccine Confidence" , the National Institutes of Health)
Repeat: "Misinformation surveillance" "disinformation agents" " the
ulterior motives of these actors "??
Really? Now who's sounding paranoid?
This is very scary stuff. Agents of the state now identify critics of the Covid vaccine
as their mortal enemies. How did we get here? And how did we get to the point where the
government is targeting people who don't agree with them? This is way beyond Orwell. We have
entered some creepy alternate universe.
Here's more on the topic from a statement by Arthur C. Evans Jr., PhD, CEO of the American
Psychological Association, in response to the approval by an advisory panel of the Food and
Drug Administration of a vaccine against COVID-19:
"We recognize that there are pockets of resistance to vaccines , distrust of the
medical establishment and misinformation about vaccines generally .Some populations
are understandably less likely to accept vaccinations due to a legacy of mistrust rooted in
unethical public health practices.
"It is critical that leaders across the political spectrum unite behind messages of
vaccine safety and transparency." ..
Enlist credible spokespeople who can connect with diverse communities, especially
those where mistrust and skepticism run high. When leaders talk about vaccines as standard
practices, as opposed to options, people are more likely to accept them. Research
suggests building trust and providing clear information about vaccines can improve
vaccination uptake rates. It is critical that leaders across the political spectrum unite
behind vaccine safety and transparency, clearly explaining what is in the vaccine and what it
does and doesn't do in the body.
Consider the wide variety of factors that motivate human behavior. Behavioral science
indicates that people are more likely to adhere to vaccine recommendations when they believe
they are susceptible to the illness, when they want to protect others, when they believe
the vaccine is safe or at least safer than the illness, and when their concerns and questions
are managed respectfully by doctors and experts." ( "APA Welcomes Step Toward
First U.S. Vaccine Approval" , American Psychological Association)
Is it really ethical for the APA to be involved in a mass vaccination campaign? Is this the
role an organization like this should play in a democratic society? Should the APA use its
unique understanding of human behavior to persuade people on behalf of the government and big
pharma? And, more importantly, if behavioral psychologists helped to shape the government's
strategy on mass vaccination, then in what other policies were they involved? Were these the
"professionals" who conjured up the pandemic restrictions? Were the masks, the social
distancing and the lockdowns all promoted by "experts" as a way to undermine normal human
relations and inflict the maximum psychological pain on the American people? Was the intention
to create a weak and submissive population that would willingly accept the dismantling of
democratic institutions, the dramatic restructuring of the economy, and the imposition of a new
political order?"
These questions need to be answered.
Surprisingly, the resistance to vaccination is nearly as strong today as it was a year ago.
According to PEW Research:
(only) "69% of the public intends to get a vaccine – or already has .
Those who do not currently plan to get a vaccine (30% of the public) list a range
of reasons why. Majorities cite concerns about side effects (72%), a sense that vaccines were
developed and tested too quickly (67%) and a desire to know more about how well they work
(61%) as major reasons why they do not intend to get vaccinated.
Smaller shares of those not planning to get a vaccine say past mistakes by the medical
care system (46%) or a sense they don't need it (42%) are major reasons why they don't plan
to get a vaccine; 36% of this group (11% of all U.S. adults) say a major reason they would
pass on receiving a coronavirus vaccine is that they don't get vaccines generally.
The new national survey by Pew Research Center, conducted Feb. 16 to 21 among 10,121 U.S.
adults. (
"Growing Share of Americans Say They Plan To Get a COVID-19 Vaccine – or Already
Have ", PEW Research)
So, despite the nonstop propaganda blitz, a significant portion of the population remains
unconvinced, unimpressed and steadfast. Go figure? Of course, this is just Round 1. Soon,
persuasion will turn into coercion, and from coercion to outright force. It's already clear
that air-travel will require vaccine passports, and that public transit, concerts, libraries,
restaurants and, perhaps, even grocery stores could follow soon after. Vaccination looks to be
the defining issue of the next few years at least. And those who resist the edicts of the state
will increasingly find themselves on the outside; outcasts in their own country.
anonymous [408] Disclaimer
March 25, 2021 at 9:07 pm GMT • 4.8 days ago
Right. US government policy is ulterior constraint and coercion of voluntary consent to
medical experimentation in the meaning of Nuremberg Code Article 1, and it's illegal in
federal and universal-jurisdiction law. APA got with the program on torture, so of course
they're going to help with coercive medical experimentation.
The first time it goes to court, they lose. This is why you see Pharma shills like That
Would Be Telling breezily trying to rush approval – Oh, we'll get oodles of data now,
so we don't have to wait so long for final approval!! Final approval opens up new
possibilities for corrupt Big Pharma coercion under color of law.
But the case law encourages deference to emergency action to contain an outbreak. So as
more people knuckle under and get shot up, the outbreak goes away, the exigency no longer
weighs against denial of our rights. If the health emergency continues after extensive
vaccination, well, Why the hell is that? So judicial review is something Big Pharma will
avoid at all costs, not least because it might open the ultimate can of worms, violations of
the *False Claims Act* to obtain a *fraudulent EUA* . Big Pharma corruptly suppressed
alternatives to justify the EUA. This is a litigation bonanza that will make the tobacco
settlement and opioid claims look like chump change.
Wade Hampton
March 26, 2021 at 8:29 am GMT • 4.3 days ago
A pharmaceutical company is typically responsible for the harm done by new drugs it has
developed. The Covid-vaccines are being released under emergency use authorizations which
shield the Pharma companies from such liability under most circumstances.
To minimize the liability related to new drug development, a typical new drug goes through
a development process which takes 6-7 years of a clinical work (testing on increasing numbers
of test subjects) to gain approval. During the clinical phase, 4 out of 5 drug candidates
typically fail because of inefficacy or harmful side effects.
These vaccines are being released after only one year of clinical testing, so essentially,
we are using the entire population as test subjects. And if experience is any guide many of
them (perhaps all of them) will fail due to harmful side effects.
I am going to wait at least two years. By then, we should have a pretty good idea of the
reality of the situation. I am providing a useful service to the drug development process by
being a member of the "control group".
TTSSYF
March 26, 2021 at 11:00 am GMT • 4.2 days ago
@Dumbo
My father was sick for several days with a respiratory illness and tested positive for the
virus. He had had the first of two Moderna shots three weeks prior.
BorisMay
March 26, 2021 at 11:45 am GMT • 4.2 days ago
Unbelievable that anyone with a brain still watches a television or listens to a radio. No
wonder the US is screwed, just like the UK is.
Observator
March 26, 2021 at 12:36 pm GMT • 4.1 days ago
@Wade Hampton harma Technology Focus reported these activities on 2/23/21, online at
https://www.pharmaceutical-technology.com/news/company-news/pfizer-latin-american-vaccine/
In 2009 Pfizer was assessed the largest fine in history for deliberate medical fraud
https://www.justice.gov/opa/pr/justice-department-announces-largest-health-care-fraud-settlement-its-history
but after lengthy appeals their attorneys managed to get the judgment reduced by almost two
billion dollars.
Mefobills
March 26, 2021 at 1:28 pm GMT • 4.1 days ago
@mongoos opinion." -Joseph Goebbels, Hitler's Reichsminister Of Propaganda
That's right. It was to protect the population from internal enemies.
By then Bernays had already created propaganda techniques, and NSDAP thought leaders were
figuring out ways to combat the big lie from finance oligarchs of the west.
Do you really think that the average sheeple can think for themselves? Only a small fraction
of the population is capable of critical thought. It has always been that way – a large
component of the population wants to be told what to do, and they want to do the right
thing.
If they were critical thinkers they wouldn't be wearing a mask while in their car driving
alone.
Demguy
March 26, 2021 at 1:33 pm GMT • 4.1 days ago
They say that vaccines are "safe". My definition of"safe" is that the chance of dying post
vaccine is the same as any other vaccine. VAERS data shows 166 deaths for all of 2020. As of
3-11-21, there have been 1642 deaths, 50X the rate. If they would just come out and say the
death rate is higher but you still have a 1000 times greater chance of dying without it, I'd
get it. But instead I'm wondering what else they're lying about.
Also, they say to trust the science, but I never hear from scientists, only public
relations, profiteers, etc. You'll get a much more honest answer from the car mechanic than the
salesman.
Liza
March 26, 2021 at 1:42 pm GMT • 4.1 days ago
The Center for Countering Digital Hate (CCDH), led by Imran Ahmed, has published a hit
list of the top 10 "anti-vaxxers" they want eradicated from public platforms
CCDH, while anonymously funded, can easily be linked to a number of technocratic centers
within the globalist network that seeks to take over global governance through the Great
Reset
from Dr. Mercola's latest article, of today, March 26th.
The level of corruption of science (and medicine is just a branch of science) in the USA is
really astounding. It is Lysenkoism, pure and simple. And vaccine debate, or absence of thereof
is just a tip of the iceberg, one manifestations of corrupt nature of neoliberalism in the USA
and the level of amorality and corruption of the neoliberal elite. After all the essence of
neoliberalism is "profits before people".
Notable quotes:
"... it's what it looks like to me too... pfizer must be laughing all the way to the bank, or blackrock - whatever.. i guess the johnston vaccine or whatever will have to be pushed harder too.. https://www.holdingschannel.com/13f/blackrock-inc-top-holdings/ ..."
gottlieb , Mar 30 2021 16:10 utc |
15
Well these aren't vaccines as much as flu-shots. Indeed they're already buzzing about
combining the annual flu jab with the covid 'vaccine' for inoculation once or twice a year
depending on the severity of variant season. Vaccines are supposed to offer protection
against disease for long periods of time. The flu shot isn't a vaccine and neither are these
Covid jabs. And contrary to a comment above these 'vaccines' have proven very effective to
'cure' serious Covid patients, much like the gene-therapies being used to great effect.
I certainly wouldn't take the experimental mRNA 'vaccines' until much more data is in. Is
there a reason the mRNA rabies vaccine hasn't been approved after years of trying? And of
course folks are quick the forget the Moderna/Pfizer medicines have not been approved either
except for "emergency use."
And now finally there is out in the open debate about the origins of the 'novel' Corona
virus of which so many react as if it is not novel at all. Not to say we'll ever know the
truth - imagine the legal liability of setting off a global pandemic.
There is something rotten in the state of covid. Let's put on our gasmasks and get to the
bottom of it.
ptb , Mar 30 2021 16:21 utc |
17
@15 gottlieb
Well these aren't vaccines as much as [seasonal] flu-shots.
That seems to be a very significant possibility.
james , Mar 30 2021 16:25 utc |
18
it's what it looks like to me too... pfizer must be laughing all the way to the bank,
or blackrock - whatever.. i guess the johnston vaccine or whatever will have to be pushed
harder too.. https://www.holdingschannel.com/13f/blackrock-inc-top-holdings/
james , Mar 30 2021 16:25 utc |
19
it is hard not to be cynical..
norecovery , Mar 30 2021 16:53 utc |
23
Most people are not grasping the serious wrong-headedness of this mass vaccination effort.
I transcribed a germane section of Dr. Geert Vanden Bossche's interview so folks here can
please read it until they understand what he's saying. (I inserted punctuation and paragraphs
to make it more readable.)
https://www.youtube.com/watch?v=ZJZxiNxYLpc
"If you go to war, you better make sure you have the right weapon. The weapon in itself
can be an excellent weapon, and that is what I'm saying about the current vaccines, I mean
just brilliant people who have been making these vaccines in no time and with regulatory
approval and everything, so the weapon in itself is excellent. The question is, is this the
right weapon for the kind of war that is going on right now? And there, my answer is
definitely no. Because these are prophylactic vaccines, and prophylactic vaccines should
typically not be administered to people who are exposed to high infectious pressure. So don't
forget we are administering these vaccines in the heat of a pandemic.
"So in other words, while we are preparing our weapon, we are fully attacked by the virus
– the virus is everywhere – so that is a very different scenario from using such
vaccines in a setting where the vaccinee is barely or not exposed to the virus. And I'm
saying this because if you have a high infectious pressure, it's so easy for the virus to
jump from one person to the other. So, if you're immune response is just mounting, as we see
right now with a number of people who get their first dose – they get their first dose,
the antibodies are not fully mature, [inaudible] are not very high, so their immune response
is sub-optimal. But they are in the midst of this war. While they are mounting an immune
response they are fully attacked by the virus. And every single time – I mean, this is
textbook knowledge – every time you have an immune response that is sub-optimal in the
presence of an infection, in the presence of a virus that infects that person, you are at
risk for immune escape. So that means that the virus can escape from the immune response.
"So I'm saying that these vaccines – I mean, in their own right of course, are
excellent – but to use them in the midst of a pandemic and do mass vaccinations,
because then you provide within a very short period of time with high antibody [types ?]
[inaudible] I mean, that wouldn't matter if you could eradicate if you could prevent
infection. But these vaccines don't prevent infection – they protect against
disease.
"Because unfortunately, we look no further than the end of our nose, in the sense that
hospitalization, that's all that counts – you know, getting people away from the
hospital. But in the meantime, you're not realizing that we give, all the time during this
pandemic, by our interventions the opportunity to escape the immune system. And that is of
course a very, very dangerous thing, especially when we realize that these guys they only
need 10 hours to replicate.
"So we think that by making new vaccines – new vaccines against the new infectious
strains – we think we're going to catch up. It's impossible to catch up. The virus is
not going to wait until we have those vaccines ready. I mean, this thing continues. As I was
saying, the thing is, I mean, if you do this in the midst of a pandemic, that is an enormous
problem. These vaccines are excellent, but they are not made for administration to millions
of people in the midst, in the heat of a pandemic. So that is my point."
Mina , Mar 30 2021 16:56 utc |
25
BBC buries detail about the new AZ problemshttps://www.bbc.com/news/world-europe-56580728
https://www.dw.com/en/berlin-halts-astrazeneca-vaccines-for-under-60s/a-57049301
https://www.business-standard.com/article/current-affairs/coronavirus-vaccine-germany-reports-more-astrazeneca-clot-cases-121032900737_1.html
Luckily, the EU has approved a change of name of the AZ vaccin
https://www.ema.europa.eu/en/medicines/human/EPAR/vaxzevria-previously-covid-19-vaccine-astrazeneca
https://www.brusselstimes.com/news/eu-affairs/162559/astrazeneca-vaccine-now-renamed-as-vaxzevria-ema-european-eu-uk-swedish-lakemedelsverket/
But this latest point is not mentioned by most MSM of course...
Digital Spartacus , Mar 30 2021 16:57 utc |
26
James @ 19
It's impossible to not be cynical.
norecovery , Mar 30 2021 17:16 utc |
30
Mass vaccination apparently is accelerating the mutation of more dangerous variants. Do
the experts not understand that the antigen-specific antibodies the vaccinations are
eliciting, actually compromise people's innate broadly-based immune resistance to
variants?
psychohistorian
31
@ defaultcitizen | Mar 30 2021 16:55 utc | 24 who wrote
"
Thanks for that and the sentiments about what b has to go through to keep churning out the
truth he finds within his bias like we all have.
We are an interesting species struggling to evolve or perish it seems and yet adding my
textual white noise to yours feels positive in some way and so I do it. I think it is a small
percentage that don't feel the impotent rage of our social system and that rage is causing it
to lose trust.
I have been waiting over 50 years for the failure tipping point in the private finance
based social system and I feel it is close. But I have to admit I felt more positive in the
middle of the Occupy movement because their were people in the streets and it was focused on
Wall Street....and it sure as heck isn't now.....sigh
Jackrabbit
32
Mina @Mar30 16:56 #25
AstraZeneca has been plagued with problems that get lots of media attention (production
problems, suspected health problems, etc.)
And the J&J vaccine is still hard to find. There are now dozens of places to get a
vaccine in NYC but I could only find 4 or 5 that give the J&J vaccine (along with one of
the mRNA shots) - at least two of which note that they are not giving "first dose" shots and
another says (in a FAQ on their site) that they are only receiving Moderna vaccines "at this
time".
IMO we are being herded into the mRNA vaccines.
But if you complain to others about that (as I have) you are treated as though you are
"anti-vaxx / anti-science.
!!
norecovery , Mar 30 2021 17:46 utc |
34
karlof1 – The "anti-vaxxer – anti-science" smear is analogous to
"anti-American" if one criticizes U.S. foreign policy. Simplistic demonization is encouraged
by the mainstream media with news delivered in sound bites in order to dumb down the populace
and manufacture consent (or paranoia).
karlof1
36
norecovery @30--
That's why I see getting vaccinated now as a waste of time and medicine. My lifestyle
hasn't changed much at all with the pandemic, although my employment of precautions has
soared. That will change with our cross-country road trip during the month of April as we
interact with many more people and visit their homes. Yes, aside from lodgings, they'll be
kin--but--unprotected interactions with kin are often the source of infection. As we see
cases soar once again, it's clear that the vaccine was seen as some sort of panacea when it's
not that at all. People ought to wonder why they're prompted to get a new flu shot annually;
it's because it mutates and a different formula's required. I've never had a flu shot and
don't get the flu, mainly because of my lifestyle. What's most important for me is my
preferred vaccine--Sputnik V--isn't available in my nation and may never be approved for use
here. For me, the AIDS experience is my reference--Sex wasn't deadly until it suddenly was
(All STDs were never considered in the same league) which prompted a change in behavior. Same
with COVID, although flu is clearly a deadly virus for many.
Q: What data did the FDA use to make the decision to authorize Pfizer-BioNTech COVID-19 Vaccine
for emergency use?
A: Pfizer-BioNTech COVID-19 Vaccine is authorized to prevent coronavirus disease 2019
(COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in
individuals 16 years of age and older.
FDA evaluated and analyzed the safety and effectiveness data from clinical trials conducted
in tens of thousands of study participants and manufacturing information submitted by
Pfizer-BioNTech. FDA has determined that the totality of the available data provides clear
evidence that Pfizer-BioNTech COVID-19 Vaccine may be effective in preventing COVID-19 and
support that the known and potential benefits outweigh the known and potential risks of the
vaccine's use in millions of people 16 years of age and older, including healthy individuals.
Q: What data is available to the public to review?
A: FDA posted data and analysis in a briefing document made available in connection with the
December 10, 2020, meeting of the Vaccines and Related Biological Products Advisory Committee.
Following issuance of the
emergency use authorization , the Letter of Authorization, Fact Sheets and Full EUA
Prescribing Information are
posted on FDA's web site. FDA has also posted the review memo for Pfizer-BioNTech COVID-19
Vaccine, which summarizes FDA's review of the safety and effectiveness data, including clinical
data, submitted in support of the request for emergency use authorization.
Q: How well does Pfizer-BioNTech COVID-19 Vaccine prevent COVID-19?
A: The data to support the EUA include an analysis of 36,523 participants in the ongoing
randomized, placebo-controlled international study, the majority of whom are U.S. participants,
who completed the 2-dose vaccination regimen and did not have evidence of SARS-CoV-2 infection
through 7 days after the second dose. Among these participants, 18,198 received the vaccine and
18,325 received saline placebo.
... 8 COVID-19 cases in the vaccine group and 162 COVID-19 cases in the placebo group. Of
these 170 COVID-19 cases, 1 in the vaccine group and 3 in the placebo group were classified as
severe.
Q: Can people who have already had COVID-19 get the Pfizer-BioNTech COVID-19
Vaccine?
A: Among all study participants, 3% had evidence of infection prior to vaccination, and
among participants with evidence of infection prior to vaccination, more confirmed COVID-19
cases occurred in the placebo group compared with the vaccine group. While relatively few
confirmed COVID-19 cases occurred overall among participants with evidence of infection prior
to vaccination, available data suggest that previously infected individuals can be at risk of
COVID-19 (i.e., reinfection) and could benefit from vaccination.
Q: If a person has received the the Pfizer-BioNTech COVID-19 Vaccine, will the vaccine protect
against transmission of SARS-CoV-2 from individuals who are infected despite
vaccination?
A: Most vaccines that protect from viral illnesses also reduce transmission of the virus
that causes the disease by those who are vaccinated. While it is hoped this will be the case,
the scientific community does not yet know if the Pfizer-BioNTech COVID-19 Vaccine will reduce
such transmission.
Q: What safety information did FDA evaluate to authorize the Pfizer-BioNTech COVID-19 Vaccine
for emergency use?
A: The available safety data to support the EUA include 37,586 of the participants enrolled
in an ongoing randomized, placebo-controlled international study, the majority of whom are U.S.
participants. These participants, 18,801 of whom received the vaccine and 18,785 of whom
received saline placebo, were followed for a median of 2 months after receiving the 2nd dose.
This is consistent with the recommendations set forth in FDA's October 2020
Guidance on Emergency Use Authorization for Vaccines to Prevent COVID-19
The most commonly reported side effects were pain at the injection site, tiredness,
headache, muscle pain, chills, joint pain, and fever. Side effects typically started within two
days of vaccination and resolved 1-2 day later. Of note, more people experienced these side
effects after the second dose than after the first dose, so it is important for vaccination
providers and recipients to expect that that there may be some side effects after either dose,
but even more so after the second dose.
FDA also evaluated additional safety data from the larger database that included
participants enrolled later during the study who had shorter follow-up (the total database
included 43,448 participants, 21,720 of whom received vaccine and 21,728 of whom received
saline placebo) . FDA determined that the findings were similar to those in the population of
participants with a median follow-up of 2 months after the 2nd dose.
Q: Is information available about serious adverse events?
A: Serious adverse events, while uncommon (<1.0%), were observed at slightly higher
numerical rates in the vaccine study group compared to the saline placebo study group, both
overall and for certain specific adverse events occurring in very small numbers. These
represented common medical events that occur in the general population at similar frequency.
Upon further review by FDA, these imbalances do not raise a safety concern, nor do they suggest
a causal relationship to vaccination for the vast majority of reported serious adverse
events.
Serious adverse events considered by FDA to be plausibly related to the vaccine or
vaccination procedure were one case of shoulder injury at the vaccination site and one case of
swollen lymph node in the armpit opposite the vaccination arm.
No safety concerns were identified in subgroup analyses by age, race, ethnicity, medical
comorbidities, or prior SARS-CoV-2 infection.
Severe allergic reactions, including anaphylaxis, have been reported following
administration of Pfizer-BioNTech COVID-19 Vaccine during mass vaccination outside of the
clinical trial setting. Information pertaining to severe allergic reaction is included in
the Fact Sheet for Vaccine Providers, Fact Sheet for Vaccine Recipients and the EUA Prescribing
Information.
Additional adverse reactions, some of which may be serious, may become apparent with more
widespread use of the Pfizer-BioNTech COVID-19 Vaccine.
Table 4. Systemic reactions in persons aged >55 years, Pfizer-BioNTech COVID-19
vaccine and placebo
Table 4. Systemic reactions in persons aged >55 years, Pfizer-BioNTech COVID-19 vaccine
and Placebo
Dose 1
Dose 2
Pfizer-BioNTech Vaccine
Placebo
Pfizer-BioNTech Vaccine
Placebo
Fever
≥38.0°C
26 (1.4)
7 (0.4)
181 (10.9)
4 (0.2)
≥38.0°C to 38.4°C
23 (1.3)
2 (0.1)
131 (7.9)
2 (0.1)
>38.4°C to 38.9°C
1 (0.1)
3 (0.2)
45 (2.7)
1 (0.1)
>38.9°C to 40.0°C
1 (0.1)
2 (0.1)
5 (0.3)
1 (0.1)
>40.0°C
1 (0.1)
0 (0)
0 (0)
0 (0)
Fatigue a , n (%)
Any
615 (34.1)
405 (22.6)
839 (50.5)
277 (16.8)
Mild
373 (20.7)
252 (14.1)
351 (21.1)
161 (9.8)
Moderate
240 (13.3)
150 (8.4)
442 (26.6)
114 (6.9)
Severe
2 (0.1)
3 (0.2)
46 (2.8)
2 (0.1)
Grade 4
0 (0)
0 (0)
0 (0)
0 (0)
Headache a , n (%)
Any
454 (25.2)
325 (18.1)
647 (39.0)
229 (13.9)
Mild
348 (19.3)
242 (13.5)
422 (25.4)
165 (10.0)
Moderate
104 (5.8)
80 (4.5)
216 (13.0)
60 (3.6)
Severe
2 (0.1)
3 (0.2)
9 (0.5)
4 (0.2)
Grade 4
0 (0)
0 (0)
0 (0)
0 (0)
Chills a , n (%)
Any
113 (6.3)
57 (3.2)
377 (22.7)
46 (2.8)
Mild
87 (4.8)
40 (2.2)
199 (12.0)
35 (2.1)
Moderate
26 (1.4)
16 (0.9)
161 (9.7)
11 (0.7)
Severe
0 (0)
1 (0.1)
17 (1.0)
0 (0)
Grade 4
0 (0)
0 (0)
0 (0)
0 (0)
Vomiting b , n (%)
Any
9 (0.5)
9 (0.5)
11 (0.7)
5 (0.3)
Mild
8 (0.4)
9 (0.5)
9 (0.5)
5 (0.3)
Moderate
1 (0.1)
0 (0)
1 (0.1)
0 (0)
Severe
3 (0.2)
0 (0)
1 (0.1)
0 (0)
Grade 4
0 (0)
0 (0)
0 (0)
0 (0)
Diarrhea c , n (%)
Any
147 (8.2)
118 (6.6)
137 (8.3)
99 (6.0)
Mild
118 (6.5)
100 (5.6)
114 (6.9)
73 (4.4)
Moderate
26 (1.4)
17 (0.9)
21 (1.3)
22 (1.3)
Severe
3 (0.2)
1 (0.1)
2 (0.1)
4 (0.2)
Grade 4
0 (0)
0 (0)
0 (0)
0 (0)
New or worsening muscle pain a , n (%)
Any
251 (13.9)
149 (8.3)
477 (28.7)
87 (5.3)
Mild
168 (9.3)
100 (5.6)
202 (12.2)
57 (3.5)
Moderate
82 (4.6)
46 (2.6)
259 (15.6)
29 (1.8)
Severe
1 (0.1)
3 (0.2)
16 (1.0)
1 (0.1)
Grade 4
0 (0)
0 (0)
0 (0)
0 (0)
New or worsening joint pain a , n (%)
Any
155 (8.6)
109 (6.1)
313 (18.9)
61 (3.7)
Mild
101 (5.6)
68 (3.8)
161 (9.7)
35 (2.1)
Moderate
52 (2.9)
40 (2.2)
145 (8.7)
25 (1.5)
Severe
2 (0.1)
1 (0.1)
7 (0.4)
1 (0.1)
Grade 4
0 (0)
0 (0)
0 (0)
0 (0)
Use of antipyretic or pain medication
358 (19.9)
213 (11.9)
625 (37.7)
161 (9.8)
a Mild: does not interfere with activity; moderate: some interference with
activity; severe: prevents daily activity; Grade 4: emergency room visit or hospitalization for
severe fatigue, severe headache, severe muscle pain, or severe joint pain.
b Mild: 1 to 2 times in 24 hours; moderate: >2 times in 24 hours; severe:
requires intravenous hydration; Grade 4: emergency room visit or hospitalization for severe
vomiting.
c Mild: 2 to 3 loose stools in 24 hours; moderate: 4 to 5 loose stools in 24
hours; severe: 6 or more loose stools in 24 hours; Grade 4: emergency room visit or
hospitalization for severe diarrhea. Unsolicited Adverse Events
Reports of lymphadenopathy were imbalanced with 58 more cases in the vaccine group (64) than
the placebo group (6); lymphadenopathy is plausibly related to the vaccine. Lymphadenopathy
occurred in the arm and neck region and was reported within 2 to 4 days after vaccination. The
average duration of lymphadenopathy was approximately 10 days. Bell's palsy was reported by
four vaccine recipients and none of the placebo recipients. The observed frequency of reported
Bell's palsy in the vaccine group is consistent with the background rate in the general
population, and there is no basis upon which to conclude a causal relationship.
Serious
Adverse Events
Serious adverse events were defined as any untoward medical occurrence that resulted in
death, was life-threatening, required inpatient hospitalization or prolongation of existing
hospitalization, or resulted in persistent disability/incapacity. The proportions of
participants who reported at least 1 serious adverse event were 0.6% in the vaccine group and
0.5% in the placebo group. The most common serious adverse events in the vaccine group which
were numerically higher than in the placebo group were appendicitis (7 in vaccine vs 2 in
placebo), acute myocardial infarction (3 vs 0), and cerebrovascular accident (3 vs 1).
Cardiovascular serious adverse events were balanced between vaccine and placebo groups. Two
serious adverse events were considered by U.S. Food and Drug Administration (FDA) as possibly
related to vaccine: shoulder injury possibly related to vaccine administration or to the
vaccine itself, and lymphadenopathy involving the axilla contralateral to the vaccine injection
site. Otherwise, occurrence of severe adverse events involving system organ classes and
specific preferred terms were balanced between vaccine and placebo groups.
Data source: FDA
briefing document external icon
Oriental Voice , Mar 25 2021 1:00 utc |
72
@Posted by: JB | Mar 24 2021 23:47 utc | 64
....why is there almost no mention of treatment.
There were mentions of treatments, just not in the US. I don't know about whether the same
has been in Europe, but in China very early on during the pandemic, various treatments were
tried and discussed. China drew on its experience of fighting SARS, and their findings were
actually published, such as in Lancet. I believe Italy consequently made routine use of one
of the method, that of serum from recovered patients (and later in the US too) on patients in
critical care units, which was first tried and endorsed in China. Serum wasn't a panacea but
in most cases found helpful. However, in China itself the popular treatment was a combination
of traditional western medicine for pneumonia and traditional Chinese herbal medicine for
respiratory ailments. The findings were conveyed to countries that China assisted early on,
such as Italy and Serbia. Chinese herbal medicine was also included in aid packages that were
sent oversea to stranded Chinese expats. China also discussed at length the use of
remdesivir, and dismissed it as being ineffective.
Actually there were discussions of treatments in the US too, if you recall Ole Pres Trump
urged the drinking of Dittol, Lysol, and other germ killers. I didn't recall him urging the
use of injection method, but like always there are daredevils in the US that went that far
:)
uncle tungsten , Mar 25 2021 2:58 utc |
78
JB #37
Just listen to this doctor's testimony in the Texas legislature on TREATMENT of Covid-19:
See this link
Just one quote: "COVID - 19 has always been a treatable sickness"
Well said and thank you. My government posts a pathetic thing entitled "Covid 19
Vaccination and treatment" and there is ZERO information on early stage treatment. It is all
vaccine, vaccine, vaccine.
When I next visit my GP I will ask her for details of her treatment regime should I ever
receive a +ve test but I suspect what the answer will be.
Every disease is treatable to some extent. I have the Chinese Covid treatment manual of
considerable volume, fully translated to english.
Here is version 7 March 2020 and it is no doubt thoroughly revised since that date.
The almost total surrender of professionals in medical practice to self censorship and
the brutal insistence on toeing the line to the official mantra is religious obscurantism of
the worst order. It is the totalitarian stuff that led to the witch hunts and fatwas and the
excommunications and now the cancel culture.
The advocates of this oppression of clinical practice are the enemies of humanity and
the saboteurs of science.
That brief video is well worth considering as it demands an answer as to why this path
of death causing ignorance was ever advocated let alone accepted. Let a thousand flowers
bloom and a thousand ideas be considered.
DaveNItUp
16
It looks like the vaccinated will be the petri dishes from which the variants arise, but
the unvaccinated who will be vilified...sadistically genius...that's how hegemon rolls
I'm opting out of this sick game myself as long as possible.
Bluedotterel , Mar 24 2021 17:32 utc |
4
I don't know how important or reliable this is, but Pfizer does have an impressive rap
sheet as a corporate criminal, Netanyahu, well...
https://www.unz.com/gatzmon/the-probe-into-the-israeli-vaccine-policy-and-its-outcome-is-beyond-damning/
"In the document the CP (Civilian Probe) points at a government attempt to conceal its
dealing with Pfizer. The document states that "the Pfizer-Israel agreement is suffocated with
redacted segments, consequently, it is not possible to analyze it legally and/or fully grasp
Its implications as far as public health is concerned This concealment casts a heavy shadow
over anyone who took part in the (Israeli/Pfizer) negotiations ".
The industry needs some good PR right now. After all, its refusal to share its vaccine
technology could end up costing millions of lives in the developing world. In addition, it
could mean trillions of dollars of lost output as countries need to shut down large segments
of their economy. But the NYT is there to help. It ran a lengthy article about the issue,
which contains much useful information, but it maintains a framing favorable to the
pharmaceutical industry. At the end of the piece, after giving the argument for broader
sharing of technology and over-riding the industry's government-granted patent monopolies,
the piece tells readers: "But governments cannot afford to sabotage companies that need
profit to survive."
If the reporters/editors had read their piece, they would know that the companies in
question had already made large profits, through being paid directly for their research and
building manufacturing facilities, as was the case with Moderna and BioNtech (Pfizer's German
partner), or with advance purchase agreements. No one is suggesting that these companies
should not make a profit, so it is not clear on what planet this assertion originated.
It is possible to make profits directly on government contracts, as major military
contractors like Lockheed and Boeing could explain to the New York Times. The advantage of
having direct contracts for biomedical research is that a requirement of the contract could
be that all findings are fully open-source so that researchers all over the world can benefit
from them. (I discuss a mechanism for direct funding in chapter 5 of Rigged
... ... ...
It is probably worth mentioning inequality in this piece. The NYT, like most intellectual
types, has done considerable hand-wringing over inequality in recent years, both overall and
racial inequality. It is a safe bet that giving more money to pharmaceutical companies will
mean more inequality and certainly benefit whites far more than Blacks. It might be useful if
the paper paid a little attention to the policies that create
inequality instead of just bemoaning it as an unfortunate feature of the economy.
mary s •
5 days ago
Yes, the NYT is really good at covering the impact of policies that increase inequality
and perpetuate structural racism but avoids drawing any lines to the policies themselves --
and the politics that create these policies -- by treating the status quo as a kind of
state of nature.
Rath R. Weird
•
6 days ago
Innovation in vaccine design comes from advances in fundamental science, which is funded
not by companies, but by NIH and NSF (predominantly). Pharma employs scientists trained
using federal funds, freely uses federally funded resources, open access publications and
open source software paid for through federal funds, buys up commercializable technologies
in form of startups that grow out of federal science and funded by SBIR and STTR grants,
kills most of them and overcharges taxpayers for the product. That's rarely mentioned. As
is the fact that pharma actually sucks at the only thing that they are supposed to be good
at - manufacturing. Quality problems have been plaguing AstraZeneca, Pfizer, and Moderna -
something that is discussed in trade publications and FDA meetings but doesn't make it to
the NYT or TV news.
Alicia Carrot
Rath R. Weird •
5 days ago
This is spot on! Taxpayer funded research, yet the conglomerates are holding the patents
and making a fortune off of open sourced information.
Finally, COVID vaccinations are re-accelerating in US and EU...
Source: Bloomberg
And while cases are up modestly (are PCR tests picking up spike proteins from the mRNA
vaccines?), death rates continue to tumble...
Rdm
March 25, 2021 at 9:11 pm GMT • 23.5 hours ago
@Anonymous etting where lots of people are taking, you do come out as anti-vaxxer
sentiment. That's where social pressure builds in and some weak mind cave in or Some took it
because their career is on the line.
There's only 32% of healthcare workers getting the vaccine here in the States. It's
like the MSM and some people from higher up are pushing the idea that vaccination is a must
and suggesting the vaccine passport.
What in the world, the United States of America, the beacon of Truth, the land of the
Free, pioneers of Science caved into this idea of vaccine must be administered to
everyone? The same can be said for all other social phenomena as well...
Excessive zeal might hurt. I would understand vaccination of faculty, especially older one.
But students are young and young people do not have the same level of risk from COVID-19as older
people. If vaccine has side effects Rutgers University will be liable for damages.
Rutgers University is requiring students to get the COVID-19 vaccine before they come back
for the fall semester, and one expert thinks that other colleges will do the same.
"Rutgers is on fairly solid ground and we're likely to see a good number of universities,
both public and private, start to mandate the vaccine," Eric Feldman, professor of medical
ethics and health policy at the University of Pennsylvania Carey Law School, told Yahoo Finance
Live (video above).
Rutgers, a public university in New Jersey, is the first prominent U.S. higher education
institution to
mandate COVID vaccines for the fall semester. Students will be required to show proof of
vaccination -- or receive an exemption -- before coming to campus to attend classes or live in
university housing.
Students who are under the age of 17 will only be eligible for the Pfizer vaccine, while
older students will be able to receive a Moderna, Pfizer, or Johnson & Johnson
inoculation.
oldhippie , Mar 21 2021 17:43 utc |
22
The trio of linked articles in top post concerning covid are all excellent. Each
highlights how very little is known, still, concerning viral transmission.
> [W]e do express our concern at the UK's decision to increase its nuclear weapons
arsenal, which is contrary to its obligations under Article VI of the NPT. It could have
a damaging impact on global stability and efforts to pursue a world free of nuclear
weapons.
At a time when nuclear weapon risks are higher than they have been since the Cold War,
investments in disarmament and arms control is the best way to strengthen the stability
and reduce nuclear danger. <
Yves Smith makes the suggestion that for starters we should just open some windows. Get
some ventilation. Get some fresh air. When I was still employed I was a house painter.
Way back in sixties and seventies painters learned drills for how to paint every surface of a
window. This is no longer required. Most windows are never opened. In newer homes it is
quite unusual to find windows that have ever been opened . Simplifies painting
enormously.
Poor people live in small dank dwellings and open the window. The rich still believe in
fresh air, have trouble finding painters who know what to do with double hung sash. Everyone
else believes in the miasma.
Windows are sealed shut. Sealed shut to keep out the unknown. Heating or air
conditioning is on 100% of the time. Opening windows is something very old people or very
rich people do, otherwise Americans do not.
The flip side of that is performative masking. When out of doors, even in the most
uncrowded spaces, the maskies are never seen without the mask. Not science, fear.
Drug companies are lobbying the Biden administration to block a push at the WTO by India,
South Africa and about 80 other countries for a temporary waiver on patent protections for the
new vaccines. The pharmaceutical industry argues that innovation as well as vaccine quality and
safety depend on maintaining exclusive intellectual property rights.
"Eliminating those protections would undermine the global response to the pandemic,"
industry executives and the Pharmaceutical Research and Manufacturers of America, their
powerful lobbying group, warned President Biden in a letter this month. Biden has sided with
the drug companies so far. The United States on March 10 joined Britain, the E.U. and
Switzerland in blocking the push for waivers.
In an exclusive interview with Lester Holt, Pfizer Chairman and CEO Albert Bourla discusses
the company's Covid-19 vaccine -- including the potential for a booster shot, vaccine trials
for children and more.
Fatm
Marq ,2 weeks
ago
and does anyone expect a CEO to tell the truth about his company's product?
4 days ago
Do you really trust this guy? Research The World Economic Forum, read who they are tied to
and the goals the have (in their own words) you will be shocked
Yu WuDu 1 week
ago
Welcome to technocracy! Oh your Antivirus definitions aren't up to date, we need to plug
you into Windows update before we can let you onto the Internet of Idiots.
1 week ago
How good is this vaccine if, and I quote "the weakling that who are affect the whole
society" (great English but that's just a side note) So his product does not provide immunity
longer than 6 months essentially, requires a yearly dose (profit) and requires 100% to take
it in order to work. What a joke!
1 week ago
-- Pfizer former chief respiratory research scientist (Dr. Yeadon) Most in depth honest
information on C19 https://www.youtube.com/watch?v=II4wkMKCt-c&t=29s
FactsOver Fiction 2 weeks ago
As CEO, much of Bourla's compensation is in stock. He's a very well-paid drug salesman. He
won't tell us the objective truth about his company's vaccine. It would hurt stock price and
his own wealth. C'mon, NBC ... Interview an objective scientist. This is just an ad in
disguise.
andrew kis 2
weeks ago
pfizer need get advices from expert financial, how to improve spinoff and improve
shareholder interest to make a better company. dividend, number of shareholder, debt ,
variant of products.
1 week ago
(edited)
So the data suggests 52% immunity after 1st dose and 6 months protection with current
data, but possible a 3rd dose at 6 months or a year to cover variants and unknown protection
after 2nd dosage after 6 months, but 95% in the first 3 months. OKAAAAYYY.. ahhh.. hummm.. i
think i'll keep the mask on after the 3rd dose! oops, wait 2nd dose, but maybe no 3rd.
nevermind. "Doctor Bourla, are you optimistic"? .....Ahhhhh, well Lester, yes, no and maybe
but we'll have to wait and see...
4 days ago
I'd like to know why you haven't asked the CEO why his company gets blanket immunity???
Why did you not ask this man how many people have died so far after getting your second
dose?? And can you please tell us what some of the really serious adverse effects that some
people have been experiencing after the second dose??
What are the long-term effects of this vaccine on people's brain?, is there any indication
that this gene therapy which is being called a vaccine will cause early-onset dementia
because of Spike protein will start attacking the brain?
How many pregnant women have had a miscarriage after getting a second dose or even first
dose for that matter,??
What are the long-term effects of this gene therapy on women that are in childbearing
ages??
What will the gene therapy that's being called a vaccine do to the fetus when it comes to
full term are there any indications that there's going to be some long-term effects like
birth defects or genetic effects problems with the ability of this fetus to develop to full
term in reference to their sexual organs?? The reason I mention these things is because these
people that are associated with this vaccine believe in Eugenics and believe in depopulation
because of not only their psychosis but because of climate change we absolutely have to
reduce the population!!! Is this gene therapy vaccine being used to sterilize many human
beings so that we don't get into this overpopulation and then we will not be able to deal
with climate change???
And why haven't we asked this man has his company ever worked on an mRNA vaccine before
and ever tested on any animals whatsoever prior to this covid-19 planned pandemic??
If the answer is yes and these animals were Gravely injured there for this mRNA couldn't
come to full fruition and now it's being used on human beings because we're in this plan
pandemic is this just another way to experiment on the population with this mRNA gene
therapy? Another question if there was no plan pandemic would Pfizer have rolled out an mRNA
vaccine for the cold which is caused by a Coronavirus?
Does anybody think that Pfizer Maderna or anybody else would be getting approval to
experiment on the masses if there wasn't a covid-19 planned pandemic??
How come nobody is asking the CEO where is he getting the biological material to make this
mRNA?? I am just really really really curious white nobody wants to ask that question and why
people are allowing these people to inject them and they had no idea where these companies
are getting the MRNA from is it from aborted fetuses is it from jellyfish is it from where
what biological stores are they getting this mRNA
from.?????????????????????????????????????????????
Before you decide to take this vaccine why don't you see if you can get the answers to any
of these questions and my challenge to you is that you will not I repeat you will not be
getting the answer to any of these question. And the story you just will not get the answer.
The person that sticking you with this gene therapy won't tell you your doctor won't tell you
the media won't tell you dr. Fauci won't tell you and I bet you anything that CEO will not
tell you... WAKE UPPPP
2 weeks ago
Older adults who received a single dose, the proportion testing positive for antibodies
was just 34.7 per cent in those aged 80 and over for the Pfizer vaccine.
2 weeks ago
In "immunological language"..NOTHING. Any benefits, only risks and secondary effects
2 weeks ago
I am frustrated to read the raft of cynical comments on Pfizer's achievement in takIng the
vaccine from a lab success to a huge mass immunisation program. Before mindlessly bashing
pharmaceutical companies find out the answer to the question "Why are you not terrified of
polio". I am old enough to remember the last of the polio epidemics, the terror and the
social disruption. Stopped dead by Dr Salk and big pharma. If you lack the scientific
knowledge to criticize intelligently and propose improvements, say nothing
DJ Pomare 2
weeks ago
Covid deaths US 523,082 UK 122,415 Mexico 184,474 Canada 21,915 China 4,636 Australia 909
NZ 26 Taiwan 9. Two thirds of the Covid variants originate from the US making Covid the US
virus. There are 15 Covid variants, 10 from the US, 2 from the UK and 1 each from South
Africa, Brazil and China. Traitor Trump's "Do nothing" pandemic strategy will be written into
the history books as America's biggest-ever failure.
1 week ago
this guy is a vetrenarian. no surprise that he is treating people like animals.
2 weeks ago
Why are you not reporting the side effects and death happening to many post vaccine? Why
are you not reporting that people in Israel are being coerced into taking this experimental
product and without proper knowledge and informed consent?
2 weeks ago
(edited)
The twice repeated 52% number is purposeful lie, not a slip-up or confusion. Why did
Lester not call him out on this? 52% includes cases before the vaccine even had a chance to
take effect. Lester was totally hoodwinked. Moderna was much more upfront on their data.
2.16M subscribers
SUBSCRIBE
Pfizer has become a terror. The US pharma company is reportedly asking for military bases and sovereign assets as guarantee
for vaccines. WION's Palki Sharma has the details.
,
1 week ago (edited)
I am
from Patagonia, Argentina and what the journalist says is TRUE...! We went with the SputnikV and China's Sinopharm. Cheers
Indian brothers...!
,
2 weeks ago
Boycott money-hungry companies such as Pfizer.
S Gomz
,
1 week ago
Pfizer is going the CCP way. Loot the poor and the desperate.
,
1 day ago
"Borders of sovereignty and dignity" should always be kept in mind !
World renown vaccine specialist, Geert Vanden Bossche, gave a groundbreaking interview this
week risking his reputation and his career by bravely speaking out against administration of
#Covid19 vaccines.
In what may be one of the most important stories ever covered by The Highwire, the vaccine
developer shared his extreme concerns about these vaccines in particular and why we may be on
track to creating a global immunity catastrophe.
Could someone clarify one thing: is Dr. Bossche referring to all the COV2 vaccines or just
the mRNA ones (i.e. Pfizer and Moderna)?
Polite question
The vaccine companies admit there will be adverse effects, including death, but claim that
the benefits out-weigh these risks (millions of lives saved without proof, etc.). The companies
and the CDC does claim, however, that the spike protein mRNA will never get into the cell
nucleus and alter cellular DNA. This is a provable lie. Stem cells divide to replace cells
damaged by SARS viruses. When the stem cell is dividing, the nuclear membrane dissolves. Hence
the spike mRNA can alter the DNA by reverse transcription. Another possibility is the
nanocapsule will penetrate the nuclear membrane. If the spike protein contributes to
antibody-dependent enhancement (ADE) of disease, then permanently encoding the spike protein in
stem cell DNA will likely cause long-term chronic or recurring disease. Auto-immune attacks
will damage organs, and the repair and replacement cells will elicit a new round of auto-immune
attacks. Many scientists on the boards of these vaccine companies have research programs on
stem cells and must know these are viable risks. Vaccinated persons who develop disease or die
should have organ tissues assayed for spike protein DNA. That would prove one way or the other
if intentional lies are being delivered to the public.
Excellent and practical information. Unfortunately, there are a lot of people that have been
made to believe that the only solution is the current vaccine. But if you watch the interview
in its entirety, Geert does NOT denounce vaccines. He denounces THIS ONE.
All any of us can do, before blindly rolling up our sleeves, is be INFORMED. And not be so
arrogant that we refuse to listen and heed warnings and advice. And unless you are anywhere as
educated and knowledgeable as Geert, I trust you will leave your "karening " to yourselves
lives depend on it.
He has posted his letter to governments etc., on his LinkedIn account. Its worth a read.
Has it been even proven medically/scientifically that this virus actually exists? There are
many professionals coming out now saying it has not been medically proven that this is an
actual (non-flu) virus. And additionally, whatever happened to the flu? Has Covid replaced it
or defeated it or ? Correct me if I am wrong but seasonally the flu kills 50k-60k people. And
then how many people have actually died as a DIRECT result of this alleged COVID-19 virus?
I suggest most Virologists are over educated thespians with silver tongues.
Bacteria have always been the deadliest because they can infect, thrive & kill in humans
with healthy immune systems. I suspect bacterial pneumonia was one of the leading causes of
death until antibiotics became available. Plasmodium Protozoa [Malaria pathogen] continue to
kill 500,000/year. The number would likely be in the millions had we not discovered effective
treatments.
However, PRIONS are the most deadly pathogen known to man. All prion diseases have longer
incubation periods than most other pathogens and they are always lethal. They are incredibly
small so extremely difficult to detect and even harder to kill. Many suspect that Alzheimer's
syndrome is caused by some type of prion.
If I were a Godless, Crazy Megalomaniac with an agenda of ruling the World and eliminating
several billion useless humans using up my global resourses:
The highly inaccurate pcr test was the cause of this so called pandemic of a virus that has
not been isolated. I urge everyone to go to some of Reiner Fuellmich interviews where he
explains. He has international EXPERTS. Also has a WHO whistleblower interview.
The reason for decline in cases is because the northern hemisphere is coming out of their
flu season, nothing to do with the vax. 24
What would the implications be for, say, blood transfusions, in the future?
Go back in history & look at the 1918 Spanish flu, masks mandates, vaccines, the war
& the Global monetary change system that occurred all at the same time. Coincidence, I
think not. Discernment & common Sense should have prevailed by now. I pray for the ones who
are not woke🙏🏻 31
If Geert is correct, it seems that the pandemic was used to justify the development of a new
technology that is not necessarily the most applicable to the current situation but would be a
versatile tool with many questionable potential applications going forward; an enticing toy, if
you will, for those who might think that the world is their laboratory. We need to be informed
by this without succumbing to alarmism or panic.
What is unclear to me is why this scientist (Geert) claims that he has no problem with the
vaccines being developed to fight covid-19, yet also says they permanently disable or
ineffectuate one's own natural immunity. That is a crazy, catastrophic outcome of a vaccine by
itself. Totally unacceptable
So there are 2 issues really – a) how the covid-19 vaccines actually operate within
the human body, causing harm (by permanently knocking out a person's natural immunity); and b)
the effect of mass vaccination of sub-effective vaccines during a pandemic, driving increasing
viral lethality that society or science will not be able to counter. Two completely separate
issues, but they are not treated here as separate concerns.
I would really like to see more examination, analysis and explanation of the first concern.
If the general population understood how harmful the vaccine actually is to themselves
personally, it would demotivate a large percentage of the population to accept the vaccine, and
possible dramatically reduce the risk of the 2nd concern.
He has post doctoral training in Animal virology and he is spreading misinformation. He has
not been on any significant academic site. He probably did work on animal diseases with the
companies you cite.
The biggest over reaction in all of human history which is becoming something more because
of human over reaction – do not take this vaccination. I know I will not willingly take
it.
I trust my natural immune system against any and all man-made interferences! I have reached
76 years of age with no interference from the "scientists". I care for my God-given protection
and it works! In England the NK cells are called T-cells and they give orders for the bone
marrow to make Killer T-cells to destroy pathogens. Those in power are on a culling of humans
and these genetic engineering injections will do what they are supposed to do!!
If Dr. Bossche is so talented and worked for Gates a GAVI, (He calls not-for-profit) why was
he not involved in the development of the mRNA injections? His name never comes up. Hsaive 1
day ago
Variants Do Not Exist Because SARS-CoV-2 does not exist -- - Dr. Geert Vanden Bossche Says
"Halt All Covid-19 Mass Vaccinations Immediately" – BUT BEWARE! .Bossche then claims the
global population must undergo another round of mass vaccinations!https://tinyurl.com/azyfa8fs
I read Dr Vanden Bossche's letter he seems to be advocating we don't mess with herd immunity
vaccines interfere with natural immunity, etc. Sweden chose this option initially in the
pandemic and that approach has been reversed lately because too many people died. He is
experienced enough to propose concrete steps to be taken that could mitigate against the
dangers of the possibilities he brings up i wish he'd done that. As a 60 something year old
person with some co-morbidities i do not have a low risk if i got COVID i can't wait to get my
second shot. As for new variants they are caused by mutations of the virus and if there is less
virus there will be less mutations trying to link vaccines to somehow be a cause of variants is
very fuzzy logic.
What baffles me; they have been giving flu shots for years due to new varients. Question we
need to ask is have we seen a more virulent strain due to this
Clueless Joe , Mar 15 2021 22:33 utc |
80
US worrying about vaccine competition is so stupid when only a handful of countries have
got their hands on enough vaccines right now, and when US and UK are hoarding them like
crazy. It's not a 0-sum game for now, every bit helps. Gee, EU is in a bad state due to all
pharmas failing to deliver.
Besides, it's funny to see US complaining about Russia badmouthing MRNA (so Pfizer and
Moderna) when it's Astra-Zeneca which is gets gloomy headlines on a daily basis.
That said, I'd have no issue with Western countries relying on MRNA vaccines and taking
the bulk of them, as long as it means the easier to produce and distribute, Sputnik, AZ, J/J,
the Chinese ones, are reserved for the rest of the world; it's probably the best way to
ensure most countries will vaccinate their most vulnerable citizens in a realistic timeframe
- at least before the year is over, if not earlier.
As for Latin America, Chile is doing great, and is relying mostly on Sinovax for now if I
remember correctly - like many others, it probably ordered a ton of other vaccines, but won't
need them, so hopefully they'll be sent to neighbouring countries instead.
vk
86
China's response to the USA's official claims:
West
'weaponizes' vaccines to divide world aimed at maintaining hegemony
"The West does not see vaccines from a professional and scientific perspective and now
wants to use its technological advantages to squeeze China. While the West accuses China of
engaging in vaccine diplomacy, the very one that wants to engage in vaccine diplomacy is
the West," said Zuo.
--//--
@ Posted by: suzan | Mar 15 2021 21:33 utc | 69
Human adenovirus is a completely different technology than chimpanzee adenovirus, and both
are completely different technologies from mRNA. Just three completely different things.
All viruses interact with their hosts' DNA and can potentially alter them forever. Indeed,
we can restore fragments from very old viruses on the basis of DNA of third species. That is
a natural and unavoidable aspect of life, and cannot and will never change.
Either way, the debate you bring up is moot point, because DNA mutation is not the issue
with mRNA and chimpanzee adenovirus. The crux of the debate is this: human adenoviral
vaccines are an already existing technology, tried and tested. We know they work and we know
they're safe. That's not the case with the other two, which are completely untried and
untested until last year.
Debsisdead , Mar 15 2021 23:36 utc |
87
Right now it is difficult to ascertain whether the euro -scare over the A-Z jab causing
blood clots is tosh or not. The Pfizer jab also had a recipient suffer a blood clot, in
amerika, early in the vaccine rollout so it is not inconceivable that all covid vaccines may
have a propensity for inducing thrombosis in a small percentage of recipients.
There is a little evidence however which indicates that at least some of the thrombosis
deaths occured outside the range of 'normal' for thrombosis. Norway and Denmark two countries
with well established public health systems and far more comprehensive than most other
countries medical databases of their patients, were the first to blow the whistle. There were
allegedly features of these post jab thromboses which took them outside the range of
normal.
The deaths occurred in citizens at a younger age than is normal for thrombosis death and
the blood clots occurred in lungs which had a lower than usual number of platelets in the
blood, which is the opposite of what one would expect since platelets are an important part
of clotting, how is that people with lower than usual platelets in their blood developed
clots.
On the other hand the entire yarn may be just another story put out by the puppets of
competitors in an extremely lucrative immature market.
That includes involvement by 'intelligence' services located in embassies.
I agree it is wrong and publicising it is essential, but as I said there should be no
surprise. Aotearoa has recently (about two weeks ago), announced that the population will all
be vaccinated with the Pfizer mRNA vaccine. The jabs will be free or extremely low cost for
most (certainly much less than the USD $60 Pfizer demands) and I had been wondering how
Pharmac, the national agency which makes decisions on all drug purchases managed to beat
Pfizer down. Pharmac has a reputation for favouring generics ahead of hi-cost originals.
Perhaps they didn't, although I reckon Pharmac being Pharmac they would have got a pretty
good deal but maybe not as good as usual since Aotearoa governments, particularly ersatz left
administrations have a habit of doing easy deals with five eyes partners as a way of avoiding
agreeing to actions that will alienate voters, even worse lose trade or even sometimes tho
rarely, because the inhumanity is too great.
eg Australia is in
big trouble with China over PM Morrison's stupid claims about covid and Uyghur chinese,
whereas Aotearoa is not. Despite pressure from USuk, Aotearoa hasn't jumped aboard the "let's
all sledge China" ship. If that was achieved by kowtowing to amerikan bullies over less
vital, less public and less divisive issues, good on them. That is a major from me who has
little other than contempt for the neolib twats in control of Aotearoa.
Or it could be that it is like the AZ thrombosis thing could be, no connection at all.
norecovery , Mar 15 2021 23:42 utc |
88
K @ 84 – I agree 100%, and would add there are other ulterior motives besides profit
and gaining public consent, namely attempting to exert political and economic control of
competing/dissenting countries. The fact that some of the world's elite have organized such
contemptuous mafia-like organizations that demonstrate total disregard for human life and
dignity is enough to seriously question their motives in this case as well.
U.S. And Its Five Eye Partners Use 'Persuasion', Sabotage And Disinformation To Gain
Vaccine Supremacy
The U.S. and some of its allies are engaged in efforts to malign the Russian Sputink V
vaccine and to promote the more expensive mRNA vaccines produced by 'western' companies.
Back in November we warned that the
vaccine competition would be ruthless :
The mRNA vaccines hyped in the U.S. media are simply too expensive to be used around the
world. If we want to limit the global effects of the SARS-CoV-2 pandemic we will have to use
the cheaper vector based vaccines.
That the AstraZeneka vaccine was immediately attacked in U.S. media by an unqualified
writer quoting an investment bank and the U.S. pharma promoting (Remdesivir!) Antony Fauci is
quite suspicious. Pfizer and Moderna expect to make billions of dollars with their vaccines.
They will use all possible ways and means to defeat any potential competition.
Vladimir Putin, the President of Russia,
recently noted how unfair competition practices are used to keep some vaccines away from
nations who urgently need it:
Producers are struggling for the global vaccine market worth $100 billion, Russian President
Vladimir Putin said on Thursday.
Some producers compete unfairly, sell a small batch of vaccines at a lower price on the
condition to be an exclusive supplier, Putin said, speaking at a video meeting on measures to
boost investment activity in Moscow.
"We see how competitors behave in the global vaccine market worth $100 billion. They come,
sell a small batch of their vaccine at a discount, on the condition that everything else will
be purchased only from this producer," he said.
To no one's astonishment the U.S. government is directly involved in manipulations of
vaccine accessibility. As Brazil Wire
found :
The US Department of Health and Human Services recently published its Annual Report for 2020.
"2020 was one of the most challenging years in the history of our country and in the
history of the Department of Health and Human Services", former US Secretary of Health and
Human Services Alex Azar introduces the report.
"There is an end to the pandemic in sight", he continues, "with the delivery of safe and
effective vaccines through Operation Warp Speed".
Tucked away on page 48, the report shockingly reveals how the US pressured Brazil to
reject Russia's Sputnik V vaccine.
The HHS Annual Report is here . On page 5 it
says:
Developing a strategy for supporting global vaccine access : HHS's Office of Global Affairs
(OGA) led the development of an interagency strategy, coordinated through the National
Security Council, to provide international access to COVID-19 vaccines once domestic needs
are met .
"Once domestic needs are met" is certainly not an altruistic or even reasonably prioritizing
strategy one should be proud of. A sensible effort to save lives and to end the pandemic would
prioritize risk groups in every country of this planet before inoculating people at home who
have little risk of serious Covid-19 complications.
On page 47 the HHS report notes that the U.S. is coordinating with its Five Eyes spy
partners on vaccine 'messaging':
Combating vaccine hesitancy globally : OGA leads a group of the Five Eyes countries (U.K.,
Canada, Australia, New Zealand and the United States) on vaccine confidence, aligning our
nations' efforts and sharing best practices to enhance vaccine confidence messaging globally.
One page on we learn what such communication entails:
Combatting [sic!] malign influences in the Americas : OGA used diplomatic relations in the
Americas region to mitigate efforts by states, including Cuba, Venezuela, and Russia, who are
working to increase their influence in the region to the detriment of US safety and security.
OGA coordinated with other U.S. government agencies to strengthen diplomatic ties and offer
technical and humanitarian assistance to dissuade countries in the region from accepting aid
from these ill-intentioned states. Examples include using OGA's Health Attaché office
to persuade Brazil to reject the Russian COVID-19 vaccine, and offering CDC technical
assistance in lieu of Panama accepting an offer of Cuban doctors.
"To persuade Brazil to reject the Russian COVID-19 vaccine" is, simply said, criminal
behavior that has near genocidal consequences. Brazil is currently getting swamped with a
more
infectious variant of the SARS-CoV-2 virus and its medical institutions are
near a breakdown :
"It feels like we're putting a Band-Aid on a bullet wound," said Eduarda Santa Rosa Barata, a
31-year-old infectologist who works in three ICUs in the north-eastern capital of Pernambuco
state, all now stretched to the limit. "We're engaged in damage reduction You open new beds
and they fill up immediately."
A few days earlier, Barata had admitted a 37-year-old man who had no underlying medical
conditions but whose lungs were so badly damaged he needed intubation. "It seems so random,"
she said. "It's a bizarre disease. It's frightening."
Panama, which under U.S. pressure rejected an offer from Cuba for medical support, has one
of the highest death rates from Covid-19. That is one reason why its economy shrank by 18% .
The HHS report also speaks of Bolivia :
Opening Bolivia to health diplomacy : After decades of silence between the U.S. and Bolivia,
OGA re-established health diplomatic relations with the Ministry of Health of Bolivia
following national elections. Re-engaging allows the U.S. to strengthen ties in the region,
which is important for influence in regional and multilateral fora , including the Pan
American Health Organization.
What was "following national elections" in Bolivia was
a fascist coup which produced repression and tyranny. The U.S. used its cooperation with
the coup plotters to influence other organizations.
Meanwhile the U.S. is also falsely stating that Russia is spreading vaccine disinformation.
Following a Wall Street Journal piece planted by U.S. officials these
claimed , without evidence, that Russia was sowing fear about the mRNA vaccines:
On Sunday, the Wall Street Journal reported that four publications, all serving as fronts for
Russian intelligence, have targeted Western-produced COVID-19 vaccines with misleading
coverage that exaggerates the risk of side effects and raises questions about their efficacy.
The State Department confirmed that report on Monday, saying U.S. officials had identified
four Russian online platforms that were spreading disinformation about the COVID-19
vaccines.
However paragraph 21 of the original WSJ piece, coauthored by Iraq WMD
propagandist Michael Gordon,
acknowledged :
In each case, the Russian outlets were repeating actual news reports ,,,
The 'Russian outlets' repeated the news 'western' news agencies were distributing. It is
nice though to see acknowledged that such is often disinformation.
There are some signs that the U.S. is coordinating with its spy partners to malign the
very
efficient Sputnik V vaccine . The British Royal United Services Institute (RUSI) recently
put up a comment that warns of Russia's soft power gain
through vaccine diplomacy especially in South America:
Sputnik V's rapid foray into new markets in Latin America may indeed have longer-term
implications in an area that has traditionally been the US's backyard. Argentina gratefully
received more than half a million doses in January. It served as an embassy of sorts for
Sputnik V; reportedly, Argentinian delegations to Moscow in late 2020 translated reams of
details into Spanish and shared these with Bolivia, Peru, Mexico, Uruguay and Chile to speed
up their ability to decide. Bolivia's first batch arrived at the end of January. By
mid-February, Mexico received its first 200,000 doses. By mid-March, Brazil and Peru appeared
close to sealing respective deals.
This is followed by musings about potential sabotage targets:
There are several factors that could make Sputnik V's current bounce shortlived. The
inability to deliver supplies quickly is an immediate one. Russia has acknowledged its
production squeeze, raising doubts about its ability to honour its vaccine pledges. It is
dependent on plants in the likes of Brazil, India and South Korea upholding good
manufacturing practice and delivering at speed and scale on Moscow's promise to provide
hundreds of millions of quality vials quickly.
The piece closes with an ominous call to action:
The biomedical science of Sputnik V may well be genuinely welcome worldwide, once full data
is available and has been appropriately interrogated. But the corresponding political
ramifications of deeper and wider Russian influence globally may not be so beneficial. The UK
and the US must not be blindsided to the full extent of Russian vaccine diplomacy already
underway.
The U.S. efforts to prevent Russian vaccine distribution failed in Argentina where President
Alberto Fernández has led an early
and successful effort to introduce the Russian vaccine:
Amid plenty of public skepticism, Buenos Aires sent missions to Moscow in October and
December 2020 to inspect data from the vaccine's phase 3 trial.
An Argentine presidential aide said the delegation had translated hundreds of pages of
information about the vaccine into Spanish -- necessary for approval -- which it later shared
with other governments in the region, including Bolivia, Peru, Mexico, Uruguay, and
Chile.
This is how, a day before the phase 3 results were published, trucks of Sputnik V shots
were already trundling through Bolivia's countryside. A photo of a delivery in a
poultry truck draped in a Bolivian flag -- a creative (and health department-
approved ) solution for cold storage requirements -- went viral. Argentina began
vaccinating with Sputnik this past December, meanwhile, and Mexico announced the purchase of
24 million Sputnik doses on Jan. 25.
U.S. efforts to dissuade countries from acquiring Sputnik V have not be fully successful.
That again requires to launch a propaganda campaign to malign Sputnik V wherever it is
distributed:
Maxim A. Suchkov @m_suchkov - 15:35 UTC · Mar 13,
2021
1. #Putin: "Global market for #COVID19 vaccines is worth $100 billion. We see how
competitors of our producers behave: they enter a country [that is in need for vaccines],
sell a small batch of vaccines on a discounted price but condition the sale with that...
2. "...the country will only purchase that vaccine from that producer in the future. So,
there's a real fight for the markets".
3. $100 billion is a big market. #Russia makes over $15 bln on arms sales (unofficial
stats have it as high as $55 bln), about $25 bln for agricultural sales; around the same
amount on gas sales (thou it depends on supplies), oil and oil products a little over than
$100 bln.
4. So all of a sudden there's this huge market and there's heavy fight over it.
@dimsmirnov175 cites an anonymous "source in the #Kremlin" who said that Russian intel
services are aware that their foreign counterparts seek to launch a massive infowar against
#Russia/n vaccines
5.The source reportedly said that soon there'll be many reports over #Russia/n vaccines
inefficiency & that they even health dangerous. Allegedly, even "staged cases of massive
losses of human life after using Sputnik V will be propagated via @USAID, @georgesoros
@thomsonreuters
6. The target audience for this campaign will be European countries who registered
#SputnikV for their emergency use – #Hungary, #Slovakia, #Montenegro, #SanMarino and
N.#Macedonia.
7. On a parallel track,#US & allies, according to the "Kremlin source" 'd release
"investigations" about "incompetence of #Russia/n specialists in vaccination & immunology
to halt their certification by @WHO, other relevant agencies , lower demand for RU vaccines
from other countries
8. "The #Kremlin source" adds #US "aggressively promotes @pfizer, eyes to make sure US
free of not only from the payment of possible compensation to citizens in lawsuits in the
event of side effects, but also from liability for negligence of the direct manufacturer"
9.#SputnikV now world's 2nd in terms of demand with 50+ countries having provided permit
for its use. Struggle for markets in #Europe,#LatinAmerica,#Africa #Asia will get even bigger
when we'll [most likely] learn that vaccination is not a one time deal but a seasonal routine
/END
PS.This chart is telling in the kinda tricks one may pull: #Russia's #SputnikV completed
all the stages, but designers of the chart (1) put it at the bottom (2) don't use its product
name (3) mark it with (*) caveating its effectiveness as if ABC "independently fact-checked"
others
ABCnews - bigger
Graphics like the above are only one example of media manipulations in support of 'western'
vaccine 'diplomacy'.
This is more than just arrogance:
The West's reaction was not exactly objective in August 2020 when Russia presented the
world's first corona vaccine. Words like "vaccine muck from Moscow", "nasty vaccine
propaganda", and accusations of "clumsy manipulations" of a "high-risk experiment on humans".
Distrust, malice and suspicion were easier to find. One newspaper quipped that Sputnik V was
effective not only against the virus, but also against "homosexuality as well as epilspsy and
hives."
The Five Eyes, their intelligence agencies and friends are pulling all possible strings to
win the markets for their vaccines. The
continuous delaying of the
official EU authorization for Sputnik V is obviously a part of this sabotage
scheme .
That these efforts will keep people away from other good and available vaccines and that
this will inevitably cost a number of them their lives, is seen as a reasonable price for
gaining vaccine supremacy.
Posted by b on March 15, 2021 at 12:16 UTC |
Permalink
Paco , Mar 15 2021 12:32 utc |
1
Nice compilation B on what basically is another big sign of western decadence and immorality.
As you very well state what is needed is a global vaccination of groups at risk to avoid
mutations and new variants of the virus, and not vaccination within borders while others
wait. Carl , Mar 15 2021 13:02 utc |
2
Reminds me of the government's efforts against Rearden metal in the novel Atlas Shrugged. One
must appreciate the irony that the US, the epicenter of Randian ideology, is trying this.
Mauro , Mar 15 2021 13:49 utc |
7
They are shameless, ast it is declared even in their U.S. Department of Health & Human
Services annual report, look at page 49 !
https://www.hhs.gov/sites/default/files/2020-annual-report.pdf
"Strengthening Health Cooperation and U.S. Humanitarian Leadership
Examples include using OGA's Health Attaché office to persuade Brazil to reject
the Russian COVID-19 vaccine, and offering CDC technical assistance in lieu of Panama
accepting an offer of Cuban doctors."
Jackrabbit
10
The Russia-USA vaccine battle obscures another, possibly more important one: mRNA
vaccines vs. all the rest.
Moderna got much of its early funding from the US Military. The Military is interested in
mRNSA as a bio-weapons defense - the tech allows quick formulations to protect soldiers. But
the ability to better defend against bio-weapons also makes USA use of bio-weapons more
likely. Just the side that has an effective defense against ballistic missiles is more likely
to use them.
Given such knowledge, one can question the many problems of the OxfordAstroZeneca (OAZ)
vaccine (latest: Norway is looking into the possibility that the OAZ vaccine causes blood
clots) and the late entry of the J&J vaccine (a full three months behind Sputnik V and
Sinopharm).
But wait, there's more: By not fighting SARS-COV-2 effectively (like some countries did),
mutations were virtually certain to happen. That makes the mRNA technology incredibly
valuable for ability to quickly adjust to new strains. And who knows what other viruses will
unexpectedly /sarc pop up in the near future?
Will American sheeple ever be allowed to question the Trump Administration many failures
in fighting the pandemic - starting with Trump's bogus air travel ban and his lying about the
severity of the virus? Not likely. New York State Governor Cuomo is now being hounded out of
office with flimsy sex allegations to (IMO) prevent a review of the policy of sending people
home to "self-isolate". "Self-isolate" and the "bend the curve" goal (instead of defeat the
virus) virtually guaranteed that the pandemic would continue to spread.
!!
migueljose , Mar 15 2021 15:03 utc |
13
librul@3
snake , Mar 15 2021 15:03 utc |
14
what this summary of the vaccine shows me is that the nation states are marketing agents
and mafia like defenders of the makers of the products of those private parties who have
control over the nation states (government).
clearly the nation state system and its agencies have by their actions proven themselves
to be a problem in need of fixing for the 8 billion people who occupy the planet.
jared , Mar 15 2021 15:18 utc |
15
Early on, there was reporting that the novel (as in recently created) corona virus was
mutating rapidly - approximately every 4th transmission was claimed.
psychohistorian
16
When you live in a social system that has global private finance at its core, what do you
expect?
The West is proud of its barbarism and flaunts its lie/cheat/steal mentality. We are
standing by hopeful as that meme drives itself into the ground taking many with it. We just
hope it isn't all of us in a pique of self loathing when the bottom is near.
What a shit show to live in the middle of. It is almost like folk think its weird to do
things for the right reasons instead of profit....and they call themselves Christians as they
blindly follow their devilish leadership.
jared , Mar 15 2021 15:33 utc |
17
Hypothetically, genetic research gives us the means of widespread, genetically targeted,
destruction and new tools for pharmaceutical development. Dangerous situation in a
neo-liberal world order.
Sam F , Mar 15 2021 15:52 utc |
19
Of course Russia has no need to spread fear about US mRNA vaccines, because these are the
most expensive and difficult to distribute, and the US has conspired to prevent any
humanitarian distribution, an historic disgrace. Many will long remember that Russia offered
vaccines at cost while the US maximized profits, and Bill Gates obliged Astrazeneca to seek
profit rather than humanitarian distribution.
Christian J. Chuba , Mar 15 2021 15:56 utc |
20
Russia vs the U.S. deaths per million
But Russian vaccine production has underperformed. I cannot even find a number for
it but if I look at deaths per million, 6 day rolling average, Russia is not in a sustained
downtrend yet. When a country reaches heard immunity, this will go into a sustained
downtrend. Russia has not even been able to vaccinate their own population...
carl s. , Mar 15 2021 16:50 utc |
25
librul @3
Can someone please explain
the following ?
"Johnson & Johnson's vaccine is the third coronavirus vaccine to receive FDA approval,
but the first vaccine requiring just one shot for vaccination. The drug showed a 67
percent effectiveness against moderate to severe COVID-19 infections and about an 85
percent effectiveness against the most serious illnesses . While two other FDA-approved
vaccines have efficacy rates in the 90s, Johnson & Johnson's drug was shown to
prevent 100 percent of hospitalizations in a clinical study of around 44,000 participants
in the United States. "
If the jab has a 67% efficacy against moderate to severe infections, how can it have an 85
percent effectiveness against the most severe infections? How can it prevent 100% of
haspitalizations in 44,000 subjects? Unless perhaps the figure of 67% represents people who
took the shot after contracting the disease? But that doesn't make sense either.
Statistical illiteracy on the part of the writer? How much of all that is true?
carl s.
Digital Spartacus , Mar 15 2021 16:42 utc |
23
@ Christian J. Chuba 20
Funding
Jackrabbit
29
james @Mar15 16:56 #26
... so what vaccine are you going to be getting?
mRNA vaccines may be the only game in town if the virus keeps mutating quickly and/or new
viruses are introduced.
What I object to is the near complete lack of cynicism. Many moa readers will recall the
phrase: "Question Authority"
!!
m , Mar 15 2021 17:49 utc |
30
@25 carl s.That's the number according to international standards and rhe number which allows
comparison to other vaccines. All the other quoted numbers are just there in order to
obfuscate the fact that it is significantly less efficient than the mRNA vaccines.
Jackrabbit
31
Follow-up to @Mar15 17:45 #29
The 'woke' are currently focused on race and sex with some concern for inequality and a
living wage. 'Anti-war' isn't yet on the radar screen for most of them, though it should
be.
!!
Jackrabbit
12
Follow up to my comment @Mar15 14:45 #10
Gilad
Atzmon has written about Israel's 100% vaccination program and questioned if it may lead to
new, more virulent, forms of the virus
To anyone paying attention, this warning is a fore-shadowing.
!!
juliania , Mar 15 2021 20:58 utc |
64
jackrabbit @ 12, thanks SO much for that excellent video link! As the two participants
were discussing, I had the thought that the vaccine situation they are analyzing is very much
like the GMO experimentation we have all been subjected to around the world when those seeds
were presented to us, and the virus being a part of our life system, is like the weeds which
were enabled by the practise of using GMO seeds and then spraying the crops with virulent
herbicides those seeds were now inoculated to resist --- it all meant that the situation in
farmer's fields, while the crops themselves survive (much as do inoculated with the vaccine
persons) the situation at large gets worse!
It is an excellent conversation also on the side issue of whether science benefits from
shutting down dissent. We should all think about that!!
Mina , Mar 15 2021 21:04 utc |
65
On BioNTech; designing the vaccine on a table corner in a few hours
https://www.businessinsider.com/pfizer-biontech-vaccine-designed-in-hours-one-weekend-2020-12?international=true&r=US&IR=T Mina , Mar 15 2021 21:07 utc |
66
Soon we'll all be making vaccines in our kitchenhttps://www.dw.com/en/german-coronavirus-vaccine-inventor-being-investigated/a-56828943
Jen , Mar 15 2021 21:10 utc |
67
Tannenhouser @ 57:
Vaccines in the strict sense of the term use weakened or inactive forms of the virus they
target to stimulate the immune response. MRNA vaccines don't: they insert a protein
resembling a protein on the coronavirus's outer coat into the RNA of your cells so your body
makes these proteins itself to prime the immune response. That's my understanding and I stand
to be corrected by others.
oldhippie , Mar 15 2021 21:38 utc |
70
john @ 68
That first link in your post is to Geert van den Bossche and is an excellent interview.
Worth the time. Somewhat annoying music at start, in all ways the best take I have
encountered on how mRNA works. Much more accessible than some of what that author has been
putting in print.
suzan , Mar 15 2021 21:33 utc |
69
@ Jackrabbit
The Adenovirus vector vaccines are DNA vaccines. The primary difference between them
(Sputnik V, Astrozenica, J & J and some more) is the type of Adenovirus vector used, for
example human or chimp, how they are cultured, and the specifics of production and
processing.
All of them use a segment of DNA that codes for a Covid-2 Spike protein which is
genetically inserted into the adenovirus delivery system.
The mRNA vaccines use nanolipids to stabilize the mRNA segments and similarly code for
Covid-2 spike protein.
The adenovirus DNA vaccines enter the cell nucleus where they begin the process
transcribing DNA code to mRNA, the desired antigen trigger of the immune process. The mRNA to
protein production factories are the ribosomes, housed in the (non nuclear) cytoplasm.
These DNA and mRNA vaccines all differ from traditional first-order vaccines which culture
the virus being targeted, kill it so it can not reproduce, and injected it into the patient,
a process called innoculation (dead virus jab which stimulates wide variety of anitbodies),
vs vaccination (nucleic acid code traveling on a vector or in nano lipid packet which
stimulates production of a specific antigen "spike" protein in this instance.
One problem I haven't heard any assessment about is what happens in the cell when degraded
forms of genetic code, either mRNA or DNA, resulting from perhaps shoddy manufacture or
sloppy handling? Would there still be biological activity? Producing what proteins?
Quality control across the process and delivery system is probably of extreme importance
in ensuring vaccine safety.
oldhippie , Mar 15 2021 21:53 utc |
73
Suzan @ 69
That is an excellent question. Also there is no certainty what is happening when all
apparently goes to plan. Extensive tissue sampling and analysis needs doing. Best way to do
all of that is on autopsy. Autopsies are not being done. It is as if no one wants to
know.
oldhippie , Mar 15 2021 20:56 utc |
63
Tannenhouser @ 57
Main difference is mRNA is absolutely new. There has never before been an mRNA product
turned loose on the general population. Moderna had a rabies investigational product that did
get as far as human testing, it was shut down early. Moderna we know is funded by DARPA,
In-Q-Tel, Bill Gates, Jeffrey Epstein. In existence for thirty or forty years, depending
which story you desire to believe. Never had a saleable product until now. Trust us.
The Pfizer mRNA product is entirely acquired from BioNTech. Try to find out anything about
them. Next try to find out anything about them that passes the laugh test.
If you want to know something about how mRNA gene therapy is alleged to work would suggest
reading or watching what Geert van den Bossche has been saying since he started to talk. He
is a vaccine developer. A man who has spent his career in the lab creating vaccines. He
believes in vaccines. Formerly worked with GAVI and Gates Foundation. Not an anti-Vaxxer.
karlof1
35
It's Profit over People yet again, and such shouldn't be any surprise. The
geopolitical aspects show an extremely desperate Outlaw US Empire that has lost all its soft
power through its inhumane behavior. That it thinks it can recoup some of what it lost by
continuing to act inhumanely proves the absolute sordid quality of the minds at work. And
then there's the lies and deceit, and to think that the people managing this campaign are
allowed to raise children!
Having discovered that Mexico has Sputnik V, I'll be going South as soon as I get my
renewed passport.
Erelis , Mar 15 2021 19:42 utc |
53
So the end result is a world with uneven levels of vaccination. Seems like this will
simply keep covid around for a very long time for the sake of anti-Russia geopolitics and big
Western pharma profits. The world will end up becoming a medical dystopia for years to
come.
vetinLA , Mar 15 2021 19:47 utc |
54
Erelis @ 53; "So the end result is a world with uneven levels of vaccination. Seems like
this will simply keep covid around for a very long time for the sake of anti-Russia
geopolitics and big Western pharma profits. The world will end up becoming a medical dystopia
for years to come."
Yep, afraid you're right.....But then hey, profits uber alles....
james , Mar 15 2021 19:53 utc |
55
@ 29 jackrabbit... thanks... i see this much the same way as you....
@ 37 b... thanks for this additional article.. i quote from it below..
"There are lots of players in the vaccine version of the great game. Both China and Russia
are aggressively practicing vaccine diplomacy. As is the EU. The primary goal of U.S. vaccine
diplomacy seems to be to ensure the profits of Big Pharma, rather than on maximizing the
number of people vaccinated, in the shortest possible time. Could these priorities shift?
Perhaps. Time will tell. India has stepped forward to represent the perspective of developing
countries, drawing on its role as a major vaccine manufacturer – and perhaps sometime
soon – developer."
b
37
Indian Vaccine Manufacturers: U.S. Use of Wartime Export Controls Threatens World Vaccine
Production
Peter Williams , Mar 15 2021 18:31 utc |
38
The NY Times has a surprisingly nearly unbiased article on all available vaccines and
their testing stages etc. https://www.nytimes.com/interactive/2020/science/coronavirus-vaccine-tracker.html?
Sputnik V is being distributed in Russia. My daughter and her boyfriend, as nursing
students were required to be vaccinated, or show antibodies from a recovered case of
COVID-19. My daughter has had COVID-19 and fully recovered, and her boyfriend had his first
vaccination. Unlike most western countries, there is no panic, and lockdowns are on an as
needed basis.
Russia reacted very quickly to the virus and closed its borders early.
karlof1
41
Blue Dotterel @40--
As S commented here several weeks ago, Russian travel agencies and Aeroflot were arranging
special vaccine charters I might also take advantage of, and Mexico has a long history of
welcoming medical patients from El Norte seeking treatments unavailable here.
K , Mar 15 2021 23:14 utc |
84
If you go to the US CDC website you will see that all current vaccines for Covid are only
under "emergency" approval.
I don't want a jab that is messing with my DNA in the first palce but I absoliutely don't
want one that is not yet fully tested.
In addition what does "fully tested" even mean in a corrupt system where you can hardly
find a single truth on any topic in 24 hours of news broadcasting?
How is it that people are ultra critical of political corruption yet as happy as lambs to
trust BIg Pharma in spite of endless lies, corruption and human damage in the last 100 years.
Why isn't it obvious that Big Pharma is part of the problem. You can't be part of the problem
and the solution at the same time.
There is a place for vaccines but for vaccines to fit into the category of preventative
medicine, like good food, exercise, vitamins etc or modalities like acupuncture or herbalism
etc , they also need to prove they are as harmless as good food, intelligent exercise or
vitamins. In my opinion they should be part of any national health system, subject to the
most rigorous and independent testing, and they should be free.
Preventative medicine should have an almost zero chance of killing or maiming anyone.
Otherwise it's just the product of the same philosophy of "collateral damage" than Empires
use to control the human world.
I question vaccine logic when it denies the human capacity to evolve to protect itself and
I especially question Vaccines for profit. I'm not an anti vaxxer, but I am also not going to
happily inject a cocktail of chemicals and animal/human DNA proteins directly into my
bloodstream. I am well aware that vaccines have used dead or active animal proteins for a
very long time, part of the reason why i try to avoid them at all costs.
Where is the research that proves that injecting foreign DNA into our blood is safe long
term for the overall health of human beings , not just for immunity to one disease? Obviously
the current vaccines are not killing people in great numbers, but they
Saying that we just don't know is naive. Obviously bio tech labs have been experimenting
for decades on the effect of genetic mutation on animals and humans. Just as they knew the
long terms outcomes of GMO crops but kept is secret, they will also be well aware of the long
terms effects of GMO vaccines and also keeping it very secret.
There doesn't need to be a micro chip in a vaccine to make it a bio weapon.
Will the gene activating vaccines become a biological weapon just as GMO seeds have?
I've watched presentations explaining the science of the current vaccines, and I do not
feel at all re-assured that the genetic response will behave as predicted in every case, or
even in any case. Gaining immunity from Covid is pointless if it renders people more
succeptable to potentially worse health conditions down the track.
I have no expertise in this field, I'm just a concerned human being trying to make sense
of very complicated science that also happens to have no legal liability. What could possibly
go wrong? Einstein would be sympathetic given what happened with his science.
We should be questioning the argument for vaccines over antibody testing and preventative
medicine at the very least. But that is not even a mainstream conversation at this point.
Somebody mentioned in the comments that in Russia you can get antibody testing and not
need the vaccine. This sounds more like a balanced approach to me. That isn't an option in
most places that I am aware of.
Manufacturing of consent for genetic intervention in humans is now happening very
successfully all over the world due to covid. The created hysteria that vaccines are the only
way to save the planet is so reminiscent of WMD's in Iraq and GMO seeds in the developing
countries . Anyone notice that millions of Indian farmers are now rejecting the Bio-Tech
because GMO seeds and their accompanying poisons are destroying lives and the planet?
These are not separate issues.
Suddenly there is a $100 Billion covid Vaccine market. And strangely Pharma seems to be
the only class that is a-political and borderless. Even making profits in our favourite anti
western countries. What a coup! And how is this possible?
I never really understood the intense media campaign against anti-vaxxers until now. I
mean why would a relatively few traumatised parents really be a bother to Big Pharma? The
answer is that they aren't.
Creating a public enemy and gaining consent was the goal and boy has it worked a
treat!
Just in time for the biggest Vaccine $$$$ jackpot of all time.
ted01 , Mar 15 2021 23:28 utc |
85
john | Mar 15 2021 21:31 utc | 68
Thanks for that link to the Geert Vanden Bossche interview.
It is worth repeating - Mass Vaccination in a Pandemic - Benefits
versus Risks
I would hope that every MOA reader would take the time to watch it.
A.L. , Mar 15 2021 20:43 utc |
60
A long one, sorry about this...
I'm not an epidemiologist nor medically trained on trial procedures and norms but i have
the following questions:
1. Efficacy figures:
2. Viral exposure post inoculation:
e.g. A cohort that are made up of front line workers in a hotpot/basket case like Brazil
will necessarily be more prone to be exposed to the virus than say a cohort that fairly
represents the population. Conversely a vaccine tested on a less exposed cohort will also
more likely to get a better efficacy figure.
So is this why we're seeing lower and sometimes inconsistent figures on particular
vaccines. The sinovac coronavac comes to mind. Figures in Brazil was wildly different to
others in turkey and Indonesia.
... Actually i smell political meddling with the Brazil trial, similar to what b pointed
out in his piece, but i digress.
3. Endpoint
What I'm saying is there's a lot of cherry picking, manipulations, stacked decks and
absolute bullshit because of vaccine politics. Sadly the sheeple are buying it all.
For me, because of my need to travel to both the 'free world' and the totalitarian regime
that is China, i will probably need to get jabbed by 2 vaccines due to the vaccine politics
that is taking shape right in front of your eyes. It pains me to think that in doing so I'll
make another 2 doses unavailable to someone else.
What can you do: i do believe all the vaccines are effective and if you're otherwise
healthy you should go and take the jab, whichever one (may be pass on the AZ for now). Your
govt have already blown your money on it, and they don't have a long use-by date.
The world is acutely supply-limited and your support to vaccinate will ironically slow
down the empire in trying to corner the vaccine market politically. Why? Because they will
not be able to spin up production as quickly as RUS+CHN+other countries who are working with
RUS+CHN to spin up their own production.
At the end MRNA is a mil tech and i can't see the 'free world' giving that up to anyone
else until its common knowledge. So the longer it is supplied-limited, the better for the
uptake of the other vaccines to put a nip on the brewing vaccine-racism where you can only
travel to certain places depending on which jab you took.
Thanks for reading.
Kapusta , Mar 15 2021 22:07 utc |
76
I am absolutely appalled by the blinkered focus on vaccines to the detriment of
therapeutic treatment. Of course, no one should be surprised by this, considering, as Putin
puts it, there is now a sudden and lucrative $100 billion c19 vaccine market (what
incentive!). So the entire medical world (minus a few) discovered that c19 was amenable to
vaccine production and completely buried efforts to discover/develop successful
treatments.
Ask anybody (in the global north) that has had c19 what they were told to do. Just about
all of them will probably say that they were told to go home and self-care/quarantine until
they have symptoms that are bad enough for them to be hospitalized. Doctors don't want to
treat c19 because they've been told by government guidance that there is no treatment
(a complete lie!). Meanwhile, those few brave doctors have actually tried to treat patients
before they get worse and there have been a few discoveries (IVM is the best example) of
various treatments that are highly effective.
So now we find even the least vulnerable, such as 20/30 year olds, all clamoring to
get a vaccine, any supposed vaccine, when all they really need is some vit D and to take
varied prophylaxis proven to work and they'd be perfectly fine. A responsible gov response
would be to vaccinate the most vulnerable and treat the least vulnerable. Instead, we have
mass hysteria to vaccine all human beings alive and still force 3 year olds to mask and take
two tests a week, all for the sake of protecting pharma profits. Absurd.
john , Mar 15 2021 21:31 utc |
68
Gosh, there's so much enthusiasm for inoculation around here one almost forgets that there
are many of us, even
inside the industry, who don't want ANY of these injections.
And as a kind of aside, the extreme harvesting of their blue blood is apparently wreaking
havoc on the horseshoe crab
community , an extremely important link in the old ecological chain.
suzan , Mar 15 2021 21:33 utc |
69
@ Jackrabbit
The Adenovirus vector vaccines are DNA vaccines. The primary difference between them
(Sputnik V, Astrozenica, J & J and some more) is the type of Adenovirus vector used, for
example human or chimp, how they are cultured, and the specifics of production and
processing.
All of them use a segment of DNA that codes for a Covid-2 Spike protein which is
genetically inserted into the adenovirus delivery system.
The mRNA vaccines use nanolipids to stabilize the mRNA segments and similarly code for
Covid-2 spike protein.
The adenovirus DNA vaccines enter the cell nucleus where they begin the process
transcribing DNA code to mRNA, the desired antigen trigger of the immune process. The mRNA to
protein production factories are the ribosomes, housed in the (non nuclear) cytoplasm.
These DNA and mRNA vaccines all differ from traditional first-order vaccines which culture
the virus being targeted, kill it so it can not reproduce, and injected it into the patient,
a process called innoculation (dead virus jab which stimulates wide variety of anitbodies),
vs vaccination (nucleic acid code traveling on a vector or in nano lipid packet which
stimulates production of a specific antigen "spike" protein in this instance.
One problem I haven't heard any assessment about is what happens in the cell when degraded
forms of genetic code, either mRNA or DNA, resulting from perhaps shoddy manufacture or
sloppy handling? Would there still be biological activity? Producing what proteins?
Quality control across the process and delivery system is probably of extreme importance
in ensuring vaccine safety.
juliania , Mar 15 2021 21:44 utc |
71
I would hope others will look at the video @ 12 - lots of meat in that for a discussion
and very important information from the Israeli vaccinations for the covid virus! I look
forward to further consideration of the thesis. The important part is that the findings don't
disagree with the efficacy of the vaccine, they simply point to a change in the virus itself
being somehow linked to the vaccinations. I would like to know if this is also the case when
vaccinations of the more traditional type are being used, or whether this is only true of
certain ones.
And again, if this is a false correlation, I would like to know that as well. I've sent
the video to my daughter who is a hospital worker.
juliania , Mar 15 2021 22:36 utc |
81
mina @ 52, thanks for your link. The headline to the article reads: "SARS-CoV-2 evolution
during treatment of chronic infection." I was only able to read a line at a time, due to the
set up on my computer, but it looks as though it is a more clinical study of patients being
treated with remisidivir (sp? sorry) on the virus as they were being treated, and that those
mutations were occurring rapidly during course of treatment. One wonders, then, is that a
corroboration of the study linked @ 12 but not specifically related to any vaccine per se,
and does it mean that the mutations are occurring within the hospitalization process in
general (and possibly also out in the environment) as well as in conjunction with vaccine
jabs, so that while some get treated, others are more likely to suffer from those mutations?
Or as seems to be the claim at the video, are the virulent mutations occurring in conjunction
with the vaccinations only?
The video supposes that more vaccinations may be necessary as the virus mutates and other
dangerous ones come on scene. The question being can the human body suffer these annually or
more often as well as, say,they have had less potent 'flu vaccinations every year? (That's
assuming the 'flu jabs are harmless, but I won't go there.)
I'm not a clinical expert, but it seemed the mutations were occurring in Mina's link in a
petri dish, not just out in the general atmosphere, and that those mutations seem to be less
virulent, not more. Whereas in the video @ 12, the deaths had doubled in conjunction with the
vaccinations.
I'm not anti vax per se. But this is a different situation from other cases. It really
does need to be studied without the economic factor entering in, so that the best solution
can be taken, or the world is going to be very badly off just following what powerful nations
tell them to do.
LA_Goldbug 5 hours ago
Study carefully the graphs of deaths in retirement homes in Ireland !!!
https://twitter.com/Thorgwen/status/1370662165800230913
plus this
PHE found a 48% increase in infection risk among over 80s in the week after the first
jab. The FDA found 40%. Now a study from Denmark finds 40%. Will the Government publish the
data to set our minds at ease?
https://twitter.com/toadmeister/status/1370763011426770946
Vinividivinci 12 hours ago
Must watch...real science.
https://www.brighteon.com/257797f0-06fa-4596-be69-af71bb3adc21
-- [NOTE: interesting video; not junk]
In the last 24 hours, a number of national governments including Denmark, Norway, Thailand,
and Iceland, announced that they will temporarily halt the use of the COVID-19 vaccine that was
developed by AstraZeneca and Oxford University.
The Danish Health Ministry stated that the suspension was a precautionary measure following
dozens of reports of blood-clotting by patients who had been vaccinated. There has been at
least one fatality.
As I've written many times before, I'm not anti-vaccine. But I am pro-data and
pro-reason.
And it seems sensible to pause and assess the data when a brand new and comparatively
untested vaccine may be linked to serious side effects.
The problem, of course, is that this story doesn't conform to the narrative that the media
wants you to believe. So they're either NOT reporting on it, or they're running counter-stories
to reinforce their agenda.
Newsweek already came to the rescue with an article stating unequivocally that there is "no
evidence to show COVID vaccines have caused deaths or serious illnesses. . ." including blood
clots.
Another article entitled "What to Know About Serious Covid Vaccine Reactions" dismissed any
potential reaction, including death, by declaring "no connection to vaccines has been
established."
The Associated Press wrote, "The vast majority of people being vaccinated at the moment are
elderly or have got underlying diseases", and that "it would be difficult to determine whether
a vaccine shot is responsible" for blood clots.
(Nevermind that you could apply that same argument to COVID deaths, i.e. the vast majority
of COVID deaths are elderly or people with underlying diseases, so we should simply ignore that
data when making policy decisions )
Certainly most vaccinations worldwide have shown, at least in the short term, few side
effects. And it's obviously possible that the blood clot issues may not be related to the
vaccine.
But it's extraordinary that the media is willing to deliberately ignore any signs or data
that might undermine what they want you to believe.
Greed is King 14 hours ago
First, a couple of quotes from this article, with my comments following each. And then an
article that ties the two together, and MUST BE READ.
"Professor of Government Ethics Played Key Role in Nursing Home Death Coverup
Last spring, the New York Governor Andrew Cuomo ordered nursing homes to admit patients
who had recently been treated for Covid-19. This led to a spike in Covid deaths inside
nursing homes, which are filled with elderly people in the highest risk category for serious
Covid-19 cases."
The exact same thing happened in the UK, elderly and in some cases DYING elderly patients
were sent back to their care home from the hospitals they were being treated in, AGAINST the
wishes of the care homes and medical ethics, even though it was known they were infected with
the virus, the care homes were ORDERED to take them back. So, guesss what happened ?, that`s
right, THOUSANDS OF DEATHS , of both the sent back and those in the care home that then
became infected. THAT WAS ALL OFFICIALLY SANCTIONED.
Several nations halt distribution of AstraZeneca Covid vaccine
"The problem, of course, is that this story doesn't conform to the narrative that the
media wants you to believe. So they're either NOT reporting on it, or they're running
counter-stories to reinforce their agenda. Newsweek already came to the rescue with an
article stating unequivocally that there is "no evidence to show COVID vaccines have caused
deaths or serious illnesses. . ." including blood clots. Another article entitled "What to
Know About Serious Covid Vaccine Reactions" dismissed any potential reaction, including
death, by declaring "no connection to vaccines has been established."
When investigating a series of crimes, the police look for any possible connections, the
common denominator that ties the crimes together and thereby highlights possible
suspects.
So what`s the common denominator in ALL of these blood clot deaths ?, they ALL HAD HAD THE
VACCINE !!!!. Now if that`s not a smoking gun, a starting point of investigation, WTF IS
????.
The articles bullet points.
The AstraZeneca vaccine is being promoted for developing countries, in part because it
doesn't require the deep-freeze cold storage that mRNA vaccines do, so the logistics
surrounding distribution are less complex
Patents and royalties for the AstraZeneca vaccine are held by a private company called
Vaccitech, investors of which include Google Ventures, the Wellcome Trust, the Chinese
branch of Sequoia Capital, the Chinese drug company Fosun Pharma and the British
government
While AstraZeneca has promised it will not make any profit from its vaccine, there's a
time limit on this pledge. The not-for-profit vow expires once the pandemic is over, and
AstraZeneca itself appears to have a say when it comes to declaring the end date
The AstraZeneca COVID-19 vaccine was co-developed by Adrian Hill, who has long-term
ties to the British eugenics movement through his work with the Wellcome Trust's Centre for
Human Genetics and affiliation with the Galton Institute, formerly the U.K. Eugenics
Society
Members of the Galton Institute have called for population reduction in Latin America,
South and Southeast Asia and Africa, the very areas where the AstraZeneca vaccine is being
promoted
Amazing isn`t it that Gates and his Welcome Trust keep on coming up in connection with the
virus, coincidence ?. Probably not. It`s also very deeply concerning and ALARMING to find the
BRITISH GOVERNMENT itself implicated !!!, VERY CONCERNING AND ALARMIN INDEED !!!.
Link to article.
https://articles.mercola.com/sites/articles/archive/2021/03/13/oxford-astrazeneca-eugenics-links.aspx
?
Steven Keith
• a day
ago
As reported by FDA/CDC:
https://www.fda.gov/media/1...
Kary Mullis: PCR Test Inventor Calls Dr Fauci a Fraud (polymerase chain reaction, or
reverse transcription polymerase chain reaction)
https://odysee.com/@Quantum...
CDC "Gold Standard" (PCR) Polymerase Chain Reaction test. False Positive Problem:
https://www.nejm.org/doi/fu...
Disturbing Vaccine Facts - (The WHO etc. "Experts & Leaders" of infectious disease
proving from their own mouths Vaccines are not safe)
https://www.bitchute.com/vi...
Norway Investigates Whether AstraZeneca Vaccine Caused Deadly Blood Clots
BY TYLER DURDEN
FRIDAY, MAR 12, 2021 - 10:34
Update (1124ET):
As the first AstraZeneca shots arrive in South America via
the WHO's Covax program, the international public-health agency has promised to investigate reports that the vaccine may be
linked to dangerous blood clots.
https://platform.twitter.com/embed/Tweet.html?dnt=false&embedId=twitter-widget-0&frame=false&hideCard=false&hideThread=false&id=1370409477749551104&lang=en&origin=https%3A%2F%2Fwww.zerohedge.com%2Fcovid-19%2Fnorway-investigates-whether-astrazeneca-vaccine-caused-deadly-blood-clots&siteScreenName=zerohedge&theme=light&widgetsVersion=e1ffbdb%3A1614796141937&width=550px
* * *
Yesterday, Europe's
already
struggling
COVID vaccine rollout took another hit when
more
than half a dozen nations
stopped doling out COVID vaccines created by AstraZeneca following reports that some patients
who received the vaccine developed life-threatening lung clots, with at least one person having subsequently died as a
result.
While health authorities in Denmark, one of the first countries to halt the AstraZeneca-Oxford jab, said it was impossible
to tell if there was any connection, the spate of suspicious cases is apparently enough to prompt health authorities to
take a closer look. On Friday morning, Thailand became the first non-European country to halt the AstraZeneca vaccine,
while several other nations, including Canada, Australia, the Philippines and South Korea, have all said they would move
forward.
Bulgaria became the latest European nation to suspend the vaccine on Friday. According to
Reuters
,
the Bulgarian government wants the EMA to send over a written statement outlining its argument about why it should allow
vaccinations to go forward.
The World Health Organization on Friday said there is no reason to stop using the
Oxford-AstraZeneca coronavirus vaccine, as a growing number of countries in Europe and
elsewhere have moved to halt its use over blood clot concerns.
Italy, Romania and Thailand joined at least eight
European nations this week in suspending the injections either from specific batches or as
part of a total freeze, citing the potential adverse events despite a
lack of formal evidence that the shot is unsafe.
A WHO spokeswoman, Margaret Harris,
said at a briefing that an advisory committee was investigating reports of individuals
falling ill or dying after developing blood clots in the post-vaccination period, but that no
causal link had been established.
vk
8
Western
media should investigate deaths and serious injuries related to Pfizer vaccine
Christian Daily, a Los Angeles-based media outlet, reported on Friday that according to a
whistleblower, COVID-19 vaccinations from the Pfizer shots have resulted in a significant
number of deaths and serious injuries in a German nursing home. The report said, "A
conscientious whistleblower, who is also a caregiver at the nursing facility where the
incident happened, stepped forward to expose what transpired behind the scenes of the
COVID-19 vaccine rollout, a report says."
[...]
The coverage reported, "Seven out of 31 people living in the nursing home died after
getting injected with their first dose of Pfizer's COVID-19 vaccine. The whistleblower
added that after the second dose was administered, one died and eleven more got seriously
sick." Christian Daily analyzed that, "This means that out of the 31 elderly people that
got vaccinated in that nursing home, 25 percent of them died shortly after while the lives
of 36 percent were jeopardized."
[...]
The article also looked back to prior deaths from other European countries of elderly
people after receiving the COVID-19 vaccines produced by Western companies including
Pfizer. For example, 46 elderly people in a Spanish nursing home died following their
vaccinations, and 16 senior citizens died after getting vaccine shots in Switzerland.
Our problem is not so much bad will (and here I disagree with my esteemed colleague
Mike
Whitney ) but the noble and quixotic desire to save mankind from some perceived peril. P.G.
Wodehouse tells us of four scouts who, in their quest for a good deed, helped an old lady to
cross the street, and reported to their guide. All four of you were needed for that, asked an
amazed guide. Well, she put up quite a strong resistance, they replied. Until recently, only
governments played God and that was bad enough. But now every Tom, Dick and Harry with an extra
billion dollars in his pocket wants to save mankind.
snake , Oct 4 2020 14:41 utc |
7
Very interesting week.. what I saw was a lot of people are beginning to understand how
dysfunctional the USA government has become.. The oligarchs who own the International Nation
State Franchising operation. .you know, the franchises that govern the local nation states
are being discovered one by one, as part of the dysfunction that has been used to manipulate
all of hamanity . .
Most people have begun to under the meaning of having a President that is not elected by
the people and that it does not matter if the people go to the poles and vote, because their
vote does not count, the electoral college appoints both President and VP.
Most people are beginning to understand their concerns are not explainable because the
government is conducted in secret and the media, 92% owned by just 6 people world wide. has
complete control over the information environments <=in each separate nation state. The
MSM is where, until recently, most people got their information from <= so most people's
information until recently has been completely shaped by the private owners of the media that
controls each franchised nation state separately.
The meaning to democracy <=actually to lack of it, of a six person owned, private
monopoly in media is starting to become understood by everyone, even the guy that cleans the
commodes: those who must cover up their sins and those seeking to discover the sins of those
seeking to hide their sins <=everyone is beginning to understand. Private control, by
monopoly ownership of media, has protected the nation state franchisees from being discovered
for too long. The nation state system has not only allowed, but fostered and promoted global
unrest. Media is independent of top down nation state control, its an alternative way that
the owners of the Franchise system enforce their intentions and control the narrative.. The
USA has not been shy about acting on behalf of desperate private media to prevent out of the
box disclosures about global corruption < intent clearly shown in the trial going on in
Britain designed to bring Julian Assange into prosecution range. Documents Mr. Assange
disclosured revealed how those who govern and those who benefit by Useing government
accomplish their corruptions. Devil forbid! The Assange extradition trial reports that
disclosing crimes of those in government is light years more terrible than holding up a
corner grocery store.
Government
power depends on citizen dependence.
So much freedom from those who govern <=its difficult to move about.
lulu , Nov 27 2020 18:04 utc |
121
A European court declares the RT-PCR test worthless.https://www.rt.com/op-ed/507937-covid-pcr-test-fail/
Posted by: Palinurus | Nov 27 2020 10:21 utc | 102
The judges in Portugal drew their conclusion basing on the following technicalities:
1.
The judges also said that only a doctor can "diagnose" someone with a disease, and were
critical of the fact that they were apparently never assessed by one .
nothing about PCR test "worthless".
In the eyes of this court, then, a positive test does not correspond to a Covid case. The
two most important reasons for this, said the judges, are that, "the test's reliability
depends on the number of cycles used '' and that "the test's reliability depends on
the viral load present .'
higher the cycle threshold
(Ct) of a PCR test is, the higher the chance of the test turning out
positively.
According to the research paper linked in your RT article Correlation
Between 3790 Quantitative Polymerase Chain Reaction–Positives Samples and Positive Cell
Cultures, Including 1941 Severe Acute Respiratory Syndrome Coronavirus 2 Isolates ,
Several recent publications, based on more than 100 studies, have attempted to propose a
cutoff Ct value and duration of eviction , with a consensus at approximately
Ct >30 and at least 10 days, respectively. However, in an article published in
Clinical Infectious Diseases, Bullard et al reported that patients could not be contagious
with Ct >25 as the virus is not detected in culture above this value.
The real argument is probably whether decision-makers (doctors, public health
authority) should take the lower Ct for PCR tests or not, which affects their consequential
decisions, for example, quarantine time of 10-day vs 14-day, the effectiveness control of
Covid 19 contagion.
vk
123
@ Posted by: Palinurus | Nov 27 2020 10:21 utc | 102
lulu @ 121 is correct: diagnosis ≠ track and tracing.
PCR is just for track and tracing, not for diagnosis. The diagnosis protocol is much
longer and burdensome, and includes an MRI of the lungs if I'm not mistaken (and can only be
made by a doctor). The Portuguese judges are, therefore, also correct.
vk
129
@ Posted by: oldhippie | Nov 27 2020 19:23 utc | 127
There are two problems with your theory:
1) Fauci is not a reliable source;
2) China uses a 40-cycle PCR test, used it on Wuhan's entire population (almost 10
million) after a scare and found no positive results.
We already talked about the Portuguese case. The judges were probably amid a labor dispute
and, in a pro-business decision, reiterated that PCR is not diagnosis.
oldhippie , Nov 27 2020 19:46 utc |
130
vk @ 129
Administer a test 10 million times and every result the same? And you believe this?
Amplify a signal by a trillion and there is never a problem with noise? Oh, it is in Chinese
wonderland, makes perfect sense.
Always apples and oranges with you. Same as it it would be talking to an illiterate. Or a
wall.
uncle tungsten , Mar 1 2021 3:07 utc |
55
Gilad Atzmon reports:
The global Pfizer jab is deadly effective.
... no one can deny the astonishing fact that in just 8 weeks of mass vaccination
the total number of Covid-19 deaths in the Jewish State almost doubled from the number
accumulated in the prior ten months...
At the time Israel vaccinated itself, it was witnessing a sharp exponential rise in
morbidity and death. Palestine, literally the same land, saw its number of cases and deaths
plummeting.
Bourla [Pfizer CEO] and PM Netanyahu should make an intellectual effort and explain to
us how it's possible that in Gaza, an open-air prison and one of the most densely populated
pieces of land on this planet, the numbers of Covid-19 cases are minimal and without a
'vaccine.'
But Palestine is not alone, as the situation in Jordan is similar. While Israel saw its
Covid-19 death figures breaking through the roof, Jordan's Covid-19 deaths from
mid-November onwards look like a slippery slope. [down that is]
And then there is another ghastly issue revealed in this closed experiment:
Since Israel morphed into a nation of Guinea pigs, a virus that used to prey on the elderly
and those with severe health issues has now changed its nature completely. After just 2
months of a 'successful' mass vaccination campaign, 76% of new Covid-19 cases are under 39.
Only 5.5% are over 60. 40% of critical patients are under 60. The country has also detected
a sharp rise in Covid-19 cases amongst pregnant women, with m ore than a few in critical
condition. In the last few weeks, new-born Covid-19 cases saw a large 1300% spike (from 400
cases in under two-year-olds on November 20 to 5,800 in February 2021).
The evidence collected in Israel points at a close correlation between mass vaccination,
cases and deaths. This correlation points at the possibility that it is the vaccinated who
actually spread the virus or even a range of mutants that are responsible for the radical
shift in symptoms above.
Atzmon closes with black humor:
I am obviously not the only one who sees that something went dramatically wrong in Israel.
A group of dissenting researchers who looked into the numbers involved with the current
Pfizer Israeli experiment
published a detailed study two week ago. "We conclude" they wrote, "that the Pfizer
vaccines, for the elderly, killed during the 5-week vaccination period about 40 times more
people than the disease itself would have killed, and about 260 times more people than the
disease among the younger age class."
Based on the Pfizer/Israeli 'laboratory' experiment, I drew the following sarcastic
conclusion: If you catch coronavirus you may die, but if you follow the Pfizer path, not
only do you have a 95% chance to survive on top of the 99.98% provided by Covid-19, you may
also kill some other people on the way.
vk
18
Danger of
mRNA vaccines to elderly under spotlight after 16 deaths in Switzerland
Swissmedic said the average age of the deaths was 86 and most of them had pre-existing
diseases, adding there was no evidence to suggest that the vaccines were the cause of
death.
However:
A Chinese immunologist who requested anonymity told the Global Times that the large-scale
use of mRNA vaccines carries the risk of causing abnormal immune dysfunction, allergy or
even death, especially among the elderly and people with underlying diseases.
So we have a situation where a vaccine against a disease that mainly kills the elderly
can't be used on the elderly. Awesome design.
Sometimes I'm in awe with grandiosity of the Western intellect.
Bluedotterel , Feb 27 2021 9:23 utc |
39
So, why not take a Big Pharma vaccine?
https://www.rt.com/op-ed/516525-racist-big-pharma-state-experiments/
"Then you have the testing of the antibiotic Trovan in Kano, Nigeria, to assess its
effectiveness against meningitis. Eleven children died in the trial – five after taking
Trovan, six after taking an older antibiotic used as a comparison drug.
Others suffered blindness, deafness, and brain damage, which may or may not have been due
to the trials. We'll never know, because the Big Pharma company responsible settled out of
court when sued by the Nigerian government (denying us the whole truth but giving off very
guilty vibes), having been accused of conducting an illegal study with no permission from the
children or their parents.
The name of the company? Pfizer. And you wonder why black Africans (or any other sane
person) might be wary of a vaccine with that name on it. "
Jen , Feb 27 2021 11:06 utc |
40
Bluedotterel @ 39:
There was also a tetanus shot drive in Kenya many years ago that targeted women and girls
in the main: odd when you think that men and boys tend to spend more time outdoors doing
things that put them at higher risk of getting puncture wounds or wounds infected with
tetanus bacteria. Some people associated with the Roman Catholic Church in Kenya decided to
do some investigation and discovered that the tetanus shots contained sterility agents.
steven t johnson , Feb 27 2021 15:19 utc |
45
jen@40 speaks of a "sterilizing agent" in anti-tetanus vaccines in Kenya. I did not know
there was any chemical agent capable of sterilizing women with a single shot. What was this
stuff?
blue dotterel@39 tells a fairly plausible horror story about Pfizer and Trovan, except for
the part about how more children dead *from another antibiotic* is somehow evidence against
Pfizer and Trovan.
gm , Feb 27 2021 15:53 utc |
47
@ m | Feb 27 2021 15:24 utc | 46
For starters:
HCG [Human chorionic gonadotropin] Found in WHO Tetanus Vaccine in Kenya Raises Concern in
the Developing World
October 17, 2017 Researchgate pdf
Lots of stuff pops up when you run the search: "kenya tentanus sterilisation".
james , Feb 27 2021 17:09 utc |
54
@ jen and others - tetanus shots... aside from agreeing with @ Piotr Berman | Feb 27 2021
16:18 utc | 48, i would just like to point out it is typically the women who are planting and
gardening... working with the soil increases the risk posed which the tetanus shot is
supposed to lessen... i wonder if this ought to be factored into all this??
Jen , Feb 27 2021 20:25 utc |
61
Steven Johnson @ 45, M @ 46, Piotr Berman @ 48 and others:
As GM @ 47 has referenced, the agent found in the tetanus vaccines is HCG which is
produced naturally by a woman's body during pregnancy. When combined with a weakened tetanus
toxin and introduced into the human body, the combination induces the immunity system to
react against both tetanus and HCG. The Kenyan Catholic bishops' group had the vaccines
tested in 4 laboratories in Kenya and the labs found HCG in the shots.
The WHO tetanus vaccination program, begun in the 1990s, targeted women and teenage girls
in Kenya as a high proportion of newborn babies die from tetanus as a result of the umbilical
cord being cut with unsanitised instruments. I must admit I was not aware of this when I
posted my earlier comment and did some more reading after posting. The mothers themselves are
also often at the risk of contracting tetanus from giving birth, often through tears that
occur naturally in the vaginal region. The custom of female genital mutilation that may still
occur in parts of Africa despite govt bans in many countries adds to the tetanus risk. In
addition many girls are married off at a young age.
Abby Ohlheiser wrote a November 2014 article for The Washington Post on the tetanus
vaccination program in Kenya. Barflies should be able to find it on Google or other search
engines.
What is the relevance of this discussion besides being an addition to Bluedotterel's
mention of the RT.com article stating that people of colour were wary of COVID-19 vaccines
because of past history in which they were guinea pigs for medical experiments? The relevance
is that there are fears and rumours that the Pfizer/Biontech mRNA treatment for the COVID-19
virus contains instructions for cells to replicate a spike protein on the coronavirus's coat
that is the same as or similar to a protein that helps the placenta attach to the uterine
wall. There is concern that the treatment will induce the immunity system to react against
the protein in a pregnant woman's body leading to miscarriage. Whether the effects of the
treatment might be long-term or not, long after the initial inoculation, is another
issue.
Piotr Berman , Feb 27 2021 21:15 utc |
63
https://pubmed.ncbi.nlm.nih.gov/1618603/
The linked article seems to be about the vaccine developed in India that matches what Jen
described as used in Kenya.
30-40 years ago, Indian government was interested in improved methods of birth control,
and Indian labs developed and tested such vaccine. It seems like a legitimate birth control
method, the described tests were on women with at least two children, presumably with proper
consent, although later the issues of consent etc. were a hot political subject in India.
BTW, hGC is present in men too, and in animals, anti-hGC antibodies were affecting
(eliminating) male fertility as well.
On one hand, the anti-fertility vaccination described there requires three shots, and
perhaps the fourth one if the achieved level of anti-hGC antibodies is too low, so if used as
one-shot tetanus vaccine, it may be ineffective. On the other hand, surreptitious use of such
vaccine, without the consent for their designed effect, is not ethical.
gm , Feb 27 2021 22:15 utc |
64
Speaking of 'under-the-table'/underhanded stealth vaccines...
EXCLUSIVE: Dr. [Ralph (gain of function virus researcher)] Baric Was Reviewing
Moderna's and Dr. Fauci's Nih-NIAD Coronavirus Vaccine in December 2019! What's Going
On?
https://www.thegatewaypundit.com/2021/02/huge-exclusive-dr-baric-reviewing-modernas-dr-faucis-coronavirus-vaccine-december-2019-know/
On DECEMBER 12, 2019 an agreement was signed (pg 105) that Dr. Ralph Baric of the
University of North Carolina would receive "mRNA corona virus vaccine candidates developed
and jointly-owned by NIAID and Moderna"
Dr. Lawrence Sellen Twitter
Feb 26, 2021; 11:26 pm
https://www.documentcloud.org/documents/6935295-NIH-Moderna-Confidential-Agreements.html
Section applying to material transfer of experimental mRNA CV therapy vaccine candidate(s)
to Baric labs/UNC: Pgs 105-107.
Ralph Baric's signature: 12/12/2019; pg 107.
[For those whose memory is fuzzy, 12/12/2019 was ~1.5 months *before* Wuhan Covid
pandemic outbreak was publically acknowledged by US.gov/CDC/NIH/WHO or China !?]
gm , Feb 23 2021 17:30 utc |
230
One-Third of Deaths Reported to CDC After COVID Vaccines Occurred within 48 Hours of
Vaccination
According to new data released today, as of Feb. 12, 15,923 adverse reactions to COVID
vaccines, including 929 deaths, have been reported to the Centers for Disease Control and
Prevention's (CDC) Vaccine Adverse Event Reporting System (VAERS) since Dec. 14, 2020.
VAERS is the primary mechanism in the U.S. for reporting adverse vaccine reactions.
Reports submitted to VAERS require further investigation before a determination can be made
as to whether the reported adverse event was directly or indirectly caused by the
vaccine.
[...]
The latest VAERS data show that 799 of the deaths were reported in the U.S., and that
about one-third of those deaths occurred within 48 hours of the individual receiving the
vaccination.
As is consistent with previous VAERS data reports, 192 of the reported deaths -- or 21%
-- were cardiac-related. As The Defender reported earlier this month, Dr. J. Patrick
Whelan, a pediatric rheumatologist, warned the U.S. Food and Drug Administration in
December that mRNA vaccines like those developed by Pfizer and Moderna could cause heart
attacks and other injuries in ways not assessed in safety trials.
Of the 929 deaths reported since Dec. 14, 2020, the average age of the deceased was
77.8 and the youngest was 23. Fifty-two percent of the reported deaths were among men,
45% were women and 3% are unknown. Fifty-eight percent of the deaths were reported in
people who received the Pfizer vaccine, and 41% were related to the Moderna vaccine.
States with the highest reported number of deaths were: California (71); Florida (50);
Ohio (38); New York (31); Kentucky (41); Michigan (31); and Texas (31).
Full story link
As Chris Martenson (PhD in pathology from Duke University) outlines in the 2020 Year in
Review with Dave Collum (PhD Columbia, Chemistry, teaches at Cornell): a medical "case" is
one in which a patient is presenting symptoms and requires medical attention. That's a case.
PCR tests were never meant to discern whether somebody is an "infected case" or not, and as
Collum elaborated in that same interview, "with a Cycle Threshold over 35, you can get a
positive PCR test out of a dog's ass".
Daily new cases of COVID-21 hospitalizations and COVID-19 and COVID-21 related deaths
will exceed medical care facilities capacity. Expected Q1 – Q2 2021.
According to the media, this is true. According to reality, it isn't. In CNN-style "fact
checking" parlance, it would thus score as "partially true".
"Covid Related Deaths" is a well worn catch-all. What is known to anybody keeping track: the
vast majority of COVID fatalities are with COVID, not from it. We all know this, for some
reason it doesn't seem to matter. The overall survival rate for this thing is somewhere around
97% or higher. Most people don't know anybody in their immediate circle of friends and family
that have actually died from it.
It can be terrible virus to catch and become sick with, and it's tragic to die from. But the
majority of people either exhibit flu like symptoms and shrug it off or remain completely
asymptomatic. Overall it causes fewer fatalities to society than either alcohol (3 million
deaths per year, globally) or driving (1.5 million) or for that matter air pollution at 4.2
million.
Enhanced lock down restrictions (referred to as Third Lock Down) will be implemented.
Full travel restrictions will be imposed (including inter-province and inter-city). Expected
Q2 2021.
A British View of the Imposture NICK KOLLERSTROM JANUARY 25, 2021 3,300
WORDS 222
COMMENTS REPLY Tweet Reddit Share Share Email Print More RSS
2020 saw 14% more deaths than average, last year in England & Wales and that amounted to
seventy-five thousand extra deaths. We here use the
Office of National statistics figures, as it gives total weekly deaths, plus also for
comparison an average value of corresponding weekly deaths over the previous five years.
[1]
That compares with the figure of ninety thousand deaths for the
entire United Kingdom, due allegedly to covid-19.
We here ask and answer the question, what caused that excess of deaths ? The answer
will not be certain, but will be the simplest possible explanation. By Occam's razor we are
obliged to take it.
For the first quarter of last year, deaths in England and Wales were down : for
whatever reason, overall weekly mortality was 3% below the yearly average. Then around
the spring equinox on March 23 rd Lockdown was announced and suddenly, deaths surged
right up so that thousands of extra deaths started happening week after week. That continued
all through April and May and then finally, in the first week of June Britons were allowed out
again: with relief we could walk the streets and parks, cafes and pubs opened up again.
Those months of Lockdown saw fifty-nine thousand excess deaths (see graph). That
comes from counting the eleven weeks ending 27 March to the 5 th June, as being the
lockdown period.
The question arises as to what caused them? Could it have been, for example, the shock? The
month of April averaged ninety percent more deaths than usual! Then May was not quite so
bad, as folk got used to the grim new reality.
In the weeks after the Lockdown i.e. after the first week of June the whole excess of deaths
suddenly vanished. Over the next four months deaths remained exactly average compared to
previous years.
The graph shows this distinct, three-stage process.
OBNS data for weeks ending
3rd Jan to 20th March
12 weeks
138,916
143,738
-4,822
-3%
27 March to 5 June
11 weeks
168,396
109,703
+58,693
+54%
LOCKDOWN
12 June to 9 Oct
18 weeks
166,392
165,808
+584
0%
These figures suggest that it is the lockdown itself and not any virus, that caused the
excess deaths.
We're here reminded of a careful
survey done last May which found that, in all countries with reliable death-figures, their
increase in mortality began after the
lockdown was imposed and not before. There is a very simple difference between cause and
effect: the cause comes first, before the effect!
A second Lockdown was imposed over the month of November. This lacked the same terror and
shock value of the first and so only reached a net 18% excess of mortality: for the five weeks
from week ending 6 November to that of 4th December there were nine thousand excess deaths,
compared to the seasonal average.
Figure: weekly data from the Office of National Statistics
for 2020, comparing total mortality per week with an estimated average from the previous five
years.
After the autumn equinox as the nights grew longer the government again started to terrorise
the population with talk of the 'dark winter' to come. Somehow they knew that a 'second wave'
was coming, and so there would have to be a 'second lockdown' and no Christmas. Here's what I
said in a podcast on 20 th
October :
They are trying to resuscitate another big scare, trying to claim there is a second wave
come this autumn, they have started drumming up fear again, they have imposed these levels of
Lockdown which are rather terrifying. A lot of stress they are putting on people, I've been
wondering, are the deaths going to go up again like last time?
Did that happen? The figures show as before a surge around the time of the lockdown and just
before it, however this time it did not vanish after the lockdown. That's because there was not
really any easing up. On the contrary yet more draconian measures were announced, with the
unheard-of measure of police stopping people walking outdoors, to ask them if they had good
reason to be out of their house? Meeting friends was forbidden, etc. That pressure pushed up
the mortality even more and we here especially note the 'Christmas week' ending 25
th December, with a whopping 45% excess mortality. That is not a merry Christmas,
it's an extra three and a half thousand people popping off (as compared to previous years) in a
week, caused presumably by shock and despair of Xmas being cancelled. The week after that it
was still very high, 26% excess, as folk faced the bleak new year.
It helps to express that excess mortality as overall monthly means, for the last few months
of 2020. Thus taking each month as a whole and selecting four weeks of data for each month:
September from weeks ending
11 Sept to 2 Oct.
+4%
October
9 Oct to 30th Oct
+7%
November
6 Nov to 27 Nov
+18%
December
4 Dec to 1st Jan
+21%
Slowly the excess deaths (comparing, as before, with previous years) have increased through
the autumn and winter. The month of December had ten thousand extra deaths. Should one take the
government's view, that these deaths were caused by the CV19 virus, and that the
increasingly severe restrictions were a necessary response to 'contain' the spread of this
virus? A simpler hypothesis would be that there is no virus killing people, whereas the stress
of bankruptcy, solitude, loneliness, etc. imposed by government edicts really has been killing
people. Thus for example 'tier 4' was announced on 19 th December for large parts of
England and that resulted in the highest mortality for the week following. That knockout
blow to everyone's Christmas – never banned since the days of Oliver Cromwell – had
the deep impact, driving up the mortality index.
Overall it would appear to be the government's lockdown policy that has been killing people
and not some new disease. Stress, loneliness, fear and despair have been causing the
excess of deaths: together with emptying out of hospitals, especially of old folk and
cancellation of normal services because of the 'pandemic.' If the government knows this, then
it is a population-reduction program.
A recent
US CDC report agreed with the approach we've here taken, that the significance of CV19 can
only be appreciated in terms of total mortality. Published on the John Hopkins University
website on 22 nd November (but soon removed), it endorses the view that no virus is
killing people, any more than normal flu, whereas deaths from other causes are being
re-classified as Covid19:
According to new data, the U.S. currently ranks first in total COVID-19 cases, new cases
per day and deaths. Genevieve Briand, assistant program director of the Applied Economics
master's degree program at Hopkins, critically analyzed the effect of COVID-19 on U.S. deaths
using data from the Centers for Disease Control and Prevention (CDC) in her webinar titled
"COVID-19 Deaths: A Look at U.S. Data."
From mid-March to mid-September, U.S. total deaths have reached 1.7 million, of which
200,000, or 12% of total deaths, are COVID-19-related. Instead of looking directly at
COVID-19 deaths, Briand focused on total deaths per age group and per cause of death in the
U.S. and used this information to shed light on the effects of COVID-19.
She explained that the significance of COVID-19 on U.S. deaths can be fully understood
only through comparison to the number of total deaths in the United States.
After retrieving data on the CDC website, Briand compiled a graph representing percentages
of total deaths per age category from early February to early September, which includes the
period from before COVID-19 was detected in the U.S. to after infection rates soared.
Surprisingly, the deaths of older people stayed the same before and after COVID-19. Since
COVID-19 mainly affects the elderly, experts expected an increase in the percentage of deaths
in older age groups. However, this increase is not seen from the CDC data. In fact, the
percentages of deaths among all age groups remain relatively the same.
"The reason we have a higher number of reported COVID-19 deaths among older individuals
than younger individuals is simply because every day in the U.S. older individuals die in
higher numbers than younger individuals," Briand said.
Briand also noted that 50,000 to 70,000 deaths are seen both before and after COVID-19,
indicating that this number of deaths was normal long before COVID-19 emerged. Therefore,
according to Briand, not only has COVID-19 had no effect on the percentage of deaths of older
people, but it has also not increased the total number of deaths.
These data analyses suggest that in contrast to most people's assumptions, the number
of deaths by COVID-19 is not alarming. In fact, it has relatively no effect on deaths in the
United States
When Briand looked at the 2020 data during that seasonal period, COVID-19-related deaths
exceeded deaths from heart diseases. This was highly unusual since heart disease has always
prevailed as the leading cause of deaths. However, when taking a closer look at the death
numbers, she noted something strange. As Briand compared the number of deaths per cause
during that period in 2020 to 2018, she noticed that instead of the expected drastic increase
across all causes, there was a significant decrease in deaths due to heart disease. Even more
surprising, as seen in the graph below, this sudden decline in deaths is observed for all
other causes.
This trend is completely contrary to the pattern observed in all previous years.
Interestingly, as depicted in the table below , the total decrease in deaths by other
causes almost exactly equals the increase in deaths by COVID-19. This suggests, according to
Briand, that the COVID-19 death toll is misleading. Briand believes that deaths due to heart
diseases, respiratory diseases, influenza and pneumonia may instead be recategorized as being
due to COVID-19.
Base on this analysis, the best way to end the ongoing mass-killing of elderly Britons would
be to terminate the lockdowns and resume normal life. As Dr Simone Gold (of Frontline Doctors )
well explained , CV19
is just 'killing' elderly people who were about to die anyhow. It cannot be shown that 'having'
CV19 i.e. testing PCR-'positive' contributed to shortening their life. So that isn't a causal
connection, i.e. the alleged illness has not 'caused' their death. That's why the
age-distribution of CV-19 is indistinguishable from that of the normal population.
The average age of death in England & Wales is 81.5 years, while the average age of
'Covid-19 fatalities' is
82.4 years (ONS data). What this tells us is very simple: the disease does not
exist.
The concept of PCR 'testing' has always been
fraudulent . The so-called PCR 'test' multiplies up fragments of nucleotide-chains and the
number of 'positive' cases depends on the multiplication factor used as
well as how many persons are tested. There will never come a time when the virus is 'cured' or
'solved' or whatever people imagine the government is trying to do (if it knows!), such that
the PCR test ceases to generate 'positive' tests. No-one will ever give you evidence that
people who test 'positive' get ill more often than others. Is there an aim of government
policy, aside from terrorising the populace? Is it to kill the virus? That can never happen
because the virus isn't alive.
he World Health Organization has now backtracked over the PCR 'test', saying (January 13
th ) it is merely a
diagnostic tool that can assist. It now advises –
Where test results do not correspond with the clinical presentation, a new specimen should
be taken and retested using the same or different NAT technology.
In other words, a single PCR test should not be used for diagnosing Sars-Cov-2
infection. It's merely a guide!
Most PCR assays are indicated as an aid for diagnosis, therefore, health care providers
must consider any result in combination with timing of sampling, specimen type, assay
specifics, clinical observations, patient history, confirmed status of any contacts, and
epidemiological information.
So we finally have it that the PCR cannot be relied upon a diagnostic test. Which is
exactly what its inventor Kary Mullis said. So forget all of the figures you've heard about
'cases' and 'covid deaths' – they cannot be relied upon.
If one did want to believe there was a disease associated with this virus, then surely we'd
agree with Dr Alexander Myasnikov, appointed last year as Russia's chief medical advisor.
In an interview he explained how the world had greatly over-reacted to the CV19 story and
death numbers in the West were greatly over-counted. He added:
"It's all exaggerated. It's an acute respiratory disease with minimal mortality."
Thus the former Chief Medical Officer of Ontario has recently
challenged his government's policy saying, "We're Being Locked-down for an Infection
Fatality Rate of Less than 0.2%?" and the lockdown is not "supported by strong science." He
here means, that for those who test PCR-positive one in five hundred will die. The time-period
here involved needs to be defined, eg it could be one month: we all die, and given the median
age of alleged-CV19 deaths is around 80 that could well be a normal rate of mortality –
especially if they are PCR-testing everyone admitted to hospitals.
Last November a
Cornish nurse went public, saying the hospital wards had been empty over months when it was
claimed they were overflowing. She said whenever they had flu patients they were classified as
Covid: 'flu and Covid cases are now recorded as 'the same thing' on death certificates.' . That
wouldn't be necessary if the disease really existed. Not surprisingly, the flu this winter has
mysteriously vanished . One woman who walked round her local hospital filming its empty
wards was
arrested by police entering her home the next day.
The virus itself cannot be shown to exist, by which we mean that it cannot be reliably
differentiated from all the other normal coronaviruses, that have been with us since time
began. It has never been isolated, let's be clear about that. Last April an
EU science department admitted :
" No virus isolates with a quantified amount of the SARS-CoV-2 are currently
available "
And the same thing was echoed a few months later by the US Centre for Disease Control:
" Since no quantified virus isolates of the 2019-nCoV are currently available ,
assays [diagnostic tests] designed for detection of the 2019-nCoV RNA were tested with
characterized stocks of in vitro transcribed full length RNA " [2]
In other words, nobody can hold a test-tube or petri-dish and say, 'Here is COVID-19.'
Published gene-sequences of the alleged virus are mere hypothetic constructs. Yes some disease
broke out in Wuhan in November 2019 and yes the Chinese authorities published a gene-sequence
allegedly of it, but so what?
Fear Porn Promotion
The government needs your fear. It wants your attention but knows that it has no
prospect of improving your life in any way. Thus we have a health minister who knows nothing
about health or well-being: he can get your attention by telling you that you won't be able to
fly without a vaccine. They need your fear, and in the last century the government was
able to arouse your fear by threatening to press the nuclear button. That doesn't work any
more. The UK govts latest exercise in fear-porn advises citizens to behave as if they are
ill . ('Act like you've got it') Yes, that sounds just like how to promote health.
It further promotes the diabolical idea that perfectly healthy persons can transmit disease
('anyone can spread it'). Here one could quote the WHO expert Dr Maria van Kerkhove: 'From the
data we have, it still seems to be rare that an asymptomatic person actually transmits onwards
to a secondary individual. Its very rare.' (Head of the WHO Emerging disease and zoonosis unit
at a news briefing from the UN agency's headquarters at Geneva, 6.6.20). Admittedly she was
pressured to backpedal and retract, but she did say it. [3]
In the words of the Daily Mail , 'Terrifying new TV ads' are being promoted by the
Government (23 Jan 2021) The above fear-porn promotion is through the US media agency Omnigov,
who signed a 110 million Lockdown advertising
deal – on March 2 nd , three weeks before the Lockdown.
The journalist Neil Clark commented [4] on 'the report in the
Daily Telegraph newspaper that the UK government struck a deal worth £119m with an
American advertising company, OMD Group, urging people to 'Stay Home, Stay Safe' a full three
weeks before Boris Johnson ordered a lockdown. Think about what this means.' That meme 'Stay
home Stay safe' would have been blueprinted the previous year at the US 'Event 201' by Bill
Gates et. al. Fear blocks out rational, coherent thought which is why the government
needs it.
People may be forgetting how debilitating winter flu can be and how it can last for weeks.
Now they want to call it COVID. Let's here support Prof. Dolores Cahill, who has been looking
at the sequencing of PCR testing. In Ireland it was found that of fifteen hundred PCR tests
'all of them were influenza A and B, not one of them were SARS-COV2.' Her group will be seeking
legal action where the tests come back as influenza rather than the specific CV19 and doctors
can be sued for medical negligence. ( Corbett Report, 23 mins)
That sounds like a promising way of dealing with this phantomic virus.
'Is this an epidemic of despair?' asked that perceptive commentator
Peter Hitchins . Scientists are trained not to take notice of emotions and instead to look
for things, objects as causative agents, whereas here we agree with Peter Hitchens that the
negative soul-conditions of the populace caused by government policies are leading to death.
Hitchens' article quotes the distinguished professor of medical microbiology, Sucharit
Bhakdi:
'He said that older people had the right to make efforts to stay fit, active, busy and
healthy. But he warned that the shutdown of society would condemn them to early death by
preventing this.
'Social contacts and social events, theatre and music, travel and holiday recreation,
sports and hobbies, all help to prolong their stay on earth. The life expectancy of millions
is being shortened.'
In a prediction that has turned out to be terribly accurate, he added: 'The horrifying
impact on the world economy threatens the existence of countless people. The consequences for
medical care are profound. Already services to patients who are in need are reduced,
operations cancelled, practices empty, hospital personnel dwindling. All this will impact
profoundly on our whole society.'
That is what is killing people, there is no other pandemic.
We're here concerned with UK, however for comparison let's end with
a graph showing the US weekly mortality rate over 2020, showing the very same effect.
The graph shown an excess of 280k deaths above normal-expected levels, following the
lockdown. The web-page hosting this graph states 'The large spike in deaths in April 2020
corresponds to the coronavirus outbreak.' I'm here suggesting a different view.
By Nick
Kollerstrom , PhD, author of The Great British coronavirus Hoax, A Sceptics view
(banned by Amazon.)
Notes
[1] Using fifty-two weeks
i.e. 364 days of the year, from the week ending 3 rd January 2020 to that of 1
st January 2021, the ONS compares a week in 2020 with the average value for
2015-9.
[2] CDC '2019-Novel
Coronavirus Real-Time PCR Diagnostic Panel performance characteristics' p.39, 13.7.20. This has
been scrubbed from the Web, but see BMJ response to it.
[3] A huge Chinese study
of ten million around Wuhan between May and June showed 'no evidence that positive cases
without symptoms spread the disease': Nature 20.11.20 'Post-lockdown SARS-CoV-2 nucleic
acid screening'.
[4] RT 'Covid-19 reverse
psychology' by Neil Clarke, 28.10.20, deleted but preserved on the Hugo Talks video
Coronavirus variants: What they do and how worried you should be
The Ars guide to the coronavirus variants
BETH MOLE
-
1/28/2021,
7:00 PM
Enlarge
/
Coronaviruses
Getty | BSIP
102
WITH
66 POSTERS PARTICIPATING
SHARE ON FACEBOOK
SHARE ON TWITTER
Covid-19 Coverage
Coronavirus variants: What they do and how worried you should be
Basic pandemic safety limits spread in schools
"We're failing": Ex-Warp Speed leader proud, deflects blame on vaccines
"I can't tell you how much vaccine we have," new CDC head says
"Complete incompetence:" Biden team slams Trump's COVID work
View more stories
Ever since the novel coronavirus,
SARS-CoV-2, began jumping from human to human, it's been mutating. The molecular machinery the virus uses to read and
make copies of its genetic code isn't great at proofreading; minor typos made in the copying process can go uncorrected.
Each time the virus lands in a new human victim, it infects a cell and makes an army of clones, some carrying genetic
errors. Those error-bearing clones then continue on, infecting more cells, more people. Each cycle, each infection
offers more opportunity for errors. And, over time, those errors, those mutations, accumulate.
Some of these changes are meaningless. Some are lost in the frenetic
viral manufacturing. But some become permanent fixtures, passed on from virus to virus, human to human. Maybe it happens
by chance; maybe it's because the change helps the virus survive in some small way. But in aggregate, viral strains
carrying one notable mutation can start carrying others. Collections of notable mutations start popping up in viral
lineages, and sometimes they seem to have an edge over their relatives. That's when these distinct viruses -- these
variants -- get concerning.
Scientists around the world have been closely tracking mutations and
variants since the pandemic began, watching some rise and fall without much ado. But in recent months, they have become
disquieted by at least three variants. These variants of concern, or VOCs, have raised critical questions -- and alarm -- over
whether they can spread more easily than previous viral varieties, whether they can evade therapies and vaccines, or
even whether they're deadlier.
Here, we'll run down what we know and what we don't know about these
variants. With much research yet to be done, there's a lot of unanswered questions. But researchers are working quickly
to address the most important unknowns. High on the list is whether the vaccines we already have will be effective
against the variants. So far, it seems likely that they will be. Still, the virus is sending a clear message: with
rampant transmission accelerating viral evolution, more variants will arise and we need to be prepared.
With more data becoming available by the day, we'll update this story
with significant findings as they come along. Before we get to the data we have, a quick note on names: it's problematic
to identify diseases or infectious agents -- in this case, virus variants -- based on where they were identified. Such
geographic associations risk creating stigma and may discourage reporting, so there is an
active
discussion
in the scientific community about how best to name the current variants. In the interim, it has become
all too common to refer to these by their country of origin. We'll try to avoid that as much as possible while making
clear which variants we're talking about.
B.1.1.7
Alternate names
:
501Y.V1 and VOC 202012/01
70
In early December 2020, researchers and officials in the UK began
warning of a new variant that seemed to be spreading abnormally fast while carrying an unusually large number of
mutations -- 23. The first record of the variant in the UK stretched back to two samples taken from infected people on
September 20 and September 21. In a matter of weeks, the variant began making up a larger and larger proportion of total
cases there. Researchers quickly suspected the variant had evolved to become more transmissible -- that is, it's able to
spread more easily from person to person.
Advertisement
me title=
Transmission
Data analyses since December have supported that hypothesis, but
researchers are still working out exactly how much more transmissible it is compared to earlier versions. In early
January, UK researchers released preliminary results from a series of models that estimated the variant tacks on
an
additional 0.36 to 0.68 onto SARS-CoV-2's observed reproduction number
. That means, on average, people infected with
B.1.1.7 will go on to infect an
additional
0.36 to 0.68 people on top of how many
they would have infected if they were carrying an earlier version of the virus. More recent estimates have been roughly
in this range, suggesting B.1.1.7 has around a
47
percent
or
56
percent increase
in transmission.
B.1.1.7 has now been detected in more than 60 countries beyond the UK,
including the United States, where it has been found in
at
least two dozen states
. A
modeling
study
published by the US Centers for Disease Control and Prevention on January 15 estimated that it will become the
predominant strain in the US in March.
Mutations
Some of the mutations B.1.1.7 carries seem to help explain the virus's
newfound ability. The variant carries
23
mutations
in all: 13 mutations that change the virus's protein sequences (non-synonymous), four deletions, and six
synonymous mutations. Of B.1.1.7's mutations, eight occur in the virus's spike protein, the now notorious club-like
protein that juts out from the virus's spherical particle. That spike is what the virus uses to latch onto and infect
cells, which the protein accomplishes by binding a receptor on the outside of human cells called ACE2.
So far, we know that
at
least three
of B.1.1.7's eight spike mutations may be relevant to the variant's boosted transmission. Chief among
them is a mutation that changes one of the spike proteins' critical amino acids -- the amino acid at position 501 of
spike's protein sequence. Specifically, the mutation changes the amino acid at 501 from an asparagine (N) to a tyrosine
(Y), so the mutation is written as N501Y. The 501 amino acid is critical because it lies within the area of spike that
directly binds to ACE2 -- called the receptor binding domain (RBD) -- and it is one of just six key contact residues in the
RBD.
Lab
experiments
have suggested that changing from an N to a Y at 501 increases spike's ability to bind ACE2, and
experiments
in mice
linked the mutation to increased infectiousness and disease.
After N501Y, there's P681H. The mutation at position 681 -- changing the
amino acid from a proline (P) to a histidine (H) -- falls near a unique furin cleavage site on SARS-CoV-2's spike protein.
For SARS-CoV-2 to successfully get into a cell after binding ACE2, the spike protein needs to be cleaved into its two
subunits by enzymes. The split changes spike's conformation and activates it, allowing it to fuse itself to the cell
membrane and dump its contents into the now-infected cell. In
animal
studies
, the furin cleavage site seemed to boost the virus's ability to enter cells. Researchers suspect the new
mutation may boost entry further.
Enlarge
/
A patient prepares to receive an injection of the
Oxford/AstraZeneca COVID-19 vaccine by Royal Navy medics at a vaccination center set up at Bath racecourse in Bath,
southwest England.
Adrian DENNIS / AFP / Getty Images
The third spike mutation known to be significant is a deletion of six nucleotides in its genetic
code, which leads to the loss of two amino acids at positions 69 and 70 in the spike protein. It's unclear what this
deletion does for the virus exactly, but it has arisen a number of times in different lineages, suggesting it
offers
an advantage
. For now, there is one clear consequence for researchers: the deletion messes up a diagnostic test for
SARS-CoV-2. The test is a three-target RT-PCR test, meaning it works by detecting three snippets of the SARS-CoV-2
genome, including one in the gene that codes for spike. When this 69-70 deletion is present, the test will show up
negative for the spike gene but positive for the other two SARS-CoV-2 genetic sequences. This result is referred to as "
S
gene dropout
" and is now used to help identify infections caused by B.1.1.7.
Advertisement
me title=
These three mutations are the most notable in B.1.1.7 for now. There's
scant data on the other 20, but researchers are working swiftly to assess what each might do on its own or in
combination with the others.
Disease
severity/mortality
When researchers first raised concerns about B.1.1.7, all of those
issues related to increased transmissibility. Preliminary evidence looking at infection outcomes did not suggest that
B.1.1.7 was causing more severe disease or more deaths than other virus strains. Still, some saw little comfort in this,
given that any increase in the total number of infections still leads to more severe cases and deaths in absolute
numbers.
The situation took a darker turn January 21, when a UK government
advisory group -- NERVTAG -- found
preliminary
evidence
that "there is a realistic possibility that infection with VOC B.1.1.7 is associated with an increased risk
of death compared to infection with non-VOC viruses."
So far, some experts are not yet convinced by the preliminary evidence
presented, and they're calling for much more data before any conclusions are drawn. For one thing, the full data sets
behind some of the analyses done so far have not been published, and some of them relied on comparing small numbers of
deaths in people infected with B.1.1.7 with larger numbers of deaths in people infected with other strains. Some experts
also wonder whether the calculated increase in deaths could simply be explained by overburdened hospitals rather than a
deadlier variant.
Vaccine
efficacy
With increased infectiousness and the possibility of being deadlier, a
critical question raised by B.1.1.7 is whether or not the current vaccines we have -- mRNA vaccines from Pfizer/BioNTech
and Moderna -- will work against the variant. So far, the answer appears to be yes.
On January 19, researchers at Pfizer and BioNTech released
a
non-peer reviewed study
where they pitted antibody-laden blood from 16 people given their mRNA vaccine (BNT162b2)
against a pseudovirus that carried B.1.1.7's mutated spike protein. The researchers found that the vaccines' antibodies
were just as good at neutralizing the pseudovirus with B.1.1.7's mutated spike protein as they were at neutralizing a
pseudovirus with the spike protein from a reference SARS-CoV-2 virus.
"These data make it unlikely that the B.1.1.7 lineage will escape
BNT162b2-mediated protection," the researchers concluded.
Likewise, on January 25, Moderna released its own
non-peer
reviewed study
, which was similar in design. They tested the antibodies from eight people given their mRNA vaccine
against a pseudovirus bearing B.1.1.7's mutated spike protein. Again, the antibodies neutralized the pseudovirus at
levels comparable to those seen with a pseudovirus carrying a reference spike protein.
Yet
another
similar study
, led by researchers at Columbia University and released January 26, found the same results. Antibodies
from 12 people who received Moderna's vaccine and 10 people who received Pfizer's vaccine were able to neutralize a
pseudovirus containing B.1.1.7's mutated spike protein, with only a modest drop in potency compared with neutralization
of a pseudovirus carrying a reference spike protein.
Down South , Jan 26 2021 17:58 utc |
9
Vaccine manufacturer Merck has abandoned development of two coronavirus vaccines, saying
that after extensive research it was concluded that the shots offered less protection than
just contracting the virus itself and developing antibodies.
The company announced that the shots V590 and V591 were 'well tolerated' by test
patients, however they generated an 'inferior' immune system response in comparison with
natural infection.
Merck Scraps COVID Vaccines; Says It's More Effective To Get The Virus And Recover
Moneycircus
UK Column News – 22nd January 2021
SUGGESTS MANY TESTS ARE PRODUCING FALSE POSITIVEShttps://www.who.int/news/item/20-01-2021-who-information-notice-for-ivd-users-2020-05
KEEP TESTING AND YOU WILL FIND ANYTHING – EXACTLY WHAT KARY MULLIS SAID
GBP 500 BRIBE FOR A JAB UNDER CONSIDERATION
PM WON'T COMMIT TO ENDING LOCKDOWN
STILL NO INFORMATION ON WHETHER DEATHS ARE RISING OR WHY
CENSORSHIP RULES AS SOCIAL MEDIA UPHOLD GOV NARRATIVEhttps://www.spiked-online.com/2021/01/20/it-is-a-journalists-duty-to-question-lockdown/W
MHRA'S CEO JUNE RAINE: NOTHING UNUSUAL IN ADVERSE REACTIONS
UNIONS NOW OBLIGING MEMBERS TO COMPLY WITH VACCINATIONS.
OVER-50s SAGA GROUP FALLS IN LINE WITH VAX PASSPORTS
JUST SAY NO -- CONVENTION ON BIOETHICS AND HUMAN RIGHTS
"The consent should, where appropriate, be expressed and may be withdrawn by the person
concerned at any time and for any reason without disadvantage or prejudice."
Mike Robinson: the principle is there but it is not binding in any way
NORTHERN IRELAND LOCKDOWN EXTENDED TO MAR 5
U.S. PRESIDENTIAL INSTALLATION FAKENESS
GUSHING MEDIA FINALLY FREE
CNN Jeff Zeleny: Their majesties Obama, Bush and Clint, recorded a video reflecting "the
majesty of the passage of power, importance of upholding democracy".
CNN overcome with Biden on stage with Obama "The comforting sight of the Clintons and the
Bushes and the Obamas, the Avengers, the Marvel superheroes back together, with their friend
Joe Biden all of them sharing the view of a lot of Americans that we did narrowly avert
catastrophe all there to butress their buddy Joe Biden."
Patrick Henningsen: see the infantilization of politics. It has become a spectator sport
and politicians have become Marvel superheroes.
EXECUTIVE ORDER: MASK WEARING AND DISTANCING ON FEDERAL PROPERTY
BBC: KAMALA HARRIS A PRESIDENT IN WAITING?
FOREIGN POLICY OUTLOOKhttps://www.politico.eu/article/uk-pitch-joe-biden-china-us-trade/
MARK SEDWILL RUNNING UK FOREIGN POLICY
MACRON CALLS ON BIDEN FOR GREATER U.S. INVOLVEMENT
Moneycircus
Moneycircus
UK Column News – 22nd January 2021
MAGICAL BAGHDAD BOMBING DAY AFTER BIDEN INSTALLATION
ISIS 'WE BOMBED RANDOM MARKET -- PLEASE OCCUPY IRAQ AGAIN.'
RACHEL LEVINE, ASST HEALTH SECRETARY
https://www.pennlive.com/news/2020/05/health-secretary-rachel-levines-removal-of-mom-from-care-home-amid-epidemic-draws-scrutiny.html
LIBERTY GROUPS RESIST FURTHER CLAMPDOWN ON "TERROR"https://www.naacpldf.org/wp-content/uploads/No_Domestic_Terrorism_Charge_1_19_2021-1.pdf
ASSANGE PARDON REPORTEDLY BLOCKED BY MITCH MCCONNELL
CHATHAM HOUSE MASTERCLASS IN MANIPULATING PUBLIC PERCEPTIONS
https://player.vimeo.com/video/320913130
Sitting in the front row was the UK's Jonathn Van Tam, Deputy Chief Medical Officer for
England
Marc van Ranst's Masterclass on Manipulating Public Fear for CFR-Chatham Ho.:That is true in every
year (laughter) but talking about fatalities gets attention because people don't usually
think about anyone dying from influenza.
Mike Robinson: The point he made about deaths is important. You take a number that is
normal, it happens every year but it is not usually reported. You start reporting it and
people think there is something special about that number. Then you add on the effects of
lockdown and you say this is really serious, even though the excess mortality is little
different to what's happened in history."
Simples!
UK Column News – 22nd January
2021
https://www.youtube.com/embed/edln7eWn4ck?version=3&rel=1&showsearch=0&showinfo=1&iv_load_policy=1&fs=1&hl=en-US&autohide=2&wmode=transparent
Moneycircus
Moneycircus
The Chatham House video can be watched here. Download this handy masterclass on manipulating
public fear before it's deleted. MP4 downloader
Moneycircus
Moneycircus
Clarification: It was MSNBC national affairs analyst John Heilemann who said seeing the
past presidents standing next to Biden was
"like the Avengers, sort of the Marvel superheroes, back up there together. "
Barbara Ann ,
23 January 2021 at 08:08 PM
Patrick
From the ZH article; "None of this was for your health. It was to get rid of Orange Man
Bad".
100%. The WHO's revised guidance
effectively says the majority of infection data from PCR testing is meaningless. ZH notes
Florida as a possible exception. The original guidance issued on 2020/12/14 seems to have
been scrubbed from the WHO's website but was archived here: ( https://web.archive.org/web/20210102051357/https://www.who.int/news/item/14-12-2020-who-information-notice-for-ivd-users).
">https://www.who.int/news/item/14-12-2020-who-information-notice-for-ivd-users).">https://web.archive.org/web/20210102051357/https://www.who.int/news/item/14-12-2020-who-information-notice-for-ivd-users).
The revised guidance calls for a retest upon a weak positive* result and publication of the
Ct value along with the result.
*Why no retest after a weak negative, am I missing something re the risk of false negative
results? Otherwise weeding out false positives only looks a lot like a policy to drive down
reported infection rates.
The next stage of course is for the CDC to update their guidance (not updated since
October) and revise the stats - hey presto pandemic over, all under the Biden
administration.
This is the most audacious, yet transparent, PSYOP of all time. I just can't believe
someone, somewhere doesn't have hard intel. on whoever is running it.
Introduction: using a technique to lock down society
All current propaganda on the COVID-19 pandemic is based on an assumption that is
considered obvious, true and no longer questioned:
Positive RT-PCR test means being sick with COVID. This assumption is misleading .
Very few people, including doctors, understand how a PCR test works.
RT-PCR means R eal T ime- P olymerase C hain R eaction.
In French, it means: Réaction de Polymérisation en Chaîne en Temps
Réel.
In medicine, we use this tool mainly to diagnose a viral infection.
Starting from a clinical situation with the presence or absence of particular symptoms in a
patient, we consider different diagnoses based on tests.
In the case of certain infections, particularly viral infections, we use the RT-PCR
technique to confirm a diagnostic hypothesis suggested by a clinical picture.
We do not routinely perform RT-PCR on any patient who is overheated, coughing or has an
inflammatory syndrome!
It is a laboratory, molecular biology technique of gene amplification because it looks for
gene traces (DNA or RNA) by amplifying them.
In addition to medicine, other fields of application are genetics, research, industry and
forensics.
The technique is carried out in a specialized laboratory , it cannot be done in any
laboratory, even a hospital. This entails a certain cost, and a delay sometimes of several days
between the sample and the result.
Today, since the emergence of the new disease called COVID-19 ( CO rona VI rus D isease-20
19 ), the RT-PCR diagnostic technique is used to define positive cases, confirmed as SARS-CoV-2
(coronavirus responsible for the new acute respiratory distress syndrome called COVID-19).
These positive cases are assimilated to COVID-19 cases, some of whom are hospitalized or
even admitted to intensive care units.
Official postulate of our managers: positive RT-PCR cases = COVID-19 patients. [1]
This is the starting postulate, the premise of all official propaganda, which justifies all
restrictive government measures: isolation, confinement, quarantine, mandatory masks, color
codes by country and travel bans, tracking, social distances in companies, stores and even,
even more importantly, in schools [2].
This misuse of RT-PCR technique is used as a relentless and intentional strategy by some
governments , supported by scientific safety councils and by the dominant media, to justify
excessive measures such as the violation of a large number of constitutional rights, the
destruction of the economy with the bankruptcy of entire active sectors of society, the
degradation of living conditions for a large number of ordinary citizens, under the pretext of
a pandemic based on a number of positive RT-PCR tests, and not on a real number of patients
.
Technical aspects: to better understand and not be manipulated
The PCR technique was developed by chemist Kary B. Mullis in 1986. Kary Mullis was awarded
the Nobel Prize in Chemistry in 1993.
Although this is disputed [3], Kary Mullis himself is said to have criticized the interest
of PCR as a diagnostic tool for an infection, especially a viral one.
He stated that if PCR was a good tool for research, it was a very bad tool in medicine, in
the clinic [4].
Mullis was referring to the AIDS virus (HIV retrovirus or HIV) [5], before the COVID-19
pandemic, but this opinion on the limitation of the technique in viral infections [6], by its
creator, cannot be dismissed out of hand; it must be taken into account!
PCR was perfected in 1992.
As the analysis can be performed in real time, continuously, it becomes RT (Real-Time)
– PCR , even more efficient.
It can be done from any molecule, including those of the living, the nucleic acids that make
up the genes:
DNA (deoxyribonucleic acid)
RNA (Ribonucleic Acid)
Viruses are not considered as "living" beings, they are packets of information (DNA or RNA)
forming a genome.
It is by an amplification technique (multiplication) that the molecule sought is highlighted
and this point is very important.
RT-PCR is an amplification technique [7].
If there is DNA or RNA of the desired element in a sample, it is not identifiable as
such.
This DNA or RNA must be amplified (multiplied) a certain number of times , sometimes a very
large number of times, before it can be detected. From a minute trace, up to billions of copies
of a specific sample can be obtained, but this does not mean that there is all that amount in
the organism being tested.
In the case of COVID-19, the element sought by RT-PCR is SARS-CoV-2, an RNA virus [8].
There are DNA viruses such as Herpes and Varicella viruses.
The most well known RNA viruses , in addition to coronaviruses, are Influenza, Measles,
EBOLA, ZIKA viruses.
In the case of SARS-CoV-2, RNA virus, an additional specific step is required, a
transcription of RNA into DNA by means of an enzyme, Reverse Transcriptase.
This step precedes the amplification phase.
It is not the whole virus that is identified, but sequences of its viral genome.
This does not mean that this gene sequence, a fragment of the virus, is not specific to the
virus being sought, but it is an important nuance nonetheless:
RT-PCR does not reveal any virus, but only parts, specific gene sequences of the virus.
At the beginning of the year, the SARS-CoV-2 genome was sequenced.
It consists of about 30,000 base pairs. The nucleic acid (DNA-RNA), the component of the
genes, is a sequence of bases. In comparison, the human genome has more than 3 billion base
pairs.
Teams are continuously monitoring the evolution of the SARS-CoV-2 viral genome as it evolves
[9-10-11], through the mutations it undergoes. Today, there are many variants [12].
By taking a few specific genes from the SARS-CoV-2 genome, it is possible to initiate RT-PCR
on a sample from the respiratory tract.
For COVID-19 disease, which has a nasopharyngeal (nose) and oropharyngeal (mouth) entry
point, the sample should be taken from the upper respiratory tract as deeply as possible in
order to avoid contamination by saliva in particular.
ll the people tested said that it is very painful [13].
The Gold Standard (preferred site for sampling) is the nasopharyngeal (nasal) approach , the
most painful route.
If there is a contraindication to the nasal approach, or preferably to the individual being
tested, depending on the official organs, the oropharyngeal approach (through the mouth) is
also acceptable. The test may trigger a nausea/vomiting reflex in the individual being
tested.
Normally, for the result of an RT-PCR test to be considered reliable, amplification from 3
different genes (primers) of the virus under investigation is required .
"The primers are single-stranded DNA sequences specific to the virus. They guarantee the
specificity of the amplification reaction. " [14]
"The first test developed at La Charité in Berlin by Dr. Victor Corman and his
associates in January 2020 allows to highlight the RNA sequences present in 3 genes of the
virus called E, RdRp and N . To know if the sequences of these genes are present in the RNA
samples collected, it is necessary to amplify the sequences of these 3 genes in order to
obtain a signal sufficient for their detection and quantification. "[15].
The essential notion of Cycle Time or Cycle Threshold or Ct positivity threshold [16].
An RT-PCR test is negative (no traces of the desired element) or positive (presence of
traces of the desired element).
However, even if the desired element is present in a minute, negligible quantity, the
principle of RT-PCR is to be able to finally highlight it by continuing the amplification
cycles as much as necessary.
RT-PCR can push up to 60 amplification cycles, or even more!
Here is how it works:
Cycle 1: target x 2 (2 copies)
Cycle 2: target x 4 (4 copies)
Cycle 3: target x 8 (8 copies)
Cycle 4: target x 16 (16 copies)
Cycle 5; target x 32 (32 copies)
Etc exponentially up to 40 to 60 cycles!
When we say that the Ct (Cycle Time or Cycle Threshold or RT-PCR positivity threshold) is
equal to 40, it means that the laboratory has used 40 amplification cycles , i.e. obtained 2
40 copies.
This is what underlies the sensitivity of the RT-PCR assay.
While it is true that in medicine we like to have high specificity and sensitivity of the
tests to avoid false positives and false negatives, in the case of COVID-19 disease, this
hypersensitivity of the RT-PCR test caused by the number of amplification cycles used has
backfired.
This over-sensitivity of the RT-PCR test is deleterious and misleading!
It detaches us from the medical reality which must remain based on the real clinical state
of the person: is the person ill, does he or she have symptoms?
That is the most important thing!
As I said at the beginning of the article, in medicine we always start from the person: we
examine him/her, we collect his/her symptoms (complaints-anamnesis) and objective clinical
signs (examination) and on the basis of a clinical reflection in which scientific knowledge and
experience intervene, we make diagnostic hypotheses.
Only then do we prescribe the most appropriate tests, based on this clinical reflection.
We constantly compare the test results with the patient's clinical condition (symptoms and
signs), which takes precedence over everything else when it comes to our decisions and
treatments.
Today, our governments, supported by their scientific safety advice, are making us do the
opposite and put the test first, followed by a clinical reflection necessarily influenced by
this prior test, whose weaknesses we have just seen, particularly its hypersensitivity.
None of my clinical colleagues can contradict me.
Apart from very special cases such as genetic screening for certain categories of
populations (age groups, sex) and certain cancers or family genetic diseases, we always work in
this direction: from the person (symptoms, signs) to the appropriate tests, never the other way
around.
This is the conclusion of an article in the Swiss Medical Journal (RMS) published in 2007,
written by doctors Katia Jaton and Gilbert Greub microbiologists from the University of
Lausanne :
PCR in microbiology: from DNA amplification to result interpretation :
"To interpret the result of a PCR, it is essential that clinicians and microbiologists
share their experiences, so that the analytical and clinical levels of interpretation can be
combined."
It would be indefensible to give everyone an electrocardiogram to screen everyone who might
have a heart attack one day.
On the other hand, in certain clinical contexts or on the basis of specific evocative
symptoms, there, yes, an electrocardiogram can be beneficial.
Back to RT-PCR and Ct (Cycle Time or Cycle Threshold).
In the case of an infectious disease, especially a viral one, the notion of contagiousness
is another important element.
Since some scientific circles consider that an asymptomatic person can transmit the virus,
they believe it is important to test for the presence of virus, even if the person is
asymptomatic, thus extending the indication of RT-PCR to everyone.
Are RT-PCR tests good tests for contagiousness? [17]
This question brings us back to the notion of viral load and therefore Ct .
The relationship between contagiousness and viral load is disputed by some people [18] and
no formal proof, to date, allows us to make a decision.
However, common sense gives obvious credence to the notion that the more virus a person has
inside him or her , especially in the upper airways (oropharynx and nasopharynx), with symptoms
such as coughing and sneezing, the higher the risk of contagiousness , proportional to the
viral load and the importance of the person's symptoms.
This is called common sense , and although modern medicine has benefited greatly from the
contribution of science through statistics and Evidence-Based Medicine (EBM), it is still based
primarily on common sense, experience and empiricism.
Medicine is the art of healing .
No test measures the amount of virus in the sample!
RT-PCR is qualitative : positive (presence of the virus) or negative (absence of the
virus).
This notion of quantity, therefore of viral load, can be estimated indirectly by the number
of amplification cycles (Ct) used to highlight the virus sought.
The lower the Ct used to detect the virus fragment, the higher the viral load is considered
to be (high).
The higher the Ct used to detect the virus fragment, the lower the viral load is considered
to be (low).
Thus, the French National Reference Centre (CNR), in the acute phase of the pandemic,
estimated that the peak of viral shedding occurred at the onset of symptoms, with an amount of
virus corresponding to approximately 10 8 (100 million) copies of SARS-CoV-2 viral
RNA on average (French COVID-19 cohort data) with a variable duration of shedding in the upper
airways (from 5 days to more than 5 weeks) [19].
This number of 108 (100 million) copies/μl corresponds to a very low Ct.
A Ct of 32 corresponds to 10-15 copies/μl.
A Ct of 35 corresponds to about 1 copy/μl.
Above Ct 35, it becomes impossible to isolate a complete virus sequence and culture it!
In France and in most countries, Ct levels above 35, even 40, are still used even today!
The French Society of Microbiology (SFM) issued an opinion on September 25, 2020 in which it
does not recommend quantitative results, and it recommends to make positive up to a Ct of 37
for a single gene [20]!
With 1 copy/μl of a sample (Ct 35) , without cough, without symptoms, one can understand
why all these doctors and scientists say that a positive RT-PCR test means nothing , nothing at
all in terms of medicine and clinic!
Positive RT-PCR tests, without any mention of Ct or its relation to the presence or absence
of symptoms, are used as is by our governments as the exclusive argument to apply and justify
their policy of severity, austerity, isolation and aggression of our freedoms, with the
impossibility to travel, to meet, to live normally!
There is no medical justification for these decisions, for these governmental choices!
In an article published on the website of the New York Times (NYT) on Saturday, August 29,
American experts from Harvard University are surprised that RT-PCR tests as practiced can serve
as tests of contagiousness, even more so as evidence of pandemic progression in the case of
SARS-CoV-2 infection [21].
The
Covid-19 Numbers Game: The "Second Wave" is Based on Fake Statistics
According to them, the threshold (Ct) considered results in positive diagnoses in people who
do not represent any risk of transmitting the virus!
The binary "yes/no" answer is not enough, according to this epidemiologist from the Harvard
University School of Public Health.
"It's the amount of virus that should dictate the course of action for each patient
tested. "
The amount of virus (viral load); but also and above all the clinical state, symptomatic or
not of the person!
This calls into question the use of the binary result of this RT-PCR test to determine
whether a person is contagious and must follow strict isolation measures.
These questions are being raised by many physicians around the world, not only in the United
States but also in France, Belgium ( Belgium Health Experts
Demand Investigation Of WHO For Faking Coronavirus Pandemic ), France, Germany, Italy, the
United Kingdom, the United States and the United Kingdom. in Germany, Spain
According to them: " We are going to put tens of thousands of people in confinement, in
isolation, for nothing. " [22]. 22] And inflict suffering, anguish, economic and
psychological dramas by the thousands!
Most RT-PCR tests set the Ct at 40, according to the NYT. Some set it at 37.
"Tests with such high thresholds (Ct) may not only detect live virus but also gene
fragments, remnants of an old infection that do not represent any particular danger," the
experts said.
A virologist at the University of California admits that an RT-PCR test with a Ct greater
than 35 is too sensitive. " A more reasonable threshold would be between 30 and 35, "
she adds.
Almost no laboratory specifies the Ct (number of amplification cycles performed) or the
number of copies of viral RNA per sample μl.
Here is an example of a laboratory result (approved by Sciensano, the Belgian national
reference center) in an RT-PCR negative patient:
No mention of Ct.
In the NYT, experts compiled three datasets with officials from the states of Massachusetts,
New York and Nevada that mention them.
Conclusion?
" Up to 90% of the people who tested positive did not carry a virus. "
The Wadworth Center, a New York State laboratory, analyzed the results of its July tests at
the request of the NYT: 794 positive tests with a Ct of 40.
" With a Ct threshold of 35 , approximately half of these PCR tests would no longer be
considered positive ," said the NYT.
"And about 70% would no longer be considered positive with a Ct of 30 ! "
In Massachusetts, between 85 and 90% of people who tested positive in July with a Ct of 40
would have been considered negative with a Ct of 30, adds the NYT. And yet, all these people
had to isolate themselves, with all the dramatic psychological and economic consequences, while
they were not sick and probably not contagious at all.
In France, the Centre National de Référence (CNR), the French Society of
Microbiology (SFM) continue to push Ct to 37 and recommend to laboratories to use only one gene
of the virus as a primer.
I remind you that from Ct 32 onwards, it becomes very difficult to culture the virus or to
extract a complete sequence, which shows the completely artificial nature of this positivity of
the test, with such high Ct levels, above 30.
Similar results were reported by researchers from the UK Public Health Agency in an article
published on August 13 in Eurosurveillance
: " The probability of culturing the virus drops to 8% in samples with Ct levels above
35." [23]
In addition, currently, the National Reference Center in France only evaluates the
sensitivity of commercially available reagent kits, not their specificity: serious doubts
persist about the possibility of cross-reactivity with viruses other than SARS-CoV-2, such as
other benign cold coronaviruses. [20]
It is potentially the same situation in other countries, including Belgium.
Similarly, mutations in the virus may have invalidated certain primers (genes) used to
detect SARS-CoV-2: the manufacturers give no guarantees on this, and if the AFP fast-checking
journalists tell you otherwise, test their good faith by asking for these guarantees, these
proofs.
If they have nothing to hide and if what I say is false, this guarantee will be provided to
you and will prove their good faith.
We must demand that the RT-PCR results be returned mentioning the Ct used because beyond
Ct 30, a positive RT-PCR test means nothing.
We must listen to the scientists and doctors, specialists, virologists who recommend the
use of adapted Ct, lower, at 30 . An alternative is to obtain the number of copies of viral
RNA/μl or /ml sample. [23]
We need to go back to the patient, to the person, to his or her clinical condition
(presence or absence of symptoms) and from there to judge the appropriateness of testing and
the best way to interpret the result.
Until there is a better rationale for PCR screening, with a known and appropriate Ct
threshold, an asymptomatic person should not be tested in any way.
Even a symptomatic person should not automatically be tested, as long as they can place
themselves in isolation for 7 days.
Let's stop this debauchery of RT-PCR testing at too high Ct levels and return to clinical,
quality medicine.
Once we understand how RT-PCR testing works, it becomes impossible to let the current
government routine screening strategy, inexplicably supported by the virologists in the safety
councils, continue.
My hope is that, finally, properly informed, more and more people will demand that this
strategy be stopped , because it is all of us, enlightened, guided by real benevolence and
common sense, who must decide our collective and individual destinies.
No one else should do it for us, especially when we realize that those who decide are no
longer reasonable or rational.
Summary of important points :
The RT-PCR test is a laboratory diagnostic technique that is not well suited to clinical
medicine.
It is a binary, qualitative diagnostic technique that confirms (positive test) or not
(negative test) the presence of an element in the medium being analyzed. In the case of
SARS-CoV-2, the element is a fragment of the viral genome, not the virus itself.
In medicine, even in an epidemic or pandemic situation, it is dangerous to place tests,
examinations, techniques above clinical evaluation (symptoms, signs). It is the opposite that
guarantees quality medicine.
The main limitation (weakness) of the RT-PCR test, in the current pandemic situation, is
its extreme sensitivity (false positive) if a suitable threshold of positivity (Ct) is not
chosen. Today, experts recommend using a maximum Ct threshold of 30.
This Ct threshold must be informed with the positive RT-PCR result so that the physician
knows how to interpret this positive result, especially in an asymptomatic person, in order
to avoid unnecessary isolation, quarantine, psychological trauma.
In addition to mentioning the Ct used, laboratories must continue to ensure the
specificity of their detection kits for SARS-CoV-2, taking into account its most recent
mutations, and must continue to use three genes from the viral genome being studied as
primers or, if not, mention it.
Overall Conclusion
Is the obstinacy of governments to use the current disastrous strategy, systematic screening
by RT-PCR, due to ignorance?
Is it due to stupidity?
To a kind of cognitive trap trapping their ego?
In any case, we should be able to question them, and if among the readers of this article
there are still honest journalists, or naive politicians, or people who have the possibility to
question our rulers, then do so, using these clear and scientific arguments.
It is all the more incomprehensible that our rulers have surrounded themselves with some of
the most experienced specialists in these matters.
If I have been able to gather this information myself, shared, I remind you, by competent
people above all suspicion of conspiracy, such as Hélène Banoun, Pierre Sonigo,
Jean-François Toussaint, Christophe De Brouwer, whose intelligence, intellectual honesty
and legitimacy cannot be questioned, then the Belgian, French and Quebec scientific advisors,
etc., know all this as well.
So?
What's going on?
Why continue in this distorted direction, obstinately making mistakes?
It is not insignificant to reimpose confinements, curfews, quarantines, reduced social
bubbles, to shake up again our shaky economies, to plunge entire families into precariousness,
to sow so much fear and anxiety generating a real state of post-traumatic stress worldwide, to
reduce access to care for other pathologies that nevertheless reduce life expectancy much more
than COVID-19! [24]
Is there intent to harm?
Is there an intention to use the alibi of a pandemic to move humanity towards an outcome it
would otherwise never have accepted? In any case, not like that!
Would this hypothesis, which modern censors will hasten to label "conspiracy", be the most
valid explanation for all this?
Indeed, if we draw a straight line from the present events, if they are maintained, we could
find ourselves once again confined with hundreds, thousands of human beings forced to remain
inactive, which, for the professions of catering, entertainment, sales, fairgrounds,
itinerants, canvassers, risks being catastrophic with bankruptcies, unemployment, depression,
suicides by the hundreds of thousands. [25-26-27-28]
The impact on education, on our children, on teaching, on medicine with long planned care,
operations, treatments to be cancelled, postponed, will be profound and destructive.
"We risk a looming food crisis if action is not taken quickly." [29].
It is time for everyone to come out of this negative trance, this collective hysteria ,
because famine, poverty, massive unemployment will kill, mow down many more people than
SARS-CoV-2!
Does all this make sense in the face of a disease that is declining, over-diagnosed and
misinterpreted by this misuse of overly sensitively calibrated PCR tests?
For many, the continuous wearing of the mask seems to have become a new norm.
Even if it is constantly downplayed by some health professionals and fact-checking
journalists, other doctors warn of the harmful consequences, both medical and psychological, of
this hygienic obsession which, maintained permanently, is in fact an abnormality!
What a hindrance to social relations, which are the true foundation of a physically and
psychologically healthy humanity!
Some dare to find all this normal, or a lesser price to pay in the face of the pandemic of
positive PCR tests.
Isolation, distancing, masking of the face, impoverishment of emotional communication, fear
of touching and kissing even within families, communities, between relatives
Spontaneous gestures of daily life hindered and replaced by mechanical and controlled
gestures
Terrified children, kept in permanent fear and guilt
All this will have a deep, lasting and negative impact on human organisms, in their
physical, mental, emotional and representation of the world and society.
This is not normal!
We cannot let our rulers, for whatever reason, organize our collective suicide any
longer.
Translated from French by Global Research. Original source: Mondialisation.ca
Dr Pascal Sacré is a physician specialized in critical care, author and renowned
public health analyst, Charleroi, Belgium. He is a Research Associate of the entre for Research
on Globalization (CRG)
****
Professionals whose references and comments are the basis of this article in its scientific
aspect (especially and mainly on RT-PCR):
1) Hélène Banoun
https://www.researchgate.net/profile/Helene_Banoun
PhD, Pharmacist biologist
Former INSERM Research Officer
Former intern at the Paris Hospitals
2) Pierre Sonigo
Virologist
Research Director INSERM, worked at the Pasteur Institute
Heads the Virus Genetics Laboratory in Cochin, Paris.
Participated in 1985 in the sequencing of the AIDS virus.
3) Christophe De Brouwer
PhD in Public Health Science
Honorary Professor at the School of Public Health at ULB, Belgium
4) Jean-François Toussaint
Doctor, Professor of Physiology at the University of Paris-Descartes
Director of IRMES, Institute for BioMedical Research and Sports Epidemiology
Former member of the High Council of Public Health
***
As
we first pointed out on Wednesday, Israel - which has been leading the world in the race to
vaccinate its entire (relatively small) population - is quickly learning that Pfizer's COVID-19
jabs
aren't nearly as effective as the 95% efficacy rate advertised via the Phase 3 trial
results released by the company and the FDA.
The chart below, first shared as part of Pfizer's Phase 3 trial data, suggested that there
might be a short delay before immunity begins in patients who received the vaccne.
However, in Israel, health experts revealed yesterday that the immunity provided by the
vaccine, especially during the initial weeks between the first and second dose, might be even
lower than all that.
Because on Wednesday, Dr. Nachman Ash, better known to some as "Israel's Dr. Fauci", said
the first batch of COVID jabs didn't increase immunity as much as they had hoped.
He told local media Army Radio that "many people have been infected between the first and
second injections of the vaccine," adding that It can take 10 days or more for the immunity to
kick in.
Of course, none of this is particularly unexpected. As
we first reported three weeks ago , local media in Israel reported that hundreds of
patients had been infected after receiving their first dose.
Israel also saw its fair share of patients with "adverse" health reactions,
with one doctor even passing away shortly after receiving the first dose , as the country
rushed to vaccinate its citizens with jabs that are still very much untested.
Meanwhile, in the US, Joe Biden and his administration are invoking wartime powers to secure
supplies of critical raw materials needed for vaccine production, as a recent logistical
slip-up ruined 21 shipments of the Moderna vaccine, forcing NYC to delay more than 20K jab
appointments.
iambrambles 3 hours ago (Edited)
I must be the only one who read the Pfizer BioNTech docs.
Out of around 30,000 people, half were given vaccines and half placebos.
In the placebo population of 15,000, something like 130 got COVID
In the vaccination population of 15,000, something like 20 got COVID
The 95% is a complete and utter fabrication, made by comparing that 20 to the 130.....out
of 30,000. We all know how Big PHarma cheats the system: they tailor the sample population.
For example, if the placebo population was 90% >50yo/10% <50yo, and the vaccination
population was 89% >50yo/11% <50yo, you would find that indeed, that 1% (150 people)
could easily swing the result, when the result is:
99.3% placebo didnt get covid
99.93% vaccinated didnt get covid
Pandelis 3 hours ago
if that was true, dr. faucistein would have noticed it ...
iambrambles 2 hours ago (Edited)
Re-read the study. It was 44,000, and in total, out of 44,000, 180 got COVID (150 placebo
to 30 vaccinated).
The first round of Pfizer vaccine was wholly ineffective, at 52%. They cherrypicked 94
individuals out of ths study to share the results, and after the second dose, the effectivity
rate was 92%.
So in all, I dont think anyone noticed how ridiculous this vaccine is in the first place:
if youre 99% likely to not even GET covid, why would you get a vaccine?
The second question is, why didnt Pfizer share results of specifically at danger groups,
like those 55+ or with pre-existing conditions?
And it was 44,000 people across 152 countries....so the results are simply too prone to
error to even be relevant. 44,000 and only 180 in total contracted COVID, how could you make
heads or tails of the data?
_arrow
xpxhxoxexnxixx 7 hours ago (Edited) remove link
The short answer to both of these questions regarding the COVID-19 'casedemic' and the
fallacy of asymptomatic PCR testing is YES and YES!
The only answer was always yes. No one should be surprised that everyone in the political
'health sector' managed to delay or ignore any real science , not in the name of the truth
mind you, but because of their opposition to the administration.
That's right, there's really no other way to put it. We had initial science, which in any
movie script would have been that one moment where the 'nobody' scientist gets called into
the Whitehouse to explain his life saving discovery. Instead, in our reality, those
scientists were ridiculed and told they were either wrong, or the science wasn't accurate
enough (never mind wanting to further support it so we could confirm or deny). These people
played games in hopes of running out the clock.
Put yourself in an alternate role- if you were in a position to make official guidelines
and recommendations and you realized there was science (mind you, people that spend their
careers doing this) that said 'there is a good probability that doing xyz will save a
life'..would you decide not to explore it? Would you decide not to share it with others?
Wonder what would have happened if let's say, the 'pandemic' would have occurred two years
into presidency instead of the last 3/4 of it. Just throwing that out there for thought.
Now, when the dust settles, suddenly the WHO, Fauci and everyone else is willing to admit
the science. I guess better late than never.
Give Me Some Truth 6 hours ago (Edited)
Plus, "new cases" are almost certainly going to plummet on their own . Reasons: We will
soon leave the "cold land flu" season, fewer people will be tested, and the number of people
who have already contracted the virus continues to grow. This means that the pool of people
who could test positive in the future will be much smaller (because people who have already
had the virus now have acquired natural immunity).
Bottom line: The coming huge decline in "new cases" will almost assuredly have nothing to
do with the number of people who have received both doses of the vaccine.
Demologos 6 hours ago remove link
Masks are great for spreading viruses and bacterial infections unless strict protocols are
followed. Remember last year when every news report on Covid ended with a segment on mask
hygiene and proper fitting? Me neither.
Ajax_USB_Port_Repair_Service_ 8 hours ago (Edited)
The CT will be lowered AFTER 100 days of masks and then the Biden miracle happens.
Luci Feric 8 hours ago
* miracle
You're welcome!
Luci
Ajax_USB_Port_Repair_Service_ 8 hours ago
Thank you Luci. I knew that didn't look right.
Luci Feric 8 hours ago
You're welcome!
karzai_luver 9 hours ago
The WHO/NIH/CDC are political grifters.
The leaderships are political hacks.
Why they still have any cred is unreal.
They have been late wrong and lie forever.
The examples are too numerous to post here.
dark pools of soros 9 hours ago
same reason people still eat fast food... the flashy marketing
crow1234 9 hours ago
Here's my surprised face 😮
F all this ****!
Give Me Some Truth 9 hours ago
Excellent analysis and kudos for highlighting the key role of the PCR tests in
establishing the narrative.
However, the key reason the PCR tests WILL be changed was not mentioned: This HAS to
happen to "prove" that the vaccines "work."
Once the PCR tests are changed, cases will plummet by 90 percent. The "miracle vaccines"
will get all the credit.
More importantly, by changing the PCR tests t his precludes the possibility of large
numbers of people "testing positive" AFTER receiving two doses of the vaccine. This would not
be good for the old credibility and trust of authorities and "public health officials" who
have been pushing mass vaccination.
P.S. I still wonder if the tens of thousands of people in the vaccine trial weren't tested
with PCR tests that had already been "adjusted." This would explain those "95 percent
effective" claims.
tangent 9 hours ago
That is likely all true, but it has the ridiculous flaw of people with the vaccine still
getting the same positive rates as those without the vaccine. Very funny! But then again,
people don't seem to snap into reality when they learn the population is still going up same
as last year and the year before that... very foolish thinking to think that is a
pandemic.
Notable quotes:
"... As a reminder, "cycle thresholds" (Ct) are the level at which widely used polymerase chain reaction (PCR) test can detect a sample of the COVID-19 virus. The higher the number of cycles, the lower the amount of viral load in the sample; the lower the cycles, the more prevalent the virus was in the original sample. ..."
Right On Cue For Biden, WHO Admits High-Cycle PCR Tests Produce COVID False Positives
BY TYLER DURDEN THURSDAY, JAN 21, 2021 - 6:30
Were the 'conspiracy theorists' just proven right about the "fake rescue plan" for
COVID? Did the 'science-deniers' just get confirmation that it was political after all ? The short answer to both of these questions regarding the COVID-19 'casedemic' and the
fallacy of asymptomatic PCR testing is YES and YES!
We have detailed the controversy surrounding America's COVID "casedemic" and the misleading
results of the PCR test and its amplification procedure in great detail over the past few
months. As a reminder, "cycle thresholds" (Ct) are the level at which widely used polymerase chain
reaction (PCR) test can detect a sample of the COVID-19 virus. The higher the number of cycles,
the lower the amount of viral load in the sample; the lower the cycles, the more prevalent the
virus was in the original sample.
Numerous epidemiological experts have argued that cycle thresholds are an important metric
by which patients, the public, and policymakers can make more informed decisions about how
infectious and/or sick an individual with a positive COVID-19 test might be. However,
as JustTheNews reports, health departments across the country are
failing to collect that data .
In fact, as far
back as October, we brought the world's attention to the COVID-19 "casedemic" and the
disturbing reality of high-cycle threshold PCR tests being worse than useless as indicators of
COVID-19 "sickness".
PJMedia's Stacey Lennox said at the time:
Biden will issue national standards, like the plexiglass barriers in restaurants he spoke
about during the debate, and pressure governors to implement mask mandates using the federal
government's financial leverage.
Some hack at the CDC or FDA will issue new guidance lowering the Ct the labs use , and
cases will magically start to fall.
In reality, the change will only eliminate false positives, but most Americans won't know
that.
Good old Uncle Joe will be the hero, even though it is Deep-State actors in the health
bureaucracies who won't solve a problem with testing they have been aware of for months. TDS
is a heck of a drug.
https://lockerdome.com/lad/13084989113709670?pubid=ld-dfp-ad-13084989113709670-0&pubo=https%3A%2F%2Fwww.zerohedge.com&rid=www.zerohedge.com&width=830
And now,
as Lennox explains in detail below, we have been proved 100% correct as less than one hour
after President Biden's inauguration, the WHO proved us right .
In August of last year, The New York Times published an article stating that as many as
90% of COVID-19 tests in
three states were not indicative of active illness . In other words, they were picking up
viral debris incapable of causing infection or being transmitted because the cycle threshold
(Ct) of the PCR testing amplified the sample too many times.
Labs in the United States were using a Ct of 37-40. Epidemiologists interviewed at the time
said a Ct of around 30 was probably more appropriate. This means the CDC's COVID-19 test
standards for the PCR test would pick up an excessive number of false positives. The Times
report noted the CDC's own data suggested the PCR did not detect live virus over a Ct of 33.
The reporter also noted that clinicians were not receiving the Ct value as part of the test
results.
Yet a PCR test instruction document from the CDC that had been revised five times as of July 13, 2020 ,
specified testing and interpretation of the test using a Ct of 40. On September 28, 2020, a
study published
in the journal Clinical Infectious Diseases from Jaafar et al. had asserted, based on
patient labs and clinical data involving nearly 4,000 patients, that a Ct of 30 was appropriate
for making public policy. An update to the CDC instructions for PCR testing from December 1, 2020 , still uses a
Ct of 40.
Shortly before the New York Times article was published, the
CDC revised its COVID-19 test recommendations , saying that only syptomatic patients should
be tested . The media went insane, and Dr. Fauci
went all over television saying he was not part of the decision to change the testing
standards:
"I am concerned about the interpretation of these recommendations and worried it will give
people the incorrect assumption that asymptomatic spread is not of great concern. In fact it
is."
So, of course, the Mendacious Midget™ had spoken, and the guidelines went back to
testing everyone, all the time, with an oversensitive test.
The idea that asymptomatic spread was a concern as of August was just one of many lies Dr.
Fauci told. At the beginning of the pandemic in late January, he said:
The one thing historically that people need to realize is that even if there is some
asymptomatic transmission, in all the history of respiratory borne viruses of any type,
asymptomatic transmission has never been the driver of outbreaks. The driver of outbreaks is
always a symptomatic person. Even if there is a rare asymptomatic person that might transmit,
an epidemic is not driven by asymptomatic carriers.
There is not a single study or meta-analysis that differs from Fauci's original
assessment.
Today, within an hour of Joe Biden being inaugurated and signing an executive order
mandating masks on all federal property, the WHO
sent out a notice to lab professionals using the PCR test . It said:
WHO guidance Diagnostic testing for SARS-CoV-2 states that careful interpretation of weak
positive results is needed ( 1 ).
The cycle threshold (Ct) needed to detect virus is inversely proportional to the patient's
viral load.
Where test results do not correspond with the clinical presentation, a new specimen should
be taken and retested using the same or different NAT technology.
literally one hour after Biden takes the oath, the WHO admits that PCR testing at high
amplification rates alters the predictive value of the tests and results in a huge number of
false positives pic.twitter.com/iDtXmappRw
-- Andy Swan (@AndySwan)
January 20,
2021
This translates to "in the absence of symptoms, a high Ct value means you are highly
unlikely to become ill or get anyone else sick in the absence of very recent exposure to an
infected person."
Dr. Fauci knew this in July when he said that tests with a Ct above 35 were likely
picking up viral debris or dead virus .
Even at a Ct of 35, the incidence of virus samples that could replicate is very low,
according to Jaafar et al.
The only state I know that requires reporting the Ct with every test is Florida,
which started this policy in December .
The WHO went on, stating:
Most PCR assays are indicated as an aid for diagnosis, therefore, health care providers
must consider any result in combination with timing of sampling, specimen type, assay
specifics, clinical observations, patient history, confirmed status of any contacts, and
epidemiological information.
In short, a positive PCR test in the absence of symptoms means nothing at a Ct of higher
than 30, according to the experts interviewed by the New York Times and according to Jaafar et
al. Yet positive tests is the number CNN loves flashing on the screen.
If the percentage found by the Times in August holds, there have been approximately 2.43
million actual cases to date, not 24.3 million.
There is also no way to calculate the deaths from COVID-19 rather than deaths with some dead
viral debris in the nostrils.
What I have referred to as the "casedemic" since September will be magically solved just in
time for Joe Biden to look like a hero. For doing absolutely nothing.
Do not tell me there is not a politicized deep state in our health agencies. Do not ever
tell me I need to listen to Dr. Anthony Fauci again. And every business owner who has been
ruined because of lockdowns due to a high number of "cases" should be livid. Any parent whose
child has lost a year of school should be furious.
None of this was for your health. It was to get rid of Orange Man Bad.
now they will drop the cycle rates and you can watch the curve go negative... like
magic... because the new magic man isn't the bad man and the masks he ordered
worked!!!!!
-- Andy Swan (@AndySwan) January 20,
2021
As an aside, this also clearly explains the disappearance of the "flu" during this season as
the plethora of high Ct PCR Tests supposedly pointing to a surge in COVID are nothing of the
sort.
As
Stephen Lendman noted previously , claiming "lockdowns stopped flu in its tracks,
(outbreaks) plummet(ting) by 98% in the United States" ignored that what's called COVID is
merely seasonal influenza combined with false positives (extremely high Ct) from PCR-Tests.
And for that reason, the great 2020 disappearing flu passes largely under the mass media's
radar. Media proliferated mass deception and the power of repetition get most people to believe
and having successfully "killed the flu", they will now do the same with COVID... and, if
allowed by our betters, we will all return to the new normal they desire.
Give Me Some Truth 5 hours ago remove link
The governor of Florida has proposed a law that is ingenious, or at least very important
(if passed). He simply wrote into his proposed bill that labs have to disclose the cT levels
in all "positive" COVID results.
He obviously put this language in the bill/regulations because he knew "public health
officials" would try to continue to conceal this information.
If this law is enacted, we will learn WHEN the PCR tests were adjusted . We will then be
able to see how the number of "positive cases" changes (read: declines significantly).
Here's hoping this law is enacted (with no loopholes) ... and that many more states enact
the same legislation.
philipat 9 hours ago
Loved that banner at the Vienna protest last weekend "Make Infuenza Great Again"
Fed-up with being Sick and Tired 7 hours ago
...The CT standards have been all over the place and inconsistent. It became quite clear
to my family and myself when we started readin: "ASYMPTOMATIC COVID cases surge" MONTHS
AGO!
The smartest little kid in our family, a young Girl at age 15 and is a BIG fan of Biology
and has decided that Virology will be her studies in college, said: "Daddy, is there a
disease if there are no symptoms?"
NO ONE AROUND THE TABLE had a clear answer. There were attempts and then the press started
talking: "YOU CAN CARRY COVID and not know it, so wear a mask!!!"
The ludicrous nature this entire charade started to unfold! SO, 40 degrees, you are not
stupid, just ignorant of the facts.
Go out and do your own homework before you continue to act like an expert in Virology. YOU
ARE NOT. We are all bystanders to a fraud perpetrated for nefarious reasons.
Boing_Snap 6 hours ago
Educated people know that these Tests were fake, the propaganda used was not for our
consumption, just the masses whom are only looking at headlines, which is the majority of
humanity.
Putting the manipulation of the tests together with a, heavens forbid a "Conspiracy
Theory", kept the indoctrinated away from looking at it. So now that is changing, good.
The Indoctrinated are most of the population, they range across the spectrum, scholars and
professionals included. Getting them to think for themselves will not be easy.
Oceania2020 6 hours ago (Edited)
Some of the dumbest words ever spoken...
"Google it".
checkessential 4 hours ago
At least FB and Twitter will prove that whatever you Google is true regardless of the
facts.
meowmix105 6 hours ago (Edited)
You imbicile, here's a link along with the first two paragraphs from article_
https://www.10news.com/news/local-news/san-diego-county-very-likely-flu-shots-covid-19-measures-keeping-influenza-cases-low
"So far this season, the county has recorded 39 influenza cases, compared to 1,220 cases
at this point last season. Flu season generally runs from October through May, with flu
activity peaking in December and February. The county says it's "very likely" physical
distancing, hand washing, and mask-wearing are contributing to the low flu activity".
As Fed-up with being Sick and Tired stated - you've got to be absolutely clueless and or
completely ignorant to not see these idiotic and contradictory statements by the San Diego
county health dept.....
When the noble coronavirus is the common flu virus to begin with! Yet, there's record
number of people getting covid all while having historically low cases of the flu _ thanks to
the masks! 🤯🤯 wake up ffs
xpxhxoxexnxixx 5 hours ago
So then how would you explain the inability for the WHO, Fauci and anyone else in that
club not using the publicly available data since April, as you said, and revising the way we
test and measure 'cases'? Biden would never go against the media lol so unless you have a
link gtfo.
MrBoompi 4 hours ago
This is a straw man argument. No diagnostic test like this is 100% accurate and nobody
would ever make such a stupid claim. But what if someone had, accurately, stated that the pcr
test is 5% accurate?
THIS IS TRUE
Ophiuchus PREMIUM 9 hours ago
Do you think they will admit Building 7 was a controlled demolition?
Dash8 6 hours ago
There's nothing left of it, it was all shipped to china with the rest of the
evidence...
Ophiuchus PREMIUM 9 hours ago (Edited)
Do you think they will admit that powerful politicians in America are controlled by sex
with young children?
They will never admit to anything.
All politicians in positions of power, rape and murder children. Lin Wood knows. Start
there.............
"Referring to Speaker of the House Dennis Hastert as a "serial child molester", a federal
judge imposed a sentence of 15 months in prison, two years' supervised release, and a
$250,000 fine. Hastert was imprisoned in 2016 and was released 13 months later." --- Why not
15 years? When politicians in D.C. get caught raping children, it's a slap on the wrist.
Suzy Q 8 hours ago
I have not researched this at all and cannot verify any of it, but here it is
https://steverotter.com/arrests-and-executions-of-famous-people-2020/
Except, I have looked at the part about wrinkled flags. I can only go so far down the
rabbit hole before I have to stop.
JRobby 7 hours ago (Edited)
Yea, just post it anyway. You are probably safe in a secure area.
There are at least 7 or 8 major Psy Ops running right now not to mention hundreds of minor
ones.
Suzy Q 2 hours ago
There are things that cannot be unseen and I'd prefer not to see those things.
daveO 30 minutes ago (Edited)
"G5 said many other people are going to face justice, but only one will have a public
trial -- John Brennan, the Anti-Trump American intelligence official who served as the
Director of the CIA from March 2013 to January 2017. He will have a public trial, and if
convicted, will be hanged."
If so, I hope the hanging is televised.
"Some find it difficult to believe that McCain and GHWB were executed. What is the point
of killing a dying person?
This would explain Beijing Biden's inauguration with 200K flags and no civilians.
Livingston 7 minutes ago
A Pay-Per-View of John Brennan being hanged would be a huge money maker. Could probably
balance the budget singlehandedly!
daveO 38 minutes ago
Bingo! It's why Hunter fled Delaware to marry a "movie producer" in May, 2019.
philipat 8 hours ago
No, that's not how these things work. You NEVER admit anything, just bury the facts,
censor as much as possible (to control the narrative) and stick to the official narrative
always no matter how discredited or ridiculous it may be. In fact, the strategy is "If you
can't win the debate don't have the debate".
And BTW, not only Building 7
Hal n back 7 hours ago (Edited)
Look at your car insurance card. After an accident, do not admit you were wrong.
for that, because of frivilous lawsuts there ends up being unnecessary settlement by
insurers to avoid trial.
the plaintiffs and attys usually avoid a counter suit so they have no problem
The legal system has many issues.
and congress has a lot of lawyers.
Dear Old Hedge 6 hours ago
And the others may have been George Lucas's Industrial Light & Magic, or Project Blue
Beam, or something related: https://newspunch.com/cia-pilot-presents-evidence-that-no-planes-hit-towers-on-911/
Would anything really surprise anyone at this point?
JethroBodine_ 5 hours ago (Edited)
Never ever believe anything the CIA says. Everything they say is a limited hangout.
Planes hit the towers but certainly were not the cause of three sky scrappers falling at
near free fall speed, symmetrically and into their own footprint.
That said, a jumbo jet did not hit the pentagon!
systemsplanet 8 hours ago
One day people who rushed out to inject the covid vaccine will begin to question what the
hell they just injected in their arm.
deadcat2 8 hours ago
The kind of sheep that do that are the sort that complain if there are no lamb chops for
dinner.
prairie oysters PREMIUM 7 hours ago
There is (I hope) a very clever metaphor buried in "lamb chops."
Giant Meteor 6 hours ago
Lambs get slaughtered .. eaten
Or placed in petting zoos
SwmngwShrks 5 hours ago
Its a Simpsons reference..."D'Oh!"
JRobby 7 hours ago
No THEY won't
EVER
Same reason they do this totally obvious $h!t.
GreatUncle 7 hours ago
We can only hope we get too hang people for the "intentional" 1st degree murder of
1000's.
Sick Monkey 7 hours ago
The flu is one of many infectious diseases. It's like we traveled through space and landed
on a planet that has only two infectious diseases. They focus on those two like some sort of
marketing campaign. A gold mine for big tech. Get your shot today! Call now and we'll throw
in another 2 of your choice. Buy one and get another two for free. Limited time offer.
Marla Singer 9 hours ago
When you think about the lengths the permanent fusion party had to go to to get their
candidate over the finish line: constant media bombardment against Trump, nation wide
lockdowns, social media blackouts, election fraud, false flag events, and a militarized
inauguration, I have to imagine it's a pretty fragile win.
camel717 6 hours ago
This is what I've been trying to tell people. After everything the democrats, celebrities
pandering, media etc. did to keep Trump out, as well as the mail in ballots (which, if didn't
happen, Trump would've won in a landslide) did to help Biden win, he barely ******* won. HE
BARELY WON.
It was made out to look like the entire world was against Trump and he still won sans
fraud and mail in ballots.
The future isn't as bleak as people think. There will be another red wave in 2022 I
suspect, unless mail ins continue to be the norm which democrats certainly will try because
it's their only path to victory at this point.
Iron Lady 1 hour ago
Xiden's inauguration video on commietube had 16,000 down votes and 4,000 up votes last I
checked. The views were very low.
Trump's farewell at Andrews had 800,000 views in real time at RSBN.
Cautiously Pessimistic 9 hours ago
It has not even been a full 24hrs since Biden was sworn in and already the shenanigans
have started. Once again, Trump, his administration and that small part of the press that
still has journalistic integrity is proven right. This was predicted. It will be interesting
to see what else moves from the conspiracy theory to the CONSPIRACY FACT column over the next
days and weeks.
Crash N. Burn 8 hours ago
Time to file a writ of quo warranto? From constitution.org :
" A writ of quo warranto is not a petition, but a notice of demand, issued by a demandant,
to a respondant claiming some delegated power, and filed with a court of competent
jurisdiction, to hold a hearing within 3 to 20 days, depending on the distance of the
respondant to the court, to present proof of his authority to execute his claimed powers. If
the court finds the proof insufficient, or if the court fails to hold the hearing, the
respondant must cease to exercise the power. If the power is to hold an office, he must
vacate the office.
The writ is unlike a petition or motion to show cause, because the burden of proof is on
the respondant, not on the demandant. "
Could be highly entertaining.
Ophiuchus PREMIUM 8 hours ago
It matters not as it will never be covered by the controlled media.
thunderchief 9 hours ago
Scamdemic. Enough said.
GreatUncle 7 hours ago
I prefer to view it as a tool.
The virus was intentionally released to create the desired effect and it was equally
useful to get rid of Trump at the same time.
Still think vaccine id - digital id - digital currency and the economic lock for the
globalists is the end game to usher in the great reset where everybody will be made a
slave.
Even now more and more Karen's are pushing for everybody to be forced vaccinated or
excluded from society where they will die a lingering economic death.
Walter Melon 7 hours ago
Up vote - who here knew this was going to happen a year ago?
AAA 7 hours ago
Not a whole year ago but atleast a couple of months :)
Hal n back 7 hours ago
It started when singapore reported its ct was 35. Not 40.
vealparm 1 hour ago
You can research my posts here....I was proclaiming the "ConVid-19 scam" way back in the
early spring.
I am 77 and have been around the block a few times with lying lawyers and politicians, I
called Fauci an actor/operative the second time I saw him and hear his spiel. The more I
learned about him and his past left me with no doubt.
We have all lived a dystopian tyranny for the past year engineered by world wide hard
Leftists.
Neil Patrick Harris 9 hours ago
Sure the timing is suspect but I doubt they will suddenly lift lockdowns and let us go
back to normal. This is about much more than removing Trump, it's The Great Reset.
Ophiuchus PREMIUM 8 hours ago
I call it the 'Great Extermination'.
Suzy Q 8 hours ago
de Blahsio is demanding NYC reopen, as if it was the business owners that demanded the
shut down. What a clown
philipat 8 hours ago
Yes agreed, Covid was a cover vehicle which allowed various different agendas to be
implemented simultaneously. Primarily the Global financial Reset. And since they are still
not ready with that, the covid scam will have to be extended for a good amount of time yet
(At least another 12-18 months). That is why the "beaking news" about mutations to more
deadly strains which will require new measures, new vaccines etc (Except that, just by magic,
the existing vaccines still work just fine against the existing mutations so the vaccination
campaign can continue. But they seemingly already are able to predict that the future mutant
strains will not and will require new vaccines. More gravy for big pharma, more controls
etc.)
Unknown User 1 hour ago
They want to issue electronic documents and money to control all movement and activity of
the entire world.
OutWithLibs 7 hours ago (Edited)
Passed a line of cars yesterday waiting for the control vaccine. No less than 4 miles
long, undoubtedly several hours in their cars. Upon completing errands I returned the same
way and the line was disbursing. Apparently the county ran out of shots. People are so scared
they'll wait in line for something that is not known to cure anything, caused death after
injection, invented faster than any vaccine in history and has never had trials. The control
is almost complete. Just add vaccination certificates to shop, buy gas, go see grandma, and
the communism will be complete.
CaMuPaSh 9 hours ago (Edited)
You know it's about over when:
Astra-Zeneca mfg. facility in India is burning down (today).
Astra-Zeneca mfg. facility in Wales is in danger of flooding (today).
Pfizer (a Rothschild Co. thanks to E. Macron) has fizzled.
Sputnik (RU) is being accepted by an increasing number of countries. EU, ME SA
Mutti Merkle is going for Sputnik.
...and the U.S.?
....a distant last.
The only thing selling in the ussa is masks (made in CN) for the next 100 days.
Oh, the days of reconciliation and roses are upon us with a vengeance.
Suzy Q 8 hours ago
Explosion
https://welovetrump.com/2020/12/23/unexplained-explosion-destroys-worlds-second-largest-hydroxychloroquine-raw-material-factory/
steve golf 8 hours ago
Who needs a vaccine really?
GreatUncle 7 hours ago
Not a vaccine more like gene therapy if it does not use any of the viral component in
it.
So you have the gene therapy but you will still catch the virus the intent is for your
body to have been mutated to switch on your immune system more violently to fight it.
Thing is that response is not going to be good for some folks as the response itself puts
pressure on your body just like the virus.
Virus does not kill you the symptomatic response does.
LA_Goldbug 6 hours ago
The lady's English is not perfect, but the information is very valuable,
https://www.bitchute.com/video/hvtMOdAKeAzh/
GoldmanSax 8 hours ago
We told you there was no pandemic. We kept reporting there were no deaths around us and
some posters kept arguing we were covid holocaust deniers. We were right and you were a shill
for an evil agenda.
The world is under attack. Most governments are onboard. Why do you need a vaccine
passport for a pandemic that never happened?
youngman 8 hours ago
because of the money involved.....billions of dollars for the drug companies
Bob Lidd 8 hours ago
it's all about control at this point.......
steve golf 8 hours ago (Edited)
fake vaccination certificates will be easy to print. Problem is getting it on the
database, if there is one, and there will be, but will airlines check the database or just
look at the certificate?
Cobb 8 hours ago
If only there was a digital certificate or better yet a way to insert a gel into the skin
that could provide pertinent data when scanned.
toejam 2 hours ago
What are you talking about? The vaccine is to kill or maim you. How is this not
understood?
pods 8 hours ago
Is anyone shocked? 100 days of diapers combined with a million or so vaccine shots and
voila, gone by spring.
Nobody will hang. The machine will roll on until the next financial blowup. Then probably
aliens will cause us to print 20 trillion more in debt.
We are Rome, circa 470 AD.
buzzsaw99 8 hours ago
Nobody will hang...
we might hang if we complain about it long enough.
Indelible Scars 8 hours ago
It's hard to believe that people are still falling for this AT ALL.
NIRP-BTFD 8 hours ago
Humanity reached peak stupidity.
AlphaDawg 8 hours ago (Edited)
Hands up, in Feb, March I was worried. An engineered P4 lab CCP virus.
By April, after saying wait for next 2 weeks a couple of times, I realised it was a
complete SCAM.
Not to mention the supression of Hydroxy and airports open.
GreatUncle 7 hours ago
Same ... the reality though never became what was being reported so by end of April I
started having very serious doubts over it. Then the more you learned it became to obvious
this was a hoax "lethal" virus although the virus may exist.
Then you find out that most who actually died were unfit overweight with existing medical
condition to me implies there is a virus but not dangerous to many people.
Now the majority of the population in society because of the Karen's are now incarcerated
by unfit overweight people with 2 or more comorbidities.
No-Go zone 6 hours ago
... that sheeple ...
Lanka 9 hours ago
The false positives of the PCR tests were known 6 months ago. Historically, ZH would have
reported that in timely fashion. Another failure of ZH, cow-towing to the MSM.
NIRP-BTFD 9 hours ago
ZH are opportunistic money makers. They got paid of to do covid propaganda early on.
deadcat2 8 hours ago
Not true. I've read number of articles on ZH saying the PCR test was producing false
positives and posters like me have been saying this from the very beginning. I suggest you
read Lew Rockwell's site if you want a really good insight into the covid farce.
BaNNeD oN THe RuN 6 hours ago (Edited)
There are multiple Tylers reporting multiple POVs.
There is "Wuhan Lab" Tyler, who was dominant at the start.
ImpliedVol 2 hours ago
ZH has been reporting on PCR tests. The first article about it was posted in March of
2020.
https://www.zerohedge.com/health/can-we-trust-covid-19-test-what-you-need-know-about-elisa-and-rna-tests
Try paying attention next time.
Mr. Belding 6 hours ago
masks stopped all other flu but not covid. It takes a ****** commie to believe that.
TRM 5 hours ago
It's the longer name man. You know that 0.1 micron "influenza" is stopped but the 0.1
micron "covid-19" isn't. It's all those extra letters in the name that masks, distancing
& lockdowns work on.
HANGTHEOWL 7 hours ago
"Were the 'conspiracy theorists' just proven right about the "fake rescue plan" for
COVID?"
We are not conspiracy theorists,,,we are people telling you the truth,,,,,,
Notice even when they have to admit we were right,,they try to demonize us at the same
time,,,,,,
uchibenkei 6 hours ago
yeah. were the conspiracy theorists right? why not ask "were the mainstreamers lying this
whole time?"
HANGTHEOWL 6 hours ago
egg-zactly,,,,,,
deadcat2 8 hours ago
I'm in the UK (a cesspit on the edge of Europe) and I've been asking from the start,
including emailing members of parliament, who decided that the PCR test should be amplified
45 times? Was it a government minister, some committee of scientists, or the laboratories
themselves? WHO MADE THE DECISION to amplify the PCR test 45 times and why? The creator of
the test, Kerry Mullis, stated that it should never be amplified more than 30 times. He even
said the PCR test wasn't suitable to test for an infection either.
Had the test been limited to 30 times, there would have been next to no 'cases' as they
are called and perfectly healthy people with no symptoms would not find themselves under
house arrest in their millions.
Stinkbug 1 8 hours ago
And where is Kerry Mullis now, when we need him? Dead. A couple of months after exposing
Fauci publicly, died at age 56 of 'pneumonia'.
Parasiticfilth 2 hours ago (Edited)
So if COVID is so contagious, why do they have to go all the way up your nasal cavity,
almost to your brain to get a sample?
Shouldn't there be samples everywhere?
I mean apparently the virus spreads faster than Kamala Harris' legs.
HANGTHEOWL 2 hours ago
That is just another part of this hoax that does not make sense,,,,,,if you dig into the
history of virology,,you find the same nonsense time and time again,,,,,take rabies for
instance,,,they say that rabies is transmitted by the saliva of the animal when it bites
you,,,,but they have to kill the animal and check the brain to actually see if it had
rabies,,,,,,why not just test the saliva,,,???,,why,,,??,,because rabies is just another
fraud,,,,
duck_fur 2 hours ago
I'd never put those two things together. You're right. Why not test the saliva since it
was the alleged vector of transmission? That really does not make sense.
HANGTHEOWL 1 hour ago
Many years ago,,I read an old study from some university they did back in the early
40's,,maybe even 30's,,,where they took the heads of dogs that had died from natural
causes,,and sent them in to be tested for rabies,,,,they came back positive,,,,it seems what
they test for in the brain as a marker for rabies,,,is also found in healthy brains,,,,,,it
is just another one of the fraud Louis Pasteur's scams,,,
duck_fur 2 hours ago
Hehe...that's funny right there. Upvote for you.
WesternCommunity 2 hours ago
Heels Up Harris. Pulled herself up by her kneepads, with the ugly looks like a polished
turd Willie Brown, Speaker of the Calffornia State Assembly.
Cobb 8 hours ago
Day 2 of Biden regime and he's still a huge POS.
Smokey PREMIUM 8 hours ago
Getting huger by the hour
Farmerz 6 hours ago
Trump was stupid not to fire this Fauci guy, another Clinton lapdog.
Eric Post 6 hours ago
Fauci is civil service, it doesn't not come under any president to fire him.
Farmerz 6 hours ago
We all read the tweets Fauci wrote "fawning" over Clinton here on ZH months ago. At
minimum, Trump could have brought out a different face explaining the test cycle standard the
CDC was using. Could have been mentioned at the debates. Wasn't.
Trump just didn't do his homework.
Iron Lady 1 hour ago
Please. If Trump had pushed back at all they would have just called him a science denier
like they do the rest of us.
Red Corvair 6 hours ago
Trump is not part of the establishment, but he was part of the game all along. He never
drained that swamp. And look and behold, that swamp is more alive and kicking than ever.
Hoss N. Pfeffer 4 hours ago
And now after defeating Trump the alligators are emboldened, aggressive, and hungry.
Everybody All American 6 hours ago
Dr. Fauci was brought to the fore by none other than Mike Pence I do beilieve.
Reaper 6 hours ago
Everything the government says is a lie.
Voice_of_Doom 6 hours ago
Just goes to show you the amazing power the globalist have and how well organized they
are.
LA_Goldbug 6 hours ago
They own the Media and the Politicians !!!!
scytalerules 6 hours ago
"globalists" "chicoms" lol
George Bayou 6 hours ago
They still can't prove effectiveness of masks but continue to swear by them.
convid21 7 hours ago
Even with a CT of 30, your still going to get 50% false positives
At 15 you'd get some Negatives but not many false Positives.
This test should not be used it's not accurate, not reliable and not fit for purpose.
It's doesn't have any science in it all.
The Governments are only using this to invoke fear in the Public by finding False
Positives.
In their view it's better to find more than less, and more leads to lockdowns which
demands a VAXX.
Which means the VAXX is a result of Fraud.
Pair Of Dimes Shift 7 hours ago
The nasal test is QUANTITATIVE not QUALITATIVE.
Completely useless for the application.
Even the antibody test isn't 100% because not everybody produces IgG all of the time when
an infection is present.
LA_Goldbug 6 hours ago
More about this here,
https://twitter.com/michaelmina_lab/status/1350162790569402368
T.Gracchus 1 hour ago
Covid 19 is not a disease, or a virus.
It is a political football.
Anyone who believes in it is a paid-for moron, or maybe just a common or garden idiot.
Obamanism666 2 hours ago
Start wearing the mask or 2 masks then go up to Karens and lambast them for only one mask.
The mask is also good for hiding your mouth when doing sheep sounds...... drive the Karens
crazy.
Made sheep sounds on the subway today, 5 People got really upset.
Could be even better that wearing a MAGA hat to trigger them.
If caught just say "well if I act like a sheep, I might as well sound like one"
WesternCommunity 1 hour ago
"Biiiddddeennnn!Biiiddddeennnn! Kaahhhhmmmaaallllaaaaa...."
Dogspurt 1 hour ago
Go lick the live rail, dumbass!
Tigbits 1 hour ago
You appear to be the last remaining covidtard troll in the group downvoting everyone.
Soon, you will be out of a job trolling on here. 🤣🤣🤪🤪
Klaus Smith 6 hours ago
Creepy Joe just inaugurated and Covid disappears. YES! That's the hero we need! Hail
Biden!
Space-Time Continuum 7 hours ago (Edited)
All thanks to the most popular president of all times, as we've seen all those million
people there at the inauguration cheering for him.
Pro_sanity 1 hour ago
It still sucks to be vindicated. Plus it was so obvious. Anyone who didn't see through
this from very early on is a total nit wit who shouldn't be allowed to even drive a car.
Shirley Yugest 6 hours ago
There is no covid-19 pandemic. There is only covid-19 panic. The reason for this is the
"DEM" in panDEMic is now in the WH.
9-Month Cycle 7 hours ago
We knew that last year. The inventor himself let everybody know what was up with AIDS
testing in Africa years ago. Run it over and over and over and everybody is positive.
Come on, man!! David Icke.... Alex Jones..... do you not gather information online? Only
watch the boob tube?
Pair Of Dimes Shift 7 hours ago
Welcome to what some of us knew 6 months ago, normie sheep!
vk
149
Health workers refusing vaccine is new growing US problem
According to a recent Kaiser Family Foundation poll, 29 percent of those who work in a
health care delivery setting said they would probably not, or definitely would not, take
the vaccine, even if it were free and deemed safe by scientists.
Experts say the reasons for vaccine hesitancy among health workers are similar to
concerns held by the general population, including worries about potential side effects.
Some may also be taking a wait-and-see approach to find out how the vaccine affects people
who take it earlier.
"I am definitely concerned that health care workers are electing to wait to get
vaccinated," said Nancy Messonnier, director of the CDC's National Center for Immunization
and Respiratory Diseases.
Those healthcare workers know their system. They're not stupid.
vk
110
Hacked emails
allegedly detail how EU drug regulator was pressured to approve Pfizer jab despite 'problems'
with the vaccine
vk
111
In the article @ 109:
According to Le Monde, the hacked documents primarily detail issues that the EMA had with
the Pfizer/BioNTech drug. The regulator apparently had three "major issues" with the
vaccine: certain manufacturing sites used for its production had not yet been inspected,
data on batches produced for commercial use were still missing, and, most importantly,
available data revealed qualitative differences between the commercial batches and those
used during clinical trials.
Those worries confirm my fears over those mRNA vaccines: there's an abyss that separates
theory from practice, and another abyss after that that separates practice from
manufacturing, in medical/biological sciences. The human body is not your average machine: it
is millions of times more complex.
And those worries are purely practical. Even the theory behind the mRNA therapy/vaccine is
still far from complete; the field of epigenetics is still very young, a little more than ten
years old, and there's a lot to investigate.
gm , Jan 18 2021 16:46 utc |
101
Re: vk | Jan 18 2021 12:58 utc | 89
Moderna and Pfizer mRNA products UNDER US Law, are mislabeled; they do not fit the legal
definition for being vaccines.
They are *experimental synthetic gene therapy/chemotherapy agents*, according to this
MD/JD person:
https://www.bitchuteDOTcom/video/AuvhMTMoby41/
( Replace "DOT" with "." in link)
And Pfizer is being sued for using the patented fluorescent 'reporter gene' *mNeonGreen*
in their mRNA drug process w/o being licenced.
Their first about PcR tests pretty educational.
Gaius_Marius 2 days ago 14 Jan, 2021 01:32 PM
No proof that those deaths were solely attributed to a respiratory virus. It is suspected at
best.
Ellen77 Gaius_Marius 2 days ago 14 Jan, 2021 09:08 PM
The portuguese court ruled that When running PCR tests with 35 cycles or more – the
accuracy dropped to 3%, meaning up to 97% of positive results could be false positives.
AwareAussie Gaius_Marius 2 days ago 14 Jan, 2021 05:09 PM
But there is proof that_death_stats have been_faked, that the_alleged virus is not
as_dangerous as they promote, that_there is another_agenda behind_lockdowns, etc etc. I also
suspect that this crazy_boss_story is another bigpsyop, as it would likely be an exceedingly
rare event to take measures such as those mentioned. In any case I'd_quit on the_spot if any
employer tried that with me.
oddthinker 2 days ago 14 Jan, 2021 02:14 PM
Nuremburg Code provisions of informed consent are international law. Neither government
bodies and agencies, or private and public employers may coerce you into accepting the role
of a long term trial subject for an experimental drug. Agency and free will is yours to
refuse that drug.
AMstone oddthinker 2 days ago 14 Jan, 2021 11:32 PM
Unit 731 was never disbanded, just relocated.
V.B. 2 days ago 14 Jan, 2021 08:53 PM
the covid hoax is absolute madness, it must be stopped, it's rapidly spiraling into something
worse than north korea, worse than worst sharia countries, people are losing all their
freedoms, are being fined massively for noncrimes, medical experiments are done on people
without their full consent, how this madness can go on for this long is beyond me, are people
really that dumb? This isn't black death, it isn't even remotely close, some very old, very
sick people probably died a few month earlier, yes it's bad, no it's not excuse to destroy
world, kill economies, stop all other medical care - measures that will kill way more than
covid-19(84) ever will Average covid victim in UK is 82.4 year old, and that's above average
life expetency in UK, according to many studies anywhere between 96 and 99% of people who
supposedly died of covid had co-morbidities - meaning they were seriously sick even before
catching it It's absolute farce, and the biggest hoax, biggest evil joke in history. Besides
they tried it before in 2009 with the swine flu, it was very much similar to this, there was
also rushed vaccine that had bad side effects, massive corruption that enabled it got exposed
and it faded into obscurity but people never learned.
V.B. V.B. 2 days ago 14 Jan, 2021 09:00 PM
You should present facts to all your mоrоn friends who still support this hoax,
if they can't make a case for their support (which is not possible if you follow all facts
anyway) - and they still refuse to admit they are wrong then stop talking to them, you are
indirectly helping to support this hoax by being friends and supporting people who support
useless and harmful covid measures like lockdowns and masks, sacrafices must be made
otherways you will lose all, you are already losing all, you can't even meet thos
іdіоts anymore in much of the Western world and beyond with all the curfews
and ban on visits. I am already doing the very thing - I presented clear facts, clear logic
to one of my long term half-friends and he refused to budge even one inch, all his arguments
boiled down to calling me 'conspiracy theorist' and refusing to even admit possibility that
goverments might have gone rogue or fallen for the hoax themselves. However during the
discussion I uncovered that he is a secret leftist, he never talked about his political
views, but this discussion forced out certain facts that revealed that he has leftist
poltical views despite being reasonably wealthy bussinessman, and you would think it's the
proletariat that support socialism...
SavantMan 2 days ago 14 Jan, 2021 04:59 PM
We need to instill fear in the people who make these decisions. I think the time has come for
there to be actual repercussions for these pieces of you know what.
AwareAussie SavantMan 2 days ago 14 Jan, 2021 05:22 PM
The solution is both peaceful and lawful. Revert back to common law (the highest laws of the
lands edit: dating back to the Magna Carta), convene common law courts and juries, and hold
those traitors and criminals accountable. This is what happened in the last American civil
war, but it is well hidden. It is coming back now very fast. Research it and get on board
right now.
HappyBag 2 days ago 14 Jan, 2021 08:08 PM
I read that about the plumbing firm, well that's easily resolved, the plumbers can go self
employed. I would certainly never work for an employer that dictated my health or demanded my
records. Then the public can then make their own choice on who does their work - a barmy boss
who dictates mandatory vaccinations (what next, no smokers and nobody who has the odd beer?),
or a normal person?
vk
9
19% or 95%?
US expert challenges Pfizer vaccine's efficacy, triggers debates in China
Authored by John Hunt, M.D. via InternationalMan.com,
In the setting of COVID-19, almost every country in the world closed its borders, locked
down its citizens, and forced businesses to close. Today, most governments still restrict
travel, economic activity, and social gatherings.
The justification for these unprecedented measures has been a growing number of COVID-19
cases. This has unleashed an epidemic of COVID testing - with PCR and rapid antigen tests as
the means of identifying positive COVID cases. Our very own Dr. John Hunt examines the science
behind COVID testing, whether the testing paradigms are effective, and the rationality behind
government response to the virus.
What COVID tests mean and don't mean
RT-PCR tests can be designed to be highly sensitive to the presence of the original viral
RNA in a clinical sample. But a highly sensitive test risks poor specificity for actual
infectious disease.
Rapid antigen tests are different. They measure viral protein. They do so by reacting a
clinical sample with one or two lab-created antibodies that are labeled with a measurable
marker. These antigen tests are often poorly specific, meaning they can show as positive in the
absence of any actual viral protein or any COVID disease.
For a lab test, what does it
mean to be sensitive ? What does it mean to be specific ?
I'll use COVID to help explain these terms. In order to do this correctly, we need to avoid
using the language of the media and government because those institutions tend to mislead us
via language manipulation. For example, they've wrongly taught us that a COVID-positive test is
synonymous with COVID- disease. It isn't, as you will soon see.
So for this article, I will use the term "Relevant Infectious COVID Disease" to mean a
condition, caused by COVID-19, in which a patient is sickened by the virus or has (in their
airways) living replicating virus capable of being transmitted to others. This seems a fair
definition of what we should be caring about in this disease. If the patient isn't sick and
isn't capable of transmitting the disease, then any COVID RNA or protein that may appear in a
test is not relevant, nor infectious, and therefore of little to no consequence.
about:blank
me title=
You can think of a test's sensitivity like this: In a group of 100 people who absolutely
have Relevant Infectious COVID Disease, how many people does the test actually report as
"positive?" For a test that is 95% sensitive, 95 of these 100 patients with the true disease
will be reported by the test as COVID positive and 5 will be missed.
Specificity : In a group of 100 people who absolutely do not have Relevant Infectious COVID
Disease, how many will be reported by the test as "negative?" For a test that is 95% specific,
95 of these healthy people will be reported as COVID-negative and 5 will be incorrectly
reported as COVID-positive
Sensitivity and Specificity are inherent characteristics of a test, not of a patient, not of
a disease, and not of a population. These terms are very different than Positive Predictive
Value (PPV) and Negative Predictive Value (NPV). PPV and NPV are affected not only by the
test's sensitivity and specificity but also by the characteristics of the people chosen to be
tested and, particularly, the patients' underlying likelihood of actually having true Relevant
Infectious COVID Disease. The Positive Predictive Value -- the chance a positive test actually
indicates a true disease -- is greatly improved if you test people who are likely to have
COVID, and, importantly, avoid testing people unlikely to have COVID.
If you do a COVID test with 95% sensitivity and 95% specificity in 1,000 patients who are
feverish, have snot pouring out of their noses, are coughing profusely, and are short of
breath, then you are using that test as a diagnostic test in people who currently have a
reasonable up-front chance of having Relevant Infectious COVID Disease. Let's say 500 of them
do actually have Relevant Infectious COVID Disease, and the others have a common cold. This 95%
sensitive test will correctly identify 475 of these people who are truly ill with COVID as
being COVID-positive, and it will miss 25 of them. This same test is also 95% specific, which
means it will falsely label 25 of the 500 non-COVID patients as COVID-positive. Although the
test isn't perfect it has a Positive Predictive Value of 95% in this group of people, and is a
pretty good test overall .
But what if you run this very same COVID test on everyone in the population? Let's
guesstimate that the up-front chance of having Relevant Infectious COVID in the US at this
moment is about 0.5% (suggesting that 5 out of 1000 people currently have the actual
transmittable disease right now, which is a high estimate). How does this same 95%
sensitive/95% specific test work in this screening setting? The good news is that this test
will likely identify the 5 people out of every 1000 with Relevant Infectious COVID! Yay! The
bad news is that, out of every 1000 people, it will also falsely label 50 people as
COVID-positive who don't have Relevant Infectious COVID. Out of 55 people with positive tests
in each group of 1000 people, 5 actually have the disease. 50 of the tests are false positives.
With a Positive Predictive Value of only 9%, one could say that's a pretty lousy test. It's far
lousier if you test only people with no symptoms (such as screening a school, jobsite, or
college), in whom the up-front likelihood of having Relevant Infectious COVID Disease is
substantially lower.
The very same test that is pretty good when testing people who are actually ill or at risk
is lousy when screening people who aren't.
In the first scenario (with symptoms), the test is being used correctly for diagnosis. In
the second scenario (no symptoms), the test is being used wrongly for screening .
A diagnostic test is used to diagnose a patient the doctor thinks has a reasonable chance of
having the disease (having symptoms like fever, cough, a snotty nose, and shortness of breath
during a viral season).
A screening test is used to check for the presence of a disease in a person without symptoms
and no heightened risk of having the disease.
A screening test may be appropriate to use when it has very high specificity (99% or more),
when the prevalence of the disease in the population is pretty high, and when there is
something we can do about the disease if we identify it. However, if the prevalence of a
disease is low (as is the case for Relevant Infectious COVID) and the test isn't adequately
specific (as is the case with PCR and rapid antigen tests for the COVID virus), then using such
a test as a screening measure in healthy people is forcing the test to be lousy. The more it is
used wrongly, the more misinformation ensues.
Our health authorities are recommending more testing of asymptomatic people. In other words,
they are encouraging the wrong and lousy application of these tests. Our health officials are
doing what a first-year medical student should know better than to do. It's enough of a
concerning error that it leaves two likely conclusions:
1) that our leading government health officials are truly incompetent and/or
2) that we, as a nation, are being intentionally gaslighted/manipulated. Or it could be
both.
(Another conclusion you should consider is that my analysis of these tests is incorrect.
I'm open to a challenge.)
So what if you, as an individual, get a positive PCR test result (one that has 95%
specificity) without having symptoms of COVID-19 or recent exposure to a true Relevant
Infectious COVID Disease patient? What do you do? Well, with that positive test, your risk of
having COVID has just increased from less than 5 in 1,000 (the general population risk) to
about somewhere perhaps 5 in 55 (the risk of actual Relevant Infectious COVID Disease in
asymptomatic people with a COVID-19-positive test). That's an 18-fold increase in risk,
amounting to a 9% risk of you having Relevant Infectious COVID Disease (or a 91% chance of you
being totally healthy). That may be a relevant increase in risk in your mind, enough that you
choose to avoid exposing your friends and family to your higher risk compared to the general
population. But if the government spends resources to contact-trace you, then they are
contact-tracing 91% of people uselessly. And they are deciding whether to lock us down based on
the wrong notion that COVID-positive tests in healthy people are epidemiologically accurate
when indeed they are mostly wrong.
For the 50 asymptomatic low-risk people falsely popping positive out of each group of 1,000,
what makes them pop positive? For a rapid antigen test, it is because the test is never meant
for use as a screening test in healthy asymptomatic people because it's not specific enough.
For a PCR test, positivity confidently means that there was COVID RNA in that sample, sure, but
your nose or mouth very likely just filtered some dead bits of viral debris from the dust
particles in the air as you walked through CVS to get the test before you learned you were
supposed to use the drive-through. PCR can be way too sensitive.
A few strands of RNA are irrelevant. Even a few hundred fully intact viral particles are not
likely to infect or cause disease. Humans aren't that wimpy. But keep in mind that there is a
very small chance that the test popped positive because you are about to get sick with
COVID-19, and the test caught you, by pure luck, just before you are to become sick.
On top of this wrong use of diagnostic tests as screening tests, the government has been
subsidizing hospitals for taking care of COVID-19-positive patients. Let's say a hospital
performs a COVID test 4 times during a hospital stay as a screening test in a patient who has
no symptoms of COVID. If that test pops positive once and negative three times, the hospital
will report that patient as having COVID-19, even though the one positive result is highly
likely to have been a false positive. Why do hospitals do this testing so much? In part,
because they'll get $14,000 more from the government for each patient they declare has
COVID-19.
When we see statistics of COVID-19 deaths, we should recognize that some substantial
percentage of them should be called "Deaths with a COVID-19-positive test." When we see reports
of case numbers rising, we should know that they are defining "case" as anyone with a
COVID-19-positive test, which, as you might now realize, is really a garbage number.
Summary:
We have an epidemic of COVID-positive tests that is substantially larger than the
epidemic of identified Relevant Infectious COVID Disease. In contrast, people with actual,
mild cases of COVID-disease aren't all getting tested. So the data, on which lockdowns are
supposedly justified, are lousy.
The data on COVID hospitalizations and deaths in the US are exaggerated by a government
subsidization scheme that incentivizes the improper use of tests in people without
particular risk of the disease.
Avoid getting tested for COVID unless you are symptomatic yourself, have had exposure to
someone who was both symptomatic and tested positive for COVID, or have some other personal
reason that makes sense.
Know that getting tested before traveling abroad puts you at a modest risk of getting a
false-positive test result, which will assuredly screw up your trip. It's a new political
risk of travel.
There is a lot more to this viral testing game, and there are a lot of weird incentives.
There are gray areas and room for debate.
Yes, the COVID disease can kill people. But a positive test won't kill anybody. Sadly,
every COVID-positive test empowers those politicians and bureaucrats who have a
natural bent to control people -- the sociopaths and their ilk.
* * *
John Hunt, MD is a pediatric pulmonologist/allergist/immunologist, a former tenured
Associate Professor and academic medical researcher, who has extensive experience and
publications involving PCR, antigen testing, and analysis of respiratory fluid. He is
internationally recognized as an expert in aerosol/respiratory droplet collection and analysis.
He's also Doug Casey's coauthor for the High Ground novels Speculator, Drug Lord, and the just-released
Assassin , and he is a founding member of the LLC that owns International Man.
* * *
Unfortunately, most people have no idea what really happens when a government goes out of
control, let alone how to prepare How will you protect yourself in the event of an economic
crisis? New York Times best-selling author Doug Casey and his team just released a guide that
will show you exactly how.
Click here to download the PDF now .
Stonebird , Jan 10 2021 17:23 utc |
17
First, the funniest comment I have seen for a long while (Elijah Magnier)
https://twitter.com/ejmalrai/status/1347926280864473088/photo/1
------Two things I would like information or opinion on are as follows;
In France, those that are about be vaccinated by Pfizer must sign a legal form that is 56
pages long (not a joke ! - Including by seniors with pre or declared-alzheimers), which, I
presume, covers all possible forms of immunity for Pfizer, and unwanted side effects,
expected or not. BUT does this "form" have hidden traps? One possible trap is that the French
Government have signed one of the secret "accords" that give big Pharma the "right" (ability)
to sue the French or other Governments if for any reason they do not make the profit they
"expected or wanted" to make.
The Governments concerned will have to make up any shortfall. even if due to popular
pressures on the Gov. The "settlement" was to be overseen by an ISDN (arbitration) tribunal.
Whose three members were taken from 15 US law firms specializing in Company (Corporate) law,
even if one nominally was supposed to represent the Government. No input from "other
interested parties" was to be allowed, and deliberations and names of "Lawyers" were also to
be kept secret.
This was one part of the Trade "agreement" on services. The one which was to be kept
secret for five years and those signing it to remain anonymous. Was it in fact signed?
Was it in fact signed by other Governments as well. This would go a long way to explain the
obsessions by some Ministers to force vaccinations against common sense. (on children
etc)
gm , Jan 10 2021 17:16 utc |
16
This is just one individual case; but the condition is so rare that it does require
independent investigation about potential side effects of the vaccine. Is immune
thrombocytopenia one of them ?
https://www.news4jax.com/news/florida/2021/01/08/miami-beach-doctors-death-after-covid-19-vaccine-under-investigation/
MIAMI BEACH, Fla. – Questions remain in the death of a 56-year-old Miami Beach doctor
who died Sunday, just a little over two weeks after receiving the COVID-19 vaccine, our
sister station WPLG-TV in Miami reported.
Gregory Michael, M.D., whose website states he was in private practice in obstetrics and
gynecology at Mount Sinai Medical Center, received the vaccine at the hospital where he was
affiliated on Dec. 18.
It is not clear, however, if the 56-year-old doctor's death is related to the shot, but
an investigation is underway.
A Facebook post by Michael's wife described him as "very healthy." His website said he
was an avid tournament and big game fisherman and also a rescue certified scuba diver.
His wife said that three days after getting the shot, Michael noticed severe broken
blood vessels on his feet and hands, prompting him to go the emergency room.
There, he was diagnosed with immune
thrombocytopenia
She said her husband was an advocate of the vaccine.
A spokesperson from Mount Sinai, who cited patient privacy restrictions, said in a
statement:
"To the extent that we are aware of an incident involving any patient, the appropriate
agencies are contacted immediately and have our full cooperation."
Florida's Department of Health confirmed that they referred the case to the Centers for
Disease Control for investigation. A CDC spokesperson told Local 10 News that "they will
evaluate the situation as more information becomes available and provide timely updates on
what is known and any necessary actions."
* When immune system attacks/destroys platelet cells in the blood
More Here:https://www.the-sun.com/news/2105759/dr-gregory-michael-miami-coroanvirus-vaccine-dead/
gm , Jan 10 2021 19:27 utc |
38
Re: "I have what I suppose to be a foolish question about the Pfizer vaccine, which in
order to remain viable has to be kept in an extreme frozen condition until being used. The
question is, what happens to the vaccine as it is brought to human body temperature, (which
is, I assume, what must be done before it can be safely injected)?"
-juliania | Jan 10 2021 18:03 utc | 21
Not a foolish question at all--and not one that I have yet heard any of the Holy Annointed
Vessels of Covid Science TRUTH (ie Dr. 'Gain of Function' Fauci, Bill Gates et al) give an
understandable explanation for.
Speaking purely from the perspective of someone with technical background in the
chemistry/medical fields and having no direct insider info about the Pfizer mRNA vaccine
specifically,
the vaccine's Spike protein coding mRNA 'payload' must be packaged inside a protective
"liposome" a synthetic lipid bi-layer vesicle.
The liposome protects the mRNA payload from being chewed up/destroyed while it is still in
the extracellular space (blood plasma, lymph etc) by plasma nucleases before the spike mRNA
is able reach and enter the body's cells where it is then replicated and translated into
(antigenic [immune system recognizing/inducing]) viral spike proteins.
The RNA-liposome vesicles have a limited stability at room temperature in aqueous saline
conditions, and an even shorter half-life in the blood stream at body temperature. They are
most stable when keptvery cold in deep freeze <~70 degree C) with some physiologically
compatible "antifreeze" (eg polyethylene glycol, polypropylene glycol, or syrupy sugar-like
mixtures) that keep liposome-disrupting ice crystals from forming during the deep freeze
storage temps.
Now to address your question, my guess is the reconstitution procedure is to bring the
antifreeze-stablized -70C vaccine vials to >0 degrees C, and then add physiological
saline, and then inject within the protocol-defined stability-safe time range.
Gwyn
An interview with Professor Dolores Cahill about the potentially lethal effects of mRNA
vaccines:
https://thewallwillfall.org/2021/01/07/why-people-will-start-dying-a-few-months-after-the-first-mrna-vccines/
Cal
Mike Ellwood (Oxon UK)
George Mc
I presume that people who get the vaccine(s) will then start testing positive with the PCR
test, if they are tested soon afterwards, or even some time afterwards. And so they should,
really, since, in a sense, they have been "infected" with some version of the so-called
virus. At least that's more or less how vaccination is supposed to work, isn't it?
If that does start happening, I will be fascinated (in a blackly comic way) to see the
official reaction. I think it's all going to go very pear shaped (even more than it is now),
in ways we probably can't begin to imagine yet.
Notable quotes:
"... A risk reduction of 0.84%. Oh! A barely perceptible "efficacy." ..."
"... An analysis of available positive RT-PCR tests and mortality results led the Oxford Centre for Evidence Based Medicine estimated a very tentative COVID 19 Case Fatality Rate (CFR) of around 1.4%. Based upon the figures reported to the FDA by Pfizer and BioNTech, this indicates a broad population based mortality risk from COVID 19 of 1.4(0.88/100) which is 0.012%. ..."
"... If we look at the "V-Safe Active Surveillance for COVID 19 Vaccines" reported by the U.S. Center For Disease Control (CDC), early indications of the recorded "Health Impact Events" (HIE) reveal a worrying level of adverse reactions from the mRNA vaccine. The CDC define an HIE as: ..."
"... On December the 18th 112,807 people were injected with the Pfizer/BioNTech vaccine in the U.S. Of these, 3,150 were subsequently unable to perform normal daily activities, unable to work, required care from doctor or health care professional . This is an HIE rate of 2.8%. ..."
"... This suggests that among the first 10 million people to receive the vaccine in the UK, around 280,000 may find themselves unable to perform normal daily activities, unable to work and require medical care as a result. As it is the most vulnerable who are the first to receive this vaccine, given the tiny risk of mortality from the COVID 19 disease, it is by no means clear that this is a risk worth taking. ..."
"... The obvious problem with these vaccines, is that no reliable fit for purpose diagnostic test exists as of this moment. As far I know, no one in power is even talking about any need for an effective test. How are they able to prove that a vaccine is effective without a reliable, valid test? ..."
"... Rahm Emmanuel said "never let a crisis go to waste". Crisis do not need to be real motivate the necessary panic for a change. ..."
"... What is the evidence so far on side effects and long-term effects of Covid vaccinations? Obtained in half a year on test subjects and within a week on nursing home residents? ..."
OVID 19 vaccine trials appear to have caused some confusion. Hopefully, this article might
help clear things up a bit. People genuinely appear to believe that the COVID 19 vaccines have
undergone clinical trials and have been proven to be both safe and effective. That belief is
simply wrong.
The main point is this. If you decide to have Pfizer and BioNTech's experimental mRNA-based BNT162b2 (BNT) vaccine, or any other
claimed COVID 19 vaccine for that matter, you are a test subject in a drug trial.
The mRNA in the BNT vaccine was sequenced from the 3rd iteration of the original WUHAN
published Genome SARS-CoV-2 (MN908947.3). However, the WHO protocols Pfizer used to produce the
mRNA do not appear to identify any nucleotide sequences that are unique to the
SARS-CoV-2 virus. When
investigator Fran Leader questioned Pfizer they confirmed:
The DNA template does not come directly from an isolated virus from an infected
person.
Nor are there any completed clinical trials for these vaccines. Trials are ongoing. If you
are jabbed with one, you are the guinea pig. This may be fine with you but it's not a leap of
faith I or my loved ones wish to take. However, everyone is different.
On December the 8th the BBC reported
a study in the Lancet and categorically stated:
The Oxford/AstraZeneca Covid vaccine is safe and effective, giving good protection,
researchers have confirmed
The BBC had no justification to make this claim. The
study in the Lancet did not confirm anything of the sort. The researchers wrote:
ChAdOx1 nCoV-19 has an acceptable safety profile and has been found to be efficacious
against symptomatic COVID-19 in this interim analysis of ongoing clinical trials.
This was an interim analysis funded by, among others, CEPI and the Bill and Melinda
Gates Foundation. The analysis was based upon trials which are years from completion and
haven't reported anything. The researchers also stated:
There were no peer-reviewed publications available on efficacy of any severe acute
respiratory syndrome coronavirus 2 (SARS-CoV-2) vaccines
There is no clear scientific evidence establishing either the safety or efficacy of proposed
COVID 19 vaccines. The BBC and other MSM reports that this evidence exists are false.
We are going to focus on Pfizer and BioNTech's BNT vaccine but all the manufacturers have
essentially exploited the same trick. The regulators and governments have worked with the
pharmaceutical corporations to conflate the limited data from the initial, or phase one, trials
with the incomplete and ongoing data collection from the substantially larger phase two and
three trials. The MSM have then falsely claimed the 1,2,3 phase trials are complete and
insinuated that the untested data demonstrates vaccine efficacy and safety.
In reality, not only has the reporting of existing data been manipulated to show efficacy
that isn't evident in the raw data itself, the most important and meaningful phases of the
trials have barely begun, let alone been completed.
Recently the UK Financial Times
reported that the UK regulators (the MHRA) are due to approve Astrazeneca/Oxfords AZD1222
[ChAdOx1] COVID 19 Vaccine. The FT revealed an anonymous statement from the UK Department of
health:
The medicines regulator is reviewing the final data from the University of
Oxford/AstraZeneca phase 3 clinical trials to determine whether the vaccine meets their
strict standards of quality, safety and effectiveness.
Thus giving the public the impression that the trials are complete and that the regulators
have strict safety standards. The 1,2,3 phase trial for AZD1222 was registered with the U.S.
Centre for Disease Control as
clinical trial NCT04516746 [Archived 29th December 2020]. It is incomplete and the
estimated end date is February 21st 2023. The CDC state:
No Study Results Posted
Astrazeneca are years away from reporting any "final data." It is impossible for the
UK Department of Health to review it, because it doesn't exist.
NCT04516746 is one of four trials of AZD1222. Another
Russian arm of the AZD1222 trial was suspended after a Suspected Unexpected Serious Adverse
Reaction (SUSAR) event occurred. The SUSAR supposedly happened in the United Kingdom after a 37 year old
women developed inflammation of the spinal chord. It appears the Russian Ministry of Health
have yet to reinstate their arm of the Astrazeneca/Oxford trial while it has resumed in the UK
and elsewhere.
Clinical Trial NCT04516746:
[Archived 29.12.2020] , [Contemporary
Link] WHAT VACCINE TRIALS?
On November 18th Pfizer and BioNTech announced they had
concluded their phase three trial of BNT. They had demonstrated efficacy of 95% and U.S.
Food and Drug Administration's (FDA's) Emergency Use Authorization (EUA) safety data
milestone had been met.
The only part of this claim that was true was compliance with FDA emergency safety data
milestones. They have not concluded their phase three trials. They haven't even fully
completed phase one.
Under section 564 of the Federal Food, Drug, and Cosmetic Act (FD&C Act ) so called
"unapproved" drugs are allowed on the market in emergencies . Similarly, in the
UK, authorisation under Regulation 174 of the Human Medicine Regulations 2012 (as amended)
permits the same.
Having also been approved in the UK, this is why the Medicines and Healthcare products
Regulatory Agency (MHRA) state:
This medicinal product does not have a UK marketing authorisation
The fact that there are no completed clinical trials for the Pfizer and BioNTech BNT vaccine
also
explains why the FDA State:
Additional adverse reactions, some of which may be serious, may become apparent with more
widespread use of the Pfizer-BioNTech COVID-19 Vaccine.
The FDA also
noted :
[There is] currently insufficient data to make conclusions about the safety of the vaccine
in sub-populations such as children less than 16 years of age, pregnant and lactating
individuals, and immunocompromised individuals ..[the] risk of vaccine-enhanced disease over
time, potentially associated with waning immunity, remains unknown.
Yet the first people to receive this vaccine are the most vulnerable in society, many of
whom are immunocompromised. The precautionary principle appears to have been abandoned. The
notion that the purpose of the BNT vaccine roll out is to save life appears
untenable.
The Pfizer announcement enabled politicians to pretend to cry on national television while
others were really excited. UK Prime Minister
Boris Johnson said it was "fantastic news," and the BBC said it was "good
news" and "really encouraging." Everyone was thoroughly impressed with the 95%
effective claim.
However, this was based upon relative risk reduction . That is the
declared percentage difference between the vaccinated group's 8/18310 chance (0.044%) of
developing COVID 19 against a 162/18319 (0.88%) chance of COVID 19 symptoms without the
vaccine. As this larger group of 43,000 people have yet to be trialled, there is no basis for
this claimed outcome. But it is what it is, and we can use these reported figures here.
It should be noted this only refers to an alleged reduction of COVID 19 symptoms among those
who have the virus. The tested endpoints do
not demonstrate that the vaccine will either reduce the spread of infection or save lives.
It should also be noted that these figures suggest the threat from COVID 19 is vanishingly
small.
Using Pfizer's figures, the relative risk reduction is 100(1 – (0.044/0.88)). Which is
95%. Voila!
This sounds fantastic and is a much better marketing strategy than reporting the absolute
risk reduction. The absolute risk of developing COVID 19 symptoms without the vaccine is
supposedly 0.88% and with the vaccine 0.044%. In absolute terms, the effectiveness of the
vaccine is (0.88-0.044)%.
A risk reduction of 0.84%. Oh! A barely perceptible "efficacy."
By using the relative instead of absolute risk reduction, the mainstream media (MSM) were
free to market the mRNA vaccine for Pfizer and BioNTech (and other interested parties) with
impressive sounding claims . These
weren't remotely truthful, not only because they relied upon statistical manipulation but
because no one had a clue about BNT's safety or efficacy. To this day, there are no clinical
trial results.
THE CLINICAL TRIALS THAT DON'T EXIST
An analysis of available positive RT-PCR tests and mortality results led the Oxford Centre for
Evidence Based Medicine estimated a very tentative COVID 19 Case Fatality Rate (CFR) of
around 1.4%. Based upon the figures reported to the FDA by Pfizer and BioNTech, this indicates
a broad population based mortality risk from COVID 19 of 1.4(0.88/100) which is 0.012%.
Please bear this incredibly remote risk in mind as we discuss the early indication of the
apparent threat to public health presented by the mRNA vaccine.
It is reasonable to work in terms of population risk because, while the chance of COVID 19
mortality seemingly increases with age, with the average age of death being 82 and a mortality
distribution indistinguishable from standard mortality, the intention is to give the vaccine to everybody .
If we look at the "V-Safe Active Surveillance for COVID 19 Vaccines" reported by the
U.S. Center For Disease Control (CDC),
early indications of the recorded "Health Impact Events" (HIE) reveal a worrying level
of adverse reactions from the mRNA vaccine. The CDC define an HIE as:
Unable to perform normal daily activities, unable to work, required care from doctor or
health care professional
On December the 18th 112,807 people were injected with the Pfizer/BioNTech vaccine in the
U.S. Of these, 3,150 were subsequently unable to perform normal daily activities, unable to
work, required care from doctor or health care professional . This is an HIE rate of 2.8%.
This suggests that among the first 10 million people to receive the vaccine in the UK,
around 280,000 may find themselves unable to perform normal daily activities, unable to work
and require medical care as a result. As it is the most vulnerable who are the first to receive
this vaccine, given the tiny risk of mortality from the COVID 19 disease, it is by no means
clear that this is a risk worth taking.
CDC Presentation:
[Archived 19.12.2020] ,
[Original]
Not that any of the other vaccines seem any better. So far the CDC have noted
more than 5,000 HIE's for all vaccine being trialled on the population. Clearly, the
potential exists that the vaccines will contribute to more deaths than the disease they
allegedly protects vulnerable people against.
The Pfizer/BioNTech trial was registered as clinical trial number NCT04368728 with the CDC. Having recently
discussed what I am about to share with you with people who simply refused to believe the
evidence of their own eyes, I think it is important to stress that this is the Phase 3 Clinical
Trial which Pfizer claimed they had concluded in their press release. There isn't another one.
This is it .
The CDC state:
When available, study results information is included in the study record under the Study
Results tab .After study results information has been submitted to ClinicalTrials.gov, but
before it is posted, the results tab in the study record is labeled "Results Submitted.
At the time of writing (21st December 2020) as can be seen by date of the archived ClinicalTrials.gov web-page , the Study Results tab
reads "No Results Posted." That is because there are no posted or submitted results from the
Pfizer BioNTech trial of the BNT162b2 vaccine:
No Study Results Posted on ClinicalTrials.gov for this Study
Mainstream media reports , giving the
impression that these vaccines have been found to be effective and safe are not
evidence and they are not based on science. They are based on political policy and they report
dangerous pseudo-scientific babble, masquerading as science journalism.
There will of course be mindless anti-rationalists who will call
this dangerous antivaxxer nonsense. All the time insisting that it is perfectly safe to give a
vaccine with a questionable safety profile, for which there are no completed clinical trials,
to the most vulnerable people in our society.
I am running out of patience with these people.
VACCINE SAFETY?
The start date for NCT04368728 was April 29th and the estimated trial completion date is
January 27th 2023. The estimated end date of the primary or phase one of a three phase
trial is June 13th 2021.
According to the " Current Primary Outcome Measures," the minimum time frame for
Pfizer to assess serious adverse events (SAE's) is "6 months after last dose." This is the
minimum term for assessing SAE's in phase one of the trial.
Phase one is the only part of the NCT04368728 trial to have been
completed and published . It was published on the 14th October, 5 months and two weeks
after the start date. Most of that period was taken up with recruitment an allocation. The
minimum term for assessing SAE's has not been met during Phase One.
During Phase One, 195 participants were split into 13 groups of 15 people. In each group 12
received one of two potential mRNA vaccine candidates (either BNT162b1 or BNT162b2) and 3 a
placebo.
39 people aged between 18-55 and another 39 people aged between 65-85 received the BNT
vaccine, now approved for global distribution. The threat of COVID 19, though tiny overall, is
statistically zero for
those aged 18-55. Those with any measurable risk from COVID 19 were in the older age group.
Of the 39 older people who received 2 doses of BNT about half of them experienced
"fatigue," roughly 15% had "chills" and 3 of them had a fever. The
common side effects of BNT included nausea, headache (a very common BNT induced nervous
system disorder) arthralgia and myalgia (very common), fatigue, chills and fever (again very
common.) Other than fatigue, no one in the placebo group suffered these problems.
Safety and Immunogenicity of Two RNA-Based Covid-19 Vaccine Candidates: Figure 3,
'Participants 65 – 85 yr of age'
[Archived 29.10.2020] , [Original]
The study states:
Pfizer was responsible for the trial design; for the collection, analysis, and
interpretation of the data; and for the writing of the report.
Therefore, it is reasonable to conclude that while Pfizer see the side effects of their
vaccine as fatigue, chills and fever, the CDC refer to them as people who can't work and
need medical care.
The UK Medical and Healthcare products Regulatory Agency (MHRA) approved the BNT vaccine, to
be given to vulnerable British people, based upon a study of 39 older people. This study
reported a pretty high adverse reaction rate. It was produced exclusively from the R&D of
the vaccine manufacturer. The MHRA questioned nothing.
They "approved" BNT in the certain knowledge that there were no completed clinical
trials for this vaccine. In their Public Assessment Report they state:
At the time of writing, the main clinical study is still on-going .It was concluded that
BNT162b2 has been shown to be effective in the prevention of COVID-19. Furthermore, the side
effects observed with use of this vaccine are considered to be similar to those seen with
other vaccines. Therefore, the MHRA concluded that the benefits are greater than the
risks.
This conclusion and approval not only lacks supporting evidence it is utterly at odds with
what little is known about BNT. While Pfizer and BioNTech only completed trials of the vaccine
on 39 relevant test subjects, the results, even from this practically inconsequential effort,
suggest the risk from the vaccine is greater than the risk presented by COVID 19. By a
considerable margin.
This undoubtedly explains why the MHRA ordered software from European suppliers to deal with the slew
of vaccine adverse reaction they presumably anticipate. They stated:
The MHRA urgently seeks an Artificial Intelligence (AI) software tool to process the
expected high volume of Covid-19 vaccine Adverse Drug Reaction (ADRs) .it is not possible to
retrofit the MHRA's legacy systems to handle the volume of ADRs that will be generated by a
Covid-19 vaccine.
From the way the manufacturers, politicians, regulators and the MSM have approached vaccine
safety, it is clear that they collectively have a total disregard for the welfare of vulnerable
people. We really must put aside this infantile notion that "the authorities" care about
us or our loved ones. We mean nothing to them.
COVID 19 is only an appreciable risk for the
most vulnerable in society. It is a risk to the infirm elderly and people with existing
life threatening conditions.
If we look at the exclusion criteria
for Phase One, these people were not in the cohort tested. Anyone with high blood pressure,
asthma, diabetes or a high BMI were excluded from the alleged safety trial. But the vaccine is
being given to the most vulnerable first.
Of the 39 older people at most risk in the phase one study, none of them had the serious
comorbidities which the overwhelming majority of those who die "with" COVID 19 possess.
The people actually at risk from COVID 19 nominally entered the BNT trials at phase 2 and 3.
However, it appears every effort has been made to limit, if not completely remove, their number
too. "Immunocompromised or individuals with known or suspected immunodeficiency," were
excluded.
Immunodeficiency is caused by a wide range of health conditions
. Conditions such as undernutrition, polytrauma, stress after surgery, diabetes and cancer lead
to immunodeficiency. The people with the comorbidities associated with so called COVID 19
deaths were practically ruled out from the BNT vaccine trials.
NCT04368728 was designed as a 1,2,3 trial with all phases running concurrently. With regards
to assessing safety Pfizer described systemic events as:
Fever, fatigue, headache, chills, vomiting, diarrhea, new or worsened muscle pain, and new
or worsened joint pain as self-reported on electronic diaries.
The first 360 subjects randomised into the phase 2 and 3 trials underwent monitoring for
systemic events for less than a week, following each dose:
In the first 360 participants randomized into Phase 2/3, percentage of participants
reporting systemic events [ Time Frame: For 7 days after dose 1 and dose 2 ]
The same cohort of 360 test subjects were also monitored for Serious Adverse Events (SAE's)
for up to 6 months in phase 2 and 3:
In the first 360 participants randomized into Phase 2/3, percentage of participants
reporting serious adverse events [ Time Frame: From dose 1 through 6 months after the last
dose]
Pfizer also intend to report the percentage of all test subjects who suffer SAE's:
Percentage of participants in Phase 2/3 reporting adverse events [ Time Frame: From dose 1
through 6 month after the last dose ]
But there are no reported results from either phase 2 or 3. No one has the faintest idea
what the health risks of BNT are, especially for those it is supposedly designed to protect,
and no one in authority gives a damn. Phase 2/3 clinical trials are now a moot point
anyway.
The regulatory agencies have already approved the vaccine and health services have started
injecting people with BNT. They do so after the manufacturers failed to properly test its
safety on a 39 people who were in the at risk group but did not have the comorbidity
that leads to claimed COVID 19 deaths.
The degree to which people have been misled into believing that these vaccines are known to
be either safe or effective is almost beyond imagination.
Sadly, we don't need imagination. The evidence is clear.
Paul Nicholls
The've been practicing this scam for a while now. Everything happening now has already had
a few dry runs, perfecting all aspects of the current hoax.
James Corbett September 2012:
https://www.corbettreport.com/corbett-report-radio-226-pandemic/
Judith Nailer
Can you clarify when you say the larger group of 43,000 people have yet to be trialled.
Because I read in the following:
How Scientists Know The
Approved COVID-19 Vaccines Are Safe
that "Pfizer's Phase lll trial has been published in a peer–reviewed journal and
included over 40,000 volunteers in 152 sites worldwide".
Kalen
Death porn continues:
from ABC
California funeral homes run out of space as pandemic rages.
We are led to believe that mountains of corpses pile up because .. of ongoing massive
COVID die out.
In order to keep up with the flood of bodies, Maldonado has rented extra 50-foot
(15-meter) refrigerators for two of the four facilities she runs in LA and surrounding
counties. Continental has also been delaying pickups at hospitals for a day or two while they
deal with residential clients.
Pure panic. Only to be informed why we have piling up bodies in hospitals and
mortuaries.
Bob Achermann, executive director of the California Funeral Directors Association, said
that the whole process of burying and cremating bodies has slowed down, including embalming
bodies and obtaining death certificates. During normal times, cremation might happen within a
day or two; now it takes at least a week or longer.
so to summarize typical for flu season increased numbers of flu, pneumonia deaths are
processed six to seven times slower than a year ago, causing obvious pile up.
Like with sex porn, COVID death porn is best left unexamined in detail not scrutinized too
much, better left to porn induced sick imagination targeting consumers, otherwise reality
will turn them off.
Igor
The obvious problem with these vaccines, is that no reliable fit for purpose diagnostic
test exists as of this moment. As far I know, no one in power is even talking about any need for an effective test. How are they able to prove that a vaccine is effective without a reliable, valid test?
Rahm Emmanuel said "never let a crisis go to waste". Crisis do not need to be real motivate the necessary panic for a change.
Edith Igor
I suspect they are only testing whether the persons immune system produces some tcells etc
from giving them this rubbish they cannot possible then infer one will be immune to any sort
of cold, flu or pneumonia
Schmitz Katze
Moderna admits here that what they inject with their vaccines is an "operating
system."
"Our mRNA technology platform functions very much like an operating system on a computer. It is designed so that it can
plug and play interchangeably with different programs" I can´t find anything what a vaccinated person is supposed to do when the operating
system inside his/her body crashes -- It´s Doctor Bill´s ultimate solution to
solve climate change, I suppose.
https://www.modernatx.com/mrna-technology/mrna-platform-enabling-drug-discovery-development
axisofoil
Very clever mass detention and forced vaccination bill.
https://www.nysenate.gov/legislation/bills/2021/a416
Cal axisofoil
It used to be the case that if we felt unwell we'd take time off to stay at home to
recover, or that we'd go to hospital.
This new bill makes it possible for a healthy person to be tested (with a fraudulently
used PCR test) to prove positive, followed by forced incarceration in a detention centre as
if a common or garden prisoner.
Imprisonment without trial for no crime in the land of the free.
I have the feeling the rich will not be targeted, only the poor. If this was happening in
North Korea people would be horrified. Any politician enabling this act is enabling fascism
and tyranny.
JoeC Cal
It's so obvious what this asymptomatic bullshit is all about.
Judith Cal
Call me clueless, but this doesn't have a chance of actually passing does it?? Will they put everyone on trains at Grand Central and ship you off? For your own good?
livingsb livingsb
taking a shit on the floor and pissing on the curtains, then tearing off the roof .
October
Wow. Britain is going to mix vaccines according to this . In France meanwhile, after getting off to a very slow start, they're thinking of
appointing an advisory committee of randomly selected citizens (?) to define their
immunisation strategy.
Said committee will submit its report in the summer .
moneycircus October
I call them Britain's Scient-icians. They make it up as they go along. From the NYT article "There are no data on this idea whatsoever," said John Moore, a vaccine expert at Cornell
University. Officials in Britain "seem to have abandoned science completely now and are just
trying to guess their way out of a mess."
Kalen
As author pointed out no SC2 viral genetic material is used in Pfizer, Moderna and AZN
bioagents wrongly called vaccines .. because they do not have them available (or they do not
exist). In fact even Chinese making so called traditional attenuated vaccines or Russians
making adenovirus vector bioagents do not have them either. Instead of entire virus they use
only spike protein only for achieving immunogenicity. But where the spike proteins come
from.
ABC explained in September on AZN example.
Britain's Oxford University and AstraZeneca are making what scientists call a "viral
vector" vaccine but a good analogy is the Trojan horse. The shots are made with
a harmless virus – a cold virus that normally infects chimpanzees
– that carries the spike protein's genetic material into the body. [infecting human
cells] Two possible competitors to AZN are made with different human [common] cold
viruses.
Yes. What is being tried on people by Moderna Pfizer, AZN and others are experimental
bioagents that solicit antibodies that alledgedly block common cold's subclass of
coronaviruses' spikes, not particularly SC2 virus spikes because they do not have them
isolated.
No supposed experimental "vaccines" make any attempt to eradicate, neutralize SC2 virus
itself if it exists, (if COVID exists) as so far there is no proof of either.
Those phantom pseudo-vaccines supposedly to protect us from phantom disease have nothing
to do with published SC2 virus RNA or with COVID clinical disease they are bio-technological
experiments with drug delivery systems aimed as harvesting human cell to production of
certain proteins altering cell functions and metabolism.
In this particular case Moderna and Pfizer bioagents make regular human cells grow non
human protein spikes fooling immune system into increasing antibody production, marking human
cells for eradication and attacking human cells by killer TCells (Lymphocytes).
Those are human cells, not infected by active reproducible virus that are being destroyed
according to the mRNA vaccine model and that is why unprecedented in comparison with other
vaccines prevalence of severe disease like, incapacitating symptoms of infection with
artificial bioagents themselves. Anything beyond little redness and swollen tissue around
injection site not to mention loss of consciousness is cause of serious concern.
if this is the case those experimental "vaccinations" developed with no animal studies to
establish safety and toxicity set up perfect conditions for cytokines shocks, pathogen
priming and ADE all longer term deadly complications of coronavirus vaccinations encountered
in the past coronaviruses vaccine research.
Mark R. Elsis
Understanding What They Mean By 'Risk Reduction' Is Critical by Dr. Thomas Cowan
(12:52) https://www.bitchute.com/video/yosb8WE9IvPc
Jean
In Quebec City (Canada), the first doses of Pfizer/Biotech vaccine were for the folks and
employees of an old age pensioners residence. They got their shot on Dec. 14. On Dec. 30, 66
vaccinated residents and 20 employees got COVID. Explanation from health authorities: the
vaccines needs 14 days to be efficient. But positive tests were announced after 14 days.
Here's the article in French:
https://ici.radio-canada.ca/nouvelle/1760058/eclosion-covid-chsld-saint-antoine-quebec-vaccin
And yesterday, I fell on this Sputnik article: 240 Israelis Test Positive for Coronavirus
After Getting
Vaccinated
https://sputniknews.com/middleeast/202101021081631205-240-israelis-test-positive-for-coronavirus-after-getting-vaccinated/
So, does that means that you have more chance to catch the virus by being vaccined against
it?
Jacques Guy
https://www.youtube.com/watch?v=C1-0XKYAZII
This sums it up quite nicely. There are other who say essentially the same thing, perhaps
from a different angle.
Money might be a secondary, short-term benefit, but money as understood today won't
probably matter for very long anymore.
It's about total control solidified by technologies. Eventually, eradicating people deemed
non-essential. The psychopaths probably think that they can manage with robots.
Well, if that happens, the solace for us, who fall by the wayside, will be that the world
created by the TFIC will eventually atrophy, implode. These fuckers have no culture, no vital
creativity. They thrive on technocratic dullness, control. They can live on what's creative
spirits have created thus far, but that will only take them so far.
Paul Guy
As other commenters have eluded too the introduction of health passports are coming,
digital IDS, the Chinese social credit system.
It's a fascist global coup from the WEF, IMF, Gates, Big Tech etc.
Unfortunately too many people and even those who know something isn't right are thinking
it's just hysteria or the governments don't know what they're doing.
Schmitz Katze
What is the evidence so far on side effects and long-term effects of Covid vaccinations?
Obtained in half a year on test subjects and within a week on nursing home residents?
Questions like this and common sense will be banned in the near future. Sheep will bleat
ten times a day: Vaccination is good because the government is only ever concerned with our
welfare and health. Apart from that, vaccinating with an untested vaccine is Kismet.
For sane people, if one follows the Pfizer/Biontech package insert, the vaccination is a
dareDevil act. With some probability, the vaccinated person will only become slightly ill
– even that is not certain – but he/she can still become infected and infect
his/her fellow men.
People in Germany are inundated with magazine covers the likes of Der Stern with
headlines:"Vaccination is charity" with Christmas nativity scene. This is the most malicious
manipulation I have seen about experimental m RNA-based vaccinations so far. The opposite is
the case. Pharmaceutical corporations use people who are vaccinated now as guinea pigs for
their studies which are laid out on the two following test years.https://shop.stern.de/de_DE/einzelhefte/einzelausgaben/stern-epaper-53-2020/1990689.html
Steve
The background to the mRNA tech in this opinion piece is interesting
" Scientific breakthroughs like this don't come from nowhere. Messenger RNA was first
discovered in the early 1960s but it wasn't until the late 1980s that scientists learned how
to make it from scratch. Then a new hurdle emerged. When scientists injected mRNA into
animals, it induced such a severe immune response that the animals died. It was Dr Katalin
Kariko, working with immunologist Dr Drew Weissman, who figured out how to stop
that severe immune response from happening. And that was crucial for mRNA vaccines to be
trialled in humans."
http://www.stuff.co.nz/national/health/coronavirus/300195200/covid19-turning-our-bodies-into-vaccine-factories
Paul JudyJ
As most of the vaccinated people are in care homes it would be interesting to know how
many of them have subsequently tested PCR positive.
This hasn't been mentioned anywhere.
But then again the 'vaccine' doesn't protect against infection or transmission and just
symptoms as we are told.
Hallelujah Paul
Except that it causes the same symptoms as the alleged disease it has to prevent.
TFS JudyJ
Does this help you?
https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2020-12/slides-12-19/05-COVID-CLARK.pdf
Check out the section on Health Impact Events.
Major Covid Vaccine Glitch Emerges: Most Europeans, Including Hospital Staff, Refuse To
Take It BY TYLER DURDEN SUNDAY, DEC 27, 2020 - 21:50
All is not going according to plan in the biggest global rollout of what is arguably the
most important vaccine in a century, and it is not just growing US mistrust in the covid
injection effort that was rolled out in record time: an unexpected spike in allergic reactions
to the Pfizer/BioNTech vaccine (and now, Moderna
too ) may prove catastrophic to widespread acceptance unless scientists can figure out what
is causing it after the FDA's rushed approval, and is also why as we
reported yesterday , scientists are scrambling to identify the potential culprit causing
the allergic reactions.
Making matters worse, Europe rolled out a huge COVID-19 vaccination drive on Sunday to try
to rein in the coronavirus pandemic but even more Europeans than American are sceptical about
the speed at which the vaccines have been tested and approved and reluctant to have the
shot.
While the European Union has secured contracts drugmakers including Pfizer, Moderna and
AstraZeneca, for a total of more than two billion doses and has set a goal for all adults to be
inoculated next year, this is looking increasingly like a pipe dream: according to recent
surveys, the local population has expressed "high levels of hesitancy" towards inoculation in
countries from France to Poland, with many used to vaccines taking decades to develop, not just
months.
"I don't think there's a vaccine in history that has been tested so quickly," Ireneusz
Sikorski, 41, said as he stepped out of a church in central Warsaw with his two children.
"I am not saying vaccination shouldn't be taking place. But I am not going to test an
unverified vaccine on my children, or on myself."
Smart: why take the risk of getting vaccinated when others will do it, resulting in the same
outcome.
Surveys in Poland, where distrust in public institutions runs deep, show that fewer than 40%
of people planning to get vaccinated. Worse,
according to Reuters on Sunday, only half the medical staff in a Warsaw hospital where the
country's first shot was administered had signed up. And if the doctors don't trust the
vaccine, one can be certain that the broader population will refuse to take it.
The situation is similar in Spain, one of Europe's hardest-hit countries, where 28-year-old
singer and music composer German summarizes the skepticism of a broad range of the population,
and plans to wait for now.
"No one close to me has had it (COVID-19). I'm obviously not saying it doesn't exist
because lots of people have died of it, but for now I wouldn't have it (the vaccine)."
A Christian Orthodox bishop in Bulgaria, where 45% of people have said they would not get a
shot and 40% plan to wait to see if any negative side effects appear - meaning only 15% of the
population will actually volunteer for a vaccine in the near future - is in the tiny minority
when it comes to taking the vaccine.
about:blank
about:blank
me title=
"Myself, I am vaccinated against everything I can be," Bishop Tihon told reporters after
getting his shot, standing alongside the health minister in Sofia. He spoke about anxiety over
polio before vaccination became available in the 1950s and 1960s.
To be sure, the establishment is pounding the table on why the vaccines are safe despite the
record short time in development (even though not even the "scientists" can explain what is
behind the spike in vaccine allergic reactions), and claiming that the new technology behind
the mRNA vaccine is all one needs to know... when it is precisely this new technology that is
sparking the skepticism.
"We'll look back on the advances made in 2020 and say: 'That was a moment when science
really did make a leap forward'," said Jeremy Farrar, director of the Oxford University
Clinical Research Unit, which is backed by the Wellcome Trust. Oxford also received $750MM from
Bill Gates in June in the billionaire's quest to vaccinate the world against Covid.
Only problem: nobody in Europe seems to care about these "scientific" justifications.
Independent pollster Alpha Research said its recent survey suggested that fewer than one in
five Bulgarians from the first groups to be offered the vaccine - frontline medics,
pharmacists, teachers and nursing home staff - planned to volunteer to get a shot.
An IPSOS survey of 15 countries published on Nov. 5 showed then that 54% of French would
have a COVID vaccine if one were available. The figure was 64% in Italy and Spain, 79% in
Britain and 87% in China.
Since then things have gone far worse, and a more recent IFOP poll showed that only 41%
people in France would take the shot . This means that a vast majority will not .
French
Healthcare workers applaud Mauricette, a 78-year-old woman, after she received the first dose
of the Pfizer-BioNTech coronavirus disease vaccine in the country.
Not even in Sweden, where public trust in authorities is absurdly and inexplicably high, is
there a universal trust in the vaccine, with at least one in three saying they won't get the
shot: "If someone gave me 10 million euro, I wouldn't take it," Lisa Renberg, 32, told Reuters
on Wednesday.
Meanwhile, in a paradoxical attempt to force more to sign up - not realizing that it will
only have the precisely opposite effect - Polish Prime Minister Mateusz Morawiecki urged Poles
on Sunday to sign up for vaccination, saying the herd immunity effect depended on them. Critics
have accused Warsaw's "nationalist leaders" of being too accepting of anti-vaccination
attitudes in the past in an effort to garner conservative support. Well... let's check back on
said attitude in 10 years and see if perhaps it was the right one.
For now, however, the more European governments pressure their populations to get immunized,
the fewer the people who will actually sign up and the worse the vaccine rollout will be, that
much we can be 100% sure of.
Christian J. Chuba , Dec 28 2020 22:43 utc |
20
OT: but related, vaccines distributed the U.S. breathlessly announced the success
of operation warp speed and claimed that 20M doses would be distributed (shots in arm) by the
end of this year, now we know the number is 2M .
Does anyone know how many doses of Sputnik V have been distributed year to date?
Latest outrage
US Demanding Iran's Vaccine Payments Go Through Its Banks the headline tells you what you
need to know. Is there any end to our depravity?
Yesterday in a especial program at private TV, it was stated by several representatives of
the medical profession all very snobishly dressed, that there have not been other adverse
effects so far except headhache, and joints pain..whic his not true, there have been also
transverse mielitys, several anaphilactic shocks, and even deaths...
Telated, and with respect Brexit, one wonders how it is that after Brexit comes into effect,
and after the EU populations are submitted to harsh restrictions of movements and meeting,
especially travelling since March, several whole families of Britons managed to get into our
countries carrying the new strain of the virus which is 70% more virulent...How is that UK
citizens are more free than nationals, and what the Brexit serves for...
One would say that this new strain came so opportune to be blamed in case of a possible
failure of the few experimented vaccines, or, if not, the population will be blamed for no
vaccinating themselves enough. This way the governments wash their responsability in the
previous misshandling of this pandemic,ingtroduce curtails of freedoms and rights which
previously would have been impossible to do without fierce contestations in the streets, and
avoid answering why they did not forced the laboratories instead into investigating on drugs
that cure the Covid-19 infection, as the one administered to Trump is being investigated right
now in the UK...Of course, drugs that cure an infection which anyway could dissapear in a year
automathically ends profitting from vaccines.
One watch at all this data and gets the impression that he is being taken for a ride...
All of the above are legitimate questions the cintizenry are making to themselves, in lack
of public comparecence of officials and heads of laboratiories implied to public and open
questioning. The secrecy of all this highly controbutes to the distrust of the people. the
people is being treated as herd, and never better said, illiterates who can not see further
their own extende arm, and used a guinea pigs while morevoer left to pay the bill, as the
ammount to be spent in these vaccines is an astronomic price which, of course, will never be
taken out from the oligarchs.
Posted by: H.Schmatz | Dec 27 2020 15:55 utc |
6 Conflict of interests between major Big Pharma corporations and official drug
organisms:
Pfizer-BioNTech Vaccine Efficacy? Where is the evidence to prove it? What's behind all that
"fanciful" and encouraging news? And what about the links between state vaccine regulatory
agencies and the pharmaceutical industry?Thread.
https://twitter.com/Herbert_Keg/status/1343155319187394561
Posted by: H.Schmatz | Dec 27 2020 16:12 utc |
7
That should have been in the first paragraph. There were so far less than ten severe allergic
reactions,no death, with more than 1 million vaccinated. That is 1 in 100,000 cases. About
the same rate that allergic reactions to penicillin are reported. Meanwhile the U.S. has seen
100 deaths per 100,000 from Covid-19.
Do you think 1 in 100,000 is acceptable? I don't think it is, at least for a vaccine that's
intended (I know it won't, but it would if it could) to for more than 7 billion people, against
a disease that has a mortality rate of circa 1.5%.
Notice that the Pfizer and Moderna vaccines, so far, have only been inoculated on VIPs or
healthcare professionals. Those who had grave anaphylactic episodes did so in a secure
environment, inside fully equipped hospitals, ready to be saved if needed.
Now imagine a Third World environment, where billions of people would received the vaccine
and be ready to go a few minutes later.
Luckily, the Third World will mainly receive the Chinese and Russian vaccines, which cause,
as far as we know, no allergic reactions. Now imagine a world where China and Russia didn't
exist, a world where capitalism reigned supreme, and 7 billion had to receive the Pfizer and
Moderna vaccines. This would make the Holocaust look like a book for children - and I mean that
in the literal sense, not invoking Goodwin's Law (just make the calculations).
Penicillin is a completely different case: it was the only game in town when it came out,
and the flu killed a lot more than the antibiotic did. Flu was basically a death sentence to a
child before penicillin was discovered, and was a serious threat even to an adult. Besides,
Penicillin is a cure, not a vaccine - completely different scenarios, as the person with a flu
lives in a different risk-reward system than a person who may or may not ever get COVID-19.
Vaccines that kill one in 100,000 patients do exist (e.g. yellow fever, which is a live
virus vaccine) - but they are for exotic and much deadlier diseases, so a much lower number of
people are inoculated with it and the risk is well worth it. To release such an expensive and
risky vaccine when there are cheaper and safer options is irresponsible on the part of the
laboratories, in my opinion.
Posted by: vk | Dec
27 2020 16:25 utc |
8
Vk - 1 in 100,000 is incredibly good. Be assured that any vaccine that would potentially be
effective against this virus would have at least this level of issue. That we don't know the
complications rate of the Russian or Chinese vaccines does not mean that the rates are
zero!
As to your argument, you don't see the benefit of vaccinating where potentially millions of
people could die and the economies be completely wrecked? What the hell?
Posted by: Caliman | Dec 27 2020 17:33 utc |
17
Caliman @ 17
No allergic reactions from Sputnik
V
Posted by: arby | Dec 27 2020 18:10 utc |
19
Two interesting interviews from Germany.
(1) In this interview with ZDF, Prof. Wolf-Dieter Ludwig, who is the head of the drug
commission of physician in Germany, considers the development of Covid vaccines as a positive
thing but finds faults with politicians, especially German health minister Spahn, for putting
political pressure on the European Medicines Agency (EMA) to accelerate the approval of
vaccines, especially the Pfizer/BioNTech vaccine. Prof. Ludwig also belongs to EMA management
board. Most importantly, when asked whether he'd take the vaccine, his response was NO.
That's because he feels that we hardly know anything about its long term adverse effects
. https://www.zdf.de/nachrichten/politik/corona-impfstoff-zulassung-kritik-ludwig-100.html
there exist hardly any preclinical toxicological and pharmacological data (phases 1 and
2) . He points out that even in cases of orphan drugs, the regulation allows a telescoping
of the Phase 3 clinical study, but NEVER of the preclinical studies. In his words, the way
Phases 1 and 2 have been skipped is criminal in nature. At the very end of the interview
(which is in German), he quotes the response from Pfizer as "No data available" on his
request for toxicological and pharmaceutical data from preclinical studies!!
He also notes that recently Swissmedic (national authorization and supervisory authority for
drugs and medical products in Switzerland) has concluded that the Pfizer vaccine submission
lacks evidence of safety, efficacy and quality! Swissmedic is independent of EMA.
https://www.youtube.com/watch?app=desktop&v=iiTrttV7Q8A&feature=youtu.be
Prof. Hockertz is a past director of institute for experimental toxicology and clinical
toxicology at University of Hamburg Eppendorf. And before that he was a member of the
directorate of Fraunhofer Institutes for Toxicology and Environmental Medicine in Hannover.
I am not saying that the vaccine is dangerous - I have no data to support that conclusion.
But there is no data to support that the vaccine is safe either.
Posted by: Nathan Mulcahy | Dec 27 2020 19:44 utc |
26
@vk
You, as usually, in your apparently well informed kinda Marxist narrative, insert always
some of disinfo which makes me suspect about your real golas here.
You are stating that the Pfizer vaccine was admnistered only to a few VIPs...
Which VIPS are those? Do not be you referring to Pence? He could well have been inoculated
with phisiologic solution as he is reincident, like that time when he transported empty aid
boxes in the past for another photo op. Another example, please?
They are inoculating first super elders, in their last 80s and 90s in the nursing homes,
mainly private, young nurses and nursing home employees working there...which points at that
thosve employees probably would be fired if they do not agree on being vaccinated
They have taken the caution to not inoculate first the people between 50 and 60 which are
those who most could suffer a serious adverse effect, by the possible presence of
preconditions, in fact the most prejudiced by Covid-19 infection....
In fact, not even in Russia there are officials vaccinated yet, and that even with the less
harmful Russian vaccine....
In the press some are displaying a huge effort naming this event a "estelar moment for
humanity"...
The people, over whom all the sticks fall, have not but producing memes due the current
histeria displayed on TV and MSM...
https://twitter.com/i/status/1342968855598133250
Posted by: H.Schmatz | Dec 27 2020 20:04 utc |
27
URGENT
News about the Covid-19 Vaccine
Dr Vernon Coleman
Excerpt from transcript of 3:47 min video:
I have just seen a report from `ACIP Covid-19 Vaccine Work Group at CDC' in the US. (ACIP
stands for Advisory Committee on Immunisation Practices.)
This is a report on anaphylaxis following m-RNA covid-19 vaccine receipt, and the report
includes a table headed: 'V-Safe Active Surveillance for Covid-19 Vaccine'.
The table lists the number of registrants with a recorded first dose by December 18th as
112,807 and the number of Health Impact Events as 3,150.
Health Impact Events are defined as individuals, `unable to perform normal daily
activities, unable to work, required care from doctor or health professional'.
That is 2.79%, and it is within days of receiving the vaccine.
If 60 million people in the UK have the vaccine we can, therefore, expect 1.67 million
people to be unable to work, perform normal daily activities and to require care from a
doctor or health professional.
If six billion people worldwide have the vaccine, we can expect 167 million people to be
`unable to work, perform normal daily activities, require care from doctor or heath
professional'.
And that is just the short-term effect of the vaccine. We obviously don't know what will
happen in the months and years ahead.
ACIP COVID-19 Vaccines Work Group
Posted by: pogohere | Dec 28 2020 1:23 utc |
65
65 cont'd
The transcript of the video: Urgent News about the Covid-19
Vaccine'
from vid: URGENT
News about the Covid-19 Vaccine
3:47 min
ACIP COVID-19 Vaccines Work Group
Anaphylaxis Following m-RNA COVID-19
Vaccine Receipt
Thomas Clark, MD, MPH
scroll down to Slide 6
Posted by: pogohere | Dec 28 2020 1:31 utc |
68
@65 & 68 pogohere
Thank you. I'm not sure we're seeing what we think we're seeing here.
In the CDC report, page 4 says 6 cases of anaphylaxis were discovered by 2300 hours, EST on
December 18.
Page 6 cites the number of Health Impact Events as 3,150, and this at an earlier time, 1730
hours, EST on December 18.
After studying this, I conclude that they are not claiming 3,150 cases of anaphylaxis in the
data tabulated from earlier that night.
I currently assume that page 6 is referring to surveillance measures taken rather than cases
found - the slide is titled "V-safe Active Surveillance for COVID-19 Vaccines". So, this would
mean that they had monitored those patients for anaphylaxis as of 1730 hours, but in the data
finalized as of 5.5 hours later they were only reporting 6 cases.
I actually hope this is the case, although I'm not a fan of the Pfizer vaccine. If I'm
wrong, and Dr. Coleman's take is correct, then the world just blew up - but I would think we'd
hear more about this. Anaphylaxis is serious and mandates medical attention. This is the UK, at
the very start of a rapid rollout, so I have to think that a major occurrence would spill into
broad alarm that we'd hear.
The CDC report is
here .
Posted by: Grieved | Dec 28 2020 3:24 utc |
76
H.Schmatz , Dec 24 2020 18:35 utc |
17
The origins of the RT-PCR on which it is based our whole strategy against the Covid-19
pandemic, how it was created and in a rush published in a scientific private review, without
obliged previous peer review, and which the conflict of interests are and how some people are
profiting from this pandemic:
Turning science into a botch for profit and at the expense of the health of the whole
world
Merry Christmas! Take care of your and yours!
Top German virologist casts doubt on fears of new 'highly contagious' UK Covid-19
strain 21 Dec, 2020 18:09 Get short
URL
News of a supposedly
highly infectious coronavirus strain being discovered in the UK has led to a flurry of travel
bans. Now, a top German scientist says the mutation might not be as dangerous as we were led to
believe.
The statement that the new strain of Covid-19 is 70 percent more contagious is nothing, but
a claim made by politicians so far, Christian Drosten, the head of the virology department at
the Berlin's Charite center -- one of Europe's largest university hospitals -- told the German
radio broadcaster Deutschlandfunk.
"Suddenly, there is this figure out there, 70 percent, and no one even knows what is
meant by that," he said. The virologist believes there is just not enough data to really
say that the new strain is any more dangerous than the other existing ones.
ALSO ON RT.COM New
Covid-19 strain found in UK spreads FASTER, is already in nearly 60 local authority areas
– health secretary
The data provided by the British scientists on the new strain is still incomplete, Drosten
said, adding that even preliminary analysis results would arrive within a week. The fact that
discovery of a new strain coincided with a sharp rise of new infection cases in southeast
England also does not necessarily mean that the new virus is to blame, the virologist
believes.
"The question is whether the virus is to blame or whether it was just a local epidemic
outbreak, or the lockdown was not so strict and transmission mechanisms were in place in an
area where this particular strain happened to be," he said.
It was also too early to say whether this virus actually transmits faster. To do so, one
needs to "look at who infected whom and how long it took," Drosten explained, adding
that "one would be surprised" if such a parameter as the virus infectiousness would
significantly change all of a sudden now.
What is known so far is that a mutation present in the new strain lets it form a stronger
binding with human cells. Still, according to Drosten, that does not automatically mean quicker
reproduction since the virus stays with one cell for a longer period of time than it could and
probably should to successfully replicate.
ALSO ON RT.COM EU countries shutting
down travel to and from UK amid new highly infectious Covid-19 strain scare
The scientist also said that similar coronavirus mutations already repeatedly appeared
during the pandemic only to disappear at some point. He also said that the new strain is
unlikely to affect any coronavirus vaccine's effectiveness since an immune response formed
through vaccination is a complex process that would hardly be affected by a minor change in the
virus structure.
Still, Drosten admitted that the officials were right to be cautious and temporarily ban all
travel to and from the UK now that the whole situation is still unclear. "Of course, as a
politician, one has to act out of caution here," he said, adding that the current policy
approaches could be "corrected" once more information is available.
The discovery of a new coronavirus strain prompted many nations to suspend all travel to and
from the UK. The list of countries that joined the international quarantine of the UK includes
the Netherlands, Belgium, Italy, France, Germany and Poland, as well as Russia. Some nations
outside Europe, like Iran, Argentina, Chile and El Salvador also cut transportation links with
the UK.
Turkey and Saudi Arabia, meanwhile, suspended travel not just to the UK but to other nations
as well. The moves came as British Prime Minister Boris Johnson said that the new Covid-19
strain is supposedly 70 percent more contagious and announced a strict Tier 4 lockdown in part
of the country, including London.
ALSO ON RT.COM Russia
halts flights to UK for a week as world reacts to news of newly detected British Covid-19
mutation
Like thi
qasimodo 8 hours ago 21 Dec, 2020 05:44 PM
Certain countries try to portray this Covid as the plaque. If we remember even the WHO
confirmed that the Covid is way milder than the common flu. So if we are not obliged to get a
flu shot, we certainly don't need the Covid "God knows what's in it" vaccine. In the winter
months, especially December every year millions of people get the flu, and in some cases its
unfortunately deadly. But the authorities are trying to say that every case of the flu is
Corona virus which is basically a big lie. It is something new, but way milder and in most of
the cases our body can fight it off. Vaccination is being rushed, the FDA had no real
solution to resolve the ifs and buts, and now out of a sudden they have approved it, and we
have a deadly virus that's going to vipe our civilisation of the planet?That's a lot of
disinformation and rubbish. But the big question is liability? These farmaceutical giants
clearly say that in case of any trouble they won't be liable? So why would anyone want it if
there's no guarantee for a human life? If someone thinks that the vaccine is going to save
us, they are just delusional. Get a flu shot if you badly want to stop the panic and you will
be OK. The Covid 19 vaccine in my opinion is a rushed experiment, and needs time to prove
itself worthy...
Guest 11 hours ago 21 Dec, 2020 03:31 PM
It's a single amino acid change in the spike protein associated with the ACE receptor
mechanism that gives the virus access to a cell. There are many such changes going on and it
came via Europe and did not original in the UK. Talk about talked up, hyperboli and general
incompetence. And I'm not talking about this article!
Hoarsewhisperer , Dec 22 2020 2:14 utc |
32
In a press conference on Saturday, Chief Science Adviser Patrick Vallance said B.1.1.7,
which first appeared in a virus isolated on 20 September, accounted for about 26% of
cases in mid-November. "By the week commencing the ninth of December, these figures were much
higher," he said. "So, in London, over 60% of all the cases were the new variant."
Johnson added that the slew of mutations may have increased the virus' transmissibility by
70%.
Not being an ??-ologist, that paragraph indicates to me that a virus with greater
transmissibiliy will REPLACE/DISPLACE the original Covid19 strain. Since the emerging
consensus among virologists is that the B.1.1.7 variant is no more deadly than the original,
then the only reason it matters is that more people will catch the mutated version than would
have caught COVID19 - thus putting more pressure on an already over-stressed healthcare
system.
Since it looks as though a vaccine isn't going to be a Silver Bullet for many months, if
not many, many months, I find it peculiar that more effort wasn't expended on pursuing a
TREATMENT to reduce the severity of COVID symptoms.
I caught CGTN News this morning and China has officially abandoned a 'promising' TREATMENT
it was working on because the stats indicate that it doesn't work...
Petri Krohn
77
I do not think the B.1.1.7 strain is any more infectious than over SARS-COV-2 strains. It
prevails because UK has reached a level of herd immunity against the other strains.
It is falsely claimed that a 70% infection rate is required for herd immunity. The 70%
applies to vaccines, which are distributed evenly throughout the population. For the epidemic
to calm down only a very small portion of the population needs to become immune. This same
population is most likely to spread the infection but also most likely to be infected. For
any vaccination campaign it would be difficult to find this vector population, but the virus
will find it all by itself. It now seems that this vector population is young people who
frequent bars and nightclubs. A bartender in
ski resorts can infect hundreds, but he is also most likely to be first infected.
"British medical journal The Lancet published research on Phase I and Phase II clinical
trials of the vaccine, revealing no adverse effects in patients and triggering an effective
immune response. More than 50 countries have requested roughly 2.4 billion doses across India,
Brazil, China, Argentina, South Korea and numerous others."
Posted by: groucho | Dec 21 2020 1:02 utc |
47
groucho , Dec 20 2020 19:50 utc |
19
CDC Launches Probe, Issues New Guidelines After Thousands Negatively Affected Following New
Covid Vaccine"
As of Dec. 18, 3,150 out of 272,001 recipients reported what the agency terms "Health
Impact Events" after getting vaccinated. The definition of the term is: "unable to perform
normal daily activities, unable to work, required care from doctor or health care
professional."
The problem is that CT ( number of amplifications) is an arbitrary and is not reported.
See https://www.gene-quantification.de/real-time-pcr-handbook-life-technologies-update-flr.pdf
WHO (finally) admits PCR tests create false positives Warnings concerning high CT value of
tests are months too late so why are they appearing now? The potential explanation is
shockingly cynical. Kit Knightly
The World Health Organization released a guidance memo on December 14th, warning that
high cycle thresholds on PCR tests will result in false positives .
While this information is accurate, it has also been available for months, so we must ask:
why are they reporting it now? Is it to make it appear the vaccine works?
The "gold standard" Sars-Cov-2 tests are based on polymerase chain reaction (PCR). PCR
works by taking nucleotides – tiny fragments of DNA or RNA – and replicating them
until they become something large enough to identify. The replication is done in cycles, with
each cycle doubling the amount of genetic material. The number of cycles it takes to produce
something identifiable is known as the "cycle threshold" or "CT value". The higher the CT
value, the less likely you are to be detecting anything significant.
This new WHO memo states that using a high CT value to test for the presence of Sars-Cov-2
will result in false-positive results.
To quote their own words [our emphasis]:
Users of RT-PCR reagents should read the IFU carefully to determine if manual adjustment
of the PCR positivity threshold is necessary to account for any background noise which may
lead to a specimen with a high cycle threshold (Ct) value result being interpreted as a
positive result.
They go on to explain [again, our emphasis]:
The design principle of RT-PCR means that for patients with high levels of circulating
virus (viral load), relatively few cycles will be needed to detect virus and so the Ct
value will be low. Conversely, when specimens return a high Ct value, it means that many
cycles were required to detect virus. In some circumstances, the distinction between
background noise and actual presence of the target virus is difficult to ascertain.
Of course, none of this is news to anyone who has been paying attention. That PCR tests
were easily manipulated and potentially highly inaccurate has been one of the oft-repeated
battle cries of those of us opposing the "pandemic" narrative, and the policies it's being
used to sell.
Many articles have been
written about it, by many experts in the field, medical
journalists and other
researchers . It's been commonly available knowledge, for months now, that any test using
a CT value over 35 is potentially meaningless.
Dr Kary Mullis, who won the Nobel Prize for inventing the PCR process, was clear that it
wasn't
meant as a diagnostic tool , saying:
with PCR, if you do it well, you can find almost anything in anybody."
And, commenting on cycle thresholds, once said:
If you have to go more than 40 cycles to amplify a single-copy gene, there is something
seriously wrong with your PCR."
The MIQE guidelines for
PCR use state:
Cq values higher than 40 are suspect because of the implied low efficiency and generally
should not be reported,"
This has all been public knowledge since the beginning of the lockdown. The Australian
government's
own website admitted the tests were flawed, and a court in Portugal ruled they
were not fit for purpose .
Even Dr Anthony Fauci has publicly admitted that a cycle
threshold over 35 is going to be detecting "dead nucleotides", not a living virus.
Despite all this, it is known that many labs around the world have been using PCR tests
with CT values over 35, even into the low 40s.
So why has the WHO finally decided to say this is wrong? What reason could they have for
finally choosing to recognise this simple reality?
The answer to that is potentially shockingly cynical: We have a vaccine now. We don't need
false positives anymore.
Notionally, the system has produced its miracle cure. So, after everyone has been
vaccinated, all the PCR tests being done will be done "under the new WHO guidelines" ,
and running only 25-30 cycles instead of 35+.
Lo and behold, the number of "positive cases" will plummet, and we'll have confirmation
that our miracle vaccine works.
After months of flooding the data pool with false positives,
miscounting deaths "by accident" , adding "Covid19
related death" to every other death certificate they can stop. The create-a-pandemic
machine can be turned down to zero again.
as long as we all do as we're told. Any signs of dissent – masses of people refusing
the vaccine, for example – and the CT value can start to climb again, and they bring back
their magical disease .
Hugo
In an interview, Dr. Wodarg said he had checked his own blood oxygen saturation with a
simple test on his finger after wearing a mask for several minutes. It had dropped from 98
to 94 percent. It is different when climbers hike in regions with low oxygen levels; the
organism gets used to this and reacts by producing red blood cells. 50 percent of the
oxygen we take in is consumed by our brain alone.
That is why the consequences for children wearing a mask are so devastating: their
brains are still growing. The constant inhalation of their own carbon dioxide makes them
sleepy, lame, unfocused and listless. In addition, the mask creates a hotbed of moisture in
which germs thrive. If, on the other hand, we snort into the crook of our arms, they dry
out. Open windows prolong life. Especially for smokers, whose organism is pre-damaged, for
example, by a lifelong lack of oxygen.
TFS
Former Brexit Party letter to the Secretary of State for Health:
Testing for Coronavirus and Government lockdown policieshttps://www.thebrexitparty.org/letter-to-secretary-of-state-for-health/
JudyJ
TFS
Excellent letter, reply requested by 22 December. A long list of questions to be
answered but, if the Government truly has a grip on what they are doing and can demonstrate
that they have the supporting evidence, the questions should not be difficult to answer.
When I was a civil servant in a London HQ many years ago now, we regularly received
requests like this, often with 24 hours notice to reply, and we would have to drop
everything else to deal with them. All the receiving Minister's office do is send the
request to the appropriate policy unit where responsibility for drafting answers could be
shared between any number of staff – one member of staff might deal with, say, three
simple questions or one more complex question. But meeting the deadline should not be a
problem if one assumes the information is readily accessible as we would be led to believe.
We shall see.
Quote from letter: "We trust that this letter will be taken seriously"
In my best pantomime voice 'Oh no it won't.'
aspnaz
Read chapter 11 "What happened to the scientific method" of Kary Mullis's (inventor of
the PCR test) "Dancing in the mind field" ( https://b-ok.cc/book/1523791/8aa4c2 ) to get his
take on why these people are so corrupt.
In summary, he describes what I would call the "Science Industrial Complex" which is
basically useless people leaching money from the government teat by creating "imminent
disasters" that scare the population, and hence motivate the politicians, into handing out
research grants for the most ridiculous projects without any real scientific proof, such as
climate change.
Here is an extract:
Imagine two hypothetical labs competing for public funds.
from "Dancing in the mind field" by Kary Mullis, inventor of the PCR test.
-CO
aspnaz
There are different sciences that use different methods. The so-called "scientific
method" itself is based on speculative philosophical principles that cannot be proven in or
by science since they specify the very conditions required for the scientific knowledge
process to exist and to operate.
aspnaz
-CO
Mirriam-Webster defines it as: "principles and procedures for the systematic pursuit of
knowledge involving the recognition and formulation of a problem, the collection of data
through observation and experiment, and the formulation and testing of hypotheses".
Can you illustrate your point with some examples of scientific methods that differ from
the above?
I think that Mullis is pointing out where the above scientific method, however you may
want to describe it but involving the fundementals of proof of a hypothesis using empirical
evidence, has been overtaken by commercial interests in a way that uses the credibility of
the scientific method to sell untested hypotheses that provide some financial gain to the
sponsor.
norecovery , Dec 19 2020 15:53 utc |
44
Jay @ 24
"Can you clarify what you find questionable about the corona virus vaccines?"
Disclaimer: I am not an epidemiologist or medical professional. I get information from
various sources especially OTHER THAN mainstream media. Some of those credible sources, such
as Dr. Mike Yeadon ,
subsequently have been censored because they don't purvey the medical establishment's
requisite narrative. This is what I have learned:
These COVID-19 vaccines can be characterized as 'experimental.' Some past vaccines have a
spotty record. They typically require many years of clinical trials to determine safety and
efficacy. A vaccine for Coronavirus has never been developed before, in spite of having been
researched to combat previous epidemics of SARS and MERS. This one was completed in a very
short time, and the handling and delivery requirements are stringent.
True efficacy and the protocol used for testing the presence of viral infection in the
relatively small clinical trials are unclear. We know the rt-PCR test to identify the
presence of "COVID-19 infection" has been misapplied on a large scale. The FDA approval of
these vaccines is based on that test, which has been proven to show a large proportion of
false positives. A Portuguese high court ruled against the legality of this test to determine
infection. Effectiveness of a vaccine is probably very short term, possibly only a few weeks.
It is unknown whether natural immunity in a healthy individual (the body's own defense) might
be equally effective.
Potential side effects are yet to be revealed, besides the few documented cases of
allergic reactions thus far. Potential long term health impacts are unknown, and due to the
Pfizer-BioNTech and Moderna vaccines' 'invasion' of the body with mRNA at the cellular level,
they could be serious. Only time will tell, so one must ask, "do I want to volunteer to
become a clinical test subject?"
Social controls, so-called "immunity passes" which may not even have validity, are an
infringement on individual freedoms and rights and are already being used in some places.
That also paves the way for future vaccination requirements against a person's will, and
given the financial imperatives of the medical establishment and its collusion with
oligarchs, there may exist ulterior motives that are unacceptable.
Norwegian , Dec 17 2020 15:52 utc |
8
@vk | Dec 17 2020 15:44 utc | 6
SECOND health worker in Alaska suffers allergic reaction after getting Pfizer Covid-19 jab
librul , Dec 17 2020 16:33 utc |
14
I just archived the following webpage at http://web.archive.org/
https://www.historyofvaccines.org/content/articles/vaccine-development-testing-and-regulation
This stage involves basic laboratory research and often lasts 2-4 years.
Many candidate vaccines never progress beyond this stage because they fail to produce
the desired immune response. The pre-clinical stages often lasts 1-2 years and usually
involves researchers in private industry.
I happen to have scheduled an appointment with my primary care doctor early in
January.
My first question will be about *which* vaccine.
I just found this quote somewhere:
Note to self: "feel quite happy about that".
Maybe there is actually something to the good doctor's advice
Smile, don't be a corpse.
librul , Dec 17 2020 20:47 utc |
37
@Posted by: librul | Dec 17 2020 16:33 utc | 14
I posted @14 an article. Here is a section from the article I didn't mention.
VAERS
The CDC and FDA established The Vaccine Adverse Event Reporting System in 1990. The goal
of VAERS, according to the CDC, is "to detect possible signals of adverse events associated
with vaccines." (A signal in this case is evidence of a possible adverse event that emerges
in the data collected.) About 30,000 events are reported each year to VAERS. Between 10%
and 15% of these reports describe serious medical events that result in hospitalization,
life-threatening illness, disability, or death.
VAERS is a voluntary reporting system. Anyone, such as a parent, a health care provider,
or friend of the patient, who suspects an association between a vaccination and an adverse
event may report that event and information about it to VAERS. The CDC then investigates
the event and tries to find out whether the adverse event was in fact caused by the
vaccination.
Over 4,000 adverse reactions (hospitalization, life-threatening illness, disability, or
death) to vaccines are *reported* each year.
I would say let's see what next year's numbers are. Except who the heck will trust their
numbers?
Vaccines were clearly rushed. Also the nature of coronaviruses makes creation of vaccine like
shooting at moving target. So each of them is more dangerous then usual and it is unclear how
useful they are. How much it is difficult to tell.
Norwegian , Dec 17 2020 17:35 utc |
21
Clearly, the lockdowns and medical tyranny is not a phenomenon isolated from the power
struggle, it is obviously a weapon of the establishment, used against the people, to prevent
them from organizing independently.
I am also hearing considerable chatter that many medical professionals including doctors
and nurses are going to REFUSE to take the poorly tested and questionable Covid vaccine for
fear of damaging side effects. And why should they? Why take a vaccine for a virus that
only threatens less than 0.3% of the public outside of nursing homes?
We have to offer people a choice outside of tyranny, otherwise many will go along with the
tyranny.
Thanks again.
utu December
15, 2020 at 4:29 pm GMT • 7.4 hours ago
@Bert anonymous
pro HCQ people that IMO were completely flawed.
' vitamins D and C " . – Is there a decease that a claim that vitamins C and
D are a panacea for it would not be heard?
" Latin America and South Asia " – There is good reason that in Western
science double blind studies are believed to be necessary to verify various claims. There are
places in the less developed countries that are less strict and it is very likely that they
jump to unwarranted conclusions by Western science standards. Should the claims coming from
the third world be researched and evaluated in the West? Yes, absolutely.
Notable quotes:
"... PCR-tests (their essential details are not known to you or me) can be easily used to artificially, adjust" the number that you need as a legitimatization for your politics. Yes, there are without doubt that many dead people. ..."
Down South , Dec 13 2020 21:06 utc |
36
So let me point out the key part for you:
the paper that established the Drosten PCR test for the Wuhan strain of coronavirus that
has subsequently been adopted with indecent haste by the Merkel government along with WHO
for worldwide use–resulting in severe lockdowns globally and an economic and social
catastrophe–was never peer-reviewed before its publication by Eurosurveillance
journal. The critics point out that, "the Corman-Drosten paper was submitted to
Eurosurveillance on January 21st 2020 and accepted for publication on January 22nd 2020. On
January 23rd 2020 the paper was online."
Incredibly, the Drosten test protocol, which he had already sent to WHO in Geneva on 17
January, was officially recommended by WHO as the worldwide test to determine presence of
Wuhan coronavirus, even before the paper had been published.
As the critical authors point out, for a subject so complex and important to world
health and security, a serious 24-hour "peer review" from at least two experts in the field
is not possible.
uncle tungsten , Dec 13 2020 21:41 utc |
43
Down South #36
How is it possible that a credible scientific study in the means to test for COVID-19 is
completed, peer-reviewed and accepted as the general standard in less than a couple of
weeks after China announces the emergence of a new virus ?????
Thank you for every word in your post. +++ The frenetic scramble to demonstrate the
infallibility of private financed science over public funded and cautious institutions seems
to be the driver here. As soon as I grasped the Bill Gates link with the WHO it was clear
that neo liberal economics had engulfed the world leading health institution.
You simply cannot believe their blather as it is entirely at the service of neo liberal
economics and therefore propaganda first, second, and third with a veneer of science fact
somewhere.
Meanwhile USA
passenger flights arrive in Sydney. No doubt 'PCR screened'
Hausmeister , Dec 13 2020 23:03 utc |
50
Down South | Dec 13 2020 21:06 utc | 36 and @vk 30
I applaud you, Down South, and I cannot see the qualification vk has for his claims. I
would not sign each sentence of the Engdahl paper but as a gross evaluation it is
correct.
Hausmeister , Dec 13 2020 23:54 utc |
59
vk | Dec 13 2020 23:17 utc | 53
Sorry, that is nonsense. The Drosten paper has not been peer-reviewed. That first. How
deep the scientific flaws in it are neither you or I can assess. And the hair-rising
conflicts of interest were never communicated.
As sad canuck | Dec 13 2020 22:45 utc | 48 showed with a brilliant example these
PCR-tests (their essential details are not known to you or me) can be easily used to
artificially, adjust" the number that you need as a legitimatization for your politics. Yes,
there are without doubt that many dead people. But again: in this politicized
environment neither you nor I know what the reason of their death was.
William Gruff , Dec 13 2020 23:57 utc |
60
...Even if we assume that half of the PCR covid results are false positives, what would
that establish? Wouldn't that just demonstrate that the fatality rate is twice as high? And
isn't diagnosis still done by a doctor anyway? The tests are just screening.
Basically, what is with the hyperventilating about false positives? What am I missing
here?
vk
19
7) China is doing PCRs since the dawn of time and there is not an explosion of new cases
as the anti-PCR squad is claiming. On the contrary: when they decided to re-test all the
Wuhan inhabitants with obligatory PCR tests, they found none, zero, nada positive
results.
Blue Dotterel , Dec 13 2020 19:00 utc |
22
Posted by: Down South | Dec 13 2020 17:55 utc | 16
As I understand it, the false positives are a result of poorly conducting the analyses
through putting the samples through too many cycles. If you intensify the concentration of
the virus more than 25 cycles, you are likely to get false positives. This apparently has
been a problem in the US and other EU countries.
Any country that conducts the test properly significantly reduces the probability of false
positives.
Most likely China, among others, does it properly
Down South , Dec 13 2020 19:51 utc |
25
Blue Dotterel @ 22
Exactly so.
None of them are arguing that COVID-19 does not exist, it is that the maximum reasonably
reliable Ct value is 30 cycles.and as you increase the cycles above that you start getting
more false positive results as only non-infectious (dead) viruses are detected.
The issue that the report raised is that the WHO and Drosden are recommending a Ct of
45 . The higher the cycles the more the "cases" the more drastic the action the
government will take to bring the number of "cases" down.
Therefore, to ensure that the government action is reasonable it is necessary to ensure
that the information the government is using to justify such action is indeed reasonable and
justifiable.
You have to be an absolute idiot to think that government diktats should simply be obeyed
and not questioned especially by people who have the necessary credentials to evaluate such
information.
js , Dec 13 2020 22:28 utc |
47
Well, it is sad to note absolute lack of intellectual curiosity about something that most
likely will not pass without profoundly changing western societies. On side note it would be
good to recognise both taoist and christian way of handling the exception of sickness –
being sick of sickness is way less dangerous than people being religiously afraid of
contamination, of sick people, and organising accordingly.
Most likely this, now already mental, curse will not pass before one or all of the
following happens:
One could say these are the markings of global sanitary dictature. Or, this could be the
way to make formal the hidden features of the system currently in use. The spooky license
will be made official. All the tracking, etc.
The Drosten testing non-protocol is faulty to the core, and – without doubt –
it is enabling corruption of both politics and science (cormandrostenreview.com).
Resulting actions are criminal in their essence – that is the reason why we are
seeing leaders of nations acting in such a bizarre way. The truth is being established by the
means of spectacle. Once harsh and overdecisive, then lacking in resoluteness – even in
the EU the countries still can not coordinate simple and relevant statistics.
China has nothing to gain from this virus, hence there it is mostly over and done with.
Seems to go for Russia as well.
Still, they are playing the ball. Wonder why?
sad canuck , Dec 13 2020 22:45 utc |
48
vk @ 40 said "of course the scientific standards for times of emergency do fall because of
time constraints. That doesn't mean the debunk attempts aren't equally flawed".
I'm sorry but this is not the way science works and cutting corners during emergencies is
an even worse practice. The amplification issue, lack of Standard Operational Protocol, and
clear bias and hijacking of the peer review process for this paper which formed the
foundation of PCR implementation is utterly and completely outrageous. But of course not
surprising. It's clear that all UN agencies including WHO have been corrupted. Right from the
beginning there has been a consistent and widespread effort to discredit any testing method
aside from PCR. Are you not even remotely interested why?
It's easy to see how COVID testing with a flawed PCR testing procedure rolls out and I
will give you an example from a place that I am familiar with. COVID has magically
disappeared in Thailand, but large number of positive cases are appearing in Thai who are
returning and in foreign visitors. These PCR positives are occurring in spite of all
returnees having tested negative just prior to boarding their flight to Thailand. Almost all
of the positives in returning residents are also of the asymptomatic variety. I would wager
that the amplification level for a domestic PCR test is 25 while the returning resident test
level is set at 35 or higher. Lacking transparency and a Standard Operational Protocol for
the RT-PCR test, including a universally accepted amplification level, you can create any
result you want, any time, any place. These are serious issues and you can't label people who
have issues with scientific integrity as deniers or misleading.
The entire justification of PCR as a public health tool (as opposed to a diagnostic tool)
has been vaporized and I cannot for the life of me understand why you don't "get it" or the
wider implications.
b
13
Accidentally deleted this comment by gm:
EARLY OUTPATIENT TREATMENT Protocols & Strategies to manage COVID-19 Pandemic Dr Peter
McCullough,11/27/20https://www.youtube.com/watch?v=kJ1fkKqK7T8
gm , Dec 13 2020 17:35 utc |
14
RE: "None of these experts talk about the way to stop COVID before it hits"
-Posted by: Lurk | Dec 13 2020 17:13 utc | 11
That is not correct in the case of Dr. McCullough.
In both the late Oct YT at #8 and the late Nov YT at post #9 he addresses the "Four
Pillars of Pandemic Response", with the first pillar being *preventative actions*
(masks/transmission limiting measures/index case tracking etc).
McCullough also points out in the latter YT that, in the case of the US, Canada, UK and
much of western EU, 'First Pillar' measures have failed miserably to stop the resurgent wave
of covid.
In late November Debs is dead and I wrote about the ruthless
vaccine competition . The cause were the ambiguous results of the non-profit AstraZeneca
vaccine trials which led to delighted criticism from those who prefer commercial vaccine
suppliers.
The good news today is that cooperation between vaccine developers is still possible and can
lead to better results.
As Debs had opined:
In the real world that means if the AstraZeneca vaccine is more than 60% efficacious (which
is better than any flu vaccine - 95% is new big pharma BS IMO) and has no major side effects
(one case of MS tells us nothing for the reason I outlined above), then it will be that or
nothing for a sizeable slab of the world's population.
If everyone falls for big pharma's transparent attempt to stop this possible vaccine in
its tracks, prior to testing completion, then that will mean no vaccine for billions of our
fellow humans , so rather than joining in the big pharma sabotage, it makes better sense to
consider that vaccine more objectively than de Noli, that Harvard minion of corporations
seems to do.
I agreed with that and discussed the most likely reason why the AstraZeneca vaccine did not
create a higher efficacy:
The AstraZeneca vaccine uses an adenovirus as 'vector' to deliver a DNA sequence that human
cells then use to create one specific (but harmless) SARS-CoV-2 protein. The immune system
will then learn to attack that protein. Afterwards it should be able to protect against
SARS-CoV-2 infections.hyped by Prof. de
Noli on RT , uses two doses with different human adenoviruses (Ad-26, Ad-5) as
vectors to increase the chance of inoculation. Other vaccine developers, CanSino Biologics
and Johnson & Johnson, are also using adenovirus vectors. Sinopharm's vaccine uses an
inactivated SARS-CoV-2 virus.
AstraZeneca found by chance that its vaccine works best when the first dose is smaller
than the second one. Vector immunity can explain why this is the case.
A first high dose will create some immunity against the SARS-CoV-2 virus but also some
immunity against the vector virus, the chimpanzee-originated adenovirus. When a first high
dose has trained the immune system to fight the vector virus the second 'booster' vaccine
dose using the same vector will become inefficient. A lower first dose can make sure that the
second higher dose is not prematurely defeated by vector immunity but can still do its
work.
Unbeknownst to me the Russian developers of the Sputnik V vaccine had come to the same
conclusion:
Notable quotes:
"... Multiple COVID-19 vaccines are currently in phase 3 trials with efficacy assessed as prevention of virologically confirmed disease. WHO recommends that successful vaccines should show disease risk reduction of at least 50%, with 95% CI that true vaccine efficacy exceeds 30%. However, the impact of these COVID-19 vaccines on infection and thus transmission is not being assessed. Even if vaccines were able to confer protection from disease, they might not reduce transmission similarly. ..."
"... A note before I begin: This is not a recommendation not to be vaccinated against Coronavirus. It's an encouragement to decide for yourself and your family when to be vaccinated and which vaccine to choose based on the most accurate information available. That said, let's proceed. ..."
"... "Done right, vaccines end pandemics. Done wrong, pandemics end vaccines." -- Andy Slavitt here ..."
"... Based on the numbers released from phase 3 trials, the Pfizer vaccine is 95% effective, but 1% of the time . In the same way, the Moderna vaccine is 94% effective, but 2% of the time . ..."
"... For comparison, let's look at the absolute numbers from the Moderna test. In the unprotected population, 1.23% of the people who could have been exposed to the virus, got it. In the vaccinated population exposed to the same conditions, a little less than 0.07% got the virus. Subtracting the two, the absolute gain in protection was 1.16% -- that is, taking the vaccine bought you a little over 1% in absolute protection. ..."
"... any studies or testing on fertility? what about breast feeding? what about long term symptoms? [ hint ; the manufacturers have nothing] what does that tell you? ..."
"... Pharma/FDA: "We can't worry about that right now. We have a pandemic to fight. And investors to consider. And year-end bonuses are coming up. And a political class looking for a quick fix." ..."
"... Indeed we can't worry about that now say Pharma, that's why you absolutely must completely indemnify us from any financial repercussions too. ..."
"... just yesterday the Pfizer vaccine vaccine reported a number of issues with allergic reactions. It raised the question on whether they deliberately excluded people with known allergies from their test subjects (this is not uncommon in early drug testing as a safety precaution). If even 1% have a serious allergic reaction, this would throw the benefit/risk balance out. ..."
"... Is it O/Z, or the Pfizer one? NHS yesterday issued a guideline to stop vaccinating anyone with "history of allergic reactions", which was for Pfizer vaccine. ..."
"... That "1% of the time" and "2% of the time" reflects the approximate likelihood that a subject from among the test groups was exposed to a high enough dose of SARS2-CoV to cause symptoms and a positive PCR test over the course of the trial. It has absolutely zero to do with the efficacy or lack thereof of the vaccines. Let me repeat that. The overall proportion of infection among all trial participants has no bearing, in and of itself, on the actual efficacy. ..."
"... As such, this Pfizer vaccine and possibly the Moderna one too if it has the same problem, will require that patients be monitored for anaphylactic symptoms for some significant duration of time (an hour?) after the injection. Now consider this potential possibility in light of the other logistical difficulties surrounding the vaccine distribution and administration to huge numbers. It probably won't be via drive-thru service. ..."
"... Well, the anaphylaxis, regardless of state of health, indicates that there are antigens present in the formulation which are unrelated to the protein the vaccine will manufacture in cells. While it can even be a mucopolysaccharide rather than a protein, the fact remains that the carrier is not benign and we are not being provided with all the information. ..."
"... Yep, I am wondering of the consequences of rushing out the vaccines and I am convinced the pressure is 99% political. There are governments too eager to announce mass vaccination and putting too much confidence in early reports so worried they are with the socioeconomic impact of the pandemic. And this can show (will show) problematic if mass vaccination is started before a thorough examination of further trial results and problems like allergic reaction and others that might surge in the course of the trials. ..."
"... We provide people very little education and most others end up specialists. Yet at the same time everyone knows everything and needs to know everything because everyone is trying to screw you over. And worse yet, most people do not know that they are stupid or can speak about a topic knowing they are probably wrong. ..."
"... It's all so damn stressful I will just take my chances without the vaccine and be as careful as I can not to infect others. I know a lot about human biology, but not enough about vaccines and the companies and the people who own them. I do not trust the government because it is controlled by corporations and not the people. ..."
"... Can the pharma companies stand behind the claim that it's 95% effective without resorting to numerical semantics or lobbying for liability shields? If so then by all means tell the public that the vaccines are 95% effective. If they say "well we did say it's 95% but what we meant was " then we are in the territory of bait and switch. ..."
"... There's too much at stake to leave even little room for exaggerated claims from profiteers because the anti-vaxxers will have a field day exploiting any discrepancy between claimed and actual performance for these vaccines and guess what, with that will go public trust. ..."
"... people are going to alter their behaviour based on these claims once vaccinated, so 95% should mean 95% in absolute terms and contra-indications should also be clearly communicated to at-risk populations. Auditable transparency should be the name of the game, if we've learnt anything from the 737max debacle it's that companies, when left to their own devices, place profit ahead of human lives. ..."
"... Why should Vietnam show a terrible "absolute effectiveness" compared to France if the goal is to analyze the same vaccine? As the number of people exposed to the virus approaches the entirety of the population (if half were vaccinated and all members are susceptible to infection) the number would approach the vaccine efficacy as the companies define it. ..."
"... I would even ditch the '95% effective' language. They need to say 'if 10,000 people were exposed to the virus, ordinarily about n1 would get infected. With this vaccine, the number infected was n2. This is language people can grasp. ..."
"... I was born three years before doctors began giving a new drug on the market declared safe in pregnancy to mothers for morning sickness. It was called Thalidomide. ..."
"... The second surprise from these protocols is how mild the requirements for contracted Covid-19 symptoms are. A careful reading reveals that the minimum qualification for a case of Covid-19 is a positive PCR test and one or two mild symptoms. These include headache, fever, cough, or mild nausea. This is far from adequate. These vaccine trials are testing to prevent common cold symptoms. ..."
"... A temperature of 104.9 in an adult with a functional immune system (we are not talking about babies and kids – they are different) is extraordinary after a vaccination. 104.9 means that the immune system has been activated enough to take it up a few notches to DEF CON 1. This is very unusual in infectious disease – some parasites and ameba do this routinely – and things like sepsis syndrome can – but for the most part, getting a temperature up this high is definitely not normal. It is certainly not a good sign for a vaccine. A vaccine should not be stimulating the immune system to this degree – EVER. Idiosyncratic reactions in a very rare patient is one thing – if this is happening more often – this is not a good sign for that vaccine. ..."
"... This is medically important for two reasons. 1) That level of fever if sustained can damage permanently multiple organs. 2) Vaccines should simply not be activating the immune system to that degree – it is completely inappropriate. It is very normal for people to have a brief temp of 99 or 100 after a vaccine – this is a completely different level. ..."
"... The Vaccine Drumbeat in my jurisdiction is increasing and I'm sure will become deafening. Talk show radio hosts actually giving medical advice. No recommendations to consult with a doctor regarding your personal health circumstances and risks or those of your loved ones. ..."
"... This is all orchestrated by Public Health officials who apparently have never heard of personal health care. We are all just one big Herd. To me this is a desecration of the doctor patient relationship by so-called health professionals. All of which is extremely dangerous and bad medical advice. ..."
"... Re: companies mandating staff to be vaccinated to market their establishments as "safe". The tone and substance of the post is clearly meant to be a "proceed with caution" advisory on taking the vaccine, despite the author being at pains to emphasize that it's not an "encouragement to reject vaccines". ..."
"... Don't forget they are using flawed PCR tests and except for Moderna in the US all other countries and companies where studies have been conducted are using another vaccine instead of a true saline or inert placebo. ..."
"... Not to mention most of these Pharmaceutical Companies have been sued for tens of billions of dollars for harmful drugs , buried information, fraud ect. We're supposed to trust them with safety studies for medical products they have indemnity for. Thank you for pointing out how deceptive these numbers can be for the average person. ..."
"... The problem is, given the PCR is acknowledged to generate a lot of false positives, then the success rate will be overstated, because the denominator in the success rate calculations will be swollen with subjects who didn't actually have the CV19 virus to start with ..."
'95% Effective' May Not Mean What You Think It Means
December 10, 2020 by Yves Smith
Yves here. It's good to see Tom Neuburger discussing a possible misperception by some of
what the "95% effective" Covid mRNA vaccine results touted by Pfizer and Moderna mean, when
they are on the verge of receiving an FDA Emergency Use Authorization to allow their
release.
While we have your attention, we'll point out another misperception, which the press is
amplifying, that having been vaccinated would prevent the recipient from transmitting Covid.
For instance, some business owners are saying they will require employees to be vaccinated, not
because they are concerned about worker safety, but because they intend to market their venue
as safe for customers by virtue of having vaccinated staff.
At this point, the effect of any of the Covid vaccines on disease transmission is a known
unknown. From
Wired in late November :
The problem is, a Covid-19 vaccine that only prevents illness -- which is to say, symptoms
-- might not prevent infection with the virus or transmission of it to other people. Worst
case, a vaccinated person could still be an asymptomatic carrier. That could be bad.
The article further points out that so far, only the Oxford/AstraZeneca vaccine has evidence
that it reduces transmission, as opposed to protecting recipients of the disease.
A more technical explanation from The
Lancet , in September:
Multiple COVID-19 vaccines are currently in phase 3 trials with efficacy assessed as
prevention of virologically confirmed disease. WHO recommends that successful vaccines should
show disease risk reduction of at least 50%, with 95% CI that true vaccine efficacy exceeds
30%. However, the impact of these COVID-19 vaccines on infection and thus transmission is not
being assessed. Even if vaccines were able to confer protection from disease, they might not
reduce transmission similarly.
Challenge studies in vaccinated primates showed reductions in pathology, symptoms, and
viral load in the lower respiratory tract, but failed to elicit sterilising immunity in the
upper airways. Sterilising immunity in the upper airways has been claimed for one vaccine,
but peer-reviewed publication of these data are awaited.
The sterlizing immunity claim came
from Phase 1 trials of the Novavax vaccine .
By Thomas Neuburger. Originally published at Substack
Excessive haste could have fatal consequences, since public trust and wide vaccination
are the only ways any vaccine, even the best ones, can work.
A note before I begin: This is not a recommendation not to be vaccinated
against Coronavirus. It's an encouragement to decide for yourself and your family when to be
vaccinated and which vaccine to choose based on the most accurate information available. That
said, let's proceed.
"Done right, vaccines end pandemics. Done wrong, pandemics end vaccines." -- Andy
Slavitt here
People in the United States, along with people in all of the rest of the world, are eager
for a vaccine that provides immunity to the Covid-19 virus. Drug manufacturers, with a market
of tens of billions of injections to sell into, are eager to roll one off the production
line. Both groups are highly incentivized to get a vaccine into distribution quickly.
Hundreds of Billions in Potential Revenue
Let's look at the revenue side first. Here, for example, is what the three leading vaccine
candidates are projected to cost in the UK according to a recent Sky
News piece :
In two years the earth is projected to hold 8 billion
people , and most leading vaccine candidates require at least two doses. Let's be
conservative: If Moderna, say, sold its Covid vaccine to 1 billion people at ₤28 (about
$37) per dose, the revenue stream from those sales would turn into real money fast -- $74
billion in revenue at retail prices in less than two years.And that's for capturing
less than a sixth of the global market. A vaccine manufacturer that captures a third of
that market would swim in wealth till the climate crisis took us all.
For comparison, consider Moderna's recent revenue profile .
For the last few years, Moderna income has run between $60 and $200 million per year. Revenue
for just the last quarter , however, jumped to $158 million. Moderna is clearly set for
a windfall.
Needless to say, something like $100 billion or more in revenue would more than cover the
cost of Covid vaccine development, so why the high price retail prices? One can only guess.
How Effective Is "Effective"?
About effectiveness, much is claimed. From the same Sky News article:
The UK has become the first country in the world to approve the Pfizer/BioNTech COVID-19
vaccine for use.
The government says the jab [vaccine], which has been given the green light by independent
health regulator MHRA, will be rolled out across the UK from early next week.
Studies have shown the jab is 95% effective and works in all age groups. [emphasis
added]
Moderna claims similar effectiveness -- 94% -- for its own vaccine candidate. But what does
effectiveness mean?
To a lay person, a phrase like "95% effective" means one of two things: either that she or
he, upon exposure to the virus, is protected 95% of the time, or that 95% of the people who
take the vaccine are protected 100% of the time.
And this is where the mutual eagerness of the two highly motivated groups -- the public; the
profiteers -- intersect. The public wants to hear "95% effectiveness" and think it knows what
those words means. The drug companies want the same thing as the public; it wants the public to
think it knows what those words mean.
But in the world of drug advertising, the word "effective" does not mean what you think it means . The other way to
look at effectiveness is this: Based on the numbers released from phase 3 trials, the Pfizer
vaccine is 95% effective, but 1% of the time . In the same way, the Moderna vaccine is
94% effective, but 2% of the time .
Relative Effectiveness
To sort this out, let's look at real numbers, thanks to Twitter friend David
Windt.
For the Moderna product, the phase 3 trial contained 30,000 individuals divided between
those given the vaccine and those given a placebo. Let's assume that individuals in each group
were allowed to roam freely "in the wild" -- that is, told to live their regular lives among
the general population, including going out infrequently, staying masked, and practicing social
distance -- as opposed being proactively and aggressively exposed to the virus by the
researchers, which would be highly immoral, to say the least.
In the Moderna vaccinated group, 11 people out of 15,000 got the virus (by Moderna's
definition of what "got the virus means") for an overall infection rate of 0.07% . (There's
disagreement about whether the drug company's "got the virus" measurements are well chosen; see
the Forbes article "
Covid-19 Vaccine Protocols Reveal That Trials Are Designed To Succeed ." But we'll ignore
that point for now.)
In the Moderna placebo group, 185 people of 15,000 got the virus, for an overall infection
rate of 1.23% .
Do you see where this is headed? If you divide 0.07% by 1.23%, you get a 5.7% infection rate
-- or inversely, a 94% protection rate, which is what's claimed. But that's a percentage of a
percentage, a ratio of a ratio, something called the "relative rate" in the medical profession.
What this really means is that, of the 1.23% of people who would have gotten the virus in the
vaccinated group, 94% of them didn't.
But Moderna isn't testing 30,000 people who are infected with the virus, or even 15,000
people. Only 185 people "got the virus" (by their definition) in the placebo group. That
population was reduced to 11 people with vaccination. These are very small numbers. As stated
above, the Moderna vaccine is 94% effective -- but only 1.23% of the time.
(For another way to see that using a percentage of a percentage, or a ratio of a ratio, is
confusing, consider an advertisement that claims a company's new product is "twice as
effective" as its old one. If the old product was effective only 2% of the time, and you knew
this, would you buy the new one?)
Infection rates in those clinical trials seem low, by the way, which could be just an
accident of statistics, or something off in their way of measuring who is counted as infected.
From the start of the pandemic until now, the overall disease rate for Maricopa County, a
high-infection zone, is 5034 per
100,000 people , or 5% . At the lower end, the overall disease rate for Multnomah County, a
less-infected but still urban county, is 2363 per
100,000 people , or 2.4% .
Both rates are higher than the infection rates of the Moderna and Pfizer placebo groups. As
stated, Moderna's placebo group experienced a 1.23% infection rate, and Pfizer's placebo group
was infected just 0.75% of the time. Does this
indicate a difference in how "infection" is determined, or just something else about these
studies? Hard to tell at this point.
None of this is to imply dishonesty on the part of the drug companies. Measuring
"effectiveness" using the relative rate of infection is common in that world. It's just more
meaningful when the overall infection rate of a pathogen is, say, 70% or higher, instead of 5%
or less.
Absolute Effectiveness
For comparison, let's look at the absolute numbers from the Moderna test. In the
unprotected population, 1.23% of the people who could have been exposed to the virus, got it.
In the vaccinated population exposed to the same conditions, a little less than 0.07% got the
virus. Subtracting the two, the absolute gain in protection was 1.16% -- that is, taking the
vaccine bought you a little over 1% in absolute protection.
The numbers for the Pfizer vaccine are similar. According to Windt , "the
infection rate was reduced slightly, from 0.75% to 0.04% – that's "95% efficacy" [but]
these results do NOT mean that 95% of those vaccinated are protected." In absolute terms,
taking the Pfizer vaccine reduced the risk of getting the virus by just 0.71%.
Do you trust any of these drug manufacturers and their massively under-tested vaccines
enough that you would take whatever risk is associated with their product to gain that amount
of protection? I know good doctors who won't, and others who will.
Testing and Public Trust
I want to point to two articles about testing and public trust. First from MIT in November,
consider
this caution about public trust:
Covid-19 vaccines shouldn't get emergency-use authorization
Public trust in vaccines is already in decline. The FDA should proceed with
caution.
The pace of covid-19 vaccine research has been astonishing: there are more than 200 vaccine candidates in
some stage of development, including several that are already in phase 3
clinical trials , mere months after covid-19 became a global public health emergency. In
order for the FDA to approve a vaccine, however, not only do these clinical trials need to be
completed -- a process that typically involves following tens of thousands of participants
for at least six months -- but the agency also needs to inspect production facilities, review
detailed manufacturing plans and data about the product's stability, and pore over reams of
trial data. This review can easily take a year or more.
Excessive haste could have fatal consequences, since public confidence and wide vaccination
are the only ways any vaccine, even the best ones, can work: "Public health experts caution
that vaccines don't protect people; only vaccinations do . A vaccine that hasn't gained enough
public trust will therefore have a limited ability to control the pandemic even if it's highly
effective." [emphasis mine]
This Forbes article from September, titled "
Covid-19 Vaccine Protocols Reveal That Trials Are Designed To Succeed ," argues that the
vaccine trials it examined measure efficacy by testing for the wrong things -- the absence or
presence of symptoms, especially mild ones:
One of the more immediate questions a trial needs to answer is whether a vaccine prevents
infection. If someone takes this vaccine, are they far less likely to become infected with
the virus? These trials all clearly focus on eliminating symptoms of Covid-19, and not
infections themselves. Asymptomatic infection is listed as a secondary objective in these
trials when they should be of critical importance.
It appears that all the pharmaceutical companies assume that the vaccine will never
prevent infection . Their criteria for approval is the difference in symptoms between an
infected control group and an infected vaccine group. They do not measure the difference
between infection and noninfection as a primary motivation. [emphasis added]
Is this true of the latest trials? Last September is forever in Covid years. I'll look at
this side of the issue in a follow-up piece, but my early research says that the Forbes
point is still valid. If this turns out to be the flaw Forbes thinks it is, public trust
could be even more greatly eroded as these vaccines fail to deliver what's we're led to expect
of them.
To Vaccinate or Not To Vaccinate?
As I said before, this is an not an encouragement reject the vaccines. It's an
encouragement to decide about them wisely by considering a number of factors -- your need to
feel "safe," your need to end this constant quarantine, and society's need to inoculate nearly
everyone, versus your trust in the approval process, your personal level of caution, and the
benefit of taking a relatively untested product to reduce your Covid risk by maybe 2% in
absolute terms.
There are Covid hot-spots after all, areas of the country and the world where
infections are soaring, and even low infection rates come at a heavy price. Covid has changed
for the worse both the way we live and our
economy . And people do die from it.
Maybe the first vaccines out of the gate, perhaps these three, will be everything a mother
could want for her family and nation. But even if these products are are very very good, they
have to be trusted to be effective.
If that trust is given blindly, and then betrayed, the consequences will be severe.
Savita
December 10, 2020 at 3:46 am
any studies or testing on fertility? what about breast feeding? what about long term
symptoms? [ hint ; the manufacturers have nothing] what does that tell you?
Dean
December 10, 2020 at 6:01 am
Pharma/FDA: "We can't worry about that right now. We have a pandemic to fight. And
investors to consider. And year-end bonuses are coming up. And a political class looking for
a quick fix."
Adrian D.
December 10, 2020 at 6:31 am
Indeed we can't worry about that now say Pharma, that's why you absolutely must completely
indemnify us from any financial repercussions too.
Dwight
December 10, 2020 at 1:22 pm
And since media depend on our ad dollars, we can control the PR repercussions.
westkentim
December 10, 2020 at 2:57 pm
The Wodarg/Yeadon petition to the EMA (which, contrary to some reports, does not say "it
causes sterilisation") is worth reading
https://2020news.de/en/dr-wodarg-and-dr-yeadon-request-a-stop-of-all-corona-vaccination-studies-and-call-for-co-signing-the-petition/
Yeadon appears to be being branded as a nut in the mainstream British media (and, indeed,
Associated Press have published an article refuting the allegation that the vaccine causes
sterility, by disproving assertions that Wodarg & Yeadon did not make.) In my book, that
probably means he is not 180 degrees wrong
bob
December 10, 2020 at 4:05 pm
Put "sterilization" in the press release and Karen is going deep undercover to sniff it
out. She knows what's up. She found documents on the website
It's all for the children! ..
PlutoniumKun
December 10, 2020 at 3:48 am
I don't know the answer to this, but just yesterday the Pfizer vaccine vaccine reported a
number of issues with allergic reactions. It raised the question on whether they deliberately
excluded people with known allergies from their test subjects (this is not uncommon in early
drug testing as a safety precaution). If even 1% have a serious allergic reaction, this would
throw the benefit/risk balance out.
The potential harm of getting his roll out badly wrong could be catastrophic for public
health policy for decades to come. I've a very bad feeling that there have been too many
incentives built in to cut corners and fudge data. Who wants to be the mid level scientist in
one of those companies with an awkward question to raise during a weekly meeting? We may well
be throwing a dice and hoping for the best, rather than focusing on getting the right
answer.
vlade
December 10, 2020 at 4:04 am
Is it O/Z, or the Pfizer one? NHS yesterday issued a guideline to stop vaccinating anyone
with "history of allergic reactions", which was for Pfizer vaccine.
If it's just one vaccine, it could be an oversight. If both/all, it could be a real
problem – as you say, a potential catastrophe for decades.
GramSci
December 10, 2020 at 8:04 am
Is the sample skewed?
If I had severe or eve moderate allergies, I wouldn't volunteer for a drug test,
especially given the current state of US health scare.
Stephen the tech critic
December 10, 2020 at 4:18 am
With all due respect, the author and his Twitter friend seem very confused about how to
interpret the efficacy numbers. The quantitative reasoning is fundamentally erroneous.
> The other way to look at effectiveness is this: Based on the numbers released from
phase 3 trials, the Pfizer vaccine is 95% effective, but 1% of the time. In the same way, the
Moderna vaccine is 94% effective, but 2% of the time.
That "1% of the time" and "2% of the time" reflects the approximate likelihood that a
subject from among the test groups was exposed to a high enough dose of SARS2-CoV to cause
symptoms and a positive PCR test over the course of the trial. It has absolutely zero to do
with the efficacy or lack thereof of the vaccines. Let me repeat that. The overall proportion
of infection among all trial participants has no bearing, in and of itself, on the actual
efficacy.
Note that these percentages are smaller than the overall "rate" of infection (proper term
would be "proportion") in e.g. Maricopa Cty, AZ because the latter proportions are with
regard to the entire pandemic whereas the proportions observed in the vaccine studies reflect
the limited duration of the study. Also keep in mind that a fair amount of data collection
likely happened over the summer before the cases started skyrocketing again.
With that said, the problem, such as it is, with the low percentage of people who got
infected is that it reduces the effective sample size, relative to the number of people who
actually enrolled in the study. However, the sample sizes are not so small as to be
inadequate to demonstrate high efficacy for the purposes of these trials.
Now, there are plenty of caveats here if you really want to pick these thing apart. The
author correctly notes that these studies demonstrate efficacy in terms of getting full-blown
symptomatic COVID-19, not in terms of preventing transmission or avoiding the disease
entirely.
Also, the results only apply to the *sampled population*, which are the people among the
test subjects who became positive. Is that population *representative* of the whole
population? Does it include children? The elderly? People of different social class and/or
living situations? People of different "colors"? People with history of severe allergies? And
are the proportions of each of these (and any others I *can't* think of) similar within the
sampled population as in the whole population?
Second, the result assumes that the study is blinded. Blinded means that subjects don't
know whether they have been given a real vaccine or a placebo. If subjects are not blinded,
they may alter their own behavior accordingly. For example, a test subject who knows (s)he is
vaccined might be more nonchalant about social interactions, which could increase their
frequency of exposure to COVID vs. subjects who knew they got placebo.
While the studies themselves have surely taken precautions to avoid accidentally
un-blinding the subjects (unless an adverse reaction occurs, which is handled separately in
the data), the media has reported repeatedly and extensively, while these trails are
on-going, that side-effects are common. This is very bad because this information gives test
subjects knowledge they can use to judge whether they are actually vaccinated or not. Even if
said subjects are wrong in their assessment, simply believing they have extra knowledge can
change their behavior, and if this phenomenon is not identical between the placebo and
experimental groups, it will throw off the results. An analogy in the legal world is how
jurors are advised not to watch or listen to news reports about the trial they are serving
in. Whether they choose to believe or disbelieve the reported information, it has the
potential to harm their impartiality.
By the way, I'm not trying to defend these vaccines or their manufacturers for their own
sake. The author is correct that these vaccines are "under-tested", and I believe pushing
them onto the market so quickly comes with substantial risks, both directly to public health
and indirectly via potential severe damage to trust and credibility. I adhere to the maxim
that Murphy was an optimist, and Murphy would say that there's a lot that can go wrong in
this scenario.
Yves
Smith
December 10, 2020 at 4:44 am
Thanks. I was concerned that the emphasis trying to undercut the 95% claim was overegged,
but I had separately been bothered by how small the effective sample was. It appears the
Pfizer sample was skewed by excluding people who were allergic and not having read their data
release, it isn't clear how up front they were about that (you'd think the NHS wouldn't have
gone about injecting their staff willy nilly and getting two severe bad reactions the first
day if they had had a clue).
Stephen the tech critic
December 10, 2020 at 6:21 am
You're welcome, but I'm not sure I explained as well as I could have.
The reports of serious allergic reactions from the Pfizer vaccine on its debut day
surprised me. I imagined lots of things that could go wrong, but two bad reactions on the
first day? Perhaps these incidents will be limited to people with "a history of serious
allergic reactions", but I also know that anaphylaxis is unpredictable and I know many people
anecdotally who only had such a reaction later in life.
As such, this Pfizer vaccine and possibly the Moderna one too if it has the same problem,
will require that patients be monitored for anaphylactic symptoms for some significant
duration of time (an hour?) after the injection. Now consider this potential possibility in
light of the other logistical difficulties surrounding the vaccine distribution and
administration to huge numbers. It probably won't be via drive-thru service.
Adrian D
December 10, 2020 at 6:50 am
As I understand it the 2 people in the UK who suffered the reaction were aware of their
allergy issues and carried epi-pens, but the allergic effects just weren't flagged in any of
the resources accompanying the rolled-out vaccine or asked of them when they got the jab.
Which rather speaks of a rushed and botched process to me.
Phacops
December 10, 2020 at 9:42 am
Well, the anaphylaxis, regardless of state of health, indicates that there are antigens
present in the formulation which are unrelated to the protein the vaccine will manufacture in
cells. While it can even be a mucopolysaccharide rather than a protein, the fact remains that
the carrier is not benign and we are not being provided with all the information.
In the Adenovirus carrier vaccines the virus shell is in itself immunogenic, which makes a
booster problematic unless, as with Sputnik 5, different adenoviruses are used for the
primary and booster.
I intend to be vaccinated, but I'm witholding judgement until more data is presented about
the currently highlighted vaccines until I see data on either attenuated virus or adjuvated
purified protein vaccines.
Coming from a time before polio vaccination, what I have not lost sight of is the fact
that vaccination in general has been breathtakingly successful in improving and maintaining
our health at low cost.
larry
December 10, 2020 at 9:07 am
AZ say that Phase III of their trials was double blind with 40k subjects. The official
title of the study is A Phase III Randomized, Double-blind, Placebo-controlled Multicenter
Study in Adults to Determine the Safety, Efficacy, and Immunogenicity of AZD1222, a
Non-replicating ChAdOx1 Vector Vaccine, for the Prevention of COVID-19 whose start date was
August 2020, Primary completion date as March 2021, and Estimated study completion date as
February 2023. A lttle more data can be found at https://clinicaltrials.gov/ct2/show/NCT04516746
(ClinicalTrials.gov of the NIH).
One could be forgiven for thinking that the trials are currently not finished. If so, does
that mean the vaccine was rushed out with all the consequences resulting from that?
Ignacio
December 10, 2020 at 12:51 pm
Yep, I am wondering of the consequences of rushing out the vaccines and I am convinced the
pressure is 99% political. There are governments too eager to announce mass vaccination and
putting too much confidence in early reports so worried they are with the socioeconomic
impact of the pandemic. And this can show (will show) problematic if mass vaccination is
started before a thorough examination of further trial results and problems like allergic
reaction and others that might surge in the course of the trials.
It is absolutely unwise to throw ourselves into a rush based on early reports that account
for very little exposure time and which are biased by the nature of the vaccine. One cannot
even suppose that the placebo group and the vaccinated group behaved similarly given the high
reactogenicity reported by the vaccines (particularly the RNA vaccines). This reports were
obtained with data gathered about 12 weeks after the trial start. Imagine, given that two
shoots were provided and each shoot produces quite a nasty reaction that can last nearly a
week, nearly 20% of the time the subjects that were vaccinated were suffering symptoms
related with the vaccination and this would alter their behaviour significantly compared with
the placebo subjects.
Given the time course of antibody production after vaccination, with a peak shortly after
the second shoot, the results are biased by the peak and the real protective rate will be
different when specific immunoglobulin levels decline. One can consider this 95% efficacy as
transient efficacy and we will almost certainly see that further data reveals a sharp
reduction. Repeating 95%! 95! all the time will probably result in a sense of deception later
that could be counterproductive.
I don't think data is fudge, that would be really, really stupid, but it is being badly
misinterpreted and can conduct to cutting corners to mass deployment with unintended
consequences.
Yves
Smith
December 10, 2020 at 4:15 pm
Yes, but as the post does explain, that 40K participants translates into a very small
number that contracted the disease (and in the injection group, were assumed to have gotten
it but beat it back). So the effective sample was way way smaller.
Phacops
December 10, 2020 at 10:16 am
Exactly. The number of infections are so small that while one may estimate efficacy, the
power of the estimate (beta error; calling something true when it is in fact, false) is high.
The best I could really see statistically given the data is the ability to reject the null
hypothesis in a F-test (no difference between the groups) with reasonable confidence (1
– alpha; the chance of rejecting something as false when it is in fact true).
As with any sample from a larger population, it is important to understand the uncertainty
of the estimate, which at least Oxford/AZ is providing.
Otto V.
December 12, 2020 at 7:18 am
They published the CI, and if I recall correctly it was 95% of something like 92%-98.5%
effective. The sample size was just big enough to calculate it, but just so. But what's more
important, in my opinion, is that the method they used to calculate the effectiveness of the
vaccine are the same they use for every other vaccine. I.e.: they're not doing exception for
this one, which is important. We know it's a Phase III study with the limitations of all
Phase III studies.
David
December 10, 2020 at 6:09 am
Ah, thanks. I was puzzled by the argument, because it seemed a bit like saying that
routinely carrying umbrellas did not provide 95% protection against rain because it only
rained some of the time. More relevantly, though, consider vaccinations against tropical
diseases. I've had many and need to check on them before I go to certain countries. They are
generally considered highly effective – it's assumed, 100% or nearly so in some cases.
But if, say, 10000 vaccinated people visit a country in the course of a year, but only 500
come into contact with a contagious source (which would not be surprising) and none get ill,
then the efficacy of the vaccine would presumably only be 0.05% according to the logic of the
article. So what, as a layman, am I missing, (apart from the issue of sample size)?
Stephen the tech critic
December 10, 2020 at 6:31 am
> Ah, thanks. I was puzzled by the argument, because it seemed a bit like saying that
routinely carrying umbrellas did not provide 95% protection against rain because it only
rained some of the time.
Exactly, and thanks for your concise example.
Thuto
December 10, 2020 at 7:11 am
isn't this precisely why the burden of interpreting the efficacy claims shouldn't be
offloaded to the general public? If the numbers require a level of maths proficiency not many
can lay claim to to interpret then therein lie opportunities for misrepresentation via
numerical sleight of hand, which if history is anything to go by, will be exploited to
hoodwink an unsuspecting public, especially with a pot of gold filled to the brim with
billions of dollars lying in wait. Most laymen don't have the maths chops to pick apart the
claims and will most likely throw their hands in the air and walk away with "it's 95%
effective" as the takeaway, caveats of data interpretation be damned. The efficacy should be
communicated to the public in as simple and absolute terms as possible, in a language that is
a sharp departure from that usually employed in the fine print of legal documents to make
things unintelligible while embedding opportunities for plausible deniability should things
go belly up.
Krystyn Podgajski
December 10, 2020 at 7:56 am
I think what was said here is important. We provide people very little education and most
others end up specialists. Yet at the same time everyone knows everything and needs to know
everything because everyone is trying to screw you over. And worse yet, most people do not
know that they are stupid or can speak about a topic knowing they are probably wrong.
It's all so damn stressful I will just take my chances without the vaccine and be as
careful as I can not to infect others. I know a lot about human biology, but not enough about
vaccines and the companies and the people who own them. I do not trust the government because
it is controlled by corporations and not the people.
rusti
December 10, 2020 at 8:49 am
A nice visual would answer this question but I can't find one with DuckDuckGo.
There are two separate groups of people (each 15,000 in the Moderna case), placebo and
vaccine. We'll measure the (small) subset of each group that gets infected and compare the
numbers.
If 100 in the placebo group get infected and 100 in the vaccine group get infected, that
vaccine was 0% effective. No apparent benefit from the vaccine, outcomes look identical.
If 100 in the placebo group and 50 in the vaccine group get infected, that vaccine was
about 50% effective. Not great. Maybe the severity of disease was less in the vaccine group,
but that's a secondary goal and not what we're measuring primarily.
100 in the placebo group and 5 in the vaccine group get infected. That's called 95%
effective.
The size of our trial dictates our level of confidence in these numbers. If our original
groups of people were tiny and/or we have barely any infections in either group, we can't say
much anything with confidence because small numbers of infections in either group can swing
the numbers in either direction.
Thuto
December 10, 2020 at 9:16 am
I was an engineering major so I have no issues with interpreting the data, however it's
laid out. The same can't be said for some members of the general public, hence my assertion
that the claims on efficacy should leave very little room for "depends on how you look at it,
absolute vs relative" interpretations that will serve only to confuse.
Can the pharma
companies stand behind the claim that it's 95% effective without resorting to numerical
semantics or lobbying for liability shields? If so then by all means tell the public that the
vaccines are 95% effective. If they say "well we did say it's 95% but what we meant was "
then we are in the territory of bait and switch.
There's too much at stake to leave even little room for exaggerated claims from profiteers
because the anti-vaxxers will have a field day exploiting any discrepancy between claimed and
actual performance for these vaccines and guess what, with that will go public trust.
rusti
December 10, 2020 at 10:01 am
I can get behind what you're saying, but how might you suggest this be communicated? It
seems like a failure of the press if they can't convey the essential fact that there were two
groups of people and it looks like there were significantly fewer (but not zero) infections
among the 15,000 that got the vaccine.
People (especially managers) usually want one single metric to compare even if it's
woefully inadequate. Quantifying reductions in infection or maybe severe disease seem like
reasonable single-metric comparisons to me.
Thuto
December 10, 2020 at 10:38 am
The 95% efficacy claim shouldn't depend on the lens you wear to interpret the data, that's
my point. As Stephen the tech critic mentions, people are going to alter their behaviour
based on these claims once vaccinated, so 95% should mean 95% in absolute terms and
contra-indications should also be clearly communicated to at-risk populations. Auditable
transparency should be the name of the game, if we've learnt anything from the 737max debacle
it's that companies, when left to their own devices, place profit ahead of human lives.
rusti
December 10, 2020 at 11:26 am
I guess "absolute effectiveness" as a metric like the author defines it is might be a
reasonable for people assessing their individual risk or as a public health metric but it's a
moving target and totally specific to a certain population over a certain span of time, so
it's not especially useful for comparing vaccines. I don't think explaining it sounds any
easier than the other numbers.
Why should Vietnam show a terrible "absolute effectiveness" compared to France if the goal
is to analyze the same vaccine? As the number of people exposed to the virus approaches the
entirety of the population (if half were vaccinated and all members are susceptible to
infection) the number would approach the vaccine efficacy as the companies define it.
Thuto
December 10, 2020 at 11:45 am
Our back-and-forth is proving my point, you and I are somewhat equipped with the
intellectual/statistical/mathematical wherewithal to do an analytical deep dive and look at
the data from different angles, some (most?) people aren't. It's this knowledgeable that the
general population lack the mathematical grasp to make sense of marketing claims, especially
those presented as numbers, that companies exploit to mislead the public. That's why I
contend that the claims should be presented as simply as possible, stripped of opportunities
for profiteers to obsfuscate anything. Freebird has a suggestion below, which I'm 100% on
board with
freebird
December 10, 2020 at 10:40 am
Exactly. I would even ditch the '95% effective' language. They need to say 'if 10,000
people were exposed to the virus, ordinarily about n1 would get infected. With this vaccine,
the number infected was n2. This is language people can grasp.
Thuto
December 10, 2020 at 11:46 am
Exactly
Stephen the tech critic
December 10, 2020 at 4:30 pm
Except that even the above language can still be interpreted through different "lenses".
Certainly with the relatively sample size, it should be clarified that there's a pretty big
"bubble" of uncertainty around the 'n', just considering the basic statistics.
But suppose that for the 75 years and older population the vaccine only works at 50%
efficacy, so if I'm 81.5 years old and the TV tells me that the vaccine prevents "9500 out of
10000 infections", I might take myself out of isolation when that may be otherwise
ill-advised. Likewise, if I'm an allergy sufferer, I might want to know if said suffers have
a 1 in 100 chance of a severe allergic reaction vs. say 1 in 10000 for the general populace.
So how do we communicate all these nuances in a way that makes them understandable to the
wider public? I don't really see an easy way.
In a sense, this is what doctors and regulatory authorities are supposed to do for people,
but much of that is broken right now. Western societies have utterly failed to contain the
virus when it doing so would have been much easier, and they refuse to take the steps
required to contain it now. They have forced themselves into a situation with no
alternatives. They are grasping for a "Hollywood solution" in the form of a high-tech vaccine
"developed in a single weekend".
Mel
December 10, 2020 at 12:10 pm
Where n/10000 is so small, if I wanted to be a Covid-denier I would point to that tiny
number and argue that not getting vaccinated is already 100%-1.23% = 98.77% effective.
To get it right, I have to think about the period of the trial. In X week trial period, my
chance of infection might be 1.23%.
At 4X weeks it approaches 5%.
16X weeks (caeteris paribus) we're talking about serious risk.
But 16X might be a year, and we need test results sooner than that.
Aumua
December 10, 2020 at 12:58 pm
if I wanted to be a Covid-denier I would point to that tiny number and argue that not
getting vaccinated is already 100%-1.23% = 98.77% effective.
That's similar to a (fallacious) argument people use all the time, which is that there's a
99.whatever% chance of survival if you get Covid-19.
ProNewerDeal
December 10, 2020 at 1:44 pm
I hate that fallacy, the binary of 0.X% COVID death vs 99.Y% full recovery. It ignores
Long COVID risk, potentially affecting 20% of symptomatic patients per a UK study. It ignores
the pain, medical cost (especially in no-Medicare4All Murica), & lost-wages opportunity
cost of a non-death hospitalized case.
It is shameful that Long COVID is barely discussed by public health experts, politicians,
or CorpMedia.
rusti
December 10, 2020 at 1:26 pm
if 10,000 people were exposed to the virus, ordinarily about n would get infected
I don't think anyone can possibly put a number on this. It seems like the answer is likely
to be 10,000 unless some people have some innate immunity for reasons we don't understand.
Exposure isn't really binary, someone singing in a phone booth choir with a sick person is
much more likely to get infected than if they were just passing by a sick person in the
grocery store.
It's a very different statement than what the post author tries to capture with "absolute
accuracy" which scales from zero (no cases) to the vaccine efficacy for a whole
population.
Tom Bradford
December 10, 2020 at 3:49 pm
Surely the only way to achieve "absolute accuracy" would be to ensure that both groups are
a) identical in age ranges from 0 – 100, sex and biology/medical history, b) subject
100% of both groups to identical exposure to the virus, and c) isolate both groups from each
other and the general population for a fortnight to prevent additional exposure from outside.
In the absence of the above there is too much scope for a) deliberate and nefarious
manipulation, and b) uncontrollable input influencing the numbers. IMHO.
I was born three years before doctors began giving a new drug on the market declared safe
in pregnancy to mothers for morning sickness. It was called Thalidomide.
I won't be taking this one.
The Historian
December 10, 2020 at 4:21 pm
Exactly! We can never know what 'n' is unless we purposely expose a population to Covid
and then measure how many of them come down with the disease – and to me, that would be
a highly unethical test to employ. So that 'n' as described is meaningless at best.
All we can know is how many people given the placebo come down with the disease v. how
many of the group that get the vaccine come down with the disease and go from there. We know
that not all of the people in either group will be exposed since most of them probably are
taking precaution they can to avoid the disease like most of us – which means that the
numbers of people who do get Covid will be small – and that is where 'statistically
significant' comes into play. If there is any criticism it would be there – did they
test enough people and long enough to get statistically significant numbers?
If you want 'absolute accuracy', then you have to be willing to throw ethics out the
window and purposely give people Covid. Then you can study the effects and get 'real numbers'
if that is what is necessary to convince the critics.
Yves
Smith
December 11, 2020 at 1:21 am
But they don't know how many were infected. This is a leap of logic in your example. They
had a number of infections identified in each group and INFERRED an infection rate, as in
assumed that the rate of contracting the disease was the same in the injected group as in the
control.
There's more cause for pause given that a top HIV expert pointed out that the bar for
designating an infection is too low:
The second surprise from these protocols is how mild the requirements for contracted
Covid-19 symptoms are. A careful reading reveals that the minimum qualification for a case
of Covid-19 is a positive PCR test and one or two mild symptoms. These include headache,
fever, cough, or mild nausea. This is far from adequate. These vaccine trials are testing
to prevent common cold symptoms.
https://www.forbes.com/sites/williamhaseltine/2020/09/23/covid-19-vaccine-protocols-reveal-that-trials-are-designed-to-succeed/
rusti
December 11, 2020 at 1:44 am
Where is the leap in my logic? A lower threshold for diagnosing disease (risking more
false or dubious positives) is bad for the pharma companies.
False positives in the vaccine group are disproportionally worse for efficacy when the
manufacturers want to be able to claim an order of magnitude fewer infections for that
group.
Jeff W
December 10, 2020 at 10:19 am
Ah, thanks. I was puzzled by the argument, because it seemed a bit like saying that
routinely carrying umbrellas did not provide 95% protection against rain because it only
rained some of the time.
I'm glad it wasn't only me, although I was thinking along the lines that parachutes are
highly effective in only the 1–2% of the population that goes skydiving. (But, to
analogize to COVID-19 somewhat, you'd end up in a plane about to be pushed out without
expecting it or wanting to.) It struck me as a way not to interpret the
statistics.
Nameful
December 10, 2020 at 11:09 am
But if, say, 10000 vaccinated people visit a country in the course of a year, but only
500 come into contact with a contagious source (which would not be surprising) and none get
ill, then the efficacy of the vaccine would presumably only be 0.05% according to the logic
of the article.
Actually, it would about 0% plus whatever smoothing coefficient you choose to apply for
your prior (Jeffreys would give 0.5 / 500.5 = ~0.1%). The number of vaccinated people here is
has an indirect impact, via Bayesian chaining – it will give you a confidence interval
for the number of exposed people (via a binomial with the maximum at about 500/10000 = 5%),
which is then propagated into the confidence interval of the number of infected ones.
Cocomaan
December 10, 2020 at 6:43 am
What was the testing protocol for people who were asymptomatic? That is, we're the 95% of
people all tested, or just assumed free of disease?
Cocomaan
December 10, 2020 at 7:03 am
Apparently I can't form a sentence this early in the morning.
My concern is that the vaccine creates a class of people who are asymptomatic carriers
that 1) continue to spread the disease and 2) may still have damage from the disease, because
we have seen that asymptomatic carriers can still get lung and heart damage .
How would you know someone is an asymptomatic carrier unless you tested them?
Otto V.
December 10, 2020 at 8:55 am
Is that population *representative* of the whole population? Does it include children?
The elderly? People of different social class and/or living situations? People of different
"colors"? People with history of severe allergies? And are the proportions of each of these
(and any others I *can't* think of) similar within the sampled population as in the whole
population?
Probably. No. Yes. Yes. Yes. Unlikely. Close. Also, no pregnant people. But the vaccine
has not been approved for children nor pregnant people.
Second, the result assumes that the study is blinded.
It was randomized and double-blinded.
the media has reported repeatedly and extensively, while these trails are on-going, that
side-effects are common
The common side effect was redness, swelling, and pain in the injection area. Mild side
effects in less than 10% (otherwise, it would have not been approved by the NHS). I don't
think that's enough to "unblind" participants, at least in significant numbers.
The author is correct that these vaccines are "under-tested"
Do we know if they've weakened the criteria in the approval process? Because I might be
wrong/misinformed, but from what I've read, any other vaccine at any other time would get a
Phase IV approval with the data provided.
I do agree with the part that we shouldn't lift all the restrictions just because we have
the vaccine. Only when and if infection rates drop down to anecdotal, we can slowly and
carefully begin to get back to normal (whatever that may be).
Yves
Smith
December 10, 2020 at 4:20 pm
You are understating the side effects. Many people feel like crap for a day:
High fever, body aches, headaches and exhaustion are some of the symptoms participants
in Moderna and Pfizer's coronavirus vaccine trials say they felt after receiving the
shots.
While the symptoms were uncomfortable, and at times intense, they often went away after
a day, sometimes less.
https://www.cnbc.com/2020/10/01/coronavirus-vaccine-trial-participants-exhaustion-fever-headaches.html
john
December 10, 2020 at 5:49 pm
Is feeling crap for a day a mild symptoms ? i don't know either way in terms or what
is considered mild, but it doesn't sound too severe.
The article appears to over egg the efficacy concerns. Did they want people 30, 000 to be
deliberately infected to test the exact number. I think a large number of human challenge
trials are ongoing. I think its reasonable to except the efficacy to be over 80% but the
exact number is to be determined with further studies.
Yves
Smith
December 10, 2020 at 6:37 pm
If you can't take a day off from work, and many can't, it's not trivial. And Pfizer
appears to have underplayed the fever issue. Some experts took note of the fact that everyone
who took the Pfizer vaccine in the trials was encouraged to take acetaminophen afterwards.
That's not normal. IM Doc wrote this in today's Links:
Thank you for the link regarding the nurse who had the reaction to the vaccine.
A few words of clarification for your readers from a physician of 30 years.
A temperature of 104.9 in an adult with a functional immune system (we are not talking
about babies and kids – they are different) is extraordinary after a vaccination.
104.9 means that the immune system has been activated enough to take it up a few notches to
DEF CON 1. This is very unusual in infectious disease – some parasites and ameba do
this routinely – and things like sepsis syndrome can – but for the most part,
getting a temperature up this high is definitely not normal. It is certainly not a good
sign for a vaccine. A vaccine should not be stimulating the immune system to this degree
– EVER. Idiosyncratic reactions in a very rare patient is one thing – if this
is happening more often – this is not a good sign for that vaccine.
The nurse in the article is absolutely correct – a temperature of 104.9 after a
vaccine administration is a grade 4 reportable event.
This is medically important for two reasons. 1) That level of fever if sustained can
damage permanently multiple organs. 2) Vaccines should simply not be activating the immune
system to that degree – it is completely inappropriate. It is very normal for people
to have a brief temp of 99 or 100 after a vaccine – this is a completely different
level.
From what I can tell in the Pfizer documents – "fever" is not uncommon as a side
effect to their vaccine. I cannot determine in any location what their parameters are for
"fever". As stated above – it is accepted that multiple vaccines will give a patient
a slight fever as a side effect maybe up to a day. But not 104.5. How many of these
patients classified as "fever" in their information and glossies were actually 103? 104?
There is no transparency – and that is the problem.
And if you read the comments above from those who are statistically well versed, the issue
is that the effective sample is so small that there is a high degree of statistical
uncertainty around the efficacy numbers. And that's before getting to the fact that messenger
RNA technology (the one used in the Pfizer and Moderna vaccines) have never before been used
(except in a Zika trial of ~100, too small to be reliable) and the long term effects are
unknown.
There are plenty of MDs who never prescribe a new med that has been out less than a year
to patients. I won't take the Pfizer or Moderna vaccine. I'll wait for a conventional vaccine
(there are plenty in trials, so several are likely to win approval).
nn
December 10, 2020 at 10:53 am
But as I understand it, the point is precisely that the sample is unrepresentative. What
the trials did is ethical equivalent of randomly choosing 185 people, vaccinating them, then
infecting then with the virus and then observing that only 11 got sick.
Just 185 seems really low.
Stephen
December 10, 2020 at 11:24 am
I really appreciate the explanation. There is another element that has bothered me from
the beginning of the phase 2/3 trial: that any and all symptoms are self reported. I'm in the
Pfizer trial and received the doses in August and I asked repeatadly what level of
pain/discomfort/deviation from the norm would warrant reporting and was told ANY change. But
I am curious how many asked that and actually did it. Meaning, my guess is that the level of
infections in the placebo group is actually higher when combined with the truly asymptomatic.
But the same may be true in the vaccine group as well. They are trying to root out the
asymptomatic spread with challenge trials, if they get approved.
Cuibono
December 10, 2020 at 1:11 pm
You are right about his weird choice of language but his point is accurate
in ANY medical intervention one wants to know BOTH Relative efficacy and Absolute.
This vaccine reduced the RELATIVE rate of infections dramatically.. But since the overall
incidence of infections was low, the ABSOLUTe reduction was very small. This is also true of say STATINs in low risk patients.
Maritimer
December 10, 2020 at 4:43 am
The Vaccine Drumbeat in my jurisdiction is increasing and I'm sure will become deafening.
Talk show radio hosts actually giving medical advice. No recommendations to consult with a
doctor regarding your personal health circumstances and risks or those of your loved
ones.
This is all orchestrated by Public Health officials who apparently have never heard of
personal health care. We are all just one big Herd. To me this is a desecration of the doctor
patient relationship by so-called health professionals. All of which is extremely dangerous
and bad medical advice.
Nick Alcock
December 11, 2020 at 1:11 pm
They're trying to prevent people who *cannot* take the vaccine for whatever reason from
dying, by encouraging people who are merely worried but have no actual reason not to take the
vaccine other than paranoia and ungrounded conspiracy-mongering to take the bloody thing.
This seems like, y'know, their job, and entirely praiseworthy.
The disease *does* see us as one big herd, or rather as a pile of individual infectable
cells. It seems right to deal with the response to it on the same level.
Thuto
December 10, 2020 at 5:00 am
Re: companies mandating staff to be vaccinated to market their establishments as "safe".
The tone and substance of the post is clearly meant to be a "proceed with caution" advisory
on taking the vaccine, despite the author being at pains to emphasize that it's not an
"encouragement to reject vaccines".
Some quarters of the labour market are clearly going to
render this moot for the serfs who'll be required to either sign up to be guinea pigs or lose
their jobs, wow. Swallow the tail risk of unknown medium to long-term health effects of these
rapidly developed vaccines for the short term gain of a (most likely crap) salary? So agency
over one's health is now signed over to employers as a means to eke out a meagre existence,
double wow.
Barry Disch
December 10, 2020 at 5:13 am
Don't forget they are using flawed PCR tests and except for Moderna in the US all other
countries and companies where studies have been conducted are using another vaccine instead
of a true saline or inert placebo.
Not to mention most of these Pharmaceutical Companies have been sued for tens of billions of
dollars for harmful drugs , buried information, fraud ect. We're supposed to trust them with
safety studies for medical products they have indemnity for. Thank you for pointing out how
deceptive these numbers can be for the average person.
rusti
December 10, 2020 at 8:18 am
Don't forget they are using flawed PCR tests
Can you elaborate on why PCR testing is flawed? What better alternative is there for
determining an infection with high specificity?
westkentim
December 10, 2020 at 3:08 pm
My understanding (and my understanding of all this is not perfect!) is that PCR tests are
flawed (a) because they iterate an amplification process until they find something, and that
something could be the remnants of another CV caused by a cold you had 3 months previously
and (b) at least in the UK, the testing labs are not necessarily as well-versed in the hygiene
procedures you need to avoid cross-contamination. So there is a high risk of false
positives.
Moreover, if I am reading the background to the clinical trials correctly, they count as
"success" situations where someone who has one positive PCR test plus some fairly common cold
symptoms does not then go on to develop full-blown CV19 symptoms. The problem is, given the PCR is acknowledged to generate a lot of false positives, then the success rate will be
overstated, because the denominator in the success rate calculations will be swollen with
subjects who didn't actually have the CV19 virus to start with
(I can't quite believe that the test can be that dumb, so perhaps I am totally wrong about
that? But I fear I am not.)
rusti
December 10, 2020 at 11:46 pm
The Cycle Threshold of a sample (for PCR tests that provide it) gives some indication of
the quantity of virus in the sample. I think that for only viral fragments a very high CT
value (low amount of virus) will be an indicator that repeat testing may be necessary. I
haven't read the actual protocols to learn how they handle this.
The problem is, given the PCR is acknowledged to generate a lot of false positives, then
the success rate will be overstated
I don't follow your thinking here, if false positives are equally distributed across the
placebo and vaccine groups then it will make the vaccine look less effective.
Let's say 100 people really get infected in the placebo group and 10 in the vaccine group
(90% efficacy). If you add an equal number of false positives to both groups, it can only
push efficacy number down. If we add 10 to each group, efficacy is down to ~80%. If we add 20
to each group, efficacy is down to 75%.
Synoia
December 10, 2020 at 5:46 am
Treating symptoms and not the underlying disease appears very profitable to me. How can
that possibly create herd immunity?
Does that mean herd immunity is achieved when a significant number are asymptomatic,
infected and capable of infecting the uninoculated?
I am assuming that infected asymptomatic individuals are capable of infecting others.
Samuel Conner
December 10, 2020 at 7:20 am
A question that this raises for me is whether sterilising immunity is conferred by the
innate immune response to infection with live virus.
If not, then "herd immunity" would not be achieved by letting the virus "run" through the
population, as has been advocated by some. The commentary I have seen on this generally
assumes that people who have recovered from infection are not only protected from disease
symptoms, but cannot for some length of time become reinfected and asymptomatic spreaders.
Perhaps they can.
This is a very bad prospect for vulnerable populations.
lincoln
December 10, 2020 at 2:36 pm
If a vaccinated individual can still transmit COVID, then herd immunity may not be practical.
"Herd immunity is a form of indirect protection from infectious disease ..Immune
individuals are unlikely to contribute to disease transmission, disrupting chains of
infection, which stops or slows the spread of disease. The greater the proportion of immune
individuals in a community, the smaller the probability that non-immune individuals will come
into contact with an infectious individual."
ahimsa
December 10, 2020 at 5:54 am
There is a comic meme going around at the moment:
1st mouse says: Are you going to get vaccinated?
2nd mouse replies: Are you mad? They haven't completed the human trials!
Dean
December 10, 2020 at 6:22 am
I'm still having a hard time wrapping my head around this. What do the 'numbers' look like
for a proven vaccine that's been around for several decades or more (e.g. smallpox, polio,
etc)?
Are these vaccines truly "95% effective": illness prevented and infection eliminated in
95% of everyone vaccinated. Period?
Am I thinking about this the right way?
Thank you.
The Historian
December 10, 2020 at 9:39 am
Let's just make this simple.
Not everyone is going to be exposed to Covid-19 just like not everyone is going to be
exposed to the flu. So why do you take the flu vaccine? Isn't it because if you are unlucky
and DO get exposed, you have some protection from getting sick?
Not everyone was going to be exposed to small pox or polio, but for those that were
unlucky enough to get exposed, those vaccines protected MOST of them from getting the
diseases, I'm not sure what the 'effectiveness' of those vaccines were, but you don't hear of
small pox or polio pandemics any more. Isn't that what a vaccine is supposed to do?
The reason for getting a Covid-19 vaccine is just the same. You may never be exposed to
Covid-19 so the vaccine will have nothing to protect you from – so, according to this
article, it's effectiveness for you will be zero. Remember only 185 of 15,000 people who were
taking the placebo got exposed. So, if you are unlucky and do get exposed, wouldn't you like
to have some protection from what Covid-19 can do? And what the numbers are saying is that IF
you do get exposed to Covid-19 that you have a 95% chance of being protected and NOT getting
that disease. To me that sounds a whole lot better than nothing!
I call articles like the above "fun with math". They send you down the wrong path when it
comes to what you can rationally expect from vaccines and they provide fodder for the
anti-vaxxers.
That said, I wish we had more time to see what the possible side effects are, but sadly
Covid is killing people at a too rapid pace for us to wait for the perfect vaccine.
Burritonomics
December 10, 2020 at 10:17 am
Exactly. I'd like to write a long form rebuttal to this article, but I have to go to work
in 30 minutes.
"It sucks, and is bordering on intentionally misleading" is my short form response.
My thinking is like I'm being given a choice between two syringes: one has an unknown dose
of Covid-19. The other is the vaccine.
I'll be getting the vaccine as soon as I can.
Jeff W
December 10, 2020 at 8:26 pm
" bordering on intentionally misleading"
I thought so, too.
Brian (another one they call)
December 10, 2020 at 10:37 am
I have a growing problem with the claims without any proof of efficacy. One of the vaccine
makers bragged about creating the vaccine "one weekend" Vaccines take years to develop. That
these are miraculously appearing within months by companies with a financial interest in
being first. In a word, bushwa.
Don Cafferty
December 10, 2020 at 12:57 pm
I am not an expert or have medical training. I do read a lot. Re "Vaccines take years to
develop", you are correct. From my reading, the basic science for mRNA started in 1983. What
happened afterwards has irony. The principle scientist/investigator repeatedly had difficulty
in getting grant money to do her study because granting agencies did not think that the mRNA
would be accepted by the human body. It was thought that the auto immune system would
automatically reject it. The principle scientist/investigator failed to get tenure at her
university because she was not able to bring much grant money to the university. Nonetheless,
she persevered and finally together with a collaborator, they found a way of introducing mRNA
without alerting the immune system. Their work was published in 2005. Their work was largely
unnoticed except for two people who saw the medical opportunity provided by mRNA. Further
study was done and eventually medical science and entrepreneurship merged together which led
to the formation of BioNtech (based on the words, "biopharmaceuticals", "New",
"Technologies") and Moderna (based on the words "Modified", "RNA"). Neither BioNtech nor
Moderna had a vaccine a year ago. Instead, they had the technology. When the genetic code for
the virus was released to the world by Chinese scientists, BioNtech and Moderna could then
program their mRNA technology for the Sars-Cov-2 virus. With their technology, it could be
said that they already had a head start in making the vaccine. The principle scientist and
her collaborator work separately. One is now employed with Moderna and the other is with
BioNtech.
rosemerry
December 10, 2020 at 5:46 pm
None of the "Western" developers would of course now give any credit to their Chinese
helpers!!! We only hear of "China steals our intellectual property."
Remember the days when Jonas Salk refused to patent and make money from his polio
vaccine?
Nick Alcock
December 11, 2020 at 1:13 pm
They had a head start in making this vaccine *and possibly all future ones too*. This is a
game-changer: it's quite possible that future diseases may routinely have a vaccine entering
clinical trials *days* after its genome is known, rather than having to work on it for months
to decades first.
(Now all we have to do is convince people that it's not a dark plot and that actually
these things do save lives.)
Count Zero
December 11, 2020 at 6:20 am
I too am getting dizzy with all these statistics and caveats. I have had a flu jab every
year for the last 12. I have had bugs of one kind or another over the years but I only had
some kind of flu once -- this February as it happens. There is no way that anybody can
estimate how many flu bugs I was exposed to and what their impact would be on a healthy man
in his 60s in the last decade. Anyway, I don't worry about the statistics but make a simple
risk assessment. Is the risk of a flu vaccine less than the risk of getting flu? The answer
has to be yes.
With covid19 vaccinations I don't much care whether it's efficacy can be measured as 95%
or 70% or 60%. Anything is better than nothing. Anyway, it's like wearing masks. Its efficacy
depends upon large numbers of people being vaccinated. I help protect you as well as myself
and you protect me as well as yourself. I worry that large numbers of people will decide not
to have any vaccine, ensuring that covid19 will continue to kill unprotected people.
Only one thing concerns me at present. Safety. Sadly, enough doubts have been raised about
the two new experimental vaccines to make me think the risk is not worth it. I will wait for
the Oxford vaccine to become available I think -- while trying to keep a sensible open-minded
watching brief.
IdahoSpud
December 10, 2020 at 6:36 am
There is no reason that you should go right out and get poked with these barely-tested,
and IMHO experimental vaccines.
Salk and Sabin were hailed as heroes – which they were – for giving humanity
polio vaccines. What has gone down the memory hole though, is how Pharma family blogged up
the production of the vaccines. You should really check these links to see how bad this
was/is.
https://en.wikipedia.org/wiki/Cutter_Laboratories
(children vaccinated with live polio virus that survived the production process)
https://en.wikipedia.org/wiki/SV40 (90% of US
children and 60% of adults inoculated with polio vaccine contaminated with a monkey virus
that turns out be carcinogenic – it's also passed down in-utero, so we all have
increased likelihood of certain cancers, thanks pharma)
Public health is standing between greedy sociopaths and a big pile of cash, and it'll
probably get run over. I fail to see why we should expect a sound vaccine in this
environment.
Nick Alcock
December 11, 2020 at 1:16 pm
I haven't seen my parents in a year. My parents haven't seen anyone in a year.
There's a bloody good reason to go out and get vaccinated for us!
There's a reason for everyone else too: some old and vulnerable people won't be able to
get vaccinated, which means they'll be stuck in isolation until enough people have
been vaccinated that they don't need to worry about dying of this thing every time they go
out in public or meet anyone ever.
Adrian D.
December 10, 2020 at 6:44 am
Whether or not the vaccine is capable of interrupting transmission absolutely should have
been front and centre in these studies especially when it's presented to people with an
extremely low chance of being harmed by the virus (ie. the fit & young who might be the
ones likely to be affected by any fertility issues).
It could be assumed that less severe symptoms means less chance for spread which may be
the case, but then I can't see how logically that fits with the mainstream view that of the
virus as something that is transmitted asymptomatically so readily anyway? (Although I think
this asymptomatic spread idea is probably wildly overblown).
Otto V.
December 10, 2020 at 9:09 am
Asymptomatic and presymptomatic are not the same. Studies show that most of the
asymptomatic people who transmit the disease end up developing symptoms (I've seen systematic
reviews that show anything between 83% to 94%). I.e.: asymptomatic transmission is possible,
but mostly by presymptomatic people.
Red
December 10, 2020 at 7:38 am
The early bird gets the worm, but the second mouse gets the cheese!
Kevin C. Smith
December 10, 2020 at 8:16 am
As a practical matter, I expect that these vaccines will reduce the incidence and severity
of both disease and transmission in the treated populations, and do so with little risk to
the treated indivduals, so that there is very likely to be a net benefit to a treated
individual, to the population of treated individuals, and [to a lesser exent] to the
non-treated individuals in the general population.
I am confident that more information will emerge to support and refine the above
hypotheses. It will only be a matter of degree. Speaking as a 69 year-old physician, I would
take any of the three leading vaccines at the first opportunity. I expect that when we look
back in a few years we will see that the immunized population did better than the age-sex-etc
matched non-immunized population. To some extent, my wife and I are relying on unbalanced
articles like this to at least temporarily deter some people from having the vaccine, so that
we can get to the front of the line more quickly.
Thuto
December 10, 2020 at 8:55 am
Out of curiosity, what informs your confidence in these vaccines apart from the press
releases and efficacy claims from the pharma companies developing them? Is it something we
the general public aren't privy to that physicians have given the heads up on? I'm in now way
being flippant, it's just that a good number of doctors I know personally wouldn't go near
any of these vaccines, at least not until there's enough data backing up their efficacy in
the real world.
Otto V.
December 10, 2020 at 9:20 am
it's just that a good number of doctors I know personally wouldn't go near any of these
vaccines, at least not until there's enough data backing up their efficacy in the real
world.
That's a pretty contradictory position. You don't get real world data unless real world
people take the vaccine. Very telling of those -probably wealthy- doctors to let others
assume that risk. Let's not forget that tens of thousands of people already took the vaccine
with significantly fewer assurances. I guess it's alright to go to poor and desperate people
first? That's what I call solidarity and prosocial behavior.
Thuto
December 10, 2020 at 9:53 am
No, the doctors aren't convinced by the studies and the claims emerging from that, at
least not yet. If signing up to be a guinea pig for something you're not entirely convinced
of is your idea of solidarity and pro-social behaviour then by all means, go right ahead,
they're not stopping you. By the way, more data can be the result of more extensive clinical
trials with better designed studies that aren't "designed to succeed", and is not limited to
being obtained from poor people being lined up to volunteer as guinea pigs, as you imply.
In any event all of this "being at the head of the queue" talk is academic for us in
Africa, the big wealthy nations have resolved to hoard the supplies of whatever credible
vaccine becomes available. Maybe you could lobby them to share in the name of solidarity.
Otto V.
December 12, 2020 at 7:34 am
If signing up to be a guinea pig for something you're not entirely convinced of is your
idea of solidarity and pro-social behaviour then by all means, go right ahead, they're not
stopping you
If you put it like that, and people interpret it like that, no clinical trials ever would
happen, except in Nazi Germany, where they forced people to submit to medical experiments
(see, we can all be overly dramatic). If the vaccine is not good enough for you, it shouldn't
be good enough for anybody, and we never get a vaccine for anything, ever.
Therefore, yes, I will gladly accept the vaccine once it's my turn, because at this point
is civic duty and safety is as guaranteed as any other Phase IV drug. Again, the two
alternatives are being a hypocrite or not having a vaccine.
Maybe you could lobby them to share in the name of solidarity
Even better, I advocate to allow the vaccine to be produced in developing countries
freely, without IP concerns. I doubt the wealthy countries will accept the proposal, but I
also hope those countries will ignore international law and manufacture it for local
consumption anyway.
freebird
December 10, 2020 at 10:47 am
I don't know if it's selfishness on the doctors' part, or just so much familiarity with
the avarice of the pharmaceutical industry that they don't trust the data that has been
molded into a neat report, likely as not full of hidden flaws or deliberately misleading
conclusions. Unfortunately the truth will not come out til a lot of people have taken the
vaccines, and I can't blame a front line worker for not wanting to be at the front of the
line.
Otto V.
December 12, 2020 at 7:44 am
I don't doubt the avarice of Big Pharma. I count on it. But the people who actually
developed the vaccine and actually run the experiments won't see a penny of the billions
Pfizer is going to make with this vaccine. At that point, I would expect at least a couple of
trustworthy sources, with a conscience and without billions to blind it, would blow the
whistle on any data manipulation. Like all conspiracies, the more people are involved, the
shorter they live. Thousands have participated in the Phase III. So far, all the complains
come from people who don't trust Pfizer because Pfizer is not trustworthy, and people who are
concerned for political reasons. And don't get me wrong, you can't trust Pfizer and there are
clear political concerns, but as long as it's just that, keeping an eye open and taking the
vaccine is the right thing to do. Again, because otherwise we probably won't get a vaccine in
decades, if ever.
The Rev Kev
December 10, 2020 at 9:14 am
Don't be in such a rush to get to the head of the que-
https://www.youtube.com/watch?v=arwZcw0Ejcc
Wyoming
December 10, 2020 at 9:23 am
I 2nd Thuto here.
I have a good friend who is a practicing MD dealing with Covid patients who I talk to
regularly about the vaccines and the epidemic. He has a low opinion of how the trials have
been conducted and thinks that there is a high chance of several surprising issues popping up
(like the adverse reactions mentioned above). He, contrary to you, intends to let the early
vaccine recipient's finish the more comprehensive testing which should have occurred as part
of the stage 3 trials.
Thor's Hammer
December 10, 2020 at 10:51 am
Dr. Smith
Conventional vaccines like those for Polio and Smallpox utilize modified or disabled forms
of the disease pathogens to stimulate antibodies to provide resistance when they encounter
the disease "in the wild." We have decades of experience and millions of cases using this
type of vaccine which lends a high level of confidence that a new conventional vaccine can be
used safely on a new pathogen.
MD's like yourself have years of experience and training in identifying and treating
disease -- certainly far beyond that of the the average layman. But you are also the product
of a culture that determines how you think about your practice. For example, "Only medicines
that have gone through the approval and patent process are suitable for human use." Or, "All
medicines obtained from foreign countries are suspect or dangerous." Or: "Authorities like
the AMA, NIH or WHO are the only reliable sources of information" Or: "Deviating from
approved practice can/will result in lawsuits and being barred from practicing medicine."
By all means dash to the head of the Pfizer/Moderna Corvid vaccine line. We need more
willing volunteers like yourself so authorities like Bill Gates won't have to test new
vaccines on poor children in Africa and India to determine whether the side effects include
sterility or the re-emergence of Polio.
Kurtismayfield
December 10, 2020 at 11:22 am
This.
Considering the questions that people have been asking on this website on how the mRNA
vaccine works, I doubt that most people understand that this is not like the other vaccines
that people have taken, and uses a completely different mechanism for eliciting an immune
response than traditional vaccines.
Nick Alcock
December 11, 2020 at 1:23 pm
It uses exactly the same mechanism: presentation of an antigen on cell surfaces. It even
uses the same antigen as some of the more conventional SARS-CoV-2 vaccines. The
antigen is even produced in the same place: the inside of the recipients' cells. The only
unusual thing is where the RNA comes from that is used to do this: is it on its own, or does
it come packaged with other viral RNA implementing a complete working virus not common in
human populations which has been modified to produce this antigen?
(I don't know why anyone would consider it safer to take a traditional vaccine which has
an actual working virus in it, even if said virus only causes a mild cold, than it would be
to take these new ones which have no viral replication machinery whatsoever . The
Moderna/biontech stuff is new, but not because it was previously believed unsafe, merely
because eukaryotes are vicious to naked RNA outside their cells and destroy it on sight with
some of the most efficient enzymes known because, well, it's a sign of viral infection. So
RNA-based vaccines never got close to getting inside enough cells to be useful, so you needed
a whole viral capsid to do the job, like the more traditional Astra-Zeneca vaccine.
That's the problem that's been solved.)
Kevin C. Smith
December 10, 2020 at 12:47 pm
There will be some who make the specious argument that only ~2% of the subjects in the
study got symptomatic Covid, so "big deal". That sort of argument would carry more weight if
it had been expressed in terms of "cases per unit time". In this case, it looks as though the
median time was about 2 months.
I expect that as time goes on we would find that a very large proportion of the control
group [maybe 10%] would develop clinical symptoms, and a much larger proportion would develop
asymptomatic disease [which carries a poorly defined risk of serious but silent damage to the
heart, brain, etc].
As good studies emerge, like BioNTech, we can read the original peer reviewed literature
and the commentaries on it, and draw our own conclusions:https://www.nejm.org/doi/full/10.1056/NEJMe2034717?query=RP
Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccinehttps://www.nejm.org/doi/full/10.1056/NEJMoa2034577?query=RP
Tom Bradford
December 10, 2020 at 4:09 pm
To some extent, my wife and I are relying on unbalanced articles like this to at least
temporarily deter some people from having the vaccine, so that we can get to the front of the
line more quickly.
Fine by me. The more human guinea-pigs that stand between me and this stuff – and
remain standing – the more likely I'll be to take it. Eventually. Tho' if your
confidence is justified and you help take Runder1 perhaps I won't even have to risk it.
Paolo
December 10, 2020 at 9:22 am
While there are some clear misunderstandings about these numbers from both sides, several
pointed out that we have zero knowledge about other aspects of the vaccine, such as:
We should be focused on better testing (both developing and administering), pervasive
contact tracing, and innovative technologies such as air filtering with vertical flow, better
masks, better public support for masks, better strategies for isolating sick individuals in
crowded situations, better treatments. What terrifies me about the vaccine craze is that it
is distracting everyone from doing the right things not just to stem the death toll from this
pandemic, but also from using this as a learning experience to be better prepared for the
next one.
There is the expression "closing the barn doors after the cows have gone." A more complete
analogy in this case would be "a fire started in the barn, luckily the cows were able to run
out the open door. We went into the barn and closed the door from the inside without a fire
extinguisher."
Olivier
December 10, 2020 at 9:24 am
The COVID coverage by Michael Haseltine on Forbes is well worth reading. His Sep.
23 piece titled
Covid-19 Vaccine Protocols Reveal That Trials Are Designed To Succeed is especially
relevant.
KLG
December 10, 2020 at 10:18 am
William A. Haseltine, who was a pioneer during the early HIV/AIDS epidemic.
Yves
Smith
December 10, 2020 at 10:19 pm
This part is damning:
The second surprise from these protocols is how mild the requirements for contracted
Covid-19 symptoms are. A careful reading reveals that the minimum qualification for a case
of Covid-19 is a positive PCR test and one or two mild symptoms. These include headache,
fever, cough, or mild nausea. This is far from adequate. These vaccine trials are testing
to prevent common cold symptoms.
https://www.forbes.com/sites/williamhaseltine/2020/09/23/covid-19-vaccine-protocols-reveal-that-trials-are-designed-to-succeed/
rusti
December 10, 2020 at 11:51 pm
Why is that damning? The lower their threshold for a positive, the more likely they are to
have false positives. False positives in the vaccine group make the efficacy values
plunge.
It is totally counterproductive if the intention is to game the results. Then the smart
play would be to only count serious disease.
Milton
December 10, 2020 at 10:00 am
By tomorrow, according to Worldmeters, 5% of the population in the US will have tested
positive for c-19-studies have put the actual penetration of those infected at anywhere from
2X to 10X the counted numbers (16 million, or so). Are persons that have been tested
positive, or carry antibodies, exempt from any mass vaccination program? It seems to me the
enormous rush to get vaccines to market is the fear that, lockdowns notwithstanding, we are
heading towards that time when a majority of the US population will have already become
infected. I can envision the panic in big phamas boardrooms as the see that every week
another million potential customers are removed from their expected profit sheets.
The Rev Kev
December 10, 2020 at 10:08 am
It's worse than that. Not long ago some were saying how the number of American dead in
this pandemic was approaching the number killed in Vietnam. Now the daily total exceeds that
lost on 9/11 and is accelerating.
Thor's Hammer
December 10, 2020 at 11:27 am
Not to worry. Simply denying the ability to fly, work, drive a car, or go to the
supermarket to everyone without a digital vaccine certification card will ensure a high level
of compliance with the Universal Mandate and continued joy in the boardrooms of Pfizer. The
goal is to monetize Pharma Power, not to control Corid19. So bringing all those who have
self-vaccinated by contacting a mild case of the disease or have a strong T-cell immunity
response into the Fold is just good business.
Speaking of business opportunities, printing black market certification cards @ $100 each
promises to put BitCoin to shame.
About that 5% of the US population that have tested positive:
Aumua
December 10, 2020 at 1:31 pm
The goal is to monetize Pharma Power, not to control Corid19.
I assume it's probably some degree of both. I mean just cause something might be
true doesn't mean it is true.
At the conventional PCR Cr of 40 about 5% will have a viral loading such that they are
actively spreading infection to others. The other 95% could be more accurately termed as
false positives.
I also question these numbers and/or reasoning. Do you have a link supporting this
statement?
Thor's Hammer
December 10, 2020 at 3:28 pm
I too have a problem with the way my source arrived at their 97% false positive claim. The
internal logic is indeed correct, but it feels like using statistics in a less than
transparent manner.
https://www.rt.com/op-ed/507937-covid-pcr-test-fail/
https://www.zerohedge.com/medical/covid-19-rt-pcr-test-how-mislead-all-humanity-accepting-societal-lock-downs
marku52
December 10, 2020 at 4:02 pm
I had read that a cycle rep of about 25 was more commonly used. 40 would pick up a lot
false positives.
Petter
December 10, 2020 at 2:02 pm
Regarding monetizing Pharma Power: The Norwegian institute CEPI – Coalition for
Epidemic Preparedness Innovations was founded in 2017 with the goal (amongst others) of being
in the forefront in the development of vaccines for new infectious diseases and their
distribution at an affordable price (or no price if countries can't afford it) throughout the
world. Funding for CEPI has come from the governments, trusts and foundations. Read all about
it here.https://cepi.net
What happened with CEPI and the development of Covid vaccines? The pharma companies would
not give up their right to determine prices, for "competitive business reasons".
Goggle Translate of an NRK article:
https://www.nrk.no/dokumentar/ble-makteslost-vitne-til-dod-_-selv-om-vaksinen-fantes-1.15060685
In a sensational article, Hatchett explains what happened to CEPI's policy:
CEPI's rules are based on the idealism on which the coalition was founded. However,
several multinational vaccine companies said they did not "reflect the business reality of
vaccine developers," according to the CEPI director. They also disliked the fact that CEPI
should be able to set the price.
For industry, the rules were simply not in line with a competitive business model,
according to Richard Hatchett.https://www.sciencedirect.com/science/article/pii/S0264410X19317190#
!
Gerald Posner discusses CEPI in a New York Times article (from March): https://www.nytimes.com/2020/03/02/opinion/contributors/pharma-vaccines.html
-- -
But what has played mostly out of public view over that same time was the organization's
failed effort to get large pharmaceutical firms to agree to be partners without insisting on
substantial profits or proprietary rights to research that CEPI helped to finance and produce
(my bolding). That did not surprise many industry observers who knew that since the 1930s,
the National Institutes of Health had spent over $900 billion on grants that drug firms
relied on to patent brand-name medications.https://www.youtube.com/watch?v=Glu9wA4HjE0
Kevin C. Smith
December 10, 2020 at 5:02 pm
Several lines of evidence show that immunity after COVID-19 wanes quite rapidly, and that
immunity after immuniztion with several of the vaccines persists quite nicely, both in animal
and human models. The reason for this is that the vaccines are engineered to stimulate strong
defensive responses which include both antibody-mediated immunity and T-cell mediated
immunity. Many of the vaccine candidates include adjuvants, which are materials which
facilitate and enhance the immune response to the antigens in the vaccine.
martin horzempa
December 10, 2020 at 10:47 am
just a thought to all who venture here now and again,
thanks Yves
p fitzsimon
December 10, 2020 at 11:36 am
The big unknown is of course the number of people in the test population who were actually
exposed to the infection. If everyone in the test population were exposed and only 11 of the
15000 vaccinated developed symptons then we have 11/15000 or 99.9% effectiveness. However, if
only 5% (1500)were actually exposed to infection during the test period then we have 11/750
or 98.5%, which looks pretty good. Does this sound logical? Ok the other unknown is the
number of people in the vaccinated population whose own immune systems would have defeated
the virus without the vaccine. That's where the ratio helps 1-11/185 or 94% effective. Looks
good to me.
Otto V.
December 12, 2020 at 7:57 am
The assumption is that the exposure rate was the same in both groups, therefore the
expected number of infections in both groups should be about the same. The inoculated group
had 5% the number of cases of the placebo group, and that's where the 95% effectiveness rate
comes from. Whether you like how they calculated it or not, the important thing to understand
is that there's nothing special or ad-hoc about this method, this is how they calculate the
effectiveness of all vaccines (and prophylactic treatments in general), and the effectiveness
of a good flu vaccine is around 60%, and it's frequently as low as 40%.
Greg S.
December 10, 2020 at 12:17 pm
I thought this was a sober and sobering post from Peter Doshi the assoicate editor at the
British Medical Journal.
https://blogs.bmj.com/bmj/2020/11/26/peter-doshi-pfizer-and-modernas-95-effective-vaccines-lets-be-cautious-and-first-see-the-full-data/
Cuibono
December 10, 2020 at 1:18 pm
The author also fails to address one other important issue: the trials have so far not
demonstrated that these vaccines prevent real morbiidity mortality.
Mike Smitka
December 10, 2020 at 1:22 pm
Stopping transmission would be nice. But instilling sufficient immunity to not become
seriously ill, much less die, is REALLY nice. If we could cut our current 3,000 deaths a day
by even 50%, wouldn't that be great?
Note I am a month into recovery from COVID, caught from my son, who probably caught it
from anti-maskers at the factory where he works. (He's in a high-metal-dust environment, his
clothes are a different color by the end of the day, so for someone to not wear a mask is
political correctness taken way too far.) We were both fortunate – he was back to
12-hours days once his quarantine was done. I still have some head cold symptoms, but it is
that time of year. However, I know multiple people who have been hospitalized, and one person
who died. One 30-something RN whose avocation is boxing (eg, he was in extraordinary physical
condition) ended up critical. And all this was before Thanksgiving, before the current
explosion of cases and consequent deterioration of the care that those critically ill will
receive.
As to the math, it's unfortunate from a statistical sense that right now wasn't the core
of the testing period. The number of cases among the placebo group would be far higher, and
it would be easier to explain to the vast majority of the population who are not trained in
statistical thinking. Even there humility is needed: I have formal training, graduate school
courses in math stats and econometrics, and decades of empirical work employing that
training. Nevertheless my reflexes remain those of a normal human in terms of misperceiving
the impact of long odds. I have to consciously apply my training.
Finally, the above paragraph reflects a mind game. It's not unfortunate in a human sense
that the vaccines are far enough along to grant provisional approval. If only they'd been
available even earlier
Skip Intro
December 10, 2020 at 2:35 pm
Am I being overly cynical, or does it occur to anyone else that making a vaccine that just
prevents symptoms but doesn't prevent infection and transmission will tend to make the virus
endemic, rather than extinguishing it. This will gradually increase the dangers to the
unvaccinated population, creating a class of sick whose 'access' to vaccination has not
actually provided vaccine. Assuming the vaccination will need to be refreshed, it also
creates a large group of hostages repeat customers. -- Nice lungs you got
there, it'd be a shame if somethin' were to happen to 'em
Baldanders
December 10, 2020 at 5:32 pm
And here we see the inevitable result of poor analysis: the author speculates the vaccine
may not prevent transmission; of course, many readers interpret this as "the vaccine doesn't
stop transmission" and now will spread this speculation as rock hard fact.
I'm starting to think the best health measure we could take would be to dismantle the
internet. Crowdsourced wisdom will be our end.
tegnost
December 10, 2020 at 8:37 pm
another option is ending public health as a path to riches, as this is the primary reason
for most of the skepticism, who would you like to blame that on?
Seems to me it's the inevitable result of a broken health care system
Skip Intro
December 11, 2020 at 12:59 am
Your reading comprehension seems poor.
rusti
December 11, 2020 at 1:19 am
By requiring that the vaccine provides durable sterilizing immunity you've set the bar
higher, maybe by orders of magnitude, I don't think the science is there for anyone to know
for this virus.
I think Mike Smitka makes a compelling case for setting a lower threshold in preventing
serious disease is priority number one, and one can say that without being a shill for the
pharma companies. If none of the vaccines provide durable immunity it is of course great for
their collective bottom lines, but if you know of an immunologist who thinks that they're
doing so deliberately I would be very interested to see a link.
Nick Alcock
December 11, 2020 at 1:27 pm
Errr this disease is endemic. With approaching a billion likely cases at this
point, extinguishing it is a pipe-dream. It'll be almost as hard to exterminate as it is to
exterminate the flu. That horse has left the barn. It probably left the barn before the end
of last year
Mike Smitka
December 12, 2020 at 10:13 am
Indeed. At least at present, however, there is one big difference with flu: low levels of
mutation (perhaps zero = a single strain) for the surface proteins of SARS-CoV-2, so that the
vaccines currently being approved will continue to be effective. So while we may need a
booster every year or two, depending on how long the immunity from a given vaccine, it will
"work."
In contrast flu vaccines protect against only a few strains (the most common vaccine type
in the US targets 3), but with many, many strains in circulation at any given time (and new
ones arising on a regular basis), those may not be the right strains. Hence new vaccines are
developed 2x a year to target the strains epidemiologists predict will be the most prevalent.
They can for example look at the strains prevalent in the winter in the southern hemisphere,
and use what they see to guide their choices. Ditto what's going on in winter in the north to
guide vaccines for administration in the south. Needless to say, those predictions are not
always accurate, and even if they do target the 3 most prevalent strains, you may by chance
be exposed to one of the strains not included. Adding more strains to the flu vaccine doesn't
work, as the body won't react equally to all of them: put in 6 strains, and your body may
generate weak immunity to 2, very weak to another 2, and none at all to the last 2. (My body
might develop moderate immunity to 1 and none to 5.)
Over time we may see substantive mutations that affect vaccine efficacy. But with the
current vaccines, it would in principle be possible to wipe out the virus that causes COVID,
assuming that a very high proportion of the population gets vaccinated (and potentially
revaccinated), and constant monitoring for new zoonotic outbreaks among humans catching it
from animal populations in which it would remain endemic.
I don't expect that to happen. That's because, thankfully, average mortality rates for
COVID are well under 1%, whereas for smallpox they were 20%-30%. Too many people will be lax
about immunizations, while governments will not enact the draconian policies that would be
needed to offset that – unlike if we saw a reemergence of smallpox.
Lins
December 10, 2020 at 11:20 pm
I am frustrated but hopeful that viable treatments will be approved for use like CytoDyn's
Leronlimab. I personally would choose a proven safe and effective treatment vs any of the
vaccines!
rusti
December 10, 2020 at 11:56 pm
Antiviral treatments or monoclonal antibodies are only useful if you apply them very early
in the course of disease. Most people, by the time they show up in the hospital, can not
benefit from these treatments and can have worse outcomes. I suggest searching for Dr. Daniel
Griffin's material about the "phases of covid" to understand how clinical protocols are
evolving.
Eric J
December 12, 2020 at 1:07 am
The real questions is
"With only about 20,000 people have received this Pfizer's vaccine. Will unexpected
safety issues arise when the number grows to millions and possibly billions of people? Will
side effects emerge with longer follow-up? Implementing a vaccine that requires two doses
is challenging. What happens to the inevitable large number of recipients who miss their
second dose? How long will the vaccine remain effective? Does the vaccine prevent
asymptomatic disease and limit transmission? And what about the groups of people who were
not represented in this trial, such as children, pregnant women, and immunocompromised
patients of various sorts?"
Otto V.
December 12, 2020 at 8:02 am
I can 100% answer at least the last question: the vaccine has not been approved for
children nor pregnant woman, and immunocompromised people never get vaccines. They are
protected by herd immunity or not at all. Same for people with allergic reactions to any of
the vaccine components.
As usual, we won't have the answer to most of the other questions until we're further into
Phase IV, which just started.
Philthy_Stacker 2 hours ago (Edited) remove link
Several vaccine candidates are expected to induce the formation of humoral antibodies
against spike proteins of SARS-CoV-2. Syncytin-1 (see Gallaher, B., "Response to nCoV2019
Against Backdrop of Endogenous Retroviruses" -
http://virological.org/t/response-to-ncov2019-against-backdrop-of-endogenous-retroviruses/396
, which is derived from human endogenous retroviruses (HERV) and is responsible for the
development of a placenta in mammals and humans and is therefore an essential prerequisite
for a successful pregnancy, is also found in homologous form in the spike proteins of SARS
viruses.
There is no indication whether antibodies against spike proteins of SARS viruses would
also act like anti-Syncytin-1 antibodies. However, if this were to be the case this would
then also prevent the formation of a placenta which would result in vaccinated women
essentially becoming infertile.
To my knowledge, Pfizer/BioNTech has yet to release any samples of written materials
provided to patients, so it is unclear what, if any, information regarding (potential)
fertility-specific risks caused by antibodies is included.
DrBrown 8 hours ago (Edited)
Cycle threshold is everything with the PCR test. Anything above 35 is rubbish. 97% false
positives. Chris Martenson just presented some compelling information regarding these tests.
A recent paper basically shoots down a paper ( Corman-Drosten paper ) that was rushed to
press (before any real peer review) in January 2020 that declared the PCR test the end all
best way to test for covid. NOT TRUE. It was never meant for this purpose and is now being
grossly abused by TPTB. The paper says:
3. The number of amplification cycles (less than 35; preferably 25-30 cycles); In case of
virus detection, >35 cycles only detects signals which do not correlate with infectious
virus as determined by isolation in cell culture [reviewed in 2]; if someone is tested by PCR
as positive when a threshold of 35 cycles or higher is used (as is the case in most
laboratories in Europe & the US), the probability that said person is actually infected
is less than 3%, the probability that said result is a false positive is 97% [reviewed in
3]
Most testing sites are using a cycle threshold of 40 or more meaning the results mean
nothing. In fact many labs are using a CT of 47! The paper goes on to say:
3. The number of amplification cycles It should be noted that there is no mention anywhere
in the Corman-Drosten paper of a test being positive or negative, or indeed what defines a
positive or negative result. These types of virological diagnostic tests must be based on a
SOP, including a validated and fixed number of PCR cycles (Ct value) after which a sample is
deemed positive or negative. The maximum reasonably reliable Ct value is 30 cycles. Above a
Ct of 35 cycles, rapidly increasing numbers of false positives must be expected . PCR data
evaluated as positive after a Ct value of 35 cycles are completely unreliable. Review Report
by an International Consortium of Scientists in Life Sciences (ICSLS) - Corman-Drosten et
al., Eurosurveillance 2020 (Updated: 29.11.2020) Citing Jaafar et al. 2020 [3]: "At Ct = 35,
the value we used to report a positive result for PCR, <3% of cultures are positive." In
other words, there was no successful virus isolation of SARS-CoV-2 at those high Ct values.
Further, scientific studies show that only non-infectious (dead) viruses are detected with Ct
values of 35 [22]. Between 30 and 35 there is a grey area, where a positive test cannot be
established with certainty. This area should be excluded. Of course, one could perform 45 PCR
cycles, as recommended in the Corman-Drosten WHO-protocol (Figure 4), but then you also have
to define a reasonable Ct-value (which should not exceed 30). But an analytical result with a
Ct value of 45 is scientifically and diagnostically absolutely meaningless (a reasonable
Ct-value should not exceed 30). All this should be communicated very clearly. It is a
significant mistake that the Corman-Drosten paper does not mention the maximum Ct value at
which a sample can be unambiguously considered as a positive or a negative test-result. This
important cycle threshold limit is also not specified in any follow-up submissions to
date.
Hillary's Fish Taco 6 hours ago remove link
The PCR test will go down in history as the biggest part of this scamdemic. Covid 19 was a
novel virus resulting in a bad flu that killed the elderly and the already ill.
That will be Covid's legacy...the politicians will be shamed for all eternity.
For The First Time, A US State Will Require Disclosure Of PCR 'Cycle Threshold' Data In
COVID Tests by Tyler
Durden Sun, 12/06/2020 - 10:45 Twitter Facebook Reddit Email Print
We have detailed the controversy surrounding America's COVID "casedemic" and the misleading
results of the PCR test and its amplification procedure in great detail over the past few
months.
As a reminder, "cycle thresholds" (Ct) are the level at which widely used polymerase chain
reaction (PCR) test can detect a sample of the COVID-19 virus. The higher the number of cycles,
the lower the amount of viral load in the sample; the lower the cycles, the more prevalent the
virus was in the original sample.
Numerous epidemiological experts have argued that cycle thresholds are an important metric
by which patients, the public, and policymakers can make more informed decisions about how
infectious and/or sick an individual with a positive COVID-19 test might be. However,
as JustTheNews reports, health departments across the country are
failing to collect that data .
Here are a few headlines from those experts and scientific studies:
1. Experts compiled three datasets with officials from the states of Massachusetts, New York
and Nevada that conclude: "Up to 90% of the people who tested positive did not carry a
virus."
2. The Wadworth Center, a New York State laboratory, analyzed the results of its July
tests at the request of the NYT: 794 positive tests with a Ct of 40: " With a Ct threshold of
35 , approximately half of these PCR tests would no longer be considered positive ," said the
NYT.
"And about 70% would no longer be considered positive with a Ct of 30! "
3. An appeals court in Portugal has
ruled that the PCR process is not a reliable test for Sars-Cov-2 , and therefore any
enforced quarantine based on those test results is unlawful.
4. A new study from the
Infectious Diseases Society of America , found that at 25 cycles of amplification, 70% of
PCR test "positives" are not "cases" since the virus cannot be cultured, it's dead. And by
35: 97% of the positives are non-clinical.
5. PCR is not testing for disease, it's testing for a specific RNA pattern and this is the
key pivot. When you crank it up to 25, 70% of the positive results are not really "positives"
in any clinical sense , since
it cannot make you or anyone else sick
So, in summary, with regard to our current
"casedemic", positive tests as they are counted today do not indicate a "case" of anything.
They indicate that viral RNA was found in a nasal swab. It may be enough to make you sick, but
according to the New York Times and their experts, probably won't. And certainly not sufficient
replication of the virus to make anyone else sick. But you will be sent home for ten days
anyway, even if you never have a sniffle. And this is the number the media breathlessly
reports... and is used to fearmonger mask mandates and lockdowns nationwide...
https://platform.twitter.com/embed/index.html?dnt=false&embedId=twitter-widget-0&frame=false&hideCard=false&hideThread=false&id=1335459652004286466&lang=en&origin=https%3A%2F%2Fwww.zerohedge.com%2Fmedical%2Ffirst-time-us-state-will-require-disclosure-pcr-test-cycle-data&partner=tweetdeck&siteScreenName=zerohedge&theme=light&widgetsVersion=ed20a2b%3A1601588405575&width=550px
about:blank
about:blank
me title=
All of which is background for an intriguing decision made by Florida's Department of Health
(and signed off on by Florida's Republican Governor Ron deSantis).
For the first time in the history of the pandemic, a state will require that all labs in the
state report the critical "cycle threshold" level of every COVID-19 test they perform .
All positive, negative and indeterminate COVID-19 laboratory results must be reported to
FDOH via electronic laboratory reporting or by fax immediately. This includes all COVID-19
test types - polymerase chain reaction (PCR), other RNA, antigen and antibody results.
Cycle threshold (CT) values and their reference ranges , as applicable, must be reported
by laboratories to FDOH via electronic laboratory reporting or by fax immediately.
Full press release below:
Try this on for size, pulled it from the comments at Naturalnews.com :
I have a PhD in virology and immunology. I'm a clinical lab scientist and have tested 1500
"supposed" positive Covid 19 samples collected here in S. California. When my lab team and I
did the testing through Koch's postulates and observation under a SEM (scanning electron
microscope), we found NO Covid in any of the 1500 samples.
What we found was that all of the 1500 samples were mostly Influenza A and some were
influenza B, but not a single case of Covid, and we did not use the B.S. PCR test.
We then sent the remainder of the samples to Stanford, Cornell, and a few of the University
of California labs and they found the same results as we did, NO COVID. They found influenza A
and B.
All of us then spoke to the CDC and asked for viable samples of COVID, which CDC said they
could not provide as they did not have any samples. We have now come to the firm conclusion
through all our research and lab work, that the COVID 19 was imaginary and fictitious. The flu
was called Covid and most of the 225,000 dead were dead through co-morbidities such as heart
disease, cancer, diabetes, emphysema etc. and they then got the flu which further weakened
their immune system and they died. I have yet to find a single viable sample of Covid 19 to
work with. We at the 7 universities that did the lab tests on these 1500 samples are now suing
the CDC for Covid 19 fraud. the CDC has yet to send us a single viable, isolated and purifed
sample of Covid 19.
If they can't or won't send us a viable sample, I say there is no Covid 19, it is
fictitious. The four research papers that do describe the genomic extracts of the Covid 19
virus never were successful in isolating and purifying the samples. All the four papers written
on Covid 19 only describe small bits of RNA which were only 37 to 40 base pairs long which is
NOT A VIRUS. A viral genome is typically 30,000 to 40,000 base pairs. With as bad as Covid is
supposed to be all over the place, how come no one in any lab world wide has ever isolated and
purified this virus in its entirety? That's because they've never really found the virus, all
they've ever found was small pieces of RNA which were never identified as the virus anyway. So
what we're dealing with is just another flu strain like every year... play_arrow 30
play_arrow
Gunston_Nutbush_Hall 3 hours ago (Edited)
Tks my point exactly in general, setting aside any Trump innuendo but keeping straight up
"scientific method(s)"
And if I were to continue my post it would be similar based upon what you have written
hereto:
Sorry Rick DeSantis, the question I would have been really impressed by you asking is not
the back end falsifiable PCR testing but the front end question I have been asking for 12
months!: please provide me from five different independent laboratories, via independent gold
standard, an empirically isolated, separated, purified, and replicated as sole direct
external biological causation agent, for one or all "COVID19" symptoms to any human being, as
"contagious/pathogenic" "virus."
I would nominate Rick DeSantis for the Nobel Prize on that experiment! ;-)
Sardonicus 3 hours ago
No one is testing for, or counting, financial deaths.
There are way more of those.
sparkadore 2 hours ago
The brainwashing is very real. The MSM simply report the daily memo sent to them by the
spin Doctors in the alphabet agencies. Social media and search engine algorithms have been
adjusted to assist you in RightThink.
That leaves the comment section in zh as the voice in the wilderness.
God help us all.
Bastiat 2 hours ago
Heard from a friend the other day: an elderly health compromised couple both got ill and
went to the doctor to get tested for flu. The doctor tested them for COVID and, surprise,
they both came back "positive." No test for flu. So, 2 new "COVID cases" and perhaps another
"COVID" death. Meanwhile flu deaths have dropped off the chart for the season.
Decimus Lunius Luvenalis 3 hours ago
And this is how the imbecile Biden and his ilk will claim 'victory' over the vid. They
chose 'cases' as the benchmark so they'll simply change how a 'case' is defined all the while
hiding behind the 'science' while never citing the 'science' or explaining why their cherry
picked 'science' is valid.
How interesting that 'science' has now been transformed by those that desire to 'rule'
into religious mystery. It must be believed, never questioned, you are guilty of something
and therefore must self-regulate, but they'll provide absolution.
idontcare 2 hours ago (Edited)
Truth if you consider that only 6% of the 277K+ deaths have been categorized as CV19
deaths without co-morbidities according to the CDC's own data. My # just uses the total # of
"reported deaths" ("w/ CV" not necessarily "from CV") accdg to the CDC.
Patrick Bateman Jr. 1 hour ago
I just divided 260,000 by 350 million. My math might be off. But that 99.999 stretches out
even farther into the 9's if we take out the Covid deaths with co-morbidities and use the
6%.
We are destroying an entire way of life and allowing the media, state, and others to
dictate our behavior in our homes over a stronger variant of the flu that has virtually no
chance of killing us. You can go mad thinking about it too much
ThePub'Lick_Hare 2 hours ago
Time for every state to follow Florida by class action suit. This farce has gone on too
long. Kudos to Florida for taking the initiative. Now at last people can ask relevant
questions and insist on proper protocol. The Portuguese High Court saw false COVID testing
for what it is, the spark and flame of a reign of terror. Time to douse the flames and the
douche-bags inflaming the scam-demic.
Ajax_USB_Port_Repair_Service_ 3 hours ago (Edited)
Lowering the test magnification nation wide would be a brilliant covid rescue plan for
whoever wins the presidency.
daveO 3 hours ago
Whoever wins the presidency is not running this SCAMDEMIC. But, yes, they will do it by
spring.
Ajax_USB_Port_Repair_Service_ 2 hours ago (Edited)
" Whoever wins the presidency " Will get the credit.
Agree, covid hysteria is being controlled by some group more powerful than our
president.
deFLorable hillbilly 2 hours ago (Edited)
Ron DeSantis is the best governor, by far, in any of the 57 states.
He is fearless and pro-American.
PS- I forgot about Noem in SD. It’s a tie. That chick rocks red, white and blue
too.
LiberateUS 2 hours ago (Edited)
#3 .Desantis is extremely knowledgeable about the pcr test, extremely intelligent, and a
person of integrity. C 19 is just another annual flu that affects only already sick or very
elderly people. He knows that, and using CT of 25 or lower will reveal only people who have a
virus load that will cause symptoms and illness. Those are the people that need medical
attention. Everyone has small virus particles in their bloodstream, which are harmless.
Vaccines inject viruses into your bloodstream.
bustdriver 2 hours ago
"Approximately 150,000 people die every day, worldwide. That’s 52 million people
that have died so far this year. Cardiovascular diseases (CVDs) are the number 1 cause of
death globally, taking an estimated 17.9 million lives each year. Close to 800,000 people die
due to suicide every year, which is one person every 40 seconds.
Coronavirus has killed 1.5 million people worldwide so far this year.
fackbankz 2 hours ago
I bet you'll see a marked decrease in deaths from CVDs in 2020 because a lot of them are
being blamed on Covid-1984.
Highly recommended !
The lockdowns are based on surging "cases" which are based on positive PCR test results.
However, what exactly is a positive PCR test result? What does it mean? As Dr. Tommy Megremis
summarized recently :
If you are generally aware, the PCR test is used to amplify small amount of genetic
material so as to recognize patterns of DNA by "cycling." (Also, for RNA virus, the RNA is
converted to DNA in order to be detected, it's just the way the test works) This is how we
have been able to recognize the genomes in Egyptian mummies and Wooly Mammoths. It works
because if you amplify and cycle enough times to "grow" legitimate DNA fragments, you get
something with with a fair amount of specificity. W hat is becoming more and more apparent is
that the PCR test was not designed as a diagnostic tool for infection, and really cannot
function as one without having a huge amount of false positives, period.
When it comes to COVID, the presence of viral particles picked up by the PCR technique
does not and has not been quantitatively linked to an active "symptomatic" infection. It
simply cannot be so, because infection threshold as a result of viral load is different for
each patient. It turns out, if you "cycle" over around 25 times, the false positivity of
COVID infection starts getting very high.
I and others have explained in blogs how people can be exposed to virus, and mount a
simple innate immune response and never know any differently. When you test these people with
very low viral loads, who are not sick, you can find the viral RNA code that is used to
"diagnose" if you cycle enough times. The last I read, Labcorp cycles at least 40 times to
detect viral genome fragments. The PCR test was never intended for diagnosis of infection but
as a qualitative test for presence of parts of a virus genome. I know there has been some
confusion circulating the net about what the inventor Kary Mullis had said about that. But we
walk daily with people who have any number of parts of killer virus or bacterial genomes
which one could pick up with a PCR test if one had the specific test for it. Would we claim
that that individual was an infected patient? No!
So given all that, PeakProsperity's Chris
Martenson explains below , in great details, the answer to the most important question you
should ask if you or a loved one gets a positive PCR test result .
"What's the Cycle Threshold (CT) value for that test?"
Sounds wonky but it's actually really important to understand. A low CT value means someone
is loaded with virus. A high value, oppositely, means less of a viral load.
Beyond a certain level the load is insufficient to either infect someone else or be of any
clinical or epidemiological relevance whatsoever.
The problem? Governments all over the country and world are basing their decisions on CT
values that are very high. Too high.
https://www.youtube.com/embed/eWqNl4UUlH0
https://lockerdome.com/lad/13084989113709670?pubid=ld-dfp-ad-13084989113709670-0&pubo=https%3A%2F%2Fwww.zerohedge.com&rid=www.zerohedge.com&width=890
* * *
Links:
WHO PCR 47 (!) Cycles
https://www.who.int/diagnostics_laboratory/eul_0489_185_00_path_covid19_ce_ivd_ifu_issue_2.0.pdf?ua=1
CT over 35 is non-infectious
https://www.infectiousdiseaseadvisor.com/home/topics/covid19/ct-value-may-inform-when-patients-with-covid-19-can-be-safely-discharged/
Cycle Thresholds Too Damn High
https://www.nytimes.com/2020/08/29/health/coronavirus-testing.html
Corman Drosten retraction request
https://cormandrostenreview.com/report/
Bad Testing Video Sept 1
NEVER MISS THE NEWS THAT MATTERS MOST
ZEROHEDGE DIRECTLY TO YOUR INBOX
Receive a daily recap featuring a curated list of must-read stories.
https://youtu.be/ZFNdsRHKUM4
UK PCR positive standards
https://www.england.nhs.uk/coronavirus/wp-content/uploads/sites/52/2020/03/guidance-and-sop-covid-19-virus-testing-in-nhs-laboratories-v1.pdf
Kansas CT cutoff of 42
https://www.coronavirus.kdheks.gov/DocumentCenter/View/1505/SARS-CoV-2-COVID-19-PCR-Ct-Cutoff-Values-PDF
-- 10-5-20
span
6 hours ago remove link
Jon Rappoport (excellent blog) nails it in some of his recent posts.
.
"July 16, 2020, podcast, 'This Week in Virology': Tony Fauci makes a point of saying the
PCR Covid test is useless and misleading when the test is run at '35 cycles or higher.' A
positive result, indicating infection, cannot be accepted or believed.
"Here, in techno-speak, is an excerpt from Fauci's key quote: ' If you get [perform the
test at] a cycle threshold of 35 or more the chances of it being replication-competent [aka
accurate] are miniscule you almost never can culture virus [detect a true positive result]
from a 37 threshold cycle even 36 '
"Too many cycles, and the test will turn up all sorts of irrelevant material that will be
wrongly interpreted as relevant.
"That's called a false positive.
"What Fauci failed to say on the video is: the FDA, which authorizes the test for public
use, recommends the test should be run up to 40 cycles. Not 35.
"Therefore, all labs in the US that follow the FDA guideline are knowingly or unknowingly
participating in fraud. Fraud on a monstrous level, because millions of Americans are being
told they are infected with the virus on the basis of a false positive result, and
"The total number of Covid cases in America -- which is based on the test -- is a gross
falsity.
"The lockdowns and other restraining measures are based on these fraudulent case
numbers.
play_arrow
GenuineAmerican 3 hours ago
Fauci has lied again the PCR maximum cycle for a accurate test results is 25 NOT 35. PCR
is run, or should be run at 21-25 cycles everything else will give a false positive. Had a
friend in Scottsdale MAYO. I had to go to this god-forsaken place to get him out. They were
running the PCR at 42 cycles to keep him in the hospital because he had very, very good UNION
insurance!! The health industries are all crooks, lying to people to get more money being
paid to the orgainizations by the feds.
BaNNeD oN THe RuN 7 hours ago
IQ tests were always seriously flawed, just like the PCR test
https://medium.com/incerto/iq-is-largely-a-pseudoscientific-swindle-f131c101ba39
It does not measure creative or lateral thinking ability at all.
I had scores that put me in the top 0.5% but I had no illusion that made me anything more
than a good test taker.
NatsarimAmericanoLion 6 hours ago
Giorgio Palmas 21 hours
ago
U.S TOTAL DEATHS
choctaw charley 5 hours ago remove link
so what's the purpose behind the bogus plandemic. In order to institute a one world
plantation several things have to happen. Foremost is the sense of "nationhood". a nation can
be thought of as modeled on the family unit. We look similar, we share religious beliefs,
economic and political views and we have a common history which we take pride in. We trust
rely on and help another. If you have half a brain you don't need me to describe how all
these are under attack. So how does the plandemic play into this? Yesterday you neighbor was
your neighbor. Today he is behind a mask because the government tells you that he is a threat
to you and your family and you to his! The plandemic was used to to hugely expand the mail-in
ballot fraud further driving in the wedge suspicion. Then there is this: when you get your
covid test there will be a permanent file created with your name on it. It will contain your
genetic code and the test result. this will become the social register that is all over
Europe. Get a traffic ticket; late in making a payment; engage in disapproved political
activity as I am doing at this moment? All these will find their way into your file and will
in the future determine the rate you pay on your home mortgage whether you can be employed in
a government job, what you have to endure to board a commercial aircraft etc. There is also a
great likelihood that contained in the vaccine will be a tracking component. Consider also
population segment most vulnerable to covid: older retired people drawing on an already
bankrupt social security ponzi scheme. Hitler referred to these as "Useless Eaters". He had a
system in place to rid society of these. Later these faciliries were expanded to include the
Jewish population.
flyonmywall 9 hours ago
I've done lots of PCR in my life. If you have to do over 35 cycles to detect or amplify
something, you're probably barking up the wrong tree or there is something wrong with your
assay.
Once you ramp up the cycles to past 35-40 cycles, you're just amplifying non-specific
competing amplification products, of which there are always some.
You could have the best designed primers in the world, there is always some random ****
that happens to get amplified at high cycle counts.
Zero-Hegemon 4 hours ago
False positives are beneficial for obtaining COVID money and creating hysteria.
KimAsa 9 hours ago (Edited)
these psychopaths have redesignated the normal course of annual deaths from heart disease,
and other common ailments that old people die from, to Covid 19, to create the illusion of a
deadly pandemic. they claim to have isolated this virus out of one side of their mouth, out
the the other side they claim it has mutated (how many times?) so can't produce proof that
this virus even exists. and out of their ******* they claim to have developed a vaccine?
this is and always has been about the vaccinating the public for free moral agency
prevention.
Ride_the_kali_yuga 9 hours ago
Covid "tests" are an efficient way to feed the false pandemic narrative with nonsensical
numbers of "contaminations". Masks are a mark of submission.
africoman 9 hours ago
Re-posting someone's comment from this article
Here
If the masks work -- Why the six feet?
If the six feet works -- Why the masks?
If both of the above work -- Why the lockdowns?
If all three of the above work -- Why the vaccine?
If the vaccine is safe -- Why protect it with a no liability clause?
If the vaccine is safe---Why not test it on animals first before using it on
humans?
If SARS-CoV-2 exists -- Why has it never been isolated?
If SARS-CoV-2 has never been isolated -- How can an effective vaccine be
developed?
If the RT-PCR test works -- Why so many false positives?
If Kary Mullis, the inventor of the RT-PCR test who conveniently died in August 2019,
says his test shouldn't be used to diagnose infectious diseases -- Why use it to detect
SARS-CoV-2?
If there is an epidemic---Why so many empty hospitals?
If large numbers of people are dying from SARS-CoV-2---Why so many fake causes of death
on death certificates?
If SARS-CoV-2 exists -- Why give doctors financial incentives to diagnose
SARS-CoV-2?
If the official COVID-19 narrative is defensible -- Why censor people who dispute this
narrative?
by John Wear, (retired) lawyer, accountant, and author.
Excellent points, now let's threw a monkey wrench in it to the Operation Warp Speed
play_arrow
Schooey 6 hours ago
Its all BS
KimAsa 9 hours ago (Edited)
these psychopaths have redesignated the normal course of annual deaths from heart disease,
and other common ailments that old people die from, to Covid 19, to create the illusion of a
deadly pandemic. they claim to have isolated this virus out of one side of their mouth, out
the the other side they claim it has mutated (how many times?) so can't produce proof that
this virus even exists. and out of their ******* they claim to have developed a vaccine?
this is and always has been about the vaccinating the public for free moral agency
prevention.
Ms No 8 hours ago
They actually murdered people with the lockdown too though. Knowingly and
premeditated...certainly some of those were also declared covid.
smacker 8 hours ago
" this is and always has been about the vaccinating the public "
Correct.
That has become clear. What we are only now slowing learning is what the sinister motive
is.
kellys_eye 9 hours ago
Is the test for Covid or Covid-19. Can it tell the difference? The 'normal' flu and
influenza are both corona viruses and this is the 'high season' for such cases in the
Northern hemisphere.
Strangely (or not) the incidence of actual flu and influenza are suspiciously MUCH lower
than they should be.
Ergo - tests that prove 'positive' for Covid are likely either false OR reporting on the
flu/influenza.
The LIES keep mounting and mounting.
Harry Tools 5 hours ago
there is no pandemic
RedNeckMother 3 hours ago
I will add another: FDA: 40 recommendation for testing
And let's not forget the comments by Fauci that if they're testing at 35 they're going to
get a lot of false positives.
There's an attorney in Ohio who has filed a FOI to obtain all the ct levels used by the
labs testing in Ohio. It will be very interesting once that is revealed - I'm sure our
governor already knows the answer. If I recall, the NYT itself did an article on this very
topic awhile back and estimated that 90% of the positive results in CT and NY were bogus. And
going from 40 to 35 I believe reduces positives by 63%.
We're being played.
MoreFreedom 5 hours ago remove link
Dr. Martenson's videos are very good. He's clear.
As for "the science" and scientists, we all make mistakes. If we didn't make mistakes, we
wouldn't have scientists pointing out other scientist's mistakes. But it's not a question of
whose science is correct, it's that science is no excuse for taking away peoples'
liberty.
SRV 7 hours ago
The inventor of the test (Dr Kary Mullis) was very outspoken that it was NOT developed for
human virus confirmation...he died of cancer just weeks before the first Covid cases
(hmmmm).
It's in your face proof of the scam we're all being subjected to that almost no one ever
questioned (brilliant move really)... ONE cycle above 35 (each cycle doubles the
amplification) will explode the the false positives.
And... if you have no symptoms you DO NOT have the virus (remember how much play the
"asymptomatic" BS story got early on... another psyop). Notice how none of the athletes never
get sick and are back in two weeks... yet it's never questioned by a soul paid to look the
other way!
smacker 9 hours ago
" What is becoming more and more apparent is that the PCR test was not designed
This is not knew and didn't need to become "more and more apparent".
The inventor of the PCR test Kary Mullis is on video record stating it. Sadly his
expert
It's time to prepare the gallows and stock up with rope.
smacker 7 hours ago remove link
The PCR test is used precisely because it can be manipulated to produce as many "cases" as
wanted.
Just turn the dial up on "amplification cycles" and hey presto, you get as many positives
as you want.
The cases are not genuine cases but simply PCR positive tests, but are reported as "cases"
and then
The idea is "FEAR Management" which allows draconian CovID rules like lockdowns and tiers
and
It then ramps up demand for vaccines which is the ultimate objective. Initially (or soon
after), the
We are seeing in plain sight the biggest coup ever against mankind.
It must be stopped.
smacker 7 hours ago remove link
The PCR test is used precisely because it can be manipulated to produce as many "cases" as
wanted.
Just turn the dial up on "amplification cycles" and hey presto, you get as many positives
as you want.
The cases are not genuine cases but simply PCR positive tests, but are reported as "cases"
and then
The idea is "FEAR Management" which allows draconian CovID rules like lockdowns and tiers
and
It then ramps up demand for vaccines which is the ultimate objective. Initially (or soon
after), the
We are seeing in plain sight the biggest coup ever against mankind.
It must be stopped.
A Japanese research team said Wednesday that it has detected neutralizing antibodies in 98%
of people six months after they were infected with SARS-CoV-2. Another study performed in the
UK found that antibodies found evidence that antibody
levels start to degrade within six months.
The team, led by Yokohama City University professor Takeharu Yamanaka, is already planning
to conduct a follow-up study to see whether these people will still have such antibodies a year
after their infections.
But in the survey data released Wednesday, researcher checked blood samples from 376 people
who had already recovered - the largest study of its type in Japan. The samples were collected
six months after the patients were infected.
According to a report on the study published by Nippon, Yamanaka said that "in general,
people with neutralizing antibodies are believed to carry a low risk of reinfection...This
gives some hope" for the effectiveness of the vaccines that are soon to be delivered to the
public.
As the west prepares to roll out the first wave of COVID-19 vaccinations, scientists will be
watching closely for more data to try an ascertain whether COVID-19 can truly be defeated, or
whether it might morph into a flu-like seasonal infection.
By Peter Andrews , Irish science journalist and writer based in London. He has a
background in the life sciences, and graduated from the University of Glasgow with a degree in
genetics A peer review of the paper on which most Covid testing is based has
comprehensively debunked the science behind it, finding major flaws. They conclude it's utterly
unsuitable as a means for diagnosis – and the fall-out is immense.
Last week, I reported on a landmark ruling from
Portugal, where a court had ruled against a governmental health authority that had illegally
confined four people to a hotel this summer. They had done so because one of the people had
tested positive for Covid in a polymerase chain reaction (PCR) test – but the court had
found the test fundamentally flawed and basically inadmissible.
Now the PCR testing supremacy under which we all now live has received another crushing
blow. A peer review from
a group of 22 international experts has found 10 "major flaws" in the main protocol for such
tests. The report systematically dismantles the original study , called the
Corman-Drosten paper, which described a protocol for applying the PCR technique to detecting
Covid.
The Corman-Drosten paper was published on January, 23, 2020, just a day after being
submitted, which would make any peer review process that took place possibly the shortest in
history. What is important about it is that the protocol it describes is used in around 70
percent of Covid kits worldwide. It's cheap, fast – and absolutely useless.
ALSO ON RT.COM Landmark
legal ruling finds that Covid tests are not fit for purpose. So what do the MSM do? They ignore
it The 10 deadly sins
Among the fatal flaws
that totally invalidate the PCR testing protocol are that the test:
is non-specific, due to erroneous primer design
is enormously variable
cannot discriminate between the whole virus and viral fragments
has no positive or negative controls
has no standard operating procedure
does not seem to have been properly peer reviewed
Oh dear. One wonders whether anything at all was correct in the paper. But wait – it
gets worse. As has been noted previously , no
threshold for positivity was ever identified. This is why labs have been running 40 cycles,
almost guaranteeing a large number of false positives – up to 97 percent, according to
some
studies.
The cherry on top, though, is that among the authors of the original paper themselves, at
least four have severe conflicts of interest. Two of them are members of the editorial board of
Eurosurveillance, the sinisterly named journal that published the paper. And at least three of
them are on the payroll of the first companies to perform PCR testing!
ALSO ON RT.COM YouTube
removes lockdown-sceptical interview with renowned immunologist Dr Mike Yeadon for 'violating
terms of service' Heroes we deserve
The 22 members of the consortium that has challenged this shoddy science
deserve huge credit. The scientists, from Europe, the USA, and Japan, comprise senior molecular
geneticists, biochemists, immunologists, and microbiologists, with many decades of experience
between them.
They have issued a demand to Eurosurveillance to retract the Corman-Drosten paper, writing:
" Considering the scientific and methodological blemishes presented here, we are confident
that the editorial board of Eurosurveillance has no other choice but to retract the
publication. '' Talk about putting the pressure on.
It is difficult to overstate the implications of this revelation. Every single thing about
the Covid orthodoxy relies on 'case numbers', which are largely the results of the now
widespread PCR tests. If their results are essentially meaningless, then everything we are
being told – and ordered to do by increasingly dictatorial governments – is likely
to be incorrect. For instance, one of the authors of the review is Dr Mike Yeadon, who
asserts that, in the
UK, there is no 'second wave' and that the pandemic has been over since June. Having seen the
PCR tests so unambiguously debunked, it is hard to see any evidence to the
contrary.
ALSO ON RT.COM All vaccines,
including the new Covid ones, carry a tiny risk of serious side effects. But does that mean we
shouldn't take them? The house of cards collapses
Why was this paper rushed to publication in January, despite clearly not meeting proper
standards? Why did none of the checks and balances that are meant to prevent bad science
dictating public policy kick into action? And why did it take so long for anyone in the
scientific community to challenge its faulty methodology? These questions lead to dark
ruminations, which I will save for another day.
Even more pressing is the question of what is going to be done about this now. The people
responsible for writing and publishing the paper have to be held accountable. But also, all PCR
testing based on the Corman-Drosten protocol should be stopped with immediate effect. All those
who are so-called current 'Covid cases', diagnosed based on that protocol, should be told they
no longer have to isolate. All present and previous Covid deaths, cases, and 'infection rates'
should be subject to a massive retroactive inquiry. And lockdowns, shutdowns, and other
restrictions should be urgently reviewed and relaxed.
Because this latest blow to PCR testing raises the probability that we are not enduring a
killer virus pandemic, but a false positive pseudo-epidemic. And one on which we are destroying
our economies, wrecking people's livelihoods and causing more deaths than Covid-19 will ever
claim.
Think your friends would be interested? Share this story!
The statements, views and opinions expressed in this column are solely those of the author
and do not necessarily represent those of RT.
gm , Dec 2 2020 0:16 utc |
187
Good one from Vanessa Beeley:
On Sean Penn as possible US deep state tool
Article also touches upon:
-reclusive Israeli billionaire, Vivi Nevo, who sounds from the write-up like a latter
day Jeffrey Epstein replacement figure
-use of covid rt-Pcr tests in US under ulterior motives as a HIPPA dodge to mass-collect
DNA for Big data/Big tracking and other purposes.
The PCR test, DNA harvesting and false positives
The validity of the PCR tests in diagnosing Covid-19 has been the subject of much
scientific discussion with a growing number of medical experts and analysts dismissing
the PCR test as unreliable and inconclusive due to the high percentage of false
positives. It is also claimed that this widespread DNA collection under the pretext of
Covid-19 could be a covert genetic information harvest on the pretext of extracting viral
DNA from all the genetic material.
I spoke with a medical expert who will remain anonymous for security reasons and he
informed me that the PCR test is "not designed to diagnose disease." He told me:
"The test identifies a genetic sequence being present in a sample and then copies
it, thereby increasing the amount of genetic material. Each test cycle copies and
increases the genetic material. A specific amount of GM is required to meet a threshold
of detection. The test will keep copying until it is possible to say the virus is
"detected". Therein lies the problem. After "Covid" infection, when the virus has been
removed by the immune system, some viral genetic debris can remain for many months. A
tiny fragment viral, genetic material debris will be found and multiplied by many, many
cycles until the detection threshold is reached. This is a false positive."
He informed me that most labs are running upwards of 40 cycles. "In at least 4
examples of RT PCR testing in the US, it was found that 90% of the positive tests were
actually false."
He also told me "the real reason they are pushing the testing is control. They want a
rapid test to be used every day, multiple times per day to gain entry to school, work,
restaurants, entertainment centres etc. It is conditioning."
The sinister question is whether all this genetic DNA information is passed on to
undisclosed entities for "research purposes" without the patient's knowledge.
gm , Dec 2 2020 1:37 utc |
188
Clear explanation of meaning of "Ct" (cycle threshhold) in nCoV "+" pcr test [ie What's
garbage and what's not]:
https://www.youtube.com/watch?v=eWqNl4UUlH0
By Peter Andrews , Irish science journalist and writer based in London. He has a
background in life sciences, and graduated from the University of Glasgow with a degree in
genetics. Four German holidaymakers who were illegally quarantined in Portugal after one
was judged to be positive for Covid-19 have won their case, in a verdict that condemns the
widely-used PCR test as being up to 97-percent unreliable.
Earlier this month, Portuguese judges upheld a decision from a lower court that found the
forced quarantine of four holidaymakers to be unlawful. The case centred on the reliability (or
lack thereof) of Covid-19 PCR tests.
The
verdict , delivered on November 11, followed an appeal against a writ of habeas corpus
filed by four Germans against the Azores Regional Health Authority. This body had been
appealing a ruling from a lower court which had found in favour of the tourists, who
claimed that they were illegally confined to a hotel without their consent. The tourists
were ordered to stay in the hotel over the summer after one of them tested positive for
coronavirus in a PCR test - the other three were labelled close contacts and therefore made to
quarantine as well.
Unreliable, with a strong chance of false positives
The deliberation of the Lisbon Appeal Court is comprehensive and fascinating. It ruled that
the Azores Regional Health Authority had violated both Portuguese and international law by
confining the Germans to the hotel. The judges also said that only a doctor can "diagnose"
someone with a disease, and were critical of the fact that they were apparently never assessed
by one.
READ MORE They were also scathing about the reliability of the PCR (polymerase chain reaction) test,
the most commonly used check for Covid.
The conclusion of their 34-page ruling included the following: "In view of current
scientific evidence, this test shows itself to be unable to determine beyond reasonable doubt
that such positivity corresponds, in fact, to the infection of a person by the SARS-CoV-2
virus."
In the eyes of this court, then, a positive test does not correspond to a Covid case. The
two most important reasons for this, said the judges, are that, "the test's reliability
depends on the number of cycles used'' and that "the test's reliability depends on the
viral load present.'' In other words, there are simply too many unknowns surrounding PCR
testing.
Tested positive? There could be as little as a 3% chance it's correct
This is not the first challenge to the credibility of PCR tests. Many people will be
aware that their results have a lot to do with the number of amplifications that are
performed, or the 'cycle threshold.' This number in most American and European labs is
35–40 cycles, but experts have claimed that even 35
cycles is far too many, and that a more reasonable protocol would call for 25–30 cycles.
(Each cycle exponentially increases the amount of viral DNA in the sample).
Earlier this year, data from three US
states – New York, Nevada and Massachusetts – showed that when the amount of the
virus found in a person was taken into account, up to 90 percent of people who tested positive
could actually have been negative, as they may have been carrying only tiny amounts of the
virus.
The Portuguese judges cited a study conducted by "some of the leading European and world
specialists," which was published by Oxford Academic at the end of September. It showed that
if someone tested positive for Covid at a cycle threshold of 35 or higher, the chances of that
person actually being infected is less than three percent, and that "the probability of
receiving a false positive is 97% or higher."
While the judges in this case admitted that the cycle threshold used in Portuguese labs was
unknown, they took this as further proof that the detention of the tourists was unlawful. The
implication was that the results could not be trusted. Because of this uncertainty, they stated
that there was "no way this court would ever be able to determine" whether the tourist
who tested positive was indeed a carrier of the virus, or whether the others had been exposed
to it.
READ MORE Sshhh – don't tell anyone
It is a sad indictment of our mainstream media that such a landmark ruling, of such obvious
and pressing international importance, has been roundly ignored. If one were making (flimsy)
excuses for them, one could say that the case escaped the notice of most science editors
because it has been published in Portuguese. But there is a full
English translation of the appeal, and alternative media managed
to pick it up.
And it isn't as if Portugal is some remote, mysterious nation where news is unreliable or
whose judges are suspect – this is a western EU country with a large population and a
similar legal system to many other parts of Europe. And it is not the only country whose
institutions are clashing with received wisdom on Covid. Finland's national health authority
has
disputed the WHO's recommendation to test as many people as possible for coronavirus,
saying it would be a waste of taxpayer's money, while poorer South East Asian countries are
holding off on ordering
vaccines, citing an improper use of finite resources.
Testing, especially PCR testing, is the basis for the entire house of cards of Covid
restrictions that are wreaking havoc worldwide. From testing comes case numbers. From case
numbers come the 'R number,' the rate at which a carrier infects others. From the 'dreaded' R
number comes the lockdowns and the restrictions, such as England's new and baffling tiered
restrictions that come into force next week.
The daily barrage of statistics is familiar to us all by this point, but as time goes on the
evidence that something may be deeply amiss with the whole foundation of our reaction to this
pandemic – the testing regime – continues to mount
vk
107
Pushed by Pandemic, Amazon Goes on a Hiring Spree Without Equal
The First World is leaving the "sweet spot" of its capitalist development stage, marked by
a relatively inflated petit-bourgeois middle class, and is reentering a proletarianization
phase. Call it the reproletarianization of the First World.
Looks like Marx was right all along.
vk
105
@ Posted by: Debsisdead | Nov 27 2020 1:35 utc | 69
You didn't read the link I provided. I'll recap:
1) Western Big Pharma "forgot" how to develop new vaccines over these last decades because
they're not profitable. That opened the gates for Gamaleya to occupy the sector, therefore
dominating the main technology used today, human adenovirus; (see Dmitriev's "forbidden
op-ed").
2) Sputnik V and Sinovac (and other Chinese variants) use a known, tested and tried
technology for their vaccines - human adenovirus -, while Pfizer, Moderna and AstraZeneca use
untested and untried technologies (mRNA and chimpanzee adenovirus). It is the difference
between the known and the unknown, except that this time hundreds of millions of human lives
are at the table. We suspect the Western pharmaceuticals are resorting to these exotic
technologies because they want something they can patent and sell at monopolistic prices to
national governments; (see Dmitriev's "forbidden op-ed" and his "questions")
3) mRNA technology is only effective theoretically. In the real world, it potentially has
devastating effects on the human body. It is already known it can potentially cause
infertility. It very likely has carcinogenic properties; (see Dmitriev's "questions")
4) chimpanzee adenovirus technology doesn't make any sense when you already have a viable
human adenovirus option. Besides the fact that it can cause more adverse effects on a human
(because the virus is strange to the human organism), the doctor I linked raised the question
of contamination when extracting the adenovirus from the chimpanzees (contamination rate of
10%, or one in ten). It also cause sever spinal cord inflammation - contrary to the official
version in much more than one patient. It also probably killed a healthy 28-year old subject
in the Brazilian trials (the Brazilian MSM initially "leaked" he was on the placebo group;
later even this version was put into doubt)
5) silver bullet vaccines are very rare (e.g. polio). Most likely scenario, these vaccines
will just shield you from a severe case of COVID-19, thus relieving the pressure over the
national healthcare systems. Deaths of COVID-19 only begin to pile up exponentially after the
limit of the healthcare system is surpassed (Italy). That's the "line of death", after which
COVID-19 really begins to ravage entire populations. In this scenario, it doesn't make any
sense not to go with the tried and tested technology of human adenovirus, over which Gamaleya
has primacy, or, second best, the Chinese vaccines, which will be produced the most because
China has manufacture supremacy. In the Russian and Chinese options, you have the choice
between the best and the most available - a common decision any working class family takes
daily in the free market for the purchase of their goods;
6) AstraZeneca will still have privileges in the British market. Evidence of this is the
British MSM being the first to publish the fake news that it had 90% efficacy, while the
American MSM went with the 70% figure. Make no mistakes: the AstraZeneca will be the only
option in the NHS for the British people, with or without transverse myelitis;
7) The "half dose" mistake simply doesn't happen in the Big Pharma. It is simply not
believable. The story is clearly a pathetic attempt of the British to create a comparison
with the story of the penicillin discovery (by a British scientist), which also happened by
accident. There wasn't half dose and, even if that really happened (the doctors involved
should be immediately fired), you would be giving credence to the homeopathy thesis, which
states the lower the dose, the stronger the effect. Doesn't make any sense.
AstraZeneca, by the way, is already feeling the heat. It will have to redo its trials
because nobody was born yesterday:
AstraZeneca considers extra global vaccine trial as questions mount
Down South , Nov 22 2020 17:17 utc |
9
Interesting read from F William Engdahl who takes a deeper look at the Pfizer
vaccine
Suspicious events
However it seems Albert Bourla, the CEO of Pfizer, doesn't share the confidence of his
own claims. On the day his company issued its press release on the proposed vaccine
trials, he sold 62% of his stock in Pfizer, making millions profit in the deal. He made
the sell order in a special option in August so it would not appear as "insider selling",
however he also timed it just after the US elections and the mainstream media
illegitimately declared Joe Biden President-elect.
It seems from appearances that Bourla had a pretty clear conflict of interest in the
timing of his press release on the same day.
What's
Not Being Said About Pfizer Coronavirus Vaccine
karlof1
60
It appears the Outlaw US Empire has put all its chips on the table in favor of vaccines
providing the path to "normalcy" :
"US Covid-19 vaccinations may begin as soon as December 11, reach enough people for
return to normalcy in May – program chief."
When was it determined that the two potential vaccines on offer have "efficacy rates of
about 95 percent" since the reports posted here were extremely dubious about them being
effective at all? More:
"An FDA vaccine advisory committee is scheduled to meet on December 10 and may grant
Pfizer's request for emergency use authorization that day, Dr. Moncef Slaoui said on Sunday
during an interview with CNN's Jake Tapper. The Trump administration stands ready to ship
the vaccine to immunization sites in all 50 states within 24 hours, he said, so the first
doses would be administered to recipients on December 11 or December 12."
As for a vaccine being a panacea, this is from the editorial I linked @56:
"The US has made certain breakthroughs in vaccine development, but so have China, Russia
and other countries. The US' attitude toward vaccines seems much too optimistic. As WHO
Director-General Tedros Adhanom Ghebreyesus said on November 16, ' A vaccine will
complement the other tools we have, not replace them a vaccine on its own will not end the
pandemic .'" [My Emphasis]
So yet again, the USA's citizenry is being told by the two institutions it trusts the
least--federal government and media--that the End is Near IF they imbibe the new
Miracle.
Gilead's remdesivir is not recommended for patients hospitalized with COVID-19, regardless
of how ill they are, as there is no evidence the drug improves survival or reduces the need for
ventilation, a World Health Organization panel said on Friday.
As researchers struggle to understand what makes infection with COVID-19 so mild in some
cases, and so deadly in others, we have kept a close eye out for any new links between symptoms
different strains of the virus. And on Wednesday we noticed new comments from South Australia's
top health official who warned that a particularly deadly strain of SARS-CoV-2 is circulating
in the state.
Chief Health Officer Professor Nicola Spurrier explained that the reason for the recently
imposed six-day lockdown is the fact that "this particular strain has had certain
characteristics" she said.
The State of South Australia,
which became home to this dramatic scene yesterday , is also bracing for the risk that this
new strain could spread more quickly, in addition to being more deadly. Professor Spurrier said
a typical generation, or stage, of the virus was only about three days.
"We also know, because of that characteristic, that what we call a generation, is only
about three days and a generation is when one case is passing it on to the next level, and
then that (next) level, so if they pass it on to two people, they will pass it on to another
lot of people, and that is your third generation," she said.
Already, the virus has progressed to the fifth generation, she said.
"At the moment in SA we have done contact tracing to the fourth generation but the fifth
generation is out there in our community and at the moment we are contact tracing to get on
to that generation and that is the Woodville pizza bar."
Authorities have traced the local outbreak to a pizza shop in Parafield. The cluster began
with a worker at Peppers Warmouth, which is being used as a quarantine hotel, was infected with
the virus.
ADKC , Nov 2 2020 3:28 utc |
76
The European Mortality Monitoring Project (EUROMOMO) has been monitoring excess mortality
in Europe since 2008 for the purpose of "detecting and measuring, on a real-time basis,
excess number of deaths related to influenza and other possible public health threats across
participating European Countries."
EUROMOMO's key metric is called the "z-score". Briefly, z-scores remove differences due to
seasons and populations so that they are directly comparable with different countries and
different time periods. More details on z-scores:
What is
a z-score?
The following link shows "z-scores by country":
Z-scores by country
The user can adjust the period sliders to examine any length of time between 2015 and
2020. For example, to examine the UK's z-scores for 2020 simply adjust the sliders to the
range 2020-01 to end (currently 2020-42). The user will be able to see that while there was a
problem with excess mortality for the period from 2020-12 to 2020-22 there has been no real
problem since. Also, the user will notice that a significant number of countries (e.g.
Austria, Denmark, Germany [partial, Hesse & Berlin only], Greece, Hungary, Norway) never
had any excess mortality problem.
Vasco da Gama , Nov 1 2020 23:49 utc |
56
Covid-19 is a dangerous disease and I take precautions to protect myself. However, the
public depiction of the disease in the media and the actions being taken by most
governments cannot but raise some very serious questions.
Posted by: Nathan Mulcahy | Nov 1 2020 18:14 utc | 16
THIS! Thank you for all your post Nathan! I was just about contributing some information
that ties in precisely with your concern:
COVID-19: Council adopts a recommendation to coordinate measures affecting free
movement (13-10-2020)
Based on this data, the ECDC should publish a weekly map of EU member states, broken down
by regions, to support member states in their decision-making. Areas should be marked in
the following colours:
green if the 14-day notification rate is lower than 25 and the test positivity rate
below 4%
orange if the 14-day notification rate is lower than 50 but the test positivity
rate is 4% or higher or, if the 14-day notification rate is between 25 and150 and the
test positivity rate is below 4%
red if the 14-day notification rate is 50 or higher and the test positivity rate is
4% or higher or if the 14-day notification rate is higher than 150
grey if there is insufficient information or if the testing rate is lower than
300
You will notice how the measures to be taken by individual countries are absolutely (as
in 100%) dependent on the worst metric possible according to the demonstrated
performance of rtPCR tests. We are being recommended to use the wrong metric! None of us
wishes any of our health systems to collapse, however their occupancy objectively varies
with the cumulative individual immune response of the population NOT with the
precariously measured transmissibility of SARS-CoV-2 via rtPCR tests. Remember that the
only reason we are worried about virus transmissibility is because of eventual severe
developments of the disease in a fraction of the population and a possible breakdown of
health systems as a consequence.
The relevant failure of rtPCR testing is its inability to estimate accurately the viral
load (let's not put in question the assumption that viral load is the most important
criteria for a severe development of C-19, while also leaving aside aggravating
comorbidities). rtPCR testing, under the current state of knowledge, is the equivalent of
measuring a patient's temperature with a thermometer but no doctor knows the average body
temperature, and its natural healthy interval, nor would the thermometer provide a number
on a scale, merely reporting that a patient has something other than "0". This would
constitute a USELESS thermometer.
From the same recommendation as above, quote:
Member states should not restrict the free movement of persons travelling to or from
green areas. [LOL - great opening, they know full well under these criteria there will be
barely any in the next months]
If considering whether to apply restrictions, they should respect the differences in
the epidemiological situation between orange and red areas and act in a proportionate
manner. They should also take into account the epidemiological situation in their own
territory.
Member states should in principle not refuse entry to persons travelling from other
member states. Those member states that consider it necessary to introduce restrictions
could require persons travelling from non-green areas to:
undergo quarantine
undergo a test after arrival
Member states may offer the option of replacing this test with a test carried out
before arrival.
Member states could also require persons entering their territory to submit passenger
locator forms. A common European passenger locator form should be developed for possible
common use.
"Test, test, test" remember? The above simply becomes arbitrary according to the
criteria defined. This is not policy based on solid science! Such arbitrary policies
usually serve unstated purposes (I'll refrain here to expand on those) while throwing some
false pretext to the masses in order to seek their consent, exploiting their limited
ability to validate the pretext as legitimate science.
------------------------------------------------------------------------------------
So then... what could be a valid metric that allows us to prevent "eventual severe
developments of the disease and a possible breakdown of health systems"? This is the
question we should be asking! Myself, I would be satisfied, in substitution of rtPCR
testing, with the use of new Hospitalizations, ICU and even Deaths as much better metrics,
since these are true fractions of the disease development against any population and even
allow to calibrate for its health system performance, much less vulnerable to duplications
and false positive accounting.
rtPCR testing is absolutely absurd for the purposes it is being used (ie. country wide
government response policy), instead of being limited to clinical diagnostic tool of the
individual suspect of some respiratory disease to be used by a qualified practitioner, and,
at best, a screening tool to get a handle on local outbreaks (schools, workplaces,
residences, etc).
Hanging on this fallacy lies the destruction of most western economies and an ominous
verge into the police state, neither are overstatements given what we have seen so far.
Nathan Mulcahy , Nov 1 2020 23:51 utc |
57
@ Posted by: Jen | Nov 1 2020 22:08 utc | 43
Thanks for the link, Jen. But it's not that a PCR test cannot detect a SARS-cov2
virus. The problem is that there is no standardized and validated PCR test for detecting
SARS-Cov2 virus. I believe in Germany alone there are 200+ variations of the test currently
being used.
My concerns about the remaining four points remain.
Nathan Mulcahy , Nov 2 2020 0:02 utc |
60
@ Posted by: Vasco da Gama | Nov 1 2020 23:49 utc | 56
Thanks for adding additional meat to my argument, including the issue with "viral load",
which together with the state of the immune system of the host will decide whether or not
an infected person will get sick. PCR can be extremely sensitive but that's only part of
the picture.
And as I have mentioned in my response to Jen I am yet to find good answers to my
remaining the 4 points in my first post (#16)
If this is humor, this is very dark humor. The saddest thing of all in this is that very
little of Glenn's excellent article is new. One of Donald Trump's presidency greatest
accomplishment has been to show me how the main stream media 'plays' its dirty games... The
entire mainstream media collectively abandoned its integrity during the last decade.
It's beyond what Orwell could have ever possibly imagined. Targeted gaslighting on an
individual basis using social media to brainwash people into believing whatever they want you
to believe?
Oct 29
I just paid for an annual subscription out of a total frustration with the current
outrageous, unfair, evil and dishonest media situation in the US (and elsewhere also).
Totalitarism is approaching and I have decided to participate in the fight against the
threatening darkness. Good luck.
Loooks like they reliable detemine only that fact that you do not have infection.
But a positive test can well be a false positive, due to excessive multiplication.
Though the whole world relies on RT-PCR to "diagnose" Sars-Cov-2 infection, the science is
clear: they are not fit for purpose By Torsten Engelbrecht and
Konstantin
Demeter Global Research, October 18, 2020
OffGuardian 27 June 2020 Theme: Intelligence , Science and Medicine
https://www.facebook.com/plugins/like.php?action=&app_id=&channel=https%3A%2F%2Fstaticxx.facebook.com%2Fx%2Fconnect%2Fxd_arbiter%2F%3Fversion%3D46%23cb%3Dfab1b412cde68%26domain%3Dwww.globalresearch.ca%26origin%3Dhttps%253A%252F%252Fwww.globalresearch.ca%252Ff2afe1228cac1a%26relation%3Dparent.parent&container_width=0&href=https%3A%2F%2Fwww.globalresearch.ca%2Fcovid19-pcr-tests-scientifically-meaningless%2F5717253&layout=button_count&locale=en_US&sdk=joey&send=false&show_faces=false
https://apis.google.com/u/0/se/0/_/+1/fastbutton?usegapi=1&size=medium&count=true&origin=https%3A%2F%2Fwww.globalresearch.ca&url=https%3A%2F%2Fwww.globalresearch.ca%2Fcovid19-pcr-tests-scientifically-meaningless%2F5717253&gsrc=3p&jsh=m%3B%2F_%2Fscs%2Fapps-static%2F_%2Fjs%2Fk%3Doz.gapi.en.76xGL2Yny_o.O%2Fam%3DwQE%2Fd%3D1%2Fct%3Dzgms%2Frs%3DAGLTcCPLubAJPE__-DfP0tDIR1-cduAt3Q%2Fm%3D__features__#_methods=onPlusOne%2C_ready%2C_close%2C_open%2C_resizeMe%2C_renderstart%2Concircled%2Cdrefresh%2Cerefresh&id=I0_1603254137966&_gfid=I0_1603254137966&parent=https%3A%2F%2Fwww.globalresearch.ca&pfname=&rpctoken=15880150
3499
First published on June 29, 2020
Lockdowns and hygienic measures around the world are based on numbers of cases and
mortality rates created by the so-called SARS-CoV-2 RT-PCR tests used to identify "positive"
patients, whereby "positive" is usually equated with "infected."
But looking closely at the facts, the conclusion is that these PCR tests are meaningless
as a diagnostic tool to determine an alleged infection by a supposedly new virus called
SARS-CoV-2.
Unfounded "Test, Test, Test, " mantra
At the
media briefing on COVID-19 on March 16, 2020 , the WHO Director General Dr Tedros Adhanom
Ghebreyesus said:
We have a simple message for all countries: test, test, test."
The message was spread through headlines around the world, for instance by
Reuters and the BBC
.
Still on the 3 of May, the moderator of the Heute j ournal -- one of the most
important news magazines on German television -- was passing the mantra of the corona dogma
on to his audience with the admonishing words:
Test, test, test -- that is the credo at the moment, and it is the only way to really
understand how much the coronavirus is spreading."
This indicates that the belief in the validity of the PCR tests is so strong that it
equals a religion that tolerates virtually no contradiction.
But it is well known that religions are about faith and not about scientific facts. And as
Walter Lippmann, the two-time Pulitzer Prize winner and perhaps
the most influential journalist of the 20th century said:
"Where all think alike, no one thinks very much."
So to start, it is very remarkable that Kary Mullis himself, the inventor of the
Polymerase Chain Reaction (PCR) technology, did not think alike. His invention got him the
Nobel prize in chemistry in 1993.
Unfortunately, Mullis passed away last year at the age of 74, but there is no doubt that
the biochemist regarded the PCR as
inappropriate to detect a viral infection .
The reason is that the intended use of the PCR was, and still is, to apply it as a
manufacturing technique, being able to replicate DNA sequences millions and billions of
times, and not as a diagnostic tool to detect viruses.
How declaring virus pandemics based on PCR tests can end in disaster was described by
Gina Kolata in her 2007 New York Times article Faith in Quick Test Leads to
Epidemic That Wasn't .
Lack of a valid gold standard
Moreover, it is worth mentioning that the PCR tests used to identify so-called COVID-19
patients presumably infected by what is called SARS-CoV-2 do not have a valid gold standard
to compare them with.
This is a fundamental point. Tests need to be evaluated to determine their preciseness
-- strictly speaking their "sensitivity"[1] and "specificity" -- by comparison with a "gold
standard," meaning the most accurate method available.
As an example, for a pregnancy test the gold standard would be the pregnancy itself. But
as Australian infectious diseases specialist Sanjaya Senanayake, for example, stated in an
ABC TV interview in an answer to
the question "How accurate is the [COVID-19] testing?" :
If we had a new test for picking up [the bacterium] golden staph in blood, we've already
got blood cultures, that's our gold standard we've been using for decades, and we could
match this new test against that. But for COVID-19 we don't have a gold standard test."
Jessica C. Watson from Bristol University confirms this. In her paper "Interpreting a COVID-19 test
result" The British Medical Journal , she writes that
there is a "lack of such a clear-cut 'gold-standard' for COVID-19 testing."
But instead of classifying the tests as unsuitable for SARS-CoV-2 detection and COVID-19
diagnosis, or instead of pointing out that only a virus, proven through isolation and
purification, can be a solid gold standard, Watson claims in all seriousness that,
"pragmatically" COVID-19 diagnosis itself, remarkably including PCR testing itself, "may
be the best available 'gold standard'." But this is not scientifically sound.
Apart from the fact that it is downright absurd to take the PCR test itself as part of the
gold standard to evaluate the PCR test, there are no distinctive specific symptoms for
COVID-19, as even people such as Thomas Löscher, former head of the Department of
Infection and Tropical Medicine at the University of Munich and member of the Federal
Association of German Internists, conceded to us[2].
And if there are no distinctive specific symptoms for COVID-19, COVID-19 diagnosis --
contrary to Watson's statement -- cannot be suitable for serving as a valid gold
standard.
In addition, "experts" such as Watson overlook the fact that only virus isolation, i.e. an
unequivocal virus proof, can be the gold standard.
That is why I asked Watson how COVID-19 diagnosis "may be the best available gold
standard," if there are no distinctive specific symptoms for COVID-19, and also whether the
virus itself, that is virus isolation, wouldn't be the best available/possible gold standard.
But she hasn't answered these questions yet – despite multiple requests. And she has
not yet responded to our rapid response post on her article in which we address exactly the
same points, either, though she wrote us on June 2nd : "I will
try to post a reply later this week when I have a chance."
No proof for the RNA being of viral origin
Now the question is: What is required first for virus isolation/proof? We need to know
where the RNA for which the PCR tests are calibrated comes from.
As textbooks (e.g., White/Fenner. Medical Virology, 1986, p. 9) as well as leading virus
researchers such as Luc
Montagnier or Dominic Dwyer state , particle purification -- i.e. the separation of an
object from everything else that is not that object, as for instance Nobel laureate Marie
Curie purified 100 mg of radium chloride in 1898 by extracting it from tons of pitchblende --
is an essential pre-requisite for proving the existence of a virus, and thus to prove that
the RNA from the particle in question comes from a new virus.
The reason for this is that PCR is extremely sensitive, which means it can detect even
the smallest pieces of DNA or RNA -- but it cannot determine where these particles came from
. That has to be determined beforehand.
And because the PCR tests are calibrated for gene sequences (in this case RNA sequences
because SARS-CoV-2 is believed to be a RNA virus), we have to know that these gene snippets
are part of the looked-for virus. And to know that, correct isolation and purification of the
presumed virus has to be executed.
Hence, we have asked the science teams of the relevant papers which are referred to in the
context of SARS-CoV-2 for proof whether the electron-microscopic shots depicted in their in
vitro experiments show purified viruses.
But not a single team could answer that question with "yes" -- and NB., nobody said
purification was not a necessary step. We only got answers like "No, we did not obtain an
electron micrograph showing the degree of purification" (see below).
We asked several study authors "Do your electron micrographs show the purified virus?",
they gave the following responses:
Study 1: Leo L. M. Poon; Malik Peiris. "Emergence of a novel human coronavirus
threatening human health" Nature Medicine , March 2020"The image is the virus budding from an infected cell. It is not purified
virus."
Study 2: Myung-Guk Han et al. "Identification of Coronavirus Isolated from a Patient in
Korea with COVID-19", Osong Public Health and Research Perspectives , February
2020"We could not estimate the degree of purification because we do not purify and
concentrate the virus cultured in cells."
Study 3: Wan Beom Park et al. "Virus Isolation from the First Patient with SARS-CoV-2 in
Korea", Journal of Korean Medical Science , February 24, 2020"We did not obtain an electron micrograph showing the degree of
purification."
Study 4: Na Zhu et al., "A Novel Coronavirus from Patients with Pneumonia in China",
2019, New England Journal of Medicine , February 20, 2020"[We show] an image of sedimented virus particles, not purified ones."
Regarding the mentioned papers it is clear that what is shown in the electron micrographs
(EMs) is the end result of the experiment, meaning there is no other result that they could
have made EMs from.
That is to say, if the authors of these studies concede that their published EMs do not
show purified particles, then they definitely do not possess purified particles claimed to be
viral. (In this context, it has to be remarked that some researchers use the term "isolation"
in their papers, but the procedures described therein do not represent a proper isolation
(purification) process. Consequently, in this context the term "isolation" is misused).
Thus, the authors of four of the principal, early 2020 papers claiming discovery of a new
coronavirus concede they had no proof that the origin of the virus genome was viral-like
particles or cellular debris, pure or impure, or particles of any kind. In other words, the
existence of SARS-CoV-2 RNA is based on faith, not fact.
We have also contacted Dr Charles Calisher, who is a seasoned virologist. In 2001,
Science published an "impassioned plea to the younger generation" from several
veteran virologists, among them Calisher, saying that:
[modern virus detection methods like] sleek polymerase chain reaction [ ] tell little
or nothing about how a virus multiplies, which animals carry it, [or] how it makes people
sick. [It is] like trying to say whether somebody has bad breath by looking at his
fingerprint."[3]
And that's why we asked Dr Calisher whether he knows one single paper in which SARS-CoV-2
has been isolated and finally really purified. His answer:
I know of no such a publication. I have kept an eye out for one."[4]
This actually means that one cannot conclude that the RNA gene sequences, which the
scientists took from the tissue samples prepared in the mentioned in vitro trials and for
which the PCR tests are finally being "calibrated," belong to a specific virus -- in this
case SARS-CoV-2.
In addition, there is no scientific proof that those RNA sequences are the causative agent
of what is called COVID-19.
In order to establish a causal connection, one way or the other, i.e. beyond virus
isolation and purification, it would have been absolutely necessary to carry out an
experiment that satisfies the four Koch's postulates. But there is no such experiment, as
Amory Devereux and Rosemary Frei
recently revealed for OffGuardian .
The
Tests: The Achilles Heel of the COVID-19 House of Cards
The necessity to fulfill these postulates regarding SARS-CoV-2 is demonstrated not least
by the fact that attempts have been made to fulfill them. But even researchers claiming they
have done it, in reality, did not succeed.
One example is a study published in Nature
on May 7 . This trial, besides other procedures which render the study invalid, did not
meet any of the postulates.
For instance, the alleged "infected" laboratory mice did not show any relevant clinical
symptoms clearly attributable to pneumonia, which according to the third postulate should
actually occur if a dangerous and potentially deadly virus was really at work there. And the
slight bristles and weight loss, which were observed temporarily in the animals are
negligible, not only because they could have been caused by the procedure itself, but also
because the weight went back to normal again.
Also, no animal died except those they killed to perform the autopsies . And let's not
forget: These experiments should have been done before developing a test, which is not
the case.
Revealingly, none of the leading German representatives of the official theory about
SARS-Cov-2/COVID-19 -- the Robert Koch-Institute (RKI), Alexander S. Kekulé
(University of Halle), Hartmut Hengel and Ralf Bartenschlager (German Society for Virology),
the aforementioned Thomas Löscher, Ulrich Dirnagl (Charité Berlin) or Georg
Bornkamm (virologist and professor emeritus at the Helmholtz-Zentrum Munich) -- could answer
the following question I have sent them:
If the particles that are claimed to be to be SARS-CoV-2 have not been purified, how
do you want to be sure that the RNA gene sequences of these particles belong to a specific
new virus?
Particularly, if there are studies showing that substances such as antibiotics that
are added to the test tubes in the in vitro experiments carried out for virus detection can
"stress" the cell culture in a way that new gene sequences are being formed that were
not
previously detectable -- an aspect that Nobel laureate Barbara McClintock already drew
attention to in her Nobel Lecture back in
1983 .
It should not go unmentioned that we finally got the Charité – the employer
of Christian Drosten, Germany's most influential virologist in respect of COVID-19, advisor
to the German government and co-developer of the PCR test which was the first to be
"accepted" (
not validated! ) by the WHO worldwide – to answer questions on the topic.
But we didn't get answers until June 18, 2020, after months of non-response. In the end,
we achieved it only with the help of Berlin lawyer Viviane Fischer.
Regarding our question "Has the Charité convinced itself that appropriate
particle purification was carried out?," the Charité concedes that they didn't use
purified particles.
And although they claim "virologists at the Charité are sure that they are
testing for the virus," in their paper ( Corman et
al. ) they state:
RNA was extracted from clinical samples with the MagNA Pure 96 system (Roche, Penzberg,
Germany) and from cell culture supernatants with the viral RNA mini kit (QIAGEN, Hilden,
Germany),"
Which means they just assumed the RNA was viral .
Incidentally, the Corman et al. paper, published on January 23, 2020 didn't even go
through a proper peer review process , nor were the procedures outlined therein accompanied
by controls -- although it is only through these two things that scientific work becomes
really solid.
Irrational rest results
It is also certain that we cannot know the false positive rate of the PCR tests without
widespread testing of people who certainly do not have the virus, proven by a method which is
independent of the test (having a solid gold standard).
Therefore, it is hardly surprising that there are several papers illustrating irrational
test results.
For example, already in February the health authority in China's Guangdong province
reported that people have fully recovered from illness blamed on COVID-19, started to test
"negative," and then
tested "positive" again .
A month later, a paper published in the Journal of Medical Virology showed that 29 out
of 610 patients at a hospital in Wuhan had 3 to 6 test results that flipped between
"negative", "positive" and
"dubious" .
A third example is a study from Singapore in which tests were carried out almost daily
on 18 patients and the majority went from "positive" to "negative" back to "positive" at
least once, and up to five times in one
patient .
Even Wang Chen, president of the Chinese Academy of Medical Sciences, conceded in February
that the PCR tests are
"only 30 to 50 per cent accurate"
etter to the WHO's coronavirus response team and to Anthony S. Fauci on March 22, 2020,
saying that:
It has been widely reported in the social media that the RT-qPCR [Reverse
Transcriptase quantitative PCR] test kits used to detect SARSCoV-2 RNA in human specimens
are generating many false positive results and are not sensitive enough to detect some real
positive cases."
In other words, even if we theoretically assume that these PCR tests can really detect a
viral infection, the tests would be practically worthless, and would only cause an unfounded
scare among the "positive" people tested.
This becomes also evident considering the positive predictive value (PPV).
The PPV indicates the probability that a person with a positive test result is truly
"positive" (ie. has the supposed virus), and it depends on two factors: the prevalence of the
virus in the general population and the specificity of the test, that is the percentage of
people without disease in whom the test is correctly "negative" (a test with a specificity of
95% incorrectly gives a positive result in 5 out of 100 non-infected people).
With the same specificity, the higher the prevalence, the higher the PPV.
In this context, on June 12 2020, the journal Deutsches Ärzteblatt published
an article in which the PPV has been calculated with
three different prevalence scenarios .
The results must, of course, be viewed very critically, first because it is not possible
to calculate the specificity without a solid gold standard, as outlined, and second because
the calculations in the article are based on the specificity determined in the study by
Jessica Watson, which is potentially worthless, as also mentioned.
But if you abstract from it, assuming that the underlying specificity of 95% is correct
and that we know the prevalence, even the mainstream medical journal Deutsches
Ärzteblatt reports that the so-called SARS-CoV-2 RT-PCR tests may have "a shockingly
low" PPV.
In one of the three scenarios, figuring with an assumed prevalence of 3%, the PPV was
only 30 percent, which means that 70 percent of the people tested "positive" are not
"positive" at all . Yet "they are prescribed quarantine," as even the Ärzteblatt notes
critically.
In a second scenario of the journal's article, a prevalence of rate of 20 percent is
assumed. In this case they generate a PPV of 78 percent, meaning that 22 percent of the
"positive" tests are false "positives."
That would mean: If we take the around 9 million people who are currently considered
"positive" worldwide -- supposing that the true "positives" really have a viral infection --
we would get almost 2 million false "positives."
All this fits with the fact that the CDC and the FDA, for instance, concede in their files
that the so-called "SARS-CoV-2 RT-PCR tests" are not suitable for SARS-CoV-2 diagnosis.
In the "CDC 2019-Novel
Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel" file from March 30, 2020, for
example, it says:
Detection of viral RNA may not indicate the presence of infectious virus or that
2019-nCoV is the causative agent for clinical symptoms"
And:
This test cannot rule out diseases caused by other bacterial or viral pathogens."
And the FDA admits
that :
positive results [ ] do not rule out bacterial infection or co-infection with other
viruses. The agent detected may not be the definite cause of disease."
Remarkably, in the instruction manuals of PCR tests we can also read that they are not
intended as a diagnostic test, as for instance in those by
Altona Diagnostics and Creative Diagnostics[
5 ].
To quote another one, in the product announcement of the LightMix Modular Assays produced
by TIB Molbiol -- which were developed using the Corman et al. protocol -- and
distributed by Roche we can read:
These assays are not intended for use as an aid in the diagnosis of coronavirus
infection"
And:
For research use only. Not for use in diagnostic procedures."
Where is the evidence that the tests can measure the "viral load"?
There is also reason to conclude that the PCR test from Roche and others cannot even
detect the targeted
genes .
Moreover, in the product descriptions of the RT-qPCR tests for
SARS-COV-2 it says they are
"qualitative" tests , contrary to the fact that the "q" in "qPCR" stands for
"quantitative." And if these tests are not "quantitative" tests, they don't show how many
viral particles are in the body .
That is crucial because, in order to even begin talking about actual illness in the real
world not only in a laboratory, the patient would need to have millions and millions of viral
particles actively replicating in their body.
That is to say, the CDC, the WHO, the FDA or the RKI may assert that the tests can measure
the so-called
"viral load," i.e. how many viral particles are in the body. "But this has never been
proven. That is an enormous scandal," as the journalist
Jon Rappoport points out .
This is not only because the term "viral load" is deception. If you put the question "what
is viral load?" at a dinner party, people take it to mean viruses circulating in the
bloodstream. They're surprised to learn it's actually RNA molecules.
Also, to prove beyond any doubt that the PCR can measure how much a person is "burdened"
with a disease-causing virus, the following experiment would have had to be carried out
(which has not yet happened):
You take, let's say, a few hundred or even thousand people and remove tissue samples
from them. Make sure the people who take the samples do not perform the test.The testers will
never know who the patients are and what condition they're in. The testers run their PCR on
the tissue samples. In each case, they say which virus they found and how much of it they
found. Then, for example, in patients 29, 86, 199, 272, and 293 they found a great deal of
what they claim is a virus. Now we un-blind those patients. They should all be sick, because
they have so much virus replicating in their bodies. But are they really sick -- or are they
fit as a fiddle?
With the help of the aforementioned lawyer Viviane Fischer, I finally got the
Charité to also answer the question of whether the test developed by Corman et al. --
the so-called "Drosten PCR
test" -- is a quantitative test.
But the Charité was not willing to answer this question "yes". Instead, the
Charité wrote:
If real-time RT-PCR is involved, to the knowledge of the Charité in most cases
these are [ ] limited to qualitative detection."
Furthermore, the "Drosten PCR test" uses the unspecific E-gene assay as preliminary
assay , while the Institut Pasteur uses the same assay as
confirmatory assay .
According to Corman et al., the E-gene assay is likely to detect all Asian viruses , while
the other assays in both tests are supposed to be more specific for sequences labelled
"SARS-CoV-2".
Besides the questionable purpose of having either a preliminary or a confirmatory test
that is likely to detect all Asian viruses, at the beginning of April the WHO changed the
algorithm, recommending that from then on a test can be regarded as "positive" even if just
the E-gene assay (which is likely to detect all Asian viruses! )
gives a "positive" result .
This means that a confirmed unspecific test result is officially sold as
specific .
That change of algorithm increased the "case" numbers. Tests using the E-gene assay are
produced for example by Roche
,
TIB Molbiol and
R-Biopharm .
High CQ values make the test results even more meaningless
Another essential problem is that many PCR tests have a "cycle quantification" (Cq) value
of over 35, and some, including the "Drosten PCR test", even have a Cq of 45.
The Cq value specifies how many cycles of DNA replication are required to detect a real
signal from biological samples.
"Cq values higher than 40 are suspect because of the implied low efficiency and
generally should not be reported," as it says in the MIQE guidelines
.
MIQE stands for "Minimum Information for Publication of Quantitative Real-Time PCR
Experiments", a set of guidelines that describe the minimum information necessary for
evaluating publications on Real-Time PCR, also called quantitative PCR, or qPCR.
The inventor himself, Kary Mullis, agreed,
when he stated :
If you have to go more than 40 cycles to amplify a single-copy gene, there is something
seriously wrong with your PCR."
The MIQE guidelines have been developed under the aegis of Stephen A. Bustin , Professor of Molecular
Medicine, a world-renowned expert on quantitative PCR and author of the book A-Z of
Quantitative PCR which has been called "the bible of qPCR."
In a recent podcast interview Bustin points out that "the use of such arbitrary Cq
cut-offs is not ideal, because they may be either too low (eliminating valid results) or too
high (increasing false "positive" results)."
https://www.podbean.com/media/player/znrvk-d932a7?from=usersite&vjs=1&skin=1&fonts=Helvetica&auto=0&download=1
And, according to him, a Cq of 20 to 30 should be aimed at, and there is concern regarding
the reliability of the results for any Cq over 35.
If the Cq value gets too high, it becomes difficult to distinguish real signal from
background, for example due to reactions of primers and fluorescent probes, and hence there
is a higher probability of false positives.
Moreover, among other factors that can alter the result, before starting with the actual
PCR, in case you are looking for presumed RNA viruses such as SARS-CoV-2, the RNA must be
converted to complementary DNA (cDNA) with the enzyme Reverse Transcriptase -- hence the "RT"
at the beginning of "PCR" or "qPCR."
But this transformation process is "widely recognized as inefficient and variable,"
as Jessica Schwaber from the Centre for Commercialization of Regenerative Medicine in Toronto
and two research colleagues pointed out in a 2019
paper .
Stephen A. Bustin acknowledges problems with PCR in a comparable way.
For example, he pointed to the problem that in the course of the conversion process (RNA
to cDNA) the amount of DNA obtained with the same RNA base material can vary widely, even by
a factor of 10 (see above interview).
Considering that the DNA sequences get doubled at every cycle, even a slight variation
becomes magnified and can thus alter the result, annihilating the test's reliable informative
value.
So how can it be that those who claim the PCR tests are highly meaningful for so-called
COVID-19 diagnosis blind out the fundamental inadequacies of these tests -- even if they are
confronted with questions regarding their validity?
Certainly, the apologists of the novel coronavirus hypothesis should have dealt with these
questions before throwing the tests on the market and putting basically the whole world under
lockdown, not least because these are questions that come to mind immediately for anyone with
even a spark of scientific understanding.
Thus, the thought inevitably emerges that financial and political interests play a
decisive role for this ignorance about scientific obligations. NB, the WHO, for example has
financial ties with drug companies, as the British Medical Journal
showed in 2010 .
And
experts criticize "that the notorious corruption and conflicts of interest at WHO have
continued, even grown" since then. The CDC as well, to take another big player, is
obviously no better
off .
Finally, the reasons and possible motives remain speculative, and many involved surely act
in good faith; but the science is clear: The numbers generated by these RT-PCR tests do not
in the least justify frightening people who have been tested "positive" and imposing lockdown
measures that plunge countless people into poverty and despair or even drive them to
suicide.
And a "positive" result may have serious consequences for the patients as well, because
then all non-viral factors are excluded from the diagnosis and the patients are treated with
highly toxic drugs and invasive intubations. Especially for elderly people and patients with
pre-existing conditions such a treatment can be fatal, as we have outlined in the article
"Fatal
Therapie."
Without doubt eventual excess mortality rates are caused by the therapy and by the
lockdown measures, while the "COVID-19" death statistics comprise also patients who died of a
variety of diseases, redefined as COVID-19 only because of a "positive" test result whose
value could not be more doubtful.
Addendum: We thank Eleni Papadopulos-Eleopulos and Val Turner in particular who made
valuable contributions to the realization of this article.
*
Note to readers: please click the share buttons above or below. Forward this article to
your email lists. Crosspost on your blog site, internet forums. etc.
Torsten Engelbrecht is an award-winning journalist and author from Hamburg, Germany. In
2006 he co-authored Virus-Mania with Dr Klaus Kohnlein, and in 2009 he won the German Alternate
Media Award . He has also written for Rubikon, Süddeutsche Zeitung, Financial Times
Deutschland and many others.
Konstantin Demeter is a freelance photographer and an independent researcher. Together
with the journalist Torsten Engelbrecht he has published articles on the "COVID-19" crisis in
the online magazine Rubikon, as well as contributions on the monetary system, geopolitics,
and the media in Swiss Italian newspapers.
Notable quotes:
"... COVID-19 spreads mainly among people who are in close contact (within about 6 feet) for a prolonged period. ..."
"... "Current data do not support long range aerosol transmission of SARS-CoV-2, such as seen with measles or tuberculosis. Short-range inhalation of aerosols is a possibility for COVID-19, as with many respiratory pathogens. However, this cannot easily be distinguished from 'droplet' transmission based on epidemiologic patterns. Short-range transmission is a possibility particularly in crowded medical wards and inadequately ventilated spaces ." ..."
"... Kimberly A. Prather, PhD, Distinguished Chair in Atmospheric Chemistry, Scripps Institution of Oceanography, UC San Diego. ..."
"... Linsey C Marr, PhD, Charles P. Lunsford Professor of Civil and Environmental Engineering, Virginia Tech. ..."
"... Donald K Milton, MD, DrPH, Professor of Environment Health at The University of Maryland School of Public Health. ..."
Right now, the CDC website does not acknowledge that aerosols typically spread SARS-CoV-2
beyond 6 feet, instead
saying :
" COVID-19 spreads mainly among people who are in close contact (within about 6 feet)
for a prolonged period. Spread happens when an infected person coughs, sneezes or talks,
and droplets from their mouth or nose are launched into the air and land in the mouths or
noses of people nearby. The droplets can also be inhaled into the lungs."
The site says that respiratory droplets can land on various surfaces, and people can become
infected from
touching those surfaces and then touching their eyes, nose or mouth. It goes on to say,
"Current data do not support long range aerosol transmission of SARS-CoV-2, such as
seen with measles or tuberculosis. Short-range inhalation of aerosols is a possibility for
COVID-19, as with many respiratory pathogens. However, this cannot easily be distinguished
from 'droplet' transmission based on epidemiologic patterns. Short-range transmission is a
possibility particularly in crowded medical wards and inadequately ventilated
spaces ."
Confusion has surrounded the use of words like "aerosols" and "droplets" because they have
not been consistently defined. And the word "airborne" takes on special meaning for infectious
disease experts and public health officials because of the question of whether infection can be
readily spread by "airborne transmission." If SARS-CoV-2 is readily spread by airborne
transmission, then more stringent infection control measures would need to be adopted, as is
done with airborne diseases such as measles and tuberculosis. But the CDC has told CBS News
chief medical correspondent Dr. Jonathan LaPook that even if airborne spread is playing a role
with SARS-CoV-2, the role does not appear to be nearly as important as with airborne infections
like measles and tuberculosis.
All this may sound like wonky scientific discussion that is deep in the weeds -- and it is
-- but it has big implications as people try to figure out how to stay safe during the
pandemic. Some pieces of advice are intuitively obvious: wear a mask, wash your hands, avoid
crowds, keep your distance from others, outdoors is safer than indoors. But what about that "6
foot" rule for maintaining social distance? If the virus can travel indoors for distances
greater than 6 feet, isn't it logical to wear a mask
indoors whenever you are with people who are not part of your "pod" or "bubble?"
Understanding the basic science behind how SARS-CoV-2 travels through the air should help
give us strategies for staying safe. Unfortunately, there are still many open questions. For
example, even if aerosols produced by an infected person can float across a room, and even if
the aerosols contain some viable virus, how do we know how significant a role that possible
mode of transmission is playing in the pandemic?
Aerosols can be thought of as cigarette smoke. While they are most concentrated close to
someone who has the infection, they can travel farther than 6 feet, linger, build up in the air
and remain infectious for hours. As a consequence, to lessen the chance of inhaling this virus,
it is vital to take all of the following steps:
Indoors:
Practice physical distancing -- the farther the better.
Wear a face mask when you are with others, even when you can maintain physical
distancing. Face masks not only lessen the amount of virus coming from people who have the
infection, but also lessen the chance of you inhaling the virus.
Improve ventilation by opening windows. Learn how to clean the air effectively with
methods such as filtration.
Outdoors:
Wear a face mask if you cannot physically distance by at least 6 feet or, ideally,
more.
Whenever possible, move group activities outside.
Whether you are indoors or outdoors, remember that your risk increases with the duration of
your exposure to others.
With the question of transmission, it's not just the public that has been confused. There's
also been confusion among scientists, medical professionals and public health officials, in
part because they have often used the words "droplets" and "aerosols" differently. To address
the confusion, participants in an August workshop on airborne transmission of SARS-CoV-2 at the
National Academies of Sciences, Engineering, and Medicine suggested these definitions for
respiratory droplets and aerosols::
Droplets are larger than 100 microns and fall to the ground within 6 feet,
traveling like tiny cannonballs.
Aerosols are smaller than 100 microns, are highly concentrated close to a
person, can travel farther than 6 feet and can linger and build up in the air, especially
in rooms with poor ventilation.
All respiratory activities, including breathing, talking and singing, produce far more
aerosols than droplets. A person is far more likely to inhale aerosols than to be sprayed by a
droplet, even at short range. The exact percentage of transmission by droplets versus aerosols
is still to be determined. But we know from epidemiologic and other data, especially superspreading
events , that infection does occur through inhalation of aerosols.
In short, how are we getting infected by SARS-CoV-2? The answer is: In the air. Once we
acknowledge this, we can use tools we already have to help end this pandemic.
Kimberly A. Prather, PhD, Distinguished Chair in Atmospheric Chemistry, Scripps
Institution of Oceanography, UC San Diego.
Linsey C Marr, PhD, Charles P. Lunsford Professor of Civil and Environmental
Engineering, Virginia Tech.
Donald K Milton, MD, DrPH, Professor of Environment Health at The University of Maryland
School of Public Health.
bevin , Oct 4 2020 15:16 utc |
13
Discussion of Trump's illness tends to obscure the reality that he, unlike most
Americans and others who suffer from the virus, is getting proper treatment and all the
necessary care to deal with the virus.
Most of those who have died did not get anything like that treatment, indeed they were
left to die by Healthcare systems which are almost all infected by obsessions with profit
and efficiency which have led to the dismantling- often in 'socialised' systems such as
those in the UK and Canada- of nursing staffs and ICU capacity.
In Ontario, disabled people are charging the hospital system with having adopted a
triage protocol which, essentially, puts patients with disabilities at the bottom of the
list when treatment is being rationed. This is a practice which long pre-dates the current
pandemic, as do many of the administrative malpractices which have contributed to death
tolls in the "west" far exceeding those in the Far East where life is more valued.
In the UK the SKAWKBOX blog has released an Amnesty report which it describes as having
destroyed government claims
It suggests that
"*the huge number of deaths caused by COVID-19 in care homes – well over 18,000 at
the very least, but in reality almost 30,000 based on 'excess' deaths attributable to
likely undiagnosed cases
"That's geriatricide – the murder of our old and vulnerable."
https://skwawkbox.org/2020/10/04/expendable-amnesty-report-explodes-tories-protective-ring-care-home-lie-and-confirms-thousands-of-elderly-knowingly-sentenced-to-death/#comments
'False' positive Covid-19 tests saw non-contagious people counted as fresh infections
& triggered 2nd wave alarm – Belgian media 5 Oct, 2020 15:36 / Updated 2 hours
ago Get short URL
Over a half of
coronavirus infections revealed this summer by one of Belgium's biggest labs were old and no
longer contagious, but were still reported as new cases, local media discovered.
Belgian daily newspaper Het Laatste Nieuws examined the tests carried out by AZ Delta, one
of the largest labs in the country, and made a stunning discovery. Almost half of all positive
cases reported throughout June, July and August were actually people with an old infection.
The problem, it turns out, lies in the PCR Covid-19 tests. The paper reports that scientific
data reveals virus particles can be detected up to 83 days after the actual infection. This led
to instances where people were no longer contagious, but were still registered as positive
cases. According to HLN, all of these people had to be quarantined.
Belgian experts sounded the alarm in mid-July, when coronavirus numbers spiked after a
relief in June, and even insisted that the second wave had already begun for the country.
"We may have had to deal with old infections largely in the summer months," the lab's
clinical biologist Frederik Van Hoecke told the paper.
ALSO ON RT.COM
Paris to shutter bars for 2 weeks as French capital placed on Covid-19 high alert
The revelation comes as countries look to reintroduce restrictions to curb the spread of the
virus.
If you like this story, share it with a friend!
LONDON – Research to develop a safe, effective, and widely available COVID-19 vaccine
is advancing rapidly. But when it will happen is not clear. Much depends on how we govern the
production and distribution of new drugs. While the World Health Organization's COVID-19
Technology Access Pool promises to foster accessibility, the actual availability of vaccines
and treatments also will hinge on local manufacturing capacity, which in many countries has
been eroded by deindustrialization.
Moreover, while universal testing remains a feasible, cost-effective, and immediately
available method of managing the pandemic until a vaccine arrives, this approach also requires
manufacturing capacity and sound governance in the public interest. Yet even in advanced
economies, over-reliance on the private sector may prevent governments from maximizing test
production and deployment. For example, the British government has proposed a "moon shot"
testing program, yet its actual strategy needs clarification.
Such a mission-oriented approach requires a holistic, systems-level perspective,
particularly when it comes to "wicked problems" like public-health crises and climate change,
which involve a wide range of complex socioeconomic and technological issues. Implementing
universal testing will require contributions from a sprawling network of actors and
institutions. To be truly effective, any such program must be designed to generate systemic
resilience and public value.
As has been demonstrated by the Nobel laureate economist Paul Romer, the epidemiologist
Michael Mina, a recent IMF working paper, and many others, a properly designed universal
testing program could bring the pandemic to an end within just a few months. The missing
ingredients are industrial policies and other government measures to coordinate and steer
production, in order to eliminate the bottlenecks that the private sector faces.
The necessary testing technology of rapid immunodiagnostic tests -- such as saliva-based
antigen tests that are similar to home pregnancy tests and cost less than $5 -- already exists.
Although these tests are sub-optimal in sensitivity compared with the standard polymerase chain
reaction (PCR) tests, they are specific enough to detect infections at scale in settings where
disease prevalence is high; and, crucially, they do not require centralized laboratory
facilities.
Therefore, with a purposeful program design that carefully considers the functionality and
limitations of the technology deployed, rapid tests can enable decentralized universal testing
programs at the community level. For example, tests could be made available free of charge at
local pharmacies, with the expectation that everyone test themselves on a regular basis and
self-isolate if positive. The same kits could be used as "infection-free" passports for
admission to public spaces such as schools and workplaces. In this case, a new market would
likely emerge as airlines, malls, restaurants, and cafes start purchasing cheap, rapid tests so
that they can get back to business.
Rapid testing can help to expand and complement the universal testing strategy already being
rolled out locally (such as the free mandatory testing at MIT and Georgetown University in the
United States, weekly testing of employees at German workplaces, and the population-wide
testing campaign in Wuhan), which currently rely on PCR tests.
Similar strategies need to be launched at the national level, especially in low- and
middle-income countries where the affordability and scalability of molecular testing is low.
Many countries have the capacity to produce a sufficient supply of tests at a cost that would
pale in comparison to those inflicted by the pandemic. The number of tests needed globally over
a year to supply a weekly testing regimen would be equivalent to less than half the number of
cans of soda consumed annually. Moreover, scaling up production of antigen tests could be done
relatively quickly, and would be a minor effort compared to the U.S. mobilization for World War
II.
While billions of dollars are being funneled toward vaccine development and production,
additional funding also must be directed toward strengthening our testing infrastructure. At $5
per unit, the cost of testing the world's population every week would come to around $2
trillion. That is far less than the pandemic-related loss of global income during this period
(as measured by the difference between pre- and post-pandemic growth forecasts) and fiscal
stimulus so far this year, an estimated total of $20 trillion. And these comparisons don't
account for the costs of lost lives or the potential benefits of achieving new economies of
scale in test production -- a spillover that could enable the eradication of the seasonal
flu.
There are potentially steep challenges beyond production, of course. As practical as
universal testing is, any such effort could still come under pressure if governments believe
they must choose between different production needs for vaccines, anti-viral drugs, personal
protective equipment, and expanded medical facilities.
But universal testing must not be viewed as a separate item on a larger list of priorities.
The point of a mission-oriented approach is to create dynamic public-sector capabilities and
strengthen the entire health system at once. New testing capacity should be integrated with
national and local health systems as part of a broader program design, so that each leg of the
strategy supports the others.
More broadly, COVID-19 has underscored the need for a more resilient and responsive
industrial ecosystem that can increase production of essential items quickly. Even under
current conditions, increasing the production of tests and implementing a universal testing
strategy is feasible, and could end the pandemic by year's end, while also creating the
infrastructure needed to ward off future pandemics.
All countries need to adopt a longer-term vision and shore up their manufacturing
capabilities. By leading on this issue, governments can strengthen local productive capacities
and create a new kind of economic commons. The same mission-oriented approach could then be
applied to science policy and industrial strategy, laying the groundwork for more
cross-sectoral innovations and the type of resilient manufacturing that will be needed to
tackle other highly complex global challenges. The days when we could pin all our hopes on
technological fixes are over.
Reda Cherif is senior economist at the International Monetary Fund. Fuad Hasanov is senior
economist at the International Monetary Fund and an adjunct professor of Economics at
Georgetown University. Mariana Mazzucato is professor in the Economics of Innovation and Public
Value and Founding Director of the UCL Institute for Innovation and Public Purpose.
©Project Syndicate, 2020.
vk
145
It's confirmed: Trump won't be treated with hydroxycloroquine:
Physician to the President: Health
Update on President Donald J. Trump, Oct. 2, 2020
"Following PCR-confirmation of the President's diagnosis, as a precautionary measure he
received a single 8 gram dose of Regeneron's polyclonal antibody cocktail . He
completed the infusion without incident. In addition to the polyclonal antibodies, the
President has been taking zinc, vitamin D, famotidine, melatonin and a daily aspirin."
When the cookie crumbled, no hydroxycloroquine was taken - even in a case of of initial
phase of the disease. It is below even a single aspirin in the COVID-19's treatment food
chain (which is being ministered, among other supplements, just to keep Trump's body strong
while the main drug takes effect, as is normal to old patients).
On the bright side, at least we know the name of the real deal: Regeneron.
Notable quotes:
"... Given what's at stake, Bramstedt proposes an overhaul of the submissions process to make it more efficient, while also introducing mandatory ethics and integrity training for researchers. ..."
"... "Research has the potential to enter the public domain and be used by many stakeholders, including governments and policy makers, so the data must be robust," she concludes. ..."
A leading ethicist is
sounding the alarm over a flood of potentially substandard pandemic research which may endanger
lives through ill-informed public policy, while damaging medical and scientific practice itself
in the process.
There has been a surge of almost 4,000 recently-published papers related to Covid-19, many
of which have been of questionable quality, according to Professor Katrina Bramstedt from Bond
University, Queensland, who is also secretary general at the Luxembourg Agency for Research
Integrity.
Bramstedt recently published her own study examining the poor
quality of Covid-19 research, which forms the basis of her recent criticisms.
Amid the rush to print the latest updates and 'breakthroughs' in Covid-19 research, there
has been a slew of retracted research papers, following an unprecedented number of submissions
to pre-print servers, which carry out fewer quality assurance and due diligence checks than
established medical journals.
"No research team is exempt from the pressures and speed at which COVID-19 research is
occurring. And this can increase the risk of honest error as well as deliberate
misconduct," Bramstedt says.
The rapid spread of the pandemic and the growing public thirst for information forced
researchers into overdrive looking for treatments, vaccines, and cures potentially endangering
patients, medical practitioners, and potentially government policy.
As of July 31, 2020, 19 published articles and 14 preprints about Covid-19 have been
retracted, withdrawn or been seriously called into question with regards to the quality of
their data. Over 57 percent of these papers come from Asia, over half of which came from
China.
There were concerns reported over falsified data, issues with methodology, irregularities in
interpretation of data, and conclusions among a multitude of other issues.
I've
lost all trust in medical research – the financial muscle of Big Pharma has been busy
distorting science during the pandemic
Even the paragons of medical research best practice, the Lancet and New England Journal of
Medicine, were forced to retract two preprints and two research papers due to the presence of
unverified data shared by all four.
"Patient harm that is significant, permanent and irreversible could result from using
faulty research results from preprints as well as published papers," she adds.
Bramstedt highlights the time and resource constraints under which researchers, their
supervisors, as well as publishers and their editors are operating under as a major factor in
the plethora of poor quality research.
Add to the mix the fact that many peer reviewers work on a voluntary basis with competing
demands on their time, especially as they face uncertainty through the pandemic, and issues
with quality control are largely inevitable.
At the same time, convening cross-disciplinary meetings of leading immunologists,
microbiologists, and lung disease specialists on a consistent basis to share, review, and
discuss research during such trying times is increasingly difficult.
Given what's at stake, Bramstedt proposes an overhaul of the submissions process to make it
more efficient, while also introducing mandatory ethics and integrity training for
researchers.
"Research has the potential to enter the public domain and be used by many stakeholders,
including governments and policy makers, so the data must be robust," she concludes.
Think your friends would be interested? Share this story!
Trends: Covid-19 coronavirus
news
Smythe_Mogg 8 hours ago 2 Oct, 2020 08:10 AM
Medical research has for long been diluted in quality by inherently inconsequential studies,
incompetently designed and/or executed studies, and pressure to value quantity over quality.
Mediocrity and worse abounds among researchers. Thus, Bramstedt's findings are all too
plausible.
Tango 8 hours ago 2 Oct, 2020 08:42 AM
Unfortunately this "ethicist" doesn't focus on the quackery that has come from the leading
government experts and researchers including Ferguson, Drosten, Zambon, Fauci, Holmes,
Rambaut, Burioni and all the rest.
Hanonymouse Tango 1 hour ago 2 Oct, 2020 03:21 PM
Yeah epidemiology used to be about tracking a disease, not a form of government... If only
these constant lockdowns and re-openings weren't destroying people's lives then I would find
it funny that politicians think they can chase statistics that lag by 2+ weeks and have it
mean anything. But it IS destroying people's lives. Those businesses and jobs are not coming
back once this mess is over.
diessa 8 hours ago 2 Oct, 2020 07:58 AM
wave of fraud and quackery in medical research re convid, actually sums it up!
Timkun 3 hours ago 2 Oct, 2020 01:09 PM
Research is an expensive endeavour. Management typically doesn't like it, because there is
usually no profit. At the university level, many "experts" are ego driven, find it hard to
admit that their theory may be wrong. IMO from years working in research, I find that because
so much money is on the line, today, research is less of an exact science. The reason; more
money and recognition for being first.
Count_Cash 8 hours ago 2 Oct, 2020 08:21 AM
Demand has a habit of overwhelming any system. Of course Covid-19 has spurred increased
research - it should have. So the system has broken and needs a few changes to make it more
efficient..... However, when there is a huge financial benefit in driving the demand, you may
well find that no matter what you do, a way will be found around it. That is the bigger
issue!
Gerald Comeau Count_Cash 7 hours ago 2 Oct, 2020 09:16 AM
Demand? This has little to do with demand? It seems to me greed and opportunism on the part
of scientists aspiring career advancement is more in line, with what is going on, than
demand.
eyeofmice 7 hours ago 2 Oct, 2020 09:21 AM
check out a real doctors Dr. Andrew Kaufman and Dr. Vernon Coleman who are exposing this hoax
and are being censored.
Logicthought 7 hours ago 2 Oct, 2020 09:39 AM
Medical Research has brought the Medical Profession into disrepute ...
Highly recommended !Notable quotes:
"... Virtually every aspect of the Syrian opposition was cultivated and marketed by Western government-backed public relations firms, from their political narratives to their branding, from what they said to where they said it. ..."
"Western government-funded intelligence cutouts trained Syrian opposition leaders,
planted stories in media outlets from BBC to Al Jazeera, and ran a cadre of journalists. A
trove of leaked documents exposes the propaganda network."
"Leaked documents show how UK government contractors developed an advanced infrastructure of
propaganda to stimulate support in the West for Syria's political and armed opposition.
Virtually every aspect of the Syrian opposition was cultivated and marketed by Western
government-backed public relations firms, from their political narratives to their branding,
from what they said to where they said it.
The leaked files reveal how Western intelligence cutouts played the media like a fiddle,
carefully crafting English- and Arabic-language media coverage of the war on Syria to churn out
a constant stream of pro-opposition coverage.
US and European contractors trained and advised Syrian opposition leaders at all levels,
from young media activists to the heads of the parallel government-in-exile . These firms also
organized interviews for Syrian opposition leaders on mainstream outlets such as BBC and the
UK's Channel 4.
More than half of the stringers used by Al Jazeera in Syria were trained in a joint US-UK
government program called Basma, which produced hundreds of Syrian opposition media
activists.
Western government PR firms not only influenced the way the media covered Syria, but as the
leaked documents reveal, they produced their own propagandistic pseudo-news for broadcast on
major TV networks in the Middle East, including BBC Arabic, Al Jazeera, Al Arabiya, and Orient
TV .
These UK-funded firms functioned as full-time PR flacks for the extremist-dominated Syrian
armed opposition. One contractor, called InCoStrat, said it was in constant contact with a
network of more than 1,600 international journalists and "influencers," and used them to push
pro-opposition talking points.
Another Western government contractor, ARK, crafted a strategy to "re-brand" Syria's
Salafi-jihadist armed opposition by "softening its image ." ARK boasted that it provided
opposition propaganda that "aired almost every day on" major Arabic-language TV networks."
"The Western contractor ARK was a central force in launching the White Helmets operation.
The leaked documents show ARK ran the Twitter and Facebook pages of Syria Civil Defense,
known more commonly as the White Helmets.
ARK took credit for developing "an internationally-focused communications campaign designed
to raise
global awareness of the (White Helmets) teams and their life saving work."
ARK also facilitated communications between the White Helmets and The Syria
Campaign , a PR firm run out of London and New York that helped popularize the White
Helmets in the United States.
It was apparently "following subsequent discussions with ARK and the teams" that The Syria
Campaign "selected civil defence to front its campaign to keep Syria in the news," the firm
wrote in a report for the UK Foreign Office." thegreyzone
--------------
Using really basic intelligence analytic tools; Occam's Razor, Walks like a duck,
Smileyesque back azimuth's, etc. it has been clear that the UK government has been deeply
involved in sponsoring and influencing the Syrian/ jihadi opposition in that miserable country.
The wide spread British Old Boys network of aspirants to the tradition of imperial manipulation
has been visible just below the surface if you had eyes to look and a brain to think.
A lot of the money for this folly came right out of USAID.
pl
https://thegrayzone.com/2020/09/23/syria-leaks-uk-contractors-opposition-media/
ISL ,
27 September 2020 at 04:03 PM
Dear Colonel agreed.
I object to the line in the article that they "played the media like a fiddle" - as it
implies the mainstream media is a victim as opposed to willing accomplice.
The American public very strongly told Obama they didn't want another invasion and war in
the middle east (red lines or not) so rather ineffective propaganda.
Moreover, I suspect that given the US public inattention to overseas events that do not
involve much US blood (in places they can not find on a map). Today's mess would be where
more or less the same if the entire IO had never happened - though maybe with less cynicism
of US/UK gov'ts and media.
OTH, it is curious how well the British Old Boys network (and US) aligns with Israeli
interests (and runs counter to US or British interests). Maybe grayzone will investigate that
(impressive) IO campaign. I think a small country in the middle east played US and UK elites
like a fiddle.
The Twisted
Genius
27 September 2020 at 04:48 PM
I've only given this article a cursory reading so far and it is clear that the Brits are
going balls to the wall on the PSYOPS/perception management front. This campaign flows
naturally from the strong material support for the Syrian "moderate rebels" provided by the
US, the Brits and probably others for years. We may still be blowing up IS jihadis, but we're
also supporting our own brand of jihadis around Al-Tanf, giving free hand to Erdogan's
jihadis along the Turkish-Syrian border and doing our best to stymie R+6 efforts to crush the
remaining jihadis and unite Syria.
The article focuses on the contractors role in PSYOP. I'm not sure if it mentions the
British government's role in this. The GCHQ's Joint Threat Research Intelligence Group
(JTRIG) probably manages most of those contractors. The British Army also has the 77th
Brigade. This brigade's slogan is: "behavioural change is our unique selling point". Gordon
MacMillan, a reserve officer with the 77th Brigade, is now Twitter's head of editorial
operations for the Middle East.
I bet we're not letting the Brits have all the fun. The CIA Special Activities Center
(formerly SAD) includes the Political Action Group for PSYOP, economic warfare and
cyberwarfare. That dovetails nicely with what CENTCOM is doing in Syria. I knew some of those
guys a while back. I remember scaring them with some of my own anarchist hacker rantings when
I was penetrating those hackers.
Our Army has fours PSYOP groups brigade-sized), two active and 2 reserve. I would think
they have advanced their methodology since I took the course at Bragg. For a few years, they
were called military information support operations (MISO) groups rather than PSYOP groups.
They have since reverted to their PSYOP name although their activities are referred to as
MISO. I don't know what the difference is.
Babak makkinejad ,
27 September 2020 at 05:10 PM
ISL
No, no, no.
There is no such small country as you describe in the Near East.
There is an self-disciplined proxy force masquerading as a state which is mostly funded by
the United States to further the religious policies of the WASP Culture Continent.
It is no accident that in this context, the names of US and UK occur often in the same
sentences; one declared a crusade to wrestle control of Plastine from Muslims, and the otber
one carried out that crusade and escalated it.
That is also the reason that US cannot end the war over Palestine or leave Islamdom
(Oil, Geostrategic considerations, arms sales, Realpolitik are just pseudo-rationications
to obscure the real war.)
Diana Croissant ,
28 September 2020 at 07:45 AM
Where is Candide (aka Voltaire) when we need him?
BABAK MAKKINEJAD ,
28 September 2020 at 09:14 AM
Ishmael Zechariah
How WASP-dom has arrived in this crusade is not, in my opinion, as significant as that it
has been waging it for more than a hundred years.
fakebot ,
28 September 2020 at 10:43 AM
"WASP Culture" is into golfing, not crusading. Erik Prince and the religious
fundamentalists, maybe, but they don't drive US policy.
Russia and/or Chinese dominion over Eurasia cannot be permitted. Their means to achieve
that would be less ethical, not that the US or UK have been prince among men and salts of the
earth, as noted in the article.
The US has tried in vain to win over hearts and minds. It has been a mostly noble effort
to bring countries like Iraq and Afghanistan into the 21st century, but it was always more of
a losing game. The problem lies too much in Islam and tribal rivalries.
Highly recommended !
Truth be told: political operatives own and run our MSM. This is why the press is called
the 'Fourth Estate'.
They are more correctly described as a Fifth Column , one far more open and sworn to
destroy our country and its foundational citizens – and taxpayers – as any that
ever operated during World War II. You would think this would be of vital interest to people
who loudly declare themselves to be "Nazi-punchers", but who time and again show themselves to
be merely low-level street terrorists informed and inspired by Mao's Red Guard and the
irredeemable thugs of the African National Congress.
One wonders what's preventing them from
mimicking the Red Terror waged by the leftists of Spain, when the battle for "freedom" involved
the disinterment of the graves of Catholic clergy to better pose the corpses in blasphemous
positions. Imagine how depraved those Mostly Peaceful protesters had to have been for even a
leftist-supporting site such as Wikipedia to baldly state
The violence consisted of the killing of tens of thousands of people (including 6,832
Roman Catholic priests, the vast majority in the summer of 1936 in the wake of the military
coup), attacks on the Spanish nobility, industrialists, and conservative politicians, as well
as the desecration and burning of monasteries and churches.
Directly in the crosshairs this time are small and medium-sized owner-operated businesses
– the true backbone of American freedom and prosperity – who have largely been
sacrificed in exchange for the knock-kneed offerings of Danegeld from our giant conglomerates,
all of whom have prospered immensely from the suffering and privation brought on by the
Democratic lockdown of society – and the total shutdown of our economy.
Think! – have you read a single article charting how the government war on small
business directly enriched Amazon.com and
world's richest autocrat, Jeff Bezos? . who then funnels his windfall into a newspaper that
blatantly pimps for the Democratic Party, which translates into a vast payday for the DNC, not
least from its newly-approved partnership with the shadowy and many-tentacled Soros-surrogate
group, BLM?
The result is what you'd expect when a fringe group operates with the full cooperation and
partnership of major industry and both political parties (don't confuse Trump with a
standard-issue Republican, please – he may have terrible flaws, but that isn't one of
them) – 10% of the population holding the other 90% in a chokehold with only one set of
rules: no arrest and prosecution for Bolshevik violence and terror ..but the zero-tolerance
heavy hand of corrupt Leviathan coming down hard against any and all citizens who fight back
or, eventually – inevitably – who even struggle against their restraints.
Short of the sudden arrival of celestial horsemen to punish the guilty and reward the
set-upon, it has become clear that the only answer is the one that the Powers That Be claim to
be dead set against: racial separatism. (Particularly when we consider that all that will be
necessary to turn America into Hell on earth will be the adoption of Ibram Kendi's First Law,
sometimes known as equality of outcome :
To fix the original sin of racism, Americans should pass an anti-racist amendment to the
U.S. Constitution that enshrines two guiding anti-racist principals: Racial inequity is
evidence of racist policy and the different racial groups are equals.
Could any "amendment" be more terrifyingly totalitarian than this?)
White and black separation would, instead, accomplish two goals, both more important than
Kendi's quick fix: we would learn soon enough about actual equality of outcomes (which
is why no Communist, black or white, wants anything to do with the creation of one more failed
basket-case black state), and much more importantly, white families can sleep secure in their
beds at night, without worrying about Apache raids at midnight, egged on and recorded for
"posterity" by that Fourth Estate/Fifth Column referred to up top. Because the fact of the
matter is that, even should some combination of government and law-enforcement halt the burning
and looting of America – as things stand now, none of the worst malefactors will ever see
the inside of a prison cell .which means any ceasefire will only be temporary, to be violently
ripped asunder the moment they sense white Americans have at last lowered their guard once
more. And living in perpetual paranoid readiness for violent uprisings and mindless destruction
is no way to live at all.
Trump has it half right, a border wall is the answer: only it needs to run
lengthwise , between the Southern and Northern borders. If we don't use the next four
years to plan out such a separation, fretting over our children's children will be a fruitless
exercise – those who aren't murdered will be captured and 'go native' .and in case you
haven't looked at a globe lately, there's no place left to run.
Majority of
One
August 21, 2020 at 4:33 pm GMT
@Miro23
As a recovering journalist, I can point out that even on a rinkydink rag in a small city,
where I got fired for being a real journalist back in the early '70's; he who owns the
presses and distribution networks calls the tune. It's a matter of working-class (no matter
how middle-class your income or social-status) versus the ownership class. The latter wins
every time.
In March, as the United States faced a shortage of COVID-19 diagnostic tests to determine who was currently infected with the
virus, the Food and Drug Administration began allowing antibody tests into the country without FDA review or formal clearance.
A COVID-19 molecular diagnostic test, sometimes referred to as a virology test, is often conducted through a nasal or throat
swab. It is designed to detect if you presently have the COVID-19 virus.
A COVID-19 antibody test, or serology test, usually involves a blood sample and determines the presence of antibodies, which may
signal that you previously had the viral infection.
"The two different types of tests give us complementary information about the pandemic," said Dr. Alex Marson, an infectious
disease specialist and the director of the Gladstone UCSF Institute for Genomic Immunology. "The one tells us about who's
actively infected. The other tells us who has been infected."
Dr. Marson and Dr. Patrick Hsu, an assistant professor of bioengineering at the University of California, Berkeley both told 60
Minutes it is presently unknown if a positive antibody test means protection from future infection.
"We do not know if a positive antibody test means that you have protective immunity," said Dr. Hsu. "It will certainly mean that
in some cases, but how much, and for how long, and how many times? We do not yet know. People should not assume that, if you have
a positive antibody test that you're immune, [that] you don't need to wear a mask, and [that] you don't need to socially
distance."
A small sample size study from China published on June 18 in
Nature
Medicine
found antibodies could fade in as soon as two to three months after the time of infection.
Both Dr. Marson and Dr. Hsu were interviewed by 60 Minutes correspondent Sharyn Alfonsi as part of a three-month investigation
into the accuracy of antibody tests available in the U.S. The physicians assembled a team of scientists to study the accuracy of
COVID-19 antibody tests in early March.
The accuracy of antibody tests are measured by their sensitivity and specificity. The sensitivity refers to a test's ability
to determine if someone has COVID-19 antibodies present in his or her body. The specificity refers to a test's ability to
distinguish who does not have COVID-19 antibodies.
In the early months of the pandemic, hundreds of companies from around the world were selling antibody tests in the U.S. with
varying levels of accuracy.
In May, the FDA amended its policy and began requiring developers of antibody tests to apply for emergency authorization and
submit data to prove their tests work. The FBI
warns
the
policy change has not stopped scammers from trying to infiltrate the U.S. market with fraudulent or inferior quality tests.
The FDA also teamed with the other government agencies including the National Institutes of Health to track the accuracy of some
antibody tests and on June 18 published
performance
results
for 21 of them.
The FDA's list includes both rapid serology tests that are often processed on-location and tests that require blood samples be
sent to a laboratory.
ARRAY / AP
"I will say that the best tests, especially tests where blood samples are being sent off to labs, seem to have responsible test
performance characteristics," Dr. Marson told Alfonsi. "Does that mean that they're perfect? No"
The FDA says the prevalence of COVID-19 in a specific area and amongst different groups of people will factor into the likelihood
of false positive or false negative results.
"I think when you ever get a positive test, it's important to undergo confirmatory testing, whether with a different antibody
test, or an independent test that looks for a different viral antigen, or a different antibody isotype," Dr. Hsu told 60 Minutes.
"This will be a way that we can guard against false positives. The statistical likelihood that you would test false positive
twice is generally quite unlikely if you use independent tests."
Getting multiple independent tests might be more difficult than it sounds.
Quest Diagnostics and LabCorp are two of the largest laboratory testing providers in the U.S. They have collectively processed
more than 3.5 million COVID-19 serology tests.
Quest told 60 Minutes it presently offers antibody tests manufactured by Abbott Laboratories, EUROIMMUN AG, and Ortho Clinical
Diagnostics. LabCorp said it currently uses serology tests made by Abbott and Roche.
Both lab companies told 60 Minutes they do not allow patients to choose which antibody test is used ahead of a sample being
processed.
Quest said the testing platform used to process a sample depends on a lab's volume and capacity. The company said it can run
200,000 serology tests per day and has conducted 2.1 million since April.
LabCorp said it began serology testing on a limited basis in March and now has the ability to run 300,000 samples a day. It does
not disclose the daily volume of antibody testing, but told 60 Minutes it has processed approximately 1.4 million tests so far.
As of June 27, the Centers for Disease Control and Prevention
reported
more
than 32 million tests have been processed in the U.S. with a positivity rate of 9%. The CDC declined to tell 60 Minutes the
specific sources of its aggregated data. A spokesperson told 60 Minutes the 32 million tests include both viral and antibody test
results. The CDC also says not all test results are reported to them.
A Government Accountability Office
report
released
on June 25, 2020 says the watchdog agency found that the CDC has made mistakes in its collection of data about COVID-19 testing.
It says the CDC was gathering data about testing that combined antibody tests with diagnostic tests in their overall testing
numbers, a practice that has been criticized by scientists as mixing apples and oranges.
The CDC made an effort to correct this practice and advise states to separate virology and serology test results, but the overall
testing numbers from prior to June may still be inaccurate. Given the problems with accuracy of some antibody tests, it is also
unclear whether all antibody positives should be considered true positives.
The video above was produced by Keith Zubrow and Sarah Shafer Prediger. It was edited by Sarah
Shafer Prediger.
Sept. 1, 2020
People may have antibodies for at least four months after they get COVID-19, a study
published Tuesday in the New England Journal of Medicine suggests.
The study pulled from a massive dataset from Iceland, looking for the presence of antibodies
in more than 30,000 blood samples. The samples came from three groups of people: those with
confirmed COVID-19 cases, those who had been exposed to the virus but weren't necessarily
infected, and those who had no known exposure.
The researchers focused on a small subset of 487 people who had had more than one antibody
test, which allowed researchers to see whether antibody levels remained stable or faded over
time. In this group, the researchers found, antibody levels increased in the first two months
after diagnosis and remained stable for the next two months.
Stefánsson said the study detected antibodies in a significant number of people who
had been asymptomatic and were never tested for COVID-19.
Not everyone developed antibodies after infection, the authors wrote, suggesting that some
people might have weaker immune responses to the virus. It's possible, however, that those
people had false positive diagnostic tests and were never sick in the first place.
The researchers noted several other interesting trends. Antibody levels were higher in older
patients and in those with more severe disease. Women also had lower antibody levels compared
to men, and smokers had lower antibody levels than nonsmokers.
"What they're seeing here is that they're inducing a pretty strong immune response," said
Jason Kindrachuk, an assistant professor of medical microbiology & infectious diseases at
the University of Manitoba in Winnipeg.
But while the data suggest that antibody levels remain stable for at least four months,
questions remain.
"What we don't know is really the million-dollar question: How do these antibodies reflect
immunity against this virus and inhibition of this virus," said Kindrachuk, who wasn't involved
with the research. "Just because you see antibodies being produced, it doesn't tell you that
those antibodies are going to act specifically against the virus."
In other words, it's unclear whether the antibodies will protect people from being
reinfected.
Confirmed cases of people being reinfected with the coronavirus are exceedingly rare. Last
week, it was reported that four people were reinfected, the only such instances out of more
than 25 million cases worldwide.
In August, the Centers for Disease Control and Prevention changed its quarantine guidelines,
saying people with confirmed COVID-19 didn't need to be tested again for three months if they
didn't develop any symptoms.
The study isn't the first to show that antibodies can stick around for some time after
infection.
The data in the new study are in line with those in a July preprint article showing that
antibody levels were stable for at least three months in patients who had recovered from the
virus in New York City, said Elitza Theel, director of the infectious diseases serology
laboratory at the Mayo Clinic in Rochester, Minnesota.
SOURCE:
DERRICK BROZE, THE LAST AMERICAN VAGABOND
S EVIDENCE MOUNTS THAT THE "GOLD STANDARD" TEST FOR DETECTING COVID-19 IS UNRELIABLE, WHY ARE HEALTH OFFICIALS AROUND THE WORLD
CALLING FOR MORE TESTS?
In the months since the COVID-19 panic began health authorities around the world have told the public to "get tested" to help
track the spread of SARS-CoV-2. However, as fear and hysteria subside, the scientific community and public at large are calling into
question the efficacy of the test used to determine a patients status. This article is a brief examination of the evidence that the
PCR test is unreliable and should not be used as a determinant for the number of COVID-19 cases or as a factor in political decisions.
HOUSTON HEALTH AUTHORITY HAS CONCERNS ABOUT PCR TEST
On August 31, I attended a press conference in Houston to
ask the Mayor and Houston Health Authority about reports regarding problems with the Texas Department of State Health Services'
numbers on COVID-19 cases. TLAV has
previously
reported on these concerns with the COVID-19 case numbers in Texas. I also had a chance to ask Houston Health Authority Dr. David
Persse about concerns around the test used to detect COVID-19.
The most common test is a polymerase chain reaction (PCR) lab test. This incredibly sensitive technique was developed by Berkeley
scientist Kary Mullis, for which he was awarded the Nobel Prize in 1993. The test is designed to detect the presence of a virus by
amplifying the virus' genetic material so it can be detected by scientists. The test is viewed as the gold standard, however, it
is not without problems.
The PCR test uses chemicals to amplify the virus's genetic material and then each sample goes through a number of cycles until
a virus is recovered. This "cycle threshold" has become a key component in the debate around the efficacy of the PCR test.
Dr. Persse says that when the labs report numbers of COVID-19 cases to the City of Houston they only offer a binary option of
"yes" for positive or "no" for negative. "But, in reality, it comes in what is called cycle-thresholds. It's an inverse relationship,
so the higher the number the less virus there was in the initial sample," Persse explained. "Some labs will report out to
40 cycle-thresholds, and if they get a positive at 40 – which means there is a tiny, tiny, tiny amount of virus there – that gets
reported to us as positive and we don't know any different."
Persse noted that the key question is, at what value is someone considered still infectious?
"Because if you test me and I have a tiny amount of virus, does that mean I am contagious? that I am still infectious to someone
else? If you are shedding a little bit of virus are you just starting? or are you on the downside?," Dr. Persse asked in the lobby
of Houston City Hall. He believes the answer is for the scientific community to set a national standard for cycle-threshold.
Unfortunately, a national standard would not solve the problems expressed by Dr. Persse and others.
UK PARLIAMENT AND SCIENTISTS HAVE CONCERNS ABOUT PCR TEST
In the first weeks of September a number of important revelations regarding the PCR test have come to light. First, new research
from the University of Oxford's Center for Evidence-Based Medicine and the University of the West of England found that the PCR test
poses the potential for false positives when testing for COVID-19. Professor Carl Heneghan, one of the authors of the study,
Viral cultures for COVID-19 infectivity
assessment – a systematic review , said there was a risk that an increase in testing in the UK will lead to an increase in the
risk of "sample contamination" and thus an increase in COVID-19 cases.
The team reviewed evidence from 25 studies where virus specimens had positive PCR tests. The researchers state that the "genetic
photocopying" technique scientists use to magnify the sample of genetic material collected is so sensitive it could be picking up
fragments of dead virus from previous infections. The researchers reach a similar conclusion as Dr. David Persse, namely that,
"A binary Yes/No approach to the interpretation RT-PCR unvalidated against viral culture will result in false positives with segregation
of large numbers of people who are no longer infectious and hence not a threat to public health."
Heneghan, who is also the the editor of BMJ Evidence-Based Medicine,
told the BBC that the binary approach is a problem and tests
should have a cut-off point so small amounts of virus do not lead to a positive result. This is because of the cycle threshold mentioned
by Dr. Persse. A person who is shedding an active virus and someone who has leftover infection could both receive the same positive
test result. He also stated that the test could be detecting old virus which would explain the rise in cases in the UK. Heneghan
also stated that setting a standard for the cycle threshold would eliminate the quarantining and contact tracing of people who are
healthy and help the public better understand the true nature of COVID-19.
The UK's leading health agency, Public Health England, released an update on the testing methods used to detect COVID-19 and appeared
to agree with Professor Heneghan regarding
the concerns on the cycle threshold. On September 9, PHE
released an update which concluded, "all laboratories should determine the threshold for a positive result at the limit of
detection."
This is not the first time Heneghan's work has directly impacted the UK's COVID-19 policies. In July, UK health secretary Matt
Hancock called for an "urgent review" of the daily COVID-19 death
numbers produced by Public Health England after it was revealed the stats included people who died from other causes.
The Guardian reported:
"The oddity was revealed in a paper by Yoon K Loke and Carl Heneghan of the Centre for Evidence-Based Medicine at Oxford
University, called "
Why no one can ever recover from Covid-19 in England – a statistical anomaly ".
Their analysis suggests PHE cross-checks the latest notifications of deaths against a database of positive test results
– so that anyone who has ever tested positive is recorded in the COVID-19 death statistics.
A Department of Health and Social Care source said: 'You could have been tested positive in February, have no symptoms,
then hit by a bus in July and you'd be recorded as a COVID death.'"
Only days after Hancock called for the review of PHE data, the UK government
put an immediate halt to its daily update of death numbers from COVID-19.
On September 8, Heneghan tweeted out another
study on the limitations of the PCR test. The study,
"SARS-CoV-2 Testing: The Limit of Detection Matters"
, examines the limit of detection (LoD) for RNA. The researchers note similar problems with the PCR test and the cycle threshold,
concluding, "the ultimate lesson from these studies bears repetition: LoD matters and directly impacts efforts to identify, control,
and contain outbreaks during this pandemic."
Heneghan also recently told the BMJ , "one issue
in trying to interpret numbers of detected cases is that there is no set definition of a case. At the moment it seems that a polymerase
chain reaction (PCR) positive result is the only criterion required for a case to be recognised."
"In any other disease we would have a clearly defined specification that would usually involve signs, symptoms, and a test
result," Heneghan explained. "We are moving into a biotech world where the norms of clinical reasoning are going out of the
window. A PCR test does not equal covid-19; it should not, but in some definitions it does."
Heneghan says he is concerned that as soon as there is the appearance of an outbreak there is panic and over-reacting. "This
is a huge problem because politicians are operating in a non-evidence-based way when it comes to non-drug interventions," he
stated.
THE EVIDENCE FOR FALSE POSITIVES IS OVERWHELMING
A recent
report from NPR outlines the dangers of false positives with the PCR tests. Andrew Cohen, director of the Center for Research
on Aquatic Bioinvasions, was hired by the state of California to study an invasion of non-native mussels. The researchers took water
samples and used a PCR test to search for genetic material from the mussels. After the tests came back overwhelmingly positive, Cohen
grew suspicious.
"I began to realize that many of these -- if not all of these -- were false positives, especially when they started being reported
in waters that had chemistry that would not allow the mussels to reproduce and establish themselves," he told NPR. NPR notes
that, depending on the lab, there was a 2 to 8 percent false positive rate.
Once COVID-19 was declared a pandemic, Cohen said he began asking if the reports of people with absolutely no symptoms and positive
PCR test results could be false positives. "I began wondering whether these asymptomatic carriers weren't in large part or in
whole part the human counterparts of those false-positive results of quagga and zebra mussels in all those water bodies across the
West," he said.
Cohen emphasized the importance of researchers taking potential false positive PCR results seriously. "As near as we can tell,
the medical establishment and public health authorities and researchers appear to be assuming that the false-positive rate in in
the PCR based test is zero, or at least so low that we can ignore it."
Cohen is correct that the scientific authorities need to take false positives seriously, especially when a person can be sent
to isolate or quarantine for weeks due to a positive test result. Even the
U.S. FDA's own fact sheet on testing acknowledges the
dangers posed by false positives:
"The CDC 2019-nCoV Real-Time RT-PCR Diagnostic Panel has been designed to minimize the likelihood of false positive test
results. However, in the event of a false positive result, risks to patients could include the following: a recommendation for
isolation of the patient, monitoring of household or other close contacts for symptoms, patient isolation that might limit contact
with family or friends and may increase contact with other potentially COVID-19 patients, limits in the ability to work, the delayed
diagnosis and treatment for the true infection causing the symptoms, unnecessary prescription of a treatment or therapy, or other
unintended adverse effects."
A CDC fact
sheet also acknowledges the possibility of false positives with the PCR test.
Professor Heneghan believes the confusion around COVID-19 has come as a result of a shift away from "evidence-based medicine."
In a recent opinion piece
published at
The Spectator , Heneghan and Tom Jefferson, a senior associate tutor and honorary research fellow at the Centre for Evidence-Based
Medicine, University of Oxford, wrote that patients have become a "prisoner of a system labelling him or her as 'positive' when we
are not sure what that label means." The two scientists offer this conclusion and warning:
Governments are producing a series of contradictory and confusing policies which have a brief shelf life as the next crisis
emerges. It is increasingly clear the evidence is often ignored. Keeping up to date is a full time occupation, and the advances
of the last 30 years have at best been put on hold.
The duties of a
good doctor
include working in partnership with patients to inform them about what they want or need in a way they can understand, and respecting
their rights to reach decisions with you about their treatment and care. Questions need to be asked as to how this will occur
if you don't see your doctor, particularly if all you have to do is queue in at a drive in to get your answer.
And ultimately what is a 'good test'? We think it's the test which helps your doctor narrow the uncertainty around the origins
and management of your problem.
RELATED ARTICLES: Tuesday, September 8, 2020 -
"Dead" Virus Cells Frequently Trigger "False Positives" In Most Common COVID Test, New Study Finds
In the past, our reports raising questions about the accuracy of COVID-19 tests have been met with accusations of 'fearmongering'
and spreading 'misinformation'.
Wednesday, June 10, 2020 -
REPORT: Over 95% of UK "Covid19" deaths had "pre-existing condition"
Over 95% of "COVID Deaths" recorded in England and Wales had potentially serious comorbidities, according to statistics released
by NHS England. RELATED ARTICLES: Tuesday, September 8, 2020 -
"Dead" Virus Cells Frequently Trigger "False Positives" In Most Common COVID Test, New Study Finds
In the past, our reports raising questions about the accuracy of COVID-19 tests have been met with accusations of 'fearmongering'
and spreading 'misinformation'.
Any test with a cycle threshold above 35 is too sensitive, agreed Juliet Morrison, a virologist at the University of California,
Riverside. "I'm shocked that people would think that 40 could represent a positive," she said.
In Massachusetts, from 85 to 90 percent of people who tested positive in July with a cycle threshold of 40 would have been deemed
negative if the threshold were 30 cycles, Dr. Mina said. "I would say that none of those people should be contact-traced, not one,"
he said.
Notable quotes:
"... PCR tests still have a role, he and other experts said. For example, their sensitivity is an asset when identifying newly infected people to enroll in clinical trials of drugs. ..."
Updated Sept. 17, 2020
The usual diagnostic tests may simply be too sensitive and too slow to contain the spread of the virus.
Tests authorized by the F.D.A. provide only a yes-no answer to infection, and will identify as positive patients with low
amounts of virus in their bodies. Credit... Johnny Milano for The New York Times
Some of the nation's leading public health experts are raising a new concern in the endless debate over
coronavirus testing in
the United States: The standard tests are diagnosing huge numbers of people who may be carrying relatively insignificant amounts
of the virus.
Most of these people are not likely to be contagious, and identifying them may contribute to bottlenecks that prevent those who
are contagious from being found in time. But researchers say the solution is not to test less, or to skip testing people without
symptoms, as recently suggested
by the Centers for Disease Control and Prevention .
Instead, new data underscore the need
for more widespread use of rapid tests , even if they are less sensitive.
"The decision not to test asymptomatic people is just really backward," said Dr. Michael Mina, an epidemiologist at the Harvard
T.H. Chan School of Public Health, referring to the C.D.C. recommendation.
"In fact, we should be ramping up testing of all different people," he said, "but we have to do it through whole different mechanisms."
In what may be a step in this direction, the Trump administration announced on Thursday that it would purchase 150 million rapid
tests.
The most widely used diagnostic test for the new coronavirus, called a PCR test, provides a simple yes-no answer to the question
of whether a patient is infected.
But similar PCR tests for other viruses do offer some sense of how contagious an infected patient may be: The results may include
a rough estimate of the amount of virus in the patient's body.
"We've been using one type of data for everything, and that is just plus or minus -- that's all," Dr. Mina said. "We're using
that for clinical diagnostics, for public health, for policy decision-making."
But yes-no isn't good enough, he added. It's the amount of virus that should dictate the infected patient's next steps. "It's
really irresponsible, I think, to forgo the recognition that this is a quantitative issue," Dr. Mina said.
The PCR test amplifies genetic matter from the virus in cycles; the fewer cycles required, the greater the amount of virus, or
viral load, in the sample. The greater the viral load, the more likely the patient is to be contagious.
This number of amplification cycles needed to find the virus, called the cycle threshold, is never included in the results sent
to doctors and coronavirus patients, although it could tell them how infectious the patients are.
In three sets of testing data that include cycle thresholds, compiled by officials in Massachusetts, New York and Nevada, up to
90 percent of people testing positive carried barely any virus, a review by The Times found.
On Thursday, the United States recorded 45,604 new coronavirus cases, according to a database maintained by The Times. If the
rates of contagiousness in Massachusetts and New York were to apply nationwide, then perhaps only 4,500 of those people may actually
need to isolate and submit to contact tracing.
One solution would be to adjust the cycle threshold used now to decide that a patient is infected. Most tests set the limit at
40, a few at 37. This means that you are positive for the coronavirus if the test process required up to 40 cycles, or 37, to detect
the virus.
Tests with thresholds so high may detect not just live virus but also genetic fragments, leftovers from infection that pose no
particular risk -- akin to finding a hair in a room long after a person has left, Dr. Mina said.
Any test with a cycle threshold above 35 is too sensitive, agreed Juliet Morrison, a virologist at the University of California,
Riverside. "I'm shocked that people would think that 40 could represent a positive," she said.
A more reasonable cutoff would be 30 to 35, she added. Dr. Mina said he would set the figure at 30, or even less. Those changes
would mean the amount of genetic material in a patient's sample would have to be 100-fold to 1,000-fold that of the current standard
for the test to return a positive result -- at least, one worth acting on.
Image
"It's just kind of mind-blowing to me that people are not recording the C.T. values from all these tests, that they're just
returning a positive or a negative," one virologist said. Credit... Erin Schaff/The New York Times
The Food and Drug Administration said in an emailed statement that it does not specify the cycle threshold ranges used to determine
who is positive, and that " commercial manufacturers and
laboratories set their own."
The Centers for Disease Control and Prevention said it is examining the use of cycle threshold measures "for policy decisions."
The agency said it would need to collaborate with the F.D.A. and with device manufacturers to ensure the measures "can be used properly
and with assurance that we know what they mean."
The C.D.C.'s own calculations suggest that it is extremely difficult to detect any live virus in a sample
above a threshold of 33 cycles
. Officials at some state labs said the C.D.C. had not asked them to note threshold values or to share them with contact-tracing
organizations.
For example, North Carolina's state lab uses the Thermo Fisher coronavirus test, which automatically classifies results based
on a cutoff of 37 cycles. A spokeswoman for the lab said testers did not have access to the precise numbers.
This amounts to an enormous missed opportunity to learn more about the disease, some experts said.
"It's just kind of mind-blowing to me that people are not recording the C.T. values from all these tests -- that they're just
returning a positive or a negative," said Angela Rasmussen, a virologist at Columbia University in New York.
"It would be useful information to know if somebody's positive, whether they have a high viral load or a low viral load," she
added.
Officials at the Wadsworth Center, New York's state lab, have access to C.T. values from tests they have processed, and analyzed
their numbers at The Times's request. In July, the lab identified 872 positive tests, based on a threshold of 40 cycles.
With a cutoff of 35, about 43 percent of those tests would no longer qualify as positive. About 63 percent would no longer be
judged positive if the cycles were limited to 30.
In Massachusetts, from 85 to 90 percent of people who tested positive in July with a cycle threshold of 40 would have been deemed
negative if the threshold were 30 cycles, Dr. Mina said. "I would say that none of those people should be contact-traced, not one,"
he said.
Other experts informed of these numbers were stunned.
"I'm really shocked that it could be that high -- the proportion of people with high C.T. value results," said Dr. Ashish Jha,
director of the Harvard Global Health Institute. "Boy, does it really change the way we need to be thinking about testing."
Dr. Jha said he had thought of the PCR test as a problem because it cannot scale to the volume, frequency or speed of tests needed.
"But what I am realizing is that a really substantial part of the problem is that we're not even testing the people who we need to
be testing," he said.
The number of people with positive results who aren't infectious is particularly concerning, said Scott Becker, executive director
of the Association of Public Health Laboratories. "That worries me a lot, just because it's so high," he said, adding that the organization
intended to meet with Dr. Mina to discuss the issue.
The F.D.A. noted that people may have a low viral load when they are newly infected. A test with less sensitivity would miss these
infections.
But that problem is easily solved, Dr. Mina said: "Test them again, six hours later or 15 hours later or whatever," he said. A
rapid test would find these patients quickly, even if it were less sensitive, because their viral loads would quickly rise.
PCR tests still have a role, he and other experts said. For example, their sensitivity is an asset when identifying newly infected
people to enroll in clinical trials of drugs.
But with 20 percent or more of people testing positive for the virus in some parts of the country, Dr. Mina and other researchers
are questioning the use of PCR tests as a frontline diagnostic tool.
People infected with the virus are most infectious from a day or two before symptoms appear till about five days after. But at
the current testing rates, "you're not going to be doing it frequently enough to have any chance of really capturing somebody in
that window," Dr. Mina added.
Highly sensitive PCR tests seemed like the best option for tracking the coronavirus at the start of the pandemic. But for the
outbreaks raging now, he said, what's needed are coronavirus tests that are fast, cheap and abundant enough to frequently test everyone
who needs it -- even if the tests are less sensitive.
"It might not catch every last one of the transmitting people, but it sure will catch the most transmissible people, including
the superspreaders," Dr. Mina said. "That alone would drive epidemics practically to zero."
An earlier version of this article, using information provided by a laboratory spokesman, misstated the number of positive coronavirus
tests in July processed by Wadsworth Center, New York's state lab. It was 872 tests, not 794. Based on that error, the article also
misstated the number of tests that would no longer qualify as positive with a C.T. value of 35 cycles. It is about 43 percent of
the tests, not about half of them. Similarly, the article misstated the number of tests that would no longer qualify as positive
if cycles were limited to 30. It is about 63 percent of the tests, not about 70 percent.
Apoorva Mandavilli is a reporter for The Times, focusing on science and global health. She is the 2019 winner of the Victor Cohn
Prize for Excellence in Medical Science Reporting. @ apoorva_nyc A
version of this article appears in print on Aug. 30, 2020 , Section A, Page 6 of the New York edition with the headline: You're Positive.
But Are You Contagious? Tests May Be Too Sensitive, Experts Say . Order Reprints
| Today's Paper |
Subscribe
By Theresa
Phillips Updated October 25, 2019
PCR stands for polymerase chain
reaction , a molecular biology technique for amplifying segments of DNA, by generating
multiple copies using DNA polymerase enzymes under controlled conditions. As little as a single
copy of a DNA segment or gene can be cloned into millions of copies, allowing detection using
dyes and other visualization techniques.
me title=
Developed in 1983, the process of PCR has made it possible to perform DNA sequencing and identify
the order of nucleotides in individual genes. The method uses thermal cycling or the repeated
heating and cooling of the reaction for DNA melting and replication. As PCR continues, the
"new" DNA is used as a template for replication and a chain reaction ensues, exponentially
amplifying the DNA template.
https://d956b974574e4d9df2e942a9641c69dc.safeframe.googlesyndication.com/safeframe/1-0-37/html/container.html
PCR techniques are applied in many areas of biotechnology including protein engineering , cloning,
forensics (DNA fingerprinting), paternity testing, the diagnosis of hereditary and/or
infectious diseases, and for the analysis
of environmental samples.
In forensics, in particular, PCR is especially useful because it amplifies even the smallest
amount of DNA evidence. PCR can also be used to analyze DNA that is thousands of years old, and
these techniques have been used to identify everything from an 800,000-year-old mammoth to
mummies from around the world.
PCR Procedure Initialization
This step is necessary only for DNA polymerases that require hot-start PCR. The reaction is
heated to between 94 and 96 °C and held for 1-9 minutes.
Denaturation
If the procedure does not require initialization, denaturation is the first step. The
reaction is heated to 94-98 °C for 20-30 seconds. The DNA template's hydrogen bonds are
disrupted and single-stranded DNA molecules are created.
Annealing
The reaction temperature is lower to between 50 and 65 °C and held for 20-40 seconds.
The primers anneal to the single-stranded DNA template. The temperature is extremely important
during this step. If it's too hot, the primer might not bind. If it's too cold, the primer
might bind imperfectly. A good bond is formed when the primer sequence closely matches the
template sequence.
Extension/Elongation
The temperature during this step varies depending upon the type of polymerase. The DNA
polymerase synthesizes a completely new DNA strand.
Final Elongation
This step is performed at 70-74 °C for 5-15 minutes after the final PCR
cycle.
Final Hold
This step is optional. The temperature is kept at 4-15 °C and strops the
reaction.
Three Stages of the PCR Procedure Exponential Amplification
During every cycle, product (the specific piece of DNA that is being replicated) is
doubled.
Leveling-off Stage
As the DNA polymerase loses activity and consumes reagents, the reaction
slows.
Plateau
No more product accumulates.
Vaccine against coronaviruses is a very tricky business as the virus tend to mutate with
time. Still it looks like Russian found some nw avenue to tackle this problem which might be more
efficient then alternatives.
Notable quotes:
"... Science Magazine ..."
"... Science Magazine ..."
Western reporters to not like to correct their own false reporting. They rather reinforce it
as much as possible. Only when overwhelmed by the facts will they silently admit that they were
wrong in the first place. Here is a prime example of how that's done.
In mid-August we exposed how 'western' media lied about the approval for phase-3 testing of
the Russian Sputnik vaccine against Covid-19. They said that Russia claimed the vaccine was
ready to go population wide. That never was the case.
'Western' Media Falsely Claim That Russia's Covid-19 Vaccine Is Ready To Go
Russia has not approved a vaccine against Covid-19 and it is not skipping large-scale
clinical trials. The Russia regulator gave a preliminary approval for a vaccine candidate to
start the large-scale clinical trial. [...]
Science Magazine is one of the few media who
got it right : ...
One of the false reports we pointed out was by the New York Times Moscow
correspondent Andrew E. Kramer:
Russia
Approves Coronavirus Vaccine Before Completing Tests
Russia has become the first country in the world to approve a vaccine for the coronavirus,
President Vladimir V. Putin announced on Tuesday, though global health authorities say the
vaccine has yet to complete critical, late-stage clinical trials to determine its safety and
effectiveness.
Russia had, as we and Science Magazine reported, never the intent to skip
large-scale clinical trials. Kramer made that up.
In new report today Kramer reinforces his previous false and disproven claims to lament
about an alleged slow distribution of the Sputnik vaccine in Russia:
Russia Is
Slow to Administer Virus Vaccine Despite Kremlin's Approval
More than a month after becoming the first country to approve a coronavirus vaccine, Russia
has yet to administer it to a large population outside a clinical trial, health officials and
outside experts say.
The approval, which came with much fanfare, occurred before Russia had tested the vaccine
in late-stage trials for possible side effects and for its disease-fighting ability. It was
seen as a political gesture by President Vladimir V. Putin to assert victory in the global
race for a vaccine.
It is not clear whether the slow start to the vaccination campaign is a result of limited
production capacity or second thoughts about inoculating the population with an unproven
product.
The Times author reinforces his own lie that Russia had declared its vaccine ready
for population wide application. It had never done that. The official registration of the
vaccine by the relevant authorities was only a necessary precondition to start the large scale
phase-3 testing of the vaccine. There never was a Russian intent to distribute the vaccine to a
large population without phase-3 testing.
In the bottom third of his long piece Kramer comes near to admitting that. There he
describes that the Sputnik phase-3 testing is now ongoing. That contradicts all of his previous
reporting on the issues though he himself never says that. But even now he is getting the
details wrong:
The trial in Russia began on Sept. 9, and Russian officials have said they expect early
results before the end of the year, though the Gamaleya Institute, the scientific body that
developed the vaccine, has scheduled the trial to continue until May.
That timeline is similar to the testing schedules announced by the three pharmaceutical
companies testing potential vaccines in the United States, AstraZeneca, Moderna and
Pfizer.
Yevgenia Zubova, a spokeswoman for the Moscow city health department, said in an interview
that the vaccine was available only to trial participants.
Those last two paragraphs, which completely debunk Kramer's original reporting, should have
been at the very top of the piece. They are buried down in paragraph 23 and 24 of a 29
paragraphs story that starts out with an epic repeat of the previously made false claims.
Kramer is wrong to say that the testing is limited to Moscow. As explained on the Sputnik
Vaccine website :
Post-registration clinical trials involving more than 40,000 people in Russia will be
launched in a week starting from August, 24. A number of countries, such as UAE, Saudi
Arabia, Philippines and possibly India or Brazil will join the clinical trials of Sputnik V
locally. [...] Mass production of the vaccine is expected to start in September 2020.
That testing of Sputnik V will also happen outside of Moscow has been confirmed
by recent reports :
Russia's sovereign wealth fund will supply 100 million doses of its potential coronavirus
vaccine to Indian drug company Dr Reddy's Laboratories, the fund said on Wednesday, as Moscow
speeds up plans to distribute its shot abroad.
It is not Russia that is fudging the testing of its vaccine. It is the Trump administration
that is
planning to do so out of political reasons:
Eric Topol @EricTopol - 18:10 UTC · Sep 19,
2020
We have the protocols. Now we know how there will very likely be an Emergency Use Approval
(EUA) for a vaccine prior to November 3. The company and political motivations are fully
aligned.
The criteria for an EUA is that it "may be effective"
https://fda.gov/regulatory-inf ... ... In 'Power Grab,'
Health Secretary Azar Asserts Authority Over F.D.A.
In contrast to the U.S. the Russian testing of its Sputnik vaccine will be -as usual- of
high integrity and will strictly follow the protocols such trials are supposed to follow. In
paragraph 29, the very last one in today's NYT story, the author at last admits as
much :
[W]hen medicines are tested, Russia has an exceptionally good track record on managing
clinical trials , according to a database of U.S. Food and Drug Administration inspections of
clinical trials around the world. The F.D.A. found a lower percentage of trials with problems
in Russia than in any other European country or the United States.
If I get the chance to chose a vaccine for myself I will rather take the one which was
developed by a highly qualified state financed research institution and approved in Russia than
one developed by some profit oriented pharmaceutic conglomerate that is in cahoots with a
politicized regulator under the Trump administration.
Posted by b on September 20, 2020 at 12:12 UTC |
Permalink
foolisholdman , Sep 20 2020 12:21 utc |
1
Very interestng clarification of well-muddied waters! Thank you for that b.
vk
2
If I get the chance to chose a vaccine for myself I will rather take the one which was
developed by a highly qualified state financed research institution and approved in Russia
than one developed by some profit oriented pharmaceutic conglomerate that is in cahoots
with a politicized regulator under the Trump administration.
To top it off, Gamaleya's vaccine simply has the better science behind it. It uses two
human adenoviruses, in opposition to the single chimpanzee adenovirus used by the AstraZeneca
one (the Chinese one also uses only one adenovirus, but I don't remember if it is human or
chimpanzee).
No other laboratory in the world is using Gamaleya's technology - which it already
dominates. Two American laboratories (Moderna and one more that I forgot the name) are
testing the untried and dangerous mRNA technology. It is very unlikely those two mRNA
vaccines will ever come out to the public; those two labs probably just cashed in their USD 2
billion checks they received from the USG.
This gives force to my original hypothesis: the Anglo-Saxon laboratories are exploiting
exotic technologies for their vaccines because they want something the can patent, thus
charging astronomical prices to the national governments and thus emerge from this pandemic
even richer.
--//--
Speaking of AstraZeneca (Oxford), it released its blueprints yesterday after "public
pressure":
A Phase III Randomized, Double-blind, Placebo-controlled Multicenter Study in Adults to
Determine the Safety, Efficacy, and Immunogenicity of AZD1222, a Non-replicating ChAdOx1
Vector Vaccine, for the Prevention of COVID-19
The USG is, behind the scenes (I already posted the link here in the open thread),
extremely worried about this vaccine.
AstraZeneca will try to get what it can get, but the fact is it's game over for them. The
thing here is that the Gamaleya alternative is better and if the USA (where the vaccine
makers will really make money) wants to get political, it will simply opt for one of the many
American vaccines that will come out - ready or not, satisfactory or not - next year. As a
British vaccine, AstraZeneca-Oxford will, at best, have to do with the British market, which
is very tiny for a big pharmaceutical company.
It is better if they just cancel the trials and abandon production.
jo6pac , Sep 20 2020 13:07 utc |
3
If I had money I'd fly to Russia for their vaccine. They made theirs for the people and in
Amerika we make it for profits and protect the makes from lawsuits.
Thanks b and vk
Clueless Joe , Sep 20 2020 13:19 utc |
4
To be frank, at this point, ironically, it's Big Pharma's own self-interest that might help
us to counter Trump's lunacy. There are enough anti-vaxxers around for them not to want a
screwed up vaccine and a big scandal that would only comfort the vaxxers and sow mistrust
among the population. They need people to assume vaccines are well done and mostly harmless
if they want to keep making profit with them. Trump is only interested in a victory in the
next few weeks, Pharma business is interested in making profits for the next decades. Tuyzentfloot , Sep 20 2020 13:22 utc |
5
The Kramer reporting is highly unusual. Normally the important information should be in the
third paragraph from the end and now it's in the sixth and seventh last.
Anyway, while I agree that this vaccine should be treated as an entirely legitimate effort
I want to add:
https://www.themoscowtimes.com/2020/09/08/leading-scientists-question-highly-improbable-russian-vaccine-results-published-in-lancet-a71384).
pnyx , Sep 20 2020 14:02 utc |
6
Kramer is not wrong, he simply lies. In the Relotius media this is standard practice when
covering politically sensitive topics, combined with omissions. Steve , Sep 20 2020 14:05 utc |
7
The Europena and Australian vassals of the USA would not be given a choice to choose the more
authetic option of the vaccine. But Israel would probably opt for the Russian version without
consequence. It's over for the West!
morongobill , Sep 20 2020 14:10 utc |
8
Get your covid 19 news here folks!
Kramer vs Kramer , Sep 20 2020 14:15 utc |
9
Kramer appears to have the right kind of nose. It is all that matters
vk
10
@ Posted by: Tuyzentfloot | Sep 20 2020 13:22 utc | 5
Nobody is saying the Gamaleya vaccine will be the second coming of the polio vaccine.
Whichever COVID-19 vaccine comes out will inevitably be imperfect (in relation to the already
tested and tried vaccines everybody takes nowadays).
Your worries are all legitimate. Indeed, Gamaleya publicly admitted phases 1 and 2 of its
trials has small samples of subjects.
However, you also have to take into account that the science is solid (two human
adenoviruses, a tested and tried technology) and that Gamaleya is the center of excellence in
adenovirus vaccine technology. That's why - and not because it is Russian - we can trust
Gamaleya's vaccine is, given the circumstances (pandemic), reliable. The fact Gamaleya
already dominated the adenovirus technology also explains why it was the first laboratory to
come out with a solution - it simply used a tested and tried method it already dominated,
while the other pharmaceuticals are basically having to relearn how to develop a vaccine
and/or are adventuring in uncharted territory because they want something they can
patent.
So yes, we can search and find defects in Gamaleya's trials - but the strongest argument
in its favor is not the trials, it's the solid science and technology behind it.
Jackrabbit
11
What will the astro-turfed libertarian mob say about vaccines?
My guess: they will support them vociferously.
Because freedumb. And Big Pharma $$$ in their pockets.
!!
Anne , Sep 20 2020 14:54 utc |
12
Vk and the wabbit - right on. And Thanks to you, B, for this clear and straightforwardly
informative piece (as usual).
Is it any surprise that the NYT uses the usual propaganda format of truth (when it accords
with the ruling elites perspective) and lies (when "reporting on" what is happening in those
"bad hat" countries)? And might I add that NPR and the BBC World Service do exactly the same
thing, boosting the US-UK-NATO worldview (which equals the western
corporate-captitalist-imperialist, oh so exceptional, ruling elites world position) while
denigrating Russia, China, Iran (and now Lukashenko - indeed the Beeb refuses to pronounce
his name properly, always reducing it to the feminine form, and believe me, as born and
raised Brit, that's deliberate) via lies, lies and more lies. And via those weasely words:
"likely," "Highly likely" and so on and on ....
All that this latest vaccine competition (western) will produce is more anti-vaxxers. And
this time round, sensibly so.
JohnH , Sep 20 2020 14:57 utc |
13
Tuyzefot (5): it is common for the NYT to lead with propaganda and bury the facts at the end
of the article.
I noticed it decades ago in articles covering Palestine. I learned to skip whatever was
printed on the front page and immediately jump to the final five paragraphs found deep within
the paper. I guess they print the facts at all there only as a bizarre way of covering their
asses in a feeble attempt at integrity.
vk
14
Just saw this, should've posted here earlier. Highly recommend reading in full:
Kirill Dmitriev: Questions on Sputnik V Vaccine Answered, Critics need to Look for Plank in
Own Eyes
Highlights:
The vaccine uses a unique two-vector human adenovirus technology which no-one else in
the world currently has for COVID-19.
[...]
On the surface the Sputnik V trial with 76 participants seems smaller in size compared
to 1,077 people that, for example, AstraZeneca had in its Phase 1-2 studies. However,
the design of the Sputnik V trial was much more efficient and based on better
assumptions.
[...]
The post-registration studies involving more than 40,000 people started in Russia on
August 26, before AstraZeneca has started its Phase 3 trial in the U.S. with 30,000
participants. Clinical trials in Saudi Arabia, United Arab Emirates (UAE), the Philippines,
India and Brazil will begin this month. The preliminary results of the Phase 3 trial will
be published in October-November 2020.
[...]
Q.: Why has the Sputnik V vaccine already become eligible for emergency use
registration?
Because of the very positive results of the Phase 1-2 trials and because the human
adenoviral vector-based delivery platform has been proven the safest vaccine delivery
platform over decades including through 75 international scientific publications and in
more than 250 clinical trials.
[...]
Some other companies are using human adenoviral vector-based platforms for their
COVID-19 vaccines. For example, Johnson & Johnson uses only Ad26 vector and China's
CanSino only Ad5 while Sputnik V uses both of these vectors. The work of Johnson &
Johnson and CanSino not only validates the Russian approach but also shows Sputnik V's
advantage as studies have demonstrated that two different vectors produce better
results than one.
[...]
The monkey adenovirus and mRNA vaccines have never been used and approved before and
their research is lagging the proven human adenoviral vector-based platform by at least 20
years. However, their developers have already secured supply contracts worth billions of
dollars from Western governments and may potentially apply for fast-track registration --
while receiving full indemnity at the same time.
At the end of the Q&A, Dmitriev counters his Western colleagues:
Question 1: Are there any long-term studies of mRNA and monkey adenovirus vector-based
technologies for carcinogenic effects and impact on fertility? (Hint: there are none)
Question 2: Could their absence be the reason why some of the leading pharmaceutical
firms making COVID-19 vaccines based on these technologies pushed the countries buying
their vaccines for full indemnification from lawsuits if something goes wrong?
Question 3: Why is Western media not reporting a lack of long term studies for mRNA and
monkey adenoviral vector-based vaccines?
Those are good questions. Very good questions.
Mark Thomason , Sep 20 2020 15:42 utc |
15
The constant Russia bashing is a disconnect from the truth and the real world.
It is annoying to wade through.
Far more important, it is crippling for a nation if its leadership actually does
disconnect from reality and believe its own fantasy.
Disconnect from reality, belief in convenient fantasy, is exactly how the Democrats went
from losing with Hillary to running again with Hillary II, the same donors and advisers and
influence peddlers pushing the same right wing triangulation by the Democratic Party.
Maybe they can squeak out a win this time. It should not be close.
Far more important, there are things that need doing, things that would win like health
care for all, that they simply won't offer or run on. We are not going to get from them what
we need, we know that, and that is why they again have a squeaker election even against a
joke like Trump.
Patrick
Armstrong
16
Perfect example of the free and unfettered press at work. What do you mean we're just a
propaganda rag? See, right down at the bottom, the bit you didn't bother to read down to,
right next to the denture ad, we told the truth. So there! Balanced and accurate reporting!
Kooshy , Sep 20 2020 16:21 utc |
17
Here in US we are getting 737maxed again this time with FDA
Kooshy , Sep 20 2020 16:28 utc |
18
Trump's "national security" state has managed to kill 200000 by him the autocrat in chief to
come out and tell the truth as he admitted so to Woodward. This fucking American national
security phobia is costing American lives more than all past 70 years of national security
wars.
aquadraht , Sep 20 2020 18:14 utc |
19
The sick transatlantic mindset is exposed here:
https://www.politico.com/news/magazine/2020/08/31/china-covid-19-vaccine-first-401636
Nice to read the comment on Global Times:http://www.globaltimes.cn/content/1199658.shtml
Tuyzentfloot , Sep 20 2020 19:34 utc |
20
@JohnH 13 , it was hm, a joke. There is indeed rule of thumb that you have to look fore the
third to last paragraph. I upgraded it into something of a law, which is then violated in
this case.
Tuyzentfloot , Sep 20 2020 20:10 utc |
21
@vk 10, I wouldn't call it my worries, just that I think B. posted a version which was too
simple and rosy. In the meantime I saw your post 14 which I roughly expected but hadn't read
about yet.
Jen , Sep 20 2020 20:17 utc |
22
Andrew Kramer's reporting on the Sputnik V vaccine is deliberately written to discredit the
Russians and anything and everything they do, which includes the way they conduct scientific
and medical research (because it's govt-funded, not funded by global pharmaceutical
corporations) and the way they run their healthcare system (not privatised).
First, Kramer says the Kremlin approved the vaccine: this is to set up Moscow and Putin in
particular as rash, so that the supposed "roll-out" of the vaccine can be (secondly)
portrayed as inefficient.
Kramer knows he is lying which is why his piece is long (he knows most NYT readers are
time-poor and want the celebrity news and baseball results) and the most important
information is squeezed into the last two paragraphs of his article.
Jen , Sep 20 2020 20:24 utc |
23
Tuyzentfloot @ 5:
I tried linking to that Moscow Times article at your link and either I hit a dead end or
the newspaper removed the article, which does not surprise me since that newspaper is as
credible as The New York Times. It used to be given away f o r free in Moscow but I believe
it now exists only as an online paper.
Tuyzentfloot , Sep 20 2020 20:32 utc |
24
@Jen, you have to remove the last two characters ').' because I omitted a space. The article
in the moscow times is ok and not too alarming. It is also not discrediting the lancet
article. Just raising concerns.
Dr. Quack? CDC's Redfield Claims Masks "Guaranteed To Protect Against COVID" by
Tyler Durden Thu,
09/17/2020 - 14:09 Twitter
Facebook Reddit Email Print
Authored by Jordan
Schachtel via The Mass Illusion,
In February, Redfield said healthy people should *not* wear masks.
https://platform.twitter.com/embed/index.html?dnt=false&embedId=twitter-widget-0&frame=false&hideCard=false&hideThread=false&id=1306270050261831683&lang=en&origin=https%3A%2F%2Fwww.zerohedge.com%2Fmedical%2Fdr-quack-cdcs-redfield-claims-masks-guaranteed-protect-against-covid&siteScreenName=zerohedge&theme=light&widgetsVersion=219d021%3A1598982042171&width=550px
Testifying before the Senate Appropriations Committee Wednesday morning, CDC Director Robert
Redfield entered further into quack doctor territory, claiming that wearing a mask protects the
wearer against the novel coronavirus, even more so than a high-efficacy vaccine.
"These facemasks are the important, powerful public health tool we have," Redfield said,
while touching both sides of his mask and unconsciously contaminating it with his hands. "I
might even go so far as to say that this facemask is more guaranteed to protect me against
COVID than when I take a COVID vaccine," he added.
https://platform.twitter.com/embed/index.html?dnt=false&embedId=twitter-widget-1&frame=false&hideCard=false&hideThread=false&id=1306274937456529415&lang=en&origin=https%3A%2F%2Fwww.zerohedge.com%2Fmedical%2Fdr-quack-cdcs-redfield-claims-masks-guaranteed-protect-against-covid&siteScreenName=zerohedge&theme=light&widgetsVersion=219d021%3A1598982042171&width=550px
This appears to be another "scientific" evolution on masks from the "public health expert"
class. At first, we were advised not to wear masks. Then, the "my mask protects you. Your mask
protects me" mantra became the widely disseminated narrative. Now, masks apparently have the
incredible power of protecting the mask wearer from the virus.
https://platform.twitter.com/embed/index.html?dnt=false&embedId=twitter-widget-2&frame=false&hideCard=false&hideThread=false&id=1306265374367850497&lang=en&origin=https%3A%2F%2Fwww.zerohedge.com%2Fmedical%2Fdr-quack-cdcs-redfield-claims-masks-guaranteed-protect-against-covid&siteScreenName=zerohedge&theme=light&widgetsVersion=219d021%3A1598982042171&width=550px
me title=
In February, Redfield said the exact opposite about masks.
https://platform.twitter.com/embed/index.html?dnt=false&embedId=twitter-widget-3&frame=false&hideCard=false&hideThread=false&id=1306290933596553217&lang=en&origin=https%3A%2F%2Fwww.zerohedge.com%2Fmedical%2Fdr-quack-cdcs-redfield-claims-masks-guaranteed-protect-against-covid&siteScreenName=zerohedge&theme=light&widgetsVersion=219d021%3A1598982042171&width=550px
In the February hearing, Redfield told Americans not to buy medical-grade
masks , saying there's "no role for these masks in the community."
There remains zero evidence that cloth masks or the earloop masks displayed by Redfield
helps to slow the spread of COVID-19 or protect the wearer from infection. No country in the
world has proven a link in slowing or stopping the spread due to mask wearing mandates, which
are in effect in countless nations.
Given the lack of demonstrated evidence supporting it, mask-wearing has become a cult-like religious
movement in the United States , one that relies on complete subservience to total
mysticism. Members of the mask movement frequently target Americans who engage in
non-compliance, likening these individuals to evil, plague-carrying menaces. Redfield's
testimony will only add fuel to the mask mania that is sowing discord in America.
In his testimony, Redfield added that a COVID vaccine probably won't be available to the
general public until
at least the second or third quarter of 2021.
"If you're asking me when is it going to be generally available to the American public, so
we can begin to take advantage of vaccine to get back to our regular life, I think we're
probably looking at third, late second quarter, third quarter 2021," he testified, adding
that first responders may have access to the vaccine before the end of the year.
Like many institutional bureaucracies in the federal government, the CDC has become plagued
with corruption and "woke" politics. A whistleblower recently revealed that the CDC was forcing
its staff to undergo "critical race theory" training.
https://platform.twitter.com/embed/index.html?dnt=false&embedId=twitter-widget-4&frame=false&hideCard=false&hideThread=false&id=1305619445520318465&lang=en&origin=https%3A%2F%2Fwww.zerohedge.com%2Fmedical%2Fdr-quack-cdcs-redfield-claims-masks-guaranteed-protect-against-covid&siteScreenName=zerohedge&theme=light&widgetsVersion=219d021%3A1598982042171&width=550px
NEVER MISS THE NEWS THAT MATTERS MOST
ZEROHEDGE DIRECTLY TO YOUR INBOX
Receive a daily recap featuring a curated list of must-read stories.
Under Redfield's leadership, the CDC dropped the ball on preparing Americans for the U.S.
coronavirus outbreak, as shown through
internal emails displaying the bureaucracy as an organizational mess.
* * *
Thanks for reading! I would be honored if you are willing to support my work and subscribe to The Mass
Illusion, my newsletter for people concerned about our "new normal."
Coronavirus measures more divisive for UK than Brexit � poll
11 Sep, 2020 10:06
Get short URL
People take part in a demonstration against the lockdown and
the use of face masks in London. � Reuters / Henry Nicholls
14
Follow RT on
"Social fractures" provoked by measures to stop the spread of the coronavirus in the UK have turned out to be deeper than
those triggered by Brexit, a think tank warned after polling thousands of people.
Around 68 percent of those
who abide by the lockdown rules have
"strong negative views"
about people who
violate the restrictions, the survey by the think tank Demos revealed.
The same goes for face
masks, with 58 percent of respondents who use protective gear saying they have
"severely
negative attitudes towards non-mask wearers."
The online survey took
place between July 31 and August 7, with 10,061 people taking part.
https://platform.twitter.com/embed/index.html?creatorScreenName=RT_com&dnt=false&embedId=twitter-widget-0&frame=false&hideCard=false&hideThread=false&id=1304344097357004801&lang=en&origin=https%3A%2F%2Fwww.rt.com%2Fuk%2F500445-uk-divide-coronavirus-brexit%2F&siteScreenName=RT_com&theme=light&widgetsVersion=219d021%3A1598982042171&width=550px
The think tank pointed out
that the Covid-19 measures have been even more divisive for the country that the referendum on Britain's future in the EU in
2016.
Only 33 percent of 'No'
voters said that they
"resent, hate, or think people who voted for Brexit are bad
people."
And the 'Yes' voters were even more positive, as only 20 percent of them had negative feelings about the 'Remainers',
according to the survey.
Demos chief executive
Polly Mackenzie said she was
"deeply worried"
by the results of the study, telling
the Mirror that there is
"the urgent need for us to come together and have a national
conversation about the future, before the divisions become too entrenched."
ALSO ON RT.COM
The
UK government's new Covid rules are authoritarian and arbitrary. How much longer will people put up with this?
The UK was severely hit by the coronavirus, already recording more than 358,000 cases of the disease and over 41,600 deaths.
A strict lockdown was
introduced in Britain in the spring to curb the spread of the virus. Despite the easing of restrictions over the past month,
most of the measures still remain in place. Mask wearing is also obligatory on public transportation and in shops, with repeat
violators facing a fine of up to �3,200 (around $4,090).
Hilarous
2 hours ago
Fear is arguably not the best advisor but useful to control and manipulate, and influence the political
landscape.
Reply
6
Gliserman
2 hours ago
Who decides what risks we are all allowed to take and what is considered a serious risk? It would be good if
the government guided us to healthy practices to resist the virus. Maybe a stipend for people to buy healthy
food and herbs and preemptive remedies. Hiding from the virus is not fighting it. Of course one wonders
about the health risk of wearing a mask and being isolated and stressed all day. Evolution has given us an
immune system. That is the PPE that needs all our attention and support. Masks optional. When you put a mask
on you are saying, "I am most likely diseased and I must protect my fellow man from --- me."
Reply
4
ClairvoyantHW
Gliserman
1 hour ago
I think maybe there are many people with a hidden alcohol problem. They say they keep distance for others
protection, but the true purpose is to gain the freedom to drink while at work or in public. Even If you
smell alcohol they can Just pretend its something they used for desinfection. Some people with bad
drinking habbits cling to it, despite it being proven useless because it proved effective as cover up.
They should be encouraged to admit to their Problem and seek help.
Reply
1
PeterTosh1
Gliserman
2 hours ago
The virus is completely new. There are no known healthy practices to resist the virus. The only good
practice is to avoid the virus completely. Evolution has taken 10s of thousands of years to get us to
where we are now, we won't be immune to this virus from one day to the next. Even if you have had it once
or twice you may get it a third time. Wearing masks and being isolated all day are apparently all that
can help you until a more permanent solution is in place. Yes, we must assume that we and all around us
can possibly be infected and so we should protect each other: us from them and them from us. This is
simple respect. Personally, I don't believe the risk is worth all this but so it is.
Reply
2
5
Show 2 more replies
Redtom799
3 hours ago
The solution is shaking yourself from this media/Gov induced fear. They have behavioural scientists talking
about health issues does that give you a clue. Viruses are everywhere. 10,000 ,000 viruses in a drop of
seawater. "
I'll never swim in the ocean again"
,
ahhhhh! lol.
There needs to be grown up
conversation about life and death and how everything has to be weighed up and put in perspective. Life is
for the living and then we all die regardless.
Reply
13
WakeUpGoyim
Redtom799
2 hours ago
You are 100% correct
Reply
4
1
PeterTosh1
Redtom799
2 hours ago
I think you are not wrong but are exagerating a bit too. Governemtns are definitely playing with us,
especially now threatening us with a "second wave". I do think that lives are important though. I have
this argument regularly with some of my best friends who are actually very narcistic. Over here, almost
all COVID19 deaths are people who are elderly and already terminally ill. All the same, the loss of life
was calculated to be an average of 10 years per death. 10 years is a good deal of time if you ask me.
Reply
3
2
Show 1 more replies
Greenbogie
4 hours ago
So what is the solution,a referendum on wearing masks or not. If you break a speed limit you get
fined,whether you agree with speed limits or not, what is the difference. Fines that hurt if more than once.
Reply
2
8
Show 2 previous replies
Keith Christian
Greenbogie
1 hour ago
I don't need to participate in a referendum to choose...... (A) breathing and relying on my own immune
system (B) A fashion Muzzle.
Reply
1
PeterTosh1
Greenbogie
2 hours ago
I believe that the solution is different for different countries. It has to be looked at in context. In
many 3rd world countries the restrictions cause more damage than the virus. In first world countries I
suppose it depends alot on culture, education and other social factors. The swedish approach turned out
to be quite effective but at a high cost of lives. The New Zealand approach has overshot the goal
somewhat. The american approach turned into absolute chaos and disaster. The UK is healthy mixture of
cultures and needs to find it's own solution.
Reply
1
1
Show 1 more replies
WakeUpGoyim
2 hours ago
Thats the whole point. Because when they bungle brexit, they have a scapegoat. They can blame it on virus
and not their failures right from the start of joining the EU in the first place. Why did they not have a
vote to join but needed a vote to exit? Elites using the sheeple as play stations
Reply
2
Simela1987
1 hour ago
"A strict lockdown was introduced in Britain in the spring to curb the spread of the virus. No, it was
introduced because of a half a million dead lie from Neil Ferguson. Sweden, Denmark never had any lockdown,
they didn't destroy their economy thank you very much so why is the lockdown still in place to begin with!?
Reply
3
1
rinoflow32
57 minutes ago
lol '...come together and have a conversation.' You're either a statist or you love freedom. The statists
want all freedoms removed because they are half humans. Maybe only a quarter or a fifth. There is no
possible compromise. Freedom lovers must win this fight or it's game over.
Reply
1
Deejer
18 minutes ago
This shouldn't be a surprise given the SAGE group advised using incentivisation and coercion to achieve
exactly this sort of disapproval. What could possibly go wrong?
Reply
eff_this
19 minutes ago
I too have severely negative attitudes to those wed to the panic, I mean mask wearers.
Reply
1
WakeUpGoyim
2 hours ago
They can blame it on this thing, when their BREXIT failes. They will have 2 scapegoats - the whites for
rioting & this breakout - why was no vote required to join the EU nor the people asked if the nation should
but a vote required to exit?
Highly recommended !From comments: "Article is poorly written by someone who does not know medical science. There
are no viral "cells" so the headline is a put off right away. The comment about "sensitivity" is
misplaced as PCR tests are too sensitive: ergo false positives. I believe "specificity" is the
word the author was searching for. If a test lumps true positives with false positives, then it
lacks specificity."
In the past, our reports raising questions about the accuracy of COVID-19 tests have been
met with accusations of
'fearmongering' and
spreading 'misinformation'.
But not today.
That's because new research from the University of Oxford's Center for Evidence-Based
Medicine and the University of the West of England has found that the swab-based technique used
for most COVID-19 testing is at risk of returning "false positives" since copies of the virus's
RNA detected by the tests might simply be dead, inactive material from a weeks-old infection.
Although patients infected with COVID-19 are typically only infectious for a week or less,
tests can be triggered by virus genetic material left over from a weeks-old infection.
The team's research involved analyzing 25 studies on the widely used polymerase chain
reaction test. PCR tests use material collected with a swab - the most common type of test
around the world, and especially in the US - then utilize a "genetic photocopying" technique
that allows scientists to magnify the small sample of genetic material collected, which they
can then analyze for signs of viral RNA.
What the researchers here have effectively found is that these PCR tests just aren't
sensitive enough to distinguish if the viral material is active and infectious, or dead and
inert.
For those who desire a more comprehensive understanding of how these tests work, the chart
below can be helpful.
Professor Carl Heneghan, one of the authors of the study, said there was a risk that a surge
in testing across the UK was increasing the risk of this sample contamination occurring and it
may explain why the number of Covid-19 cases is rising but the number of deaths is static.
"Evidence is mounting that a good proportion of 'new' mild cases and people re-testing
positives after quarantine or discharge from hospital are not infectious, but are simply
clearing harmless virus particles which their immune system has efficiently dealt with," he
told the Spectator.
Professor Heneghan added that international scrutiny might be required to avoid "the dangers
of isolating non-infectious people or whole communities." ZKnight 14 minutes ago
Fake science. How about purify the virus first and establish a gold standard for testing
first. No, of course not because the CDC has a patent for Covid-19 and nobody is allowed to try
find it to see if it exists. play_arrow LogicFusion 27 minutes ago
Everybody is a Covid-19 / Coronavirus expert now!
Read about the failed coin dealer and convicted felon's performance. It's hilarious!
Martin
Armstrong becomes Covid-19 Coronavirus Expert overnight play_arrow ducksinarow 59 minutes
ago
Covid -19 has been so politicized that I don't believe a word of any publication for or
against testing, existence of the Virus, or anything that provokes testing or issues opinions
about locking down communities. Just like the riots, Covid news is just plain boring.
play_arrow ominous 3 hours ago
Link to spectator.co.uk goes to home
page, not this story.
Where is the original story posted? play_arrow play_arrow ominous 3 hours ago (Edited)
Perhaps this
https://www.cebm.net/covid-19/infectious-positive-pcr-test-result-covid-19/
y_arrow 1 Rabbi Blitzstein 38 minutes ago
"Give me control of a nation's money, and I care not who makes the laws" - Mayer Amschel
Rothschild. play_arrow play_arrow tangent 4 hours ago remove link
People who recommend a vaccine for an entirely cured virus should lose their license to
practice medicine. 99.9% cure rate applying to people who take it before being hospitalized is
one of the biggest success stories in the history of medicine for HCQ. Not only that, but there
are multiple other likely cures that simply have not been studied well. You'd think people
would appreciate the fact that the common cold has been cured, but instead they just whine that
big pharma isn't getting those bucko bucks.
I honestly expected a ticker tape parade like in the movies when that first cure study came
out. But instead they took a massive **** on the study and on the doctor... ****ty world we
live in. ay_arrow Pair Of Dimes Shift 2 hours ago
An exec (55+) at my company is gung ho about the vaccine.
Unfortunately, I just had to give him a "wait and see" response although I know vaccines for
coronaviruses are impossible. play_arrow 2 play_arrow ThanksIwillHaveAnother 4 hours ago
(Edited)
Viruses are not full cells. They are DNA/RNA wrapped with a protein the clings to a cell
then the cell imports the DNA/RNA to start making its proteins. So what is inactive? If that
person sneezes on another person depending on immune system status that other person could get
a bad infection. y_arrow 4 CrabbyR 3 hours ago
viruses utilizes CELL structures and host DNA to replicate dna or rna according to the
viruses genetic code, the protein jacket is the final product to
disguise the virus from detection and to bind on another cell after the compromised cell
RUPTURES, there's more to it but if it cannot copy itself effectively it can become nonviable
and unable to infect another cell. It replicates DNA inside a host cell, It is not a complete
organism and cannot replicate unless it can inject its DNA into a host cell. Antibodies cling
to viruses and destroy this ability to bind to a target cell. A non viable virus has a damaged
coat or DNA RNA that has to many Dimers (damage or code breaks) Bacteria is more in line with
what you think a virus is y_arrow onewayticket2 4 hours ago (Edited) remove link
they lost me when they changed the definition of "death" to include "presumed, untested"
cases (while bI@#$% ing at me that we needed to "follow the science")....and even got busted
for the laughable motorcycle accident being classified as a covid death and the Labs that were
sending in 100% positive results. (until they were caught) play_arrow OutaTime43 4 hours ago
remove link
The test detects RNA. Not necessarily viable virus. Also, it will detect RNA presence in an
individual who may already have antibodies and may be immune. We are bombarded daily by viruses
of which we already have immunity. play_arrow sun tzu 10 hours ago
Shocking news that the South Koreans already discovered and published back in May. Western
big pharma driven medicine is garbage 😂😂😂
https://www.cidrap.umn.edu/news-perspective/2020/05/wha-passes-pandemic-probe-resolution-korea-clarifies-reinfection-reports
play_arrow
Roger Casement 10 hours ago
WTF!!!!
World Bank exporting COVID-19 Testing Kits in 2018??????
https: //
wits.worldbank.org/trade/comtrade/en/country/ALL/year/2018/tradeflow/Exports/partner/WLD/nomen/h5/product/300215
play_arrow 7 play_arrow sun tzu 10 hours ago
Interesting play_arrow play_arrow Jack Mehoff 1 more time 9 hours ago
Business as usual play_arrow play_arrow Argon1 7 hours ago
Preparation for agenda 2021 in 2017. play_arrow 1 play_arrow CrabbyR 4 hours ago
WOW.......ties a few strands from other sources together into a real ugly picture play_arrow
play_arrow Welsh Bard 10 hours ago
The professor who won the Nobel prize for work in this field, said that the way this test is
being operated with over forty cycles, means that any results are entirely meaningless.
In Britain, having spent over £15 billion setting up PCR testing systems and a shaky
test and trace apparatus on top of that, it appears that 90% of positive results now appear to
be false. This is compounded by the fact that when a hot spot develops, more testing is done to
show a rapid increase in more false positive results, meaning further new lockdowns and even
more testing to prove yet more false positive results ad infinitum.
Now whether this is by design or ineptitude, people must decide for themselves but the
outcome is utter chaos.
For those countries who have not followed the Swedish model especially countries like
Australia and New Zealand who have set up complete isolation, now face a future perpetually cut
off from the rest of the world.
Okay, new techniques will and are coming along to treat the disease like HCQ when used
correctly maybe as a prophylactic and a vaccine that will need to be constantly upgraded like
the Flu vaccine, means that the whole world has painted itself into a corner unless drastic
revision is now made to the whole sorry mess.
In the meantime, we will now be stuck with digital currency and the introduction of ID
Health Cards that will limit people in how they travel where they work and access to a whole
heap of things like government services.
Welcome to the new world order! play_arrow 1 KuriousKat 11 hours ago (Edited) remove
link
Don't tell the Shameless Aussie gov that after arresting hundreds for simply voicing doubt
on need to lockdown entire city...Next time it will be thousands and not a damn thing they can
do to stop it..These people are trickling us the truth how worthless the tests are when pretty
much everyone knows. play_arrow espirit 12 hours ago remove link
Lessee.
WHO
Imperial College
John Hopkins
CDC
Line all those peeps up against the wall, and the first one to rat gets to live.
I'll provide my own ammo... ay_arrow Sick Monkey 6 hours ago
Not everyone working in these agencies are dishonest but like you and I we have to work and
eat.
Most of them are trapped in this mess with bills to pay threatened by NDA.
Not particularly new news. Been talked about since April at least -- it's an RNA virus, it
has its own polymerase, and it leaves lots of RNA fragments in its wake.
The Corona family of viruses make 5 or 6 strands with partial copies of their RNA molecule.
negative copies are made first, and then copied again into positive copies. Finally the one big
RNA is made with the entire genome on it.
So about a dozen RNA molecules are made for each finished virus particle that is produced.
And finally, a variety of different primers are used for the PCR tests, some are matched to the
small partial RNA copies and others are matched to various features on the large whole-virus
RNA. They can give different results for the same sample.
So, someone who registers on a PCR test has probably been exposed to the virus, but the test
gives no clue as to whether it is an active infection, or the person is contagious, or they are
just coming down with it, or they got over it six months ago. play_arrow 4 play_arrow 1
10 play_arrow gordo 12 hours ago remove link
Sweden, no masks, no lock downs, ALL SCHOOLS OPEN, herd immunity, no second wave.
Still think your masks and lock downs are working muppets?
https://youtu.be/sjYvitCeMPc
SARS-CoV2 and the Rise of Medical Technocracy. Lee Merritt, M.D. play_arrow 3 play_arrow
hugin-o-munin 13 hours ago
I'm glad to see that many are starting to counter the official narrative.
We've been asleep for too long and allowed these agendas to fester to the point we're at now
where a college dropout software salesman and a former 3rd world communist terrorist (neither
of whom have any medical degree) are dictating to the world how everyone needs to get a DNA
altering vaccine and a medical ID. It's completely nuts and bonkers yet more or less the entire
planet's governments follow in 'lockstep' with ever more draconian laws and regulations
incarcerating people in their own homes, making them wear masks causing oxygen deprivation and
shutting down the entire world economy.
lay_arrow Warthog777 , 13 hours ago
Article is poorly written by someone who does not know medical science. There are no viral
"cells" so the headline is a put off right away. The comment about "sensitivity" is misplaced
as PCR tests are too sensitive: ergo false positives. I believe "specificity" is the word the
author was searching for. If a test lumps true positives with false positives, then it lacks
specificity.
Cabreado , 13 hours ago
"accusations of
'fearmongering' and
spreading 'misinformation'.
Well, much of the world has known for months now about the testing lies...
and I'd be remiss to not remind the Tylers that they indeed played a role in the fear
mongering along the way; quite intently so.
Crush the cube , 13 hours ago
https://play.google.com/store/books/details/Flavio_Bell_Covid_24?id=SxrxDwAAQBAJ
Busted, published 2018, what a scam.
Digital-Anarchy , 14 hours ago
Anyone who would use the term "virus cells", has no clue what they're talking about and
should be completely disregarded. Viruses are not cells. PCR tests are searching for
something your body produces in response to a virus as well. They are not produced
specifically for a singular virus either. The entire concept of PCR testing is garbage. This
**** was a scam from the get-go.
hugin-o-munin , 13 hours ago
Yes it is evident now that this entire pandemic is false and political. The goal seems to
be to vaccinate entire populations and the question people need to ask is - why? what for?
Aside from the obvious economic motives there are some more sinister plans that most people
will have a hard time accepting but these need to be looked at. Several years ago there were
a group of doctors and researchers that died of suspicious suicides who were collaborating
and studying vaccines and the link to autism.
The effort was led by Dr.Jeffrey Bradstreet who was researching the natural substance
GcMAF and how this could boost the immune system. What he discovered was that many vaccines
had a compound/substance called Nagalase in them that is unnatural and has a detrimental
effect on the immune system and function of GcMAF (which is produced by our own bodies) and
has no business at all being in vaccines. Just before he was able to blow the whistle on this
he also died of a suspicious 'suicide' and today most of the clinics and research groups
working on GcMAF have been destroyed and ruined. Draw your own conclusions.
snblitz , 14 hours ago
Dr. Kary Mullis invented the PCR test. He said it was ineffective for this purpose.
Though he was addressing its use in a prior virus hoax unleashed upon the world.
I bet you didn't know this scam has been used before.
That is why I was able to call out the scam right from the start. The second I saw them
using the PCR again, I knew it was from the same playbook.
snblitz , 14 hours ago
So many lies.
Viruses are not alive. They have no metabolic functions. They cannot move.
Don't believe me? Get a degree is virology or microbiology or just a read a book on the
subject. Or capture a wuhan-virus yourself and watch it under a microscope. It won't move. It
won't consume anything. It will just sit there inert.
The problem is that you are being lied to at a scale you cannot imagine.
I know, off to the fema re-education camp for me for spreading false information about the
wuhan-virus.
Though I am not the one spreading fear and hysteria.
aldousd , 13 hours ago
There article is confused, but the work of the doctor is not. Viruses use your cells to
reproduce. When your immune system targets the virus it actually kills your own cell which
has become host to the virus. The virus particles and markers, and the DNA of the virus can
be detected in these dead cells, but dead cells cannot serve as a factory for more viruses.
So it's effectively a dead virus infected cell. Not a dead virus cell.
So while the transcription of the idea here was done by an idiot, it's not an idiotic
idea. The tests cannot tell if the virus came in a living cell that is actively producing
more viruses or a dead host cell that has been assassinated by your immune system. That's
what they're talking about here.
mstyle , 11 hours ago
what about the chromosome 8 stuff that has been mentioned lately?
(since you appear to be rather intelligent)
hugin-o-munin , 11 hours ago
Thanks. Well the chromosome 8 discovery in the PCR test specifications/details is strange
and worrying because it makes you wonder why it's part of this at all. Some believe it's to
get more false positive results while others believe it is what the mRNA vaccines are
intended to target and if that's right then it's really sinister. What exactly is the plan?
To make all of us get Downs Syndrome? I don't know but judging by all their other lies and
schemes it wouldn't surprise me.
IRC162 , 14 hours ago
Fuggin progressives and their pandemic political prop. But really this reaction is the
same as their reaction to 'racial injustice'. They focus on feelings before the facts are
known in order to achieve their end, and then do their best to bury/ignore the facts when
they are gathered later.
94% COVID deaths with multiple comorbidities.
10 unarmed blacks killed by police in 2019 (6 were in self-defense).
adr , 15 hours ago
Why didn't you mention that nearly all labs are running 35-40 cycles which guarantees a
positive test, simply from noise.
The inventor of the test said if you don't find anything after 15 cycles, it probably
isn't there. After 20 cycles the noise starts to be greater than any real information. By 30,
the test is mostly noise. More than 35, the test is completely worthless.
Of course I've been saying this for five months, but most people didn't listen. After the
NYT article came out, people I know started saying, "How did you know?"
I said, "Because I have critical thinking skills. Why didn't you believe me? Name a time
I've steered you wrong."
Antiduck , 14 hours ago
333 labs in florida had 100% positivity. (stupid word.)
ZenStick , 12 hours ago
Exactly correct.
Identify as Ferengi , 15 hours ago
See above, Born2Bwired.
The PCR test is not useful for what they are using it for apparently. This has been
known since the beginning. Here is quote regarding AIDS:
"Kary Mullis, who won the Nobel Prize in Science for inventing the PCR, is thoroughly
convinced that HIV is not the cause of "AIDS". With regard to the viral load tests, which
attempt to use PCR for counting viruses, Mullis has stated: "Quantitative PCR is an
oxymoron." PCR is intended to identify substances qualitatively, but by its very nature is
unsuited for estimating numbers. Although there is a common misimpression that the viral
load tests actually count the number of viruses in the blood, these tests cannot detect
free, infectious viruses at all; they can only detect proteins that are believed, in some
cases wrongly, to be unique to HIV. The tests can detect genetic sequences of viruses, but
not viruses themselves.
What PCR does is to select a genetic sequence and then amplify it enormously. It can
accomplish the equivalent of finding a needle in a haystack; it can amplify that needle
into a haystack. Like an electronically amplified antenna, PCR greatly amplifies the
signal, but it also greatly amplifies the noise. Since the amplification is exponential,
the slightest error in measurement, the slightest contamination, can result in errors of
many orders of magnitude."
http://www.virusmyth.org/aids/hiv/jlprotease.htm
naro , 15 hours ago
NYTimes article last week suggested that only 10% of Covid positive PCR tests are
clinically significant and infectious.
Neoliberal medicine puts stents in people hearts just for money. Why neoliberal medicine
should behave differently in case of COVID-19
naro , 15 hours ago
It is important to note that detecting viral material by PCR does not indicate that the
virus is fully intact and infectious, i.e. able to cause infection in other people. The
isolation of infectious virus from positive individuals requires virus culture methods. These
methods can only be conducted in laboratories with specialist containment facilities and are
time consuming and complex.
PCR is 90% false positive as far as detection of live infectious virus. IT IS A FRAUD
I Write Code , 15 hours ago
The "PCR" tests are only testing for fragments anyhow, if they did a full sequence it
would be much more reliable - but much more slow and expensive, too.
NumbNuts , 15 hours ago
These test kits?
COVID-19 Test kits (300215) exports by country in 2018
https://wits.worldbank.org/trade/comtrade/en/country/ALL/year/2018/tradeflow/Exports/partner/WLD/nomen/h5/product/300215
4Celts , 14 hours ago
I saw this on RFB an hour ago . He showed how a link on this page had been scrubbed
already .
adr , 15 hours ago
Why didn't you mention that nearly all labs are running 35-40 cycles which guarantees a
positive test, simply from noise.
The inventor of the test said if you don't find anything after 15 cycles, it probably
isn't there. After 20 cycles the noise starts to be greater than any real information. By 30,
the test is mostly noise. More than 35, the test is completely worthless.
Of course I've been saying this for five months, but most people didn't listen. After the
NYT article came out, people I know started saying, "How did you know?"
I said, "Because I have critical thinking skills. Why didn't you believe me? Name a time
I've steered you wrong."
Spiritual Anunnaki , 15 hours ago
Wrote a memoir of a incubation patient. The coronavirus Hospital staff are pressured to
hook you up to the tubes...
adr , 15 hours ago
If you walked into a hospital coughing, they gave you paralytics and hooked you up to a
vent. Something that is only supposed to be done if you are in imminent danger of death.
The problem with paralytics, is that your body believes it is dead, and your blood starts
to coagulate. It wasn't Covid that caused the problems, it was the drugs the doctors were
forcing down patient's throats.
They should be held criminally libel, but thanks to the emergency declaration, they are
immune to prosecution.
flim_flam_man , 11 hours ago
They wanted them intubated for two reasons: nurses didn't want to deal with patients on
bipaps and other respiratory support in a conscious patient as that increases THEIR risk of
infection. AND the hospitals collected $38K/intubated patient from the fed...significantly
more than a garden variety mildly sick patient.
This went on mainly in hospitals in crappy areas that largely serve the "socioeconomically
challenged" segment of the population, which then solves the mystery as to why blacks and
hispanics have been disproportionately affected by covid.
Some
of the Gilead Remdesivir Results from Recent Studies
run75441 | August 24, 2020 9:00 pm
HEALTHCARE HOT TOPICS POLITICS Effect of
Remdesivir vs Standard Care on Clinical Status at 11 Days in Patients With Moderate
COVID-19 A Randomized Clinical Trial , JAMA, Christoph D. Spinner, MD ; Robert L. Gottlieb, MD,
PhD ; Gerard J. Criner, MD, August 21, 2020
This is a freebie so you should be able to get into this article and pickup on additional
detail. Those who were treated early on had a better result from remdesivir than those who were
treated later after contracting Covid. This was already know,.
Results: Among 596 patients who were randomized, 584 began the study and received remdesivir
or continued standard care (median age, 57 [interquartile range, 46-66] years; 227 [39%] women;
56% had cardiovascular disease, 42% hypertension, and 40% diabetes), and 533 (91%) completed
the trial. Median length of treatment was 5 days for patients in the 5-day remdesivir group and
6 days for patients in the 10-day remdesivir group.
On day 11, patients in the 5-day remdesivir group had statistically significantly higher
odds of a better clinical status distribution than those receiving standard care (odds
ratio, 1.65; 95% CI, 1.09-2.48; P = .02).
The clinical status distribution on day 11 between the 10-day remdesivir and standard care
groups was not significantly different ( P = .18 by Wilcoxon rank sum
test). By day 28, 9 patients had died: 2 (1%) in the 5-day remdesivir group, 3 (2%) in the
10-day remdesivir group, and 4 (2%) in the standard care group. Nausea (10% vs 3%), hypokalemia
(6% vs 2%), and headache (5% vs 3%) were more frequent among remdesivir-treated patients
compared with standard care.
Some Limitations: This study has several limitations. First, the original protocol was
written when COVID-19 cases were largely confined to Asia and the clinical understanding of
disease was limited to case series. This led to a change in the primary end point on the first
day of study enrollment as it became clear that hospital discharge rates varied greatly across
regions and the ordinal scale had become standard for interventional COVID-19 studies. Second,
the study used an open-label design, which potentially led to biases in patient care and
reporting of data. Third, because of the urgent circumstances in which the study was conducted,
virologic outcomes such as effect of remdesivir on SARS-CoV-2 viral load were not assessed.
Fourth, other laboratory parameters that may have aided in identifying additional predictors of
outcomes were not routinely collected. Fifth, the ordinal scale used to evaluate outcomes was
not ideal for detecting differences in patients with moderate COVID-19, especially for a
clinical situation in which discharge decisions may be driven by factors other than clinical
improvement.
Conclusions: Among patients with moderate COVID-19, those randomized to a
10-day course of remdesivir did not have a statistically significant difference in clinical
status compared with standard care at 11 days after initiation of treatment. Patients
randomized to a 5-day course of remdesivir had a statistically significant difference in
clinical status compared with standard care, but the difference was of uncertain clinical
importance.
Oui
95
The Unraveling of America
https://www.rollingstone.com/politics/political-commentary/covid-19-end-of-american-era-wade-davis-1038206/
Anthropologist Wade Davis on how COVID-19 signals the end of the American era
Food for thought ... 😉. Well written ...
Odious as he may be, Trump is less the cause of America's decline than a product of its
descent. As they stare into the mirror and perceive only the myth of their exceptionalism,
Americans remain almost bizarrely incapable of seeing what has actually become of their
country.
>
Very
informative
5.0 out of 5 stars
Very
informative
Reviewed in the United States on April 18, 2020
Verified Purchase
Update: I'm just about done reading this book. Here's a quotation:
P 278. "When scientific research interferes with politics, economics, or culture, science is most often the loser. Thus,
governments and businesses control health care for personal gains or concepts and disregard or avoid factual knowledge
and events." Sound familiar? This was written ten years ago. I understand that the last thing many people want is more
virus talk, but this book is very informative and may effect many of your actions. It also provides a long view on
identifying and treating viruses. For example, I didn't know that it took over forty years for an effective polio
vaccine. Same thing for measles.
This is from Jan 2020, but still interesting
While experts across the world search for a vaccine to tackle the dangerous new infection,
Russian health bosses have identified a trio of existing medicines to combat 2019-nCoV in
adults.
The new coronavirus can be fought with ribavirin, lopinavir/ritonavir and interferon
beta-1b, they believe. These drugs are typically used to treat hepatitis C, HIV and multiple
sclerosis respectively.
The Ministry of Health advisory not only offers recommendations, but also describes how the
treatments work and in what quantities they should be prescribed. The guidelines are intended
for doctors in hospitals throughout the country.
... ... ...
One of the drugs recommended, ribavirin, was used in the treatment of the 2003 Chinese SARS
outbreak, which infected over 8,000 people and killed 774 across 17 different countries. The
new coronavirus has shown a sizeable genetic similarity with SARS, with one sequence comparison
showing a match of 79.5%.
The ministry also instructs that, in order to prevent and reduce the severity of symptoms,
medication should be consumed within two days of contact with an infected person. Their
prevention recommendations also include sanitary and hygiene rules, such as handwashing and
wearing protective masks.
Authored
by Sarah Varney via Kaiser Health News,
As scientists race to develop a COVID-19 vaccine, experts say obesity could prove an
impediment -- a sobering prospect for a nation in which nearly half of all adults are
obese.
For a world crippled by the coronavirus, salvation hinges on a vaccine.
But in the United States, where at least 4.6 million people have been infected and nearly
155,000 have died, the promise of that vaccine is hampered by a vexing epidemic that long
preceded COVID-19: obesity.
Scientists know that vaccines engineered to protect the public from influenza, hepatitis B,
tetanus and rabies can be less effective in obese adults than in the general population,
leaving them more vulnerable to infection and illness. There is little reason to believe,
obesity researchers say, that COVID-19 vaccines will be any different.
"Will we have a COVID vaccine next year tailored to the obese? No way," said Raz Shaikh,
an associate professor of nutrition at the University of North Carolina-Chapel Hill.
"Will it still work in the obese? Our prediction is no."
More than 107 million American adults are obese, and their ability to return safely to work,
care for their families and resume daily life could be curtailed if the coronavirus vaccine
delivers weak immunity for them.
In March, still early in the global pandemic, a little-noticed study from China found that
heavier Chinese patients afflicted with COVID-19 were more likely to die than leaner ones,
suggesting a perilous future awaited the U.S., whose population is among the heaviest in the
world.
And then that future arrived.
about:blank
about:blank
me title=
As intensive care units in New York, New Jersey and elsewhere filled with patients, the
federal Centers for Disease Control and Prevention warned that obese people with a body mass
index of 40 or more -- known as morbid obesity or about 100 pounds overweight -- were among the
groups at highest risk of becoming severely ill with COVID-19. About 9% of American adults are
in that category.
As weeks passed and a clearer picture of who was being hospitalized came into focus, federal
health officials expanded their warning to include people with a body mass index of
30 or more. That vastly expanded the ranks of those considered vulnerable to the most
severe cases of infection, to 42.4% of American adults.
Obesity has long been known to be a significant risk factor for death from cardiovascular
disease and cancer. But scientists in the emerging field of immunometabolism are finding
obesity also interferes with the body's immune response, putting obese people at greater risk
of infection from pathogens such as influenza and the novel coronavirus. In the case of
influenza, obesity has emerged as a factor making it more difficult to vaccinate adults against
infection. The question is whether that will hold true for COVID-19.
A healthy immune system turns inflammation on and off as needed, calling on white blood
cells and sending out proteins to fight infection. Vaccines harness that inflammatory response.
But blood tests show that obese people and people with related metabolic risk factors such as
high blood pressure and elevated blood sugar levels experience a state of chronic mild
inflammation ; the inflammation turns on and stays on.
Adipose tissue -- or fat -- in the belly, the liver and other organs is not inert; it
contains specialized cells that send out molecules, like the hormone leptin, that scientists
suspect induces this chronic state of inflammation. While the exact biological mechanisms are
still being investigated, chronic inflammation seems to interfere with the immune response to
vaccines, possibly subjecting obese people to preventable illnesses even after vaccination.
An effective vaccine fuels a controlled burn inside the body, searing into cellular memory a
mock invasion that never truly happened.
Evidence that obese people have a blunted response to common vaccines was first observed in
1985 when obese hospital employees who received the hepatitis B vaccine showed a significant
decline in protection 11 months later that was not observed in non-obese employees. The finding
was replicated in a follow-up study that used longer needles to ensure the vaccine was injected
into muscle and not fat.
Researchers found similar problems with the hepatitis A vaccine, and other studies have
found significant declines in the antibody protection induced by tetanus and rabies vaccines in
obese people.
"Obesity is a serious global problem, and the suboptimal vaccine-induced immune responses
observed in the obese population cannot be ignored," pleaded researchers from the Mayo
Clinic's Vaccine Research Group in a 2015 study published in the journal Vaccine.
Vaccines also are known to be less effective in older adults, which is why those 65 and
older receive a supercharged annual influenza vaccine that contains far more flu virus antigens
to help juice up their immune response.
By contrast, the diminished protection of the obese population -- both adults and children
-- has been largely ignored.
"I'm not entirely sure why vaccine efficacy in this population hasn't been more well
reported," said Catherine Andersen, an assistant professor of biology at Fairfield University
who studies obesity and metabolic diseases. "It's a missed opportunity for greater public
health intervention."
In 2017, scientists at UNC-Chapel Hill provided a critical clue about the limitations of the
influenza vaccine. In a paper published in the International
Journal of Obesity , they showed for the first time that vaccinated obese adults were twice
as likely as adults of a healthy weight to develop influenza or flu-like illness.
Curiously, they found that adults with obesity did produce a protective level of antibodies
to the influenza vaccine, but they still responded poorly.
NEVER MISS THE NEWS THAT
MATTERS MOST
ZEROHEDGE DIRECTLY TO YOUR INBOX
Receive a daily recap featuring a curated list of must-read stories.
"That was the mystery," said Chad Petit, an influenza virologist at the University of
Alabama.
One hypothesis, Petit said, is that obesity may trigger a metabolic dysregulation of T
cells, white blood cells critical to the immune response.
"It's not insurmountable," said Petit, who is researching COVID-19 in obese patients. "We
can design better vaccines that might overcome this discrepancy."
Historically, people with high BMIs often have been excluded from drug trials because they
frequently have related chronic conditions that might mask the results. The clinical trials
underway to test the safety and efficacy of a coronavirus vaccine do not have a BMI exclusion
and will include people with obesity, said Dr. Larry Corey, of the Fred Hutchinson Cancer
Research Center, who is overseeing the phase 3 trials sponsored by the National Institutes of
Health.
Although trial coordinators are not specifically focused on obesity as a potential
complication, Corey said, participants' BMI will be documented and results evaluated.
Dr. Timothy Garvey, an endocrinologist and director of diabetes research at the University
of Alabama, was among those who stressed that, despite the lingering questions, it is still
safer for obese people to get vaccinated than not.
"The influenza vaccine still works in patients with obesity, but just not as well," Garvey
said. "We still want them to get vaccinated."
This new
study detailed in the Journal of the American Medical Association (JAMA) on May 20,
discovered that the angiotensin-converting enzyme 2 (ACE2), which grows in abundance as the
individual grows, might be the reason that less than two percent of all individuals infected
with SARS-CoV-2 - the virus that causes the COVID-19 disease - are children.
Researchers had suspected that COVID-19 susceptibility could be linked to the amount of gene
expression of ACE2 seen in the nasal cavity, given that the
enzyme acts as a receptor to allow the SARS-CoV-2 virus to pass into the body.
To investigate this potential link, researchers looked for a relationship between the two -
the level of gene expression of ACE2 in the nose and COVID-19 infection - by taking nasal swabs
from 305 people involved in an asthma study . Researchers hypothesized that the lower the
levels of enzyme gene expression, the less likely it is a person will be infected by
COVID-19.
Researchers said they chose to swab the nose because it is one of the first access points
for SARS-CoV-2 to infect an individual.
Samples were taken from both asthmatic (49.8 percent) and non-asthmatic patients. The 305
people involved in the study were between four to 60 years of age.
Researchers said they found a clear association between ACE2 expression and age - opening up
a possible explanation as to why most children, who tend to have lower levels of enzyme
expression, are less susceptible to COVID-19.
NEVER MISS THE NEWS THAT MATTERS MOST
ZEROHEDGE DIRECTLY TO YOUR INBOX
Receive a daily recap featuring a curated list of must-read stories.
https://lockerdome.com/lad/13084989113709670?pubid=ld-dfp-ad-13084989113709670-0&pubo=https%3A%2F%2Fwww.zerohedge.com&rid=www.zerohedge.com&width=890
Supinda Bunyavanich, professor of Genetics and Genomic Sciences and Paediatrics at Mount
Sinai, said in a
press release that the study found "that there are low levels of ACE2 expression in the
nasal passages of younger children, and this ACE2 level increases with age into adulthood.
"This might explain why children have been largely spared in the pandemic," Bunyavanich
said.
Last week we warned
readers to be cautious about new COVID-19 vaccines, highlighting how key parts of the clinical
trials are being skipped as big pharma will not be held accountable for adverse side effects
for administering the experimental drugs.
A senior executive from AstraZeneca, Britain's second-largest drugmaker, told
Reuters that his company was just granted protection from all legal action if the company's
vaccine led to damaging side effects.
...
For more color on leading vaccines in development that produce "severe" side effects, read
our latest piece titled
"Moderna COVID-19 Vaccine Induced Adverse Reactions In "More Than Half" Of Trial
Participants."
Maybe these rushed vaccines are more for optics, get consumers back into airplanes, hotels,
resorts, and malls.
The major red flag is how governments are allowing big pharma to rush experimental vaccines,
with no legal recourse if something goes terribly wrong.
As the world awaits a COVID-19 vaccine, the next big advance in battling the pandemic could
come from a class of biotech therapies widely used against cancer and other disorders -
antibodies designed specifically to attack this new virus.
Last week we warned
readers to be cautious about new COVID-19 vaccines, highlighting how key parts of the clinical
trials are being skipped as big pharma will not be held accountable for adverse side effects
for administering the experimental drugs.
A senior executive from AstraZeneca, Britain's second-largest drugmaker, told
Reuters that his company was just granted protection from all legal action if the company's
vaccine led to damaging side effects.
Notable quotes:
"... And while being overweight does not seem to increase people's chances of contracting COVID-19 according to the study, it can affect the respiratory system, and potentially immune function as well. ..."
Just in case Americans - the most obese nation in the world - needed another reason to lose
some weight, here it is.
In what is emerging as a perfidious Catch 22, at a time when the US population is rapidly
gaining weight due to mandatory work from home regulation (hence the Covid 19 pounds ) as
described
here and
here , while a surge in domestic alcohol consumption is only making the matters
worse...
... Public Health England has published a
paper titled " Excess Weight and COVID-19 Insights from new evidence ", indicating that the
risks of hospitalization, intensive care treatment and death increase progressively with
increasing body mass index (BMI) above the healthy weight range even after adjustment for
potential confounding factors, including demographic and socioeconomic factors. In other words,
the fatter one is, the higher the risk that person may die from covid.
Some more details: according to the Public Health England paper, the hazard ratios of ICU
admission patients who are overweight (BMI ≥25-29.9), obese (BMI ≥30-34.9) or severely
obese (BMI ≥35) are 1.64, 2.59 and 4.35, respectively see figure below) relative to patients
with a BMI of ≥20-24.9.
And while being overweight does not seem to increase people's chances of contracting
COVID-19 according to the study, it can affect the respiratory system, and potentially immune
function as well.
And since no crisis will ever be put to waste by a nanny state which after the covid
pandemic will control virtually every aspect of our lives, the British government plans to
initiate an anti-obesity campaign including strict rules on how junk food is advertised and
sold in the UK.
Richard Steven Hack , Aug 1 2020 10:46 utc |
89
This book is likely required reading for those who have suffered from COVID-19. It's only
76 pages, but only costs $1.99 for the Kindle edition. I downloaded a copy from the Internet
and will tuck it away for when I'm unlucky (assuming I would live long enough to try
them.)
The Coronavirus Recovery Handbook: 19 Rehab Exercises for Mild to Severe Cases of
COVID-19 - Dr. Liu Xiaodan and Dr. Shan Chunlei and their colleagues at the Shanghai
Public Health Clinical Center and Lei Shenshan Hospital in Wuhan.
Russia's health minister is preparing a mass vaccination campaign against the novel
coronavirus for October, local news agencies reported on Saturday, after a vaccine completed
clinical trials.
Health Minister Mikhail Murashko said the Gamaleya Institute, a state research facility in
Moscow, had completed clinical trials of the vaccine and paperwork is being prepared to
register it, Interfax news agency reported.
He said doctors and teachers would be the first to be vaccinated.
Highly recommended !
monty42 , 2 hours ago
" We know that wearing a mask outside health care facilities offers little, if any,
protection from infection. Public health authorities define a significant exposure to
Covid-19 as face-to-face contact within 6 feet with a patient with symptomatic Covid-19 that
is sustained for at least a few minutes (and some say more than 10 minutes or even 30
minutes). The chance of catching Covid-19 from a passing interaction in a public space is
therefore minimal. In many cases, the desire for widespread masking is a reflexive reaction
to anxiety over the pandemic."
https://www.nejm.org/doi/full/10.1056/NEJMp2006372
Revisionist claims now- " In truth, the intent of our article was to push for more
masking, not less." "
The problem of false positives from Covid-19 tests means UK is inflating its numbers � and taking wrong decisions
Rob Lyons
Rob Lyons
is a UK journalist specialising in science, environmental and health issues. He is the author of '
Panic
on a Plate: How Society Developed an Eating Disorder'.
A sign is seen at a drive-through coronavirus disease
(COVID-19) testing facility in Hyde Park, following the outbreak of the coronavirus disease, London, Britain, June 11,
2020
When seven staff at a Scottish football club tested positive for coronavirus, alarm bells went off. But really alarming was
when six of those results turned out to be wrong. Such inaccurate tests are exaggerating the problem.
Last weekend, at very
short notice, the UK reintroduced quarantine measures for people arriving from Spain. For those already in Spain, or for whom
it was too late to postpone their trip, the decision is very inconvenient. For those who can't work at home when they return,
it may mean missing out on wages for the two weeks they will have to spend in isolation when they get back. But what if the
apparent rise in cases has been exaggerated by seemingly small flaws with testing?
The potential for problems
was illustrated by Scottish football team St Mirren last week. The club, based in Paisley, a town just west of Glasgow,
reported seven positive test results for Covid-19 among its staff. Alarm bells went off about what this might mean for the new
Scottish football season. But this
"cluster"
was a mirage. When the seven people
were re-tested using a more accurate method,
just
one
of them was found to be Covid-positive.
In Spain, half of the
reported
cases
have
been in people who had no symptoms. We know that many people who test positive never suffer any symptoms. But what if many of
these people don't have Covid-19 at all?
READ MORE
International
airline body slams UK's 'unilaterally decided blanket quarantine' on travellers from Spain
If that sounds
implausible, it's important to know that tests are not perfect. There are currently two kinds of tests to see if you have the
disease. One kind, the molecular real-time polymerase chain reaction (RT-PCR) test, looks for genetic material from the virus.
This kind seems to be very accurate, but it's expensive and time-consuming. The other kind, the antigen test, detects specific
proteins on the surface of the virus. This is quicker, easier and cheaper, but it's much less accurate. In developed
countries, RT-PCR testing is the norm, but poorer countries may have to make do with antigen testing.
The difficulty at the
moment is that there are relatively few cases of Covid-19 in the community, but more and more testing is being done. So even
if the RT-PCR test has a high
"specificity"
� that is, a tiny fraction of test
results are false positives � the number could actually be quite significant. For example, let's say that 99.9 percent of the
time, a test correctly identifies someone without the disease as negative. Just 0.1 percent of tests produce false positives.
Recently, in the UK, it
was estimated that 0.04 percent of people had the virus outside of care homes and hospitals. So, if we tested 10,000 people,
we should find four cases of Covid-19, on average. Of the 9,996 other people tested, in this hypothetical example, 0.1 percent
who don't have the virus would also test positive � that's 9.996 � in other words, 10 people. So, even if the test is very
accurate indeed, we could easily end up with four positive tests from people who really do have the virus and 10 false
positives from people who don't.
For any particular
individual, the chances of the test being a false positive is small. But when we look at the big picture, we could easily be
fooled into thinking that there are many more cases than there really are. Indeed, with a test accuracy of 99.9 percent, if
you tested a million people, none of whom actually had the disease, you would produce 1,000 positive results. And for tests
with less accuracy � as with St Mirren FC � the situation could be even worse.
The UK government has now
performed nearly 11 million tests. Could there be 11,000
"cases"
that are simply
a
mistake
? In turn, that means governments and other authorities might be introducing additional restrictions on people's
lives that are actually unnecessary.
The problem of false positives is much less significant when the disease really is in wide circulation. It doesn't change the
picture much for the period from mid-March through to the start of June. (In any event, in the UK at least, there was very
little testing capacity thanks to the jaw-dropping incompetence of bodies like Public Health England.)
Let's look at the latest
figures. On Sunday, July 26, for example, 142,954 tests were processed. Of these, 747 were found to be positive. If 0.1
percent of tests are false positives, we would expect 142 of those 747 positives to be false. If the test turns out to be
slightly less accurate � perhaps 'only' 99.5 percent accurate (which still seems very good), then 710, almost all the reported
positives, could be false.
We should also bear in
mind, when trying to assess the overall situation, that there will be some false negatives. There will also be people who
don't show symptoms who do have the virus and never get tested. But this understanding shows that we do need to be careful
about reading too much into every small blip in the number of cases. We should be particularly sceptical about imposing new
restrictions like mandatory quarantine. And if we rely solely on these tests, we could have the crazy situation where Covid-19
apparently never disappears, even when nobody has got it.
Think your friends would be
interested? Share this story!
I remember signs on businesses that said "No shirts, no shoes: no service". I don't recall
morons screaming at underpaid clerks about their constitutional right not to wear a shirt or
shoes.
Population density has at least something to do with it. Big cities are the hardest hit, as
would be expected. The US death rate per capita is below that of Belgium, the UK, Spain, Italy,
Sweden, Peru (which is surprising), Chile (another surprise), and France.
John Michener 20
hours ago
I fail to see your problem with masks. My grandfather wore a gas mask on the front during
World War 1. I wear a mask, indeed a N99 mask, when sawing concrete or doing fine wood
sanding. When I was in the chemical process industry, some stations had Oxygen rebreathers to
deal with the hazards in case of accidents.
Medical staff have always worn respirators around
patients with airborne diseases, as have researchers handling such agents. Covid-19,
Tuberculosis, and late stage plague are all airborne. Wearing a mask when in a situation when
you are potentially exposed is common sense.
So wearing my N99 mask when I go shopping is a trivial additional step. I actually wear
nitrile gloves as well - I had them for dealing with paints and solvents.
Now I have had to give up eating out and going to my professional society meetings. I am
not happy about that, but I am not willfully stupid. I am approaching 70...
d_hochberg Bradley
Perry • 6
hours ago
One element of being a proper person is having some regard for the wellbeing of other
people.
stephen
pickard Bradley
Perry • 5
hours ago
To me : A proper person dresses properly for the occasion. A proper person has high
regard for both himself and others. A proper person does not smoke in a no smoking zone. A
proper person places his child in a child restraint seat while riding in a car. And on and
on with other safety festures that we accept.You get my point.
What I would have you do is to do the three things that I mentioned.
Social distance. Good hygiene protocol. And yes wear a mask. A rhetorical question.
Would you permit a surgeon and every other person in an operating room go about the surgery
masklessess?
SatirevFlesti Bradley
Perry • 10
hours ago
Real science and evidence won't convince the Coronadoom kool-aid drinkers. Masks are all
about signalling one's virtue and submission to arbitrary rules and to be seen as "doing
something". That the virus has an IFR in the range of flu and that mask are ineffective in
stopping spread of viruses doesn't matter to them. They want to force everyone to abdicate
human dignity and act in the same paranoid, abject manner as they do. It's all political
and has been form the beginning.
njoseph18 SatirevFlesti
• 8
hours ago
So if masks are ineffective, are you comfortable having your surgery team not wear masks
and breathe all over you while you're cut open? If not, why not, since masks are
ineffective?
I work in a hospital. The people who say Covid is just flu both don't understand how bad
Covid is and also don't understand how deadly the flu can be.
A third thing they don't understand is that cloth or surgical masks are about preventing
asymptomatic transmission, which is a real thing. I've seen people die from Covid that they
caught from someone who was "perfectly healthy."
It is such a simple, small thing to do, and has nothing to do with virtue signalling and
everything to do with not killing other people because you're carrying a virus and don't
know it. Some of the most Trump supporting people I've ever met work in this hospital and
wear masks everywhere they go to protect others, because they understand what Covid is.
C'mon people, if other countries can get this right without all the hand-wringing, so
Gswag99 njoseph18
• 8
hours ago • edited
weak straw man emotive argument with no basis in reason or education whatsoever.
njoseph18 Gswag99
• 7
hours ago
Umm, actually I am a frontline non clinical hospital worker. I guess you're a bot but if
my reasoning is emotive can you kindly share the peer reviewed data upon which you base
your perspective?
stephen
pickard Gswag99
• 5
hours ago
It is a good counter point. One I made above using the same anology. Relevant anologies
are powerful antidotes to careless thinking like yours.
Curious SatirevFlesti
• 4
hours ago
I didn't realize Fisher Price ran a medical school
Corporate Insiders Pocket $1 Billion in Rush for Coronavirus Vaccine David Gelles and
Jesse Drucker 11 hrs ago
On June 26, a small South San Francisco company called Vaxart made a surprise announcement:
A coronavirus vaccine it was working on had been selected by the U.S. government to be part of
Operation Warp Speed, the flagship federal initiative to quickly develop drugs to combat
Covid-19.
Vaxart's shares soared. Company insiders, who weeks earlier had received stock options worth
a few million dollars, saw the value of those awards increase sixfold. And a hedge fund that
partly controlled the company walked away with more than $200 million in instant profits.
https://products.gobankingrates.com/r/d9360ea31bf06ea8b9d0ef49288e28fb
The race is on to develop a coronavirus vaccine, and some companies and investors are
betting that the winners stand to earn vast profits from selling hundreds of millions -- or
even billions -- of doses to a desperate public.
Across the pharmaceutical and medical industries, senior executives and board members are
capitalizing on that dynamic.
They are making millions of dollars after announcing positive developments, including
support from the government, in their efforts to fight Covid-19. After such announcements,
insiders from at least 11 companies -- most of them smaller firms whose fortunes often hinge on
the success or failure of a single drug -- have sold shares worth well over $1 billion since
March, according to figures compiled for The New York Times by Equilar, a data
provider.
In some cases, company insiders are profiting from regularly scheduled compensation or
automatic stock trades. But in other situations, senior officials appear to be pouncing on
opportunities to cash out while their stock prices are sky high. And some companies have
awarded stock options to executives shortly before market-moving announcements about their
vaccine progress.
The sudden windfalls highlight the powerful financial incentives for company officials to
generate positive headlines in the race
for coronavirus vaccines and treatments , even if the drugs might never pan out.
Some companies are attracting government scrutiny for potentially using their associations
with Operation Warp Speed as marketing ploys.
For example, the headline on Vaxart's news release declared: "Vaxart's Covid-19 Vaccine
Selected for the U.S. Government's Operation Warp Speed." But the reality is more complex.
Vaxart's vaccine candidate was included in a trial on primates that a federal agency was
organizing in conjunction with Operation Warp Speed. But Vaxart is not among the companies
selected to receive significant financial support from Warp Speed to produce hundreds of
millions of vaccine doses.
"The U.S. Department of Health and Human Services has entered into funding agreements with
certain vaccine manufacturers, and we are negotiating with others. Neither is the case with
Vaxart," said Michael R. Caputo, the department's assistant secretary for public affairs.
"Vaxart's vaccine candidate was selected to participate in preliminary U.S. government studies
to determine potential areas for possible Operation Warp Speed partnership and support. At this
time, those studies are ongoing, and no determinations have been made."
Some officials at the Department of Health and Human Services have grown concerned about
whether companies including Vaxart are trying to inflate their stock prices by exaggerating
their roles in Warp Speed, a senior Trump administration official said. The department has
relayed those concerns to the Securities and Exchange Commission, said the official, who spoke
on the condition of anonymity.
It isn't clear if the commission is looking into the matter. An S.E.C. spokeswoman declined
to comment.
"Vaxart abides by good corporate governance guidelines and policies and makes decisions in
accordance with the best interests of the company and its shareholders," Vaxart's chief
executive, Andrei Floroiu, said in a statement on Friday. Referring to Operation Warp Speed, he
added, "We believe that Vaxart's Covid-19 vaccine is the most exciting one in O.W.S. because it
is the only oral vaccine (a pill) in O.W.S."
Well-timed stock transactions are generally legal. But investors and corporate governance
experts say they can create the appearance that executives are profiting from inside
information, and could erode public confidence in the pharmaceutical industry when the world is
looking to these companies to cure Covid-19.
"It is inappropriate for drug company executives to cash in on a crisis," said Ben Wakana,
executive director of Patients for Affordable Drugs, a nonprofit advocacy group. "Every day,
Americans wake up and make sacrifices during this pandemic. Drug companies see this as a
payday."
Executives at a long list of companies have reaped seven- or eight-figure profits thanks to
their work on coronavirus vaccines and treatments.
Shares of Regeneron, a biotech company in Tarrytown, N.Y., have climbed nearly 80 percent
since early February, when it announced a collaboration with the Department of Health and Human
Services to develop a Covid-19 treatment. Since then, the company's top executives and board
members have sold nearly $700 million in stock. The chief executive, Leonard Schleifer, sold
$178 million of shares on a single day in May.
Alexandra Bowie, a spokeswoman for Regeneron, said most of those sales had been scheduled in
advance through programs that automatically sell executives' shares if the stock hits a certain
price.
Moderna, a 10-year-old vaccine developer based in Cambridge, Mass., that has never brought a
product to market, announced in late January that it was working on a coronavirus vaccine. It
has issued a stream of news releases hailing its vaccine progress, and its stock has more than
tripled, giving the company a market value of almost $30 billion.
Moderna insiders have sold about $248 million of shares since that January announcement,
most of it after the company
was selected in April to receive federal funding to support its vaccine efforts.
While some of those sales were scheduled in advance, others were more spur of the moment.
Flagship Ventures, an investment fund run by the company's founder and chairman, Noubar Afeyan,
sold more than $68 million worth of Moderna shares on May 21. Those transactions were not
scheduled in advance, according to securities filings.
Executives and board members at Luminex, Quidel and Emergent BioSolutions have sold shares
worth a combined $85 million after announcing they were working on vaccines, treatments or
testing solutions.
At other companies, executives and board members received large grants of stock options
shortly before the companies announced good news that lifted the value of those options.
Novavax, a drugmaker in
Gaithersburg, Md., began working on a vaccine early this year. This spring, the company
reported promising preliminary test results and a $1.6
billion deal with the Trump administration.
In April, with its shares below $24, Novavax issued a batch of new stock awards to all its
employees "in acknowledgment of the extraordinary work of our employees to implement a new
vaccine program." Four senior executives, including the chief executive, Stanley Erck, received
stock options that were worth less than $20 million at the time.
Since then, Novavax's stock has rocketed to more than $130 a share. At least on paper, the
four executives' stock options are worth more than $100 million.
So long as the company hits a milestone with its vaccine testing, which it is expected to
achieve soon, the executives will be able to use the options to buy discounted Novavax shares
as early as next year, regardless of whether the company develops a successful vaccine.
Silvia Taylor, a Novavax spokeswoman, said the stock awards were designed "to incentivize
and retain our employees during this critical time." She added that "there is no guarantee they
will retain their value."
Two other drugmakers, Translate Bio and Inovio, awarded large batches of stock options to
executives and board members shortly before they announced progress on their coronavirus
vaccines, sending shares higher. Representatives of the companies said the options were
regularly scheduled annual grants.
Vaxart, though, is where the most money was made the fastest.
At the start of the year, its shares were around 35 cents. Then in late January, Vaxart
began working on an orally administered coronavirus vaccine, and its shares started rising.
Vaxart's largest shareholder was a New York hedge fund, Armistice Capital, which last year
acquired nearly two-thirds of the company's shares. Two Armistice executives, including the
hedge fund's founder, Steven Boyd,
joined Vaxart's board of directors. The hedge fund also purchased rights, known as
warrants, to buy 21 million more Vaxart shares at some point in the future for as little as 30
cents each.
Vaxart has never brought a vaccine to market. It has just 15 employees. But throughout the
spring, Vaxart announced positive preliminary data for its vaccine, along with a partnership
with a company that could manufacture it. By late April, with investors sensing the potential
for big profits, the company's shares had reached $3.66 -- a tenfold increase from January.
On June 8, Vaxart changed the terms of its warrants agreement with Armistice, making it
easier for the hedge fund to rapidly acquire the 21 million shares, rather than having to buy
and sell in smaller batches.
One week later, Vaxart announced that its chief executive was stepping down, though he would
remain chairman. The new C.E.O., Mr. Floroiu, had previously worked with Mr. Boyd, Armistice's
founder, at the hedge fund and the consulting firm McKinsey.
On June 25, Vaxart announced that it had signed a letter of intent with another company that
might help it mass-produce a coronavirus vaccine. Vaxart's shares nearly doubled that day.
The next day, Vaxart issued its news release saying it had been
selected for Operation Warp Speed. Its shares instantly doubled again, at one pointing
hitting $14, their highest level in years.
"We are very pleased to be one of the few companies selected by Operation Warp Speed, and
that ours is the only oral vaccine being evaluated," Mr. Floroiu said.
Armistice took advantage of the stock's exponential increase -- at that point up more than
3,600 percent since January. On June 26, a Friday, and the next Monday, the hedge fund
exercised its warrants to buy nearly 21 million Vaxart shares for either 30 cents or $1.10 a
share -- purchases it would not have been able to make as quickly had its agreement with Vaxart
not been modified weeks earlier.
Armistice then immediately sold the shares at prices from $6.58 to $12.89 a share, according
to securities filings. The hedge fund's profits were immense: more than $197 million.
"It looks like the warrants may have been reconfigured at a time when they knew good news
was coming," said Robert Daines, a professor at Stanford Law School who is an expert on
corporate governance. "That's a valuable change, made right as the company's stock price was
about to rise."
At the same time, the hedge fund also unloaded some of the Vaxart shares it had previously
bought, notching tens of millions of dollars in additional profits.
By the end of that Monday, June 29, Armistice had sold almost all of its Vaxart shares.
Mr. Boyd and Armistice declined to comment.
Mr. Floroiu said the change to the Armistice agreement "was in the best interests of Vaxart
and its stockholders" and helped it raise money to work on the Covid-19 vaccine.
He and other Vaxart board members also were positioned for big personal profits. When he
became chief executive in mid-June, Mr. Floroiu received stock options that were worth about
$4.3 million. A month later, those options were worth more than $28 million.
Normally when companies issue stock options to executives, the options can't be exercised
for months or years. Because of the unusual terms and the run-up in Vaxart's stock price, most
of Mr. Floroiu's can be cashed in now.
Vaxart's board members also received large grants of stock options, giving them the right to
buy shares in the company at prices well below where the stock is now trading. The higher the
shares fly, the bigger the profits.
"Vaxart is disrupting the vaccine world," Mr. Floroiu boasted during a virtual investor
conference on Thursday. He added that his impression was that "it's OK to make a profit from
Covid vaccines, as long as you're not profiteering."
Noah Weiland contributed reporting.
Continue
Reading
Consortiumnews
Volume 26, Number 206 � Friday, July 24, 2020
Main menu
Skip to content
About
Archives
CN Live!
From the Archive Series
In Case You Missed
October Surprise Series
Video Interviews
VIPS Memos
AFGHANISTAN
,
COMMENTARY
,
FOREIGN
POLICY
,
HISTORY
,
HUMAN
RIGHTS
,
MEDIA
,
PROPAGANDA
,
RUSSIA
,
RUSSIAGATE
,
UKRAINE
,
UNITED
KINGDON
,
UNTIL
THIS DAY--HISTORICAL PERSPECTIVES ON THE NEWS
Cold Wars & Profit
July 21, 2020
Save
Craig
Murray lambasts a Russophobic media that celebrates a supposed cyber attack on UK vaccine research, ignores collapse
of key evidence of a "hack" and dabbles in dubious memorabilia.
The Guardian's
headquarters
in London.
(Bryantbob,
CC BY-SA 3.0, via Wikimedia Commons)
By
Craig
Murray
CraigMurray.org.uk
... ... ...
Attack on UK Vaccine Research
Andrew Marr, center, in 2014.
(
Financial
Times
, Flickr)
A whole slew of these were rehearsed by Andrew Marr on his flagship BBC1 morning show. The latest is the accusation
that Russia is responsible for a cyber attack on Covid-19 vaccination research. This is another totally evidence-free
accusation. But it misses the point anyway.
The alleged cyber attack, if it happened, was a hack not an attack -- the allegation is that there was an effort to
obtain the results of research, not to disrupt research. It is appalling that the U.K. is trying to keep its research
results secret rather than share them freely with the world scientific community.
As I have
reported
before
, the U.K. and the USA have been preventing the WHO from implementing a common research and common vaccine
solution for Covid-19, insisting instead on a profit driven approach to benefit the big pharmaceutical companies (and
disadvantage the global poor).
What makes the accusation that Russia tried to hack the research even more dubious is the fact that Russia had
just
bought
the very research specified. You don't steal things you already own.
Evidence of CIA Hacks
If anybody had indeed hacked the research, we all know it is impossible to trace with certainty the whereabouts of
hackers. My VPNs [virtual private networks] are habitually set to India, Australia or South Africa depending on where
I am trying to watch the cricket, dodging broadcasting restrictions.
More pertinently,
WikiLeaks'
Vault
7 release of CIA material showed the
specific
programs
for the CIA in how to leave clues to make a leak look like it came from Russia. This irrefutable
evidence that the CIA do computer hacks with apparent Russian "fingerprints" deliberately left, like little bits of
Cyrillic script, is an absolutely classic example of a fact that everybody working in the mainstream media knows to
be true, but which they all contrive never to mention.
Thus when last week's "Russian hacking" story was briefed by the security services -- that former Labour Party Leader
Jeremy Corbyn deployed secret documents on U.K./U.S. trade talks which had been posted on Reddit, after being stolen
by an evil Russian who left his name of Grigor in his Reddit handle -- there was no questioning in the media of this
narrative. Instead, we had another round of McCarthyite witch-hunt aimed at the rather tired looking Corbyn.
Personally, if the Russians had been responsible for revealing that the Tories are prepared to open up the NHS
"market" to big American companies, including ending or raising caps on pharmaceutical prices, I should be very
grateful to the Russians for telling us. Just as the world would owe the Russians a favor if it were indeed them who
leaked evidence of just how systematically the DNC rigged the 2016 primaries against Bernie Sanders.
But as it happens, it was not the Russians. The latter case was a leak by a disgusted insider, and I very much
suspect the NHS U.S. trade deal link was also from a disgusted insider.
When governments do appalling things, very often somebody manages to blow the whistle.
On the core subject here: By necessity, a
pandemic requires a cooperative international response. Only one country has refused to do so: The US. In their supreme
arrogance, our ruling class lost track the fact that the US needs the rest of the world, not the other way way around.
We Find the Best $500 Cars to Field in the 24 Hours of Lemons Race Series
Sources: Trump erupted over Esper's flag ban
Study identifies six different "types" of COVID-19
A new study of COVID-19 , based on
data from a symptom tracker app, determined that there are six distinct "types" of the disease involving different clusters of symptoms.
The discovery could potentially open new possibilities for how doctors can better treat individual patients and predict what level
of hospital care they would need.
Researchers from
King's College London
studied data from approximately 1,600 U.K. and U.S. patients who regularly logged their symptoms in the COVID Symptom Tracker App
in March and April.
Typically, doctors will look for
key symptoms
such as cough, fever and
loss
of the sense of smell to detect COVID-19. The study, which has not been peer-reviewed, says the six different "types" of COVID-19
can vary by severity and come with their own set of symptoms.
"I think it's very, very interesting," Dr. Bob Lahita, who is not affiliated with the study, told CBSN anchors Vladimir Duthiers
and Anne-Marie Green. "Among the patients I see, those who recovered, many of them present different ways: some people with fever
and some without fever, and some with
nausea and vomiting, some people with diarrhea , etc."
The six clusters of symptoms outlined in the study are:
Flu-like with no fever: Headache, loss of smell, muscle pains, cough, sore throat, chest pain, no fever.Flu-like with fever: Headache, loss of smell, cough, sore throat, hoarseness, fever, loss of appetite.Gastrointestinal: Headache, loss of smell, loss of appetite, diarrhea, sore throat, chest pain, no cough.Severe level one, fatigue: Headache, loss of smell, cough, fever, hoarseness, chest pain, fatigue.Severe level two, confusion: Headache, loss of smell, loss of appetite, cough, fever, hoarseness, sore throat, chest
pain, fatigue, confusion, muscle pain.Severe level three, abdominal and respiratory: Headache, loss of smell, loss of appetite, cough, fever, hoarseness,
sore throat, chest pain, fatigue, confusion, muscle pain, shortness of breath, diarrhea, abdominal pain.
The first level, "flu-like with no fever," is associated with headaches, loss of smell, muscle pains, cough, sore throat and chest
pain. Patients at this level have a 1.5% chance of needing breathing support such as oxygen or a ventilator.
The second type, "flu-like with fever," includes symptoms like loss of appetite, headache, loss of smell, cough, sore throat,
hoarseness and fever. Researchers say about 4.4% of patients at this level needed breathing support.
Patients with the third type, simply described as "gastrointestinal," do not have a cough as part of their illness. Instead, they
experience headache, diarrhea, loss of smell, loss of appetite, sore throat and chest pain, and about 3.3% needed breathing support.
Lahita referred to the following three clusters of COVID-19 as the "really severe types."
In type four, or "severe level one," patients experience fatigue along with headache, loss of smell, cough, fever, hoarseness
and chest pain. Patients at this level needed breathing support at a rate of 8.6%.
Type five, "severe level two," includes the symptoms of type four along with loss of appetite, sore throat and muscle pain, and
is mainly distinguished by
confusion
.
"That means you don't know where you are or where you live, whether you are in or out of the hospital, who your relatives are,"
Lahita explained. "That is very scary." Almost 10% of patients at that level need breathing support.
The most severe type of COVID-19 is referred to as "severe level three, abdominal and respiratory," and has all the above symptoms
along with abdominal pain, shortness of breath and diarrhea. Nearly 20% of these patients need breathing support.
"Those are the severe level threes who wind up on a ventilator, and then it is touch-and-go as to whether they survive the
infection entirely," Lahita said.
The U.K. researchers also found that only 16% of patients with type one COVID-19 required hospitalization, compared with nearly
half of the patients with type six.
Patients in the severe clusters also tended to be older or with pre-existing conditions and weakened immune systems, compared
to those in the first three.
Scientists hope the discovery, once further studied, could help predict what types of care patients with COVID-19 might need,
and give doctors the ability to predict which patients would fall into which category.
"I'm very happy that these six types have been identified and can give us an idea of a prognosis going forward for patients who
are afflicted with this virus," Lahita said.
c1ue , Jul 23 2020 15:30 utc |
8
More talk about T-cells and B-cells (per Volchkov)Australia
T-cell and B-cell research
Notable quotes:
"... This boosts the hypothesis that normal speaking and breathing, not just coughing and sneezing, are responsible for spreading COVID-19 -- and that infectious doses of the virus can travel distances far greater than the six feet (two meters) urged by social distancing guidelines. ..."
"... The paper was posted to the medrxiv.org website, where most cutting-edge research during the pandemic has first been made public. ..."
"... The team managed to collect microdroplets as small as one micron in diameter. They then placed these samples into a culture to make them grow, finding that three of the 18 samples tested were able to replicate. For Santarpia, this represents proof that microdroplets, which also travel much greater distances than big droplets, are capable of infecting people. "It is replicated in cell culture and therefore infectious," he said. ..."
Scientists have known for several months the new coronavirus can become suspended in
microdroplets expelled by patients when they speak and breathe, but until now there was no
proof that these tiny particles are infectious.
A new study by scientists at the University of Nebraska that was uploaded to a medical
preprint site this week has shown for the first time that SARS-CoV-2 taken from microdroplets,
defined as under five microns, can replicate in lab conditions.
This boosts the hypothesis that normal speaking and breathing, not just coughing and
sneezing, are responsible for spreading COVID-19 -- and that infectious doses of the virus can
travel distances far greater than the six feet (two meters) urged by social distancing
guidelines.
The results are still considered preliminary and have not yet appeared in a peer-reviewed
journal, which would lend more credibility to the methods devised by the scientists.
The paper was posted to the medrxiv.org website, where most cutting-edge research during the
pandemic has first been made public.
The same team wrote a paper in March showing that the virus remains airborne in the rooms of
hospitalized COVID-19 patients, and this study will soon be published in a journal, according
to the lead author.
"It is actually fairly difficult" to collect the samples, Joshua Santarpia, an associate
professor at the University of Nebraska Medical Center told AFP.
The team used a device the size of a cell phone for the purpose, but "the concentrations are
typically very low, your chances of recovering material are small."
The scientists took air samples from five rooms of bedridden patients, at a height of about
a foot (30 centimeters) over the foot of their beds.
The patients were talking, which produces microdroplets that become suspended in the air for
several hours in what is referred to as an "aerosol," and some were coughing.
The team managed to collect microdroplets as small as one micron in diameter. They then placed these samples into a culture to make them grow, finding that three of the
18 samples tested were able to replicate. For Santarpia, this represents proof that microdroplets, which also travel much greater
distances than big droplets, are capable of infecting people. "It is replicated in cell culture and therefore infectious," he said.
Why we wear masks
The potential for microdroplet transmission of the coronavirus was at one stage thought to
be improbable by health authorities across the world. Later, scientists began to change their mind and acknowledge it may be a possibility, which
is the rationale for universal masking.
The World Health Organization was among the last to shift its position, doing so on July
7.
"I feel like the debate has become more political than scientific," said Santarpia. "I think most scientists that work on infectious diseases agree that there's likely an
airborne component, though we may quibble over how large."
The new Microsoft Edge
Linsey Marr, a professor at Virginia Tech who is a leading expert on aerial transmission of
viruses and wasn't involved in the study, said it was rare to obtain measurements of the amount
of virus present in air.
"Based on what we know about other diseases and what we know so far about SARS-CoV-2, I
think we can assume that if the virus is 'infectious in aerosols,' then we can become infected
by breathing them in," she told AFP.
Russian Elite Received 'Experimental' COVID-19 Vaccine As Early As April by
Tyler Durden Mon,
07/20/2020 - 07:22 Twitter
Facebook Reddit Email Print
Last week, we shared news of what Russia's scientific community had touted as a major
breakthrough in the development of a vaccine for SARS-CoV-2: A vaccine trial at Moscow's
Sechenov First Moscow State Medical University had yielded the first successful human trials.
The American business press slavishly parrots every Moderna press release as the company
regurgitates its Phase 1 trial results, despite the fact that the politically-connected biotech
company's stage 3 clinical trials won't begin until later this month. Meanwhile, its CEO
Stephane Bancel and other executives have cashed in on their Moderna shares,
prompting SEC chief Jay Clayton to sheepishly caution against credibility-destroying insider
selling.
Despite all of this, we didn't hear a peep out of the western press about
the Sechenov trial's accomplishments . However, a few days later, with anxieties about
Russia-backed electoral interference intensifying and 'national polls' hinting at a Biden
landslide,
the British press reported on a new 'policy paper' accusing those pesky Ruskies of trying
to steal British research involving COVID-19 vaccines. Intel shared by Canada and the US
purportedly supported this conclusion, though Russia has vehemently denied the accusations.
But that's not all: Around the same time, Foreign Secretary Dominic Raab accused Russia of
trying to meddle in the UK's December election (which returned the Tories to power and ended
the reign of opposition leader Jeremy Corbyn).
Were these reports about Russia's vaccine-trial successes merely a smokescreen? The British
might see it that way, but on Monday, US-based Bloomberg News published an interesting report
claiming that certain Russian VIPs had been administered experimental doses of a vaccine
prototype as early as April. Reportedly developed by Moscow's Gamaleya Institute and financed
by the state-run Russian Direct Investment Fund, this Russian vaccine candidate is a so-called
"viral vector vaccine" based on human adenovirus - a common cold virus fused with the spike
protein of SARS CoV-2 to stimulate a human immune response.
It's similar to a vaccine being developed by China's CanSino Biologics, according to
Bloomberg.
Scores of members of Russia's business and political elite have been given early access to
an experimental vaccine against Covid-19, according to people familiar with the effort, as
the country races to be among the first to develop an inoculation.
Top executives at companies including aluminum giant United Co. Rusal, as well as
billionaire tycoons and government officials began getting shots developed by the state-run
Gamaleya Institute in Moscow as early as April, the people said. They declined to be
identified as the information isn't public.
The Gamaleya vaccine, financed by the state-run Russian Direct Investment Fund and backed
by the military, last week completed a phase 1 trial involving Russian military personnel.
The institute hasn't published results for the study, which involved about 40 people, but has
begun the next stage of trials with a larger group.
Gamaleya's press office couldn't be reached by phone Sunday. Kremlin spokesman Dmitry
Peskov didn't respond to a text message asking whether President Vladimir Putin or others in
his administration have had the shots. A government spokesman couldn't immediately
comment.
Wait... so the Russians hacked the British vaccine research, traveled back in time, then
decided to test their vaccine prototype on some of the most powerful people in Russia's (highly
unequal) society? Well, they had to first travel to the future to steal the time-travel
technology from the Americans (bear with us...we're still piecing it all together).
The program under which members of Russia's business and political elite have been given
the chance to volunteer for doses of the experimental vaccine is legal but kept under wraps
to avoid a crush of potential participants, according to a researcher familiar with the
effort. He said several hundred people have been involved. Bloomberg confirmed dozens who
have had the shots but none would allow their names to be published.
It's not clear how participants are selected and they aren't part of the official studies,
though they are monitored and their results logged by the institute. Patients usually get the
shots - two are needed to produce an immune response Gamaleya says will last for about two
years - at a Moscow clinic connected to the institute. Participants aren't charged a fee and
sign releases that they know the risks involved.
Dmitriev of the RDIF said he and his family had taken the shots and noted that a
significant number of other volunteers have also been given the opportunity. He declined to
provide further details. The Gamaleya Institute said it vaccinated its director, as well as
the team working on the trial, when it started. In May, state-controlled Sberbank recruited
volunteers among employees to test the institute's vaccine.
O ne top executive who had the vaccine said he experienced no side effects. He said he
decided to risk taking the experimental shots in order to be able to live a normal life and
have business meetings as usual. Other participants have reported fever and muscle aches
after getting the shots.
NEVER MISS THE NEWS THAT MATTERS MOST
ZEROHEDGE DIRECTLY TO YOUR INBOX
Receive a daily recap featuring a curated list of must-read stories.
https://lockerdome.com/lad/13084989113709670?pubid=ld-dfp-ad-13084989113709670-0&pubo=https%3A%2F%2Fwww.zerohedge.com&rid=www.zerohedge.com&width=890
Is it so hard to believe that Russia had enough faith in its vaccine prototype that it would
allow certain individuals the choice of receiving an early dose? After all, EU governments are
already buying up millions of doses of Moderna's still-largely-untested vaccine candidate.
Similarly, is it possible that Russian spies were simply monitoring the competition?
Who knows? When it comes to the shadowy world of espionage, the public rarely hears the full
story. Russia's outbreak has slowed in recent weeks as it has been overtaken by India, which
now counts more than 1 million confirmed cases. Meanwhile Russia has confirmed more than
750,000 cases of Covid-19, the fourth-largest total in the world.
pdate (0935ET): A coronavirus vaccine candidate developed by Oxford and AstraZeneca has
shown promise in an early trial which found it to be safe for human consumption while reliably
producing antibodies that are effective at stopping the virus.
In what looked like a coordinated one-two punch, one of the top researchers leading the
Oxford-Astrazeneca trials said in an interview published Monday morning that the research was
making "good progress". Minutes later, the Lancet published the first Phase 1/2 trial results,
which showed that the Oxford-AstraZeneca vaccine caused "robust immune responses" and was
"tolerated" by all study subjects.
That interview was published Monday morning in the US, just minutes before the Lancet
released the results of a Phase 1/2 study of the Oxford-AZ vaccine, the most highly anticipated
COVID-19 news of the day.
There are currently more than 137 vaccine candidates undergoing preclinical development, and
23 in early clinical development, according to WHO. Of these, candidates from Moderna and the
Oxford-AstraZeneca partnership are two of the most closely followed prototypes. Governments
have already started ordering the vaccine from Moderna, even though approval is still months,
perhaps years, away.
According to the Lancet, research has shown that vaccine candidates from Cansino and
Astra-Oxford trial have been making good progress, and while they couldn't say much
conclusively, the Astra-Oxford trial showed no worrisome "adverse effects".
The Phase 1/2 trial, one of the first human studies of the vaccine, showed an appropriate
"immune response". Patients who received 2 doses instead of one saw a stronger response. All
patients who received the vaccine generated the desired immune response.
Oxford's candidate "showed an acceptable safety profile, and homologous boosting increased
antibody responses. These results "support large scale evaluation of this candidate vaccine in
an ongoing phase 3 program." The Oxford-AZ study included 1,077 participants spread across 5
test sites in and around the UK.
By comparison, Moderna has released press releases touting findings from studies with fewer
than 100 patients. The fact that 8 patients developed neutralizing antibodies
in a study that involved dozens of additional subjects was apparently news enough for Moderna,
which released a market-pumping press release on those findings a few weeks back.
Though to be sure, not everybody was impressed.
In the study, researchers measured the number of antibodies, and the strength of the immune
response, after administering single doses and double doses of the vaccine to various groups of
study subjects, and compared those results with a control group who received another vaccine.
Pain and swelling caused by the injection were easily treated with paracetemol.
There were no serious adverse events related to ChAdOx1 nCoV-19. In the ChAdOx1 nCoV-19
group, spike-specific T-cell responses peaked on day 14 (median 856 spot-forming cells per
million peripheral blood mononuclear cells, IQR 493–1802; n=43). Anti-spike IgG
responses rose by day 28 (median 157 ELISA units [EU], 96–317; n=127), and were boosted
following a second dose (639 EU, 360–792; n=10). Neutralising antibody responses
against SARS-CoV-2 were detected in 32 (91%) of 35 participants after a single dose when
measured in MNA80 and in 35 (100%) participants when measured in PRNT50. After a booster
dose, all participants had neutralising activity (nine of nine in MNA80 at day 42 and ten of
ten in Marburg VN on day 56). Neutralising antibody responses correlated strongly with
antibody levels measured by ELISA (R²=0·67 by Marburg VN; p<0·001).
The result: The vaccine candidate has been deemed safe enough to move on to 'Phase 3', which
would involve large-scale human trials.
ChAdOx1 nCoV-19 showed an acceptable safety profile, and homologous boosting increased
antibody responses. These results, together with the induction of both humoral and cellular
immune responses, support largescale evaluation of this candidate vaccine in an ongoing phase
3 programme.
Read the full Lancet paper below:
Blue Dotterel , Jul 20 2020 9:13 utc |
96
Here is an alternative, if familiar take on Masks from OffGuardian: https://off-guardian.org/2020/07/18/media-mask-mania-or-covid19-groupthink/
He correctly points out the confusion created by certain "experts":
"For anyone who has forgotten, Fauci told 60 Minutes that:
[t]here's no reason to be walking around with a mask. When you're in the middle of an
outbreak, wearing a mask might make people feel a little better and it might even block a
droplet, but it's not providing the perfect protection that people think it is. And often
there are unintended consequences – people keep fiddling with the mask and they keep
touching their face."
That was how things stood when the epidemic was new and all stops were out. And now?"
The author of the article also notes that the mask doesn't prevent you from being
infected, but of course the point is that it reduces the probability of being infected.
But he does make an astute point:
"Recently I had the poor judgment to turn on National Public Radio for about an hour,
under the impression that I was going to learn something about the day's news.
Needless to say the author did not approve of us "muzzling" ourselves, but the MSM, like
commenters here, and perhaps b do seem obsessed with the mask.
IMO, the mask is an important component in preventing more people from becoming infected,
but does not prevent all people from being infected. So, what about the people who do become
infected? its too late for the mask to help them. How do we mitigate the effects of the
disease?
For the Big Pharma mafia and its political apparatchiks in the West, its expensive
patented drugs like Remdesivir, as opposed to inexpensive out of patent chloroquine, among
others, as well as the Holy Grail for Big Pharma - a highly profitable vaccine, yet to come.
A list of drugs mostly based on CDC sourcing. The CDC, like the WHO being seriously
compromised by its conections to Big Pharma:https://www.drugs.com/condition/covid-19.html
Unfortunately, politcally motivated scientific fraud as published in the retracted Lancet
article, among others, prevents us from having an intelligent discussion of this even on Moon
of Allabama.
A final area for discussion, as important or more important than the above, is how to
approach impending "lockdowns" of the economies in the future. A potential greater tragedy
than the virus itself may be the destruction wrought on the unemployed and small businesses
that has already occurred, but promises to continue should a second wave of the virus appaer
this fall.
Admittedly, such discussions seem hopeless. We can individually control whether we wear a
mask or not, but how do we mitigate the effects of those who have already contracted the
disease, and those whose livelihood is threatened or destroyed by the "lockdowns" in response
to the disease?
I would like to see these last two areas more seriously investigated on Moon of
Alabama.
By Dr. Sherri Tenpenny – May 21, 2020 – an osteopathic medical doctor,
board-certified in three specialties. She is the founder of Tenpenny Integrative Medical Center, a medical clinic located
near Cleveland, Ohio. Her company, Courses4Mastery.com provides online education and
training regarding all aspects of vaccines and vaccination.
_____________________________
In 1965, scientists identified the first human coronavirus; it was associated with the
common cold. The Coronavirus family, named for their crown-like appearance, currently includes
36 viruses.
Within that group, there are 4 common viruses that have been causing infection in humans for
more than sixty years. In addition, three pandemic coronaviruses that can infect humans: SARS,
MERS, and now, SARS-CoV-2.
As the news of deaths in China, South Korea, Italy, and Iran began to saturate every form of
media 24/7, we became familiar with a new term: COVID-19. To be clear, the name of the newly
identified coronavirus is SARS-CoV-2, short for Severe Acute Respiratory Syndrome
Coronavirus-2. This virus is associated with fever, cough, chest pain, and shortness of breath,
the complex of symptoms that form the diagnosis of COVID-19.
The Trump administration declared a public health emergency on January 31, 2020, then on
February 2 placed a ban on the entry of most travelers who had recently been in China. On
February 4, Alex Azar, the Secretary of Health and Human Services (HHS) issued a declaration of
public health emergency and activated the Public Readiness and Emergency Preparedness Act,
otherwise known as the PREP
Act. This nefarious legislation provides complete protection of manufacturers from
liability for all products, technologies, biologics, or any vaccine developed as a medical
countermeasure against COVID-19. For those nervously waiting for the vaccine to become
available, be sure to understand the PREP Act
before rushing to the get in line.
Calls for testing – to see if a person is or isn't infected – began soon after
the emergency was declared, but performing those tests was initially slow due to an inadequate
number of test kits. As the kits became available, those
developed by the CDC had a defect: The reagents reacted to the
negative control sample , making the test inaccurate and the kits unusable.
In various
countries, thousands of test kits purchased from China were found to be contaminated with
the SARS-CoV-2 viruses. No one really knows how that happened, but theories spread like
wildfire. Could the test kit infect the person being tested? Or, did it mean the test would
return a false-positive result, driving up the numbers of those said to be infected so those in
power could implement stronger lockdowns and accelerate the hockey-stick unemployment rates?
Neither of those questions has been adequately answered.
Mandatory Testing of what?
Authorities claim that testing is important for public health officials to assess if their
mitigation efforts – "shelter in place" and "social distancing" and "wearing a mask"
– are making a difference to "flatten the curve." Officials also claim that testing is
necessary to know how many persons are infected within a community and to understand the nature
of how coronaviruses spread.
Are these reasons sufficient to give up our health freedom and our personal rights, being
tested and shamed in public?
Despite the challenges with test kits, testing began. By the end of March 2020, more than 1
million people had been tested across the US. By May 9, the number tested had grown to over
8.7M. Testing methods include a swab of the
nasal passages or by inserting a long, uncomfortable swab through the nose to scrape the back of the
throat. Specimens have also been obtained bronchoalveolar lavage, from
sputum , and from stool
specimens.
The call for mandatory testing has been gathering steam and becoming ever more onerous. In
Washington state, Governor Inslee
has declared:
Individuals that refuse to cooperate with contact tracers and/or refuse testing, those
individuals will not be allowed to leave their homes to purchase basic necessities such as
groceries and/or prescriptions. Those persons will need to make arrangements through friends,
family, or state provided 'family support' personnel .
But what do the results really mean?
Who Should Be Tested
On May 8, 2020, the CDC has listed specific priorities
for when testing should be done. As of May 16, more than 11-million samples have been
collected and more than 3700 specimens have not yet been evaluated.
High Priority
Hospitalized patients with symptoms
Healthcare facility workers, workers in living settings, and first responders with
symptoms
Residents in long-term care facilities or other congregate living settings, including
prisons and shelters, with symptoms
Priority
Persons with symptoms of potential COVID-19 infection, including fever, cough, shortness
of breath, chills, muscle pain, new loss of taste or smell, vomiting or diarrhea, and/or sore
throat
Persons without symptoms who are prioritized by health departments or clinicians
, for any reason, including but not limited to public health monitoring, sentinel
surveillance, or screening of asymptomatic individuals according to state and local
plans.
Read that last priority again: That means virtually everyone can be required to get a
test.
Is that a violation of your personal rights? And, if you submit to testing, what does a
"positive test" actually mean?
Types of Testing: RT-PCR
PCR, short for polymerase chain reaction , is a highly specific laboratory technique. The
key to understanding
PCR testing is that PCR can identify an individual specific virus within a viral
family.
Has
COVID-19 Testing Made the Problem Worse? Confusion Regarding "The True Health Impacts"
However, a PCR test can only be used to identify DNA viruses; the SARS-CoV2 virus is an RNA
virus. Therefore, multiple steps must be taken to "magnify" the amount of genetic material in
the specimen. Researchers used a method called RT-PCR, reverse transcription-polymerase chain
reaction, to specifically identify the SARS-CoV-2 virus. It's a complicated process. To read
more about it, go
here and here.
If a nasal or a blood sample contains a tiny snip of RNA from the SARS-CoV-2 virus, RT-PCR
can identify it, leading to a high probability that the person has been exposed to the
SARS-CoV-2 virus.
However – and this is important – a positive RT-PCR test result does not
necessarily indicate a full virus is present. The virus must be fully intact to be
transmitted and cause illness.
RT-PCR Testing: The Importance of Timing
Even if a person has had all the symptoms associated with a coronavirus infection or has
been closely exposed to persons who have been diagnosed with COVID-19, the probability of a
RT-PCR test being positive decreases with the number of days past the onset of symptoms.
According to a study done by
Paul Wikramaratna and others:
For a nasal swab, the percentage chance of a positive test declines from about 94% on day
0 to about 67% by day 10. By day 31, there is only a 2% chance of a positive result.
For a throat swab , the percentage chance of a positive test declines from about 88% on
day 0 to about 47% by day 10. By day 31, there is only a 1% chance of a positive result.
In other words, the longer the time frame between the onset of symptoms and the time a
person is tested, the more likely the test will be negative.
Repeat testing of persons who have a negative test may (eventually) confirm the presence of
viral RNA, but this is impractical. Additionally, repeated testing of the same person can lead
to even more confusing results: The test may go from negative, to positive, then back to
negative again as the immune system clears out the coronavirus infection and moves to
recovery.
And what makes this testing even more confusing is that the
FDA admits that "The detection of viral RNA by RT-PCR does not necessarily equate with an
infectious virus."
Let's break that down:
You've had all the symptoms of COVID19, but your RT-PCR test for SARS-CoV-2 is
negative.
3
Ways Your Cat Asks for Help Dr. Marty Ad by Revcontent Find Out More > - Advertisement -
Does that mean you're "good to go" – you can go to work, go to school or you can
travel? OR
Does that mean your influenza-like illness was caused by some other pathogen, possibly
one of the four coronaviruses that have been in circulation for 60 years? OR
Does that mean the result is a false-negative and you still have the infection, but it
isn't detectable by current tests? OR
Does that mean it was a sample was inadequately taken due to the faulty technique by the
technician? OR
Does that mean you have not been exposed, and you are susceptible to contracting the
infection, and you need to stay in quarantine?
So, what does a "positive" test actually mean? And that's the problem:
No one knows for sure.
Another Type of Testing: Antibodies
According to the nonprofit Foundation for Innovative New Diagnostics
(FIND) , more than 200 serologic blood tests, to test for antibodies, are either now
available or in development.
There are two primary types of antibodies that are assessed for nearly any type of
infection: IgM and IgG. While several new testing devices are being touted as a home test, they
are not the same as a home pregnancy test or a glucometer to you're your blood sugar. The blood
spot or saliva specimen can be collected at home, must it must then be sent to a laboratory for
analysis. It can take a few days – or longer – to get the results. With so many
tests in the pipeline, the ability to test at home will be changing over time.
The first antibody to rise is IgM. It rises quickly after the onset of the infection and is
usually a sign of an acute, or current, infection. The IgM levels diminish quickly as the
infection resolves. The
FDA admits they do not know how long the IgM remains present for SARS-CoV-2 as the
infection is being cleared.
The interpretation of an IgG antibody is more difficult. This antibody is an indicator of a
past infection. The test is often not specific enough to determine if the past infection was
caused by the SARS-CoV-2 virus or one of the four common coronaviruses that cause
influenza-like illness.
The
FDA says:
Because serology testing can yield a negative test result even if the patient is actively
infected (e.g., the body has not yet developed in response to the virus) or maybe falsely
positive (e.g., if the antibody indicates a past infection by a different coronavirus), this
type of testing should not be used to diagnose an acute or active COVID-19 infection.
Similarly, the CDC says the
following regarding antibody testing:
If you test positive:
A positive test result shows you have antibodies as a result of an infection with
SARS-CoV-2, or possibly a related coronavirus.
It's unclear if those antibodies can provide protection (immunity) against getting
infected again. This means that we do not know at this time if antibodies make you immune
to the virus.
If you have no symptoms, you likely do not have an active infection and no additional
follow-up is needed.
It's possible you might test positive for antibodies and you might not have or have
ever had symptoms of COVID-19. This is known as having an asymptomatic infection [ie you
have a healthy immune system!]
An antibody test cannot tell if you are currently sick with COVID-19.
If you test negative
If you test negative for antibodies, you probably did not have a previous infection.
However, you could have a current infection because antibodies don't show up for 1 to 3
weeks after infection.
Some people may take even longer to develop antibodies, and some people may not
develop antibodies.
An antibody test cannot tell if you are currently sick with COVID-19.
What? Wait!
Doesn't the vaccine industry call the IgG a "protective antibody"?
Isn't this the marker of immunity they assess after you've had an infection with measles
or chickenpox or mumps to determine if you are immune to future infections?
Isn't this the marker of induced immunity they are trying to achieve by administering a
vaccine?
If the FDA does not know if an IgG antibody to SARS-CoV-2 after recovering from the
infection is protective against a future infection, then they certainly don't know if an
antibody caused by a vaccine will prevent infection either.
Doesn't this completely eliminate the theory that antibodies afford protection and
antibodies from vaccines are necessary to keep you from getting sick?
Mandatory Testing – New Job Creation
Illinois U.S. Rep. Bobby L. Rush introduced the
H.R. 6666 TRACE Act on May 1.
On his website, Rush said ,
Until we have a vaccine to defeat this dreaded disease, contact tracing in order to
understand the full breadth and depth of the spread of this virus is the only way we will be
able to get out from under this.
H.R.6666 would authorize the Secretary of Health and Human Services (HHS), acting through
the Director of the CDC to award grants to eligible entities to conduct diagnostic testing and
then to trace and monitor the contacts of infected individuals. The contact tracers would be
authorized to test people in their homes and as necessary, quarantine people in place.
Where do they intend to do this testing? Besides mobile units to test people in their homes,
the bill identifies eight specific locations where the testing and contract tracing could
occur: schools, health clinics, universities, churches, and "any other type of entity" the
secretary of HHS wants to use.
The bill would allocate $100 billion in
2020 "and such sums as may be necessary for fiscal year 2021 and any subsequent fiscal year
during which the emergency period continues."
But what are they looking for?
Is your test supposed to be positive – saying you've been exposed and you've
possibly recovered?
Or is your test supposed to be negative , meaning, you are healthy?
Or does a completely negative test – negative RT-PCR test and no IgG antibody mean
you're susceptible to infection and you need to stay in quarantine?
The virus is rapidly mutating, which is rather typical of RNA viruses. In a
study published in April 2020, researchers have discovered that the novel coronavirus has
mutated into at least 30 different genetic variations. If your RT-PCR test is positive, does
this identify exposure to the pandemic virus or exposure to one of the genetic variations? The
same can be said about the vaccines under development: With each mutation, is the vaccine more
likely to be all risk and no benefit when it reaches the market?
What You Can Do
Across the nation, police are being told to not apprehend criminals but instead, to arrest
parents at playgrounds, to arrest lone surfers on public beaches, to fine ministers and
congregation members sitting in their cars listening to a service on the radio, and to restrict
movement by creating one-way sidewalks.
People have had enough. They are beginning to see the huge scam that has been perpetrated on
the entire world over a viral infection with a global death rate of
1.4% (meaning, 1.4% of people infected with SARS-CoV-2 have a fatal outcome, while 98.6%
recover). This is far fewer deaths than a severe flu season.
We're already starting to see the thrust to take our power back:
In Virginia, people went to the beaches en mass,
ignoring social distancing and the orders of the Governor to stay home.
The central California city of Atwater has declared itself a "sanctuary
city," allowing business owners and churches to open, openly defying Democratic
California
Gov. Gavin Newsom's coronavirus-related stay-at-home order.
The truth about wearing
masks is starting to come out and people are voting with their feet. Retired
neurosurgeon, Dr. Russell Blaylock, warns that not only do face masks fail to protect healthy
people from contracting an illness, but they create serious health risks to the wearer.
While they shut us down and held us hostage in our homes, they changed our society, our
lives, our world.
I am not willing to accept this is the "new normal."
I won't submit to testing.
I will refuse mandatory vaccination.
I will stop wearing a mask.
I will not be afraid of standing next to a friend or family member and will not obey the
concept of "social distancing."
I will understand that an asymptomatic carrier is a normal, healthy person and I will not
buy into the fear that I might "catch something" from a normal, healthy person.
It's time for Americans to resist with non-violent civil disobedience. Be brave. Be bold.
Put on the full armor of God, as found in Ephesians
6:10-20 in the Bible, to stand against the world rulers of this present darkness. With God
on our side, all things are possible.
*
Note to readers: please click the share buttons above or below. Forward this article to your
email lists. Crosspost on your blog site, internet forums. etc.
he American profit-based healthcare system impacts us in more ways than just our gargantuan
bill at the excretion end of an emergency room visit. Right now, our lovable idiotic inhumane
healthcare system is acting as a hurdle to the manufacture and procurement of the right drugs
to treat Covid-19.
One of the drugs currently trumpeted as our savior is
Remdesivir . Despite sounding like the name of a Hobbit in Middle Earth, some reports from
the corporate media make it sound like the drug will thrust us face-first into a fresh world of
happiness -- water parks and restaurants and random no-holds-barred make-outs with strangers. A
world where when someone sneezes, we don't dive under our desk with an adult diaper strapped on
our face as a makeshift mask.
There's only one problem. The big pharma company that owns Remdesivir, Gilead, has already
made clear their plans to profiteer from this pandemic. As The
LA
Times put
it –
Drugmaker Gillead says it's doing you a favor by setting the price for its pending COVID-19
treatment, Remdesivir, at more than $2,000 for government agencies and over $3,000 for private
insurers."
How does the CEO of Gilead, Daniel O'Day, justify this disgusting price point? He claims
they're under-pricing Remdesivir.
He said , "In normal circumstances, we would price a medicine according to the value it
provides. Earlier hospital discharge would result in hospital savings of approximately $12,000
per patient."
Public
Outcry Follows Gilead Decision to Charge $3000 for COVID Drug that Costs Pennies to Produce
Gilead announced that a five-day course of its drug Remdesivir -- used to fight COVID-19 --
will cost $3,120 despite costing pennies to produce.
MintPress News | Alan Macleod | Jul 1
The value it provides?? So, if a doctor saves someone's life with heart surgery, then that
guy owes the doctor the entire worth of the rest of his life? Millions of dollars? Maybe he
should become the surgeon's butler or wet nurse.
Saying something should cost even close to the value it provides ranks up there as one of
the stupidest arguments ever spoken. (Second only to when the people at Mountain Dew argued
that human beings would love a Doritos-flavored soft drink named "Dewitos.")
So, for a dude taking Viagra who can now get it up, he owes the makers of Viagra – what?
– sex with his wife? Or does he just owe them 300 orgasms? Or perhaps he owes them the
child he's able to produce while taking the pills. ("Dear Cialis Folks, I'm emailing to ask for
a mailing address to send you my 2-year-old, Robbie. Fair is fair. I want to give you the value
of your goods. Just be careful – he bites a lot. And he's already totally racist. Not
sure how he picked that up so young.")
But there's another catch to Gilead's price-gouging shenanigans. They didn't create
Remdesivir. We did. You and me.
Public Citizen revealed that
Gilead raked in over $70 million from taxpayers. Plus, federal scientists ran the team that
found out Remdesivir also worked against Coronaviruses. And, " The National
Institutes of Health ran the trial that led to Remdesivir's emergency use authorization,
and public funding is supporting clinical trials around the world today."
You and I paid for the creation and research behind Remdesivir. There is absolutely no
reason we should fill the pockets of Gilead's preposterously rich CEO and its board. Most
countries realize this. Most countries don't behave this way. Most countries have some tiny
modicum of respect for the lives of their citizens. America is not most countries.
Back to the
LA Times , "Nearly all other developed countries limit how much pharmaceutical
companies can charge for prescription meds. The U.S. doesn't operate like that. We allow drug
companies to charge as much as they please "
Perhaps prescription meds that cost the same as landing a man on Mars (in a pair of Jimmy
Choo heels) are the reason 42
percent of new cancer patients have their entire life savings wiped out within two years.
The average amount drained from a patient is nearly $100,000, and the entire medical costs for
U.S. cancer patients per year is $80
billion . Why ever change a system that piles such bulbous mountains of cash in the vaults
of those running the show?
Apparently most other national governments don't want to ruin the lives of every cancer
survivor. As to why not, one can only guess.
But this story gets crazier. Not only is Remdesivir way over-priced, we're not even sure it
does much. Some studies show it achieves almost nothing. Meanwhile, according to the
Intercept
[A]nother Covid-19 treatment has quietly been shown to be more effective. A three-drug
regimen offered a greater reduction in the time it took patients to recover than Remdesivir
did. People who took the combination of interferon beta-1b, lopinavir-ritonavir, and ribavirin
got better in seven days as opposed to 12 days for those who didn't take it."
However, I have yet to hear of a mad rush to hoard those drugs. Why is that? Probably
because those drugs don't have colossal marketing campaigns that would make Coca-Cola blush. In
fact there appears to be no marketing campaign whatsoever for the more effective drugs. To
figure out why that is, one simply must follow the money.
New
Research Shows Anti-Coronavirus Drugs Could Be Produced for Pennies A new study shows that
several drugs that have shown promise in fighting the coronavirus could be produced cheaply and
in en masse.
MintPress News | Alan Macleod | Apr 10
[E]ach of the
three drugs in the new combination is generic, or no longer under patent, which means that
no company stands to profit significantly from its use."
Must cut-throat late-stage capitalism always be so predictable?
Only the ridiculously profitable drugs are worth hyping. Only the money makers deserve
80,000 commercials telling every consumer to irrationally demand them. The cheap drugs that
simply – save lives – those are garbage. What's the point of saving a life if you
can't make a bundle from it? I've always said, "A life saved without extracting a shitload of
money from it, is a life lost."
I don't know that this last part needs saying, but I'm going to do it anyway. When a society
has a system built on profit, run by sociopaths, based on the manipulation of lizard-brain
impulses, then it will always end up in a race to the bottom. With unfettered capitalism we
inevitably find ourselves with the worst drugs, priced at the highest amounts, hoarded by those
who need them the least.
Unless we're talking about recreational illegal drugs. Those are cheaper than ever.
If you feel this column is important, please share it.
Feature photo | A lab technician works at the Eva Pharma facility in Cairo, Egypt, July 12,
2020, where Remdesivir is being produced. Nariman El-Mofty | AP
Lee Camp is the host of the hit comedy news show "Redacted Tonight." His new book "Bullet
Points and Punch Lines" is available at LeeCampBook.com and his standup comedy special can be streamed
for free at LeeCampAmerican.com
.
This article was published with special permission from the author. It originally
appeared at Consortium News .
Stories published in our Daily Digests section are chosen based on the interest of our
readers. They are republished from a number of sources, and are not produced by MintPress News.
The views expressed in these articles are the author's own and do not necessarily reflect
MintPress News editorial policy.
The views expressed in this article are the author's own and do not necessarily reflect
MintPress News editorial policy.
Vaccines Vaccines give broad parts of the population some level of immunity and are
considered crucial to ending the pandemic. They also take longer to develop, in part because
they must be proven to be extremely safe since they're given to healthy people. While
some researchers say a vaccine could be ready by the end of the year, others say it could
take far longer.
The vaccine is made from a harmless virus that's been altered to produce the surface spike
protein from SARS-CoV-2.
LATEST NEWS With human trials underway, the U.S. government has
pledged as much as $1.2 billion, and the company plans to produce as many as
30 million doses available in the U.K. by September. Other groups are moving to line up
access elsewhere. COMPANY Moderna Inc. NAME mRNA-1273 RECENTLY UPDATED Phase 2
Moderna's mRNA-1273 uses messenger RNA to prompt the body to make a key protein from the
virus, creating an immune response.
LATEST NEWS Moderna's vaccine produced antibodies to the
coronavirus in all patients tested in an initial safety trial. The company expects a phase 3
trial to begin July 27. COMPANY CanSino Biologics Inc. NAME Ad5-nCoV PROGRESS Phase 2
CanSino's vaccine was developed alongside China's military and is genetically engineered
with a replication-defective mutant virus.
LATEST NEWS CanSino's vaccine has received a
special authorization to be used by China's military after a study showed it generated an
immune response. President Xi Jinping says the country will make
any vaccine available as a global public good. COMPANY BioNTech SE, Pfizer Inc. NAME
multiple candidates PROGRESS Phase 2
BioNTech's BNT162 is another messenger RNA vaccine platform that the German company is
developing with Pfizer. In China, BioNTech is co-developing vaccines with Shanghai Fosun
Pharmaceutical Group.
LATEST NEWS One of the companies' vaccine candidates has shown
promising antibody responses. Further testing in up to 30,000 people may start as early as
July. COMPANY Sinovac Biotech Ltd NAME No name yet PROGRESS Phase 3
The vaccine uses inactivated virus, which can help the body develop antibodies to the
pathogen without risking infection.
LATEST NEWS Sinovac has begun human trials in China. The
company says its vaccine candidate can neutralize different strains of the virus. COMPANY China
National Biotec Group Co., Beijing Institute of Biological Products NAME No name yet PROGRESS
Phase 3
The vaccine uses inactivated virus, which can help the body develop antibodies to the
pathogen without risking infection.
LATEST NEWS With phase 2 trials complete, a vaccine
could be available as soon as the end of this year, according to an official report in May.
COMPANY Novavax Inc. NAME NVX-CoV2373 RECENTLY UPDATED Phase 2
Novavax's vaccine is meant to create antibodies that block a protein "spike" that the virus
uses to infect its host.
LATEST NEWS Novavax has received $1.6 billion from the U.S.
government as it prepares for a final-stage study as early as this fall. COMPANY Johnson &
Johnson NAME No name yet PROGRESS Preclinical
J&J is working on an unnamed adenovirus-based vaccine as well as two backups.
LATEST
NEWS J&J accelerated plans for human studies and aims to make up to
1 billion doses by the end of 2021 . J&J has said its vaccine could be ready for
emergency use by January, and it has received $456 million from the U.S. COMPANY Sanofi,
GlaxoSmithKline Plc NAME No name yet PROGRESS Preclinical
Sanofi is working on a vaccine using technology already employed in one of its flu vaccines,
which could speed development and production.
LATEST NEWS France's Sanofi has partnered with
the U.K.'s Glaxo on a project backed by U.S. funding. The companies plan to start human trials
in the second half of this year. Sanofi is also developing an mRNA vaccine with Translate Bio.
COMPANY Inovio Pharmaceuticals Inc. NAME INO-4800 RECENTLY UPDATED Phase 1
Inovio's experimental vaccine uses DNA to activate a patient's immune system.
LATEST NEWS
Inovio says an early trial showed
positive immune responses but investors complained about a lack of detail. COMPANY Merck
& Co. NAME No names yet PROGRESS Preclinical
Merck's two vaccine candidates employ exisiting technology behind its Ebola virus shot and a
measles virus vector platform discovered by the Pasteur Institute, respectively.
LATEST NEWS
Merck
has partnered with AIDS researchers to develop a vaccine using technology already employed
in its Ebola virus shot. The company has also agreed to buy biotech Themis, gaining a vaccine
candidate that uses an existing measles virus vector platform. COMPANY Imperial College London
NAME No name yet PROGRESS Phase 1
When injected, the RNA vaccine candidate delivers genetic instructions to muscle cells to
make the "spike" protein on the surface of the coronavirus.
LATEST NEWS Researchers have
received U.K. funding and have begun human trials.
Bull Gator , Jul 14 2020 5:11 utc |
73
I am a Biomedical Scientist with expertise in this area. Made antibodies and PCR tests for
a living for 35 years, I did other stuff to but I did make some World Class Antibodies and
other discoveries. My gut feeling is that all of these tests are tremendously flawed and not
reliable in any way to make any kind of decision for either the patient or society. It is
almost impossible to create a truly specific test and and it would take a considerable amount
of time and effort to get one that could be performed on large numbers of samples. At least a
year or more even with a Herculean effort. So the bottom line is it is all Bull Shit at best.
Garbage in Garbage out is what you have. Would you base anything in your life on information
that you know is inaccurate? You would have to be intoxicated, greedy or needing sex badly to
go to that place. The Scum of humanity has pushed a large number of people to that state. I
think the outcome is going to be very unpleasant for many.
A new Motherboard article interviews William, a ventilator refurbisher who's repaired at
least 70 broken ventilators that he's bought on eBay and from other secondhand websites, then
sold to U.S. hospitals and governments to help handle a spike in COVID-19 patients.
He's part of a grey-market supply chain that's "essentially identical to one used by farmers
to repair John Deere tractors without the company's authorization and has emerged because of
the same
need to fix a device without a manufacturer's permission ..." The issue is that, like so
many other electronics, medical equipment, including ventilators, increasingly has software
that prevents "unauthorized" people from repairing or refurbishing broken devices, and
Medtronic will not help him fix them... Faced with a global pandemic, hospitals, biomedical
technicians, right to repair activists, and refurbishers like William say that medical device
manufacturers are profiteering by putting up artificial barriers to repair that drive up the
cost of medical care in the United States and puts patient lives in danger. They describe
difficulty getting parts and software, delays in getting service from "authorized" technicians,
and a general sense of frustration as few manufacturers appear ready to loosen their repair
restrictions during the COVID-19 crisis.
For the past decade, medical device manufacturers have refused to sell replacement parts
and software to hospitals and repair professionals unless they pay thousands of dollars
annually to become "authorized" to work on machines. The medical device industry has
lobbied against legislation that would make it easier to repair their machines,
refused to release repair manuals , and
used copyright law to threaten those who have made repair manuals available to the public.
The technicians who are unable to gain access to repair parts, manuals, and software are not
random people who are deciding on a whim to try to fix complex medical equipment that is going
to be used on sick patients. Hospitals and trained professionals are regularly unable to fix
the equipment that they own unless they pay for expensive service contracts or annual trainings
from manufacturers.
While hospitals deal with a resurgent coronavirus that is overtaxing intensive care units
across the country, their biomedical technicians are wasting time on the phone and in
Kafkaesque email exchanges with medical device manufacturers, pleading for spare parts,
passwords to unlock diagnostic modes, or ventilator repair manuals.
The Great Covid-19 Deception and What You Need to Know to Survive
GARY HEAVIN JULY 10, 2020
1,600 WORDS
74 COMMENTS REPLY Tweet Reddit Share Share Email
Print More RSS
I've been speaking with my friends who include medical doctors and other highly educated
people about the treatments that they would seek if they were diagnosed with Covid 19. Most of
them had no idea what course of treatment they or their families might seek. This conundrum is
in part due to the massive volume of information that is being thrown at us. Much of this
information is deliberately deceptive. I am writing this article to cut through the deception
so that you and your physician can make informed decisions if and when the time comes.
This article has two purposes. First, it's imperative that you understand the great deceit
that Big Pharma, their minions at the FDA, CDC, NIH, the WHO, the MSM, and officials in high
government positions are perpetrating on you, your family, and likely your doctor.
The second purpose is to assure that you are armed with the necessary information to insure
that you receive the best treatment options from your health care provider. Knowledge is
power.
Allow me to repeat, you need to know you are being duped and you need a plan for you and
your family if you become infected with Covid 19. So let's get to it. Let me begin by stating
that I'm not a medical doctor and I m not offering medical advice. I do have a bachelors of
science degree in health, nutrition, and counseling. I've written two NY Times bestselling
books on women's health and fitness and I have been awarded an honorary doctorate degree.
However, you will need to determine your treatment options with your personal physician.
The Great Deception
When it comes to safe, effective and affordable therapies for Covid 19, Big Pharma and its
agents, i.e. Dr. Fauci and Dr. Birx and many others, appear to have an agenda to lie to you and
your physician.
The most obvious example is their ongoing effort to ridicule the treatment option of
hydroxychloroquine, Azithromycin, and Zinc. We've all watched the harsh criticism that
President Trump received when he promoted this protocol for Covid 19.
So, hydroxychloroquine has been around for almost 70 years as a treatment for malaria,
lupus, and rheumatoid arthritis. The WHO has designated it as a safe and effective medication
akin to taking an aspirin. A survey of 6,000 medical doctors affirmed it as their treatment of
choice for Covid 19.
The treatment works like this. hydroxychloroquine is an ionophore, which means it can
transport material through the cellular wall. Zinc is a mineral that stops the replication of
the Covid 19 virus within the cell. hydroxychloroquine transports Zinc into the cell so that it
can stop the replication of the virus. The Z-pak antibiotic is given to prevent opportunistic
bacterial infections like pneumonia that can occur while your immune system is engaged in
fighting your viral infection. The key to its effectiveness is to start this treatment at the
early onset of Covid 19 so that it has time to work.
How much effort has Big Pharma put into subverting this treatment regimen? In addition to
denouncing its effectiveness, from Dr. Fauci and company, constant MSM hit pieces, the
censoring of medical doctor's articles and videos from the internet, there has also been a
number of "studies" done that were literally sabotaged from the onset.
The VA hospital system reported in March that they had given hydroxychloroquine to a number
of patients. Following their release of information, the MSM ran the story with the headlines,
"VA hospital found that hydoxychloroquine doesn't work and increases the fatality rate of Covid
19." However, if you actually read the study (see
link ) you will find that only the sickest of the cohorts were given the drug. They got the
drug only after they were so far along that it would not have a chance to work and they were
not given zinc. None of these details made the MSM articles.
Another example of the Great Deception came from the British medical journal, The Lancet.
The Lancet reported that a meta study showed that hydroxychloroquine was ineffective. As a
result of this published study, France, Italy and other European countries immediately
prohibited the use of this treatment option. Within a few weeks,
it was found that the study was so badly designed and that the results were literally
fabricated . The Lancet was forced to make a retraction of the "study." Of course in the
meantime the MSM ran the original Lancet story and mislead millions of people and their
physicians.
So what could possibly be the motive behind Big Pharma's Great Deception. Well there's three
answers, money, money and money. That brings up the treatment option that Big Pharma is
promoting, Remdesivir. This lovely experimental drug, costs above $3,000 per regimen, must be
given intravenously in a hospital (five days stay around 15 grand) and
evidence shows it doesn't really work .
The other treatment option is the promised Covid 19 vaccine that they allege is forthcoming.
The NHS in Great Britain has committed to purchase a vaccine for the entire population of Great
Britain. That's a commitment of 80,000,000 doses at an agreed price of around $600 for each
vaccination. That's about $50,000,000,000. (50 Billion) That's a lot of incentive to mislead
people. This week, a US pharmaceutical company received $1.6 billion dollars towards their
efforts to make this vaccine which in the opinion of many experts, won't work on a coronavirus
and will be untested and experimental.
How does Big Pharma have
so much control over the dissemination of this information or should I say propaganda?
Well, the same answer pops up again, money. Big Pharma gave $2 billion dollars during the last
election cycle to US politicians. Big AG, the military/security complex and big oil each gave
only a paltry $1.0 billion dollars to buy the votes of our political leadership.
The MSM counts Big Pharma's advertising revenue at up to 80 percent of their income. The
internet's "masters of the universe" also kowtow to Big Pharma's influence and advertising
dollars by censoring anyone who tries to tell the American people the truth about Covid 19. It
certainly appears that anyone who is complicit in this Great Deception, a deception that is
designed to kill and terrify enough people to ultimately beg for an experimental vaccine, well,
these people would be accessories to murder.
What You Need to Know to Survive
Now, for some good news. There are several therapies that are being offered that appear to
be safe, effective and affordable. However, these therapies must be utilized early in the
disease progression.
Budesonide
Japan, Taiwan and other Asian countries have maintained a much lower fatality rate with
Covid 19 then we have here in America, in spite of the fact they live in densely populated
communities. Many people believe that it is due to their preferred method of treatment. They
use a steroid medication that is inhaled in a mist through a home use nebulizer. I'm familiar
with this since my 2 year old granddaughter needed this treatment with a similar drug for an
upper respiratory issue that she had recently. That speaks to the safety and the commonality of
this treatment. Watch the link of a
Texas doctor who shares his patient's experiences with this therapy method using the drug
Budesonide and a course of antibiotics.
Ivermectin
Another treatment option that appears to be safe
and effective is the use of the antiparasitic drug Ivermectin with the antibiotic
Doxycycline. Just one Ivermectin pill and then the course of antibiotics for ten days resulted
in a 100 percent cure rate for Covid 19 patients according to the attached study. Ivermectin
has been widely used on the continent of Africa for many years as an anti-parasitic and is
believed to be a primary reason that Covid 19 has not severely impacted the African
population.
Hydroxychloroquine & Zinc
As we've seen above, this therapeutic regimen should be considered simply due to the
efforts to prevent you from knowing the truth about it . As Shakespeare wrote, "Doth thou
protest too much?"
The challenge with this therapeutic is both finding a doctor who will prescribe it and
finding a pharmacy that will sell it. This should be between you and your doctor. Not the
governors of certain states. Considering that 20 percent of all drugs are prescribed "off
label", meaning that they are prescribed for a use other than intended, you and your doctor
should have the liberty and the responsibility to make this health care decision.
There are several other therapies that appear to be safe, effective and affordable. You may
want to research Chlorine Dioxide, intravenous ozone, high dose intravenous vitamin C and
another, glutathione which are popular treatments in the homeopathic communities.
As for me and my family, we are going to make informed and responsible decisions regarding
our health care. I hope the information I've given to you today along with the links for
further information will help you, your family and your doctor make the best decisions as
well.
Gary Heavin and his wife Diane are the founders of Curves, the world's largest fitness
franchise. Gary is the author of two NY Times bestselling books, Curves and Curves on the go.
Gary co-wrote and starred in the movie Amerigeddon. Gary is a pro-life libertarian and serves
on the advisory board of Dr. Ron Paul's Institute for Peace and Prosperity. Gary and his wife
are philanthropists who feed 10,000 children a day in Haiti and operate an orphanage outside
the slums of Mumbai. Most importantly, they are bible believing Christians.
Anon [694] Disclaimer
July 11, 2020 at 4:42 am GMT
Excellent article. Early treatment is definitely key. The French doctor who recommended
hydroxychloroquine way back in Feb. said that it needs to be given early, by the time they go
on ventilator it's no longer effective. I read in Zerohedge last week that in TX, doctors
said they simply give patients who come into the emergency room a steroid shot and send them
home with antibiotics. Usually they are already feeling much better after the steroid shot.
Even those who are hospitalized are now only staying 3-5 days.
I find it incredulous that on their website, CDC is still telling people to stay
home if they are sick, that "many people" get over it themselves without treatment, and
to *not* go to the doctor's until we are having difficulty breathing. By then it is too late!
Doctors have said that the main difference btwn Covid patients and flu patients is, with a
flu patient, when their lungs are 10% fluid, they are already having difficulty breathing,
but for some reason for Covid19, the patient does not have difficulty breathing until the
lungs are 50 to 60% fluid, which is why it's too late by the time they sought treatment.
This article discusses the low fatality rate in HK(0.4%) and Singapore(<0.1%), the
doctors there attributed it to early treatment using a different cocktail of drugs:
interferon beta-1b, which was developed to treat multiple sclerosis; ribavirin, which is used
in the treatment of hepatitis C; and lopinavir-ritonavir, also known by its brand name,
Kaletra. But again, early treatment is key.
https://www.msn.com/en-sg/news/singapore/how-hong-kong-singapore-kept-coronavirus-death-rates-low/ar-BB14CLbM
CDC is an absolute fail. I'm beginning to believe they want more people to die so Trump
would lose the election. They need to change their advice on their website before more lives
are senselessly lost. Pence as the Covid Tzar is also totally failing on his job by not
calling him out.
I'm also beginning to believe those who claim hydroxychloroquine doesn't work simply want
to keep it for themselves and their cronies to take as preventive drug. Trump has been on it
and he hasn't gotten sick, even though he's been exposed to lots of people. Something tells
me many of our congress critters and the effing Jews are already loaded up on it.
Anonymous [426] Disclaimer
July 11, 2020 at 4:50 am GMT
I can't wait for November 4th when COVID-19 ends for good and all the masks and social
distancing bullshit ends. Thankfully this C-19 psyops will last just 8 months and not the 2+
years the Russian collusion BS was drawn out to. Though sadly with the former it has further
eviscerated working/middle-class America. I'm guessing that was part of the plan as well.
Quinsat
July 11, 2020 at 5:24 am GMT
The great Covid deception is it hasn't fulfilled Koch's postulates.
Smokey
July 11, 2020 at 5:51 am GMT
I believe Mr. Heavin more than I believe the government, and the CDC in particular.
But that could also apply to a Numerologist vs the gov't, so there's that.
I don't believe Jeffrey Epstein died a natural death any more than I believe the
mainstream media is the least bit impartial. They used to try. They tried to keep the news
and the Op-Ed pages separate. But that was then and this is now
This is getting fun!
So, I used to believe that cops were always the good guys, and that federal judges
were above politics. Oh, and they would never lie, or take a bribe. And I believed that
priests would never, ever molest a boy, or even girl (did I get that backward?), or even use
bad words around them. And I believed Scoutmasters took Boy Scouts up into the mountains for
the fresh air and Indian lore OK, this is starting to sound ridiculous.
Except, now I'm not sure what to believe any more.
Can anyone tell me ?
Chris in
Cackalacky
July 11, 2020 at 5:57 am GMT
@Kirt
No offense but do you know how many people claim to have had Covid before Covid was cool?
I don't know anyone who has tested positive but I know 25 people who claim they had or have
it. In the past three years there have been severe influenzas making the rounds, there is no
denying that. And why should routine flu and colds take a holiday just because our criminal
elites tell us there is a special disease we need to watch out for? My point is we are so
deceived that nobody knows up from down anymore. But at least we know one thing for sure --
hostile elites are working to deceive us.
Achilles
Wannabe
July 11, 2020 at 6:33 am GMT
My doctor suffers from a delusion common to her profession. She thinks she is a "Medical
Scientist". Actually she is a retailer for pharmaceuticals and medical technologies. She is a
sales person in a capitalist industry And should she have any questions about her real role
in a health care field which is really a substance and med tech pushing industry, her
colleagues – fellow sales people – will remind her of her professional
obligations by threatening her board certification to insure her near absolute conformity to
market standards.
But there is no getting her to understand her real role in the medical industry. She
believes her own hype or the hype created about her profession back in the 1950s when a few
genuinely useful drugs and technologies were discovered which then afforded the money making
corporate establishment the opportunity to take a humane craft and, thru the "science" of
Epidemiology -Medical speak for lying with statistics – turn professional Medicine into
probably the largest boondoggle in history. Consider the flag ship for usurious medicine
– cholesterol lowering statin drugs.
But why don't I get rid of my essentially brain dead doctor, go to to someone else?
Practically speaking, there is no one else. There are doctors who understand all this and
write books about it but they are so rare as to be useless when real sickness like bacterial
infections for which there are useful technologies like antibiotics actually occur. The most
useful thing these real scientific doctors have to say is "Don't see your doctor" unless you
have a real emergency – like an old fashion visceral type sickness – as opposed
to some epidemiologically hyped condition like, again, "high cholesterol" as the "cause" of
heart disease.
But now we have a genuine epidemic that is killing and injuring people and Medical Science
is lying to us about possible treatments. Even a Medical skeptic like myself could not have
predicted this level of base greed by our Medical pharmaceutical establishment This is
tantamount to MURDER. And we have no government -whether it be run by Democrats or
Republicans- who will take action. They are all on the Med Pharm tit and/or deluded by
"Medical Science" as well. Until we learn to help ourselves and overthrow this system, God
help us
Valka
July 11, 2020 at 6:48 am GMT
$50 billion just for Britain America doesn't stand a chance.
TheTrumanShow
July 11, 2020 at 6:58 am GMT
Thanks, Gary.
I've been reading everything counter-&-alternative to the deception I could find since
it first appeared, but had never thought to investigate therapies until reading your article.
Fortuitously, for me (in Thailand), Hydroxychloroquine is being used therapeutically and may
even be available OTC.
However, Big Medicine & Big Pharma are already here and steadily making inroads into
health care and medicine.
Gleimhart
Mantooso
July 11, 2020 at 7:10 am GMT
Whatever happened to that vaccine that some Israeli Genius Doctors claimed would be ready
in a few weeks, which was months ago now? What a shock that that never materialized.
Trygve
Blodøks
July 11, 2020 at 7:38 am GMT
You should also look into coodial silver water. I got rid of an hpv infection using it. No
side effects.
Herald
July 11, 2020 at 9:14 am GMT
The author doesn't mention Vitamin D, which is rather strange.
skrik
July 11, 2020 at 9:29 am GMT
@Gary Heavin
The Great Covid-19 Deception and
Click-baitish, much? Well, you got me in, but you seem to have a good 'treatment'
argument, and 'good luck,' both by avoiding Covid-19 in the 1st place and finding a
'collaborative+pursuasive' Dr in the 2nd = worst case, should you or one of yours gets 'hit.'
[Perish the thought.]
But IMHO, the Great est Covid-19 Deception is the negligent way most
'Western' governments have *not* taken Covid-19 properly seriously, starting of course with
US = Trump and UK = Johnson then perhaps SE 'led' by so-called expert Tegnell next in a
looong list of apparent delinquents.
Again IMHO, when Wuhan realised that they were under a bio-warfare-like attack [possibly
when they 1st saw the PRRA inclusion in the decoded genome], they reacted like cut snakes and
proceeded with the speed of fear-stricken Gazelles in a very largely successful attempt to
*suppress* the virus. But, of course, they are communists, eh? So-called 'democratic'
[in-name-only governments, many largely bolshie 'wo/men in the street'] think differently
[even to their own detriment; they just can't help themselves.]
With the possible exception of NZ = Ardern, most 'Western' governments went for
'mitigation' = 'flattening the curve,' if they took any action at all, see BR = Bolsonaro
"has accused the media of "fear-mongering"" and IIRC said something like "What can
I do?"
Here is an article, 1st found by me in March on MoA
:
"Coronavirus: The Hammer and the Dance"https://medium.com/@tomaspueyo/coronavirus-the-hammer-and-the-dance-be9337092b56
MoA blurb: 'Here is his latest in which he argues not only to "flatten the curve" but to
eradicate the virus.'
For my last IMHO, all 'Western' leaders who have acted with less than full effort =
incompetently meaning ineffectively on behalf of their 'own people' should be prosecuted for
their negligence. rgds
GeeBee
July 11, 2020 at 9:34 am GMT
A good article all around, except that the population of the UK is nowhere near eighty
million. The latest figure I can find gives 66 million. Also, your attempt to invoke the Bard
('As Shakespeare wrote, "Doth thou protest too much?"') is lamentably botched. Try 'Methinks
the lady doth protest too much'. (Hamlet's mother Gertrude says it of what she regards as
overacting in a play that Hamlet has arranged for his mother and her husband, the usurper
Claudius, to watch).
Justvisiting
July 11, 2020 at 10:37 am GMT
It is a great idea to have a candid discussion with your doctor/nurse on the issue of big
pharma's economic power and how it creates conflicts of interest in the medical
profession.
Many doctors/nurses already knew it and will quickly agree, many more "get it" after you
explain it to them.
If your doctor is so brainwashed by "experts" that they think you are an "anti-science
kook", time to get a new doctor!
gotmituns
July 11, 2020 at 10:40 am GMT
@Kirt
Bingo – it's all a total bunch of malarkey. All the BS isn't aimed at people our age
(I'm 76), it's aimed at the milennials and younger. It is shaping them for the "Brave New
World" that they will live.
Simon
Tugmutton
July 11, 2020 at 10:48 am GMT
First let me say that the virus has never been satisfactorily isolated and does not meet
Koch's postulates, which leads some people to speculate that it does not exist at all. The
symptoms are so various as to be nonsensical; whatever the virus may be, last winter, that
led to all the hospitalizations is open to question. Certainly the fear-porn spewed out 24/7
by the corporate media led to high levels of anxiety among the credulous and many of these no
doubt presented as Covid-19 patients even though they were in fact suffering from the flu or
a bad cold. Once in the hands of the quacks, nosocomial infections and intubation really made
them sick – or dead.
As for protection against any respiratory illness, vitamin D is essential and I am
surprised the author fails to understand this. 4000 IU per day maximum.
All that aside, Covid-19 a gigantic psyop designed to usher in a world government. It was
even rehearsed in 2019 and all the wrinkles worked out beforehand.
[MORE]
Mark G.
July 11, 2020 at 10:56 am GMT
If you can't get hydroxychloroquine there is some evidence that the natural substance
quercetin found in apples and onions can act as an ionophore that transports zinc into the
cell. Instead of the z-pak, a natural antibiotic like oregano or cinnamon oil might suffice.
These items quercetin, zinc and oregano and cinnamon oil are all available down at the local
health food store. There is more evidence for the hydroxychloroquine, zinc, z-pak combination
so those would be the preferred combination if you can get them but these natural substances
might help if you can't get them and might act as a preventative to keep from getting the
virus if you use them regularly.
I have found only a few studies that support the use of these natural substances but you
need to understand that since these aren't drugs they can't be patented so there isn't the
same financial incentive to prove their effectiveness as there would be with drugs that can
be patented and then sold exclusively by one company.
UncommonGround
July 11, 2020 at 10:59 am GMT
Whether hydoxy/chloroquine works or not is something that will be clear only after there
are studies that allow to take a final conclusion. The question has been discussed critically
by the press, by medical doctors, by people. Of course, everybody knows that it's possible
that no vaccination will function or be available (we can hear this everyday on television).
Contrary to what the author says, a phamaceutical firm was happy that the medicament could be
possibly used when the question came up and some people were optimistic about it. The web
site of a German television wrote in may that it was still conceivable that hydoxychloroquine
could work in the very early stages of the disease (after first negative results). This was
only speculation.
The author mentions a talk with some friends of him and some information that he has. But
there have been a few studies, good or bad, with chloroquine with negative results. The study
of the Lancet was taken back because the data that they used was apparently not trustworthy.
This shows how difficult it is to have good and conclusive results in a short time. We can
say the same about the evidence used by the author. It doesn't mean very much. We still have
to see what happens and until now we don't know. There are efforts to find ways to treat
better the disease. In German, I read yesterday:
https://www.swr.de/swraktuell/baden-wuerttemberg/mannheim/heidelberg-neue-corona-behandlungsmethode-100.html
chuckywiz
July 11, 2020 at 11:15 am GMT
The media never talks about those who recovered from Corona virus like BOJO, the prime
minister of UK or others. What treatment the recovered patients received, how it helped them
and other information. We hear only the scary stuff.
"DR" Bill Gate of MS is an expert of globalized vaccination and his articles on the
subject have been published in several Medical Journals.
Linux_tyro
July 11, 2020 at 11:31 am GMT
I was diagnosed with an upper respiratory infection in April. Was given a Z-pack for 5
days, an inhaler, Albuterol Sulfate that I am going to refill and a pill for cough,
Benzonatate 200mg. They tested me for Flu, Pneumonia, Strep and Covid. All test came back
negative.
Now I have a sinus infection and was prescribed another Z-pack with Prednisone 250mg twice
a day for five days.
I've been feeling under the weather for months now.
Oh! Now I remember my question. How much zinc daily should we be taking?
Emslander
July 11, 2020 at 11:39 am GMT
So, now we know who the enemy is. When can we start arresting and executing them?
I've had a condition common to old men for a long time. I went to some MD from the Far
East who started immediately talking about cutting me up. I went to a second doctor, a young
American, and told him I guess I needed to be sliced and diced. He said, "Not so fast" and
recommended the regular use of two substances I could get at the vitamin store. I did so and
the matter improved to the point that I felt effectively cured.
Last week, I went back to him. He works at a large establishment that includes my regular
MD. I started telling him about how miraculous and enlightened his advice was. He quickly
shut me up and started talking about operations and antibiotics. He wouldn't even listen when
I told him that his earlier advice had worked. My presumption is that the financial people
got to him. I'd guess that they do a regular review of medical care by each physician to see
how they can better monetize their practice. Anyway, his changed tone was remarkable enough
that it had to be something like money that was involved.
mark tapley
July 11, 2020 at 11:47 am GMT
Covid 19 is just another in a long line of fake or hyped up illnesses. Remember H1N1,
H5n1, SARS1, Swine flu, Bird flu, Zika and others. AIDS was another fake disease (read Dr.
Peter Duesberg on this). The same type of hoax is being perpetrated with the current Corona
"epidemic."
Notice it supposedly began in Wuhan China. This city of 11 million has the worlds worst
air pollution. 350,000 people per year die of pneumonia in China. There are lots of people
there that can be tagged as Covid 19 victims. Also quickly touted as a hot spot by our Jew
controlled MSM was deaths in Italy. Official autopsies revealed over 99% of victims had pre
existing illness, most of them had multiple ones at an avg. age go 69.5. Latter the age went
up but I can't remember the exact figure. Remember CDC criminal Debra Brix said "we have told
the hospitals to tag everything possible as Covid 19."
Remember the fake tents set up all over and the hospital ship that looked like a relic of
WW1. The MSM kept talking about overflowing hospitals. Several people took videos of near
vacant hospitals at this time including Brian Ruhe's exposure of Vancouver's practically
empty hospital. Whenever you see the media jump all over something with all the official
spokesmen and there is no alternative opinion allowed, you known it is a gov. false flag. All
of a sudden climate change is no longer the critical topic of the day. I guess Greta Thunberg
got the covid.
The covid 19 has never been identified by the standard scientific method of the Koch's
postulates because they can't. If you have a fake virus you must have a fake test. That is
the PCR test that gives ap. 200 false positives, does not determine one Corona (cold from
another) and is not quantitative is a fake test. The numbers given by the CDC (holds 50
vaccine related patents) that is really an adjunct of big Pharma are a crock of baloney. Most
of these figures are generated from old people in the nursing homes that are given a "visual"
conformation as having covid. Note that Fauci said in February that the masks did more harm
than good. Hospitals get paid big money for labeling patients as Covid victims and many times
doctors just write it on the report.
The Zionists have hit a home run with this medical hoax and they will never give it up
unless the cucks start using their brain a little bit and figure some things out. The next
move will be manditory dangerous vaccines for all the cattle. There is big money to be made
in the vaccine scam. To get the truth on vaccines read Dissolving Illusions by Dr. Suzanne
Humphries and books by Forrest Maready.
The Covid scam has been planned for many years, this was an opportune time to spring it as
a cover for the central banks theft of trillions more while bankrupting the workers and small
businesses. The Jews at Blak Rock are big investors in masks and will now be scooping up
failed businesses everywhere just like in 08.
Emslander
July 11, 2020 at 11:47 am GMT
@Smokey
Except, now I'm not sure what to believe any more.
Can anyone tell me ?
My uncle told me a story a long time ago about a man who had his young son climb a tree in
the back yard. He let him get pretty high and then said, "Jump Johnny, Jump!" Johnny said,
"If I jump, I'll get hurt." The Dad said, "No, I'll catch you." Johnny jumped and the Dad did
nothing. The boy hit the ground and was crying, though not permanently injured.
He said to his Dad, "Father, you promised to catch me."
"Let that be a lesson," the Dad said. "Don't trust NOBODY."
Brás
Cubas
July 11, 2020 at 12:03 pm GMT
Gary is a pro-life libertarian
Well, seeing as libertarians are against government action to stop abortions, I suppose
all that a libertarian who opposes abortion is allowed to do is acting against it in their
private life; seeing as that is exactly what the pro-choice option means, you see that Gary's
position is rigorously meaningless: he is pro-life and pro-choice at the same time.
That is a really grand deception, regardless of any other claimed by this article, and all
I need to know about it.
Giancarlo M.
Kumquat
July 11, 2020 at 12:17 pm GMT
Stop feeding those Haitians!
St-Germain
July 11, 2020 at 12:24 pm GMT
Thanks for your article.
I also prefer plain facts to eloquent fiction (MSM). Your article has obvious practical
value for the public. It's a keeper. I also hope it circulates widely as an effective
antidote to virulant MSM viruses.
BTW, my first act following retirement from four decades of professional news writing was
to cancel all newspaper and magazine subscriptions. There is no utility in paying to be
misinformed.
It never ceases to amaze me that so many people who have never set foot in a news room now
regurgitate MSM propaganda as though it came down from Mt. Sinai. MSM journalism has now run
the gamut from the duty to reveal what is true, even if it hurts, to the need to say what
sounds nice, even if the reporter himself doesn't believe it. That's the definition of
PR.
anonymous [400] Disclaimer
July 11, 2020 at 12:29 pm GMT
When this wears thin they'll discover another killer virus and there'll be another
go-round. They started off saying the lockdowns were just for a brief time and then when they
got their foot in the door it was extended. Now government herding people around by diktat is
a permanent feature of American society. They'll never let it go. There's already been some
report of some other mysterious killer virus coming out of Kazakhstan so get ready. This is
the largest transfer of wealth scheme ever, the assets of the bankrupted scooped up by the
big companies.
An Easterner
July 11, 2020 at 12:38 pm GMT
'Most importantly, they are Bible believing Christians.'
That for me, as a Muslim, is the best guarantee that the person writing this article will
have written all in good faith because he or she is answerable to God.
Overall, the article was very informative and pertinent to the situation we face
today.
macilrae
July 11, 2020 at 12:47 pm GMT
The article cites imperfect studies in which hydroxychloroquine was found to be an
ineffective therapeutic for COVID19 – imperfect because the treatment was generally
started too late in the progression of the disease. The author postulates that, if treatment
were begun earlier, mortality would be drastically reduced but, unfortunately, there is no
study to support this and the majority of people suffering the symptoms of early-onset
COVID19 will recover spontaneously anyway.
Singapore, with its superb bureaucratic infrastructure, has reported over 45,000
infections but only 26 deaths – that is 4 deaths per million population. South Korea
reports 13,000+ deaths and 287 deaths (6 per million population) and Japan 20,000 cases and
981 deaths (10 per million) compare this to the USA with 364 deaths per million or the UK
with 718.
I have yet to see a convincing explanation of these shocking differences and, when asked
recently, a British government spokesman said that it is "too early" to start drawing
international comparisons – "too early" for whom you might ask? Evidently not for those
who have succumbed – by now a huge effort should have been put forth to account for the
disparity – even if the explanation is demographic as is being largely claimed. I
assume that national pride has stood in the way of seeking answers by sending study teams to
these countries.
The article recounts a number of inexpensive treatments that might work and points
to "Big Pharma" as the major reason these are not being systematically studied – that
may well be an impediment in the USA particularly – so gathering of data from East
Asia, where that influence is far less and where dramatic positive results are seen, is all
the more urgent.
Meanwhile my family will wear masks and hunker down because we have no particular plan to
implement if one of us catches this bug.
Butch
July 11, 2020 at 1:01 pm GMT
Here is a clue, stop doing ALL the things they tell you to do because its all designed to
make you sicker. Eat real food, so many people just don't get it, its garbage in and garbage
out. Curves have always been flattened by the healthy freely moving about [oops, stay home],
health from being outside, in the sun, and amongst nature is vital [oops stay inside], eating
good REAL food is how you have a good immune system [oops, dont want that we need sick people
for the pharma devils, therefore we'll allow FAST [shit] FOOD to be readily available [no
contact of course [OMG can you actually believe this crap?] Wear a mask because the covid
devil lurks everywhere [oops, retard the flow of healthy oxygen into your body, breath back
in your own exhalations of CO2 and bacteria so you can increase your odds of getting sick,
you just cant make this twisted stuff up!!!] Social distance, thats the best one? We should
be wanting to be social for many many reasons, the least of which is because we ARE social
animals, but the best way to flatten any curve is, as previously stated, assimilate it [as
humans have with all viruses] to develop herd immunity [something that you CANNOT get with a
toxic vaccination], like Sweden and Japan. STOP watching MSM and social platforms removing
truth. Actually STOP watching TV, its all designed to make you think a certain way.
Off The
Reservation
July 11, 2020 at 1:06 pm GMT
The biggest problem with this article is that it does not address the fundamental basis of
the fraud that is CV19.
The Chinese supposedly identified a new coronavirus and named it SARS-CoV-2.
Then, the WHO made a vague list of symptoms and created a syndrome called COVID19.
There is no proven connection whatsoever between the supposedly identified virus and the
syndrome.
Billing codes were created that allow the assumed or tested diagnosis of CV19.
To make matters worse, a test was created which only tests for "markers" of coronavirus
and has never been proven to connect to the above viruses or the above syndrome. Thus testing
positive or negative really has no meaning as proven by the disconnect between symptoms and
diagnosis.
Then, the government incentivized and instructed the use of the above billing codes and
created the commonly known situation of people dying "with" the syndrome even though they
died of other causes.
Add to that the manipulation of the case count, etc. Then, you have New York and New
Jersey basically murdering people with treatment. Loved ones banned from visiting homes
– for reasons they might bring the virus in – while "positive" sick patients are
brought in. Reconcile that.
I am not saying a few people aren't sick, but there is no way to deal with something while
these language tricks are going on.
The virus, the syndrome, and the tests, and the count of cases have no scientific
connection to each other. What is it you are talking about being treated for? The flu?
CW2isComing
July 11, 2020 at 1:14 pm GMT
@Gleimhart Mantooso
Yes, where IS that Wonder of Modern Medicine anyway? We were breathlessly told of its
soon-to-be release; I even thought that it was peculiar that the Israelis were so
serendipitously working on just the right strain of coronavirus as to be in the forefront of
vaccine development.
Miracles happen.
Except when they don't. And, to summarize here, there has NEVER been a stable/effective
vaccine for the coronavirus family of viruses. NEVER.
As in, NEVER.
Adûnâi Website July 11, 2020 at 1:22
pm GMT
@skrik bio-warfare-like attack [possibly when they 1st saw the PRRA inclusion in the
decoded genome], they reacted like cut snakes and proceeded with the speed of fear-stricken
Gazelles in a very largely successful attempt to *suppress* the virus. But, of course,
they are communists, eh?"
Finally some sense in the sea of conspiratards. It is fascinating to observe the insanity
of White nations – they will cling to their clearly delusional beliefs to the end, even
when an alternative is presenting itself this whole time.
Wearing a mask apparently turns you into a slave. Believing in the existence of the virus
makes you a shill. Pure anarchism, just without the bombs.
The comment #19 by UncommonGround is decent as well.
anon [327] Disclaimer
July 11, 2020 at 1:25 pm GMT
Best cure for C-19: Put Dr. Fauxci and Dr. Birx , ilk,
Doesn't need to be a big ship.
CW2isComing
July 11, 2020 at 1:35 pm GMT
@Mark G. As well (and mentioned in some of the above comments) there are many studies
indicating that adequate levels of Vitamin D may be protective. Best source: sunlight; then
fresh fish, then supplements.
The entire point of this article is "self-rescue." It is clear to me that the "official"
recommendation is to "stay home, don't come to your doctor's office/E.R. until you get
shortness of breath, etc." so as to not "overload the hospital system."
The latter advice will get you killed if you are elderly and/or have certain
co-morbidities. Treat yourself early on, be proactive towards you health; oh, also, maybe
stop shoving Cheetos down your neck, take a walk, lose some weight?
anon [624] Disclaimer
July 11, 2020 at 1:48 pm GMT
@skrik
Moon of Alabama is a controlled website that censors dissenting commenters. The Covid-19
has completely blown the cover of that site and Mr. 'b'. Do not push that site. This
unz.com site does not censor comments. Get
back to us when Mr. 'b' (or is that German Intelligence?) decides to play his role properly
again.
Gary Heavin
July 11, 2020 at 1:58 pm GMT
@Herald
Hi Herald,
Twodees
Partain
July 11, 2020 at 2:04 pm GMT
@Quinsat ch's postulates.
That's the main point of information needed if "need to know" is at the top of the list on
how to survive. A person "diagnosed with covid19" should know that the existence of this
"novel coronavirus" has not been established in any way that is based in actual science.
Such a diagnosis subjects the purportedly infected person to treatments that would be, at
best, useless. Diagnosis is the starting point for a political assault conducted by means of
"contact tracing" prescribed by an Israeli intelligence operation, and can't possibly include
any effective medical treatment.
No medical treatment exists that can cure infection with an imaginary virus.
Gary Heavin
July 11, 2020 at 2:06 pm GMT
@GeeBee
Thank you for your corrections. When I found out that Ron was going to post my article on
this website I was very excited due to the quality of its readership. People like you.
Really No
Shit
July 11, 2020 at 2:08 pm GMT
A chinaman told me that lots of chopsuey with exotic wild animals worked for his country,
whereas a wetback told me lots of beans and rice with hot sauce was the key to their success.
Here in my neighboring neighborhood, the Borough Park, I hear that bubbies are offering up
matzo ball soup with a scrawny chicken thrown in and the Bensonhurst Fredos are insisting
that had the Italian government not abandoned the age old custom of over eating pasta
fagioli, none of those paisans needlessly would have died. So, who do you believe?
Gary Heavin
July 11, 2020 at 2:10 pm GMT
@Linux_tyro
25 mg of zinc daily is what I take
Agent76
July 11, 2020 at 2:19 pm GMT
July 9, 2020 CDC May Officially Downgrade COVID From An 'Epidemic'
The coronavirus mortality rate in the United States has dropped so low that the Centers
for Disease Control and Prevention may soon stop calling the virus an "epidemic."
https://principia-scientific.org/cdc-may-officially-downgrade-covid-from-an-epidemic/
Twodees
Partain
July 11, 2020 at 2:32 pm GMT
@Emslander
"the regular use of two substances I could get at the vitamin store."
What two substances?
Alfred
July 11, 2020 at 2:39 pm GMT
@Anon
I'm beginning to believe they want more people to die so Trump would lose the
election.
I am surprised it is taking people so much time to work that one out.
The media don't want you to see this chart. That is why I won't stop shouting
CASES
Anonymousse
July 11, 2020 at 2:53 pm GMT
I had symptomatic corona. It was a day and a half of mild fever and fatigue. Basically
like the flu but not nearly as bad. Everyone else I've known that had symptomatic corona
(already a small minority of those who actually got infected woth corona) experienced the
same or even less.
If you're just about to die from something else anyway, yeah maybe such a mild disease can
give you that last little push. At that point you need to be thinking about saying confession
and your relationship to eternity not some magic drug extending your life another few
months
It's just the flu bro.
Desert Fox
July 11, 2020 at 2:54 pm GMT
Coronavirus is one of the biggest scams, frauds, psyops, mass hypnosis, in history, see
these sites for the truth about the coronavirus scam, henrymakow.com , thetruthseeker.co.uk, chuckbaldwinlive.com , thedollarvigilante.com .
Alfred
July 11, 2020 at 2:55 pm GMT
@Gleimhart Mantooso aled that they had designed a vaccine and tested it on hamsters. They
wrote that a single dose "was able to protect hamsters against SARS-CoV-2."
Their best shots: Israeli efforts to invent a coronavirus vaccine, explained (Times of
Israel)
You can be absolutely certain that the clowns above removed their masks as soon as they
were off-camera.
Trinity
July 11, 2020 at 2:58 pm GMT
The (((CoronaRona?))) Well, put it this way, the same people pushing the (((CoronaRona)))
story or the same people who told you that Germans gassed 6 gatrillion Jews in the
"holocaust." You might have a better chance at seeing Santa Claus than dying from the
(((CoronaRona.)))
During the riots, the weasel, Fauci and that female doctor whats her name, were nowhere to
be seen, and now they have returned and the (((CoronaRona))) is being looped 24/7. My guess
is that all these (((medical experts))) will recommend another lock-down until the election.
IF Biden wins, which given the corruption out there, is highly likely whether we are in
lock-down or not, the (((CoronaRona))) will fade away into the night. IF Trump is somehow is
reelected, well the (((Antifa-BLM))) types will be having another meltdown that the
(((media))) will cover 24/7, and the (((CoronaRona))) will be back page news again.
I'm (((CoronaRona))) and I approve this message.
Che Guava
July 11, 2020 at 3:13 pm GMT
This reply is both to Kirt and Garry Heavin.
For Kirt, yes, I think I already had it too, seven or eight weeks from NYE last year to
mid-Feb. of this. As I have said several times, the area near my workplace was usually full
of Chinese tourists.
I had a cough, extreme lethargy on many days, a slight fever. Water frnm my nose, always
the case for me in winter, but no sneezing. I must raise the idea with my regular doc., since
I saw him at least three times over that time.
As for our author, Heavin's article, he is clearly offering better ideas for treatments
than big pharma, but who really needs treatment?
Those who have a persistent cold-like syndrome?
Anyome identified through the polymerase chain reaction tests, which prove nothing.
Just ignore it and it will go away seems by far the wisest course.
schrub
July 11, 2020 at 3:29 pm GMT
On an entirely different topic:
WARNING: FOR THOSE WHO USE NORD VPN for their VPN service
If you select NORDVPN's "CYBERSEC" option to "block ads and malicious websites" , you will
no longer be able to get on sites like unz.com
or many other right wing sites (like Mike Rivero's site: whatreallyhappened.com for instance).
NORDVPN's CYBERSEC will, however, allow you on all the left wing sites pushed by the ADL.
This means that NORDVPN'S CYBERSEC option is probably using the ADL's filtering criteria.
I questioned NORDVPN about this "selectivity" and never received a reply.
This also means that your NORDVPN software could well be spying on you and recording your
keystrokes if you try to access to certain unapproved sites EVEN IF if the CYBERSEC option
hasn't chosen.
NORDVPN is now, curiously enough, based in Panama, a country which the US government has
been shown in the past to have considerable influence over when the need arises. (Ask Manuel
Noriega for examples)
Spread the word.
It might be time choose a different VPN sofware if you are now using NORDVPN. Anybody have
any good suggestions?
Zarathustra
July 11, 2020 at 3:33 pm GMT
I believe!
Well?
CW2isComing
July 11, 2020 at 3:35 pm GMT
@Twodees Partain
@Emslander
Yes, why are you being cryptic here–on this site–where a free exchange of
information is desirable?
Herald
July 11, 2020 at 3:38 pm GMT
@Alfred
Cases now mean positive tests and of course, no really knows what that means, other than
that more useless tests have been carried out. As the graph clearly indicates these so called
"cases" have little to do with deaths. Nor do they have anything to do with
hospitalisations.
We are clearly in the midst of an almighty scam, which is much much bigger than simply
getting rid of Trump.
Emslander
July 11, 2020 at 3:41 pm GMT
@Twodees Partain
Extract of cranberries and D-Mannos. Together they are very good. I presume that they
can't cure serious problems, but they work pretty well.
I'm not a doctor and I don't even work on TV.
Alfred
July 11, 2020 at 3:50 pm GMT
@UncommonGround ut a thorough check.
A report in The Guardian also found that the key employees of Surgisphere included a
science fiction writer and an adult movie star.
The HCQ study mess: How 3 Indian researchers put reputation of Lancet, NEJM at stake
How 3 'smart' Indian names have ruined 200-year reputation of most respected medical
journals
https://www.youtube.com/embed/-6WnSiCPYyQ?feature=oembed
Zarathustra
July 11, 2020 at 3:55 pm GMT
But putting all attempted jokes aside and talking a little bit more seriously, CNN did
become certified criminal enterprise now.
Gary Heavin
July 11, 2020 at 3:56 pm GMT
To Bras my pro-life libertarian position does not become "meaningless" as if my prolife
and libertarianism negate each other as you suggest. It's quite simple. Libertarianism
demands we not harm other persons. An unborn baby is a person.
Thomas Milton
July 11, 2020 at 3:57 pm GMT
"What you need to know" .is that this crisis has been spun from whole cloth.
Montefrío
July 11, 2020 at 3:58 pm GMT
@gotmituns e before the year is out. My bucolic life has been given a shake and I'm
scrambling to best position our family (we live on the same property) financially and
economically when BNW arrives with a vengeance. I wish to leave my grandchildren (my son, a
water well driller, is prospering, happily, but still ) wholly owned property and the houses
thereon plus one. I believe the BNW will have a distinctly local air to it in rural or
semi-rural communities: little travel, local employment save for telecommuters, detachment
from social media, different educational strategies and opportunities, etc. If you share this
belief, get cracking and pretend that the reset has already arrived and act accordingly.
schrub
July 11, 2020 at 4:00 pm GMT
AS an answer to my own question about a new secure VPN service, I just came upon this.
Anybody have any experience with this outfit?
https://protonvpn.com/about
I now wouldn't trust any VPN whatsoever service that wasn't entirely "open source".
Protonvpn claims to be "open source". (On the other hand, NORDVPN isn't open source).
https://protonvpn.com/blog/open-source/
Definition of very important term "open source" for those are unfamiliar with it:https://opensource.org/osd
If a software isn't "open source" it could potentially be spying on you. Choosing a VPN
service using "open source" software should be the PRIMARY and most critical consideration
when choosing a VPN service.
Non "open source" VPN software is open to outside manipulation and possible government
infiltration.
Wally
July 11, 2020 at 4:02 pm GMT
@Gleimhart Mantooso
asked:
– The same thing that happened to the 'Israeli Geniuses' laughable, but "historic",
attempt to put a spacecraft on the moon.
Israel's Beresheet spacecraft crashes during historic moon landing attempt :
https://www.nbcnews.com/mach/science/how-watch-israel-s-beresheet-spacecraft-attempt-moon-landing-ncna993436
Alfred
July 11, 2020 at 4:04 pm GMT
@Emslander
It suits her personality as she is a quite orderly and methodical person. However, it
means that she is incapable of critical thinking. All doctors in Australia are invited to
free seminars and meals at expensive restaurants – paid for by pharmaceutical
companies.
Sadly, she did not listen to my opinion about vaccines for our two girls. In the State of
Victoria, they give a mandatory HPV vaccine. However, HPV is only a problem for those who are
promiscuous. Furthermore, this vaccine is essentially an unknown. It is highly-expensive at
some US$300 – paid for by the tax-payers. I suspect the vaccine altered the personality
of one of our daughters. It is uncanny.
Astuteobservor
II
July 11, 2020 at 4:05 pm GMT
It seems the only way to convince retards is to kill them or let them see dead bodies
everywhere.
It is like the old saying in IT.
Everything is working, wtf does the company need you for.
Everything is falling apart, wtf does the company need you for.
On covid.
Lockdowns and quarantine is working, wtf, covid is Nothing, flu is worst.
Death count is now twice the number of the worst flu year, the lockdowns and quarantine
are the causes, not covid.
Lincoln was right, just need to make sure the 80% retards gets fooled, the other 20%
doesn't matter as their voices would be drown out by the retards.
If this covid virus is as deadly as it needs to convince the retards, nukes would have
flown. I wonder how many retards understands why that is.
Zarathustra
July 11, 2020 at 4:13 pm GMT
@Gary Heavin
Slightly increase the daily intake of butter you moron, and you will not need to worry
anymore.
Montefrío
July 11, 2020 at 4:21 pm GMT
@macilrae
I neither wear a mask nor hunker down and I'm a "double-vulnerable" (nearly 74 and mildly
diabetic). A close lady friend is the village pharmacist and when on duty wears the mask
under mild duress; neither of us wears it when alone with each other. Unless you're in a
densely populated area, better to go out and get at least half an hour of sun daily, fortify
yourself and family, keep the faith and don't succumb to manufactured fear, sez I.
Sparkon
July 11, 2020 at 4:35 pm GMT
@macilrae ak links here in the USA, sad to say. During my most recent trip to the market,
I saw perhaps 7-10% of shoppers with their masks pulled down so it was covering the mouth,
but not the nose. For the most part, these non-complying shoppers were the fat, ugly,
slovenly, and stupid looking types one would try to avoid anyway, so the pulled-down mask is
a good signal to give these types a very wide berth.
Recall that the world's experience with COVID-19 amounts to just six or seven months.
Nobody knows what this virus may do in the future, but odds are it will mutate, like all
viruses.
Vandal
July 11, 2020 at 4:41 pm GMT
@chuckywiz
The regiment I've seen published is as follows
Hydroxychloroquine 200mg twice a day for 5 days
ZPAK 500mg once a day for 5 days
Zinc Sulfate 220mg daily
Pragma
July 11, 2020 at 4:47 pm GMT
Mr. Heaven:
I found your figures regarding the vaccine cost and quantity remarkable, to say the
least.
After some research, I could find no reference of a commitment by the UK government to
purchase 80 million doses at $600 each.
I did find, however, reference to the Oxford/AstraZeneca potential vaccine AZD1222 which
is estimated to cost around 2.5 euros or about $2.80 US. This appears to be the direction
that the EU is going, but it is unclear if the UK will be part of it.
Could you please forward a link or reference for the source of your figures?
Gary Heavin
July 11, 2020 at 5:16 pm GMT
@Pragma
https://www.dailymail.co.uk/news/article-8123691/With-estimated-477-injection-potentially-billions-coronavirus-jab.html
Thim
July 11, 2020 at 5:19 pm GMT
@macilrae
Your family will wear masks, because you are slaves. Absolutely no one claims wearing a
mask will prevent you from catching a flu or cold (Corona virus).
Bardon
Kaldian
July 11, 2020 at 5:20 pm GMT
So, it's all a giant conspiracy Interesting:
https://edition.cnn.com/2020/07/10/health/coronavirus-entire-body-effects-columbia/index.html
How coronavirus affects the entire body
TheTruthSeeker
July 11, 2020 at 5:30 pm GMT
Pavia, a cure that works, challenges media silence: "Plasma kills the virus"
"Plasma kills the coronavirus." The therapy developed by the Immuno-hematology Institute
of Saint Matthew in Pavia is encouraging. In this exclusive interview with The Daily Compass
given at the end of his experimentation, director Cesare Perotti reveals the positive
results: "The treatment works; at the moment no one has died; the USA has asked for the
protocols." But nobody is talking about it: "There are other interests opposing us, but we
will address these after the scientific publication." This is how the shared treatment works,
by "using" volunteers who have recovered to help heal those who are sick.
Reference and continuation:
https://newdailycompass.com/en/pavia-a-cure-that-works-challenges-media-silence-plasma-kills-the-virus
Rubicon
July 11, 2020 at 5:53 pm GMT
@Achilles Wannabe
What Achilles Wannabe writes is ABSOLUTELY CORRECT.
If I have to, the ONLY way to purchase HDC is via my Canadian brothers. Naturally, I would
need an American doctor's prescription, but push comes to shove, I absolutely refuse going to
ANY American "medical doctor" to treat me.
Hopefully, the Canadian prescription stores would be able to fill that prescription. If
not, oh well.
jean
105
There is a racial difference in that blacks and people of color are vitamin D deficient,
as are the elderly.
Vitamin D linked to low virus death rate, study finds
https://www.sciencedaily.com/releases/2020/05/200507131012.htm
dbk
107
For commenters who've remarked on the incidences of (a) obesity, (b) diabetes and (c) high
blood pressure - other cardiovascular ailments (not sure anyone referred to [c] but it's on
most lists), these are all ultimately rooted in poverty / stress.
For commenters who remarked on the "Southern" diet and McDonald's food, many urban
neighborhoods and poor rural counties are food deserts, period. The urban elite in the South
(Black and white alike) have diets that resemble those of residents of Manhattan.
For the commenter who remarked on the absence of a national health care program in the
U.S. - yes, this is a major contributing factor but it's further complicated by other
intersecting forms of injustice which contribute to the heightened risk for Blacks who
contract the virus.
The premise of the OP is correct in my view, and the post correctly concludes the Identity
Politics is being used (by both sides) to mask the real disease.
karlof1 , Jul 10 2020 18:34 utc |
108
I must applaud b for finally bringing in the Class War into his COVID-19 analysis. What
you are genetically isn't the main factor; rather, it's your socio-economic-- CLASS
--status that matters most regarding your potential exposure to the disease. Activists within
the Outlaw US Empire have pointed to that fact going back to March, and it's certainly a big
factor fueling the ongoing protests.
Australian Financial Review
Researchers at La Trobe University in Australia have developed an augmented reality (AR)
visualization of the effects of Covid-19 on the lungs, in an effort to aid diagnosis and
treatment. The researchers converted two-dimensional (2D) computed tomography (CT) scans of
Covid-damaged lungs into three-dimensional (3D) images. Microsoft's HoloLens 2 headset lets
researchers view those images, superimposed into the space in front of their eyes. Said La
Trobe's Henry Duh, "If you only see a 2D scan, without HoloLens, you need to do more mental
rotations and reconstructions in order to figure out what it looks like in the body." The
researchers hope to use machine learning to analyze original CT scans and identify areas of the
lungs damaged by the disease.
*May Require Paid Registration
LancetGate: "Scientific Corona Lies" & Big Pharma Corruption - Hydroxychloroquine
Versus Remdesivir by Tyler Durden Fri, 07/10/2020 - 19:05
Twitter Facebook Reddit Email
Print
Authored by Prof Michel Chossudovsky via GlobalResearch.ca,
Introduction
There is an ongoing battle to suppress Hydroxychloroquine (HCQ), a cheap and effective drug
for the treatment of Covid-19. The campaign against HCQ is carried out through slanderous
political statements, media smears, not to mention an authoritative peer reviewed "evaluation"
published on May 22nd by The Lancet, which was based on fake figures and test trials.
The study was allegedly based on data analysis of 96,032 patients hospitalized with COVID-19
between Dec 20, 2019, and April 14, 2020 from 671 hospitals Worldwide. The database had been
fabricated. The objective was to kill the Hydroxychloroquine ( HCQ) cure on behalf of Big
Pharma.
me title=
https://imasdk.googleapis.com/js/core/bridge3.393.1_en.html#goog_1935385610
https://imasdk.googleapis.com/js/core/bridge3.393.1_en.html#goog_1492485158
NOW PLAYING
Harvard And MIT Sue
Meatpacking Workers Are In Danger
Trump Not Happy With CDC School Guidelines
The Unreported Cases
The CDC Single Test
Censor In Chief? VP Pence To Control Coronavirus Info
The Yeezy Loan
Cruise Ships Might Be a Safer Way to Vacation During COVID-19, Health Expert Claims
While The Lancet article was retracted, the media casually blamed "a tiny US based company"
named Surgisphere whose employees included "a sci-fi writer and an adult content model" for
spreading "flawed data"
(Guardian) . This Chicago based outfit was accused of having misled both the WHO and
national governments, inciting them to ban HCQ. None of those trial tests actually took
place.
While the blame was placed on Surgisphere, the unspoken truth (which neither the scientific
community nor the media have acknowledged) is that the study was coordinated by Harvard professor
Mandeep Mehra under the auspices of Brigham and Women's Hospital (BWH) which is a partner
of the Harvard Medical School.
When the scam was revealed , Dr. Mandeep Mehra who holds the Harvey Distinguished Chair of
Medicine at Brigham and Women's Hospital apologized:
I have always performed my research in accordance with the highest ethical and
professional guidelines. However, we can never forget the responsibility we have as
researchers to scrupulously ensure that we rely on data sources that adhere to our high
standards.
It is now clear to me that in my hope to contribute this research during a time of great
need, I did not do enough to ensure that the data source was appropriate for this use. For
that, and for all the disruptions – both directly and indirectly – I am truly
sorry. (emphasis added)
Mandeep R. Mehra, MD, MSC ( official
statement on BWH website)
But that "truly sorry" note was just the tip of the iceberg. Why?
https://lockerdome.com/lad/13084989113709670?pubid=ld-dfp-ad-13084989113709670-0&pubo=https%3A%2F%2Fwww.zerohedge.com&rid=www.zerohedge.com&width=890
Studies on Gilead Science's Remdesivir and Hydroxychloroquine (HCQ) Were Conducted
Simultaneously by Brigham and Women's Hospital (BWH)
While The Lancet report (May 22, 2020) coordinated by Dr. Mandeep Mehra was intended "to
kill" the legitimacy of HCQ as a cure of Covid-19, another important (related) study was being
carried out (concurrently) at BWH pertaining to Remdesivir on behalf of Gilead Sciences Inc.
Dr. Francisco Marty, a specialist in Infectious Disease and Associate Professor at Harvard
Medical School was entrusted with coordination of
the clinical trial tests of the antiviral medication Remdesivir under Brigham's contract with
Gilead Sciences Inc :
Brigham and Women's Hospital began enrolling patients in two clinical trials for Gilead's
antiviral medication remdesivir. The Brigham is one of multiple clinical trial sites for a
Gilead-initiated study of the drug in 600 participants with moderate coronavirus disease
(COVID-19) and a Gilead-initiated study of 400 participants with severe COVID-19.
If the results are promising, this could lead to FDA approval, and if they aren't, it
gives us critical information in the fight against COVID-19 and allows us to move on to other
therapies."
While Dr. Mandeep Mehra was not directly involved in the Gilead Remdesevir BWH study under
the supervision of his colleague Dr. Francisco Marty, he nonetheless had contacts with Gilead
Sciences Inc: "He participated in a conference sponsored by Gilead in early April 2020 as part
of the Covid-19 debate" (France Soir, May 23, 2020)
What was the intent of his (failed) study? To undermine the legitimacy of
Hydroxychloroquine?
According to France Soir, in a report published after The Lancet Retraction:
The often evasive answers produced by Dr Mandeep R. Mehra , professor at Harvard Medical
School, did not produce confidence, fueling doubt instead about the integrity of this
retrospective study and its results . (France Soir, June 5, 2020)
Was Dr. Mandeep Mehra in conflict of interest? (That is a matter for BWH and the Harvard
Medical School to decide upon).
Who are the Main Actors?
Dr. Anthony Fauci, advisor to Donald Trump, portrayed as "America's top infectious disease
expert" has played a key role in smearing the HCQ cure which had been approved years earlier by
the CDC as well as providing legitimacy to Gilead's Remdesivir.
Dr. Fauci has been the head of the National Institute of Allergy and Infectious Diseases
(NIAID) since the Reagan administration. He is known to act as a mouthpiece for Big Pharma.
Dr. Fauci launched Remdesivir in late June (see details below). According to Fauci,
Remdesevir is the "corona wonder drug" developed by Gilead Science Inc. It's a $1.6 billion
dollar bonanza.
Gilead Sciences Inc: History
Gilead Sciences Inc is a
Multibillion dollar bio-pharmaceutical company which is now involved in developing and
marketing Remdesivir. Gilead has a long history. It has the backing of major investment
conglomerates including the Vanguard Group and Capital Research & Management Co, among
others. It has developed ties with the US Government.
In 1999 Gilead Sciences
Inc, developed Tamiflu (used as a treatment of seasonal influenza and bird flu). At the
time, Gilead Sciences Inc was headed by Donald Rumsfeld (1997-2001), who later joined the
George W. Bush administration as Secretary of Defense (2001-2006). Rumsfeld was responsible for
coordinating the illegal and criminal wars on Afghanistan (2001) and Iraq (2003).
Rumsfeld maintained his links to Gilead Sciences Inc throughout his tenure as Secretary of
Defense (2001-2006). According to CNN Money (2005) :
"The prospect of a bird flu outbreak was very good news for Defense Secretary Donald Rumsfeld
[who still owned Gilead stocks] and other politically connected investors in Gilead
Sciences".
Anthony Fauci has been in charge of the NIAID since 1984, using his position as "a go
between" the US government and Big Pharma. During Rumsfeld's tenure as Secretary of Defense,
the budget allocated to bio-terrorism increased substantially, involving contracts with Big
Pharma including Gilead Sciences Inc. Anthony Fauci considered that the money allocated to bio-terrorism in
early 2002 would:
"accelerate our understanding of the biology and pathogenesis of microbes that can be used
in attacks, and the biology of the microbes' hosts -- human beings and their immune systems.
One result should be more effective vaccines with less toxicity." (WPo report)
In 2008, Dr. Anthony Fauci was granted the Presidential Medal of Freedom by president George
W. Bush "for his determined and aggressive efforts to help others live longer and healthier
lives."
The 2020 Gilead Sciences Inc Remdesivir Project
We will be focussing on key documents (and events)
Chronology
February 21: Initial Release pertaining to NIH-NIAID Remdesivir placebo test trial
April 10 : The Gilead Sciences Inc study published in the NEJM on the "Compassionate
Use of Remdesivir"
April 29 : NIH Release: Study on Remdesivir (Report published on May 22 in NEJM)
May 22, The BWH-Harvard Study on Hydroxychloroquine coordinated by Dr. Mandeep Mehra
published in The Lancet
May 22 , Remdesivir
for the Treatment of Covid-19 -- Preliminary Report (NEJM)
June 5: The (fake) Lancet Report (May 22) on HCQ is Retracted.
June 29 , Fauci announcement. The $1.6 Billion Remdevisir HHS Agreement with Gilead
Sciences Inc
April 10: The Gilead Sciences Inc. study published in the NEJM on the "Compassionate Use
of Remdesivir"
A Gilead sponsored report was published in New England Journal of Medicine in an
article entitled "Compassionate Use of
Remdesivir for Patients with Severe Covid-19" . It was co-authored by an impressive list of
56 distinguished medical doctors and scientists, many of whom were recipients of consulting
fees from Gilead Sciences Inc.
Gilead Sciences Inc. funded the study which included several staff members as
co-authors.
The testing included a total of 61 patients [who] received at least one dose of remdesivir
on or before March 7, 2020; 8 of these patients were excluded because of missing postbaseline
information (7 patients) and an erroneous remdesivir start date (1 patient) Of the 53
remaining patients included in this analysis, 40 (75%) received the full 10-day course of
remdesivir, 10 (19%) received 5 to 9 days of treatment, and 3 (6%) fewer than 5 days of
treatment.
The NEJM article states that "Gilead Sciences Inc began accepting requests from clinicians
for compassionate use of remdesivir on January 25, 2020". From whom, From Where? According to
the WHO (January 30, 2020) there were 82 cases in 18 countries outside China of which 5 were in
the US, 5 in France and 3 in Canada.
Several prominent physicians and scientists
have cast doubt on the Compassionate Use of Remdesivir study conducted by Gilead, focussing
on the small size of the trial. Ironically, the number of patients in the test is less that the
number of co-authors: "53 patients" versus "56 co-authors"
Below we provide excerpts of scientific statements on the Gilead NEJM project (
Science Media Centre emphasis added) published immediately following the release of the
NEJM article:
" 'Compassionate use' is better described as using an unlicensed therapy to treat a
patient because there are no other treatments available . Research based on this kind of use
should be treated with extreme caution because there is no control group or randomisation,
which are some of the hallmarks of good practice in clinical trials. Prof Duncan Richard ,
Clinical Therapeutics, University of Oxford.
"It is critical not to over-interpret this study. Most importantly, it is impossible to
know the outcome for this relatively small group of patients had they not received
remdesivir. Dr Stephen Griffin , Associate Professor, School of Medicine, University of
Leeds.
"The research is interesting but doesn't prove anything at this point: the data are from a
small and uncontrolled study. Simon Maxwell, Professor of Clinical Pharmacology and
Prescribing, University of Edinburgh.
"The data from this paper are almost uninterpretable. It is very surprising, perhaps even
unethical, that the New England Journal of Medicine has published it. It would be more
appropriate to publish the data on the website of the pharmaceutical company that has
sponsored and written up the study. At least Gilead have been clear that this has not been
done in the way that a high quality scientific paper would be written. Prof Stephen Evans,
Professor of Pharmacoepidemiology, London School of Hygiene & Tropical Medicine.
"It's very hard to draw useful conclusions from uncontrolled studies like this
particularly with a new disease where we really don't know what to expect and with wide
variations in outcomes between places and over time. One really has to question the ethics of
failing to do randomisation – this study really represents more than anything else, a
missed opportunity." Prof Adam Finn, Professor of Paediatrics, University of Bristol.
To review
the complete document of Science Media Centre pertaining to expert assessments click
here
April 29: The National Institutes of Health (NIH) Study on Remdevisir.
On April 29th following the publication of the Gilead Sciences Inc Study in the NEJM on
April 10,
a press release of the National Institutes of Health (NIH) on Remdevisir was released. The
full document was published on May 22, by the NEJM under the title:
Remdesivir
for the Treatment of Covid-19 -- Preliminary Report (NEJM)
The study had been initiated on February 21, 2020. The title of the April 29 Press Release
was:
"Peer-reviewed data shows remdesivir for COVID-19 improves time to recovery"
It's a government sponsored report which includes preliminary data from a randomized trial
involving 1063 hospitalized patients. The results of the trial labelled
Adaptive COVID-19 Treatment Trial (ACTT) are preliminary, conducted under the helm of Dr.
Fauci's National Institute of Allergy and
Infectious Diseases (NIAID) :
An independent data and safety monitoring board (DSMB) overseeing the trial met on April
27 to review data and shared their interim analysis with the study team. Based upon their
review of the data, they noted that remdesivir was better than placebo from the perspective
of the primary endpoint, time to recovery, a metric often used in influenza trials. Recovery
in this study was defined as being well enough for hospital discharge or returning to normal
activity level.
Preliminary results indicate that patients who received remdesivir had a 31% faster time
to recovery than those who received placebo (p<0.001). Specifically, the median time to
recovery was 11 days for patients treated with remdesivir compared with 15 days for those who
received placebo. Results also suggested a survival benefit, with a mortality rate of 8.0%
for the group receiving remdesivir versus 11.6% for the placebo group (p=0.059). (emphasis
added)
In the NIH's earlier February 21, 2020 report (released at the outset of the study), the
methodology was described as follows:
A randomized, controlled clinical trial to evaluate the safety and efficacy of the
investigational antiviral remdesivir in hospitalized adults diagnosed with coronavirus
disease 2019 (COVID-19)
Numbers. Where? When?
The February 21 repor t confirmed that the first trial participant was "an American who was
repatriated after being quarantined on the Diamond Princess cruise ship" that docked in
Yokohama (Japanese Territorial Waters). "Thirteen people repatriated by the U.S. State
Department from the Diamond Princess cruise ship" were selected as patients for the placebo
trial test. Ironically, at the outset of the study, 58.7% of the "confirmed cases" Worldwide
(542 cases out of 924) (outside China), were on the Diamond Cruise Princess from which the
initial trial placebo patients were selected.
Where and When: The trial test in the 68 selected sites? That came at a later date because
on February 19th (WHO data), the US had recorded only 15 positive cases (see Table Below).
"A total of 68 sites ultimately joined the study -- 47 in the United States and 21 in
countries in Europe and Asia." (emphasis added)
In the final May 22 NEJM report entitled Remdesivir
for the Treatment of Covid-19 -- Preliminary Report :
There were 60 trial sites and 13 subsites in the United States (45 sites), Denmark (8),
the United Kingdom (5), Greece (4), Germany (3), Korea (2), Mexico (2), Spain (2), Japan (1),
and Singapore (1). Eligible patients were randomly assigned in a 1:1 ratio to receive either
remdesivir or placebo. Randomization was stratified by study site and disease severity at
enrollment
The Washington Post applauded Anthony Fauci's announcement (April 29):
"The preliminary results, disclosed at the White House by Anthony S. Fauci, fall short of
the magic bullet or cure But with no approved treatments for Covid-19, [Lie] Fauci said, it
will become the standard of care for hospitalized patients The data shows that remdisivir has
a clear-cut, significant, positive effect in diminishing the time to recovery," Fauci
said.
The government's first rigorous clinical trial of the experimental drug remdesivir as a
coronavirus treatment delivered mixed results to the medical community Wednesday -- but
rallied stock markets and raised hopes that an early weapon to help some patients was at
hand.
The preliminary results, disclosed at the White House by Anthony Fauci, chief of the
National Institute of Allergy and Infectious Diseases, which led the placebo-controlled trial
found that the drug accelerated the recovery of hospitalized patients but had only a marginal
benefit in the rate of death.
Fauci's remarks boosted speculation that the Food and Drug Administration would seek
emergency use authorization that would permit doctors to prescribe the drug.
In addition to clinical trials, remdesivir has been given to more than 1,000 patients
under compassionate use. [also refers to the Gilead study published on April 10 in the
NEJM]
The study, involving [more than] 1,000 patients at 68 sites in the United States and
around the world (??) , offers the first evidence (??) from a large (??), randomized (??)
clinical study of remdesivir's effectiveness against COVID-19.
The NIH placebo test study provided "preliminary results". While the placebo trial test was
"randomized", the overall selection of patients at the 68 sites was not fully randomized. See
the full report.
May 22: The Fake Lancet Report on Hydroxychloroquine (HCQ)
It is worth noting that the
full report of the NIH-NIAID) entitled Remdesivir
for the Treatment of Covid-19 -- Preliminary Report was released on May 22, 2020 in the
NEJM, on the same day as the controversial Lancet report on Hydroxychloroquine.
Immediately folllowing its publication, the media went into high gear, smearing the HCQ
cure, while applauding the NIH-NIASD report released on the same day.
Remdesivir, the only drug cleared to treat Covid-19, sped the recovery time of patients
with the disease, "It's a very safe and effective drug," said Eric Topol, founder and
director of the Scripps Research Translational Institute. "We now have a definite first
efficacious drug for Covid-19, which is a major step forward and will be built upon with
other drugs, [and drug] combinations."
When the Lancet HCQ article by Bingham-Harvard was retracted on June 5, it was too late, it
received minimal media coverage. Despite the Retraction, the HCQ cure "had been killed".
June 29: Fauci Greenlight. The $1.6 Billion Remdesivir Contract with Gilead Sciences Inc
Dr. Anthony Fauci granted the "Greenlight" to Gilead Sciences Inc. on June 29, 2020.
The semi-official US government NIH-NIAID sponsored report (May 22) entitled Remdesivir
for the Treatment of Covid-19 -- Preliminary Report (NEJM) was used to justify a major
agreement with Gilead Sciences Inc.
The Report was largely funded by the National Institute of Allergy and Infectious Diseases
(NIAID) headed by Dr. Anthony Fauci and the National Institutes of Health (NIH).
On June 29, based on the findings of the NIH-NIAID Report published in the NEJM, the
Department of Health and Human Services (HHS) announced on behalf of the Trump Adminstration
an agreement to secure large supplies of the remdesivir drug from Gilead Sciences Inc. for
the treatment of Covid-19 in America's private hospitals and clinics.
The earlier Gilead study based on scanty test results published in the NEJM (April 10), of
53 cases (and 56 co-authors) was not highlighted. The results of this study had been questioned
by several prominent physicians and scientists.
Who will be able to afford Remdisivir? 500,000 doses of Remdesivir are envisaged at $3,200
per patient, namely
$1.6 billion (see the s
tudy by Elizabeth Woodworth )
The Drug was also approved for
marketing in the European Union. under the brandname Veklury.
If this contract is implemented as planned, it represents for Gilead Science Inc. and the
recipient US private hospitals and clinics a colossal amount of money.
[error in above title according to HHS: $3200]
According to The Trump Administration's HHS Secretary Alex Azar (June 29, 2020):
NEVER
MISS THE NEWS THAT MATTERS MOST
ZEROHEDGE DIRECTLY TO YOUR INBOX
Receive a daily recap featuring a curated list of must-read stories.
"To the extent possible, we want to ensure that a ny American patient who needs remdesivir
can get it . [at $3200] The Trump Administration is doing everything in our power to learn
more about life-saving therapeutics for COVID-19 and secure access to these options for the
American people."
Remdesivir for Covid-19: $1.6 Billion for a "Modestly Beneficial" Drug?
Remdesivir
versus Hydroxychloroquine (HCQ)
Careful timing:
The Lancet study (published on May 22) was intended to undermine the legitimacy of
Hydroxychloroquine as an effective cure to Covid-19, with a view to sustaining the $1.6 billion
agreement between the HHS and Gilead Sciences Inc. on June 29th. The legitmacy of this
agreement rested on the May 22 NIH-NIAID study in the NEJM which was considered
"preliminary".
What Dr. Fauci failed to acknowledge is that Chloroquine had been "studied" and tested
fifteen years ago by the CDC as a drug to be used against coronavirus infections. And that
Hydroxychloroquine has been used recently in the treatment of Covid-19 in several
countries.
According to the Virology Journal (2005) " Chloroquine is a potent inhibitor of SARS
coronavirus infection and spread". It was used in the SARS-1 outbreak in 2002. It had the
endorsement of the CDC.
HCQ is not only effective, it is "inexpensive" when compared to Remdesivir, at an estimated
"$3120 for a US Patient with private insurance".
Below are excerpts of an interview of Harvard's Professor Mehra (who undertook the May 22
Lancet study) with France Soir published immediately following the publication of the Lancet
report (prior to its Retraction).
Dr. Mandeep Mehra: In our study, it is fairly obvious that the lack of benefit and the
risk of toxicity observed for hydroxychloroquine are fairly reliable. [referring to the May
22 Lancet study]
France Soir: Do you have the data for Remdesivir?
MM: Yes, we have the data, but the number of patients is too small for us to be able to
conclude in one way or another.
FS: As you know, in France, there is a pros and cons battle over hydroxychloroquine which
has turned into a public health issue even involving the financial lobbying of pharmaceutical
companies. Why not measure the effect of one against the other to put an end to all
speculation?
MM: In fact, there is no rational basis for testing Remdesivir versus hydroxychloroquine.
On the one hand, Remdesivir has shown that there is no risk of mortality and that there is a
reduction in recovery time. On the other hand, for hydroxychloroquine it is the opposite: it
has never been shown any advantage and most studies are small or inconclusive In addition,
our study shows that there are harmful effects.
It would therefore be difficult and probably unethical to compare a drug with demonstrated
harmfulness to a drug with at least a glimmer of hope.
FS: You said that there is no basis for testing or comparing Remdesivir with
hydroxychloroquine, do you think you have done everything to conclude that hydroxychloroquine
is dangerous?
MM: Exactly.
All we are saying is that once you have been infected (5 to 7 days after) to the point of
having to be hospitalized with a severe viral load, the use of hydroxychloroquine and its
derivative is not effective.
The damage from the virus is already there and the situation is beyond repair. With this
treatment [HCQ] it can generate more complications
FS Mandeep Mehra declared that he had no conflict of interest with the laboratories and
that this study was financed from the endowment funds of the professor's chair.
He participated in a conference sponsored by Gilead in early April 2020 as part of the
Covid-19 debate.
- France Soir, translated by the author, emphasis added, May 23, 2020)
In Annex, see the followup article by France Soir published after the scam surrounding the
data base of Dr. Mehra's Lancet report was revealed.
Concluding Remarks
Lies and Corruption to the nth Degree involving Dr. Anthony Fauci, "The Boston Connection"
and Gilead Sciences Inc.
The Gilead Sciences Inc. Remdesivir study (50+ authors) was published in the New England
Journal of Medicine (April 10, 2020).
It was followed by the NIH-NIAID Remdesivir
for the Treatment of Covid-19 -- Preliminary Report on May 22, 2020 in the NEJM. And on
that same day, May 22, the "fake report" on Hydroxychloroquine by BWH-Harvard Dr. Mehra was
published by The Lancet.
Harvard Medical School and the BWH bear responsibility for having hosted and financed the
fake Lancet report on HCQ coordinated by Dr. Mandeep Mehra.
Is there conflict of interest? BWH was simultaneously involved in a study on Remdesivir in
contract with Gilead Sciences, Inc.
While the Lancet report coordinated by Harvard's Dr. Mehra was retracted, it nonetheless
served the interests of Gilead Sciences Inc.
It is important that an independent scientific and medical assessment be undertaken,
respectively of the Gilead Sciences Inc New England Journal of Medicine (NEMJ) peer reviewed
study (April 10, 2020) as well as the NIH-NIAID study also published in the NEJM (May 22,
2020).
* * *
ANNEX
Retraction by France Soir
The fraud concerning the Lancet Report was revealed in early June.
France Soir in a subsequent article (June 5, 2020) points to the Boston Connection: La
connexion de Boston , namely the insiduous relationship between Gilead Sciences Inc and
Professor Mehra, Harvard Medical School as well as the two related Boston based hospitals
involved.
(excerpts here,
to access the complete text click here translation from French by France Soir, emphasis in
the original article)
The often evasive answers produced by Dr Mandeep R. Mehra, a physician specializing in
cardiovascular surgery and professor at Harvard Medical School, did not produce confidence,
fueling doubt instead about the integrity of this retrospective study and its results.
However, the reported information that Dr. Mehra had attended a conference sponsored by
Gilead – producer of remdesivir, a drug in direct competition with hydroxychloroquine
(HCQ) – early in April called for further investigation
It is important to keep in mind that Dr. Mandeep Mehra has a practice at the Brigham and
Women's Hospital (BWH) in Boston.
That study relied on the shared medical records of 8,910 patients in 169 hospitals around
the world, also by Surgisphere.
Funding for the study was "Supported by the William Harvey Chair in Cardiovascular
Medicine at Brigham and Women's Hospital. The development and maintenance of the
collaborative surgical outcomes database was funded by Surgisphere."
The study published on May 22 sought to evaluate the efficacy or otherwise of chloroquine
and hydroxychloroquine, alone or in combination with a macrolide antibiotic.
It is therefore noteworthy that within 3 weeks, 2 large observational retrospective
studies on large populations – 96,032 and 8,910 patients – spread around the
world were published in two different journals by Dr. Mehra, Dr. Desai and other co-authors
using the database of Surgisphere, Dr. Desai's company.
These two practising physicians and surgeons seem to have an exceptional working capacity
associated with the gift of ubiquity.
The date of May 22 is also noteworthy because on the very same day, the date of the
publication in The Lancet of the highly accusatory study against HCQ, another study was
published in the New England Journal of Medicine concerning the results of a clinical trial
of remdesivir.
In the conclusion of this randomized, double-blind, placebo-controlled trial, "remdesivir
was superior to placebo in shortening the time to recovery in adults hospitalized with
Covid-19 and evidence of lower respiratory tract infection."
Concretely: on the same day, May 22nd, one study demeaned HCQ in one journal while another
claimed evidence of attenuation on some patients through remdesivir in another journal.
It should be noted that one of the main co-authors, Elizabeth "Libby"* Hohmann, represents
one of the participating hospitals, the Massachusetts General Hospital in Boston, also
affiliated with Harvard Medical School, as is the Brigham and Women's Hospital in Boston,
where Dr. Mandeep Mehra practices.
Coincidence, probably.
Upon further investigation, we discovered that the first 3 major clinical trials on
Gilead's remdesivir were conducted by these two hospitals:
"While COVID-19 continues to circle the globe with scientists following on its trail,
Massachusetts General Hospital (MGH) and Brigham and Women's Hospital (BWH) are leading the
search for effective treatment.
"Both hospitals are conducting clinical trials of remdesivir."
MGH has joined what the National Institute of Health (NIH) describe as the
first clinical trial in the United States of an experimental treatment for COVID-19,
sponsored by the National Institute of Allergy and Infectious Diseases, part of NIH . MGH is
currently the only hospital in New England to participate in this trial, according to a list
of sites shared by the hospital.
" It's a gigantic undertaking, with patients registered in some 50 sites across the
country, getting better .
"The NIH trial, which can be adapted to evaluate other treatments, aims to determine
whether the drug relieves the respiratory problems and other symptoms of COVID-19, helping
patients leave hospital earlier.**
As a reminder, the NIAID/NIH is led by Antony Fauci, a staunch opponent of HCQ.
Coincidence, probably.
" At the Brigham, two additional trials initiated by Gilead , the drug developer, will
determine whether it alleviates symptoms in patients with moderate to severe illness over
five- and ten-days courses. These trials will also be randomized, but not placebo controlled,
and will include 1,000 patients at sites worldwide. Those patients, noted Francisco Marty,
MD, Brigham physician and study co-investigator, will likely be recruited at an unsettlingly
rapid clip."
As a result, the first major clinical trials on remdesivir launched on March 20, whose
results are highly important for Gilead, are being led by the MGH and BWH in Boston,
precisely where Dr. Mehra, the main author of the May 22nd HCQ trial, is practising.
Small world! Coincidence, again, probably.
Dr. Marty at BWH expected to have results two months later. Indeed, in recent days,
several US media outlets have reported Gilead's announcements of positive results from the
remdesivir clinical trials in Boston.:
"Encouraging results from a new study published Wednesday on remdesivir for the treatment
of patients with COVID-19.**
Brigham and Dr. Francisco Marty worked on this study, and he says the results show that
there is no major difference between treating a patient with a five-day versus a 10-day
regimen.
"Gilead Announces Results of Phase 3 Remdesivir Trial in Patients with Moderate
COVID-19
– One study shows that the 5-day treatment of remdesivir resulted in significantly
greater clinical improvement compared to treatment with the standard of care alone
– The data come on top of the body of evidence from previous studies demonstrating
the benefits of remdesivir in hospitalized patients with IDVOC-19
"We now have three randomized controlled trials demonstrating that remdesivir improved
clinical outcomes by several different measures," Gilead plans to submit the complete data
for publication in a peer-reviewed journal in the coming weeks .
These results announced by Gilead a few days after the May 22 publication of the study in
the Lancet demolishing HCQ, a study whose main author is Dr. Mehra, are probably again a
coincidence.
So many coincidences adds up to coincidences? Really ?
Three UK organizations have released new reports advising people to get enough vitamin D,
either through sunlight or supplements, as a precaution against the novel coronavirus.
Several previous studies have linked vitamin D deficiency to higher risk of severe
coronavirus infection.
However, there's not yet sufficient evidence to fully understand if the nutrient plays a
causal role in preventing the disease, although it has been shown to support a healthy immune
system.
Visit Insider's
homepage for more stories .
While there's still no evidence that vitamin D can cure or prevent the coronavirus, three
major health organizations in the UK are advising people to ensure they get enough vitamin D,
from the sun or supplements, to be on the safe side.
me marginwidth=
The Scientific Advisory Commission on
Nutrition , the National Institute for Health and
Care Excellence , and the Royal
Society all published reports last month detailing what we know (and don't) about the
coronavirus and vitamin D, concluding that we need more research to fully understand the
connection.
In the meantime, however, these organizations advise a stronger emphasis on meeting the
current recommended vitamin D intake, not only as a precaution against coronavirus, but for
general health too.
Vitamin D is important for health, and might even stave off some
illnesses
Vitamin D is an essential nutrient for health, including the immune system.
Normally, humans can produce vitamin D naturally through direct exposure to sunlight -- we
also get vitamin D in certain foods, like eggs, fatty fish, and beef liver. In total, the UK
recommends people get 10 micrograms of vitamin D per day; the US recommendation is slightly
higher, 15 micrograms for most people, and 20 micrograms for those over 70.
Spending too much time indoors, whether in the colder winter months or in quarantine, can
potentially put you at risk of a vitamin D deficiency. Not enough of the nutrient is directly
linked to muscle, tooth, and bone health issues, according to the recent Royal Society
report.
That could be a problem when it comes to illness -- there's some evidence that a lack of
vitamin D is linked to infections, particularly in the respiratory tract, according to the
Scientific
Advisory Commission on Nutrition report.
But there's no evidence showing a direct
cause link between vitamin D and better coronavirus outcomes
However, while COVID-19 (the disease caused by the novel coronavirus) does attack the
respiratory system, there's no evidence vitamin D can cure or prevent the illness.
Several previous
studies have made a link between coronavirus outcomes and vitamin D deficiency -- however,
that research has included other variables that could explain the number and severity of
COVID-19 cases, and the research is far from showing a causal link.
But at least one
study has also shown no apparent link between vitamin D and coronavirus outcomes, leading s
ome researchers to remain skeptical about the possible connection .
Previous
research has cautioned consumers about exaggerated claims about vitamin D and the
coronavirus, particularly with regard to supplements or extremely high doses through an IV: too
much vitamin D can can cause a toxic buildup of calcium and lead to kidney issues,
according to the Mayo Clinic .
As such, there's still much more research to be done on the implications of vitamin D for
different coronavirus outcomes.
Charles Bangham, professor of immunology at Imperial College London and co-author of the
Royal Society paper, told the Financial Times that
Vitamin D deficiency could in part explain why people with darker skin tones have been
hardest-hit by the coronavirus. Black and brown people have more melanin that blocks UV rays
from the sun, so naturally-producing the nutrient from sunlight takes longer for people with
darker skin.
... ... ...
Read more:
Huge
doses of vitamin D will not cure or protect you from the coronavirus, a new report
says
Copper will not protect you from the coronavirus, despite its germ-killing properties, a
microbiologist says
Race
is not the reason Black Americans have a higher risk of dying from the coronavirus. It's
racism.
Read the original article on Insider
Copper metal has antimicrobial properties and can kill germs through direct contact.
The metal has been used to coat high-touch surfaces like door handles, surfaces in hospitals, and even personal items such as
masks.
However, copper isn't a cure-all, and it takes time and direct contact to destroy contaminants, so it might not always be the
best solution for preventing viral infection, according to research.
Visit Insider's homepage for more stories
.
me title=
As the US begins to tentatively return to business, despite the novel coronavirus still lurking among the population, any
potential protection has become a hot commodity.
Copper metal,
used
in products
such as door handles and key rings, is being touted as one such solution, advertised as killing the virus on
contact.
But before you click "buy" on those Instagram ads for copper patches billed as "natural hygienic germ stoppers," it's important
to distinguish between what copper is and isn't capable of doing against the virus.
It may help against germs in some instances, but it's not a panacea for prevention, since the coronavirus can still live on
copper surfaces for hours. And it's certainly no substitute for other precautions, according to Dr. Miryam Wahrman, biology
professor at William Paterson University and author of "
The
Hand Book: Surviving in a Germ-Filled World
."
me title=
"From what we're dealing with now, I don't think there's a lot of evidence to support the usefulness of copper in terms of
reducing infections," Wahrman told Insider.
"Germ-killing" ads include everything from copper discs and stickers to cell phone cases, bracelets and socks
There is a huge variety of copper products sold as "prevention tools," but they fall into four general categories.
There are wearables, such as face masks, but also tee-shirts laced with copper, and jewelry, which vendors claim "self-sanitize"
if they come into contact with contagious particles.
Then there are "sanitizers," which are bars or discs made of or coated in copper. These are designed to be rubbed on your hands
or other objects in order to sanitize them.
me title=
Touch-tools, the third category, can vary widely, but picture something that looks like bottle opener or key. You might use these
to open doors, push buttons, or even tap on touchscreens instead of directly interesting with those potentially germy surfaces.
Finally, there are copper-coated versions of everyday items you touch frequently, such as cellphone cases and door handles. The
advantage of these over their ordinary counterparts is that germs (including coronavirus) can't survive as long on copper as on
surfaces like plastic and other types of metal.
Copper can kill bacteria, but it's less effective against viruses
It's true that
research
has shown copper has antimicrobial properties
-- it can kill germs on contact in several ways, including by damaging the cell
membranes, but is most effective against bacteria, Wahrman explained.
"Copper is good as an antimicrobial against certain types of bacteria but when it comes to viruses, that's a whole different
ballgame because viruses are not living cells," she said.
me title=
An April 2020 study in the
New
England Journal of Medicine
found copper is inhospitable for the novel coronavirus as well, as the virus has a much shorter
lifespan on copper than on other surfaces such cloth, plastic, or even other metals.
That's important for environments where a lot of potential viral and bacterial particles are present, such as hospitals. A
2016
study
found that using copper components in hospitals could help prevent patients from contracting other infections while
hospitalized. According to the study, copper surfaces reduced the infection rate of patients by 58% (from 8.1% to 3.4%), and
reduced the viral load on surfaces by 83%.
However, the study found the coronavirus can still survive as long as
4
hours on copper, and it could take as long as 45 minutes for copper to reduce even a substantial amount of the virus on a surface
.
The soap, not the metal on the sink, is what really helps prevent viral contamination.
Maryna
Andriichenko/Getty Images
Most copper products do nothing more than lull you into a false sense of security, experts say
Touch-tools, which you can use to open doors, push buttons or otherwise interact with high-touch surfaces, might help by creating
a barrier between contagions and your hand, but only if you keep the tool clean, too. If you're not careful to do that, this
protective touch tool could simply be lulling you into feeling you're protected, when you're not.
me title=
"The positive thing is, you're touching fewer surfaces," Wahrman said. "But then you're going to come into contact with the part
that's been touching surfaces when you put it back in your purse or your pocket. It's going to give you a false sense of
confidence and won't occur to you that you've actually transferred germs to yourself and your home."
As an antimicrobial surface, copper could potentially still slow the spread of infection. But experts say it's highly unlikely
that, even in that unlikely scenario, it wouldn't instantly kill coronavirus germs.
"The suggestion that you can rub these items on your hands and that's going to keep you healthy, that's not scientifically
supported, especially for viruses," Wahrman said.
And face masks containing copper might be even less helpful, since in order for it to be effective, the copper needs to come into
direct contact with the virus. Copper-infused cloth would only work if the virus penetrates the fabric, defeating the purpose of
the mask in the first place.
me title=
"The face mask is a great barrier. They have a tight fiber so that they do block a lot of the viral particles and blocking them
is key," Wahrman said. "If the viral passes through the mask, it's not going to interact with the metal anyway, so it's not going
to make a difference."
For that direct contact to occur, items would need to be fully coated in copper across the entire surface. Even then, however,
the virus wouldn't be eliminated instantly. There's an additional complication, too, with cleaning copper-coated objects, since
typical
cleaning products could interfere with the chemical properties of the metal that make it effective against viruses in the first
place, according to research.
Copper might help on surfaces over time, but it can't prevent droplets direct from another person
None of these uses of copper address the most common form of contagious for the novel coronavirus, which is airborne infectious
directly from person to person.
"The big problem with the coronavirus is that it travels in droplets from one person to another who inhales it and that's how
most of the infections are happening. So there's no real way to get copper involved," Wahrman said.
me title=
So, while copper could have some promising applications, particularly in high-risk settings such as hospitals, it's not a
cure-all for the average person, and it can't replace traditional disinfectants, hand sanitizer, or good old fashioned soap and
water, according to Wahrman.
"The original advice that's tried and true is wash your hands with soap and water or use alcohol based hand sanitizer, and you've
really reduced the risk and reduced the germ load," she said.
Wearing a mask, washing your hands frequently, and maintaining social distancing are still your best bet against slowing the
spread of the virus, per the
CDC's
advice
.
somebody , Jul 6 2020 20:48 utc |
118
Posted by: Tuyzentfloot | Jul 5 2020 20:23 utc | 41
More math .
Perhaps the scariest numbers in microbiology relate to pathogenic microorganisms.
Worldwide, 16 million people die from infectious disease every year, and many of these
deaths are preventable. Approximately one in every 12 individuals, or 500 million people
worldwide, is living with chronic viral hepatitis, and the estimated number of new
chlamydial infections per year is approximately 50 million, more than the population of
South Korea. The bacterium Clostridium botulinum produces a toxin so potent that 3 grams
would be enough to kill the population of the United Kingdom and 400 grams would kill
everyone on the planet.
In total, there are ∼1,400 known species of human pathogens (including viruses,
bacteria, fungi, protozoa and helminths), and although this may seem like a large number,
human pathogens account for much less than 1% of the total number of microbial species on
the planet. On this point, ignoring questions about what actually constitutes a species,
estimates for the total number of microbial species vary wildly, from as low as 120,000 to
tens of millions and higher. Part of the reason for this large range is that we have only
sequenced 1 × 10−22% of the total DNA on Earth (although the Earth Microbiome
Project should improve this dramatically to 1 × 10−20% in the next 3 years).
This means that the fraction of microbial diversity that we have sampled to date is
effectively zero, a nice abstract entity to end on.
Have you ever wondered how Sarv-Cov-2 made it to discovery? Or how humans have managed to
survive up to now?
Tuyzentfloot , Jul 5 2020 20:23 utc |
41
Airborne ballpark math: we breathe about 500 l/h when sitting down and up to 10 times that
when exercising. When someone is ill and pushing 500 l/h of breath into a room with a
halftime of say 4 hours then after about that time this person maintains roughly 2 cubic
meters of breath in that room. For a room of 100 cubic meter that would be 2% of the air. So
during a workday you'd be breathing the breath of that other person at a dilution of the
order of 1%. Air conditioning recycles the air (maybe not completely I don't know the ratio)
so it is not ventilation where the air is replaced. Maybe airco can pick off a large part of
the particles. But that is the idea, assuming various losses and a large room you would still
breathing someone elses breath diluted by a factor thousand.So meat processing: cold air and to save energy ventilation is not good. Air is recycled a
lot. People doing physical labour a whole day, not sitting. Sounds tricky independently of
the hygiene question of dealing with industrially forcegrown animals
tucenz , Jul 5 2020 20:29 utc |
42
Tuyzentfloot | Jul 5 2020 20:23 utc | 40
You may need to put some gallons, pounds and feet in that post for the benefit
"exceptional" nation readers.
john
cronk says: July 2,
2020 at 5:18 pm GMT 500 Words
There is no exit strategy for this haphazard insanity. Once this over-reaction to a fairly
innocuous infectious agent was accepted as being necessary, there's no way to ever declare
reversion to normalcy.
In my opinion, rather than endlessly focussing on this not particularly interesting virus,
coming up with creative signboards and banners restricting movement, wrecking people's
livelihoods and painting crosses on the pavement where one must stand, we should have been onto
a more obvious problem by now. What if this HAD been a deadly pathogen? Why aren't we prepared
to quickly open special quarantine/treatment centers, disconnected from regular hospitals? And
what are we going to do about it?
This little rehearsal showed how unprepared we are should a real existential threat
arise.
[Hide MORE]There's little reason for insulin-sensitive people – with healthy immune status and
without metabolic disease – to stay home, wear a mask or 'social distance' themselves.
Since they won't be getting seriously ill, their staying home wouldn't help 'flatten the curve'
of sick people overburdening the healthcare system (as usual, to the expense of all of us). On
the contrary, active healthy people can contribute something to the economy.
The main benefit of herd immunity is that it will allow the country to function again. And
that would be good for everyone, healthy and sickly alike. The metabolically/immunologically
compromised will be vulnerable to catching the corona virus from anyone who's contracted it and
is temporarily contagious, no matter whether the carrier's general health is good or poor. And
that's the same fix that people with poor immune function are in, always and everywhere. The
answer for protecting these most vulnerable people from COVID – which is only one of the
many dangers to their health that they face – can be one of two things; the best one
being that they start eating right. And/or, we can build as much equipment and medical
facilities, where they're most needed, as they may require. Either of these solutions is much
more viable, less disruptive and less expensive than what we're doing now. And with either
solution, healthier people would no longer be punished for possessing normal human
vitality.
While governments, health agencies and scientists take steps to upgrade the availability of
care facilities, equipment and treatments, individuals should follow this
Part B (those most at risk for COVID complications- individuals with high BMI or chronic
health issues, or taking prescription medications, etc.)
AaronInMVD Website July 2, 2020 at 6:16 pm
GMT
@john
cronk with this knowledge is talk about it. Lots of talk, little action. The only active
pieces on the board are hopping around and trying to do a cultural revolution and proceeding
with an absolute poverty of energy.
This might be the most sedentary collapse ever. The world is taking a hard turn towards a
prolonged dark age and for the lack of reaction it seems people are just going with the flow.
Welcome to the future. A little bit of 1984, a heavy dose of Idiocracy, and a whole bunch of
pudgy kids trying to live out their Harry Potter headcanon.
Nevermind all the attention given to "Black Lives" while Black voices (Lest we forget the
'Shaun King is transracial' scandal of not long ago) are shut out of the conversation
Nonsense reigns!
Notable quotes:
"... The study analyzed 2,541 patients hospitalized among the system's six hospitals between March 10 and May 2 and found 13% of those treated with hydroxychloroquine died while 26% of those who did not receive the drug died. ..."
"... Among all patients in the study, there was an overall in-hospital mortality rate of 18%, and many who died had underlying conditions that put them at greater risk, according to Henry Ford Health System. Globally, the mortality rate for hospitalized patients is between 10% and 30%, and it's 58% among those in the intensive care unit or on a ventilator." Detroit News ..."
"... A long "take down" of Fauci: https://www.unz.com/audio/kbarrett_ken-mccarthy-tony-fauci-is-corrupt-to-the-core/ ..."
"... This is not Fauci's first rodeo. He's been pumping hysteria for 36 years. He always gets it wrong. He was wrong about swine flu. He was wrong about bird flu. He was wrong about Zika. He was wrong about Ebola. He wildly exaggerated AIDS. And he always is wrong in the favor of pharmaceutical companies. And he's always wrong in favor of 'we've got to develop a vaccine now. We have to throw out all the rules. ..."
"... Observational studies are never the equivalent of double-blind randomized studies; but there can still provide important and fare more readily obtained early information about these connections and conditions. ..."
"... This stuff is hard. There are lots of variations in patient populations and treatment protocols. We have to consider doses, concomitant meds (such as azithromycin), patient status at time of treatment, age, and, comorbidities. ..."
"... the recently halted NIH trial was randomized, double-blinded; this was in a hospital setting. The prophylactic trial reported at the beginning of June in NEJM (author Boulware) was also randomized, double-blinded; this was in a prophylactic setting. ..."
"A Henry Ford Health System study shows the controversial anti-malaria drug
hydroxychloroquine helps lower the death rate of COVID-19 patients, the Detroit-based health
system said Thursday.
Officials with the Michigan health system said the study found the drug "significantly"
decreased the death rate of patients involved in the analysis.
The study analyzed 2,541 patients hospitalized among the system's six hospitals between
March 10 and May 2 and found 13% of those treated with hydroxychloroquine died while 26% of
those who did not receive the drug died.
Among all patients in the study, there was an overall in-hospital mortality rate of 18%, and
many who died had underlying conditions that put them at greater risk, according to Henry Ford
Health System. Globally, the mortality rate for hospitalized patients is between 10% and 30%,
and it's 58% among those in the intensive care unit or on a ventilator." Detroit News
-----------------
No comment needed. pl
https://www.detroitnews.com/story/news/local/michigan/2020/07/02/michigan-henry-ford-health-study-finds-hydroxychloroquine-lowers-covid-19-death-rate/5365090002/
Fred
03 July 2020 at 11:38 AM
I agree, no comment is needed. Some charges for medical malpractice and malfeasance
certainly are.
John Credulous ,
03 July 2020 at 01:06 PM
Fred,
There will be no accountability: The b-stards have set the standards.
https://www.bcazlaw.com/surgical-mishaps/ medical community standards concerning treatment methods and technique, and failing to
do so can leave them liable for any resulting damages.https://www.lynchlawyers.com/blog/hospital-medical-malpractice/ medical community's standards for treating patients. This means the hospital or its
staff members cannot cause the patient harm as a result of negligence.https://www.fortheinjured.com/blog/common-medical-errors/ failure to meet these standards results in a
patient's injury or death, the at-fault party can be held liable for medical malpractice
.https://biotech.law.lsu.edu/map/TheCommunityStandard.html
A long "take down" of Fauci:
https://www.unz.com/audio/kbarrett_ken-mccarthy-tony-fauci-is-corrupt-to-the-core/
It'll be 37 years this year he's had the same job in the federal bureaucracy.
There are two million people getting a paycheck from the federal government as
employees. Who do you think the third highest paid employee in the entire federal
bureaucracy is? It's Tony Fauci.
So just to sum all this up: This is not Fauci's first rodeo. He's been pumping hysteria
for 36 years. He always gets it wrong. He was wrong about swine flu. He was wrong about
bird flu. He was wrong about Zika. He was wrong about Ebola. He wildly exaggerated AIDS.
And he always is wrong in the favor of pharmaceutical companies. And he's always wrong in
favor of 'we've got to develop a vaccine now. We have to throw out all the rules.
And his wife is Christine Grady, chief of the Department of Bioethics of the National
Institute of Health and the head of the section on Human Subject Research. She is the
person that makes decisions on what's ethical to do with human subjects. That's his
wife.
BillWade` ,
03 July 2020 at 01:09 PM
Damn it, it's too cheap!
Deap ,
03 July 2020 at 01:54 PM
Uncharted research: areas where anti-malarial drugs are sold widely over the counter - in
malaria prone parts of the world - eg: Central America, SEA and Pacific Islands. How do their
covid rates relate to these specific localities (not just generalized country numbers), where
ongoing prophylactic sales of OTC anti-malaria drugs are most prevalent?
Why does the CDC travel and tourism website info still recommend taking anti-malarial
drugs, when the other hand of our deep state bureaucrats are screaming these drugs will kill
you?
Observational studies are never the equivalent of double-blind randomized studies; but
there can still provide important and fare more readily obtained early information about
these connections and conditions.
jonst ,
03 July 2020 at 01:56 PM
No comment/s needed perhaps. But deliciously anticipated. Here, from the Committee, and
especially from the MSM. Even if only silence. Because "silence is really violence" in this
case.
John Credulous ,
03 July 2020 at 02:17 PM
FWIW, Jimmie Moglia's erudition is formidable, and as a stylist, not too distracting:
https://www.yourdailyshakespeare.com/2020/04/11/the-coronavirus-and-galileo/ As for me I am reminded of the advice that Timon of Athens gave to two robbers who came to
see him, "Trust not the physician, for his antidotes are poison, and he slays more than you
rob."
https://www.yourdailyshakespeare.com/2020/06/08/the-world-upside-down/ And here is an example, a reported 'case-study'. A prince of Persia had melancholia and
suffered from the delusion of being a cow. He would moo like a cow, crying "Kill me so that a
good stew may be made of my flesh," and would never eat anything. Avicenna was persuaded to
treat the case and sent a message to the patient, asking him to be happy as the butcher was
coming to slaughter him. The sick man rejoiced. When Avicenna approached the prince with a
knife in his hand, he asked, "Where is the cow so I may kill it."
The patient then mooed like a cow to indicate where he was. He was then laid on the ground
for slaughter. When Avicenna approached the patient pretending to slaughter him, he said,
"The cow is too lean and not ready to be killed. He must be fed properly and I will kill it
when it becomes healthy and fat. The patient was then offered food, which he ate eagerly and
gradually gained strength, got rid of his delusion, and was completely cured.
How relevant may be the Avicennian case study to the current dynamics of the pandemic I will
leave it to my possible and patient readers to decide.
Ulenspiegel ,
03 July 2020 at 02:20 PM
"No comment needed."
How do you explain the low mortality of the control group in the Michigan study?
egl ,
03 July 2020 at 02:31 PM
"Limitations to our analysis include the retrospective, non-randomized, non-blinded study
design."
turcopolier
03 July 2020 at 02:51 PM
ulenspiegel
Dr. Marc Siegel a medical correspondent for Foxnews told T. Carlson weeks ago that an
emergency treatment of this drug saved the life of his 96 year old father who was at the
point of death, cured him overnight in fact.
Babak makkinejad ,
03 July 2020 at 03:27 PM
Utenspiegel
It is a fact that cancer drugs are not uniformly effective in all patients.
The causes must be sought in the genotypes of the patients.
The differential response as well as effectiveness are not reasons to discard a
therapy.
In further news on COVID-19 Treatments I have 2 items to report:
First one:
The 3-drug mixture of Azittomycin, Naproxen, and prednisolone (oral or injectable) have
been used successfully for reduction of the inflammation of respiratory system.
3 systematic trials have been undertaken and results were conclusive in expediting faster
recovery.
Second one:
Clinical trials in Iran (in Masih Daneshvari hospital) – indicated 100% cure of
COVID-19 in 20 patients using a combination of ReciGen and Cultera (sic?) which is an AIDS
drug.
A second group of patients – 152 – had a reduction in mortality of 20% as
compared to those who were only receiving Cultera (sic.?)
https://www.cinnagen.com/Product.aspx?t=2&l=1&Id=66&f=3
The results are supposed to be published in the Journal of Immunopharmacotherapy.
The dosage was: 5 times day, 12 million units.
No side effects were reported.
egl ,
03 July 2020 at 03:57 PM
ulenspiegel:
This stuff is hard. There are lots of variations in patient populations and treatment
protocols. We have to consider doses, concomitant meds (such as azithromycin), patient status
at time of treatment, age, and, comorbidities.
A big difference: the Ford study was not randomized, not double-blinded. They used a
statistical technique to try to make the groups comparable on factors believed to be
relevant, but this is after fact. (It's a nice technique, I've used it myself, but it doesn't
magically solve all of the difficulties of retrospective analysis.)
In contrast, the recently halted NIH trial was randomized, double-blinded; this was in a
hospital setting. The prophylactic trial reported at the beginning of June in NEJM (author
Boulware) was also randomized, double-blinded; this was in a prophylactic setting.
Seward ,
03 July 2020 at 06:00 PM
Hydroxychloroquine is the active ingredient in the tonic portion of gin and tonics, which
I've been drinking for prophylactic purposes since the pandemic began.
Mina , Jul 3 2020 12:57 utc |
134
"The current work suggests that while the G614 variant may be more infectious, it is not
more pathogenic. There is a hope that as SARS-CoV-2 infection spreads, the virus might become
less pathogenic,"
i.e. that if schools had been left open, it would have spread and became less pathogenic
earlier.https://edition.cnn.com/2020/07/02/health/coronavirus-mutation-spread-study/index.html
Notable quotes:
"... Journal of Virus Eradication ..."
"... Alan MacLeod is a Staff Writer for MintPress News. After completing his PhD in 2017 he published two books: Bad News From Venezuela: Twenty Years of Fake News and Misreporting and Propaganda in the Information Age: Still Manufacturing Consent . He has also contributed to Fairness and Accuracy in Reporting , The Guardian , Salon , The Grayzone , Jacobin Magazine , Common Dreams the American Herald Tribune and The Canary . ..."
alifornia-based pharmaceutical giant Gilead Sciences has
announced that a five-day course of its antiviral drug Remdesivir -- shown in tests to
effectively fight COVID-19 -- will cost $3,120 to Americans with health insurance and $2,340 to
those on Medicaid. Yet
research published in April calculated that the drug could be produced at a profit for as
little as $0.93 per day.
The study, led by Dr. Andrew Hill from the Department of Translational Medicine, University
of Liverpool, U.K., and published in the
Journal of Virus Eradication MintPress spoke with Dr. Hill, who was dismayed by the company's announcement.
We are in a health emergency. We can't have a situation right now where people are unable
to access medicine because the prices are too high. Remdesivir is a drug that has had its
development costs paid for, in large part, by independent donors like governments and
ministries of health in China, the WHO, and the U.S. government. So why should a company be
making money in the middle of a pandemic by selling a drug which has largely been developed
independently of them?" he said.
https://platform.twitter.com/embed/index.html?creatorScreenName=AlanRMacLeod&dnt=true&embedId=twitter-widget-1&frame=false&hideCard=false&hideThread=false&id=1278229120711716865&lang=en&origin=https%3A%2F%2Fwww.mintpressnews.com%2Fpublic-outcry-gilead-charges-3000-covid-19-drug-cost-pennies%2F269110%2F&siteScreenName=MintPressNews&theme=light&widgetsVersion=9066bb2%3A1593540614199&width=500px
News of the decision led to an explosion of public anger. "As Gilead charges $3,120 for its
COVID drug, Remdesivir, remember that the drug was developed with a $70,000,000 grant from the
federal government paid for by American taxpayers. Once again, Big Pharma is set to profit on
the people's dime," wrote former Secretary of Labor
Robert Reich. "This isn't healthcare. It's extortion," appeared to be the overwhelming sentiment
on social media.
Gilead itself, however, seemed not to share this sentiment. Indeed, its
press release on the subject positioned its decision as a selfless and magnanimous gesture
of corporate philanthropy. "We approached this with the aim of helping as many patients as
possible, as quickly as possible and in the most responsible way," said its CEO, Daniel O'Day,
adding that, "under normal circumstances" the company would have charged the public $12,000 per
patient.
"A new low"
Remdesivir is an intravenous antiviral drug that has been used to fight other coronaviruses
like SARS and MERS and has shown some effectiveness against Ebola. Although far from a miracle
treatment, studies have concluded that it aids
recovery, reducing the average hospital visit for COVID-19 patients from 15 days to 11 days
when compared to a placebo. Like with everything coronavirus-related, there is no absolute
scientific consensus. In late April, the WHO accidentally leaked a
Chinese study that suggested Remdesivir may not be as effective as Gilead claims it to be.
Nevertheless, the Trump administration has now bought
up the entire world's stock of the drug, effectively confiscating it and shutting out every
other country from the medicine.
"I've been working in medicine for 32 years and I have never seen anything like it. I've
never seen a country be that brazen. We have to work together. This could be a taste of the
future. They've tried to also do this with advanced orders of vaccines. Imagine if we had a 100
percent effective vaccine and it only went to Americans," Dr. Hill told MintPress
.
At the moment people don't quite understand the gravity of the decision that the American
government has made. This is a worldwide epidemic and we have got to remember that the
clinical trials of Remdesivir were not just conducted in the United States; they were
conducted around European and Chinese centers. Patients put themselves at risk to take part
in an experimental drug trial, and the gratitude we get as other countries after our people
were involved in these studies is to be shut out of the future supply of the drug?! It is
simply ethically unacceptable. I think there are serious questions to be answered. This is a
new low ground, unfortunately," he added.
https://twitter.com/leahmcelrath/status/1277821241496408071
Gilead has been under considerable public scrutiny of late. The company, which
announced profits of $5.4 billion last year, has increased its value by $15 billion since
the pandemic began. In December, MintPress reported
that it was being sued, accused of deliberately holding back a lifesaving HIV drug to extend
the profitability of their previous, inferior one. With shades of the Remdesivir announcement,
the drug is sold in Australia for $8 per month, but the company charges Americans around $2,000
for the same dosage. "Gilead has a long history of profiteering," said Dr. Hill. "Its CEO is a
billionaire and has been accused of tax avoidance; by keeping their intellectual property in
Ireland they avoided $10 billion in taxes in 2016 and they sell drugs for between 100 and 1,000
times the cost of production. And nobody is stopping them. I think this is a taste of things to
come if we don't have better controls on the pharmaceutical industry's excesses."
As of Wednesday morning, there have been 2.73 million confirmed cases of COVID-19 in the
United States, the six worst days for the virus in terms of infections all occurring in the
previous week.
Feature photo | A lab tech displays a package of the Remdesivir at the Eva Pharma Facility
in Cairo, Egypt June 29, 2020. Amr Abdallah | Reuters
Alan MacLeod is a Staff
Writer for MintPress News. After completing his PhD in 2017 he published two books:
Bad News From Venezuela: Twenty Years of Fake News and Misreporting and
Propaganda in the Information Age: Still Manufacturing Consent . He has also contributed to
Fairness and Accuracy in
Reporting , The
Guardian , Salon ,
The Grayzone ,
Jacobin Magazine ,
Common Dreams
the American Herald
Tribune and The
Canary .
Highly recommended !Corrupt Fauci, stupid customers. IT the same neoliberal story of profiteering as a virtue all
over again.
The government bought by Big Pharma, and Big Pharma out or control with questionable drugs
and methods are two side of the same coin
On Monday, Gilead disclosed its pricing plan for Gilead as it prepares to begin charging for
the drug at the beginning of next month (several international governments have already placed
orders). Given the high demand, thanks in part due to the breathless media coverage despite the
drug's still-questionable study data, Gilead apparently feels justified in charging $3,120 for
a patient getting the shorter, more common, treatment course, and $5,720 for the longer course
for more seriously ill patients. These are the prices for patients with commercial insurance in
the US, according to Gilead's official pricing plan.
As per usual, the price charged to those on government plans will be lower, and hospitals
will also receive a slight discount. Additionally, the US is the only developed country where
Gilead will charge two prices, according to Gilead CEO Daniel O'Day. In much of Europe and
Canada, governments negotiate drug prices directly with drugmakers (in the US, laws dictate
that drug makers must "discount" their drugs for Medicare and Medicaid plans).
But according to O'Day, the drug is priced "far below the value it brings" to the
health-care system.
However, we'd argue that this actually isn't true. Remdesivir was developed by Gilead to
treat Ebola, but the drug was never approved by the FDA for this use, which caused Gilead to
shelve the drug until COVID-19 presented another opportunity. Even before the first study had
finished, the company was already pushing propaganda about the promising nature of the drug.
Meanwhile, the CDC, WHO and other organizations were raising doubts about the effectiveness of
steroid medications.
Months later, the only study on the steroid dexomethasone, a cheap steroid that costs less
than $50 for a 100-dose regimen, has shown that dexomethasone is the only drug so far that has
proven effective at lowering COVID-19 related mortality. Remdesivir, despite the fact that it
has been tested in several high quality trials, has not.
So, why is the American government in partnership with Gilead still pushing this
questionable, and staggeringly expensive, medication on the public?
Richard Steven Hack , Jun 28 2020 14:08 utc |
3
"My hunch is that by now doctors have learned much more about the disease's progression
(cytokine storm, blood clotting) and how to manage it."
I believe the UK is where the dexamethasone Study was done. Possibly more doctors are
using it. The Front-Line COVID-19 Critical Care Working Group have been pushing
corticosteroids as the main treatment in their MATH+ Protocol, and they believe the UK study
provides evidence that they are on the right track. Their Protocol specifically targets the
cytokine storm and they use heparin for the blood clots. Now if they can only get a
full-fledged trial going. Unfortunately their Web site doesn't provide much info about how
much traction they're getting promoting their Protocol.
The 1918 SF article proves that morons are morons no matter how many years have passed.
I'm sure there were such during the Black Plague. I sincerely hope the coronavirus mutates
before the second wave and starts killing all the younger people just to see their reaction
when they have to bear the brunt. Can't wait for all the "it's just the flu" BS from these
morons to dry up.
Notable quotes:
"... "Our genetic data confirm that blood group O is associated with a risk of acquiring Covid-19 that was lower than that in non-O blood groups, whereas blood group A was associated with a higher risk than non-A blood groups," the researchers wrote in their report. They found people with Type A blood had a 45% higher risk of becoming infected than people with other blood types, and people with Type O blood were just 65% as likely to become infected as people with other blood types. ..."
European
study links genes, blood type with risk of severe coronavirus infection
(CNN - June 18) A team of European scientists say they have found two genetic variations
that may show who is more likely to get very sick and die from coronavirus, and they say
they have also found a link to blood type.
Their findings, published Wednesday in the New England Journal of Medicine, point to a
possible explanation for why some people get so seriously ill with the virus, while most
barely show any symptoms at all.
(NEJM: Genomewide Association Study of
Severe Covid-19 with Respiratory Failure )
They found people with Type A blood have a higher risk of catching coronavirus and of
developing severe symptoms, while people with Type O blood have a lower risk.
"Our genetic data confirm that blood group O is associated with a risk of acquiring
Covid-19 that was lower than that in non-O blood groups, whereas blood group A was
associated with a higher risk than non-A blood groups," the researchers wrote in their
report. They found people with Type A blood had a 45% higher risk of becoming infected than
people with other blood types, and people with Type O blood were just 65% as likely to
become infected as people with other blood types. ...
June 27, 2020 at 9:41 AM
Anonymous said...
https://www.nejm.org/doi/full/10.1056/NEJMoa2020283
June 17, 2020
Genomewide Association Study of Severe Covid-19 with Respiratory Failure
BACKGROUND
There is considerable variation in disease behavior among patients infected with severe
acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the virus that causes coronavirus
disease 2019 (Covid-19). Genomewide association analysis may allow for the identification
of potential genetic factors involved in the development of Covid-19....
Coronavirus Causes Weaponized 'Tentacles' To Sprout From Infected Cells, Directly Inject
Virus Into New Ones
by Tyler Durden
Fri, 06/26/2020 - 19:25 The virus behind COVID-19 causes infected cells to sprout 'tentacles'
which allow the virus to attack several nearby cells at once - poking holes which allow the
disease to easily transfer inside.
This nightmare fuel was discovered by researchers led by the University of California, San
Francisco.
" There are long strings that poke holes in other cells and the virus passes through the
tube from cell to cell ," said UCSF's Director of the Quantitative Biosciences Institute,
Professor Nevan Krogan. " Our hypothesis is that these speed up infection. "
The images taken by scientists at the National Institutes of Health (NIH) laboratory in
the US and University of Freiburg in Germany will be published in the medical journal Cell on
Saturday.
Most viruses do not cause infected cells to grow these tentacles . Even those that do,
such as smallpox, do not have as many or the same type of branching as Sars-Cov-2, the virus
behind Covid-19. - FT
According to the report, the silver lining is that the tentacle discovery may pave the way
for a number of drugs to work against the disease - most of which were previously being used to
treat cancer.
"It totally makes sense there's an overlap in anticancer drugs and an antiviral effect,"
said Prof. Krogan, who added that cancers, HIV and SARS-CoV-2 are all searching for the
"Achilles heel of the cell."
Potential drugs include silmitasertib, made by Taiwan-based Senhwa Biosciences - which is
working with the NIH on trials in the US. The drug works by inhibiting the CK2 enzyme which is
used to build the tubes.
The drug is one of five which were found to be more effective against the virus than
Gilead's remdesivir , including FDA-approved Xospata (aka gilteritinib) made by Japan-based
Astellas Pharma, Eli Lily's FDA-approved abemaciclib (Verzenio) and ralimetinib, and dasatinib,
made by Bristol-Meyers Squibb.
Remember, the official narrative is that the virus - which specializes in infecting humans
and packs ultra-rare 'infection tentacles' - did not emerge from a Chinese biolab located at
'ground zero' for the pandemic, where scientists had previously come under international
scrutiny for conducting 'gain of function' experiments in which chimeric coronaviruses were genetically
engineered for the sole purpose of infecting humans.
But we digress.
play_arrow Shemp 4 Victory , 1 hour ago
Remember, the official narrative is that the virus - which specializes in infecting
humans and packs ultra-rare 'infection tentacles' - did not emerge from a Chinese biolab
located at 'ground zero' for the pandemic, where scientists had previously come under
international scrutiny for conducting 'gain of function' experiments in which chimeric
coronaviruses were genetically engineered for the sole purpose of infecting humans.
Well, the funny thing is that, despite all the hand-wringing histrionics of the Falun
Gong/Epoch Times cultists, the story of a "weaponized CCP virus" is still just a clickbait
fairy tale. The fact remains that there is zero evidence that the virus emerged from a
Chinese biolab. Zero. Nada. Null. The empty set.
But hey, US citizen society is articulated around monetization of conflicts (among other
things) and cannot do without it. This is how the US has killed the possibility of
debate.
Debate as a means of investigating truth requires to accept facts. In US citizenism,
admittance of facts is counter-balanced by denial of facts. Which one is better to
monetize?
When it comes to US citizens, it is always good to balance admittance with denial, trying
to figure out which one is the most profitable. US citizens always weigh whether it is more
profitable to deny or admit facts, and they usually choose profits over truth.
It is no critical thinking here, it is no education. It is US citizenism. If it is
profitable to deny facts, well, US citizens deny. And will keep denying until it is no longer
profitable.
You can apply this to all fields touched by US citizens. It never misses, because US
citizens nature is eternal.
Truth, justice, freedom: US motto.
JGResearch , 1 hour ago
It was made in Japan., and the U.K.
Japan's Demon Of BioWar Kawaoka Inserted HIV Force Multipliers Inside The Wuhan Virus - No
governments will ever state this truth. It would lead to war and even the Chinese do want
that. They want business back to normal. The Chinese are not so concern about some workers
and elders who are on the public welfare.
It is still a Bio-engineered virus, but it is from Veterinary labs that are not being
watched like Bio 4 labs, from second generation of Unit 731. Who knows bat and fish better
than anyone else, it is the Veterinary labs. Imperial Japanese have a long history with
China. For the most part, Suzuki's military-dominated cabinet favored continuing the war. For
the Japanese, surrender was unthinkable -- Japan had never been successfully invaded or lost
a war in its history, plus they were hit with two Atomic weapons. You think they forgot about
at that?
The dark side of microbiology finds its haven inside the dozens of veterinary schools
outside the authority of the WHO, CDC, NIH and equivalent professional supervisory bodies and
reporting-review systems.
Exhibit A: To summarize, a decade ago at his lab in Wisconsin with generous funding from
Japanese state institutions, Kawaoka was developing an "unstoppable flu", secretly derived
from an illegal exhumation of the Arctic frozen corpse of an Alaskan native who died in the
1918-19 influenza pandemic, which killed up to 80 million worldwide. We learned of Kawaoka's
reckless violations of science ethics from Robert Finnegan, former editor of the Jakarta
Post, who was tracking the theft of MERS and other virus samples from NAMRU-2 (U.S. Navy
Research Unit) by a senior local lab technician who personally smuggled the dangerous
materials to U Wisconsin.
Exhibit B is a 2011 research paper by Y. Kawaoka and two colleagues at his animal virology
lab at the University of Wisconsin-Madison, titled "HIV reverse-binding protein is essential
for influenza A virus replication and promotes genome-trafficking in late-stage infection".
Published in the Journal of Virology, September 2011, it's an admission of guilt for
preparing the emergence of the Wuhan contagion.
JGResearch , 1 hour ago
The original plan: The dilution of toxicity indicates the objective as being mild symptoms
diagnosed as a case of food poisoning. On a massive scale, a food poisoning scandal would
lead to the shut down of fisheries and aquaculture in a huge blow to national food
security.
However, what's so amazing about the Wuhan coronavirus was its regeneration after being
clipped of virulence-causing genes that intensify the pain of symptoms in its victims.
nCov2019 somehow reconstructed alternative sequences to replace the lopped-off gene sequence.
The Japanese ignore the morphogenetic fields of the virus.
Therein lies the rub. Prophetically, Kawaoka foresaw HIV acting in unexpected ways in
constructing new flu virions and their components, which likely explains how and why the
at-first relatively mild version bio-engineered Wuhan coronavirus was self-altered in its
third or fourth generation with highly lethal proteins, a spontaneous Gain of Function, which
transformed 2019-nCov into a raging killer.
This is exactly what occurred in early January when the Chinese government banned fishing
and consumption of fish along the entire 6,300 km (3,900 miles) length of the Yangtze
River.
JGResearch , 1 hour ago
https://www.scmp.com/news/china/society/article/3044376/china-bans-fishing-depleted-yangtze-river-10-years-protect
https://jvi.asm.org/content/85/18/9588
https://jvi.asm.org/content/85/18
DefendYourBase , 1 hour ago
JUST DA FLU!
warsev , 2 hours ago
I've read any number of articles from "experts" in the field who claim that this thing is
"engineered". The "experts" get very little play outside of a small echo chamber. I want to
know when anyone with any political clout will start shouting about it more broadly. Doesn't
seem likely.
Cthonic , 1 hour ago
accredited virologists are kept in line
http://tapnewswire.com/2016/02/list-of-over-100-dead-microbiologists/
Cthonic , 1 hour ago
have another 100 hits
https://time.com/3003840/malaysia-airlines-ukraine-crash-top-aids-researchers-killed-aids2014-mh17/
DFCtomm , 2 hours ago
I caught an episode of peak prosperity on youtube the other day and they were talking
about supercells and multiple nuclei. This makes sense. This virus behaves more like a
colonizing bacteria.
4Celts , 2 hours ago
What I was most disgusted by the " Task Force " presser today, was that the orchestrators
have noticed all of the pushback on the statistics showing the small demographic that was
most effected by this " virus . So , they put the maggot Fauci out there to say the " young "
who are asymptomatic were the cause of the " second wave " , and they should really curb
their youthful bravado and instead be very mindful that " they " could spread this to the
immunodeficient , both the elderly and the child with cancer. A totally spineless, and
despicable tact.
FrankDrakman , 2 hours ago
In Ontario, 1.3 million have been tested for the virus. Outside of nursing homes, only 960
have died.
Can you divide 960 by 1.3 million, "boob"? Let me help you.. 130,000 is 10%, 13,000 is 1%,
and 1,300 is 0.1%
960 is .078%. In other words, you have 99.92% chance of surviving this bug. Wow, 'far more
deadly than originally thought', indeed.
ilsm said...
Anonymous,
https://www.nature.com/articles/d41586-020-00502-w
"11 May -- High risk of COVID-19 death for minority ethnic groups is a troubling
mystery:"
"People who are not white face a substantially higher risk of dying from COVID-19 than
do white people -- and pre-existing health conditions and socioeconomic factors explain
only a small part of the higher risk."
"In the most sweeping study of its kind, Ben Goldacre at the University of Oxford, UK,
and his colleagues examined the medical records of more than 17 million residents of
England (E. Williamson et al. Preprint at medRxiv http://doi.org/dt9z; 2020). The analysis,
which has not yet been peer reviewed, showed that medical conditions such as diabetes are
linked to a higher risk of death from the new coronavirus."
"But the prevalence of such conditions in people who belong to minority ethnic groups
plays only a small part in the heightened risk, as does the prevalence of social
disadvantages such as low income. The researchers say that there is an urgent need for
better measures to protect people in minority ethnic groups from the disease."
This is from Nature daily Covid 19 update. Which is good reading and covers vaccines,
and anti body treatments which may be used by Autumn. See ELI Lilly and Regenron
debvelopments.
June 26, 2020 at 2:51 PM
https://www.nytimes.com/2020/06/26/us/corona-virus-latinos.html
June 26, 2020
Many Latinos Couldn't Stay Home. Now Virus Cases Are Soaring in the Community.
June 26, 2020 at 1:48 PM
JBR,
Thanks for your forbearances, misguided as you may be.
You do not answer questions, you do not like. Okay, with me. You could attempt to revise
my conclusions on your lack of openness to countering evidence.
For Fred, from my son's latest input. Fred is an RPI alum, within a years or two, with
me:
"Stockholm is the best population to test Covid theory whereby it was hit hard early and
did not have lockdowns.
The same will probably happen in states which were not hit hard during the first
wave"
The tweet thread goes on to list the states that have not yet reached the 20% threshold,
which is many, though if these states only need to reach 15-20% to exit the first wave,
then most of them are at least halfway there."
https://twitter.com/gummibear737/status/1275118332887392256?fbclid=IwAR3udQL8UNl8o05RTmtpOmlxDyVb57NptU9WqwhAzUXe9J1WfKE1FF4PYnY
Why the US is in for rocky road with or without "second wave".
Concluding any of oit due to Trump is a stretch.
June 26, 2020 at 8:57 AM
Stanford Prof: Median Infection Fatality Rate Of COVID-19 For Those Under-70 Is Just
0.04% by Tyler
Durden Mon, 06/22/2020 - 22:50 Authored by Daniel Payne via JustTheNews.com,
A scientist known for his contrarian takes to dire COVID-19 predictions has released a paper
claiming that antibody evidence suggests the median coronavirus infection fatality rate for
those under 70 is just 0.04%.
The estimate throws into sharp relief the lopsided mortality figures for the disease, which
has claimed an inordinate number of elderly people across the planet while leaving younger
individuals mostly unscathed.
John Ioannidis, a professor of epidemiology and population health at Stanford University,
argues in a paper published
earlier this month that COVID-19 "seroprevalence studies," which measure infection rates using
the presence of antibodies in blood samples, "typically show a much lower fatality than
initially speculated in the earlier days of the pandemic."
"It should be appreciated," he writes in the paper, "that [the fatality rate] is not a
fixed physical constant and it can vary substantially across locations, depending on the
population structure, the case-mix of infected and deceased individuals and other, local
factors. "
In the paper, which has not yet been peer-reviewed, Ioannidis surveyed 23 different
seroprevalence studies and found that "among people <70 years old, infection fatality rates
ranged from ... 0.00-0.23% with median of 0.04%."
The median fatality rate of all cases, he writes, is 0.26%, significantly lower than some
earlier estimates that suggested rates as high as over 3%.
In the paper, Ioannidis acknowledges that "while COVID-19 is a formidable threat," the
apparently low fatality rate compared to earlier estimates "is a welcome piece of
evidence."
"Decision-makers can use measures that will try to avert having the virus infect people
and settings who are at high risk of severe outcomes," he writes.
"These measures may be possible to be far more precise and tailored to specific high- risk
individuals and settings than blind lockdown of the entire society."
Beibdnn , Jun 19 2020 23:24 utc |
46
I live in France. From Monday 22nd June people can travel more than 100 kilometers from home
and people from outside the country can enter without travel resrictions.
However when I go out I wear a mask as do many others. People serving in shops wear a face
shield.
As I am one of those persons at risk of death from contracting the Coronavirus, my doctor
has advised me not to allow any visitors from other countries to visit until the Spring of
2021.
I don't know what the figures of infection are but national T.V. has been warning people
of a second infection arriving this winter.
It seems some European countries as was noted above are taking the crisis more seriously
than others.
Passer by , Jun 19 2020 23:30 utc |
48
Posted by: Jackrabbit | Jun 19 2020 23:09 utc | 44
Europuppets.
I said many times - in the vast majority of cases, the EU (Europe) is propping up and
covering up the US Empire.
They are eager puppets and they can not exist without the Empire. They simply degenerated
due to long puppetry where the US is the Alpha and the Omega and history starts with Big
Daddy US liberating them from themselves in 1945.
PARIS (Reuters) - French protesters on Saturday doused the country's health ministry with
red paint, to symbolize the blood of those who died from COVID-19 and to demonstrate against
poor working conditions for public sector healthcare workers.
"For years, health workers have been alerting us to the fact they don't have enough
resources with regards to staff, beds and equipment to be able to allow us to look after people
decently," Aurelie Trouve, a spokeswoman for the 'Attac' activist group which was behind the
protest, told Reuters.
They also placed a giant, medal-shaped banner dubbed 'Medal of Contempt' on the steps of the
French health ministry, to highlight what they said was the government's failure to listen to
the concerns of healthcare workers.
President Emmanuel Macron's government has decided to pay a 1,500 euros ($1,676) bonus to
public sector healthcare workers, in recognition of their role during the coronavirus
outbreak.
Yet many in the sector feel the government should do more for them, and violence broke out
this week at another protest held by healthcare workers in Paris.
The bigger problem with achieving herd immunity through infections is that it defeats the
purpose of reaching herd immunity at all.
"The whole point is to minimize death and morbidity, but even if there is a high rate of
asymptomatic or mild disease, you're still going to have millions of deaths," Rasmussen says.
"What good is herd immunity if millions of people have to die to get there?"
Remember that threshold of 60% to 80% to bring about herd immunity to Covid-19? There's a
reason for it being a range.
Jenkins says, "60% is often bandied around as the level you need to drive the reproductive
number below one, but it still takes time for transmission to go down." But adds, "the final
size of people who might be infected before you see no more transmission would be higher,
more like 80 or 85%."
Researchers call this "overshoot," where "an epidemic doesn't magically stop when you
reach herd immunity," as University of Washington biology professor Carl Bergstrom, PhD,
described it on Twitter. "You reach herd immunity not when the epidemic is nearly over, but
rather *precisely* at the epidemic peak," he explained.
Murray offers this analogy: "I think of it like a train. It's going along slowly, then
it's getting up to speed, and then you pull the brake -- but it's not going to stop
immediately. It's got to slow down."
With a current U.S. population of around 330 million people, a 60% infection rate is about
198 million people. Using the low estimate of a 0.5% death rate, nearly a million people will
die (for context, as of May 13, the official death toll was just over 80,000). If the
fatality rate is closer to 3%, nearly 6 million will die.
And that's just when the brake is pulled, when infections start to taper down. Reaching
80% means 1.3 to 7.9 million dead Americans -- with no guarantee transmission will stop.
Of course, if you're Trump (or me, for that matter), you don't give a shit how many people
die as long as it isn't you.
Posted by: Richard Steven Hack | Jun 20 2020 0:52 utc |
70
Notable quotes:
"... "We've seen a small number of laboratories that are charging egregious prices for Covid-19 tests," said Angie Meoli, a senior vice president at Aetna, one of the insurers required to cover testing costs. ..."
"... The second outcome is huge price variation, as each doctor's office and hospital sets its own charges for care. One 2012 study found that hospitals in California charge between $1,529 and $182,955 for uncomplicated appendectomies. ..."
"... "It's not unheard-of that one hospital can charge 100 times the price of another for the same thing," said Dr. Renee Hsia, a professor at the University of California, San Francisco, and an author of the appendectomy study. "There is no other market I can think of where that happens except health care." ..."
"... But American patients will eventually bear the costs of these expensive tests in the form of higher insurance premiums. In some cases, they are paying for additional tests, for flu and other respiratory diseases, that doctors tack onto coronavirus orders. Those charges are not exempt from co-payments and can fall into a patient's deductible. ..."
"... Those kinds of bills could make patients wary of seeking care or testing in the future, which could enable the further spread of coronavirus. In an April poll, the Kaiser Family Foundation found that most Americans were worried they wouldn't be able to afford coronavirus testing or treatment if they needed it . ..."
anne ,
June 16, 2020 11:05 am
https://www.nytimes.com/2020/06/16/upshot/coronavirus-test-cost-varies-widely.html
June 16, 2020
Most Coronavirus Tests Cost About $100. Why Did One Cost $2,315?
In a one-story brick building in suburban Dallas, between a dentist office and a family
medicine clinic, is a medical laboratory that has run some of the most expensive coronavirus
tests in America.
Insurers have paid Gibson Diagnostic Labs as much as $2,315 for individual coronavirus
tests. In a couple of cases, the price rose as high as $6,946 when the lab said it mistakenly
charged patients three times the base rate.
The company has no special or different technology from, say, major diagnostic labs that
charge $100. It is one of a small number of medical labs, hospitals and emergency rooms
taking advantage of the way Congress has designed compensation for coronavirus tests and
treatment.
"We've seen a small number of laboratories that are charging egregious prices for
Covid-19 tests," said Angie Meoli, a senior vice president at Aetna, one of the insurers
required to cover testing costs.
How can a simple coronavirus test cost $100 in one lab and 2,200 percent more in another?
It comes back to a fundamental fact about the American health care system: The government
does not regulate health care prices.
This tends to have two major outcomes that health policy experts have seen before, and are
seeing again with coronavirus testing.
The first is high prices over all. Most medical care in the United States costs double or
triple what it would in a peer country. An appendectomy, for example, costs $3,050 in Britain
and $6,710 in New Zealand, two countries that regulate health prices. In the United States,
the average price is $13,020.
The second outcome is huge price variation, as each doctor's office and hospital sets
its own charges for care. One 2012 study found that hospitals in California charge between
$1,529 and $182,955 for uncomplicated appendectomies.
"It's not unheard-of that one hospital can charge 100 times the price of another for
the same thing," said Dr. Renee Hsia, a professor at the University of California, San
Francisco, and an author of the appendectomy study. "There is no other market I can think of
where that happens except health care."
There is little evidence that higher prices correlate with better care. What's different
about the more expensive providers is that they've set higher prices for their services.
Patients are, in the short run, somewhat protected from big coronavirus testing bills. The
federal government set aside $1 billion to pick up the tab for uninsured Americans who get
tested. For the insured, federal laws require that health plans cover the full costs of
coronavirus testing without applying a deductible or co-payment.
But American patients will eventually bear the costs of these expensive tests in the
form of higher insurance premiums. In some cases, they are paying for additional tests, for
flu and other respiratory diseases, that doctors tack onto coronavirus orders. Those charges
are not exempt from co-payments and can fall into a patient's deductible.
Those kinds of bills could make patients wary of seeking care or testing in the
future, which could enable the further spread of coronavirus. In an April poll, the Kaiser
Family Foundation found that most Americans were worried they wouldn't be able to afford
coronavirus testing or treatment if they needed it .
Caliman , Jun 17 2020 17:28 utc |
9
Perhaps one of the well-read people here can help me find some sources. I've been puzzled
by something before and it got exacerbated by the news recently that the Polio vaccine may
be useful to prep the body, as it were, for COVID19.
What I'd be puzzled by is the following: we know there are four commonly circulating
human coronaviruses that register as "colds" in the population, sometimes nasty but
generally not dangerous, and that large %ages of us have gotten them over the years and
will continue to. While these four viruses are not identical to COVID19, they are quite
similar. And it seemed like there were some reports that people who had recently been sick
with these more common coronaviruses had some immunity to COVID19.
Has this been investigated further? Would it not make sense, if true, that the "quick
vaccine" we have been looking for could be purposeful infection by one of these common
human coronaviruses? Would this not be like using the cowpox as a way to make ourselves
more resistant to smallpox, which used to be done until the actual smallpox vaccine was
discovered?
Anyway, anybody read anything along these lines?
hopehely , Jun 17 2020 17:47 utc |
10
@Caliman | Jun 17 2020 17:28 utc | 9
Anyway, anybody read anything along these lines?
Yes, we
read it here a month ago.
albagen , Jun 17 2020 17:56 utc |
11
Well Caliman, why do you bother thinking about Covid19? It's just the flu, on tap. When
they need, they open the tap. When it suits them, they close the tap. It's Covid19 on,
Covid19 off. Sometimes it trickles or drips. We all will die some day.
In other words: "behave, or else we bring back the restrictions", but if the flow of
money stops, we will lift them, just so that you work to produce something and keep us
happy.
My suggestion: live your life to the fullest, enjoy nature and family, as if there is no
covid19, no government, no bullshit. You won't regret it.
And don't forget to give feedback here, if you follow my advice.
;)
Trial results announced on Tuesday showed dexamethasone, which is used to reduce
inflammation in other diseases such as arthritis, reduced death rates by around a third among
the most severely ill of COVID-19 patients admitted to hospital.
"This is an extremely welcome result," said Peter Horby of Oxford, one of the study leaders. "The survival benefit is clear and
large in those patients who are sick enough to require oxygen treatment, so dexamethasone should now become standard of care in these
patients. Dexamethasone is inexpensive, on the shelf, and can be used immediately to save lives worldwide."
Lead researcher, Prof. Martin Landray, says that hospital patients should now be given the steroid without delay, but that people shouldn't
try to hoard it for private use. According to the study, Dexamethasone does not appear to help milder cases - those who don't need help
breathing.
The drug has been used to treat a wide range of conditions, including asthma and rheumatoid arthritis. Notable quotes:
"... Chief investigator Prof Peter Horby said: "This is the only drug so far that has been shown to reduce mortality - and it reduces it significantly. It's a major breakthrough." ..."
By Michelle Roberts Health editor, BBC News online
A cheap and widely available drug can help save the lives of patients seriously ill with coronavirus.
The low-dose steroid treatment dexamethasone is a major breakthrough in the fight against the deadly virus, UK experts say.
The drug is part of the world's biggest trial testing existing treatments
to see if they also work for coronavirus.
It cut the risk of death by a third for patients on ventilators. For those on oxygen, it cut deaths by a fifth.
Had the drug had been used to treat patients in the UK from the start of the pandemic, up to 5,000 lives could have been saved,
researchers say.
And it could be of huge benefit in poorer countries with high numbers of Covid-19 patients.
About 19 out of 20 patients with coronavirus recover without being admitted to hospital. Of those who are admitted to hospital,
most also recover, but some may need oxygen or mechanical ventilation. These are the high-risk patients whom dexamethasone appears
to help.
The drug is already used to reduce inflammation in a range of other conditions, and it appears that it helps stop some of the
damage that can happen when the body's immune system goes into overdrive as it tries to fight off coronavirus.
The body's over-reaction is
called a cytokine
storm and it can be deadly.
In the trial, led by a team from Oxford University, around 2,000 hospital patients were given dexamethasone and were compared
with more than 4,000 who did not receive the drug.
For patients on ventilators, it cut the risk of death from 40% to 28%. For patients needing oxygen, it cut the risk of death from
25% to 20%.
Chief investigator Prof Peter Horby said: "This is the only drug so far that has been shown to reduce mortality - and it reduces
it significantly. It's a major breakthrough."
Lead researcher Prof Martin Landray says the findings suggest that for every eight patients treated on ventilators, you could
save one life.
For those patients treated with oxygen, you save one life for approximately every 20-25 treated with the drug.
"There is a clear, clear benefit. The treatment is up to 10 days of dexamethasone and it costs about �5 per patient. So essentially
it costs �35 to save a life. This is a drug that is globally available."
Prof Landray said, when appropriate, hospital patients should now be given it without delay, but people should not go out and
buy it to take at home.
Dexamethasone does not appear to help people with milder symptoms of coronavirus - those who don't need help with their breathing.
The Recovery Trial has been running since March. It included the malaria drug hydroxychloroquine which has subsequently been
ditched amid concerns that it increases fatalities
and heart problems.
Eric Feigl-Ding ✔ @DrEricDing
Replying to @DrEricDing
5) And again, Dexamethasone is cheap, available from any pharmacy, and easily obtainable anywhere in the world. This is EXACTLY
what we need, instead of a $1000 drug like remdesivir that is just marginally effective for shortening illness but not yet fully
proven for mortality.
Deap ,
15 June 2020 at 11:49 AM
Walrus, another topic doctors talk about privately are the well-known "bad doctors" who keep
getting free passes mistake after mistake, and often sit on hospital quality review
committees.
As well as talking among themselves about the large numbers of iatrogenic deaths, caused
by the medical community itself, which have long exceeded the numbers of "corona" deaths,
ginned up covid numbers or not.
Be well and thrive.
All of the UCSF doctors said they saw patients in their forties and fifties, who didn't meet
the "typical" profile for Covid-19 because they were otherwise healthy. In the Queens hospital,
where Peters worked, many of the patients were Black or Hispanic. Data shows that the virus has
hit racial and ethnic minorities worse, and studies are underway to better understand why.
Authored by Jeff Harris via The Ron Paul Institute for Peace & Prosperity, A Glaring
Omission
With the 24/7 media circus coverage of Covid-19 I find it particularly interesting that
there is an obvious glaring omission of some extremely important facts relative to dealing with
a virus, especially one that is allegedly so virulent like this one. Yes, I read all about the
critical need to shelter in place, stay inside away from other people, wash your hands
constantly, avoid touching your eyes, nose or mouth, wear your face mask and by all means
observe social distancing if you MUST venture outside for food!
Then it's repeated ad infinitum that the ONLY hope we have of ever returning to a semblance
of normalcy is to have a vaccine to protect us! Then to add some drama to this narrative the
media highlights their death-o-meter scoreboard with the implied threat that you'll be next IF
you don't obey the rules as dictated by the "experts".
But what is assiduously avoided at all cost is any reference to our most potent defense
against any virus; our body's natural immune system. Try as I might I couldn't find anything
about this first line of defense on the World Health Organizations (WHO) website or Centers for
Disease Control (CDC) website. It's as if it doesn't exist and is completely irrelevant.
If these organizations were genuinely concerned about the health of citizens they would
obviously discuss the vital role a healthy immune system plays in protecting us from illnesses.
But since they don't its obvious some other motive is at work, at least to me, and I strongly
suspect to other critical thinkers as well.
We now know from the science and data that over 90% of the people exposed to Covid-19 have
no symptoms at all or at worst a mild cold. The flu vaccines we have are only effective 30% to
60% of the time and the bugs change regularly so a vaccine that worked OK last year may barely
work at all this year. Let's learn some more about our body's immune system.
Virus
protection without a vaccine
There is an enlightening article on Web MD titled: "How to use Your Immune System to Stay
Healthy". That's a pretty straight forward title now isn't it? Early on Bruce Polsky, MD,
interim chairman department of medicine and chief division of infectious disease at St.
Lukes-Roosevelt Hospital Center in New York City says:
"We are endowed with a great immune system that has been designed evolutionarily to keep
us healthy."
The article goes on. . .
"The immune system is your body's natural defense system. It's an intricate network of
cells, tissues and organs that band together to defend your body against invaders. Those
invaders can include bacteria, viruses, parasites, even fungus, all with the potential to
make us sick. They are everywhere-in our homes, offices and backyards. . . "
The truth is no amount of social distancing, hand washing or face mask wearing is going to
eliminate our exposure to these various bugs. That's why we were created with this amazing
first line of natural defense.
Here's more from Web MD . . .
"The immune system can recognize millions of different antigens. And it can produce what
it needs to eradicate nearly all of them. When it's working properly, this elaborate defense
system can keep health problems ranging from cancer to the common cold at bay. . . "
Wow! That's pretty amazing stuff isn't it! According to Web MD a properly functioning immune
system can "keep health problems ranging from cancer to the common cold at bay." So why isn't
this "science" being included in all the other health recommendations we're being bombarded
with daily? It seems to me that any "expert" worth their salt would be talking about the
importance of a healthy immune system to stay healthy.
But there's more . . .
The Web MD article noted that failure to eat a healthy diet, sitting around not exercising,
not getting enough sleep and chronic stress can all lead to a compromised immune system. To
quote Dr. Polsky again:
". . . Lifestyle aspects are very, very important."
So if our lifestyle is very, very important to staying healthy as the good doctor says ask
yourself this question? Based on the Web M.D. article virtually all the results of the lockdown
serve to weaken our immune systems. The stress of unemployment, constant harping about
infections and rising death rates, lack of exercise and now a crack in our food distribution
system all are known to weaken the human immune system.
I also find it quite interesting that large groups of people can shop at Walmart, Home Depot
or other big box stores but they can't attend their local church even if it's a "drive through"
service?
Web M.D. says:
"Research shows that people with close friendships and strong support systems tend to be
healthier than those who lack such supports."
During times of crisis people need encouragement and their faith built up more than ever
before. Mandating people huddle in fear in their homes with constant media reports of
infections and death bombarding them continually is there any wonder peoples immune systems are
under severe stress?
Admitting their own blunder: Better late then never
Masks "are strongly encouraged in settings where individuals might raise their voice," the
CDC guidance said.
The agency also recommended limiting attendance to allow for distancing.
"Coronavirus vaccine developers are chasing outbreaks before they disappear"
Washpost
"The top teams rushing to develop coronavirus vaccines are alerting governments, health
officials and shareholders that they may have a big problem : The outbreaks in their countries
may be getting too small to quickly determine whether vaccines work
A leader of the Oxford University group, one of the furthest ahead with human trials, admits
the reality is paradoxical, even "bizarre," but said the declining numbers of new infections
this summer could be one of the big hurdles vaccine developers face in the global race to beat
down the virus.
Even as new cases are growing worldwide, transmission rates are falling in Britain, China
and many of the hardest-hit regions in the United States -- the three countries that have
experimental vaccines ready to move into large-scale human testing in June, July and August."
Washpost
---------------
Well, pilgrims it would seem that the Post staff does not see the irony in their own
writing, or perhaps they do. There have been scattered evidences of rationality there lately.
Even as Democrat governors and mayors across the country drag their feet on the re-opening of
the American economy, infection rates are falling. In the Faucibirxist view of things
everything depends on vaccine development (or herd immunity post holocaust). But, alas there
just aren't enough new, vibrant infections to make development of the vaccines convenient. What
will happen to the flow of government money to these projects if this phenomenon becomes
general knowledge. Someone at the Post should be disciplined for this indiscretion. pl
https://www.washingtonpost.com/world/europe/coronavirus-vaccine-trials-astrazeneca-moderna/2020/06/09/48f28fea-a414-11ea-898e-b21b9a83f792_story.html
Fred
10 June 2020 at 09:34 AM
"What will happen to the flow of government money to these projects if this phenomenon
becomes general knowledge."
Well Fauci is almost 80 so I think he's set for life. I hear the left wants lots of
redevelopment funds and jobs programs, with the attendant opportunities for graft that comes
with them, for thier cities which we are all assured had neither rioting nor looting.
Jim ,
10 June 2020 at 11:50 AM
Thank you Col. Lang for all the posts on novel coronavirus.
For shining light on this, this utter failure by the medical community and their various
and sundry enablers in government and in business.
On these liars and charlatans and killers and criminals.
The video below is about an hour long. It is a nurse, who worked in NYC hospital, the
alleged epi center of epi centers.
She basically says, without saying directly, but points to the fact that doctors were
murdering patients there, it seems.
She paints a picture of doctors not as scientists but as zealots, as neo neanderthals, as
craven monsters, who care not about life, the elderly, the sick, the least among us.
As Nurse Ratchets
Towards the end of video, she recounts her last day at this hospital, discussing a patient
she had nursed for many days, and who was doing fine, making progress, . . . and how she was
removed from his bed on direct orders, sent to the ER where she was not assigned, and 20
minutes later, the man she was caring for is dead.
These sorts of stories abound; this rage is not going away anytime soon. This is the rage,
and what caused it, that our "lords and masters" who censor us and tell us black is white,
and want to destroy our country. . . this is the rage they don't want to see expressed and
exposed. Will they get their way?
http://edwardcurtin.com/the-undercover-epicenter-nurse-watch-weep-and-rage/
Laura Wilson ,
10 June 2020 at 01:04 PM
Well...they can always test their vaccines in the USA. We seem not to be faring as well and
can help out. (I believe this is a glass half-full moment.)
Walter Lang
10 June 2020 at 01:27 PM
Laura Wilson
Still hysteric. if you are not over 65 and not in compromised health the disease is rarely
fatal.
optimax ,
10 June 2020 at 01:32 PM
Trump needs to stop the $600 a week federal bonus to the unemployed. My neighbor told me
about how his daughter-in-law worked one day a week as a barmaid before the virus shut the
bar down and made a little over a hundred a week. Oregon unemployment pays her 150 a week and
with the added 600 she now makes over 7 times what she did working. How many protesters and
rioters are just as flush getting paid to party in the street? Most i'd say. That makes these
government funded protests a powerful voice and recruitment tool for the Democratic Party.
Ending the federal subsidy to the unemployed would reduce, if not stop, the demonstrations
and mau-mauing of the country.
Fred
10 June 2020 at 03:17 PM
optimax,
Absolutely. There were howls of protests before Minneapolis when Georgia, Florida and
Texas started tellling people that if they recieved a recall to work notice from an employer
and refused to go they would be considered a voluntary quit and no longer eligable for
unemployment insurance payments. They'll howl again when they figure out this is all taxable
income.
LA
Sox Fan
10 June 2020 at 03:21 PM
Take everything the WaPo claims with a grain of salt. There is no real worry over lower covid
infections. What made Covid decrease was the lockdowns. Remove the lockdowns and covid
infection rates will climb, as we are seeing in the already reopened states.
Then when fall rolls around, and people are stuck indoors again, rates will skyrocket.
There will be plenty of test subjects for a vaccine.
rho ,
10 June 2020 at 09:29 PM
With the spread rate of the coronavirus, any outbreak of the infection will peter out once
the total immunity rate of the population approaches 65-70 percent.
In Bergamo (Italy), 57 percent a population sample have tested positive for coronavirus
antibodies, which means that they must have had the infection before and are now most likely
immune.
If you are a Karen, then don't listen to me, but take it from the German government's very
own propaganda outlet, Deutsche Welle:
"Out of nearly 10,000 Bergamo residents who had their blood tested between April 23 and
June 3, 57% had antibodies, indicating they had come into contact with the virus and
developed an immune response.
Health authorities said the sample size was 'sufficiently broad' to be a reliable
indicator of the presence of SARS-CoV-2 among Bergamo province's population."
https://www.dw.com/en/coronavirus-tests-show-half-of-people-in-italys-bergamo-have-antibodies/a-53739727
Nobody in Bergamo will need a coronavirus vaccine once its development is finished -
whenever that may happen, if at all.
Highly recommended !
BM , Jun 10 2020 18:11 utc |
5
Yale has published research that shows HCH + AZ has 50-fold benefits and insignificant
risks
Using
Hydroxychloroquine and Other Drugs to Fight Pandemic
Early
Outpatient Treatment of Symptomatic, High-Risk Covid-19 Patients that Should be
In the author's words:
COVID-19 is really two different diseases. In the first few days, it is like a very bad
cold. In some people, it then morphs into pneumonia which can be life-threatening. What I
found is that treatments for the cold don't work well for the pneumonia, and vice versa.
Most of the published studies have looked at treatments for the cold but used for the
pneumonia. I just looked at how well the treatments for the cold worked for the cold. There
are five studies done this way, four of hydroxychloroquine plus azithromycin and one with
hydroxychloroquine plus doxycycline, and they all show that treating the cold part of
COVID-19 -- the early part -- works very well.
The article completely decimates the arguments against using HCQ + AZ or HCQ +
doxycycline, specifically in early outpatient use.
uncle tungsten , Jun 10 2020 22:29 utc |
41
BM #5
re Yale HCQ study.
The article completely decimates the arguments against using HCQ + AZ or HCQ + doxycycline,
specifically in early outpatient use.
It is good to see real science being applied rather than voodoo shilling for big
pharma.
Still waiting for the editor resignations at Lancet and NEJM on their publication of the
hoax science article.
Let me be very clear about pharmaceuticles: the interaction of two dissimilar substances
can be extraordinary beneficial. My personal example is from a Specialist Pharmacologist that
treated a bone disease in my thumb arising from mechanical injury. He explained thus:
The bone problem has three quite separate stages of treatment.
At the first week common antibiotic remedies are vital and effective. I was too late for
that.
If that stage is missed then a common and potent antibiotic combined with a substance
commonly used to treat gout is vital. The combination of the two flattens the peak of the
antibiotic such that it is sustained in the bloodstream for 24 hours until the next dose of
the two. A fourteen day process as I recall. It was totally successful.
If that second stage is missed then late intervention is extensive use of antibiotics and
the gout remedy over months as the bone decomposition bacteria have spread throughout ones
metabolism and lodge randomly to wreak havoc. This treatment regime is punishing on the body
and digestive tract and many people cannot endure it.
This Specialist was a high street operator in nice office NOT a pharmacy.
So lets not be jumping to hasty dismissals of what may or may not 'work' and when. Humans
vary, diets vary and propensities are highly variable. It is the responsibility of scientists
to be honest and act in the best interests of humanity. Clearly the study published in the
Lancet and NEJM was fake science and those journals fell for it because of either inadequate
editorial investigation of the paper, confirmation bias, inadequate consideration of human
consequences.
The WHO stands condemned for being suckered by fake news, confirmation bias, malign
financial manipulation or perhaps inadequate investigation of the authors and claims of the
paper.
oldhippie , Jun 7 2020 23:59 utc |
45
PavewayIV @ 36
Try doing a search on Kary Mullis, creator of the PCR process. He died last year so we can
only go by past statements. He always stated that PCR was completely inappropriate and
meaningless for diagnostics or for any other clinical purpose.
CDC guidance on PCR until earlier this year was that doctors do diagnosis, not
laboratories. Doctors were allowed to consider PCR results as a factor, cautioned not to rely
on them. In current situation PCR results are the definition of COVID.
If the test is allowed to run too many cycles any sample will test positive.
And it is never entirely certain how many cycles have elapsed, clock does not tell exactly
what the RNA is up to.
We were told for months we'd never gather in public again 'because Covid-19.'
...Media, politicians and celebrities who spent the past three months lecturing Americans
about the importance of staying home and keeping at least six feet away from all other humans
lest they catch or spread the deadly coronavirus have suddenly pivoted on a dime –
seemingly as one – to cheering on those Americans defying their advice to pour into the
streets and join nationwide protests...
Posted on
May 25, 2020 by Lambert Strether of
Corrente
I was considering using "All that is fomites melts into air," but I couldn't bring myself
to, so count yourself lucky (and anyhow, it's not really true). From the beginning of the
#COVID19 pandemic, we've been washing our hands, masking up, cleaning surfaces, and social
distancing. These measures have worked (
especially masking ), but now we know more. There's mounting evidence that airborne
transmission indoors is a key -- perhaps the main -- pathway to SARS-COV-2 transmission. In
this post I want to look at why that's so, give examples, and suggest a simple heuristic to
stay safe. Material like this might also be used to inform public policy ( here ; here
) by reducing superspreader events in enclosed spaces like churches (airborne transmission via
singing), restaurants (loud talking, especially if room is noisy), bars (ditto), nursing homes
(shouting[1]), gyms (
grunting ), meat-packing plants ( shouting ), call centers (talking),
offices generally (air conditioning), and other hot spots, but working that polucy out is not
the object of this post ( see here for engineering controls for
airborne transmission , and here for covid-proofing
public spaces ).
Airborne Transmission of SARS-CoV-2 Indoors
This article from PNAS seems to be the index publication for airborne transmission. From "
The airborne
lifetime of small speech droplets and their potential importance in SARS-CoV-2 transmission
":
Speech droplets generated by asymptomatic carriers of severe acute respiratory syndrome
coronavirus 2 (SARS-CoV-2) are increasingly considered to be a likely mode of disease
transmission. Highly sensitive laser light scattering observations have revealed that loud
speech can emit thousands of oral fluid droplets per second. In a closed, stagnant air
environment, they disappear from the window of view with time constants in the range of 8 to
14 min, which corresponds to droplet nuclei of ca. 4 μm diameter, or 12- to 21-μm
droplets prior to dehydration. These observations confirm that there is a substantial
probability that normal speaking causes airborne virus transmission in confined
environments.
That experiment was done inside a box.
Vox translates to real world terms:
A crowded indoor place, then, with poor ventilation, filled with people talking, shouting,
or singing for hours on end will be the riskiest scenario. A sparsely populated indoor space
with open windows is less risky (but not completely safe). Running quickly past another
jogger outside is on the other end of the spectrum; minimal risk.
(In other words, the problem is not density or proximity; the problem is transmission of the
virus, through the air, by human vocalization[2] (of which coughing and sneezing are a small,
and symptomatic, subset.)
That would explain why masks have worked. (One could argue that masks need only be worn
indoors, but most people are constantly moving from the outdoors to the indoors and out again,
which would involved touching the mask constantly to remove and replace it; better to wear it
all the time. In any case, minimal risk, to others, is not no risk). From the South China
Morning Post, "Coronavirus: hamster research shows effectiveness of masks 'huge' in Covid-19
battle, Hong Kong scientists say":
Hong Kong scientists conducting research on hamsters have offered the first proof of what
many residents have believed all along – that wearing surgical masks can significantly
reduce the rate of airborne Covid-19 transmission.
The study, which the team called the first of its kind, found the rate of non-contact
transmission – in which the virus was transmitted via respiratory droplets or airborne
particles – dropped by as much as 75 per cent when masks were present.
(See also "
If 80% of Americans Wore Masks, COVID-19 Infections Would Plummet, New Study Says ," from
Vanity Fair.)
Examples of Airborne Transmission of SARS-CoV-2 Indoors
So far as I can tell, there are two main villains: Air conditioning, and vocalization:
Air conditioning . Here is the very first article I spotted on airborne transmission,
back on March 9, 2020. From the South China Morning Post, "
Coronavirus can travel twice as far as official 'safe distance' and stay in air for 30 minutes,
Chinese study finds "
A passenger, known as "A", boarded a fully booked long-distance coach and settled down on
the second row from the back.
The passenger already felt sick at that point but it was before China had declared the
coronavirus outbreak a national crisis, so "A" did not wear a mask, nor did most of the other
passengers or the driver on the 48-seat bus."It can be confirmed that in a closed environment
with air-conditioning, the transmission distance of the new coronavirus will exceed the
commonly recognised safe distance," the researchers wrote in a paper published in peer-review
journal Practical Preventive Medicine last Friday. They said the study proves the importance
of washing hands and wearing face masks in public places because the virus can linger in the
air attached to fine droplet particles.
Here is a seating chart of the bus:
After reading this, I altered my practice not to mask up, which I was already doing, but to
avoid (air-conditioned) public transportation entirely, and indeed air-conditioned spaces
entirely.
Here is a second example, a Chinese restaurant. From the CDC's Emerging Infectious Diseases,
" COVID-19
Outbreak Associated with Air Conditioning in Restaurant, Guangzhou, China, 2020 ":
We conclude that in this outbreak, droplet transmission was prompted by air-conditioned
ventilation. The key factor for infection was the direction of the airflow. Of note, patient
B3 was afebrile and 1% of the patients in this outbreak were asymptomatic, providing a
potential source of outbreaks among the public (7,8). To prevent spread of COVID-19 in
restaurants, we recommend strengthening temperature-monitoring surveillance, increasing the
distance between tables, and improving ventilation.
Here again is a seating chart:
I was already not going to restaurants because of the Chinese bus episode, if I had been, I
would have stopped. One can't wear a mask while eating!
Vocalization . We have several examples of vocalization (singing, shouting, talking,
grunting, etc.) causing transmission.
On March 29
, we had an event at the Skagit Valley Chorale's rehearsal in Mount Vernon, WA. Here is the
report, again from the CDC: " High SARS-CoV-2 Attack Rate Following
Exposure at a Choir Practice -- Skagit County, Washington, March 2020 ":
Following a 2.5-hour choir practice attended by 61 persons, including a symptomatic index
patient, 32 confirmed and 20 probable secondary COVID-19 cases occurred (attack rate = 53.3% to
86.7%); three patients were hospitalized, and two died. Transmission was likely facilitated by
close proximity (within 6 feet) during practice and augmented by the act of singing.
(Sadly, privacy concerns forbid a seat diagram.) I don't agree that proximity in and itself
transmits anything; it seems clear to me that singing was the issue (although transmission
through fomites was possible, as choir members put away chairs, etc.). Supporting evidence from
Missouri's Daily Journal, "
A surprising way you may risk getting Covid-19 ":
The possibility that singing might help transmit infectious diseases is not a new concept.
A 1968 article, "Singing and the Dissemination of Tuberculosis," described an elaborate box
that volunteers could talk, sing and cough into, allowing investigators to measure the
number, size and length of time airborne of individual infectious droplets they breathed out.
And a few TB outbreaks have featured singing, including one in a New Jersey church choir in
1995.
(This is good local journalism, too.) Science confirms, in "
Why do some COVID-19 patients infect many others, whereas most don't spread the virus at
all? ":
Some situations may be particularly risky. Meatpacking plants are likely vulnerable
because many people work closely together in spaces where low temperature helps the virus
survive. But it may also be relevant that they tend to be loud places, [Gwenan Knight of the
London School of Hygiene & Tropical Medicine] says. The report about the choir in
Washington made her realize that one thing links numerous clusters: They happened in places
where people shout or sing. And although Zumba classes have been connected to outbreaks,
Pilates classes, which are not as intense, have not, Knight notes. "Maybe slow, gentle
breathing is not a risk factor, but heavy, deep, or rapid breathing and shouting is."
We also have the following case in Chicago. From the CDC, " Community Transmission of SARS-CoV-2 at
Two Family Gatherings -- Chicago, Illinois, February–March 2020 ":
This report describes the cluster of 16 cases of confirmed or probable COVID-19, including
three deaths, likely resulting from transmission of SARS-CoV-2 at two family gatherings (a
funeral and a birthday party)
Here, instead of a seating diagram, we have a timeline:
I'm guessing "Happy Birthday" was sung at the birthday party, hence the greater number of
cases originating from it.
Here is the case of a South Korean call center. From the CDC, "Coronavirus Disease Outbreak
in Call Center, South Korea":
We described the epidemiologic characteristics of a COVID-19 outbreak centered in a call
center in South Korea. We identified 97 confirmed COVID-19 case-patients in building X,
indicating an attack rate of 8.5%. However, if we restrict our results the 11th floor, the
attack rate was as high as 43.5%. This outbreak shows alarmingly that severe acute
respiratory syndrome coronavirus 2 (SARS-CoV-2) can be exceptionally contagious in crowded
office settings such as a call center. The magnitude of the outbreak illustrates how a
high-density work environment can become a high-risk site for the spread of COVID-19 and
potentially a source of further transmission. Nearly all the case-patients were on one side
of the building on 11th floor. Severe acute respiratory syndrome coronavirus, the predecessor
of SARS-CoV-2, exhibited multiple superspreading events in 2002 and 2003, in which a few
persons infected others, resulting in many secondary cases. Despite considerable interaction
between workers on different floors of building X in the elevators and lobby, spread of
COVID-19 was limited almost exclusively to the 11th floor, which indicates that the duration
of interaction (or contact) was likely the main facilitator for further spreading of
SARS-CoV-2.
Here we do have a seating diagram:
It seems unlikely to me that air conditioning was the major factor, because otherwise --
HVAC mavens in the readership will correct me -- the cases would have been distributed
throughout the floor. However, what call center personnel do is talk , a lot. Hence I
would urge that vocalization is the driver, not mere proximity.
And finally, we have the case of a South Korean gym. From the CDC, " Cluster of Coronavirus Disease
Associated with Fitness Dance Classes, South Korea "
Characteristics that might have led to transmission from the instructors in Cheonan
include large class sizes, small spaces, and intensity of the workouts. The moist, warm
atmosphere in a sports facility coupled with turbulent air flow generated by intense physical
exercise can cause more dense transmission of isolated droplets (6,7). Classes from which
secondary COVID-19 cases were identified included 5–22 students in a room ≈60 m2
during 50 minutes of intense exercise. We did not identify cases among classes with <5
participants in the same space. Of note, instructor C taught Pilates and yoga for classes of
7–8 students in the same facility at the same time as instructor B (Figure; Appendix
Table 2), but none of her students tested positive for the virus. We hypothesize that the
lower intensity of Pilates and yoga did not cause the same transmission effects as those of
the more intense fitness dance classes.
Here is a really neat map of the cases ( full size version ):
We see that "high intensity" classes accounting for all the transmission; there was no
transmission from Yoga and Pilates classes. Here the vocalization would be heavy breathing,
huffing and puffing.
Heuristic of Avoid Transmission of SARS-CoV-2 Indoors
One salutary result of focusing on indoor transmission of SARS-CoV-2 is that we don't
have to get all het up [4] about photos like this anymore:
The foreground/background compressed photos of people enjoying outdoor spaces are
becoming an irresistible genre. This one from the Washington Post shows a few hundred
people in the space of a few hundred meters. In other words, reasonable numbers. The moral
panic will backfire. pic.twitter.com/MBBNNMVcXP
-- Pinboard (@Pinboard) May 25,
2020
Photographer's tricks aside, these people are outdoors; the risk is minimal (though I still
won't answer for, say, small groups of people sitting on a beach blanket, sharing beers and
singing old songs). I would avoid groups like this, but then I would anyway, virus or no
virus.
The Japanese seem to have had some success by focusing on indoor transmission as well,
following a rule called "The Three C's." Here is a poster:
Bloomberg explains, in "
Did Japan Just Beat the Virus Without Lockdowns or Mass Testing? ":
Experts are also credited with creating an easy-to-understand message of avoiding what are
called the "Three C's" -- closed spaces, crowded spaces and close-contact settings -- rather
than keeping away from others entirely.
"Social distancing may work, but it doesn't really help to continue normal social life,"
said Hokkaido University's Suzuki. "The 'Three C's' are a much more pragmatic approach and
very effective, while having a similar effect."
However, I think that knowing what we know now, we can add two more almost-C's to avoid: Air
C onditioning, and "Vo c alization (or perhaps C acophony?)
However, all in all, I think the best heuristic is offered by one Ángela Caída's
Twitter account:
This "Three C's environment is the same as a crowded, musty cave full of tightly packed,
chattering bats, which makes sense, because that's where the coronavirus evolved.
Caves are also cool, like air conditioned spaces, and while bats vocalize, I doubt they
transmit SARS-CoV-2 as well as we do[3].
So, to avoid SARS-CoV-2 airborne transmission, don't be like a bat! Avoid bat caves! Also,
learn sign language?
NOTES
[1] Thanks to the NC commentariat for
a really useful discussion on shouting in nursing homes.
[2] There is a big debate over whether
vocalization produces big and small droplets , or a continuum of droplets (with "aerosols"
at the small end) but I don't think that matters for the purposes pf this post.
[3] "Much of the cacophony in a bat cluster, the researchers suggest , is bats
voicing their annoyance with those in very close quarters around them." Bat vocalizations are "
ultrasonic ",
"repeated bursts of only a few hundred milliseconds." So making the assumption that
lower-pitched and longer human communication emits more virus, one might speculate that bats
would be less vulnerable to airborne transmission of #COVID-19 than humans.
[4] Terry Pratchett, The Truth :
"Mrs. Tilly, I think you wrote a lovely well-spelled and grammatical letter to us
suggesting that everyone under the age of eighteen should be flogged once a week to stop them
being so noisy?"
"Once a day, Mr de Worde," said Mrs. Tilly. "That'll teach 'em to go around being
young!"
gc54
May 25, 2020 at 6:21 pm
So, if you must stay in a hotel while driving interstate to avoid air travel:
– choose an older hotel with (noisy) under-window AC rather than the more efficient
but potentially deadly central HVAC in newer buildings?
– any other suggestions?
MLTPB
May 25, 2020 at 7:12 pm
Ask how much they charge for having your own (inside sanitized at home) tent on their
lawn.
WhoaMolly
May 25, 2020 at 9:47 pm
I'm depressed -- and vulnerable -- enough to seriously consider bringing along a
lightweight 2 person tent, and pop it up on top of the motel bed. Sleep, read, surf Internet
in the tent. Another option is sleeping in an RV a campground or a WLMart parking lot.
Age and health issues mean I need to start thinking this through or spend remaining years
at home.
Ugh.
Yves
Smith
May 25, 2020 at 10:39 pm
Air travel is not in the same category as riding on a bus. Airplanes have HEPA filters.
From an interview with an associate professor of aviation maintenance:
HEPA filters are a very high-intensity system of fibers that you essentially run air
through to filter out an incredible amount of contaminants -- not just dust, not just
bacteria, but moisture, any sort of contamination that could potentially harm or create an
atmosphere in the cabin or the cockpit that could harm the passengers or the crews. The
material in them is much closer together compared to cheaper air filters, and that makes it
very difficult for biological elements to penetrate them.
How common are HEPA filters?
I don't know of an airline that's operating right now that does not have HEPA-level
filters on them, but that does not mean that one does not exist. There's a certain amount
of air quality that you have to maintain in your commercial airplane. If you're flying
commercial passengers or corporate passengers, you're going to have a HEPA filter or better
air filtration system.
https://thepointsguy.com/news/airplane-air-hepa-filter/
So the risk in flying is not the air circulation. It is:
1. An unmasked person coughing, sneezing, or talking loudly, and you get their cooties
before the air gets sucked into the filtration system. Everyone on a plane is supposed to be
masked up but it's not easy to enforce, given that the airlines can't toss someone out at
39,000 feet.
2. Getting to the plane and your sear. Hard to imagine that people can stay 6 feet apart
when dealing with airline security and getting on board. Passengers are now required to be
masked up from TSA onward, so that can be enforced. Airport security can remove people.
3. Those bins at security! Filthy! Wear gloves for that part and remove/replace shortly
afterwards.
Huey Long
May 25, 2020 at 6:23 pm
HVAC maven here:
Lambert, it really depends on how the HVAC system is configured; different zones on a
particular floor may be served by different airhandlers.
Some buildings have large central A/C plants with massive airhandlers that serve the
entire building, especially in 1960's though mid 1970's vintage high-rise office towers.
Several of NYC's larger office REITs are considering installing UV equipment in the
airhandler fan chambers, but I haven't heard of any contracts being let just yet.
Cuibono
May 25, 2020 at 6:50 pm
As for the Japanese and avoiding cramped closed close contact spaces: i did not know they
had shutdown subways and trains
MLTPB
May 25, 2020 at 8:00 pm
Also places like karaoke bars were they closed in S Korea?
allan
May 25, 2020 at 6:58 pm
"Photographer's tricks aside, these people are outdoors; the risk is minimal ."
That might be true for for deep focus shots along seaside boardwalks,
It will be a very long time before my nuclear family unit ventures forth.
curlydan
May 25, 2020 at 10:02 pm
It seems like the trick might be to stay within your nuclear unit outdoors and not mix
with others. We'll need luck trying to teach that to pool bound Arkansas high schoolers (see
link below) or possibly Lake of the Ozarks revelers.
https://www.star-telegram.com/news/coronavirus/article242967096.html
I have been out mountain biking with my younger son lately. We feel pretty safe so far.
The nice thing about biking in a relatively secluded place is that we literally touch nothing
that isn't "ours". Our only debates are if we need to press a button to cross a street.
MLTPB
May 25, 2020 at 7:17 pm
Shutting down churches without shutting down trains (no HEPA filters there, presumably) if
their choral music is taped, not live performance, would seem selective, for those who do not
believe in livin on bread alone (thus spiritual nourishment is essential).
Biologist
May 25, 2020 at 7:52 pm
No quibbles with your conclusion re: airborne transmission, but the first study you cite
above ("How Covid19 spread through a Hunan bus") was retracted:
https://retractionwatch.com/2020/04/22/study-claiming-broader-spread-of-aerosolized-coronavirus-is-retracted/ http://c61.cnki.net/cjfd/Withdraw/SYYY/SYYY20200304003.pdf
rd
May 25, 2020 at 8:12 pm
One of my basic rules of thumb is to only go into buildings with very high ceilings
(typical big box store) and low density of people. There is lots of air available then for
recriculation and you should be able to avoid the virus if you generally stay away from
people. I avoid all conversation with people.
By definition, this is generally not going to be a restaurant or bar, so they are out for
the foreseeable future.
The Rev Kev
May 25, 2020 at 9:01 pm
I like the way that this article brings together so many threads and articles over the
past few months into a handy page. It looks much better when you see it all on one page and
start to make your own conclusions. Of course some of the conclusions suck as in no public
transport, no restaurants, no gyms, etc. Of course some people will not take note-
https://www.youtube.com/watch?v=OFl_KQGyyC4
When talking about church transmission I thought about something from history. About two
centuries ago many Scots followed religions that were not exactly in line with the British
Army's professed Church of England. So to avoid getting caught at their own lay services,
they would head off to a field or hill and post guards at each corner to give warning of
spies and proceed in their services.
So yes, a lot of these churches could have their services in fields while the local
sky-pilot could use a megaphone to give the service. They just need to space themselves out a
bit. More to the point, some groups forget that their people are the church and not
just the buildings that they happen to use. We have even seen services conducted over the net
or in drive-in like services. I think that, for example, those people in that Mississippi
church that had their church burnt down may have forgotten that fact.
Jackson
May 25, 2020 at 11:16 pm
No. They are waiting for the Rapture..From a NC Contributor Tom Stone, "I have no problem
with individual Christians rushing to their Heavenly Rewards, it's when they take others with
them without their consent that I see an issue.."
The Rev Kev
May 25, 2020 at 11:26 pm
In my comment I see that I neglected to say that it was not Scottish people that were
going off to fields and hills to have their lay services but Scottish Regiments .
Outdoor maskism has zero to do with science, everything to do with irrational panic at best,
and most of all top-down totalitarian control-seeking
Living in the Empire isn't quite as bad as being a victim of the Empire, but it's getting
close.
Russ
66
v> Thus in this case the propaganda has been largely monolithic:
1. Stay indoors. Don't breathe the air.
2. If you must venture into the hostile outdoors*, wear a mask**. Especially now that the
air is the cleanest it's been our whole live s, do all you can to avoid breathing it.
"Covid-19 has forced modern medicine to broaden its outlook and look for new solutions,
even in the wisdom of the past."
Indeed, it's clear where the establishment's propaganda has found wisdom.
Thus in this case the propaganda has been largely monolithic:
1. Stay indoors. Don't breathe the air.
2. If you must venture into the hostile outdoors*, wear a mask**. Especially now that
the air is the cleanest it's been our whole live s, do all you can to avoid breathing
it.
"Covid-19 has forced modern medicine to broaden its outlook and look for new solutions,
even in the wisdom of the past."
Indeed, it's clear where the establishment's propaganda has found wisdom. /div
Highly recommended !So not only ambulance service was destroyed by private equity, they now added other specialties. I wonder is those criminals who
insert unnecessary stents in patients are connected to private equity.
Images removed
Notable quotes:
"... "You can't serve two masters. You can't serve patients and investors" ..."
"... Morganroth's defense of pandemic Botox might seem odd, but it made perfect sense within the logic of the U.S. health-care system, which has seen Wall Street investors invade its every corner, engineering medical practices and hospitals to maximize profits as if they were little different from grocery stores. At the center of this story are private equity firms, which saw the explosive growth of health-care spending and have been buying up physician staffing companies, surgery centers, and everything else in sight. ..."
"... But some doctors say that the private equity playbook, which involves buying companies, drastically cutting costs, and then selling for a profit -- the goal is generally to make an annualized return of 20% to 30% within three to five years -- creates problems that are unique to health care. "I know private equity does this in other industries, but in medicine you're dealing with people's health and their lives," says Michael Rains, a doctor who worked at U.S. Dermatology Partners , a big private equity-backed chain. "You can't serve two masters. You can't serve patients and investors." ..."
"... Yet over the past decade, lawyers devised a structure that allows investors to buy a medical practice without technically owning it: the MSO, or management service organization. Today, when an investment firm buys a doctor's office, what it's actually buying are the office's "nonclinical" assets. In theory, physicians control all medical decisions and agree to pay a management fee to a newly created company, which handles administrative tasks such as billing and marketing. ..."
"... Businessweek ..."
"... When individual doctors sell, they generally receive $2 million to $7 million each, with 30% to 40% of that paid in equity in the group. After the acquisition, doctors get a lower salary and are asked to help recruit other doctors to sell their practices or to join as employees. ..."
"... Patients, for the most part, are in the dark. Unlike when your mortgage changes hands, you usually aren't notified when a big investment firm buys your doctor. Sometimes the sign on the door bearing the physician's name stays put, and subtle changes in operations or unfamiliar fees may be the only clues that anything has happened. ..."
"... At Advanced Dermatology & Cosmetic Surgery , the largest private equity-backed group in the field, with more than 150 locations across the U.S., that sense of discomfort came shortly after Audax Group bought a controlling stake in what was then a much smaller chain in 2011. The new management team introduced a scorecard that rewarded offices with cash if they met daily and monthly financial goals, according to a lawsuit filed in 2013 against the company by one of its dermatologists. The doctor alleged that the bonus program encouraged staff to do as many procedures as possible, rather than strictly addressing patients' medical needs. ..."
"... Most dermatologists use outside labs and pathologists, but private equity-owned groups buy up existing labs and hire their own pathologists. Then doctors are encouraged to refer patients within the group and send biopsy slides to the company-owned labs, keeping the entire chain of revenue in-house. ..."
"... Now comes the cost-cutting. This is supposed to be the hallmark of private equity, and, done right, it can work to the benefit of doctors and patients. But there are pitfalls unique to medicine, where aggressive cuts can lead to problems, some of them merely inconvenient and some potentially dangerous. ..."
"... A doctor at Advanced Dermatology says that waiting for corporate approvals means his office is routinely left without enough gauze, antiseptic solution, and toilet paper. Even before the great toilet paper shortage of 2020, he would travel with a few rolls in the trunk of his car, to spare patients when an office inevitably ran out. The company declined to comment. ..."
"... One paradox of the Covid-19 pandemic has been that even as the virus has focused the entire country on health care, it's been a financial disaster for the industry. And so, while emergency room doctors and nurses care for the sick -- comforting those who would otherwise die alone, and in some cases dying themselves -- private equity-backed staffing companies and hospitals have been cutting pay for ER doctors. These hospitals, like the big medical practices, make a large portion of their money from elective procedures and have been forced into wrenching compromises. ..."
"... For investors with capital, on the other hand, the economic fallout from the virus is a huge opportunity. Stay-at-home orders have left small practices more financially strained than they've ever been. That will likely accelerate sales to private equity firms, according to Marc Cabrera, an investment banker focused on health-care deals at Oppenheimer & Co. Independent doctors or groups that previously rebuffed offers from deep-pocketed backers "will reconsider their options," he says. ..."
"... Many doctors may ultimately come to regret cashing out, but it's hard to get out once you're in. As part of an acquisition, the private equity groups typically require doctors to sign yearslong contracts, with noncompete clauses that prevent them from working in the surrounding area. ..."
Not long after Gavin Newsom, the governor of California, ordered the state's 40 million residents to stay home to stop the spread
of the new coronavirus, Dr. Greg Morganroth called his team of doctors and said their dermatology group was staying open.
Morganroth is chief executive officer of the California Skin Institute
, which he founded in 2007 as a single office in Mountain View. He's since expanded to more than 40 locations using a financing
strategy that's become exceedingly common in American health care: private equity. In this case, he took out a loan from
Goldman Sachs Group Inc. that could eventually convert to an
equity stake. CSI is now the largest dermatology chain in California.
But the Covid-19 pandemic
put Morganroth in a precarious position. Most medical procedures were characterized as
nonessential by government officials and practitioners. Doctors were closing offices, and patients were staying away to limit
their potential exposure to the virus.
CSI took a different approach. Morganroth explained his thinking on April 2 in a Zoom call with more than 170 dermatologists from
around the country organized by the Cosmetic Surgery Forum, an industry conference. Contrary to what they might have heard, Morganroth
told them, they should consider staying open during the pandemic. "Many of us are over-interpreting guidelines," he said.
For a moment there was an awkward silence. Doctors had thought they were signing up for advice on how to apply for
government money that would help them meet payroll while they were shut down; they hadn't expected to be told not to shut down
at all. Morganroth continued: "We are going to be in a two-year war, and we need to make strategic plans for our businesses that
enable us to survive and to rebound."
Back at CSI, the company's front-office staff was working the phones, calling patients in some of the worst-hit areas and reminding
them to show up for their appointments, even for cosmetic procedures such as Botox injections to treat wrinkles. During the videoconference,
Morganroth argued that offering Botox in a pandemic wasn't so different from a grocery store allowing customers to buy candy alongside
staples.
"If I had a food supply company and had to stay open, and I had meat, bread, and milk, would I stop making lime and strawberry
licorice?" Morganroth asked. "I would make everything and go forward."
From a public-health point of view, some of the doctors believed, this was questionable. Common reasons for visiting a dermatologist's
office -- skin screenings, mole removals, acne consultations -- aren't particularly time sensitive. Serious matters, such as suspected
cancers and dangerous rashes, can be handled, at least initially, with
telemedicine consultations . Then doctors can weigh the risks for their patients and determine who needs to come in. In a statement,
CSI says that it followed local and state laws for staying open, while providing "necessary care" for patients, and that it had not
required doctors to come to work.
"You can't serve two masters. You can't serve patients and investors"
Morganroth's defense of pandemic Botox might seem odd, but it made perfect sense within the logic of the U.S. health-care system,
which has seen Wall Street investors invade its every corner, engineering medical practices and hospitals to maximize profits as
if they were little different from grocery stores. At the center of this story are private equity firms, which saw the explosive
growth of health-care spending and have been buying up physician staffing companies, surgery centers, and everything else in sight.
Over the past five years, the firms have invested more than $10 billion in medical practices, with a special focus on dermatology,
which is seen as a hot industry because of the aging population. Baby boomers suffer from high rates of two potentially lucrative
conditions: skin cancer and vanity. Some estimates suggest that private equity already owns more than 10% of the U.S dermatology
market. And firms have started to expand into other specialties, including women's health, urology, and gastroenterology.
There's nothing inherently wrong with any of this. But some doctors say that the private equity playbook, which involves
buying companies, drastically cutting costs, and then selling for a profit -- the goal is generally to make an annualized return
of 20% to 30% within three to five years -- creates problems that are unique to health care. "I know private equity does this in
other industries, but in medicine you're dealing with people's health and their lives," says Michael Rains, a doctor who worked
at
U.S. Dermatology Partners , a big private equity-backed
chain. "You can't serve two masters. You can't serve patients and investors."
Investment firms, and the practices they fund, say these concerns are overblown. They point out that they're giving doctors a
financial shelter from the rapidly changing medical environment, a particularly attractive prospect now, and that money from private
equity firms has expanded care to more patients. But they've also made it next to impossible to track the industry's impact or reach.
Firms rarely announce their investments and routinely subject doctors to nondisclosure agreements that make it difficult for them
to speak publicly. Bloomberg Businessweek spoke to dozens of doctors at 10 large private equity-backed dermatology groups.
Those interviews, along with information obtained from other employees, investors, lawyers, court filings, and company records, reveal
how the firms operate, and why they sometimes fail patients.
The process is never exactly the same, but there are familiar patterns, which tend to play out in five steps.
Step 1: Marriage
The strange thing about private equity money in medicine is that for-profit investors have long been prevented from buying doctor's
offices. Corporate ownership goes against a doctrine set by the American Medical
Association , the main trade group for doctors in the U.S., and is prohibited by law in many states, including Texas and New
Jersey. For most of the past 100 years, if you wanted to make money on a medical practice, you needed to have a medical license.
Yet over the past decade, lawyers devised a structure that allows investors to buy a medical practice without technically owning
it: the MSO, or management service organization. Today, when an investment firm buys a doctor's office, what it's actually buying
are the office's "nonclinical" assets. In theory, physicians control all medical decisions and agree to pay a management fee to a
newly created company, which handles administrative tasks such as billing and marketing.
In practice, though, investors expect some influence over medical decision-making, which, after all, is connected to profits.
"When we partner with you, it's a marriage," said Matt Jameson, a managing director at BlueMountain Capital, a $17 billion firm that
recently invested in a women's health company, while speaking at a conference in New York in September. "We have to believe it. You
have to believe it. It's not going to be something where clinical is completely not touched." (When contacted by Businessweek
, Jameson asked to clarify his comments. "Doctors and other qualified healthcare professionals at the providers we've invested
in make medical decisions," he said in a statement.)
The typical buyout starts with the acquisition of a big, popular practice, often with multiple doctors and several locations,
for as much as $100 million. (Investors typically pay between 9 and 12 times annual profit.) This practice functions as an anchor,
like a name-brand department store at a shopping mall, attracting patients and doctors to the new group as it expands. Then comes
the roll-up: The private equity firm purchases smaller offices and solo practices, giving the group a regional presence.
As part of the new structure, investors deal with paperwork and save money by buying medical supplies in bulk. Crucially they
also negotiate higher insurance reimbursement rates. One dermatologist who sold her practice to the California Skin Institute says
she was surprised to find out the bigger group's payouts from insurers were $25 to $125 more per visit.
When individual doctors sell, they generally receive $2 million to $7 million each, with 30% to 40% of that paid in equity in
the group. After the acquisition, doctors get a lower salary and are asked to help recruit other doctors to sell their practices
or to join as employees.
At first, doctors are generally thrilled by all of this. They have financial security and can focus on treating patients without
the stress of running a business. Patients, for the most part, are in the dark. Unlike when your mortgage changes hands, you usually
aren't notified when a big investment firm buys your doctor. Sometimes the sign on the door bearing the physician's name stays put,
and subtle changes in operations or unfamiliar fees may be the only clues that anything has happened.
Step 2: Growth
The promise of more patients is a big draw for doctors. By sharing marketing costs and adding locations, the new companies can
advertise more and attract customers. Private equity-owned practices have been diligent users of social media, announcing newly added
doctors and posting coupons on Twitter and Instagram. But these practices can be aggressive in ways that make some doctors uncomfortable.
At Advanced Dermatology & Cosmetic Surgery , the largest
private equity-backed group in the field, with more than 150 locations across the U.S., that sense of discomfort came shortly after
Audax Group bought a controlling stake in what was then a
much smaller chain in 2011. The new management team introduced a scorecard that rewarded offices with cash if they met daily and
monthly financial goals, according to a lawsuit filed in 2013 against the company by one of its dermatologists. The doctor alleged
that the bonus program encouraged staff to do as many procedures as possible, rather than strictly addressing patients' medical needs.
In some of the company's Florida offices, the doctor alleged, medical assistants responded to the bonus structure by ticking extra
boxes on exam reports, stating that doctors checked many more areas of the body than they actually had. That led to higher patient
bills, defrauding the government under its Medicare program, according to the lawsuit. The federal government declined to join the
case, and it was dismissed about a year after it was filed. Advanced and Audax declined to comment.
One-Stop Skin Care
By buying up labs and adding specialists, private equity-owned dermatology groups get paid at every step of a patient's treatment.
Data: Estimated Medicare reimbursement rates for the Miami area, Sensus Healthcare sales presentation
Private equity-backed practices also try to increase revenue by adding more-lucrative procedures, according to doctors interviewed
by Businessweek . In dermatology, this means more cosmetics, laser treatments, radiation, and especially Mohs surgeries
-- a specialized skin cancer procedure that removes growths from delicate areas like the face and neck one layer at a time, to limit
scarring. The surgery involves expensive equipment and specialized doctors, so some large medical groups keep costs down by assembling
traveling Mohs teams, who fly in from other states. Others create mobile labs in vans that set up in clinics' parking lots.
Most dermatologists use outside labs and pathologists, but private equity-owned groups buy up existing labs and hire their own
pathologists. Then doctors are encouraged to refer patients within the group and send biopsy slides to the company-owned labs, keeping
the entire chain of revenue in-house. This takes advantage of a regulatory quirk that has made dermatology, and a handful of other
specialties, attractive to private equity. Under the 1989 Stark Law, doctors aren't allowed to make patient referrals for their own
financial gain. An exception was made for some fields because it's more convenient for patients, explains Dr. Sailesh Konda, a Mohs
surgeon and professor at the University of Florida. "But that can be abused."
Step 3: Synergy
Now comes the cost-cutting. This is supposed to be the hallmark of private equity, and, done right, it can work to the benefit
of doctors and patients. But there are pitfalls unique to medicine, where aggressive cuts can lead to problems, some of them merely
inconvenient and some potentially dangerous.
A doctor at Advanced Dermatology says that waiting for corporate approvals means his office is routinely left without enough gauze,
antiseptic solution, and toilet paper. Even before the great
toilet paper shortage of 2020, he would travel with a few rolls in the trunk of his car, to spare patients when an office inevitably
ran out. The company declined to comment.
At the country's second-biggest skin-care group, U.S. Dermatology
Partners , a former doctor says a regional manager switched to a cheaper brand of needles and sutures without consulting the
medical staff. The quality was so poor, she says, they would often break off in her patients' bodies. Mortified, she'd have to dig
them out and start over. She complained to managers but couldn't get better supplies, she says. Paul Singh, U.S. Dermatology's CEO,
says the company uses a "reputable, global vendor for medical supplies." "While our group may have standardized purchasing processes,
individual providers have the autonomy to procure specific supplies that they need for a particular patient situation or patient
population," he says in a statement.
Doctors who join a private equity-backed group generally sign contracts that state they'll never have to compromise their medical
judgment, but some say that management began to intervene there, too. Dermatologists at most of the companies say they were pushed
to see as many as twice the number of patients a day, which made them feel rushed and unable to provide the same quality of care.
Others were forced to discuss their cases with managers or medical directors, who asked the doctors to explain why they weren't sending
more patients for surgery. Multiple practices also encouraged doctors to send home Mohs surgery patients with open wounds and have
them come back the next day for stitches -- or to have a different doctor do the closure the same day -- because that would allow
the practice to collect more from insurers.
That's if doctors are performing the procedures at all. At Advanced Dermatology, several doctors say they were asked to claim
that physician assistants, or PAs, were under their supervision when they weren't seeing patients in the same building, or even the
same town. Because PAs are paid less than dermatologists, this allowed the company to keep costs low while growing the business.
In a statement, Eric Hunt, Advanced's general counsel and chief compliance officer says that having PAs on staff enables the company
to "provide access to quality dermatological care to more patients."
Step 4. Rolling Up the Roll-Up
Advanced Dermatology was sold in 2016 by Audax to Harvest
Partners LP , following a pattern that's typical in the industry. At some point, after costs have been cut and profits maximized,
most private equity-owned medical groups will be sold, often to another private equity firm, which will then try to somehow make
the company even more profitable.
Having reduced most of the obvious costs, Advanced Dermatology began skimping on more important supplies, including Hylenex, according
to doctors and other employees. The drug is an expensive reversal agent used when cosmetic fillers, which are supposed to make skin
look plumper, go wrong. Not having enough is dangerous: Patients who get an injection that inadvertently blocks a blood vessel can
be left with dead sections of skin or even go blind if they don't get enough Hylenex in a matter of hours. The company says that
it stocks Hylenex in every office that performs cosmetic procedures, and that it "has no records of any provider being denied an
order for this medication."
Advanced Dermatology also started giving even more authority to PAs, according to doctors and staff. Without enough oversight
some were missing deadly skin cancers, they say. Others were doing too many biopsies and cutting out much larger areas of skin than
necessary, leaving patients with big scars. Doctors who complained about the bad behavior say they saw PAs moved to other locations
rather than fired or given more supervision. Hunt, the company's lawyer, says that all PAs get six months of training and are supervised
by experienced doctors.
The staff coined a new medical diagnosis, "pre- pre- pre-cancer"
Advanced Dermatology also put more pressure on doctors to send biopsies to in-house labs. The move made sense financially, but
some of the doctors didn't trust the lab. One of its two pathologists in Delray Beach, Fla., Steven Glanz, had a history of misdiagnosing
benign tumors, which led patients to undergo surgeries that were later found to be unnecessary, according to doctors who worked with
him. Dermatologists who warned that Glanz was a danger to patients say that their complaints to Dr. Matt Leavitt, the group's founder
and CEO, were ignored. More procedures, doctors knew, brought in more money.
Glanz, who had been with the practice since its early days, was known to read slides under a microscope with a pistol on his desk.
After he was arrested with a handgun, a folding knife, and a vial of methamphetamine crystals, he was fired and Florida's state medical
board fined him $10,000, requiring him to complete a five-hour course on ethics before he could resume practicing. But his former
colleagues were unsettled; they knew Glanz's signature was on years of reports that determined treatment for patients. Some slides
were reevaluated, and pathologists noticed mistakes. Managers told some doctors and their staff that patients, even those who'd been
misdiagnosed and had unnecessary procedures, were not to be told. Glanz pleaded guilty to stalking and a firearms violation and was
sentenced to probation. When a reporter called his office and identified herself, the receptionist hung up. Further attempts to reach
Glanz were unsuccessful. Advanced's Hunt says that he was "formally released from employment three years ago," but did not comment
further.
Of course, some doctors pushed ethical boundaries long before private equity came into the picture. But critics of the industry,
including doctors and investors, say management teams put in place by private equity firms tend to look the other way as long as
a medical practice is profitable. Of the dermatologists with the highest biopsy rates in the country (between 4 and 11 per patient,
per year), almost 25% were affiliated with private equity-backed groups, according to Dr. Joseph Francis, a Mohs surgeon and data
researcher at the University of Florida.
Medical providers may have also been blurring ethical lines at U.S. Dermatology Partners, which was until recently on its second
private equity owner, Abry Partners LLC . At four of the
company's offices in Texas, a doctor and his PAs were doing more biopsies than necessary, according to employees. These employees
say the staff routinely called patients with benign lichenoid keratosis, small brownish blotches that usually go away on their own,
and told them the growths should be removed. Under instruction from the doctor, the staff coined a new medical diagnosis, "pre- pre-
pre-cancer," and then talked patients into coming in for removal, employees say. Singh, the U.S. Dermatology CEO, says that the company
trusts doctors to make the right decisions and that it monitors them through routine audits.
Step 5: Sell-Off
In some cases the cost-cutting either becomes impossible or leads to compromises in care too obvious to ignore. In 2016 a
DermOne LLC office in Irving, Texas, had been using a faulty
autoclave machine to sterilize surgical equipment -- the state and county health departments identified 137 patients that needed
to get tested for blood-borne diseases such as HIV and hepatitis. By 2018, DermOne's backer, Westwind Investors, wanted out.
Westwind had been one of the earliest firms to build a big dermatology business -- with practices in five states -- but others
had grown larger. After the debacle in Irving, the Nevada-based firm sold DermOne's medical records and patient lists, as well as
some of its offices, to other groups. It dissolved the remaining offices, leaving some patients abruptly without care. Westwind did
not respond to repeated requests for comment. Two other private equity-backed groups, TruDerm and Select Dermatology LLC, have also
gone out of business in the past two years.
The surviving chains have been saddled with large piles of debt they're now struggling to repay. In January, U.S. Dermatology
Partners defaulted on a $377 million loan, meaning the private equity backer, Abry Partners, had to hand over the keys to its lenders,
Golub Capital ,
Carlyle Group , and
Ares Management , which will now oversee a chain with almost
100 locations, receiving 1 million visits from patients a year. Abry did not respond to requests for comment .
For the medical groups that make it, the game plan is to eventually sell to the largest players, such as
KKR ,
Blackstone Group , and
Apollo Global Management . Pioneering investors, including Audax,
are now buying practices in other fields -- a concerning development to critics who note that the areas that are currently attracting
investment, such as urology, generally involve more invasive procedures. Should doctors performing vasectomies be thinking about
the dollar-rate returns for KKR -- or any private investor?
"It's ultimately going to backfire," says Dr. Jane Grant-Kels, a veteran dermatologist and professor at the University of Connecticut
School of Medicine. "There's a limit to how much money you can make when you're sticking knives into human skin for profit."
One paradox of the Covid-19 pandemic has been that even as the virus has focused the entire country on health care, it's been
a financial disaster for the industry. And so, while emergency room doctors and nurses care for the sick -- comforting those who
would otherwise die alone, and in some cases
dying themselves
-- private equity-backed staffing companies and hospitals have been
cutting pay for ER doctors. These hospitals, like the big medical practices, make a large portion of their money from elective
procedures and have been forced into wrenching compromises.
For investors with capital, on the other hand, the economic fallout from the virus is a huge opportunity. Stay-at-home orders
have left small practices more financially strained than they've ever been. That will likely accelerate sales to private equity firms,
according to Marc Cabrera, an investment banker focused on health-care deals at Oppenheimer & Co. Independent doctors or groups that
previously rebuffed offers from deep-pocketed backers "will reconsider their options," he says.
Many doctors may ultimately come to regret cashing out, but it's hard to get out once you're in. As part of an acquisition, the
private equity groups typically require doctors to sign yearslong contracts, with noncompete clauses that prevent them from working
in the surrounding area.
As governors throughout the nation ease restrictions on businesses, Advanced Dermatology is opening its most profitable offices
first. The company received an undisclosed sum under the Cares Act, as part of the government relief package intended for health-care
workers. Hunt, Advanced's chief compliance officer, told employees in an email earlier this month that the money would be used for
protective gear, such as masks, and to replace "millions of dollars" in lost revenue.
The group had closed most of its offices since the stay-at-home orders were issued in March, cutting pay for doctors and furloughing
staff. With cities and states beginning to consider reopening, doctors and PAs say they've been told they should be prepared for
a full schedule. Hunt says the company is following the appropriate safety measures, but employees fear it will be nearly impossible
to keep patients apart in waiting rooms. Opening in a reduced capacity, they understand, is not an option.
Read more: Private Equity Ate Finance, and Now It's Taking Over the World
The more you know? Over a third of Americans apprehensive about Covid-19
vaccine, citing rushed development & trust issues
21 May, 2020 21:37
Get short URL
As the Trump administration pushes for Covid-19 vaccine development on an ever-shrinking timetable and
companies report lackluster early trials, 35 percent of Americans are less than thrilled about getting
the shot.
Operation Warp Speed, the Trump administration's unprecedented drive to create and roll out a vaccine
for the coronavirus pandemic by the end of the year, may be doing more harm than good, at least where
Americans' trust is concerned. Between the shockingly abbreviated timetable and the lack of long-term
safety testing, almost one in four Americans (24 percent) said they were not interested in the shot,
according to a Reuters poll published Thursday. An additional 11 percent were unsure about it.
Also on rt.com
Study
Trump cited in his latest attack on WHO does NOT EXIST, says editor-in-chief of prestigious medical
journal
Compounding the distrust is the polarizing figure of President Donald Trump himself, who proudly
announced the shortened timetable for vaccine development last week. Thirty-six percent of those
polled by Reuters said they would be less likely to take a potential Covid-19 vaccine if it came
recommended by Trump, while just 14 percent thought the president's seal of approval was a positive.
Trump's narrative flip-flops haven't helped his credibility on the vaccine front. From his early
reassurances that the virus would vanish in weeks, to his public conflicts with his own health
advisers over locking down and reopening the country, it's not hard to see why Americans are hesitant
to fall in line behind him on this. But the problem isn't necessarily political. Nearly half of those
uninterested in taking the vaccine said the speed of its development worried them, while over 40
percent said the vaccine would be riskier than actually contracting Covid-19 itself.
Read more
However, even 29 percent of those who said they were "
not very interested
" in the
vaccine allowed they'd be willing to change their mind if the shot was approved by the Food and Drug
Administration. The full approval process for vaccines usually takes over a decade, and even the most
optimistic experts � including Dr. Anthony Fauci, who has become the public face of the US' Covid-19
policy � believe a shot won't be ready for another year to 18 months. Rushing a vaccine to market in
the middle of a pandemic means sacrificing comprehensive safety checks for efficiency � a tradeoff
that can be disastrous, as in the case of the 2009 swine flu shot Pandemrix, which caused permanent
brain damage in over 1,000 British patients.
The parallels between Covid-19 and that epidemic are ominous � wildly inflated death predictions
had spooked the UK government into approving Pandemrix without sufficient safety data � and it surely
won't help Americans' trust in this vaccine that Trump's "
vaccine czar
" Moncef Slaoui ran
GlaxoSmithKline's vaccine division during the swine flu debacle. Nor has it been especially heartening
to discover Slaoui's extensive investments in not just Glaxo but many other drug companies working on
potential vaccines.
Slaoui earned $3 million on Monday alone from Moderna, which is still considered the leading
candidate in the vaccine race, even though the drug company has never brought a vaccine to market.
After hyping up what were essentially meaningless preliminary results, Moderna's stock shot up 25
percent, bringing his holdings to over $10 million. He pledged to donate those earnings to "
cancer
research
" after demands for him to divest reached a fever pitch. A vaccine produced at Oxford
University hasn't fared much better, with all six rhesus monkeys who received the shot becoming
infected anyway � despite a preliminary report that tried to spin the failure as representing "
some
"
success.
Also on rt.com
Define
'distribute'! Trump mobilizing MILITARY to deliver Covid-19 vaccine 'assuming we get it,' sparks
conspiracy frenzy
Threats of mandatory vaccination have unsurprisingly not helped to soothe Americans' worries over a
potentially unsafe vaccine. Fauci and other health officials have repeatedly warned the public that
there will be no return to "
normal
" without a vaccine, even as lockdown restrictions are
slowly lifted � a statement some have interpreted as a threat that the unvaccinated will be barred
from crowded public places or travel. Harvard Law Professor Alan Dershowitz went further, declaring
the government has "
police power
" to mandate Americans take a vaccine and claiming such power
is "
not debatable
" constitutionally. And other experts downplayed the very real concerns
voiced by poll respondents in favor of blaming the "
very aggressive anti-vaccine movement
."
All this is bad news for the health experts Reuters cites, who say 70 percent of Americans would
have to be immune in order to achieve "
herd immunity
" and stop the virus from spreading
through the US, where upwards of 90,000 people have died since the pandemic began.
A top US scientist has said that people should not count on a Covid-19 vaccine being
developed any time soon...
William Haseltine, the groundbreaking cancer, HIV/AIDS and human genome projects
researcher, has said the best approach to the pandemic is to manage the
disease through careful tracing of infections and strict isolation measures whenever it
starts spreading. He said that while a vaccine could be developed, "I wouldn't count on it",
and urged people to wear masks, wash hands, clean surfaces and keep a distance.
If Nigerian hackers can steal that much money, Israel, Chinese, and Russian, intel agencies
probably are in the most Fed information systems doing what they want ;-)
Notable quotes:
"... officials in Washington State may have lost "hundreds of millions of dollars" to fraudsters filing bogus unemployment claim ..."
officials
in Washington State may have lost "hundreds of millions of dollars" to fraudsters filing bogus
unemployment claim s – all the way from Nigeria.
Yes, gunshot wounds are clearly the ffect of the new coronavirus.
Health officials in Washington state said they are reassessing their Covid-19 fatality data,
warning of underreported deaths.
Even after noting that five people who died of gunshot wounds were inexplicably included in
the figures.
Notable quotes:
"... According to the Mayo Clinic, a normal pulse oximeter oxygen level reading is between 95% and 100% , and anything less than 90% is considered dangerously low, or hypoxic. Some doctors have reported COVID-19 patients entering the hospital with oxygen levels at 50% or below . ..."
Some doctors are recommending these small, inexpensive devices to help monitor
symptoms.
A pulse oximeter attaches to a finger and uses light to detect the level of oxygen in your blood.
As
coronavirus
testing efforts
continue to ramp up and
face masks
are now a part of everyday life, a small diagnostic tool that clips to the tip of your
finger is fast becoming a must-have gadget in the
fight
against the coronavirus
. It's called a pulse oximeter, and it painlessly checks your blood oxygen
level, which can be affected by lung diseases such as COVID-19.
The device was already starting to surge in popularity as word got around
that people with the
coronavirus
frequently
arrive
at the hospital with abnormally low oxygen levels
. After an
op-ed
piece in The New York Times
recommended the use of pulse oximeters to detect a frightening
condition called "silent hypoxia," sales of the devices
skyrocketed
.
Many models are sold out or on lengthy backorder online. Same with brick-and-mortar drug stores,
supermarkets and box stores.
But questions and controversy surround the at-home use of pulse oximeters. It's not entirely clear
if pulse oximeters can help detect a coronavirus infection or whether their widespread use can help
curb
the spread of COVID-19
.
Whether you already have a pulse oximeter or you're thinking about buying one, here's what you need
to know about what they do, how they work, what the results mean and how accurate they might be.
A pulse oximeter is a small medical device that measures heart rate and blood oxygen saturation.
It's usually clipped to your finger, but it can also attach to your ear, nose, toe or forehead. Some
are battery powered and provide real-time results on a small LED display on the device itself. Others
connect with a wire to a separate vital sign monitor that records even more precise information about
your heart rhythm, body temperature and blood pressure using other sensors connected to your body.
How pulse oximeters measure heart rate and oxygen
A pulse oximeter measures your blood oxygen saturation and heart rate by shining a light through
your skin and detecting both the color and movement of your blood cells. Oxygenated blood cells are
bright red, deoxygenated cells are dark red.
The pulse oximeter compares the number of bright red cells to dark red cells to calculate your
oxygen saturation as a percentage. So, for example, a reading of 99% means only 1% of the blood cells
in your bloodstream have been depleted of oxygen.
Every time your heart beats, it pushes your blood through your body in a quick pulse (which is why
"pulse" is another word for "heart rate"). A pulse oximeter, using light, detects this movement and
calculates your heart rate in beats per minute, or BPM.
Coronavirus in pictures: Scenes from around the world
See all photos
+55
More
What's a healthy oxygen level and heart rate?
According to the Mayo Clinic, a normal pulse oximeter oxygen level reading is between
95%
and 100%
, and anything less than 90% is considered dangerously low, or hypoxic. Some doctors have
reported COVID-19 patients entering the hospital with
oxygen
levels at 50% or below
.
A normal resting heart rate is between 60 and 100 BPM. Typically, lower is better, as a slower
heart rate is usually an indication of a strong cardiovascular system.
A new study from Los
Alamos National Laboratory has revealed a new, now-dominant strain of the coronavirus which
appears to be more contagious , according to the authors. Meanwhile, doctors in the United
States are wondering if the harder-hit East Coast is being hit with a different version of the
virus than the West Coast.
Emerging in early February, the new strain migrated from Europe to the East Coast of the
United States, where it became the dominant strain across the world beginning in mid-March.
Wherever the new strain has appeared, it's quickly infected far more people than earlier
strains which emerged from Wuhan, China. Within weeks it became the most prevalent strain in
some nations.
... ... ...
Emerging in early February, the new strain migrated from Europe to the East
Coast of the United States, where it became the dominant strain across the world beginning in
mid-March. Wherever the new strain has appeared, it's quickly infected far more people than
earlier strains which emerged from Wuhan, China. Within weeks it became the most prevalent
strain in some nations.
In addition to spreading faster, it may make people vulnerable to a second infection after
a first bout with the disease , the report warned.
The 33-page report was posted
Thursday on BioRxiv, a website that researchers use to share their work before it is peer
reviewed, an effort to speed up collaborations with scientists working on COVID-19 vaccines
or treatments. That research has been largely based on the genetic sequence of earlier
strains and might not be effective against the new one . - LA Times
(via Yahoo)
According to the report, fourteen mutations have been identified in the spike proteins of
SARS-CoV-2 , the protrusions on the exterior of the virus which make up its namesake 'corona.'
The report was based on a computational analysis of more than 6,000 coronavirus samples from
around the world, collected by the Germany-based Global Initiative for Sharing All Influenza
Data.
Assisted by scientists at Duke University and the University of Sheffield in England, the
Los Alamos team focused on a mutation called D614G, which controls changes in spike
proteins.
"The story is worrying, as we see a mutated form of the virus very rapidly emerging, and
over the month of March becoming the dominant pandemic form," said lead author Bette Korber, a
Los Alamos computational biologist. "When viruses with this mutation enter a population, they
rapidly begin to take over the local epidemic, thus they are more transmissible." The new
strain first appeared in Italy, almost at the same time as the original Wuhan strain appeared,
according to the report. By March 15, the mutated strain was dominant. The same was seen in New
York, which was hit by the original virus around March 15, but was overwhelmed by the new
strain within days.
The authors also warn that if the pandemic doesn't wind down during the summer as most
viruses do, it could undergo further mutations right as the first medical treatments and
vaccines - should the adhere to ambitious timelines we've been promised - begin to roll
out.
" We cannot afford to be blindsided as we move vaccines and antibodies into clinical testing
," Korber added on Facebook. "Please be encouraged by knowing the global scientific community
is on this, and we are cooperating with each other in ways I have never seen in my 30 years as
a scientist."
David
Montefiori , a Duke University scientist who worked on the report said it is the first to
document a mutation in the coronavirus that appears to make it more infectious.
Although the researchers don't yet know the details about how the mutated spike behaves
inside the body , it's clearly doing something that gives it an evolutionary advantage over
its predecessor and is fueling its rapid spread. One scientist called it a "classic case of
Darwinian evolution."
" D614G is increasing in frequency at an alarming rate , indicating a fitness advantage
relative to the original Wuhan strain that enables more rapid spread," the study said.
Different strains, different effects?
As the Times notes, doctors in the United States have begun to question whether new strains
of the virus could account for differences in how it affects different people , according to UC
San Francisco professor Alan Wu, who runs the clinical chemistry and toxicology laboratories at
SF General Hospital.
According to Wu, medical experts have speculated in recent weeks that at least two strains
of coronavirus were circulating in the US - one prevalent on the East Coast and one on the West
Coast.
"We are looking to identify the mutation," said Wu, who highlighted that his hospital has
only had a few fatalities out of the hundreds of cases it's treated, which is "quite a
different story than we are hearing from New York."
The Los Alamos study does not indicate that the new version of the virus is more lethal
than the original. People infected with the mutated strain appear to have higher viral loads.
But the study's authors from the University of Sheffield found that among a local sample of
447 patients, hospitalization rates were about the same for people infected with either virus
version.
Even if the new strain is no more dangerous than the others, it could still complicate
efforts to bring the pandemic under control . That would be an issue if the mutation makes
the virus so different from earlier strains that people who have immunity to them would not
be immune to the new version.
And if the mutation makes it back to those who have already had COVID-19, it would make
"individuals susceptible to a second infection," according to the authors.
skrik
May 6, 2020 at 8:52 am GMT
@Kratoklastes ory tract that there might even be a second receptor that the virus could
use to launch its attack.
Even more troubling is the fact that SARS-COV-2 seems to make use of the enzyme furin from
the host to cleave the viral spike protein. This is worrying, researchers say, because furin
is abundant in the respiratory tract and found throughout the body.
It is used by other formidable viruses, including HIV, influenza, dengue and Ebola to
enter cells. By contrast, the cleavage molecules used by SARS-CoV are much less common and
not as effective
I do not think that Covid-19 is 'just a flu' and I think that the panic in Wuhan started in
the next microsecond after they had decoded the [warlike!] spike. rgds
Fears that the coronavirus would mutate into a more dangerous strain appear to have been
borne out, as research has identified that a new, more contagious strain of SARS-CoV-2 has
become the dominant form worldwide. The new strain, which has been dubbed 'Spike D614G' has
been proliferating in Europe since at least mid-February, and spread to become the dominant
form during the month of March. It is far more contagious than the original strain which
emerged from Wuhan, for reasons as yet unknown.
Wherever it emerged it became dominant very quickly, and in some countries it became the
only common strain within weeks. The paper notes that the
rapid global spread of the coronavirus has provided it with "ample opportunity for natural
selection to act upon rare but favorable mutations.'' Furthermore, if the virus does not
wane away as the weather warms in summer there will be nothing to stop it mutating into more
and more strains.
Warning call
The research , which was
carried out by a joint American and British team led by Los Alamos National Laboratory, has
been released ahead of peer review as 'an early warning' to other researchers. As it
stands, scientists studying the coronavirus around the world may be analysing the genetic
sequence of the older strain, and therefore it is crucial that they collaborate with this team
to get the latest information. "We cannot afford to be blindsided as we move vaccines and
antibodies into clinical testing," the lead author Dr Bette Korber, known for her work on
HIV, said.
Because the paper has not yet been peer-reviewed, it has been published online on the server
BioRxiv. However, the reputations of the scientists involved suggest that the findings are
sound and must be taken with the utmost seriousness -- the report is 33 pages long, and short
on laughs. "This is hard news,'' said Korber of the findings.
Also on rt.com
Covid-19 mutations underestimated, Chinese scientists warn, as DEADLIEST strains grip Europe
and US
The scientists' methodology involved running computer analysis of over 6,000 coronavirus DNA
sequences collected from around the world. Although they remark that "observed diversity
among pandemic SARS-CoV-2 sequences is low'' there were no fewer than 14 different
mutations in the Spike protein sequences, just one of which is the strain that has everybody
worried.
This is the strain with the D614G mutation, which is probably causing the increased
contagiousness. The mutation affects the 'Spike proteins' on the outside of the virus, which
allow the virus to invade human cells. For this reason, these spikes have until now been the
main target of those trying to design vaccines or antiviral drugs to combat the virus. There
are currently at least 62 vaccines in development, and most of these are focused on the Spike
proteins.
Wasted efforts
Although there is not really any good news here, this may not be as bad as it sounds. There
is at present no suggestion that Spike D614G is any more deadly than the original. The British
team calculated that people were no more likely to be hospitalized by it, although they did
seem to have higher viral loads (more of the virus in their body).
But even if Spike D614G is not meaningfully different from the old strain, it does not mean
that nothing has changed. The problems introduced by multiple forms of a virus have everything
to do with immunity and vaccination. If a person had contracted and been ill with one strain,
that would still be no guarantee of immunity to another. Epidemiologists could be left every
winter having to guess what the commonest strain of coronavirus will be, as they do with the
flu.
Furthermore, the development of a vaccine relies on designing the antibodies to match
perfectly to the specific 'Spikes' on the outside of the virus. If these are mutated, any
potential vaccine might not be specific enough to target that strain. Receiving the vaccine
would provide no guarantee of immunity. This possibility is especially worrying to the study's
authors.
Also on rt.com Neither 'lab'
nor 'wet market'? Covid-19 outbreak started months EARLIER and NOT in Wuhan, ongoing Cambridge
study indicates
The authors have also been led to speculate that the wildly different outbreaks experienced
in different regions could be down to different strains. Spike D614G hit Italy in early
February, probably around the same time as the older strain hit there. Italy has been one of
Europe's worst affected countries.
And in America, just a few days after the first cases were reported in New York, Spike D614G
was the dominant form there. Contrasting New York City with the relatively mild outbreak on
America's West Coast suggests that different strains could be at play. No matter what details
transpire, it's clear that in a world with multiple strains of coronavirus, developing vaccines
or treatments is only going to get harder.
Notable quotes:
"... "Actually, wearing masks on the street is stupid. First, in the open air, it is absolutely useless, only makes it difficult for people with disabilities to breathe. But, of course, in public places, shops, probably, wearing a mask should be left. Secondly, if you do not provide the entire population with masks, it will end in the fact that a person will buy a single mask and wear it forever, which will cause much more harm to health," Zverev says. ..."
May 06, 2020 | vz.ru
The virologist also spoke about the possible introduction of a mandatory "mask regime"
throughout Russia, which is written about by the media.
"Actually, wearing masks on the street is stupid. First, in the open air, it is
absolutely useless, only makes it difficult for people with disabilities to breathe. But, of
course, in public places, shops, probably, wearing a mask should be left. Secondly, if you do
not provide the entire population with masks, it will end in the fact that a person will buy
a single mask and wear it forever, which will cause much more harm to health," Zverev
says.
He explains that after two hours of continuous wearing of the mask, it becomes wet, which
turns it from a means of protection to a means of infection with viruses and bacteria. Zverev
reminds that in addition to the coronavirus in the world, there are still a huge number of
infections that can also cause severe harm to a person, so it is not necessary to resort to
such measures yet.
Earlier, a mandatory "mask regime" was introduced in the Moscow region in order to prevent a
new coronavirus. For going out on the street without this means of protection, citizens of the
region face a fine of 4 thousand rubles.
Krollchem , May 5 2020 0:05 utc |
89
Laguerre@11
"Every time the virus replicates, there is a danger of error in the copy, which renders it
less effective for the most part, much as in human cells."
The issue is that the SARS-CoV-2 spike (S) protein that binds to ACE2 and CD147 receptors
is what allows the virus to replicate more efficiently. In a given population of viral
particles a less efficient particle would result in fewer replicates leading its mutation to
be less prevalent in a population of the coronavirus.
Thus, I would expect the virus to retain its virulence over time which leads us back to Dr
Talab's conclusion on how to stop the transmission of a virus that needs a host. A subset of
the availability of a host is what happens if the host can also be a non-human such as the
Chinese raccoon dog, ferrets or even pigs?
In discussing viral mutations it is important to also note that articles that claim to
calculate viral mutation rates fail to understand that statistics is about populations, and
not individuals. The mutation rates of a population are not well represented by the PCR test
if the mutation is not frequent enough to be seen in the amplification process (38-39
times).
I would not bet against the persistence of the SARS-CoV-2 virus S-protein and thus its
continued virulence given the probability of mutations and the loss of function by a less
virulent strain.
There may be hope in an engineered antibody that targets the viral spike protein:
https://www.zerohedge.com/health/coronavirus-defeated-experimental-antibody-targets-spike-protein
As for a vaccine, I would not hold my breath and if partially successful might result in
more deaths due the the vaccine of the cytokine storm that the virus itself.
Deap ,
04 May 2020 at 01:44 PM
What does an anti-body test do? I just had one last week and awaiting the results - was a
cruise passenger and international air passenger during the month of January in a later
suspected area. (not Asia).
Here is why I did the anti-body test: (Quest Labs - fee service, no RX- 99% accuracy -
drawn blood vial test)
1. Helps substantiate dates and areas of transmission that may not yet be in the data
pool.
2. Tracks the rates of asymptomatic or mildly symptomatic cases occurring among the
"elderly", in order to see if there is an enhanced risk of not in this age group, if there
are no underlying co-morbidities.
3. Adds demographic data specific for the travel industry.
4. Allows possible donation of anti-body serum for research and perhaps mitigation of
those who are affected.
5. Personal peace of mind -been there and done that. Freedom to move about.
6. Provides baseline for duration of immunity; resilience of immunity or data showing
re-infection can be possible.
Primarily it is for data gathering to help stop the hysteria. That was worth the time,
money and blood donation for me. We will never know the true extent of this virus, its
impacts, its initial modeling accuracy until we start plugging facts into the "expert"
hypotheticals.
Taking one for the team is the way I see it. Will I now become a local Typhoid Mary and
our house burned down if this data becomes known? Or will people stop walking out into the
roadway in faux deference to my advanced age as I pass by, from our deliciously virtue
signaling "progressive" population in blue state California.
turcopolier
04 May 2020 at 01:47 PM
Deap
"Provides baseline for duration of immunity; resilience of immunity or data showing
re-infection can be possible. Primarily it is for data gathering to help stop the hysteria."
Yes
Marina Solonos 8:18 PM - 2 May 2020
GSK partnered with Bill Gates to produce the Covid-19 Vaccine. GSK has been found guilty
for several criminal federal offenses, bribes and health violations, and paid Billions in
lawsuits including for birth defects & brain damage. https://www. drugwatch.com/manufacturers/ glaxosmithkline/ #
BillGates # QAnon # q
https--childrenshealthdefense.org-wp-content-themes-chd-theme-chd-theme
Promising
his share of $450 million of $1.2 billion to eradicate polio, Gates took control of
India's National Technical Advisory Group on Immunization (NTAGI), which mandated up to
50
doses (Table 1) of polio vaccines through
overlapping immunization programs to children before the age of five. Indian doctors
blame the Gates campaign for a devastating non-polio
acute flaccid paralysis (NPAFP) epidemic that paralyzed 490,000 children beyond
expected rates between 2000 and 2017. In 2017, the Indian government dialed back Gates'
vaccine regimen and
asked Gates and his vaccine policies to leave India. NPAFP rates dropped precipitously.
Pft , May 2 2020 23:31 utc |
49
Yesterday a preprint of a collaborative study involving medical, genomic and virology
researchers from Los Alamos National Laboratory in New Mexico-US, University Of Sheffield-UK,
Duke University in North Carolina-US, Sheffield Teaching Hospital-UK and the
NHS-Foundation-UK, was released. No quacks there.
It shows that the Spike elements of SARS-CoV-2 coronavirus is mutating
https://www.biorxiv.org/content/10.1101/2020.04.29.069054v1.full.pdf+html
It uses real-time mutation tracking in the SARS-CoV-2 coronavirus, specifically on the
Spike (S) protein because it mediates infection of human cells and is the target of most
vaccine strategies and antibody-based therapeutics.
It monitored changes over the last two months from the early strains in Wuhan to the
specific strains across the globe in conjunction with the GISAID data.
They focused on 14 specific sites on the virus and 2 Spike mutations were of particular
interests: D614G and S943P.
It was found that D614G is increasing in frequency at an alarming rate, indicating a
fitness advantage relative and enables more rapid spread. S943P is located in the fusion core
region, and is of particular interest as it is concerned with spreading via
recombination.
D614 is located on the surface of the spike protein protomer, where it can form contacts
with the neighboring protomer. The mutation allows from a structurally perspective more easy
'binding' to human host cells through a variety of ways and from a immunological function, it
disrupts antibody functions trying to attack it.
Hence the D614G mutation not only increases transmissibility, but also impacts severity of
disease.
The S943P mutation however allows recombinant strategies for the virus to evolve.
The study of the other mutation sites L5F, L8V V367F, G476S, and V483A all indicate that
he virus can easily and evolve depending and conditions, displaying characteristics that it
is even far more potent than HIV. There were also many other sites of mutations that the
study covered.
So thats not very encouraging and doesn't bode well. Not conclusive but just means this
needs watching.
... ... ...
As long as social distancing is maintained, there is no harm of people specing some time
ourdoors. Excessive zeal here is countrproductive
Angry Italian mayors
rage at people ignoring coronavirus lockdown rules - YouTube
ppermint 1
month ago
Well, walking your dog around the home for 5 minutes with no other people around, will not
spread anything and will keep a better mental health. Italians have gone from total ignorance
to total isolation - another extreme. Unfortunately, many people are undisciplined and
careless, so there's no other choice. By the way, stop running: you may already have the
virus, making any physical effort will only waste your body energy to fight the virus
spywhale 1
month ago
Its not the people in the open countryside or walking in the streets or relaxing in the
park spreading the virus its when people travel together in buses, trains or any crowded
environment.
shaun grobbelaar 2 weeks ago
Ah the open border Italian wussy is complaining about smokes. they stupid
forist1 2 weeks
ago
The Camorra are scared of the Black Axe , Maybe if the mayors stopped turning a blind eye
to the growing threat of criminal gangs on there streets instead of bullying there citizens
Italy would be a safer place to live .
NotJerry Beans 1
month ago
Poor government makes ignorant majors
Michael Lee 1
month ago
"Sweet coronavirus-flavoured cream" that's a good one, Mayor.
Eagle 4 1 month
ago
"What do you even need these haircuts for!?" 😂😂😂😂
Justin B 1
month ago
They've censored all the funny bits. Like how the mayor with the glasses says the f word a
lot and the one talking about hairdressing says the casket is closed, noones going to see
your new haircut when yo dead' 😂
P.C.
Π.Χ.Φ.Ω 1 month ago
Love them all Mediterreneans-they have such passion and fire in them . Italians, Greeks,
Spanish..LOL
Ma Sa 1 month
ago
I love the last part "why people suddenly become runners."
Sam H 1 month
ago
i love their dark humour. viva italia! what a tremendous loss of the country's elderly
population, I love italian elderly, they have so much wisdom and charisma. what a loss.
Emah Edabus 1
month ago
The best one from another clip was: if u have a party I'll send the police with
flamethrowers. They're all passionate!
Tristan Lau 1
month ago
If anyone in Italy violates the lockdown rules will be subjected to eating pineapple
pizza, the streets will be empty.
Adriana Giuro-Walla 1 month ago
"La bestialità totale!" 🤣 Grande Sindaco De Luca!
A BC 1 month
ago
I must admit, I feel so much better working from home than dragging myself to the office.
And there is so much flexibility.
Pesi Belau 4
weeks ago
The best one were the who made references to will smith and the one who threathen to send
police with torch to break party out!!
Lysander , Apr 29 2020 17:33 utc |
8
"The real threat isn't the virus that has killed 59,000 Americans. It is a nonexistent
vaccine for it."
There are many valid comments in that post, but...call me crazy...I will not be taking any
vaccine that's been rushed in a few months. Vaccines take quite a while to develop and the
consequences of taking a poorly researched one are quite severe. However, I doubt it will
come to that, as even the most optimistic vaccine estimate seems to be 18 to 24 months. By
which time herd immunity will have happened whether anyone wants it to or not.
Clearly this is much worse than any flu in the past century. But I don't blame anyone for
being suspicious when so many contract the disease either have mild symptoms or none at
all.
Ghost Ship , Apr 29 2020 17:58 utc |
11
I really can't see COVID-19 as a bio-weapon, it's far too non-specific for that, but what I
might think possible is that someone developed it plus corresponding vaccine and
anti-COVID-19 drug to make billions out of it. The longer the release of the vaccine and drug
are delayed, the more valuable they become. If someone had released the vaccine straight
after COVID-19, it might be worth a few million dollars and the authorities would be very
suspicious, but if release was delayed for a few months it would be worth billions and every
country is so desperate for a vaccine/treatment they most likely be too bothered. It'd need a
new definition for the term vulture capitalist.
Allen , Apr 29 2020 18:06 utc |
16
oldhippie@2
Can you link to that statement/story.
Let's also remember that Gilead/Rumsfeld were the driving forces with the Avian Flu Hoax
(Tamiflu) that resulted in scandals and mass profiting- Rumsfeld himself who was once CEO of
Gilead sold his Gilead shares and netted a handsome return.
https://www.globalresearch.ca/bird-flu-a-corporate-bonanza-for-the-biotech-industry/1190
https://constantinereport.com/donald-rumsfeld-gilead-the-bird-flu-hoax/
https://www.independent.co.uk/news/world/americas/donald-rumsfeld-makes-5m-killing-on-bird-flu-drug-6106843.html
Stonebird , Apr 29 2020 19:48 utc |
33
oldhippie | Apr 29 2020 16:52 utc | 2 + Allen @17
Don't forget Rumsfelds attraction to vast sums of money. After Tamiflu, Aspartame, and now
Gilead there are still the two trillion $ that disappeared from Pentagon's accounts just
before 9/11.(The records/archives were in Bat 7, and the thing that hit the Pentagon itself,
exploded in the Finance/accounts section).
So statistically, where there is Rumsfeld it is 100% certain there is something that will
be profitable. Or should that be, where there is some profit to be made from a disaster, it
ought to be statistically possible to calculate the part that goes to Rummy?
H.Schmatz , Apr 29 2020 19:59 utc |
35
So statistically, where there is Rumsfeld it is 100% certain there is something that will
be profitable. Or should that be, where there is some profit to be made from a disaster, it
ought to be statistically possible to calculate the part that goes to Rummy?
Posted by: Stonebird | Apr 29 2020 19:48 utc | 33
And why is that this obviously crony dude is always absent from scrutiny by the media and
Congress?
The latest round of 'surveillance' testing for coronavirus antibodies was
done on first responders, and found that the number who tested positive was once again
surprisingly high.
New York State has tested over 2,000 first responders for COVID-19 antibodies.
Preliminary results:
FDNY/EMT: 17.1% positive
... ... ...
For the past few weeks, more than 50 scientists have been working diligently to do something
that the Food and Drug Administration mostly has not: Verifying that 14 coronavirus
antibody tests now on the market actually deliver accurate results.
These tests are crucial to reopening the economy, but public health experts have raised
urgent concerns about their quality. The new research, completed just days ago and posted
online Friday, confirmed some of those fears: Of the 14 tests, only three delivered consistently reliable results . Even the
best had some flaws.
The research has not been peer-reviewed and is subject to revision. But the results are
already raising difficult questions about the course of the epidemic.
Surveys of residents in the Bay Area, Los Angeles and New York this week found that
substantial percentages tested positive for antibodies to SARS-CoV-2, the official name of the
new coronavirus. In New York City, the figure was said to be as high as 21 percent. Elsewhere,
it was closer to 3 percent.
The idea that many residents in some parts of the country have already been exposed to the
virus has wide implications. At the least, the finding could greatly complicate plans to reopen
the economy.
Already Americans are scrambling to take antibody tests to see if they might escape
lockdowns. Public health experts are wondering if those with positive results might be allowed
to return to work.
But these tactics mean nothing if the test results can't be trusted.
In the new research, researchers found that only one of the tests never delivered a
so-called false positive -- that is, it never mistakenly signaled antibodies in people who did
not have them.
Two other tests did not deliver false-positive results 99 percent of the time. But the
converse was not true. Even these three tests detected antibodies in infected people only 90
percent of the time, at best.
The false-positive metric is particularly important. The result may lead people to
believe themselves immune to the virus when they are not, and to put themselves in danger by
abandoning social distancing and other protective measures.
It is also the result on which scientists are most divided.
"There are multiple tests that look reasonable and promising," said Dr. Alexander Marson, an
immunologist at the University of California, San Francisco, and one of the project's leaders.
"That's some reason for optimism."
Dr. Marson is also an investigator in the Chan Zuckerberg Biohub, which partly funded the
study.
Other scientists were less sanguine than Dr. Marson. Four of the tests produced
false-positive rates ranging from 11 percent to 16 percent; many of the rest hovered around 5
percent.
Highly recommended !Notable quotes:
"... By JoNel Aleccia, Senior Correspondent at Kaiser Health News, who previously reported for The Seattle Times, NBCNews.com, TODAY.com and MSNBC.com. Originally published at Kaiser Health News ..."
By JoNel Aleccia, Senior Correspondent at Kaiser Health News, who previously reported
for The Seattle Times, NBCNews.com, TODAY.com and MSNBC.com. Originally published at
Kaiser Health News
After hearing for months about serious access issues involving tests that diagnose COVID-19
based on swabs from the nose or throat, Americans are being inundated with reports about
promising new tests that look for signs of infection in the blood.
There are high hopes for these antibody tests, which detect proteins that form in blood as
part of the body's immune response to an invading virus. Communities across the U.S. have been
rolling out the results of serological surveys that examine blood samples from people who
haven't been diagnosed with COVID-19 to see if they were, in fact, previously infected.
The thinking is, if there are blood markers that can detect when people have been infected,
such tests should be able to tell us how widely the novel coronavirus has spread. And equally
optimistic: those same antibodies could convey immunity to the disease, signaling someone is
safe from reinfection and able to get back to work.
Such high hopes, however, are running smack into the roadblocks of reality.
Infectious disease experts are raising pointed questions about the reliability of the early
tests and the studies that hinge on their results. And they warn that state and local
governments -- as well as individuals -- should be wary of shaping policy or changing behavior
based on any single report.
In the sharpest caution to date, officials with the World Health Organization on Saturday
warned against plans for proposed "immunity passports," which would allow people who have
recovered from the coronavirus to resume unrestricted travel and work.
"There is currently no evidence that people who have recovered from COVID-19 and have
antibodies are protected from a second infection," the agency wrote in a scientific brief.
Even before the WHO weighed in, other experts were urging restraint in interpreting early
results of antibody screening.
"The science is catching up," said Dr. Liise-anne Pirofski, chief of the division of
infectious diseases at the Albert Einstein College of Medicine and Montefiore Health System.
"Our ability to make a test at the moment is much greater than our understanding of what those
antibodies we are testing for mean."
In the past few weeks, more than 180 academic centers, hospitals and private manufacturers
have notified the federal Food and Drug Administration that they intend to create serology
tests for COVID-19, spokesperson Stephanie Caccomo said in an email. They've been able to jump
into the fray because the FDA in March
relaxed regulations for developing tests as part of its emergency response to the
pandemic.
But the FDA has not reviewed the vast majority of tests on the market, and their validity,
particularly point-of-care blood tests that promise rapid results within minutes, isn't clear,
said Dr. Michael Busch, director of the Vitalant Research Institute and a professor of
laboratory medicine at the University of California-San Francisco.
"Some of them have sensitivities that are quite poor," he said. "You may even miss some
infected people completely."
Other tests may flag people as positive for COVID-19 when they're not infected. That's
especially true in regions of the country with little spread of the novel virus. If the
prevalence of a disease is low, less than 5%, even an accurate test would yield a high number
of false positive results because of the way such screening tools operate.
So when people see advertisements for finger-prick antibody tests becoming widely available
at urgent care centers and medispas, they should think twice.
For one, antibody tests can't be used to diagnose the disease. Antibodies may not be present
in high enough levels to be detected in the earliest days of an infection. And because there
are several other known coronaviruses -- including those that cause the common cold -- people
infected with those viruses could produce antibodies that cross-react with those produced in
response to the new virus.
Scientists still know too little about whether antibodies to COVID-19 convey immunity that
could allow people to put away masks and halt social distancing, said Dr. Mary Hayden, director
of the division of clinical microbiology at Rush University Medical Center in Chicago.
Immunity to a virus is a complicated process that takes place over one to two weeks, the WHO
noted. The immune system makes antibodies in response to an infection. But the body also makes
T-cells that recognize and eliminate other cells infected with the virus, creating what's known
as cellular immunity. Those two processes together may help a person recover and prevent
reinfection. But it is not yet clear whether cellular immunity is required to bolster recovery
and prevent subsequent infection with COVID-19.
"We do not know whether or not the antibodies detected are protective," Hayden told
reporters last week on a call organized by the
Infectious Diseases Society of America . "We recommend that people with antibodies not
change their behavior in any way."
Scientists are hoping, however, that future COVID-19 studies may demonstrate immunity that
could last for one or two years.
Concerns about the validity of the tests have cast a shadow on several recent reports aiming
to quantify the spread of the virus in specific regions. Last week, New York Gov. Andrew Cuomo
revealed the results of a serological survey that suggested that 1 in 5 New
York City residents had been infected with the coronavirus. Statewide, the figure was
13.9%, according to the study of 3,000 New Yorkers in 19 counties who were recruited at grocery
stores.
But the results quickly drew criticism. Dr. Demetre Daskalakis, who directs the city's
disease control, warned that the tests could produce
"false negative or false positive results. " Florian Krammer, a microbiology professor at
the Icahn School of Medicine at Mount Sinai who designs such tests, tweeted -- and later
deleted -- that the results were "BS."
"I think this is too high," he said in a later tweet. "It is
possible. But a 20% plus infection rate seems too high for NYC due to a number of reasons. I
would think 6-8%, maybe 10% are closer to the truth. It would be nice to know more about the
test, its sensitivity and specificity and the test population."
Similarly, two serology studies in California, one in Santa Clara County and one in Los
Angeles County, drew wide criticism about the recruitment of subjects and the analyses
used.
In the Santa Clara study ,
Stanford University researchers tested 3,330 volunteers for antibodies showing exposure to
COVID-19; about 1.5% were positive. They concluded that meant from 48,000 to 81,000 people were
infected with the virus in the county.
"It was completely inadequate to interpret the results that 50,000 to 80,000 people were
infected," Busch said.
The L.A. study, conducted by University of Southern California researchers, concluded that
2.8%
to 5.6% of the county's adult population had been exposed to the coronavirus. That
translates to 221,000 to 422,000 adult residents who have been infected. Critics, however,
argued that the study sample was too small and that details of the methodology weren't
immediately available.
Busch understands the drive to conduct such tests.
"People are asking the questions: What's the real denominator to judge the case counts and
the death counts against?" he said. "People are urgently trying to get data."
Unfortunately, that data simply is not available yet, other experts said. This coronavirus
has never been seen before, so the science that will inform efforts to help communities respond
and recover is playing out in real time.
"The problem is that the science has not kept up with the tests," Hayden said. "Now we need
to do the research to tell what the results mean."
On the positive side, most of the scientific community has pivoted to focus on finding
solutions, said Pirofski, who was also on the IDSA call. "We just have to slow our roll."
"This is our first dive in trying to understand what's going on," she said. "I would say
it's a start."
Highly recommended !Notable quotes:
"... Media reports paint a picture of healthcare workers being hit very hard by the pandemic, but the statistics suggest otherwise ..."
"... substantially under-represented ..."
Media reports paint a picture of healthcare workers being hit very hard by the pandemic,
but the statistics suggest otherwise
A recent statistical study published
in the Health Services Journal (HSJ) provides some important facts and context:
Firstly, let's establish the data: As of 22nd April, 119 "NHS workers" were reported to have
died of Covid19. Thirteen of them were excluded from the study for being either retired or
never confirmed to work for the NHS.
That left 106 NHS staff who died of alleged Covid19.
Secondly, we should clear up the misconception that this represents just "frontline"
healthcare workers. It doesn't.
This number includes 35 nurses, 18 doctors and 27 healthcare assistants (HCAs), they are all
"frontline" workers. But it also includes 36 others (dentists, psychiatrists, porters,
administrators, receptionists etc).
Finally, let's put these numbers in some context:
The NHS is the biggest single employer in the UK. NHS England, NHS Scotland and NHS Wales
employ roughly 1.5 million people (Wikipedia estimates over 1.7 million
). That's over 4% of the 38 million working-age adults, or 2.5% of the entire population of the
UK.
As such, you would expect roughly 2.5% of the Covid19 victims to be NHS employees (assuming
proportionate distribution).
However, the 106 NHS employees represent only 0.58% of the UK's 18,200 total Covid19
casualties as of April 22nd.
To put it another way:
Any randomly selected citizen of the UK has a 1/39 chance of being
employed by the NHS. But any randomly selected "Covid19 related death" has a 1/172 chance of
being employed by the NHS.
In summary: In direct contradiction of the media coverage, healthcare workers are NOT being
disproportionately affected by Covid19. They are actually substantially
under-represented .
Highly recommended !I recommend to listen to this video in full. It is really good !
Rebecca Elliott 4
days ago
Sign of a true expert - admitting when you don't know the answer to something
Mike Rees 4
days ago
The format you have here with Dr Jenkins is really good. Almost like a podcast. You two
have a great rapport
Sarah's Tarot 4
days ago
Doctor Jenkins is so level headed. I imagine he must be a very reassuring presence for his
patients
SuperLkelley 4
days ago
As a research scientist in the life sciences at Imperial College, this interview is the
best source of information I have seen on the internet. Thank you so much.
Daily Occasions 4
days ago
This format where you ask a question and allow a detailed response was delightful!
Watching this conversation between two highly skilled and intelligent doctors who are full of
compassion has given me hope. Please do more video's like this ? Well done doctors well
done!
Highly recommended !If 99% of cases of infection happen in closed spaces and/or in open spaces with very close
and long contact (stadiums, parties, festivals, concenrts, atc) is it really wise to limit
activities in which social distancing can be maintained, such as jogging, fishing, biking,
etc
Also the policy on mitigation (complete suppression is impossible now) should vary by
locality. What is good for NYC is idiotic for rural Pennsylvania.
As the jogger struggled with police, screaming for help, she was filmed by residents who had
absolutely zero sympathy for her plight. 'What's not fair is that you go out running, you
bloody idiot!', shouted the woman apparently filming the encounter."
Coronavirus lockdown: Jogger
resists arrest in Spain and is abused by onlookers , AS.com, (21st March 2020)
Watching a fight yesterday in Walmart between couple of fat American female sweathogs over
TP convinced me that Uncle Sam will be flushed down the toilet long before the EU.
xxx
Was it one ply or 2-ply?
Emily Annette 1:50 PM - 9 Apr 2020
At the grocery. Wearing my mask. Lady behind me, snarky & loud enough to make sure I
heard, "don't guess she realizes that stupid mask won't do any good." Me: "Honey, I'm an off
duty nurse, I'm wearing it to protect YOU. But, I can take it off if you'd like." She
practically ran.
The reality of the #COVID19 pandemic
is that my patients have lost all faith in our healthcare system so even when they are very
short of breath or have low oxygen levels they refuse to go to the ER bc they're afraid they
will die in a corner and they would rather die at home.
-- uché blackstock (@uche_blackstock) April
15, 2020
A German team under Prof Streeck argues that workplaces don't spread the coronavirus as much
as play spaces: singing in a choir produces an aerosol and spray cloud, dancing together in a
room or bar, or nightclub apres-ski, also creates infective clouds, as would any confined space
where lots of people are in close contact breathing heavily. Although public health guidance
has been coy on this matter, orgies are probably best avoided.
On that theme, there are settings in which you are likely to get a big dose, a large viral
load, and others where the globules will be few and far between. As one caustic virologist
observed, getting out into the open air is a good defense against respiratory transmitted
infections: avoiding infection is a walk in the park.
Highly recommended !
Authored by
James Howard Kunstler via Kunstler.com,
The ruins of Mary McClellan Hospital stand on hill overlooking the village of Cambridge, New
York, in what was a "flyover" corner of the country until the planes stopped flying. The
hospital cornerstone was laid July 4 1917. The USA had entered the war against Germany a few
months earlier. The "Spanish" flu pandemic kicked off in January, 1918. The hospital opened in
January 1919. The flu burned out a year later. The hospital shut down for good in 2003.
I've lived around here for decades and never actually got a look at the place until I went
up there on a blustery spring Saturday before Easter to look around. I like to read landscapes
and the human imprint upon them. This one is a ghost story, not just of the bygone souls who
came and went here, but of an entire society, the nation that we used to be and stopped being
not so long ago.
This is the old main building today. It's astounding how quickly buildings begin to rot when
the human life within them is gone. The style was Beaux Arts Institutional, seen everywhere
across America in that period in schools, libraries, museums, and hospitals, an austere
neoclassicism that radiated decorum in a confident and well-run society – because
that is what we were then. Note especially, the entrance and the beautiful bronze marquee above
it. The message is this: You enter through a portal of beauty to a place of hope and trust.
This is Mary McClellan Hospital not long after it opened.
The site itself, on its hill, with views east across the state line to the Green Mountains,
speaks of authority and command.
The America of 1919 was a deeply hierarchical society. Today we regard hierarchy as a bane
and a curse. The truth is, it is absolutely required if you expect to live in a well-run
society, and proof of that is the disordered mess of bureaucratic irresponsibility we live in
today, with virtually every institution failing – well before the Covid-19 virus arrived
on the scene - and nobody called to account for anything anymore.
Hierarchy must be fit to scale to function successfully. In small institutions like this,
everybody knows who is responsible for what. That's what makes authority credible.
These are the ruins of the nursing school associated with the hospital (and also associated
with Skidmore College in Saratoga Springs, 25 miles west).
The nurses lived here, in Florence Nightingale Hall.
In the early 20th century, the profession favored young, unmarried women whose allegiance
and attention to the patients would not be distracted by the needs of a family.
Was that exploitation? Or was it simply an intelligent way to organize a hospital
subculture? The nurses lived here very comfortably. The institution cared for them,
literally.
There's no record available of what exactly these buildings were for. The one in the
foreground has a cut stone sign that says "The Junior" on it. I infer that this may have been
where a couple of young, staff, resident physicians lived, young men probably, just out of
their internships, close at hand and on-call for emergencies. The building in the background is
a rather grand country cottage, possibly the residence of the chief surgeon or the hospital
director. The hospital was, after all, a community unto itself, and it was important that
authority have a visible presence there all the time. Both buildings display architectural
grace-notes that humanized and dignify that resident authority. We no longer believe in
grace-notes for the things we build, so is it surprising that we live in a graceless
society?
This is the power plant for the whole operation, on the premises, ensuring that the
electricity would stay on at all times. In the early 20th century, electric power was the new
sine qua non of advanced civilization. America's rural electrification program really didn't
get underway until the 1930s, so it's likely that many of the farms outside the village were
not hooked up to a grid. The hospital generators must have been driven by coal, or perhaps oil.
Somebody had to attend to all that machinery. The laundry – hospitals produce a lot
of that – was also on-premises, as was all the meal preparation. The hospital maintained
a large garden to furnish some of the food. All these tasks required crews of people working
purposefully and getting paid. The hospital was a complex organism, a world within a nation
within a world.
Things rise and self-organize beautifully into fully-formed systems and after while they run
down, even while they over-grow; authority starts working more and more for its own sake and
its own benefit; hierarchy breaks down into disrespect, lack of trust, fear; and then society
loses its vital institutions, which is exactly what happened at Mary McClellan Hospital in
little Cambridge, New York.
It dwindled and then quickly collapsed. The town lost a part of itself, the part that
welcomed people in a particular kind of trouble and cared for them, as it cared for those who
did the caring. By the way, in 1919, a private room was $7-a-day (a bed on a ward was $3).
Imagine that! The town also lost a vital component of its economy. And that was all of-a-piece
with its decline into the flyover place it became in our time.
American health care, as we call it today, and for all its high-tech miracles, has evolved
into one of the most atrocious rackets the world has ever seen. By racket, I mean an enterprise
organized explicitly to make money dishonestly. This is what we've become, and the fact that we
seem to be okay with that tells you more about what we have become. The advent of Covid-19,
along with the extreme economic disorders it has triggered, will probably be the beginning of
the end of that racket. We have no idea how medicine will re-organize itself, but I'd guess
that it will happen at a much more primitive scale – because that's usually what
happens when human societies overshoot badly. Alas, history is not exactly symmetrical.
But read these photos and meditate on what we were once capable of putting together in this
land, and maybe you will find some clues about what was truly admirable about the American
condition before we stopped caring.
Highly recommended !
Whistler-Riptide
The text message from Ai Fen (艾芬), the director of the emergency department of
Wuhan Central Hospital, agreeing to be interviewed, was sent at 5 am on March 1. About half an
hour later, at 5.32 am on March 1, her colleague and director of thyroid and breast surgery
Jiang Xueqing, who was infected with new coronavirus pneumonia, died. Two days later, Mei
Zhongming, deputy director of ophthalmology at the hospital, died. He and Li Wenliang were in
the same department.
As of March 9, 2020, 4 members of the medical staff of Wuhan Central Hospital have died of
new coronavirus pneumonia infection. Since the outbreak, this hospital, located just a few
kilometers away from the Huanan Seafood Market, has become one of the hospitals in Wuhan with
the largest number of employees that are infected. According to media reports, more than 200
employees in the hospital were infected, including three deputy deans and multiple working
department directors. Multiple department directors are currently being maintained with ECMO
[extracorporeal membrane oxygenation].
The shadow of death hangs over this, Wuhan's largest tertiary hospital. A doctor told People
[a news site – EB] that in the social media group of hospital staff, almost no one spoke
publicly; they mourned and discussed in private.
This tragedy could have been prevented. On December 30, 2019, Ai Fen received a virus test
report for a patient with an unknown pneumonia. She circled the word "SARS coronavirus" in red.
When asked by a college classmate who is also a doctor, she took a picture of the report and
circulated it. That night, the report spread in doctor circles in Wuhan, and those who
forwarded the report included the eight doctors who were disciplined by the police.
This caused trouble for Ai Fen. As the original source of the information, she was
interviewed by the hospital disciplinary committee and suffered an "unprecedented and severe
reprimand"; it was said that she was acting unprofessionally by creating false rumors
(谣).
In the afternoon of March 2nd, Ai Fen did an interview with People in the Nanjing Road
location of Wuhan Central Hospital. She was sitting alone in the emergency room office. The
emergency department, which had been admitting more than 1,500 patients a day, had returned to
quiet. There was only one tramp lying in the emergency hall.
Some previous reports called Ai Fen "another severely reprimanded female doctor who has
emerged" and some people called her a "whistleblower". Ai Fen corrected this; she said she was
not a whistleblower, but the one who distributed the "whistles".
During the interview, Ai Fen mentioned the word "regret" several times, and said she deeply
regretted that she hadn't continued to whistle resoundingly after she was reprimanded at a
disciplinary review meeting. She has especial regrets when it comes to her deceased coworkers.
"If I knew then what I know now, I wouldn't care about the pressure (from my leader), and I
would [expletive] speak everywhere, all right?"
What have Wuhan Central Hospital and Ai Fen experienced in the past two months or so? The
following is what Ai Fen told us:
An unprecedented reprimand
On December 16, last year, we received a patient at the Nanjing Road emergency department.
They had an inexplicably high fever, and they weren't responding to standard medications, their
body temperature wasn't going down at all. On the 22nd, the patient was transferred to the
respiratory department, a bronchoscopy was done, and bronchoalveolar fluid taken and sent out
for high-throughput genetic sequencing. Afterwards, the coronavirus result was relayed
verbally. At that time, the colleague who was responsible for the patient told me clearly:
"Director [主任] Ai, that person's diagnosis is coronavirus". Later we learned that
the patient worked in the Huanan Seafood Market.
Immediately afterwards, December 27th, another patient arrived at Nanjing Road. He was the
nephew of a doctor in our department. He was in his 40s, without any preexisting conditions.
His lungs were in a terrible state, and his blood oxygen saturation was only 90%. He was under
hospital care for almost 10 days without any improvement, and was admitted to the respiratory
department. A flexible bronchoscopy was also done, and the alveolar lavage fluid sent for
testing.
At noon on December 30th, an old classmate at Tongji (同济) Hospital sent me a
screenshot of a WeChat conversation, which said: "You don't want to go to Huanan [Market] just
now, there are lots of people with high fever " He asked if it was true. At the time, I was
watching a CT [scan] of a typical patient with pulmonary infection on the computer. I sent him
a 11-second video of the CT and told him it was a patient who had come to our emergency
department in the morning, a Huanan Seafood Market case.
Just after 4 pm that day, a colleague showed me a diagnostic report that said: "SARS
coronavirus, Pseudomonas aeruginosa, 46 strains of bacteria [菌, bacteria and/or fungi]
which colonize the oral cavity and/or respiratory tract". I read the report very carefully many
times, and the supplementary information read: "SARS coronavirus is a single-stranded
positive-strand RNA virus. The main mode of transmission of the virus is close-range droplet
transmission or contact with respiratory secretions of patients, which can cause an unusual
pneumonia that is highly contagious and can affect multiple organ systems, also known as
atypical pneumonia."
At the time, the diagnostic report scared me, I broke into a cold sweat, this was a
terrifying thing. The patient was admitted to the respiratory department, the situation needed
to be reported to the respiratory department, but to ensure attention, I immediately phoned and
reported it to the hospital's public health division and infectious disease [?院感]
division. At that moment, the director of the respiratory department of our hospital happened
to be passing my office door, someone who had been involved with SARS. I grabbed the director
and said, "We found this in one of the patients in your department." The director took one look
and said it was worrying. I knew the matter was worrying.
After calling the hospital, I also circulated this report to my fellow-learners
(同学[; student or former classmate]). I purposely drew a red circle around the
words "SARS coronavirus, Pseudomonas aeruginosa, 46 strains of bacteria [菌, bacteria
and/or fungi] which colonize the oral cavity and/or respiratory tract" to bring the warning to
their attention. I also sent the report to the doctors in the department to warn everyone to
take precautions.
That evening, the message was spread widely; the screenshots of the transmission show the
photos of the report I'd marked with a red circle, including the ones that I later learned that
Li Wenliang passed on to the [chat] group. At the time, I was thinking it might be bad. At
10:20, the hospital passed on a message [reportedly on the Central Hospital WeChat group]. It
was a relayed notification from the city Health Protection Committee
(市卫健委). Their main point was that information on the pneumonia of
unknown cause should not be arbitrarily released, to avoid causing panic among the public; if
panic was caused by information leakage, there would be a thorough investigation
(要追责).
I was very scared at the time and immediately passed this information on to my
fellow-learners. About an hour later, the hospital sent another notice, again stressing that
information the group had on this subject could not be leaked. One day later, at 11:46 pm on
January 1st, the head of the hospital's disciplinary inspection committee sent me a message to
come [for an employee review] the next morning.
I didn't fall asleep that night, I was worried and thought things through over and over
again, but I felt that there are always two sides to everything; even if it had caused adverse
effects, it was not necessarily a bad thing to remind medical staff in Wuhan to take
precautions. At 8 o'clock the next morning, before I finished the shift, I was called in for
the disciplinary review.
In that disciplinary review, I suffered an unprecedented and very severe reprimand.
At that time, the leader of the discussion said, "We can't afford to raise our heads when we
go out for a meeting. The director of XX criticizes our hospital. As the director of the
emergency department of Wuhan Central Hospital, you are a professional, how can there be this
lack of principle, this lack of organizational discipline, this creating and spreading of false
rumours (谣)?" This is the original sentence. So I should go back to the 200-odd people
in the department to convey the news to them verbally, one by one; we can't send information by
WeChat or SMS, we can only talk face-to-face or call, we can't say anything about this
pneumonia, "you can't even tell your own husband", they said
I was utterly stunned. I hadn't been criticized for not working hard, but made to feel that
what I'd done had ruined Wuhan's prospects and its future. I felt strong depair. I am a serious
and hard-working person. I felt that everything I had done was in accordance with the rules and
well-founded. What did I do wrong? After I read the lab result, I had also reported it to the
hospital. My students and my colleagues had communicated among ourselves about how to handle
the condition of a patient, we hadn't given out any of the patient's personal information; this
is equivalent to discussing a medical case among medical students. As a clinical doctor, I
already knew that a very important virus had been found in patients. When other doctors asked,
how could you not say so? This is your instinct as a doctor, right? What did I do wrong? I have
done what a doctor and a person should normally do. I think anyone would do the same.
I was very emotional at the time, saying that I had done this, and it had nothing to do with
the rest of the people; you can just arrest me and jail me. I said that I was not suitable to
continue to work in this position, and I wanted to take a break. The leader did not agree,
saying that this was the time to test me.
I went home that night, I remember it quite clearly, I told my husband just after I walked
in the door, if something goes wrong, you must care for and raise the child -- because my
second treasure is still very young, only just over 1 year old. At the time, my husband was
perplexed by this. I didn't explain.
On January 20th, after Zhong Nanshan [prominent Chinese epidemiologist] told people [about
the epidemic], I told my husband what had happened that day. In the interim, I just warned my
family not to go to crowded places, and to wear surgical face masks when going out.
Peripheral departments
Many people worried that I was among the eight people who were admonished [by police]. In
fact, I wasn't warned by the Public Security Bureau. Later, a good friend asked me, are you a
whistleblower? I said that I am not a whistleblower, I am the one who sent the whistle.
But that disciplinary review hit me hard, it affected me very severely. When I came back, I
could see that everyone's morale had collapsed. We had been working with such drive and
dedication, and doing our jobs conscientiously. Everyone kept asking me questions, and I
couldn't answer.
All I could do was get the emergency department to focus on protection. We have over 200
people in the emergency department. From January 1st, I asked everyone to strengthen their
protection. Everyone must wear masks, hats, and use gloves (用手快消).
I remember one day, there was a nurse who did not wear a mask during the shift; I scolded him
then and there, saying "Don't come to work without a mask in the future".
On January 9th, while off-shift, I saw a patient coughing on the pre-examination table. From
that day on, I asked everyone to put a mask on both the patient and on anyone seeing the
patient, one for each person; I said, don't try to save money at this time. At the time, they
were still telling us that there was no human-to-human transmission, and I want to emphasize
here that wearing a mask to strengthen protection was a big issue.
That time was really depressing and very painful. Some doctors proposed wearing and out
layer of isolation clothing. The hospital's internal operations committee
(医院里开会) said they wouldn't allow it; they said that wearing
isolation clothing would cause panic. I asked the people in the department to wear an isolation
gown inside a white coat. This was out-of-specification and ridiculous.
We watched more and more patients arrive, as the radius of the infection area became larger
and larger. At first, they might be connected to the Huanan Seafood Market; then it spread, and
the radius became larger and larger. Many of the cases were family-transmitted. Among the first
seven people, there was a case of infection in which the mother had given the son food. The
clinic [dispensary? 诊所] boss got sick, infected by the patients who came for
injections. It was very serious, whether they got infected or not. I knew there must be
human-to-human transmission. If there was no human-to-human transmission, well, the Huanan
Seafood Market had been closed on January 1, so why were there more and more patients?
I often thought, if only they hadn't reprimanded me like that, if they'd asked for details
calmly, and then asked other respiratory experts to communicate with them, maybe the situation
would be better, and I could at least communicate a bit more in the hospital. If everyone had
been as alert on January 1, there would not be so many tragedies.
On the afternoon of January 3, in the Nanjing Road Hospital, doctors of urology gathered to
review the work of the senior director, 43-year-old Dr. Hu Weifeng (胡卫峰),
who is now in emergency care; on the afternoon of January 8, the Nanjing Road Hospital Director
[of thyroid and breast surgery] Jiang Xueqing (江学庆) also organized the
first Wuhan City breast disease patient recovery get-together
(武汉市甲乳患者康复联欢会),
on the 22nd floor. On the morning of January 11, the department reported to me that Hu Ziwei
(胡紫薇), a nurse in the emergency room of the emergency department, was
infected. She'd be the first infected nurse in the central hospital. First-off, I called the
Chief of the Medical Department to report it, and then the hospital held an emergency meeting.
At the meeting we were instructed to change the report of "double lung infection, viral
pneumonia?" to "scattered infection of both lungs"
("两下肺感染,病毒性肺炎?"
to "两肺散在感染"). At the weekly meeting of January 16th,
a deputy dean was still saying, "Everyone must have a little medical common sense, and certain
senior doctors should not go about scaring people." Another leader spoke, and continued,
"Human-to-human transmission is not possible; it can be prevented, treated and controlled." One
day later, on January 17, Jiang Xueqing was hospitalized, and 10 days later he was intubated
and put on ECMO.
The toll at the central hospital is so large, and it's connected to the lack of transparency
for our medical staff. If you look at the people who fell ill, the emergency department and the
respiratory department suffered less heavily, because we had a sense of the need for
protection, and we knew we should quickly rest and get treatment as soon as we got sick. The
worst cases are in the peripheral departments; Li Wenliang was an ophthalmologist, and Jiang
Xueqing is a nail specialist.
Jiang Xueqing was really a very good person, with excellent medical skills. He held one of
the two Chinese Physician Awards in the hospital. And yet we were neighbors, we were a unit;
I'm located on the 40th floor, he was on the 30th floor, our working relationship was very
good, but because I am too busy at work, I only met him during meetings and hospital
activities. He was a workaholic, always either in the operating room or at the clinic. No one
would go to tell him specifically, "Director Jiang, you have to pay attention and wear a mask".
He didn't have the time and energy to inquire about these things, and he must have brushed it
off with: "What's the matter? It's pneumonia." This was what people in that department told
me.
If these doctors had been warned in time, perhaps this day wouldn't have come. So that's
why, as one closely involved, I regret what I did. If I knew then what I know now, I wouldn't
have cared about the reprimand, I would have [expletive] spoken of it everywhere, to everyone,
wouldn't I?
Although I worked in the same hospital as Li Wenliang (李文亮) did before
he died, I didn't know him, because the hospital had over 4,000 people on staff and was usually
busy. The night before his death, the director of the ICU called me to borrow a cardiac press
(心脏按压器; CPR device?) from the emergency department, and said
it was Li Wenliang who was going to be resuscitated. The news shocked me. I do not understand
everything that happened to Li Wenliang, but could his condition have been affected by his
emotional state after being reprimanded? I have to ask, with my experience; I felt it
myself.
Later, when things got to this point, it proved that Li Wenliang was right. I can understand
his state of mind very easily. It could be my own. I don't feel excitement or happiness, but
regret. Regret that I didn't continue to shout out loudly at the beginning, when people
intervened and scolded us. I often find myself thinking, if only we could turn back time, and
do it right.
Just surviving is good
On the night before the city was shut down on January 23, a friend from the relevant
department called to ask me about the true situation of emergency patients in Wuhan. I said,
are you asking in a private or public capacity? He said, private. [I said,] I will tell you the
truth when I speak on my behalf: On January 21, our emergency department saw 1,523 patients,
three times as many as usual, of which 655 had fever.
The situation in the emergency department during that time will never be forgotten by those
who experienced it, it completely changes your outlook on life.
If this is a war, the emergency department is the front line. But at the time, the inpatient
wards were saturated, and basically none of the patients were accepted, and the ICU was
resolutely refused to accept them. They said that there were uninfected patients in them, and
they became contaminated as soon as they entered. More patients kept rushing in to the
emergency department, and the inpatient beds were not open, so they all piled up in the
emergency department. Patients queued for a few hours to see a doctor. We couldn't take any
time off work at all. There was no distinction between the fever clinic and the emergency
department. The hall was full of patients. The emergency room, the IV room, everywhere was
filled with patients.
Another patient's family came in, wanting a bed for their dad, who couldn't make it in from
the car, because the underground garage was closed at the time, and the car couldn't get in. I
couldn't do anything about that, but I ran to the car with people and equipment. I saw
immediately that he was already dead. What can you say, it's very difficult to bear. The man
died in the car, he didn't even get out of the car.
There was also an old man, his wife had just died at Jinyintan Hospital, her son and
daughter were infected, and she was given an IV, her son-in-law was caring for her. As soon as
I saw that she was very ill, I contacted the respiratory department to admit her to the
hospital. Her son-in-law was obviously a cultured person. He came over and wished to thank the
doctor and so on. As a result, she died. It only took a few seconds, but it was a delay of a
few seconds. That quick "thank you" weighs heavily on me.
And yet there were many people who sent their families to the ward
(监护室[; guardianship room]? in the sense of trustee), and that's the last
time you'l see them, you'll never see them again.
I remember when I came to work on the morning of the Chinese New Year [Friday, January 24,
2020]. I said that we'd take a picture to commemorate the New Year. I also sent it to a circle
of friends. No one wished anyone a happy new year that day. At the time, just surviving was
good.
In the past, if you made a small mistake, for example, if you didn't give an injection in
time, the patient might still be in trouble. Now there's no one, no one is to raise it with
you, no-one is going to take issue with it. Everyone's overwhelmed by the sudden onslaught, we
work blindly.
The patients died, and it was rare to see family members weeping and grieving, because there
were too many, too many. Some family members didn't say "Doctor, please save my family", but
said to the doctor, "Right, let's do this quickly"; it came to that. Everyone was afraid of
being infected.
The queue at the fever clinic was 5 hours long, every day. A woman waiting in line
collapsed, a woman in a leather coat, with a purse and high heels, very carefully dressed. A
middle-aged woman; no one dared to step forward to help her, and she lay on the ground for a
long time. I had to call the nurse and doctor to help her.
On the morning of January 30, I came to work. The son of a white-haired old man had died at
the age of 32. He stared blankly at the doctor giving him the death certificate. There are no
tears at all, how can one cry? There's no way to cry. From the style of his clothing, the old
man might be a rural migrant worker, there's no way to be sure. Without a diagnosis, his son
became a death certificate.
This is what I want to call for. The patients who died in the emergency department were all
undiagnosed, and their causes of death could not be confirmed. After this epidemic has passed,
I hope to give an explanation and give their families some comfort. Our patients wake
compassion, a great deal of compassion.
"Lucky"
Having been a doctor for so many years, I always felt that no difficulty could overwhelm me,
not with my experience and personality.
When I was nine, my father died of gastric cancer. At that time, I thought of growing up to
be a doctor, to save the lives of others. Later, when I did my the college entrance
examination, all my preferences were in medicine, and I finally got to go to Tongji Medical
College. After graduating from medical college in 1997, I went to the Central Hospital. I
previously worked in cardiovascular medicine, and I became the director of the emergency
department in 2010.
I feel the emergency department is one of my children. I built it up, I nurtured a
tight-knit group, which really doesn't make this situation easier, but it's what makes this
group such a treasure; I really cherish this team.
A few days ago, one of my nurses sent a message to a friends group saying "I really miss the
old big busy emergency department"; that kind of busy and this kind of busy are totally
different concepts.
Before this epidemic hit, our emergency department dealt with myocardial infarctions,
cerebral infarctions, gastrointestinal bleeding, trauma and so on. That kind of busy gives a
sense of accomplishment, it has a clear purpose, there's a smooth flow of procedures for all
the various types of patients. There are very mature procedures, there's not a single wasted
step, what to do next is not a problem. But in this time there were so many critically ill
patients whom we had no way to deal with and who couldn't be admitted to hospital, and our
medical staff was still at risk. This kind of busyness is desperate, it's deeply
distressing.
One day at 8 in the morning, a young doctor in our department sent me a WeChat, and it was
quite personal, saying they wouldn't come to work that day, not well. Since what we do here, if
someone is not well, they need to tell me about it in advance; if they tell me at 8 o'clock,
where do I go to find someone? The doctor lost their temper with me in WeChat, and said that a
large number of highly suspect cases were put back into the community by the emergency
department I led. We understand that this is sin! I understand this person, because this is a
doctor's professional ethics, but I was also anxious, and I said you can denounce me, but tell
me, what would you do if you were the director of the emergency department?
Later, the doctor came back to work after a few days of rest. The doctor didn't say that
they feared death or feared harm; no, they were affected the conditions; suddenly having to
deal with so many patients at once, they felt utterly overwhelmed.
And the work of the medics, especially for the many medics who came to support us, it was
psychologically unbearable. There were doctors and nurses in tears. Some were crying for
others, others were crying for themselves, because no-one knows when it will be their turn to
become infected.
Around mid-to-late January, the hospital's leaders also became ill, one after another,
including our director of the office and three vice-presidents. The daughter of the Chief of
Medical Services was also ill and resting at home. So basically there was no administration or
management; you just had to fight there, that was the feeling.
The people around me also started to come down with it one by one. On January 18, at 8:30 in
the morning, our first doctor collapsed, saying "I caught it just like the director did", no
fever, did a CT first off, and the lungs had a lump of ground-glass opacification
(坨磨玻璃). Not long after, the duty nurse in charge of the isolation
ward told me they'd fallen ill. That night, our head nurse fell ill. My very real first feeling
at that time was -- good luck, because falling ill early, you could get off the battlefield for
a little bit.
I've been in close contact with these three people. I just work every day with the belief
that I must fall ill. Everyone in the hospital thought I was a miracle. I've thought about it
myself, perhaps it's because I have asthma and I'm using some inhaled hormones, perhaps it
inhibits the deposition of these viruses in the lungs.
I've always felt that the people who work in the emergency department have feelings, too. In
Chinese hospitals, the status of the emergency department is relatively low among the
departments, because everyone thinks that the emergency department is nothing more than a route
into the hospital, it just needs to admit patients. During this epidemic, this sort of neglect
has always been present.
In the early days, they're weren't enough supplies. Sometimes the quality of the protective
clothing assigned to the emergency department was very poor. I was angry when I saw that our
nurses wore such clothes to work and spoke up about it in Zhouhui Qun [a WeChat group for MDs
in that hospital]. After that, many directors gave me all the protective clothing they kept in
their departments.
There were also problems with food. When there are many patients, the management gets
confused. They simply can't think that the emergency department still has to have something to
eat. Many departments had food and drink after shift changeover, they had a big spread, and
here, we had nothing. In the fever clinic's WeChat group, doctors complained: "Our emergency
department has only disposable diapers " We were the front-line response, and we had to deal
with that sort of thing, sometimes it made me really angry.
Our team is really good. Everyone held the line, they were only off work when they were
sick. More than 40 people in our emergency department were infected. I built a group of all the
sick people, originally called the "Emergency Department Sick
Group"(急诊生病群); the head nurse said that was unlucky, and
changed it to "Emergency Department Re-energizing Group"
(急诊加油群). Even the people who are sick weren't thinking in
terms of despair or blame. They were all very positive, that is, everyone had the attitude that
we needed to help one another to get thorough the crisis together.
These kids, these young people are very good, it's just that they, like me, have to live
with feeling slighted. I hope that after this epidemic, the country will also increase its
investment in emergency departments. In many countries' medical systems, the emergency
department is highly valued.
Unattainable happiness
On February 17th, I received a WeChat message from the old classmate at Tongji Hospital. He
said "Sorry" to me. I said: it's fortunate that you passed the message on and warned some
people in time. If he hadn't passed it on, they might not have Li Wenliang and the eight
others, but people would probably know less.
This time, we had the entire families of three female doctors get infected. Two female
doctors had their father-in-law and mother-in-law infected, and their husbands, and another had
her father, mother, sister, and husband infected, and five close relatives. Everyone thinks
that the virus was discovered so early on, and yet this is the result, it caused us such great
loss, took such a terrible toll.
It took this toll in many different ways, too. In addition to those who died, those who were
sick also suffered.
In our "Emergency Department Re-energizing group", people often exchange physical
conditions. Some people ask: a heart rate that's always 120 beats per minute, does it matter?
Surely it matters, they panic as soon as they move. This will affect them for life, and is
heart failure likely? It's hard to say. In the future, others will be able to go hiking and
traveling, and they might not be able to, all that is possible.
And Wuhan. You said that our Wuhan is a lively place; now it's very, very quiet on the
streets. Many things can't be bought and we have to support the whole country. A few days ago,
a nurse of a medical team in Guangxi suddenly fell into a coma while at work, and was
resucitated. Her heart restarted, but she is still in a coma. If she hadn't come to work, she
could have had a good time at home, and this kind of thing wouldn't have happened. So, I think
we owe everyone, really.
Having been through this epidemic, many people in the hospital have been hit hard. Several
medical staff below me have thoughts of resignation, including some backbones of the
department. Everyone's previous ideas, all the things everyone knows about this profession,
they're are inevitably a little shaken -- it's that you work so hard, isn't it? Just like Jiang
Xueqing, he worked too hard, he was too good to the patients, he was doing surgery every year
during [Chinese] New Year. Today, someone sent a WeChat written by Jiang Xueqing's daughter,
saying that her father's time was all given to his patients.
Myself, I've had countless thoughts of going back home to be a housewife. After the epidemic
began, I basically didn't go home, I lived separately from my husband. My sister helped take
care of my children at home. My second treasure didn't recognize me, didn't react to me when he
saw me on video. I felt very lost. It wasn't easy for me to give birth to this second child. He
was 10 kg at birth. I had to wean him abruptly -- when I made that decision, that was hard for
me to do. My husband told me that these things happen in life, and you're not only a
participant, you're also choosing to lead the team to fight this epidemic; that's also a very
meaningful act, and when everything returns to normal for everyone, then you'll remember; it's
a valuable experience to have had.
The leader (领导) talked to me on the morning of February 21st. Actually, I
would have liked to ask a few questions, such as, do you think that that criticism was wrong
that day? I hoped to be given an apology. But I dared not ask. No one said sorry to me on any
occasion. I still feel that these events are an even clearer demonstation of why each person
should stick to their own independent ideas, regardless, because if someone wants to stand up
and tell the truth, there must be someone, and the world must hear a dissenting voice,
right?
I'm Wuhanese, who doesn't love their own city? Now we remember what extravagant happiness we
enjoyed in the most ordinary life. I now feel that holding the baby, going out to play with him
on a slide, or going out to watch a movie with my husband, even things we never did all that
often in the past, they are now all a kind of happiness, an unattainable happiness.
Highly recommended !Ideologically COVID-19 is another nail in the coffin of neoliberalism.
bevin , Apr 10 2020 23:06 utc |
92
Diane Johnstone gets it right:
"...Today, quite a number of alternative media commentators are ready to believe in the
absolute power not of God but of Mammon, of the powers of Wall Street and its partners in
politics, the media and the military. In this view, nothing major happens that hasn't been
planned by earthly powers for their own selfish interest.
"Mammon is wrecking the economy so a few oligarchs will own everything. Or else Mammon
created the hoax Coronavirus 19 in order to lock us all up and deprive us of what little is
left of our freedom. Or finally Mammon is using a virus in order to have a pretext to
vaccinate us all with secret substances and turn us all into zombies.
"Is this credible? In one sense, it is. We know that Mammon is unscrupulous, morally
capable of all crimes. But things do happen that Mammon did not plan, such as earthquakes,
floods and plagues. Dislike of our ruling class combined with dislike of being locked up
leads to the equation: They are simply using this (fake) crisis in order to lock us up!
"But what for? To whom is there any advantage in locking down the population? For the
pleasure of telling themselves, "Aha, we've got them where we want them, all stuck at home!"
Is this intended to suppress popular revolt? What popular revolt? Why repress people who
aren't doing anything that needs to be repressed?...
"What is the use of locking up a population – and I think especially of the United
States – that is disunited, disorganized, profoundly confused by generations of
ideological indoctrination telling them that their country is "the best" in every way, and
thus unable to formulate coherent demands on a system that exploits them ruthlessly? Do you
need to lock up your faithful Labrador so he won't bite you?...
"....Mammon is blinded by its own hubris, often stupid, incompetent, dumbed down by
getting away with so much so easily. Take a look at Mike Pompeo or Mike Pence – are
these all-powerful geniuses? No, they are semi-morons who have been able to crawl up a
corrupt system contemptuous of truth, virtue or intelligence – like the rest of the
gangsters in power in a system devoid of any ethical or intellectual standards.
"The power of creatures like that is merely the reflection of the abdication of social
responsibility by whole populations whose disinterest in politics has allowed the scum to
rise to the top.
The lockdown decreed by our Western governments reveals helplessness rather than power.
They did not rush to lock us down. The lockdown is disastrous for the economy which is their
prime concern. They hesitated and did so only when they had to do something and were
ill-equipped to do anything else. They saw that China had done so with good results. But
smart Asian governments did even more, deploying masks, tests and treatments Western
governments did not possess..."
https://consortiumnews.com/2020/04/10/covid-19-coronavirus-and-civilization/
Highly recommended !Notable quotes:
"... Because behind today's coronavirus-inspired astonishment at conditions in developing or lower income countries, and Trump's authoritarian-like thuggery, lies an actual military and political hegemon with an actual impact on the world; particularly on what was once called the "Third World." ..."
"... In physical terms, the U.S.'s military hegemony is comprised of 800 bases in over 70 nations – more bases than any other nation or empire in history. The U.S. maintains drone bases, listening posts, "black sites," aircraft carriers, a massive nuclear stockpile, and military personnel working in approximately 160 countries. ..."
"... Since then, the United States has overthrown or attempted to overthrow the governments of approximately 50 countries, many of which (e.g. Iran, Guatemala, the Congo, and Chile) had elected leaders willing to nationalize their natural resources and industries. Often these interventions took the form of covert operations. Less frequently, the United States went to war to achieve these same ends (e.g. Korea, Vietnam, and Iraq). ..."
"... In fiscal terms, maintaining American hegemony requires spending more on "defense" than the next seven largest countries combined. Our nearly $1 trillion security budget now amounts to about 15 percent of the federal budget and over half of all discretionary spending. Moreover, the U.S. security budget continues to increase despite the Pentagon's inability to pass a fiscal audit. ..."
This March, as COVID-19's capacity to overwhelm the American healthcare system was becoming
obvious, experts marveled at the scenario unfolding before their eyes. "We have Third World
countries who are better equipped than we are now in Seattle,"
noted one healthcare professional, her words echoed just a few days later by a shocked
doctor in New York who described
"a third-world country type of scenario." Donald Trump could similarly only grasp what was
happening through the same comparison. "I have seen things that I've never seen before," he
said
. "I mean I've seen them, but I've seen them on television and faraway lands, never in my
country."
At the same time, regardless of the fact that "Third World" terminology is outdated and
confusing, Trump's inept handling of the pandemic has itself elicited more than one "banana republic"
analogy, reflecting already well-worn, bipartisan comparisons of Trump to a "
third world dictator " (never mind that dictators and authoritarians have never been
confined solely to lower income countries).
And yet, while such comparisons provoke predictably nativist outrage from the right, what is
absent from any of
these responses to the situation is a sense of reflection or humility about the "Third
World" comparison itself. The doctor in New York who finds himself caught in a "third world"
scenario and the political commentators outraged when Trump behaves "like a third world
dictator" uniformly express themselves in terms of incredulous wonderment. One never hears the
potential second half of this comparison: "I am now experiencing what it is like to live in a
country that resembles the kind of nation upon whom the United States regularly imposes broken
economies and corrupt leaders."
Because behind today's coronavirus-inspired astonishment at conditions in developing or
lower income countries, and Trump's authoritarian-like thuggery, lies an actual military and
political hegemon with an actual impact on the world; particularly on what was once called the
"Third World."
In physical terms, the U.S.'s military hegemony is comprised of 800 bases in over 70
nations –
more bases than any other nation or empire in history. The U.S. maintains drone bases,
listening posts, "black sites," aircraft carriers, a massive nuclear stockpile, and military
personnel working in approximately 160 countries. This is a globe-spanning military and
security apparatus organized into regional commands
that resemble the "proconsuls of the Roman empire and the governors-general of the
British." In other words, this apparatus is built not for deterrence, but for primacy.
The U.S.'s global primacy emerged from the wreckage of World War II when the United States
stepped into the shoes vacated by European empires. Throughout the Cold War, and in the name of
supporting "free peoples," the sprawling American security apparatus helped ensure that 300
years of imperial resource extraction and wealth distribution – from what was then called
the Third World to the First – remained undisturbed, despite decolonization.
Since then, the United States
has overthrown or attempted to overthrow the governments of approximately 50 countries,
many of which (e.g. Iran, Guatemala, the Congo, and Chile) had elected leaders willing to
nationalize their natural resources and industries. Often these interventions
took the form of covert operations. Less frequently, the United States went to war to
achieve these same ends (e.g. Korea, Vietnam, and Iraq).
In fiscal terms, maintaining American hegemony requires spending more
on "defense" than the next seven largest countries combined. Our
nearly $1 trillion security budget now amounts to about 15 percent of the federal budget
and over half of all
discretionary spending. Moreover, the U.S. security budget continues to increase despite the
Pentagon's inability to pass a fiscal audit.
Trump's claim that Obama had
"hollowed out" defense spending was not only grossly untrue, it masked the consistency of the
security budget's metastasizing growth since the Vietnam War, regardless of who sits in the
White House. At $738 billion dollars, Trump's security budget was passed in December with the
overwhelming support of House Democrats.
And yet, from the perspective of public discourse in this country, our globe-spanning,
resource-draining military and security apparatus exists in an entirely parallel universe to
the one most Americans experience on a daily level. Occasionally, we wake up to the idea of
this parallel universe but only when the United States is involved in visible military actions.
The rest of the time, Americans leave thinking about international politics – and the
deaths, for instance, of 2.5 million
Iraqis since 2003 – to the legions of policy analysts and Pentagon employees who
largely accept American military primacy as an "article of faith," as Professor of
International Security and Strategy at the University of Birmingham Patrick Porter has said
.
Foreign policy is routinely the last issue Americans consider when they vote for presidents
even though the president has more discretionary power over foreign policy than any other area
of American politics. Thus, despite its size, impact, and expense, the world's military hegemon
exists somewhere on the periphery of most Americans' self-understanding, as though, like the
sun, it can't be looked upon directly for fear of blindness.
Why is our avoidance of the U.S.'s weighty impact on the world a problem in the midst of the
coronavirus pandemic? Most obviously, the fact that our massive security budget has gone so
long without being widely questioned means that one of the soundest courses of action for the
U.S. during this crisis remains resolutely out of sight.
The shock of discovering that our healthcare system is so quickly overwhelmed should
automatically trigger broader conversations about spending priorities that entail deep and
sustained cuts in an engorged security budget whose sole purpose is the maintenance of primacy.
And yet, not only has this not happened, $10.5 billion of the coronavirus aid package has been
earmarked for the Pentagon, with $2.4 billion of that
channeled to the "defense industrial base." Of the $500 billion aimed at corporate America,
$17.5 billion is
set aside "for businesses critical to maintaining national security" such as aerospace.
To make matters worse, our blindness to this bloated security complex makes it frighteningly
easy for champions of American primacy to sound the alarm when they even suspect a dip in
funding might be forthcoming. Indeed, before most of us had even glanced at the details of the
coronavirus bill, foreign policy hawks were already
issuing dark prediction s about the impact of still-imaginary cuts in the security budget
on the U.S.'s "ability to strike any target on the planet in response to hostile actions by any
actor" – as if that ability already did not exist many times over.
On a more existential level, a country that is collectively engaged in unseeing its own
global power cannot help but fail to make connections between that power and domestic politics,
particularly when a little of the outside world seeps in. For instance, because most Americans
are unaware of their government's sponsorship of fundamentalist Islamic groups in the Middle
East throughout the Cold War, 9/11 can only ever appear to have come from nowhere, or because
Muslims hate our way of life.
This "how did we get here?" attitude replicates itself at every level of political life
making it profoundly difficult for Americans to see the impact of their nation on the rest of
the world, and the blowback from that impact on the United States itself. Right now, the
outsized influence of American foreign policy is already encouraging the spread of coronavirus
itself as U.S. imposed sanctions on Iran severely hamper that
country's ability to respond to the virus at home and virtually
guarantee its spread throughout the region.
Closer to home, our shock at the healthcare system's inept response to the pandemic masks
the relationship between the U.S.'s imposition
of free-market totalitarianism on countries throughout the
Global South and the impact of free-market totalitarianism on our own welfare state .
Likewise, it is more than karmic comeuppance that the President of the United States now
resembles the self-serving authoritarians the U.S. forced on so many formerly colonized
nations. The modes of militarized policing American security experts exported to those
authoritarian regimes also contributed , on a
policy level, to both the rise of militarized policing in American cities and the rise of mass
incarceration in the 1980s and 90s. Both of these phenomena played a significant role in
radicalizing Trump's white nationalist base and decreasing their tolerance for democracy.
Most importantly, because the U.S. is blind to its power abroad, it cannot help but turn
that blindness on itself. This means that even during a pandemic when America's exceptionalism
– our lack of national healthcare – has profoundly negative consequences on the
population, the idea of looking to the rest of the world for solutions remains unthinkable.
Senator Bernie Sanders' reasonable suggestion that the U.S., like Denmark, should
nationalize its healthcare system is dismissed as the fanciful pipe dream of an aging socialist
rather than an obvious solution to a human problem embraced by nearly every other nation in the
world. The Seattle healthcare professional who expressed shock that even "Third World
countries" are "better equipped" than we are to confront COVID-19 betrays a stunning ignorance
of the diversity of healthcare systems within developing countries. Cuba, for instance,
has responded
to this crisis with an efficiency and humanity that puts the U.S. to shame.
Indeed, the U.S. is only beginning to feel the full impact of COVID-19's explosive
confrontation with our exceptionalism: if the unemployment rate really does reach 32 percent,
as has been predicted,
millions of people will not only lose their jobs but their health insurance as well. In the
middle of a pandemic.
Over 150 years apart, political commentators Edmund Burke and Aimé Césaire
referred to this blindness as the byproduct of imperialism. Both used the exact same language
to describe it; as a "gangrene" that "poisons" the colonizing body politic. From their
different historical perspectives, Burke and Césaire observed how colonization
boomerangs back on colonial society itself, causing irreversible damage to nations that
consider themselves humane and enlightened, drawing them deeper into denial and
self-delusion.
Perhaps right now there is a chance that COVID-19 – an actual, not metaphorical
contagion – can have the opposite effect on the U.S. by opening our eyes to the things
that go unseen. Perhaps the shock of recognizing the U.S. itself is less developed than our
imagined "Third World" might prompt Americans to tear our eyes away from ourselves and look
toward the actual world outside our borders for examples of the kinds of political, economic,
and social solidarity necessary to fight the spread of Coronavirus. And perhaps moving beyond
shock and incredulity to genuine recognition and empathy with people whose economies and
democracies have been decimated by American hegemony might begin the process of reckoning with
the costs of that hegemony, not just in "faraway lands" but at home. In our country.
Highly recommended !Tucker comments on Fauci above face with estimating the number of deaths: first around 3
million, not less then 60K.
Hospitals are staying half empty. So much for Fauci flattening the curve efforts
Mike
Jordan 14 hours
ago
Being "connected" is a huge part of the cause of this mess, before internet propaganda was
limited to newspapers and magazines, it was much slower and manageable.
Don Nix 9 hours
ago
I do find it funny how wealthy folks spread the "don't worry WE will all be fine" garbage.
WE....no, tell that to someone who has lost their business and has dependents.
Karel Moulík 10 hours
ago
When everything can be solved by propaganda it's time for revolution.
Massive-Headwound Harry 12 hours
ago
I hate the "We're going to be ok. We're all in this together" ads. All of them
celebrities, pro athletes, and actors. Not one has to worry about whether they'll be able to
buy food next week. Elites telling the little people everything's ok.
Joe Shaloom 14 hours
ago
It's really sad when Tucker Carlson is the only person who ever admitted he was wrong on
Fox News. Hannity still claims he never called the virus a hoax even though he did it on
TV.
Highly recommended !
juliania , Apr 8 2020 15:04 utc |
37
My daughter who is a hospital worker showed me her mask, made by her sister. And b has posted
previously directions for making masks.
While homemade or even professional surgical mask do not protect the wearer from all
particles they do protect one much better from them than when one wears no mask at all.
A person rarely gets infected by just one virus particle. They come in millions attached
to tiny droplets. We do not know yet how the dose of the novel coronavirus that infects a
person affects the intensity of the disease. But we do know from other viruses that the
dose matters. People who catch a higher dose of viruses will usually have a more intense
disease. A mask can lower the virus load the wearer may receive.
One can
improvise a mask from simple household objects. One can sew a mask like a surgeon
does in this video .
This is my preferred model which is officially recommended by German fire departments.
(The pdf is in German but the pictures tell the story). This is the mask I made by
following those instructions.
bigger
It is made of a folded sheet cut from a triangular arm-sling out of an old first-aid
kit. A HEPA microfilter (as used in a vacuum cleaners) is in between the folded sheet. A
piece cut from a clean bag for vacuum cleaners will do as well. Do not use a sheet or
insert that is too tight to breathe through. If one does that the air will come in from the
sides of the mask and the total protection effect will be less. It can be arduous to
breathe through such a mask. If you have breathing problems leave the insert out. The
sheets alone are already good protection. There is a piece of wire from a big paper clip
fixed inside the middle of the upper seam to fit the mask tightly around the upper nose.
The lower part goes under the chin. I shaved my beard to make it a tighter fit. As I had no
sewing equipment I used a stapler to fix the seams and the ribbons.
The HEPA filter catches
particles down to 0.3 micrometer. Viruses are some 125 nanometer in diameter so they are
smaller and could slip through. But the viruses are attached to some droplet that are
bigger. HEPA filter are essentially labyrinths of small fiber and the viruses would have to
bounce multiple times to get through. Finally the dose also matters.
To clean the mask of potential viruses I put it into the oven for 30 minutes at 70C
(158F).
The science says that masks work. Everyone should use one. #MaskUp!
The advantage is you can throw them in the washing machine to clean, or even hand wash as
they are small items.
The masks in question here, surgical ones, being only meant to protect the patient from
the practitioner, seem somewhat flawed in any case.
Better to make better ones; let the Israelis have those not so good ones. A great gift
from a family member to their hardworking sibling.
There ought to be an industrial production plant producing the cloth masks with disposable
inserts - how about taking over a diaper factory - a lot of folk still use the cloth ones -
have such been totally outsourced? (I'd make 'em deluxe, organic cotton only! But for us home
bodies, an old sheet well washed, suitably patterned is better than nothing at all.)
Highly recommended !
utu April 3, 2020 at
10:45 pm GMT
@Dreadilk By
wearing a mask you reduce the probability of getting infected by x while a mask on an
infected person reduces the probability of infecting another person by y and
y>x (I can't formally prove this inequality at this point but it is intuitively
obvious to me.). Since you do not know whether you are infected or not by wearing a mask you
are protecting other more than yourself on average. This is a rare case when a selfish motive
to save your own life produce a greater good. Not wearing a mask would be an inverse-altruism
where you are willing to sacrifice yourself for an idea of killing others , i.e., doing what
a suicide bombers do who are aware of y>x calculus.
Highly recommended !
Science has tried to interview George Gao, director-general of the Chinese
Center for Disease Control and Prevention (CDC), for 2 months. Last week he responded.
Q : What mistakes are other countries making?
A: The big mistake in the U.S. and Europe, in my opinion, is that people aren't wearing
masks. This virus is transmitted by droplets and close contact. Droplets play a very important
role -- you've got to wear a mask, because when you speak, there are always droplets coming out
of your mouth. Many people have asymptomatic or presymptomatic infections. If they are wearing
face masks, it can prevent droplets that carry the virus from escaping and infecting others. Q:
People who tested positive in Wuhan but only had mild disease were sent into isolation in large
facilities and were not allowed to have visits from family. Is this something other countries
should consider?
A: Infected people must be isolated. That should happen everywhere. You can only control
COVID-19 if you can remove the source of the infection. This is why we built module hospitals
and transformed stadiums into hospitals.
Highly recommended !Jokes aside, infection on family settings might lead to more severe outcomes, as virus load is higher.
In this sense, COVID-19 behaves a lot like seasonal flu. Common rooms often mean common
pathogens and higher dose of virus then from strangers. There are some indications that the
doze of virus that you get affects the severity of the disease.
Families are great places for socialization and provide a means to stay active and engaged,
but can serve as pathogenic petri dishes
Based on current research, it takes about 2 weeks between the onset of symptoms to the
clinical recovery of patients with a mild form of the disease
Highly recommended !
On April 21, 2011, the region of Amazon Web Services covering eastern North America crashed.
The crash brought down the sites of large customers such as Quora, Foursquare, and Reddit. It
took Amazon over a week to bring its system fully back online, and some customer data was lost
permanently.
But one company whose site did not crash was Netflix. It turns out that Netflix had made
themselves "antifragile" by employing software they called "Chaos Monkey," which regularly and
randomly brought down Netflix servers. By continually crashing their own servers, Netflix
learned how to nevertheless keep other portions of their network running. And so when Amazon
US-East crashed, Netflix ran on, unfazed.
This phenomenon is discussed by Nassim Taleb in his book Antifragile : a system that
depends on the absence of change is fragile. The companies that focused on keeping all of their
servers up and running all the time went completely offline when Amazon crashed from under
them. But the company that had exposed itself to lots of little crashes could handle the big
crash. That is because the minor, "undesirable" changes stress the system in a way that can
make it stronger.
The idea of antifragility does not apply only to computer networks. For instance, by trying
to eliminate minor downturns in the economy, central bank policy can make that economy
extremely vulnerable to a major recession. Running only on treadmills or tracks makes the
joints extremely vulnerable when, say, one steps in a pothole in the sidewalk.
What does this have to do with trade policy? For many reasons, such as the recent
coronavirus outbreak, flows of goods are subject to unexpected shocks.
Both a regime of "unfettered" free trade, and its opposite, that of complete autarchy, are
fragile in the face of such shocks. A trade policy aimed not at complete free trade or
protectionism, but at making an economy better at absorbing and adapting to rapid change, is
more sane and salutary than either extreme. Furthermore, we suggest practicing for shocks can
help make an economy antifragile.
Amongst academic economists, the pure free-trade position is more popular. The case for
international trade, absent the artificial interference of government trade policy, is
generally based upon the "principle of comparative advantage," first formulated by the English
economist David Ricardo in the early 19th century. Ricardo pointed out, quite correctly, that
even if, among two potential trading partners looking to trade a pair of goods, one of them is
better at producing both of them, there still exist potential gains from trade -- so long as
one of them is relatively better at producing one of the goods, and the other (as a
consequence of this condition) relatively better at producing the other. For example,
Lebron James may be better than his local house painter at playing basketball, and at
painting houses, given his extreme athleticism and long reach. But he is so much more "better"
at basketball that it can still make sense for him to concentrate on basketball and pay the
painter to paint his house.
And so, per Ricardo, it is among nations: even if, say, Sweden can produce both cars and
wool sweaters more efficiently than Scotland, if Scotland is relatively less bad at
producing sweaters than cars, it still makes sense for Scotland to produce only wool sweaters,
and trade with Sweden for the cars it needs.
When we take comparative advantage to its logical conclusion at the global scale, it
suggests that each agent (say, nation) should focus on one major industry domestically and that
no two agents should specialize in the same industry. To do so would be to sacrifice the
supposed advantage of sourcing from the agent who is best positioned to produce a particular
good, with no gain for anyone.
Good so far, but Ricardo's case contains two critical hidden assumptions: first, that the
prices of the goods in question will remain more or less stable in the global marketplace, and
second that the availability of imported goods from specialized producers will remain
uninterrupted, such that sacrificing local capabilities for cheaper foreign alternatives.
So what happens in Scotland if the Swedes suddenly go crazy for yak hair sweaters (produced
in Tibet) and are no longer interested in Scottish sweaters at all? The price of those sweaters
crashes, and Scotland now finds itself with most of its productive capacity specialized in
making a product that can only be sold at a loss.
Or what transpires if Scotland is no longer able, for whatever reason, to produce sweaters,
but the Swedes need sweaters to keep warm? Swedes were perhaps once able to make their own
sweaters, but have since funneled all their resources into making cars, and have even lost the
knowledge of sweater-making. Now to keep warm, the Swedes have to rapidly build the
infrastructure and workforce needed to make sweaters, and regain the knowledge of how to do so,
as the Scots had not only been their sweater supplier, but the only global sweater
supplier.
So we see that the case for extreme specialization, based on a first-order understanding of
comparative advantage, collapses when faced with a second-order effect of a dramatic change in
relative prices or conditions of supply.
That all may sound very theoretical, but collapses due to over-specialization, prompted by
international agencies advising developing economies based on naive comparative-advantage
analysis, have happened all too often. For instance, a number of African economies, persuaded
to base their entire economy on a single good in which they had a comparative advantage (e.g,
gold, cocoa, oil, or bauxite), saw their economies crash when the price of that commodity fell.
People who had formerly been largely self-sufficient found themselves wage laborers for
multinationals in good times, and dependents on foreign charity during bad times.
While the case for extreme specialization in production collapses merely by letting prices
vary, it gets even worse for the "just specialize in the single thing you do best" folks once
we add in considerations of pandemics, wars, extreme climate change, and other such shocks. We
have just witnessed how relying on China for such a high percentage of our medical supplies and
manufacturing has proven unwise when faced with an epidemic originating in China.
On a smaller scale, the great urban theorist Jane Jacobs stressed the need for economic
diversity in a city if it is to flourish. Detroit's over-reliance on the automobile industry,
and its subsequent collapse when that industry largely deserted it, is a prominent example of
Jacobs' point. And while Detroit is perhaps the most famous example of a city collapsing due to
over-specialization, it is far from
the only one .
All of this suggests that trade policy, at any level, should have, as its primary goal, the
encouragement of diversity in that level's economic activity. To embrace the extremes of "pure
free trade" or "total self-sufficiency" is to become more susceptible to catastrophe from
changing conditions. A region that can produce only a few goods is fragile in the face of an
event, like the coronavirus, that disrupts the flow of outside goods. On the other hand,
turning completely inward, and cutting the region off from the outside, leaves it without
outside help when confronting a local disaster, like an extreme drought.
To be resilient as a social entity, whether a nation, region, city, or family, will have a
diverse mix of internal and external resources it can draw upon for sustenance. Even for an
individual, total specialization and complete autarchy are both bad bets. If your only skill is
repairing Sony Walkmen, you were probably pretty busy in 2000, but by today you likely don't
have much work. Complete individual autarchy isn't ever really even attempted: if you watch
YouTube videos of supposedly "self-reliant" people in the wilderness, you will find them using
axes, radios, saws, solar panels, pots and pans, shirts, shoes, tents, and many more goods
produced by others.
In the technical literature, having such diversity at multiple scales is referred to as
"multiscale variety." In a system that displays multiscale variety, no single scale accounts
for all of the diversity of behavior in the system. The practical importance of this is related
to the fact that shocks themselves come at different scales. Some shocks might be limited to a
town or a region, for instance local weather events, while others can be much more widespread,
such as the coronavirus pandemic we are currently facing.
A system with multiscale variety is able to respond to shocks at the scale at which they
occur: if one region experiences a drought while a neighboring region does not, agricultural
supplementation from the currently abundant region can be leveraged. At a smaller scale, if one
field of potatoes becomes infested with a pest, while the adjacent cows in pasture are spared,
the family who owns the farm will still be able to feed themselves and supply products to the
market.
Understanding this, the question becomes how can trade policy, conceived broadly, promote
the necessary variety and resiliency to mitigate and thrive in the face of the unexpected?
Crucially, we should learn from the tech companies: practice disconnecting, and do it randomly.
In our view there are two important components to the intentional disruption: (1) it is regular
enough to generate "muscle memory" type responses; and (2) it is random enough that responses
are not "overfit" to particular scenarios.
For an individual or family, implementing such a policy might create some hardships, but
there are few institutional barriers to doing so. One week, simply declare, "Let's pretend all
of the grocery stores are empty, and try getting by only on what we can produce in the yard or
have stockpiled in our house!" On another occasion, perhaps, see if you can keep your house
warm for a few days without input from utility companies.
Businesses are also largely free of institutional barriers to practicing disconnecting. A
company can simply say, "We are awfully dependent on supplier X: this week, we are not going to
order from them, and let's see what we can do instead!" A business can also seek out external
alternatives to over-reliance on crucial internal resources: for instance, if your top tech guy
can hold your business hostage, it is a good idea to find an outside consulting firm that could
potentially fill his role.
When we get up to the scale of the nation, things become (at least institutionally)
trickier. If Freedonia suddenly bans the import of goods from Ruritania, even for a week,
Ruritania is likely to regard this as a "trade war," and may very well go to the WTO and seek
relief. However, the point of this reorientation of trade policy is not to promote hostility to
other countries, but to make one's own country more resilient. A possible solution to this
problem is that a national government could periodically, at random times, buy all of the
imports of some good from some other country, and stockpile them. Then the foreign supplier
would have no cause for complaint: its goods are still being purchased! But domestic
manufacturers would have to learn to adjust to a disappearance of the supply of palm oil from
Indonesia, or tin from China, or oil from Norway.
Critics will complain that such government management of trade flows, even with the noble
aim of rendering an economy antifragile, will inevitably be turned to less pure purposes, like
protecting politically powerful industrialists. But so what? It is not as though the pursuit of
free trade hasn't itself yielded perverse outcomes, such as the NAFTA trade agreement that ran
to over one thousand pages. Any good aim is likely to suffer diversion as it passes
through the rough-and-tumble of political reality. Thus, we might as well set our sites on an
ideal policy, even though it won't be perfectly realized.
We must learn to deal with disruptions when success is not critical to survival. The better
we become at responding to unexpected shocks, the lower the cost will be each time we face an
event beyond our control that demands an adaptive response. To wait until adaptation is
necessary makes us fragile when a real crisis appears. We should begin to develop an
antifragile economy today, by causing our own disruptions and learning to overcome them.
Deliberately disrupting our own economy may sound crazy. But then, so did deliberately crashing
one's own servers, until Chaos Monkey proved that it works.
Gene Callahan teaches at the Tandon School of Engineering at New York University. Joe
Norman is a data scientist and researcher at the New England Complex Systems Institute.
My Gana
20 hours ago
Most disruptive force is own demographic change of which govts have known for decades.
Caronovirus challenge is nothing compared to what will happen because US ed system
discriminated against the poor who will be the majority!
PierrePaul
12 hours ago
What Winston Churchill once said about the Americans is in fact true of all humans: "Americans
always end up doing
...On Saturday, a new term caught the internet by storm, that is,
'Covidiot' – and first defined on Urban Dictionary ,
with the top definition:
"Someone who ignores the warnings regarding public health or safety. A person who hoards
goods, denying them from their neighbors."
Notable quotes:
"... Those who have regrets after realizing that COVID-19 isn't a 'pooping disease' were met with signs at various Costco locations informing them that they won't be able to return all that toilet paper, paper towels, sanitizing wipes, water, rice and lysol they bought in anticipation of a societal collapse, ..."
Those who have regrets after realizing that COVID-19 isn't a 'pooping disease' were met with
signs at various Costco locations informing them that they won't be able to return all that
toilet paper, paper towels, sanitizing wipes, water, rice and lysol they bought in anticipation
of a societal collapse, according to brobible
.
lmao Costco basically saying y'all wanted to be extra, y'all gonna deal with your millions
of toilet paper all over your house #sorrytammy
pic.twitter.com/eCFhoiDp33
-- m (@capricorngirlyy) March
19, 2020
Enjoy your lifetime supply of toilet paper and wipes you crazy #hoarders !
#Costco is not
taking any more returns. Better start figuring out what you are gonna do with 10 bags of rice
you bought! pic.twitter.com/z2U7tN7ru3
-- Xyth Lord (@Xyth_Lord)
March 19,
2020
Seriously gotta calm down 😂 Costco is not accepting returns on toilet paper,
bounty, sanitizers etc pic.twitter.com/KKRAg5n1B4
-- Theju 🌸
(@PinkCancerian) March 19,
202
Costco, meanwhile, may have over-bought in anticipation of sustained demand which has
petered out. It looks like "the whole toilet-paper craze has calmed down," tweeted one shopper.
Guess the whole toilet-paper craze has calmed down. Quiet morning at Costco. pic.twitter.com/tt6wtcFV5f
-- Sean Coleman
(@SColemanUFA) March 22,
2020
Now what to do with all that TP?
Notable quotes:
"... Speaking of "suited and booted", shouldn't these people be wearing one of those full body suits and booties over their shoes as well? ..."
Trinity
March 25, 2020 at 3:13 pm GMT
Yesterday I ventured into Wal-Mart to shop with the other local deplorable people that the elite child molesters, sexual perverts,
and sociopaths out in Hollyweird, NYC and Washington like to look down on.
Wasn't that crowded and I probably noticed about 10 customers "suited and booted" wearing various masks of different shapes
and styles and latex gloves.
Speaking of "suited and booted", shouldn't these people be wearing one of those full body suits and booties over their
shoes as well?
Highly recommended !Notable quotes:
"... Put together, they reveal how big a share of the American markets for drugs, medical devices, and protective gear is controlled by goods made overseas. The big takeaway is that the nation could be in big enough trouble if supply disruptions were to occur in normal times (say, due to natural disasters in manufacturing centers abroad). During a high-mortality pandemic like the CCP Virus, these levels of foreign dependency are high enough to guarantee significant numbers of needless deaths. ..."
"... And in fact, the import penetration trends for these products exemplify the nation's health care security weaknesses. In 2002 -- a good baseline, since that's the first year China was a member of the World Trade Organization -- imports overall accounted for 16.7 percent of all surgical appliances and supplies used in the United States (measured by value, not numbers of masks or pairs of gloves). During the first full year of the Great Recession, 2008, this share totaled 28.08 percent. ..."
"... Keeping this qualification in mind, overall, 32.41 percent of surgical appliances and supplies were imported from other countries by 2011, according to these figures. In 2016, that number reached 41.81 percent of a $33.71 billion U.S. market. It may well be higher these days, as between then and last year, U.S. overseas purchases jumped by more than 29 percent. (Interestingly, in light of domestic shortages, U.S. exports in appliances and supplies actually rose by more than 13 percent during this period!) ..."
"... Ventilators, sadly, have been in the news, too; they and related products like oxygen tents and bronchoscopes and inhalators and suction equipment are found in a big goods category called surgical and medical instruments. In 2002, imports from all corners of the world represented 22.04 percent of American consumption. By 2016, this figure stood at 35.91 percent of a $37.5 billion national market, and over the next three years, imports grew nearly 31 percent. (Exports expanded at a relatively slow 11.84 percent.) ..."
"... exclusive U.S. reliance on China for the chemical ingredients of numerous medicines has now become a major federal government concern. ..."
"... The main foreign suppliers to the American pharmaceuticals market as of last year look encouragingly diversified and encouragingly friendly. For example, Ireland was number one, with 22.15 percent of such shipments, followed by Switzerland with 14.05 percent. But third and fourth, with 8.87 percent and 8.39 percent of imports, were Germany and India, respectively, both of which have limited or embargoed their medical exports this year. And number five, at 7.38 percent, was Italy -- whose current CCP Virus devastation could easily bring about export restrictions. ..."
"... Last year, America's leading foreign supplier of surgical and medical instruments (the ventilators category) was Mexico, which sold U.S. customers 28.58 percent of the $17.62 billion of total imports. But export-curber Germany was number three, at 9.43 percent, and China was sixth, at 6.93 percent. ..."
"... Purely domestic policy steps, like mandating more stockpiling or new recycling and re-use strategies, undoubtedly can add to national medical products supplies. But even these general import penetration figures, along with the shortage reports that keep pouring in, make clear that enduring national health care security can't be restored without a major ramping up of domestic output. And since export-heavy economies like China's and Germany's will undoubtedly work overtime to keep their American health care customers -- including with all manner of predatory economic practices -- it's similarly clear that big, lasting U.S. departures from standard free trade policies will be unavoidable. ..."
Not Just China: U.S. Reliance on Foreign Medical Supplies is Staggering
The government's own numbers tell a frightening tale of how this happened, and when.
Virus pandemic having exposed scary domestic shortages of critical medical
goods ranging from safety masks to ventilators, along with potential shortages of
pharmaceuticals, political leaders across the spectrum are finally regretting having allowed so
much output of these products to migrate offshore.
China's role in global supply chains has understandably sparked much of the alarm, since its
government has all but threatened to withhold supplies of medicines whenever it wishes. But all
told, at least 38 countries (including the 27-member European Union) have curbed exports of
anti-pandemic products at some point since the CCP Virus began dominating headlines.
So
potential foreign chokeholds in the nation's health care-related supply chains appear global in
scope. The federal government's best data make clear just how widespread the problem has
become, and how steadily it's been growing.
The figures come from the government's statistics on industry-by-industry manufacturing
output and on exports and imports. (The output data can be accessed through databases created
by the Census Bureau for its Annual Survey of Manufactures that are located at this link . The
trade numbers can be retrieved at an interactive database maintained by the U.S. International
Trade Commission that's located at this link .)
Put together, they reveal how big a share of the American markets for drugs, medical
devices, and protective gear is controlled by goods made overseas. The big takeaway is that the
nation could be in big enough trouble if supply disruptions were to occur in normal times (say,
due to natural disasters in manufacturing centers abroad). During a high-mortality pandemic
like the CCP Virus, these levels of foreign dependency are high enough to guarantee significant
numbers of needless deaths.
These statistics aren't problem-free. Principally, because the manufacturing output figures
are so granular, and therefore take so long to compile, import penetration rates for these (and
other manufactures) can be calculated only through 2016. Yet the more timely import numbers can
provide a reasonable indication of whether vulnerabilities are worsening or shrinking. At the
same time, the government's main trade data aren't nearly as detailed as the production
numbers. As a result, it's not possible to know the percentage of, say, safety masks used in
the United States that are produced abroad. But it's easy to come up with this number for the
category in which masks (and other protective gear) are grouped -- surgical appliances and
supplies.
And in fact, the import penetration trends for these products exemplify the nation's health
care security weaknesses. In 2002 -- a good baseline, since that's the first year China was a
member of the World Trade Organization -- imports overall accounted for 16.7 percent of all
surgical appliances and supplies used in the United States (measured by value, not numbers of
masks or pairs of gloves). During the first full year of the Great Recession, 2008, this share
totaled 28.08 percent.
Notably, these imports from China were a tiny 1.5 percent in 2002, and had actually dropped
to 0.49 percent by 2008. By 2016, they accounted for a seemingly modest 6.54 percent of
American consumption. But here's where another weakness in the data emerges: they say nothing
about the origin of the materials, parts, and components of the final goods.
Keeping this qualification in mind, overall, 32.41 percent of surgical appliances and
supplies were imported from other countries by 2011, according to these figures. In 2016, that
number reached 41.81 percent of a $33.71 billion U.S. market. It may well be higher these days,
as between then and last year, U.S. overseas purchases jumped by more than 29 percent.
(Interestingly, in light of domestic shortages, U.S. exports in appliances and supplies
actually rose by more than 13 percent during this period!)
Ventilators, sadly, have been in the news, too; they and related products like oxygen tents
and bronchoscopes and inhalators and suction equipment are found in a big goods category called
surgical and medical instruments. In 2002, imports from all corners of the world represented
22.04 percent of American consumption. By 2016, this figure stood at 35.91 percent of a $37.5
billion national market, and over the next three years, imports grew nearly 31 percent.
(Exports expanded at a relatively slow 11.84 percent.)
Again, the China figures are small beans -- the import penetration rate for 2016 was a mere
2.35 percent. But these products often contain lots of electronics parts, and half the world's
printed circuit boards, for example, are made in the People's Republic. In other words, lots of
existing global surge capacity throughout the sector is ultimately controlled by Beijing.
Thanks to the work of researchers like the Hastings Center's Rosemary Gibson and independent
journalist Katherine Eban, heavy and sometimes exclusive U.S. reliance on China for the
chemical ingredients of numerous medicines has now become a major federal government concern.
Indeed, the Food and Drug Administration is keeping an especially close eye on the availability
of no fewer than 20 pharmaceutical products that use Chinese raw materials. (Unfortunately, the
FDA won't say what they are, which calls for some Freedom of Information Act requests,
pronto.)
But the import penetration figures make clear that supply disruptions could also originate
elsewhere. Between 2002 and 2016, drugs produced overseas more than doubled their share of
America's consumption (which stood at nearly $200 billion three years ago), from 17.23 percent
to 38.51 percent. As of 2019, moreover, U.S. drugs imports were 20.34 percent higher than in
2016.
The main foreign suppliers to the American pharmaceuticals market as of last year look
encouragingly diversified and encouragingly friendly. For example, Ireland was number one, with
22.15 percent of such shipments, followed by Switzerland with 14.05 percent. But third and
fourth, with 8.87 percent and 8.39 percent of imports, were Germany and India, respectively,
both of which have limited or embargoed their medical exports this year. And number five, at
7.38 percent, was Italy -- whose current CCP Virus devastation could easily bring about export
restrictions.
Nor is this pattern restricted to pharmaceuticals. Last year, America's leading foreign
supplier of surgical and medical instruments (the ventilators category) was Mexico, which sold
U.S. customers 28.58 percent of the $17.62 billion of total imports. But export-curber Germany
was number three, at 9.43 percent, and China was sixth, at 6.93 percent.
For surgical appliances and supplies (the masks and protective gear category), Ireland
topped the 2019 foreign supplier list, selling the United States 24.09 percent of its $18.21
billion of total imports. But China was second, at 15.29 percent, and in third place, at 9.68
percent, stood Malaysia, which banned mask exports on March 20.
Purely domestic policy steps, like mandating more stockpiling or new recycling and re-use
strategies, undoubtedly can add to national medical products supplies. But even these general
import penetration figures, along with the shortage reports that keep pouring in, make clear
that enduring national health care security can't be restored without a major ramping up of
domestic output. And since export-heavy economies like China's and Germany's will undoubtedly
work overtime to keep their American health care customers -- including with all manner of
predatory economic practices -- it's similarly clear that big, lasting U.S. departures from
standard free trade policies will be unavoidable.
Alan Tonelson is the founder of RealityChek, a public policy blog focusing on economics
and national security, and the author of The Race to the Bottom .
Highly recommended !
Kratoklastes
March 25, 2020 at 6:16 pm GMT
@thotmonger
I also remember some of early estimates of Mad Cow disease in humans in UK and they
turned out to be very exaggerated.
When the political class was trying to de-gay HIV/AIDS in 1987, they had Oprah tell
everyone that 20% of heterosexual people would be dead before 1990.
The first I learned of Oprah's jaw-droppingly sensationalist remarks, was in a piece a
couple of days ago on AmericanThinker (which sounds like a rare bird indeed, if not an
outright oxymoron – but it has good stuff from time to time).
Anyhow, it was an interesting piece – entitled
" Reflections on a Century of Junk Science " by the author of " Hoodwinked: How
Intellectual Hucksters Have Hijacked American Culture ", which I will acquire today. (The
book's 11 years old, but sounds like it will be along the same lines as Kendrick's "
Doctoring Data: How to Sort Out Medical Advice from Medical Nonsense ", which was
excellent).
Highly recommended !
US authorities are working to combat the spread of misinformation that has blossomed since the start of the coronavirus
pandemic
The US
Department of Justice announced Sunday it had shut down a website claiming to sell a
coronavirus vaccine, in its first act of federal enforcement against fraud in connection with
the pandemic.
Lawsuits had been filed against the site coronavirusmedicalkit.com, which claimed to sell
vaccines for COVID-19, the disease caused by the novel coronavirus, when in fact there is no
such vaccine, the Justice Department said in a statement.
A Texas federal judge on Saturday ordered the site to shut down, according to the statement.
Its homepage, however, was still accessible as of Sunday evening.
"Due to the recent outbreak for the Coronavirus (COVID-19) the World Health Organization is
giving away vaccine kits. Just pay $4.95 for shipping," read a statement on the homepage.
It was followed by a place to leave bank account information to pay shipping fees.
The Justice Department did not specify how many people fell victim to the scam, but the
investigation is ongoing to identify who is behind the fraud and how much money was stolen.
The intervention by the federal judiciary system is part of ongoing efforts by US
authorities to combat the spread of misinformation that has blossomed since the start of the
pandemic.
Attorney General Bill Barr last week urged federal prosecutors to make stopping
misinformation a priority and called US civilians to report all such abuses to the National
Center for Disaster Fraud.
He also warned citizens against a variety of scams including selling fake treatments online,
imitating emails from the WHO or the Centers for Disease Control and Prevention (CDC) intended
to collect personal data, and asking for donations for imaginary organizations.
Simultaneously, the US judicial system is on the warpath to combat price gouging of products
such as hand sanitizer or hygienic masks.
More than 33,000 people have been infected by the coronavirus in the US, and 416 have died,
according to a tracker managed by Johns Hopkins University.
Highly recommended !Michael Osterholm -
Wikipedia (born March 10, 1953) is an American infectious disease epidemiologist, regents
professor, and director of the Center for Infectious Disease Research and Policy at the
University of Minnesota.Scientific establishment want money, want importance, wants political influence. That create
difficult dilemma and force some people play the role of fear mongers.
parcos79 13 hours
ago
12 million views...holy cow
MKingston 1
week ago
BUMP 00:10 Intro 0:40 How bad is Coronavirus
4:00 Is
the virus an "old persons" disease 5:18 Incubation period
7:50
What can be done to prevent infection 13:45 Drug shortages 15:20 Sauna use
effect on infections 18:00 Was Coronavirus man-made
22:00
American Wild Deer diseases and Prions 32:00 Is Corona seasonal
35:00
Corona could be 10 times worse than the flu 35:25 Corona will stay around
for months 36:10 Coronavirus vs Spanish
flu 38:30 How can we prepare our
immune system 43:20 Do hand sanitizers and
masks work 50:00 We stockpile weapons more
than medical goods 54:30 Will people panic if they
are told the truth 56:00 Vaccines 1:02:00 Why a
virus would originate from China 1:11:30 What to do if you get
the flu 1:15:45 Lime disease and ticks
1:23:00
Effects of fire suppression on ecosystem 1:30:00 Vaccine for
Coronavirus
whisperingsage 4
days ago (edited)
Sick nurses working, I have experienced that in every nursing home I have worked in in the
US. In California and NV. Luckily, I found the trick, If I have a headache that won't be
resolved with hydration, I figure it's a flu, I take 4 grams of C and 20,000 IU of D, and
usually that takes care of it, no more symptoms. In the case that it persists, I keep taking
4 grams of C ever few hours and high dose D until the symptoms subside. Usually doesn't take
too long, and ( a few hours) symptoms don't get bad.
Joan Anundson-Ahr 1 day ago
Beware of any expert that promotes fearfulness and helplessness and tells us to just wait
for a "miracle" vaccine. Why didn't he tell us the truth about the success of vitamin C
therapy? Why didn't he tell us that some common medications like ibuprofen and heart
medications can impede healing of the virus.
KW0311 USMC 1
week ago
Joe doesnt like hearing his sauna and probiotics arent the cure for everything.
MiZzShiN3 7
hours ago (edited)
15:25
- 18:04
sauna myth
Aventura 2
days ago (edited)
div> It´s funny and very predictable how programmed into fear people have become
when it´s never the virus that kills you, but a weak immune system´s panick
reaction. If you believe the MSM is not aligned with certain agendas, the WHO is not
inherently corrupt, the pharmaceutical vaccine pushing industries have your best interests at
heart and doctors really know what they are talking about when they always look at the parts
as seperated and never the whole living system, then you will be shocked to learn the truth.
https://www.youtube.com/user/drvashiva/videos
I really look forward to a time, probably thanks to this crisis it will be in the not so
distant future, where people will begin to wake up, see through the BS we are being bombarded
with from the parasitical class of "rulers" or "elites". Then a paradigm shift in so many
ways will begin to take place... Greetings from a tireless truth seeker!
Gina Jonson 1
day ago div c
lass="comment-renderer-text-content expanded"> the difference between COVID 19 and the
spanish flu and the fear rampant about this comparison is that our health care system is a
little more advanced than what was available back in 1919 AND we are also so much more
informed regarding hygiene practices.........not discounting the seriousness of this
unprecendented occurrence.........but still great to focus on the "little" advantages we can
monopolise on. in order to tackle this global crisis head on and rationally
WJK 5 days ago
(edited) div
> @PowerfulJRE - Joe PLEASE have Michael Osterholm back on asap and please ask Michael
the following questions...
1) Are highly infectious airborne cold viruses killed by ozone from ozone/ion
generators(?) and
2) Why do medical facilities and schools no longer install or utilize UV disinfection
lighting like they use to utilize/install in entranceways, hallways, and rooms of hospitals
and school classrooms like they use to do 50-75 years ago(?)
Steve Ward 5
days ago
43:12 real good info about hand
sanitizer and face masks
J_M_W_77 5
days ago
N95 masks....remember kids its a one way valve on the front of those things....breath in,
and it filters the air....breath out, valve opens and the air goes out, " unfiltered". If
you're sick, these masks will not prevent you from spreading it around.
Rodney Higgins 2
days ago
China's only biosafety level 4 (BSL–4) laboratory is in Wuhan. Coincidences
happen.
Tessangela Beck 3
days ago div tabindex="0" role="article"
> Osterholm is a catalog of infectious disease info that is beyond valuable . . he's in
his 60s . . maybe the planet has others who could fill his shoes in my home state of
Minnesota; of course, I hope so! He also has a good sense of humor, managing a little chuckle
when Joe suggested if any president could get around the informed consent issue of testing
vaccines on prisoners, such as nasty rapists, it would be Trump. I'm glad to receive all the
helpful info without a steady dose of politics and conspiracy chitchat. Now I know that my
prebiotic and probiotic pills are only good for temporary relief and that my natural flora
and fauna in the gut will take over...
GAiPS 1 week ago
(edited)
51:46 "We spend about 0.001% on
public health compared to our defense department and yet look how vulnerable...it's the
bugs...it's not a war...it's not a missile...is bringing the world economy down right
now....it's a darn virus."
Noelf 1 week
ago
Can you imagine if even half the US defence budget was redirected into health care and
research!! We (the world) spend trillions on arms and now we are fighting an enemy that
bullets can't kill!! Infuriating!! 😡😡😠😠
Qidi Wang 1
day ago div tabindex="0" role="article"
> How do you draw the conclusion that such viruses would always come from China? MERS
was first discovered in the middle east, the 2009 flu originated in mexico, the Spanish flu
originated in Kansas. I mean like if you search China on the pandemic wikipedia page there's
only SARS and several flu outbreaks.
Also Wild life is not part of the cuisine in most of China, and it's really more of a
status symbol for rich people to be able to find exotic food
Niels Raider 5
days ago
In politics, nothing happens by accident. If it happens, you can bet it was planned that
way. Franklin D. Roosevelt
Roedy Green 4
days ago (edited) div tabindex="0" role=
"article"> There is another nasty virus going around here in Victoria BC Canada that is
a bit like CORVID-19.. I got it in mid-December and I am just getting over it. My friends
recovered in two to three weeks. The symptoms include a cough that goes on and on leaving you
breathless, extremely sore throat, runny nose, extreme weakness. Even the emergency room
doctor said she had it. Have you heard of it? I think I got it travelling in a Handi-dart van
with some elderly, sneezing Chinese speaking males.
Santino Rider 5
days ago (edited)
51:40 Good reminder of war
against missiles vs virus. Budgets... 53:00 his talk to
banking/finance people. Scary. Like children, whereas Michael is more analytical, like
engineers/scientists, see it all as problem-solution.
Highly recommended !
kiwiklown , Mar 22 2020 10:11 utc |
128
@Jackrabbit | Mar 21 2020 22:32 utc | 50
"These officials "failed us" in the same way that our media "fails us": they serve the
interests of the EMPIRE-FIRST Deep State."
Yuppp. Our error is to assume all 17 intelligence agencies; the presstitudes; and US
"leadership" exist to serve the American people. And so, yes, they "fail" the people. But, from the point of view of the controllers of those agencies and of those "leaders",
they hardly ever fail !!!
While the people argue over virulent minutae, they are once again helping themselves to
the US Treasury.... Trillions of USDs.... LOL
kiwiklown , Mar 22 2020 10:36 utc |
132
@Jackrabbit | Mar 21 2020 23:10 utc | 54
"Caitlin Johnstone also sees the response being manipulated to focus hate on China...."
Yuppp, blaming China, hating on China achieves several objectives:
it misdirects Americans from blaming Trump's "leadership";
it excuses Trump's mismanagement ("...the Chinese LIED...")
it absolves the CDC, 17 "intelligence" agencies, etc;
it continues The Great China Pivot started by Great Pretender Obama;
it uses current fear to mobilise Americans to hate China more;
it prepares Americans for when war on China becomes feasible;
Just look at how US leadership has been hating on Russia for the last 100 years, waiting
to whack them with a sneak attack if feasible.
kiwiklown , Mar 22 2020 11:25 utc |
137
@Jackrabbit | Mar 22 2020 2:45 utc | 79
".... was then told to STOP TESTING...... A medical person would not try to suppress testing.
That would be a "management decision" and its the Nation Security Council that was running
the show (and which had classified all discussions related to virus preparations)...."
Thanks for reminding us of Dr Chu's story. What if the US leadership:
Knew the coronavirus was already out in the wild in the US by Sep 2019;
Decided to set up China to be the "origin" to be blamed;
Realized that a "pandemic" can be the cover for kicking the table over to do the Great
Financial Reset;
Highly recommended !
Bowhead31 5
hours ago
The problem is these people no longer see themselves as public servants.
Maria Summers 6
hours ago
The Georgia Senator is just as guilty as the rest of them, regarding "Insider
Trading".
shane passey 3
hours ago
She's a crook just like the rest of the politicians. They say they be there for the
people. But they're really there to make themselves rich
@supenau
who make profits as well. I cannot remember exactly when insider trading for
them became legal but it should be no surprise to anyone paying the slightest bit of attention
that they're ALL doing it. That is one reason, at least in my semi-educated opinion, they did
not go after Trump for emoluments during Shampeachment, because THEY ALL DO IT.
That goes all the way to the White House, no doubt.
Marie on Sat,
03/21/2020 - 10:28am
Looks
as if the crisis profiteers were on top of it:
Think about this:
Weeks before you had any inkling you were going to lose your job,
was selling off millions of stocks -- and *buying* stock in a teleworking company.
-- Robert Reich (@RBReich) March 20,
2020
Highly recommended !
Curmudgeon March 18,
2020 at 5:40 pm GMT
@eah
I'm agnostic on the subject of COVID-19: its origin, how it first infected humans, its
epidemiological spread
Perhaps agnostic is not the best choice of words, but overall, I agree.
It is not impossible that the virus did not "escape" from the Wuhan Lab, but it is
unlikely.
That the Chinese have sequenced a virus to do something unexpected, then published it, is
unremarkable. That others may have done the same or similar and not published it,
would be remarkable. I would consider the "Five Eyes" and Israel entirely capable – and
likely to do that, given they operate as one.
I look to the narrative we get in North America, irrespective of the topic, and the
pattern is the same:
In context of the above, I am leaning toward that it wasn't an accident and in all
likelihood it wasn't China.
Highly recommended !
likbez , March 15, 2020 6:13 pm
In most countries COVID-19 is regional with one province (and within this province one large city) as the epicenter.
Jim Bianco's model is too primitive and as such unnecessary alarmist.
The early stages of any flu epidemic are always exponential. But from some point propagation slows down considerably as the
virus has difficulties to find new vulnerable people either because number of people with immunity increases (COVID-19 on average
lasts less then a month; often just two weeks and around 90% of cases are mild ), or the measures were taken to "flatten the curve",
or the weather or other conditions became unfavorable to the virus.
Current exponential growth can also be explained by the fact that CDC completely botched testing. So a better availability
of tests with time produces a false exponential increase in cases.
In a sense the first half of March in the USA corresponds to the first half of Jan in Wuhan when the authorities did not yet
resort to drastic actions (especially true for NYC, which looks like a giant cruise ship to me with all corresponding problems
with AC, high density of population, frequent interaction with sick people via public transport including subway as infection
points, etc ).
This is also the period when the medical personnel became the most prominent victim of the authorities incompetence.
I am no so much concerned with number of infection among "commoners" as with the number of infections of medical personnel.
Depletion of medical personnel will greatly complicate the picture.
Working in hazmat suits exhaust people, especially women, very quickly and thus make them more susceptible to the infection.
In many cases you also need to wear adult pampers. It might well be that this is an overkill for this particular infection and
less drastic measures like surgical scrubs can be as effective to protect medical workers.
Research published in Feb had found that out of 138 patients studied at one Wuhan hospital, 29% were healthcare workers. Over
3K medical workers in China were infected and at least 18 died with ~ half of them under 40. Looks like heavy contact with infected
patients make medical workers prognosis worse than for "commoners"
Retired people over 70 now should self-quarantine and outside of senior facilities they are by-and-large responsible for their
own health. When I see them on cruse ships in late Feb and March I just think how many reckless persons are among older folk.
Most of them are also wealthy enough to order food via home delivery, not to drive to the store.
Still on recent visit to department store there were a lot of grannies in the lines (and completely depleted shelves ;-). Looks
like they are braving possible infection with the regular flu, if not coronavirus as typically several people cough within the
large store.
There should be some level of individual responsibility here , especially among seniors who are retired.
But, at the same time, "Whom the Gods would destroy they first make mad"
likbez , March 16, 2020 12:34 am
Terry, March 15, 2020 7:25 pm
Thanks for your last comment Run. You saved me the trouble.
Famous quote “They had learned nothing and forgotten nothing” is applicable to the current situation in the USA. Looks like
the US authorities learned nothing from SARC epidemics, which BTW hit Toronto.
Let me clarify my previous post (which does suffers from wordiness as run75441 correctly pointed out).
There are two diseases bunged into one in COVID-19: one is flu-like and is no threat (just a nuisance and Bert Schlitz is absolutely
correct about this part) and the second is the SARC-like destructive virus pneumonia which is an extremely serious threat that
has long time health consequences for survivors (lung fibrosis of various degrees similar to those which is the consequence of
pneumonia caused by electronic cigarettes.)
Those curves above do not distinguish between them and as such have no value.
IMHO the curves that matter are “serious and critical cases” and the “medical workers who are in serious or critical conditions.”
UnionHorse , Mar 14 2020 2:48 utc |
189
Civilizations depend on toilet paper it seems. Toilet paper is the bellwether commodity of
our age. Capacity production is called for, especially neoclassic econ 101 foolishness.
Nevertheless, overtime at the paper mills is in order.
Highly recommended !This is a really brilliant satire !!! Another outstanding work. "Spread the message, not the virus" and "...when they threaten the
Stock Market." Priceless
What makes a nation civilized is not how it acts in times of peace but how it chooses to conduct itself in moments of crisis. Hoarding
stuff for months selfishly and fighting people in markets like animals is not how civilized societies deal with crisis.
Notable quotes:
"... Toilet paper is such a weird thing to be panic-buying... ..."
"... "Global emergencies- when they threaten the stock market" So sad but true ..."
"... "When they threaten the stock market." Boom. ..."
"... I love the term "local government franchise". sounds pretty synonymous to a government run by crooks and impotent political dynasties. ..."
"... I like how this started off completely taking the mick, but then turned, depressingly, into one of the most sensible summaries of our current situation. (I mean it's depressing that comedians seem to be better at communicating than our glorious leaders). ..."
"... "Italians are freaking out the Chinese are hiding out" That was just so freaking hilarious oh my God I love this channel ..."
Amarka
Honest Government Ad (govern/rule � ment/mind) | Coronavirus: Flatten The Curve
https://www.youtube.com/embed/Hks6Nq7g6P4?version=3&rel=1&fs=1&autohide=2&showsearch=0&showinfo=1&iv_load_policy=1&wmode=transparent
Vote Up 1 0 Vote Down Reply Mar 14, 2020 10:05 PM
John Gardner 23 hours ago
Toilet paper is such a weird thing to be panic-buying...
foo barf 23 hours ago
But my sphincter is far too important to let a Murdoch publication near it
JNB Brothers 23 hours ago
"Global emergencies- when they threaten the stock market" So sad but tru (climate change, equal rights etc)
John Gardner 23 hours ago
Toilet paper is such a weird thing to be panic-buying...
foo barf 23 hours ago
But my sphincter is far too important to let a Murdoch publication near it
JNB Brothers 23 hours ago
"Global emergencies- when they threaten the stock market" So sad but true (climate change, equal rights etc)
Tommy Knocker 23 hours ago (edited)
Now flying off the shelves near you: New Rupert Murdock toilet paper, as hard on your ass it is on the eyes!!!
Aurum TheBrave 23 hours ago
"When they threaten the stock market." Boom.
Charliemagne Crabajales 19 hours ago
I love the term "local government franchise". sounds pretty synonymous to a government run by crooks and impotent political
dynasties.
George Caplin 20 hours ago
I like how this started off completely taking the mick, but then turned, depressingly, into one of the most sensible summaries
of our current situation. (I mean it's depressing that comedians seem to be better at communicating than our glorious leaders).
Ison Willis 23 hours ago
If it gets not banned, its part of the sh*show.
Alexandru Popescu 23 hours ago
Lucy's heavenly voice and impeccable pronunciation � which transform the coarse language into music to our ears � perfectly
convey the urgent educational message.
Saturn666 23 hours ago
Kind of tragic when a comedy channel like this is more informative than governments.
denthy k 23 hours ago
Trump: If I'm not tested, I'm not infected.
tuseroni 20 hours ago
"i dont take responsibility at all" he did say that. not sure if he is exposed to the corona virus, but he is clearly allergic
to responsibility
resourcedragon 23 hours ago
Thank you for the "flatten the curve" message. To be honest, I had wondered whether delaying the inevitable was the way to
go - especially in view of the fact that there are going to be, indeed, already have been deaths that are due to knock-on effects
from the corona virus.
Avatar WarMech 19 hours ago
"Italians are freaking out the Chinese are hiding out" That was just so freaking hilarious oh my God I love this channel
More GOP congressmen who attended the CPAC political event last month are self-isolating --
and
one of them just flew on Air Force One with President Trump . Another was
seen on video shaking hands and chatting face to face with the president before entering
self-quarantine. ( CNBC, Reuters )
Note to Pence:
Televangelist Jim Bakker's
TV show was among
seven companies receiving FDA/FTC warnings about "fraudulent" sales pitches for
coronavirus treatments.
Highly recommended !Notable quotes:
"... One notable prediction: Osterholm lauds the Chinese for successfully working to control the outbreak -- but warns another wave of infection will follow upon workplaces and schools and shops reopening as the society begins returning to normal. ..."
Emily Dickinson , Mar 11 2020 20:52 utc |
74
james , Mar 11 2020 3:16 utc |
71
joe rogan interview today with Michael Osterholm is an internationally recognized expert in
infectious disease epidemiology from today...
https://www.youtube.com/watch?v=E3URhJx0NSw
Joe Rogan had an interesting interview with epidemiologist Michael Osterholm
yesterday. Lots of information about COVID-19.
https://www.youtube.com/watch?v=E3URhJx0NSw
One notable prediction: Osterholm lauds the Chinese for successfully working to
control the outbreak -- but warns another wave of infection will follow upon workplaces and
schools and shops reopening as the society begins returning to normal.
Tom_LX , Mar 9 2020 19:35 utc |
23
Posted by: charliechan | Mar 9 2020 19:30 utc | 20
Charli Chan ask right question.
charlie cha wonders how US counts the sick when CDC test kits are unreliable.
and unavailable in quantities necessary !!!!
Notable quotes:
"... Nothing speaks more loudly of the dumbed down, idiotic, Fakebook groupthink of the age than the current rush to buy toilet roll as a response to the Coronavirus crisis. ..."
Richard
150
No need to worry about the corona virus - it'll all be okay as long as you buy enough toilet
roll...
Nothing speaks more loudly of the dumbed down, idiotic, Fakebook groupthink of the age
than the current rush to buy toilet roll as a response to the Coronavirus crisis.
You've seen it on the tele and (un)social media – supermarket shelves denuded of bog
roll and fat birds beating seven shades of sh*t out of each other over the last bag of ass
wipe.
I mean, what the hell!? Is this how stupid and pathetic we've become? Someone sees a post
on Fakebook that says its a good idea to respond to a potentially fatal virus by buying lots
of bog roll and within 5 minutes there's a massive rush on the stuff – after all, you
gotta buy it, right, COS IT SAYS SO ON FAKEBOOK...
https://richardhennerley.com/2020/03/10/of-coronavirus-toilet-roll-and-idiocy/
Highly recommended !Notable quotes:
"... Since this is going to be a post about the coronavirus, let's start off with this PSA: wash your hands. These viruses have a lipid envelope that is crucial to their structure and function, and soaps and detergents are thus very effective at inactivating them. It's fast, it's simple, and it's one of the more useful things that any individual can do under these conditions. ..."
"... Since I read this, when I come home, I just grab a plain ordinary bar of soap, and lather up my hands real well, and leave the soap on my hands for 10 or 15 seconds or so. I now believe that ordinary soap is very effective at neutralizing this particular virus. ..."
"... So I will not go out and fight the crowds to buy some 'sanitizer'. At least not for CVD-19. ..."
blues
110
~~~~~~~~~~~~~~~~~~~~ //ScienceMag -
Pipeline
Since this is going to be a post about the coronavirus, let's start off with this PSA:
wash your hands. These viruses have a lipid envelope that is crucial to their structure and
function, and soaps and detergents are thus very effective at inactivating them. It's fast,
it's simple, and it's one of the more useful things that any individual can do under these
conditions.
This involves just a bar of soap.
This fellow is a real hot-shot big-time microbiologist. Since I read this, when I come
home, I just grab a plain ordinary bar of soap, and lather up my hands real well, and leave
the soap on my hands for 10 or 15 seconds or so. I now believe that ordinary soap is very
effective at neutralizing this particular virus.
So I will not go out and fight the crowds to buy some 'sanitizer'. At least not for
CVD-19.
I am now also taking:
~6,000IU Vitamin D3
I'm no doctor, but that is what I am taking.
bluedotterel , Mar 10 2020 6:47 utc |
112
uncle tungsten , Mar 10 2020 6:55 utc |
113
blues #111
So I will not go out and fight the crowds to buy some 'sanitizer'. At least not for CVD-19.
Recipe for sanitiser:
Remedy for toilet paper madness:
Krollchem , Mar 10 2020 8:01 utc |
115
blues@111
Good start on enhancing your immune system. Perhaps the following daily additions may
help:https://www.macleans.ca/news/canada/a-made-in-canada-solution-to-the-coronavirus-outbreak/
Pray for me, my friends, because I have the flu
... ... ...
Or, I don't know, maybe it is the Bat Flu. The more I read the
corporate press, the more I'm beginning to suspect it is. My suspicion isn't based on facts. I
don't have any of the Bat Flu symptoms. It's just a feeling like the feelings people had that
Saddam had secret WMDs, and that Trump was a Russian intelligence asset, and that the world was
going to end in the year 2012.
OK, those feelings turned out to be wrong, but this one feels like an accurate feeling, and
not like just the result of being relentlessly bombarded with hysterical headlines, pictures of
people in hazmat suits, and obsessively researching ever-changing, wildly-varying statistics on
the Internet, which I really need to stop doing that.
... ... ...
Plus, even if I just have the flu (i.e., the regular flu, not the Chinese Bat
Flu), the statistics on that are pretty scary. I don't know the numbers here in Germany, but,
according to the
CDC , since 2010, in the United States, the regular old garden variety flu has resulted in
the following, annually:
9 million – 45 million cases
140,000 – 810,000 hospitalizations
12,000 – 61,000 deaths
When you multiply all those numbers by 10 (because it's been 10 years since 2010), you
get:
90 million – 450 million cases
1,400,000 – 8,100,000 hospitalizations
120,000 – 610,000 deaths
That's 450 million possible cases and over half a million deaths, and that's just in the
United States! To make it concrete, if you stood all those dead people on top of each other,
head to toe, so that everyone was standing on everyone's head, and used them as an enormous
ladder, you could climb to the moon and back four times or once or twice at the very least.
And that's nothing compared to this Covid-19!
No, according to
The Guardian , Covid-19 is "about ten times more deadly than the seasonal flu," so
that's 610,000 deaths just this year, and if the CDC tracks it for a full 10 years, that's
pretty close to 6 million dead people, which will make it just as bad as the Holocaust
(although the Holocaust only lasted four years, so I'll have to adjust my math for that).
And, remember, that's just in the United States, which is only 4.25 percent of the total
global population. So you multiply the Holocaust by 95 percent (you can round the numbers to
make this easier) and you end up with 7 billion dead people, which is nearly every last person
on Earth, except for 700 million people! Which, OK, that sounds like a lot of people (i.e., the
700 million, not the 7 billion), but it's fewer than there were in the 14th Century; i.e.,
before the "Black Death" plague killed everybody!
... ... ...
Or, I don't know, maybe I'm overreacting. Maybe I just have the flu. I mean, what if this
whole Corona thing is just nature doing what nature does and not the end of civilization? Look,
I don't want to sound paranoid, but I can't help wondering whether this virus warrants all the
mass hysteria that the corporate media have been pumping out at us, relentlessly, for the last
two months, and the states of emergency that are being declared, and the quarantines that are
going into effect, and the curfews, and banning of public gatherings, and whatever other
"emergency measures" are going to be imposed in the coming weeks and months.
C. J. Hopkins is an award-winning American playwright, novelist and political satirist
based in Berlin. His plays are published by Bloomsbury Publishing and Broadway Play Publishing,
Inc. His dystopian novel, Zone 23 , is
published by Snoggsworthy, Swaine & Cormorant. Volume I of his Consent Factory
Essays is published by Consent Factory Publishing, a wholly-owned subsidiary of Amalgamated
Content, Inc. He can be reached at cjhopkins.com or consentfactory.org . Read other articles by C. J. .
Just been sensibly stocking up on 45 packets of pasta and noticed a lot of idiots panic
buying.
-- Simon Blackwell (@simonblackwell) March 6,
2020
To be honest, staff at my local Sainsburys were under the assumption that I've been panic
buying alcohol for the last four and a half years. #coronavirusUK
#toiletpaperpanic
(@thatjimdavis) March 6,
2020
The guy who invented hand sanitiser must be rubbing his hands together right now
-- Kate PT3 (@KateMMA3) March 5,
2020
Highly recommended !
US politicians and media are reporting approximately 500 cases of the virus in the US as
of March 8. The actual number is almost certainly much higher, however. Perhaps as much as
10-fold that number, according to some sources. Why?
There's the problem of reporting only tested cases so far, and there's still a lack of
available tests even to test and to verify all those infected without symptoms.. And even those
showing symptoms may have been determined initially as not infected by the tests, since
reportedly many of the early test kits were defective. Meanwhile, those without symptoms or
pre-symptomatic are not being tested at all.
The Fiction of Voluntary Quarantine
Then there's the policy of voluntary quarantining those who have come into contact with
someone who was tested and found infected. It's not working very well. Those who have come in
contact with carriers of the virus are asked simply to stay home. But do they? There's no way
to know, or even enforce that. The case example why voluntary quarantining doesn't work well is
Italy.
Most of the northern Lombardy region, including the financial center of Milan in that
country, is in 'lock down' right now. But all that means is voluntary quarantining. People are
asked not to leave their town, or the larger region. But is that stopping them traveling around
their town in public places? Or within the larger region? And spreading the virus there?
Apparently not. Reportedly, infection for those tested have risen in just two weeks to more
than 6,000 in Northern Italy. CNBC reports that, in just one day this weekend, that number
increased by 1200! So much for voluntary quarantines. There's no way, no sufficient personnel,
not even accepted procedures, with which to daily check on those (in Italy that means hundreds
of thousands) in voluntary quarantine.
The Real Costs to Workers
Average working class folks cannot afford to voluntary quarantine themselves. Or to stay
home from work for any reason. Even if they have symptoms. They will continue going to work.
They have to, in order to economically survive.
Consider the typical scenario in the US: there are literally tens of millions of workers who
have no more than $400 for an emergency. As many perhaps as half of the work force of 165
million. They live paycheck to paycheck. They can't afford to miss any days of work. Millions
of them have no paid sick leave. The US is the worst of all advanced economies in terms of
providing paid sick leave. Even union workers with some paid sick leave in their contracts
have, at best, only six days on average. If they stay home sick, they'll be asked by their
employer the reason for doing so in order to collect that paid sick leave. And even when they
don't have sick leave. Paid leave or not, many will be required to provide a doctor's slip
indicating the nature of the illness. But doctors are refusing to hold office visits for
patients who may have the virus. They can't do anything about it, so they don't want them to
come in and possibly contaminate others or themselves. So a worker sick has to go to the
hospital emergency room.
That raises another problem. A trip to the emergency room costs on average at least a
$1,000. More if special tests are done. If the worker has no health insurance (30 million still
don't), that's an out of pocket cost he/she can't afford. They know it. So they don't go to the
hospital emergency room, and they can't get an appointment at the doctor's office. Result: they
don't get tested, refuse to go get tested, and they continue to go to work. The virus
spreads.
Even if they have health insurance coverage, the deductible today is usually $500 to $2000.
Most don't have that kind of savings to spend either. Not to mention copays. So even those
insured take a pass on going to the hospital to get tested, even if they have symptoms.
The media doesn't help here either. Reports are typically that those who are young, middle
age, and in reasonable good health and without other complicating conditions don't die. It's
the older folks, retirees with Medicare, or with serious other conditions, that typically die
from the virus. Workers hear this and that supports their decision not to go to the hospital or
get tested as well.
Then there's the further complication concerning employment if they do go to the hospital.
The hospital will (soon) test them. If found infected, they will send them home for voluntary
quarantine for 14 days! Now the financial crises really begins. The hospital will inform their
employer. Staying at home for 14 days will result in financial disaster, since the employer has
no obligation to continue to pay them their wages while not at work, unless they have some
minimal paid sick leave which, as noted, the vast majority don't have. Nor does the employer
have any obligation legally to even keep them employed for 14 days (or even less) if the
employer determines they are not likely to return to work after 14 days (or even less). They
therefore get fired if they go to the hospital after it reports to the employer they have the
virus. Just another good reason not to go to the hospital.
In other words, here's all kind of major economic disincentives to keep an illness
confidential, to go to work, not go to the hospital (and can't go to the doctor). That risks
passing on the highly contagion bug to others–which has been happening and will continue
to happen.
Here's another financial hit for the working class: child care. Schools are beginning to
shut down. Even where no cases are yet confirmed. Stanford University just decided to
discontinue all in class sessions and revert to all online education. But what about K-6 and
pre-school? Or even Jr. high schools? When they shut down, kids must stay at home. But most
working class parents can't afford nannys or baby-sitters. Not everyone works in an occupation
or company where they can 'work from home'. Do they send the young kids to grandma's and
grandpa's, who are more susceptible to the virus? With their kids required to stay home, they
must miss work, and risk even losing their jobs. We're talking about millions of families with
6 to 12 year olds. And who knows how long the schools will remain shut down.
In short, wages lost due to self-quarantining, forced voluntary quarantining after hospital
testing, the cost of hospital emergency room visits (whether insured or not), the unknown cost
of the tests themselves (the government says it will reimburse them but they don't have the
$1,000 or more cash out of pocket in the first place), the cost of paying for nannys or
baby-sitters for young school age children when schools shut down–i.e. all result in a
massive out of pocket expense for most workers that they don't have.
Workers figure all these possibilities of financial disaster pretty quick and know that the
virus will mean a big financial hit if they miss a day's work, or even if they don't. So they
keep working, hoping they'll recover on their own, refusing to get tested because of the
potential loss of work, wages, and income, and crossing their fingers that their kids' school
districts don't shut down.
Economic Contagion Channels: Supply Chains, Demand, Asset Deflation, Defaults & Credit
Crunch
What this all means for the US economy is obvious. Household consumption was already
weakening at the end of last year. Most of consumption was driven by accelerating stock
valuations, which affect those in the top 10% who own stocks; or by taking on more
credit–credit cards, which affects the middle class and below.
Over $1 trillion in credit card debt is what has been largely driving middle income and
below consumption. Mainstream economists argue that defaults on credit card debt are only 3% or
so, and thus not a problem. But that's a gross average across all 130 million households. When
this data are broken down, middle income and below family credit card debt is around 9%, a very
high number more like 2007 when the last economic recession began.
Then there's auto debt. As of 2018, reportedly 7 million turned in their keys on their auto
loans. As in the case of credit cards, auto debt defaults will rise as well in 2020. Then
there's student debt, over $1.6 Trillion now. Defaults there are much higher than reported as
well, since actual defaults (defined as failure to pay either principal or interest) have been
redefined to something else other than actual default.
Add to all this the likelihood is very high that job layoffs will now begin by April, as the
global supply chain crisis due to virus-related cuts in production and trade. More job loss
means less wage income and thus less household spending and more inability to deal with the
costs of the virus for most working class families.
Let's not also forget the price gouging for certain products that is beginning now to
appear, both online and in stores. That reduces working class real incomes and thus consumption
too. Meanwhile, certain industries are already taking a big hit and layoffs are looming in
travel companies of all kinds (airlines, cruise ships, hotels, entertainment). In places where
the virus effect is already large, a big decline in restaurant, sports and concerts, movies,
etc. has also begun.
The two big economic contagion channels impacting employment thus far are supply chain
production and distribution reductions, and local demand for certain services (travel, retail,
hospitality, etc.).
But a third major channel has just begun to emerge: that's financial asset deflation in
stocks, oil & commodity futures, junk bonds & leveraged loans, and currency
devaluations.
Stocks' price collapse leads to business shelving investment and even cutting back
production. That means more job loss, reduced wage incomes, less spending, and economic
slowdown.
Oil and commodity prices now collapsing also lead to energy industry layoffs. More
importantly, in turn that will lead to energy junk bond market collapse–potentially
spreading to all junk bonds, leveraged loans, and even BBB grade corporate bonds (which are
really redefined junk bonds not investment grade bonds).
In other words, the collapse of supply chains, production-distribution, and industry by
industry demand in the US may become even worse should the financial markets price collapse can
lead to a general credit crunch. And that translates into a general economic real contraction.
That's precisely what happened in 2008, in a similar chain reaction from financial crisis to
real economic crisis.
Workers are aware of all this possibly leading to longer run economic stress. In the short
run, they consider possible wages loss if they reveal or report they have the virus, or get
tested: i.e. lost wage incomes: the cost of immediate medical care; the cost of child care,
etc. Better to tough it through and continue to go to work is a typical, and rational,
response.
This is already going on. Hundreds of thousands with, and without, symptoms are not being
tested; nor will most of them volunteer to be. Except for those on cruise ships who are forced
to be tested (and they're mostly retirees and elderly), few workers can afford to allow
themselves to be. The infection rate is thus already much higher and will continue to rise.
Voluntary quarantining doesn't work much (again just look at Italy, or even Germany, where in
one week cases (tested) rose from 66 to more than 1000). So out of economic necessity and to
avoid personal economic devastation, they continue to work. But that doesn't have to be.
US Policy Response: No Help for Working Class
US policy has been, is, and will continue to be a disaster. Trump's cuts to health and human
services in the past seriously hampered the US initial response. Tests had to be sent to
Atlanta and the CDC for processing. Early test kits often failed. Only now are they getting to
the states–to late to have a positive initial effect on the spread. Those suspected of
exposure to others confirmed infected were simply sent home for 'voluntary quarantine'. Initial
legislation of $8.3 billion just passed by Congress provides for 'reimbursement' for voluntary
testing, with no clarification if that covers the $1,000 hospital visit as well or just the
cost of the actual test!
There could be, however, a government response that financially supports workers and allows
them to be properly tested and treated.
An Alternative Policy Response
Why doesn't the government simply say 'go get tested for free' and the hospital will bill
the government for the costs? Not the worker pay up front with money he/she likely doesn't
have. Why isn't there emergency legislation by Congress or the states to require employers to
provide at least 14 days of paid sick leave, like other countries? And law guaranteeing
employers can't fire a worker sick with the virus for any reason? Or tax credits to working
class families for the full cost of child care–paid to a nanny or to the worker–if
they have to stay home in the event of a school district shutdown?
While business-investor tax cuts will almost certainly be the official government response,
few of the above measures for working class Americans are likely. In America working class
folks always get the short end of the economic stick. Congress and presidents pass trillions of
dollars in tax cut legislation ($15 trillion since 2001 to investors, businesses and the 1%),
but have raised taxes on the working class. Companies with billions of dollars in annual
profits pay nothing in taxes–and actually get a subsidy check from the government to
boot. Just ask Amazon, IBM, many big banks, pharmaceutical companies and more!
It can be expected the virus will have a large negative impact the standard of living and
wages of millions of working class families. They will have to bear the burden of the cost with
little help from their government. Meanwhile, businesses and investors will get bailed out,
'made whole', once again. In the process Consumption spending–the only area holding up
the economy in 2019–will take a big hit. That means recession starting next quarter is
more than a 50-50 likelihood.
In fact, the investment bank, Goldman Sachs, has just forecast that the effect on the US
economy in the coming second quarter of this year will be a collapse of GDP to 0% growth.
Join the debate on
Facebook More articles by: Jack Rasmus
Jack Rasmus is author of the recently published book, 'Central Bankers at the End of Their Ropes: Monetary Policy and
the Coming Depression', Clarity Press, August 2017. He blogs at
jackrasmus.com and his twitter handle is @drjackrasmus. His website is http://kyklosproductions.com .
Highly recommended !Notable quotes:
"... But there was no massive panic, no second by second media hysteria, over Hong Kong flu. Let me start being unpopular. "Man in his 80's already not very well from previous conditions, dies of flu" is not and should not be a news headline. The coverage is prurient, intrusive, unbalanced and designed to cause hysteria. ..."
"... It is also worthy of comment and I'm sure great relief to parents, that of the thousands of deaths, not one has been below the age of 10. ..."
The Hong Kong flu pandemic of 1968/9 was the last really serious flu pandemic to sweep the
UK. They do seem extraordinarily regular – 1919, 1969 and 2020. Flu epidemics have much
better punctuality than the trains (though I cheated a bit there and left out the 1958 "Asian
flu"). Nowadays "Hong Kong flu" is known as H3N2. Estimates for deaths it caused worldwide vary
from 1 to 4 million. In the UK it killed an estimated 80,000 people.
If the current coronavirus had appeared in 1968, it would simply have been called "flu",
probably "Wuhan flu". COVID-19 may not be nowadays classified as such, but in my youth flu is
definitely what we would have called it. The Hong Kong flu was very similar to the current
outbreak in being extremely contagious but with a fairly low mortality rate. 30% of the UK
population is estimated to have been infected in the Hong Kong flu pandemic. The death rate was
about 0.5%, mostly elderly or with underlying health conditions.
But there was no massive panic, no second by second media hysteria, over Hong Kong flu.
Let me start being unpopular. "Man in his 80's already not very well from previous conditions,
dies of flu" is not and should not be a news headline. The coverage is prurient, intrusive,
unbalanced and designed to cause hysteria.
Consider this: 100% of those who contract coronavirus are going to die. 100% of those who do
not contract coronavirus are also going to die. The difference in average life expectancy
between the two groups will prove to be only very marginal. That is because the large majority
of those who die of COVID-19 will already be nearing the end of life or have other health
problems.
... ... ...
What worries me about the current reaction to coronavirus, is that it seems to reflect a
belief that death is an aberration, rather than a part of the natural order of things. As the
human species continues to expand massively in numbers, and as it continues casually to make
other species extinct, it is inevitable that the excessive and crowded human population will
become susceptible to disease.
... ... ...
Yes wash your hands, bin your tissues, keep things clean. Don't hang around someone who has
the flu. Take advantage of everything modern medicine can do to help you. But don't be too
shocked at the idea that some sick people die, especially if they are old. We are not Gods, we
are mortal. We need to reconnect to that idea.
... ... ...
Reply
↓
Chic McGregor
March 7, 2020 at 23:05
Craig, you might want to check out https://www.worldometers.info/coronavirus/
... ... ...
It is also worthy of comment and I'm sure great relief to parents, that of the
thousands of deaths, not one has been below the age of 10.
It is unusually age selective. Whereas in many past epidemics both the elderly and very
young have been the most susceptible groups in this instance, 80% of deaths have been in the
over 60s.
Ralph Clark
March 8, 2020 at 11:36
And that could be why Europe has seen a higher death toll – do elderly people in
poor health make up a higher fraction of our population?
Flak Blag
March 8, 2020 at 02:57
Another excellent article, thank you Craig Murray. Some thoughts
When this story initially broke I was somewhat dismissive of it. I remember avian flu, and
particularly swine flu, when hysteria was purposefully whipped up in order to boost the
profits of big pharma, and of course to keep the population in it's usual state of paralyzed
anxiety. I am not qualified to comment on the suggestions other's have made relating to this
being a bio-weapon, deployed either by accident or design. As far as I can see it's too early
to tell, speculation and rumor abound, the dust has yet to settle.
I agree that it is normal and desirable for old people to die, and while I have no wish to
hasten the death of individuals within any demographic group, it seems that the current
fashion of prolonging the lives of the aged at the expense (financially and environmentally)
of subsequent generations is questionable. Perhaps it is emblematic of the mechanistic,
materialistic, individualistic and narcissistic agenda so aggressively promoted to justify
the consumerism currently infecting the world. I was taught that the debt we owe to our
parents we repay to our children, that is is better to subsist on crusts if it means our
children may have jam. Some would rather eat jam today than leave crusts for their progeny
tomorrow, maybe because as a society we see individual gratification as the meaning of
life
... ... ...
mass medical event
March 8, 2020 at 09:47
Beautiful thoughts, Craig With respect to the Corona Virus: The Patriot Act had been
prepared prior to the catastrophic event on 9/11 and was ready to be immediately enacted. One
did not see the shape of things to come while the event was unfolding.
... ... ...
Medicine opens new frontiers for exploitation because ill health is a regular earner.
There is nothing left to sell in the capitalist system but business services, Intellectual
Property and 'Apps' perhaps. The Smart Phone market is saturated. The Russians, and other
nations like Iran have still got endless supplies of gas, oil, etc.
... ... ...
MBC
March 8, 2020 at 13:06
With all respect Craig I think you may be wandering into areas you are not qualified to
judge. Mea culpa also, I am not a medic either. But I regularly see very senior medical
experts saying that they are very concerned about this virus and they must have good reason
because these people are clinicians not politicians.
As for the deaths from ordinary flu: how on earth do we know? I have had flu several times
in my life and never bothered notifying my GP. I stayed home, isolated myself, and
self-medicated. I suspect most people are the same. So the mortality of flu is limited to
serious cases which comes to GPs' attention and is therefore an underestimate and more like
0.1% or even 0.01% than the claimed 1% as most people will not report it.
Peter
March 8, 2020 at 14:38
This might put things in perspective:
Worldwide, up to 650,000 individuals die from complications of seasonal flu each year.
Take a moment to think about that. We can compare this number with other causes of death
around the globe, like 470,000 people who lose their lives to homicide and many more who do
to suicide. Nearly 1.35 million individuals die each year as a result of car accidents (an
additional 20 to 50 million suffer injuries) ..
https://www.psychologytoday.com/us/blog/finding-new-home/202003/coronavirus-countering-your-fears
nevermind
March 8, 2020 at 14:40
Thanks for a levelled coherent comparison. The hoovering up response of the media is an
obvious news management issue.
... ... ...
There are only two important happenings in all our lives, our birth and our death
everything inbetween is merely filling in time with chaws, multiplying and breathing.
glenn_uk
March 8, 2020 at 21:18
Hah!
James Penn-Dunnett
March 8, 2020 at 17:14
Nice picture Craig, you all look amazingly well.
In August '68 I caught H3N2 while stationed in Hong Kong. I was brought unconscious to the
Gurkha military field hospital in Shek Kong and was kept there until my temperature returned
to normal after a week. There was no attempt at quarantine or to trace victims or any follow
up by the authorities. The HK Police and military were too busy dealing with communists and
illegals crossing from China. Hong Kong Flu then spread to Vietnam via US sailors and other
military who used HK for shore leave from the Vietnam War.
So naturally after that experience and being a 24/7 carer I am taking precautions. No not
bulk buying but plenty of hand washing with soap, minimising people contact and trying not to
cough or sneeze near anyone.
Here are a couple of useful links:
https://mobile.twitter.com/PalliThordarson/status/1236549305189597189
https://threadreaderapp.com/thread/1235127363341553667.html
Tony_0pmoc
March 8, 2020 at 17:52
Another brilliant post by Craig Murray You survived all that, well even a couple of weeks
ago, queuing to get into jail for Julian Assange's trial. You are quite obviously as tough as
old boots. Even the CIA have given up trying to kill you. The Coronavirus, if you get it is
unlikely to have any effect on you.
Read Linh Dinh's too, check out his photography, and buy his book in Hardback – it
has High Definition photos too "Postcards from the End of America". He was born in Vietnam,
about the same age as Craig Murray, and travels around a lot, mostly by bus.
"Sick Days, Market Crash and Shut Borders"
https://www.unz.com/ldinh/sick-days-market-crash-and-shut-borders/
Tony
Patrick Haseldine
March 8, 2020 at 20:11
"Memento Mori – Unpopular Thoughts on Corona Virus" (Corrected by Wikispooks)
Consider this: 100% of those who contract coronavirus are going to die. 100% of those who
do not contract coronavirus are also going to die. The difference in average life expectancy
between the two groups will prove to be only very marginal. That is because the large
majority of those who die of COVID-19 will already be nearing the end of life or have other
health problems.
(
https://wikispooks.com/wiki/Document:Memento_Mori_%E2%80%93_Unpopular_Thoughts_on_Corona_Virus
)
rtah100
March 8, 2020 at 21:22
It is reasonable to be sceptical and phlegmatic (no pun intended), given past pandemics.
The problem with the coronavirus is that:
What that means is that entire healthcare systems will become saturated and people who
might have been expected to live will die from lack of care, not old age. It will be luck of
the draw who lives and diss, unless we agree turn off ventilation on older people in favour
of the young when they have equal survival chances if ventilated . It also means that
noncoronavirus healthcare is overwhelmed and people die indirectly.
With vigorous countermeasures, the peak of infection can be reduced, ideally below
healthcare capacity. 40% peak reduction and 20% mortality reduction was possible in 1918
where implemented. Wuhan measures reduced R0 to 0.3, I.e. Killing transmission in three
serial intervals of infection.
It is a public health and moral imperative not to be fatalistic here, Craig, and your
normal humanism is lacking here.
Roger
March 7, 2020 at 14:39
I for one have not given up, and see plenty of life to experience ahead unlike this bloke.
If it takes me out, at least I can go knowing that I have done everything possible to prevent
it. That will bring comfort. Dying for no good reason does not seem like something good to
dwell on during those last moments. The very fact that this old guy has been able to pen a
coherent and interesting article without the effects of dementia or other old age related
maladies demonstrates that even he has something left to contribute. Although in this case, I
do not agree with his message.
Steve
Hayes
March 7, 2020 at 14:44
The only evidence I have seen of mass hysteria is in the corporate mass media.
Vivian O'Bliviion
March 7, 2020 at 14:55
The American CDC rejected the notion of replicating the WHO approved Coronavirus test, in
favour of developing its own test (resulting in a delayed launch date and continued lag in
delivery). The CDC test is being billed at $1,200 (for those lucky enough to have sufficient
insurance). In S. Korea testing is free if a prospective patient is running a temperature. If
the subject is not running a temperature the test is billed at $120 (presumably this is an
approximation of cost price). Some folks in America are going to make a whole pile of money
out of the situation.
J Arther Nast
March 7, 2020 at 14:59
"The mass hysteria around the current coronavirus is being driven by a societal rejection
of the notion that the human species is part of the wider ecology, and that death and disease
are unavoidable facts, with which it ought to be part of the human condition to come to
terms".
Well Crag that's one theory, buy what about all the other stuff that's going on, reaction
to globalism, extinction, and all the other concerns. This corona virus is a seed falling on
to fertile soil in more ways than one,
Luboš
Motl
March 7, 2020 at 15:07
An excellent, wise text. I wrote a followup athttps://motls.blogspot.com/2020/03/humans-are-part-of-ecosystem.html
James Cook
March 7, 2020 at 16:13
The Swerve: How the Renaissance Began or The Swerve: How the World Became Modern: Stephan
Greenblatt tells the story of how Poggio Bracciolini, a 15th-century papal emissary and
obsessive book hunter, saved the last copy of the Roman poet Lucretius's On the Nature of
Things from near-terminal neglect in a German monastery.
I am with you Craig .. Reading Lucretius's On the Nature of Things will set you free!
Stevie Boy
March 7, 2020 at 15:21
With all the (politically motivated ?) hype, I had a look at the official mortality
figures for our annual common flu.
Fleur
March 7, 2020 at 15:24
Very sensible – and thoughtful – commentary on the latest flu episode Craig.
Thanks.
Your ruminations on the desire for, and even a belief in, the possibility of achieving
immortality (or at least a very long life) are also timely, as these drive pivotal sections
of the policy making and system creating sectors. Julian Assange has spoken about the belief
– prevalent in Silicon Valley – that a world will soon be created where we can
'upload our brains' to the cloud, and so live on forever in whatever fantasy world
appeals.
In the meantime, we live in bodies increasingly beset by toxic pollutants from chemical
additives in water, BigAg food, polluted air, over prescribed drugs, radiation from our
proliferating cellphones & wifi devices, and by stress generated by our loud, over-lit
environment and mean, abusive work environments / economic system.Despite this, many people
would rather panic over a virus than question the factors making us (and our children and
seniors) so susceptible to such viruses.
I too have a lung condition, and have also experienced several very close brushes with
death due to other factors (such as a recent, brutal home invasion). I also have experienced
the deaths of many of the people close to me – people of all ages, from a range of
factors. I suspect that those experiences make people much less afraid of death, and so much
less likely to share the current panic, or to share the very common illusion that we can live
forever – if we just spend enough on "research" and have enough superfoods, expensive
drugs (and vax).
In my view we would all be better off concentrating on making our lives MEAN something
while we have them (as Julian has done) than on obsessing over the latest media-driven
"threat to security" propaganda – be that about a virus or something else.
Sue
March 7, 2020 at 15:34
This is a vey well written and thought provoking opinion piece. However, in this case, I
do believ death and getting in infected, are both avoidable. And because few humans chose to
be irresponsible with their choices, we now have a pandemic. People all around the world are
on edge. Its not ok that millions of people died in the past pandemics, and if there was
enough information back then, those numbers would have been small. Young parents with little
children ear death a lot more than older parents, for obvious reasons. So, it's great if one
doesn't buy into the hysteria, but it's the opposite if such a person becomes the cause for
say, spreading the virus in a school!
Magic Robot
March 7, 2020 at 17:52
"chose to be irresponsible with their choices, we now have a pandemic."
Rely on newspaper, radio and TV warnings; buy into the hysteria; buy masks, wear them at
all times in public, wash hands when entering the shops to buy your food, use cards not cash
to pay, remain indoors until told otherwise, etc. OR ELSE! – Welcome to the new world
of the 'virus police.'
Weechid
March 7, 2020 at 16:54
Thank you Craig, for being a voice of reason. I was just asking if this was any worse than
other flu epidemic or if, for some reason, it was being made to seem so. I've also been
wondering why they gave it another name rather than "flu". Is it just to make it sound more
"scary" because most people don't understand that flu is more than just a bad cold? As far as
I know I am healthy and have very little to fear from this latest flu. I do look after a
relative with COPD and I'm concerned for him – in the same way that I'm concerned for
him every winter as I know flu could kill him. The hysteria is driving me up the wall so it's
good to see that some are remaining calm. The best of health to you, sir.
Mark Russell
March 7, 2020 at 16:54
I sincerely hope the virus outbreak isn't as dire as predicted, but like you, peccavi,
peccabo, *as we see the catastrophic effects of human beings on the environment, including on
other species and the climate*, it makes one wonder if it really is a catastrophe if
predictions are accurate or underestimated..
Nature's schadenfreude – our comeuppance. If it were to be a natural evolutionary
pathogen – but even if proves the stuff of nightmares and the deliberate release of an
engineered virus – would it be a "bad thing" if 99% of humanity was culled?
This feels like the final scenes in "On the Beach" with Gregory Peck. At least they still
had loo paper at the end
Jan Pietrasik
March 7, 2020 at 17:22
We in the Western imperialist nations don't like the idea of death but have no qualms
about delivering death and disease to weaker nations we sanction, bomb, invade, occupy
especially when modern warfare means there is very little risk to ourselves. Millions have
died and continue to die across MENA, many of them children in our never ending wars for
resources and geopolitical advantage sold as 'humanitarian intervention.'
matthew •
15 hours ago
My best friends brother is a physician working in the midwest town in which I live. I asked
him about all of these stories of people stealing things like hand sanitizer from clinics and
he said nothing is any different from what it was 2-3 months month ago. Maybe this is a bad
thing, but It seems that outside of the few areas right now that we are reading about in the
media, most people in this country are treating it like Baton Rouge or the city in which I
live. People in general just are not that worked up by it. I work in an urban school district
in medium size, midwestern city and so far other than a general notice to wash our hands and
not touch our face, nothing has been even talked about in regards to handling a massive
outbreak. Again, in hind sight this could be a huge mistake, but until people see this
touching places across the heartland and reaching into every corner of society it looks like
they will assume its a mostly big city, densely populated area problem. Of course if it
reaches these places it will be too late to do anything, but I guess that is how these things
always work.
AlmostNormalTexan
matthew •
an hour ago
I live in Houston and cannot find a single bottle of hand sanitizer or Clorox wipes on a
store shelf. I have been to grocery stores, Walmart, Target, dollar stores, office supply
stores, Home Depot, drug stores. Everyone is out and nobody who works there has any idea
when their stock will be replenished. Meanwhile prices for the stuff on Amazon have spiked
into the hundreds of dollars.
Funny, I thought conservatives told us that empty shelves and sky-high black market
prices only happen when socialists are in charge.
Jeremy Kee
14 hours ago
The following makes me want to riot:
"They said they would not test me because if I were wearing the recommended protective
equipment, then I wouldn't have the coronavirus."
The CDC is blaming human error - BASED ON CDC GUIDELINES - for the contraction of the
virus? Or is it more like the novel Catch 22 - if you were too mentally unwell to
fly then you were excused from missions, but if you said you were too unwell to fly then
you were clearly well enough to assess your mental health.
Nick Stuart •
5 hours ago
<gallows_humor>At least if we're all gonna die of coronavirus, there's no point in
worrying about climate change.</gallows_humor>
periol
March 6, 2020 at 1:23 pm
Some of my darker thoughts on CV have noted that if this spreads through the country,
Social Security and pension funds will be able to relax, homes will come on the market and
prices will go down, and we could even be looking at generational political turnover.
I'm not wishing for it in the slightest, but the potential is there.
Highly recommended !Creating employment insecurity was the entire point of neoliberal reforms such as
outsourcing, de-skilling and contingent employment. Neoliberal theory had it that desperate
workers work both longer and harder. And they die younger. We can view "Creepy Joe" and Trump as representatives of "neoliberal plague" The slogan
should be " No Pasaran "
( Dolores Ibárruri's famous battlecry appeal for the defense of the Second Spanish
Republic)
Notable quotes:
"... For those who aren't familiar with Albert Camus' The Plague , disparate lives are brought together during a plague that sweeps through an Algerian city. ..."
"... Through the virus, a new light is being shone on four decades of neoliberal reorganization of political economy. The combination of widespread economic marginalization and a lack of paid time off means that sick and highly contagious workers will have little economic choice but to spread the virus. And the insurance company pricing mechanism intended to dissuade people from overusing health care ('skin in the game') means that only very sick people will 'buy' health care they can't afford. ..."
"... If this last part reads like (Ayn) Randian social theory as interpreted by a budding sociopath in the basement of his dead parent's crumbling tract home, it is basic neoliberal ideology applied to circumstances that we can see playing out in real time. ..."
"... While the American response to the Coronavirus threat seems to be less than robust, there was a near instantaneous response from the Federal Reserve to a 10% decline in stock prices. ..."
"... If priorities seem misplaced, you haven't been paying attention. The statistics on suicides, divorces, drug addiction and self-destructive behavior that result from the loss of employment were understood and widely published by the early 1990s, at the peak of that era's round of mass layoffs. Creating employment insecurity was the entire point of neoliberal reforms such as outsourcing, de-skilling and contingent employment. Neoliberal theory had it that desperate workers work both longer and harder. And they die younger. ..."
"... But how likely is it that people will 'demand' too much healthcare? The starting position of Obamacare was that the American healthcare system provided half the benefit at twice the price of comparable systems. ..."
"... Milton Friedman, one of the founders of neoliberalism through the Mont Pelerin Society, produced a long career's worth of half-baked garbage economics. On the rare occasions when he wasn't helping Chilean fascists toss students out of airplanes in flight, he was pawning his infantile theories off on future Chamber of Commerce and ALEC predators. His positivism was already known to be a farce when he took it up. Here is a primer that explains why it is, and always will be, a farce. ..."
For those who aren't familiar with Albert Camus' The Plague ,
disparate lives are brought together during a plague that sweeps through an Algerian city.
Today, by way of the emergence of a lethal and highly communicable virus (Coronavirus), we --
the people of the West, have an opportunity to reconsider what we mean to one another. The
existential lesson is that through dread and angst we can choose to live, with the
responsibilities that the choice entails, or just fade away.
Through the virus, a new light is being shone on four decades of neoliberal
reorganization of political economy. The combination of widespread economic marginalization and
a lack of paid time off means that sick and highly contagious workers will have little economic
choice but to spread the virus. And the insurance company pricing mechanism intended to
dissuade people from overusing health care ('skin in the game') means that only very sick
people will 'buy' health care they can't afford.
Market provision of virus test kits, vaccines and basic sanitary aids will, in the absence
of government coercion, follow the monopolist's model of under-provision at prices that are
unaffordable for most people. The most fiscally responsible route, in the sense of assuring
that the rich don't pay taxes, is to let those who can't afford health care die. If this means
that tens of millions of people die unnecessarily, markets are a harsh taskmaster. (
3.4% mortality rate @
2X – 3X the contagion rate of the Spanish Flu @ 4 X 1918 population).
If this last part reads like (Ayn) Randian social theory as interpreted by a budding
sociopath in the basement of his dead parent's crumbling tract home, it is basic neoliberal
ideology applied to circumstances that we can see playing out in real time. According to
Ryan Grim of The Intercept, Bill Clinton eliminated the ' reasonable
pricing ' requirement for drugs made by companies that receive government funding. This has
bearing on both commercially developed Coronavirus test kits and vaccines.
Leaving aside technical difficulties that either will or won't be resolved, how would any
substantial portion of the 80% of the population that lives hand-to-mouth be effectively
quarantined when losing an income creates a cascade effect of evictions, foreclosures,
starvation, repossessions, shut-off utilities, etc.? The current system conceived and organized
to make desperate and near desperate workers labor with the minimum of pay and benefits is a
public health disaster by design.
While the American response to the Coronavirus threat seems to be less than robust,
there was a near instantaneous response from the Federal Reserve to a 10% decline in stock
prices. The same Federal Reserve that has been engineering a non-stop rise in stock prices
since Wall Street was bailed out in 2009 knows perfectly well how narrowly stock ownership is
concentrated amongst the rich -- it publishes the data. It quickly lowered the cost of
financial speculation as the cost of Coronavirus tests and a vaccine -- and the question of who
will bear them, remain indeterminate.
If priorities seem misplaced, you haven't been paying attention. The statistics on
suicides, divorces, drug addiction and self-destructive behavior that result from the loss of
employment were understood and widely published by the early 1990s, at the peak of that era's
round of mass layoffs. Creating employment insecurity was the entire point of neoliberal
reforms such as outsourcing, de-skilling and contingent employment. Neoliberal theory had it
that desperate workers work both longer and harder. And they die younger.
The brutality of the logic used by the Obama administration in constructing the ACA,
Obamacare, is worthy of exploration. The premise behind the 'skin in the game' idea is
neoliberalism 101, developed by a founder of neoliberalism, economist Milton Friedman, to
ration health care. The basic idea is that without a price attached to it, people will 'demand'
more health care than they need. That from a public health perspective, oversupplying health
care is better than undersupplying it, is ignored under the premise that public health concerns
are communistic. (Read Friedman).
But how likely is it that people will 'demand' too much healthcare? The starting
position of Obamacare was that the American healthcare system provided half the benefit at
twice the price of comparable systems. Through the 'market' pricing mechanism that
existed, the incentive was for people to avoid purchasing healthcare because it was / is wildly
overpriced. Not considered was that through geographical and specialist 'natural monopolies,'
health care providers had an incentive to undersupply health care by providing high-margin
services to the rich.
Furthermore, why would a healthcare system be considered from the perspective of
individual users? In contrast to the temporal sleight-of-hand where Obamacare 'customers' are
expected to anticipate their illnesses and buy insurance plans that cover them, the entire
premise of health insurance is that illnesses are unpredictable. Isn't the Coronavirus evidence
of this unpredictable nature? And through the nature of pandemics, it is known that some people
will get sick and other people won't. Not known is precisely who will get sick and who
won't.
While there are public health emergency provisions in Obamacare that may or may not be
invoked, why does it make sense in any case to require that people anticipate future illnesses?
Such a program isn't health care and it isn't even health insurance. It is gambling. Guess
right and you live. Guess wrong and you die. Why should we be guessing at all? Prior to
Obamacare, health insurance companies gamed the system with life and death decisions. In true
neoliberal fashion, Obamacare randomized the process as health insurers continue to game the
system.
As I understand it, the public health emergency provision in Obamacare might cover virus
testing and the cost of a vaccine if one is ever found. Great. What about care? How many
readers chose a plan that covers Coronavirus? How many days can you go without a paycheck if
you get sick or are quarantined? Who will take care of your children and for how long? How will
you pay your rent or mortgage? Who will deliver groceries to your house and how will you pay
for them? How will you make the car payment before they repossess it and how will you get to
work without it if you recover?
The rank idiocy -- and the political content, of the frame of individual 'consumers'
overusing health care quickly devolves to the fact that some large portion of the American
people can't afford to go to the doctor when they need to. Even if they can afford the direct
costs, they can't afford the indirect costs. When Obamacare was passed, the U.S. had the worst
health care outcomes among rich countries. Ten years later, the U.S. has the
worst healthcare outcomes among rich countries . And medical bankruptcies are virtually
unchanged since Obamacare was passed.
The reason for focusing on Obamacare is it is the system through which we encounter the
Coronavirus. In the narrow political sense of getting a health care bill passed, Obamacare may
or may not have been 'pragmatic.' In a public health care sense, it is a disaster decades in
the making. The problem wasn't / isn't Mr. Obama per se. It is the radical ideology behind it
that was posed as pragmatism. Mr. Obama's success was to get a bill passed -- a political
accomplishment. It wasn't to create a functioning healthcare system.
The otherworldly nature of neoliberal theory has led to a most brutal of social
philosophies. Mr. Obama later put his energy into lengthening drug company
patents to give drug companies an economic advantage provided by the government. Economist
Dean Baker has made a career out of hammering this general point home. Michael Bloomberg
benefited from government support for both technology and finance. His fortune of $16 billion
in 2009 followed stock prices higher to land him at $64.2 billion in 2020.
Donald Trump inherited a large fortune that likewise followed stock and Manhattan real
estate prices higher. Both he and Mr. Bloomberg could have put their early fortunes into
passive portfolios and received the returns that they claim to be the product of superior
intelligence and hard work. Analytically, if the variability of these fortunes tracks systemic,
rather than personal, factors, then systemic factors explain them. The same is true of most of
the great fortunes of the epoch of finance capitalism that began around 1978.
The point of merging these issues is that they represent flip sides of the neoliberal coin.
In a broad sense, neoliberalism is premised on economic Darwinism, the quasi-religious (it
isn't Darwin) idea that people land where they deserve to land in the social order. This same
idea, that systemic differences in economic outcomes are evidence of systemic causes, applies
here. However, differences in intelligence, initiative and talent don't map to systemic outcomes , meaning that
concentrated wealth isn't a reward for these.
The ignorant brutality of this system appears to be on its way to getting a reality check
through a tiny virus. Unless the Federal government figures this out really fast, most of the
bodies will be carried out of poor and working class neighborhoods like mine. Few here have
health insurance and most health care providers in the area don't take the insurance they do
have. More than a day away from work and many of my neighbors will no longer have jobs.
Evictions are a regular state of affairs in good times. There are no resources to facilitate a
larger-picture response.
Liberalism, of which neoliberalism is a cranky cousin, lives through a patina of pragmatism
until the nukes start flying or a virus hits. Getting healthcare 'consumers' to consider their
market choices follows a narrow logic up to the point where none of the choices are relevant to
a public health emergency. One I plus another I plus another I doesn't equal us. The
fundamental premise of neoliberalism, the Robinsonade I, has
always been a cynical dodge to let rich people keep their loot.
The mortality rate and contagion factor recently reported for Coronavirus (links at top)
place it above the modern benchmark of the Spanish Flu of 1918 in terms of potential lethality.
What should make people angry is how the reconfiguration of political economy intended to make
a few people really rich has put the rest of us at increased risk. These are real people's
lives and they matter.
Finally, for students of neoliberalism: there is no conflation of neoliberalism with
neoclassical economics here. Milton Friedman, one of the founders of neoliberalism through
the Mont Pelerin Society, produced a long career's worth of half-baked garbage economics. On
the rare occasions when he wasn't helping Chilean fascists toss students out of airplanes in
flight, he was pawning his infantile theories off on future Chamber of Commerce and ALEC
predators. His positivism was already known to be a farce when he took it up. Here is a primer that
explains why it is, and always will be, a farce.
Rob Urie is an artist and political economist. His book Zen Economics is
published by CounterPunch Books.
Highly recommended !Notes of disaster capitalism in action...
Notable quotes:
"... The Centers for Disease Control and Prevention (CDC) is not billing patients for coronavirus testing, according to Business Insider . "But there are other charges you might have to pay, depending on your insurance plan, or lack thereof," Business Insider noted. "A hospital stay in itself could be costly and you would likely have to pay for tests for other viruses or conditions." ..."
"... Congress needs to immediately pass a bill appropriating funding to cover 100% of the cost of all coronavirus testing & care within the United States. We will not have a chance at containing it otherwise. @tedlieu - as my rep, can you please ensure this is brought up? ..."
"... In the case of the Wucinskis, Kliff reported that "the ambulance company that transported [them] charged the family $2,598 for taking them to the hospital." ..."
"... Last week, the Miami Herald reported that Osmel Martinez Azcue "received a notice from his insurance company about a claim for $3,270" after he visited a local hospital fearing that he contracted coronavirus during a work trip to China. ..."
"... Did anyone expect the unconscionable greed of capitalism to cease when a public health crisis emerges? This is just testing for the virus, wait until a vaccine has been developed so expensive that the majority of the US populace can not afford it at all and people are dropping like flies. Wall Street, never-the-less, will continue to have its heydays ..."
"... The very idea that the defense and "Homeland" security budgets are bloated and additional funding approved year after year but the citizens of this country are not afforded 100% health coverage In a time of global health crisis that could become a pandemic. ..."
"Huge surprise medical bills [are] going to make sure people with symptoms don't get tested. That is bad for everyone." by
Jake Johnson, staff writer Public health
advocates, experts, and others are demanding that the federal government cover coronavirus testing and all related costs after several
reports detailed how Americans in recent weeks have been saddled with exorbitant bills following medical evaluations.
Sarah Kliff of the New York Times
reported Saturday
that Pennsylvania native Frank Wucinski "found a pile of medical bills" totaling $3,918 waiting for him and his three-year-old daughter
after they were released from government-mandated quarantine at Marine Corps Air Station in Miramar, California.
"My question is why are we being charged for these stays, if they were mandatory and we had no choice in the matter?" asked Wucinski,
who was evacuated by the U.S. government last month from Wuhan, China, the epicenter of the coronavirus outbreak.
"I assumed it was all being paid for," Wucinski told the Times . "We didn't have a choice. When the bills showed up, it was just
a pit in my stomach, like, 'How do I pay for this?'"
The Centers for Disease Control and Prevention (CDC) is not billing patients for coronavirus testing,
according
to Business Insider . "But there are other charges you might have to pay, depending on your insurance plan, or lack thereof,"
Business Insider noted. "A hospital stay in itself could be costly and you would likely have to pay for tests for other viruses or
conditions."
Lawrence Gostin, a professor of global health law at Georgetown University, told the Times that
"the most important rule of public health is to gain the cooperation of the population."
"There are legal, moral, and public health reasons not to charge the patients,"
Gostin said.
Congress needs to immediately pass a bill appropriating funding to cover 100% of the cost of all coronavirus testing & care
within the United States. We will not have a chance at containing it otherwise.
@tedlieu - as my rep, can you please ensure this
is brought up?
-- William LeGate (@williamlegate)
March 2, 2020
In the case of the Wucinskis, Kliff reported that "the ambulance company that transported [them] charged the family $2,598
for taking them to the hospital."
"An additional $90 in charges came from radiologists who read the patients' X-ray scans and do not work for the hospital," Kliff
noted.
The CDC declined to respond when Kliff asked whether the federal government would cover the costs for patients like the Wucinskis.
The Intercept 's Robert Mackey
wrote
last Friday that the Wucinskis' situation spotlights "how the American government's response to a public health emergency, like trying
to contain a potential coronavirus epidemic, could be handicapped by relying on a system built around private hospitals and for-profit
health insurance providers."
We should be doing everything we can to encourage people with
#COVIDー19 symptoms to come forward.
Huge surprise medical bills is going to make sure people with symptoms don't get tested. That is bad for everyone, regardless
of if you are insured. https://t.co/KOUKTSFVzD
-- Saikat Chakrabarti (@saikatc)
March 1, 2020
Play this tape to the end and you find people not going to the hospital even if they're really sick. The federal government
needs to announce that they'll pay for all of these bills https://t.co/HfyBFBXhja
Last week, the Miami Herald reported
that Osmel Martinez Azcue "received a notice from his insurance company about a claim for $3,270" after he visited a local hospital
fearing that he contracted coronavirus during a work trip to China.
"He went to Jackson Memorial Hospital, where he said he was placed in a closed-off room," according to the Herald . "Nurses
in protective white suits sprayed some kind of disinfectant smoke under the door before entering, Azcue said. Then hospital staff
members told him he'd need a CT scan to screen for coronavirus, but Azcue said he asked for a flu test first."
Azcue tested positive for the flu and was discharged. "Azcue's experience shows the potential cost of testing for a disease
that epidemiologists fear may develop into a public health crisis in the U.S.," the Herald noted.
Sen. Bernie Sanders (I-Vt.), a 2020 Democratic presidential candidate, highlighted Azcue's case in a tweet last Friday.
"The coronavirus reminds us that we are all in this together," Sanders wrote. "We cannot allow Americans to skip doctor's visits
over outrageous bills. Everyone should get the medical care they need without opening their wallet -- as a matter of justice and
public health."
Last week, as Common Dreams
reported , Sanders argued that the coronavirus outbreak demonstrates the urgent need for Medicare for All.
The coronavirus reminds us that we are all in this together. We cannot allow Americans to skip doctor's visits over outrageous
bills.
Everyone should get the medical care they need without opening their wallet -- as a matter of justice and public health.
https://t.co/c4WQMDESHU
-- Bernie Sanders (@SenSanders)
February 28, 2020
The number of confirmed coronavirus cases in the U.S.
surged by more than two
dozen over the weekend, bringing the total to 89 as the Trump administration continues to
publicly downplay the severity of the outbreak.
Dr. Matt McCarthy, a staff physician at NewYork�Presbyterian Hospital,
said
in an appearance on CNBC 's "Squawk Box" Monday morning that testing for the coronavirus is still not widely available.
"Before I came here this morning, I was in the emergency room seeing patients," McCarthy said. "I still do not have a rapid
diagnostic test available to me."
"I'm here to tell you, right now, at one of the busiest hospitals in the country, I don't have it at my finger tips," added
McCarthy. "I still have to make my case, plead to test people. This is not good. We know that there are 88 cases in the United
States. There are going to be hundreds by middle of week. There's going to be thousands by next week. And this is a testing issue."
Our work is licensed under a Creative Commons Attribution-Share Alike 3.0 License. Feel free to republish and share widely.
Harry_Pjotr
13h
Did anyone expect the unconscionable greed of capitalism to cease when a public health crisis emerges? This is just testing
for the virus, wait until a vaccine has been developed so expensive that the majority of the US populace can not afford it at
all and people are dropping like flies. Wall Street, never-the-less, will continue to have its heydays
Smerl fern 12h
A wall street bank or private predator may own your emergency room. A surprise bill may await your emergency treatment above
insurance payments or in some instances all of the bill.
An effort was made recently in congress to stop surprise billings but enough dems joined repubs to kill it. More important
to keep campaign dollars flowing than keep people alive.
fern Smerl 12h I know emergency rooms are being purchased by organizations like Tenet (because they are some of
the most expensive levels of care) and M.D.s provided by large agencies. I'm not as up on this as I should be but a friend of
mine tells me that some of this is illegal. I have received bills that were later discharged by challenge. This is worth investigating
further. Atlas oldie 11h Hmmmm A virus that
overwhelmingly kills the elderly and/or those with pre-exisitng conditions.
Sounds like a medical insurance companies wet dream. As well as .gov social security/medicare wet dream.
Just sayin'
Ticki
11h
The very idea that the defense and "Homeland" security budgets are bloated and additional funding approved year after year
but the citizens of this country are not afforded 100% health coverage In a time of global health crisis that could become a pandemic.
And as has been stated, the unconscionable idea suggested that a possible vaccine (a long way away or perhaps not developed at
all) might not be affordable to the workers who pay the taxes that fund the government? That's insane.
leftonadoorstep
11h
Another example of "American Exceptionalism." China doesn't charge its coronavirus patients, neither does South Korea. I guess
they are simply backward countries.
Barton
11h
I own my own home after years of hard work paying it off. It's the only thing of value, besides my old truck, that I have.
If I get the virus, I will stay home and try to treat it the best I can. I can't afford to go to the hospital and pay thousands in
medical bills, with the chance that they'll come after my possessions. America, the land of the _______. Fill in the blank. (Hint:
it's no longer free).
fern
1 Barton
11h
There are other ways to protect your home. Homesteading or living trust. I'm not good at this but I know there are ways to
do it. Hopefully, it would never come to that but outcomes are not certain even with treatment in this case.
Giovanna-Lepore oldie 11h
As someone
who lost a mother at 5 years old I can sympathize with your grief in losing a daughter-in-law and especially seeing her four children
orphaned. However, I think you miss the point here: This is about we becoming a society invested in each others welfare and not a
company town that commodifies everything including the health and well being of us all.
fern
1 Giovanna-Lepore
11h
I'm going by: https://www.congress.gov/bill/116th-congress/senate-bill/1129/text
As a revision it is better but flawed. It is a cost containment bill based on the same research as the republican plan with global
budgets and block grants.
Edited: I encourage you to read this:
Giovanna-Lepore
10h oldie:
Part D
Higher education is not free but they do need to become free for the students and payed by us as a society.
Part D is a scam, a Republican scam also supported by corporate democrats because of its profit motive and its privatization
Medicare only covers 80% and does not cover eye and dental care and older folks especially need these services. Medicaid helps but there are limits and one cannot necessarily use it where one needs to go.
Expanded, Improved Medicare For All is a vast improvement. because it covers everyone in one big pool and, therefore, much more dignified
than the rob Paul to pay peter system we have.
Social Security too can be improved. Why should it simply be based on the income of the person which means that a person working
in a low paying job in a capitalist system gone wild with greed will often work until they die.
Pell grants can be eliminated when we have what the French have: publicly supported education for everyone.
The demise of unions certainly did not help but it was part of the long strategy of the Right to privatize everything to the enrichment
of the few.
Yunzer SuspiraDeProfundis 10h
Thank
goodness for the "/s". Poe's Law you know
The overall competence that Canada is handling this outbreak, compared to the USA, is stark. First world (Canada) versus third-world
(USA). Testing is practically available for free, to any suspect person, sick or not, as Toronto alone can run 1000 tests a day and
have results in 4 hours. That is far more than all the US's capacity for 330 million people.
I wonder how long before Canada closes its borders to USAns? Me and my wife (both in a vulnerable age/medical group) should seriously
consider fleeing to my brother's place in Toronto as the first announced cases in Pittsburgh are probably only days away. What about
our poor cat though? We could try to smuggle her across the border, but she is a loud and talkative kitty
Greenwich
10h
Don't want to discourage anyone from any protective measures � but the
"low down" from my veggie store today was that a lot of health professionals
shop there and they think it's being hyped by media. Did get this from my NJ Sen. Menendez �
Center for Disease and Control and Prevention (CDC)
There is currently no vaccine to prevent coronavirus disease 2019 (COVID-19). The best way to prevent illness is to avoid being
exposed to this virus. However, everyday preventive actions can help prevent the spread of respiratory diseases:
Wash your hands often
Avoid close contact with people who are sick.
Avoid touching your eyes, nose, and mouth.
Stay home when you are sick.
Cover your cough or sneeze with a tissue, then throw the tissue in the trash.
For more information : htps://www.cdc.gov/coronavirus/2019-ncov/about/prevention-treatment.html
How it spreads : The virus is thought to spread mainly from person-to-person. It may be possible that a person can get
COVID-19 by touching a surface or object that has the virus on it and then touching their own mouth, nose, or possibly their
eyes, but this is not thought to be the main way the virus spreads. [Read more.]https://www.cdc.gov/coronavirus/2019-ncov/about/transmission.html )
Symptoms : For confirmed coronavirus disease 2019 (COVID-19) cases, reported illnesses have ranged from mild symptoms to
severe illness and death. Symptoms can include fever, cough, and shortness of breath.
Seeker
9h Greenwich:
Don't want to discourage anyone from any protective measures � but the
"low down" from my veggie store today was that a lot of health professionals
shop there and they think it's being hyped by media.
I agree it is being hyped by the media to the point of being fear mongering. At the same time it is being ignored by the administration to such an extent that really little almost nothing is being done. At some point the two together will create an even bigger problem.
It is like the old adage: "Just because you are paranoid doesn't mean they aren't out to get you." Each over/under reach in considering the reality of the situation has its own problem, which multiply when combined. Every morning when I wake up I say a little atheistic prayer to myself before I get out of bed: "Another day and for better or
worse...".
Seeker
8h
Well, two reported here in Florida tonight. One in my county, one in the county next door. And more of the "we already knew, but told you late". One person checked into the hospital on Wednesday. We hear it Monday night.
Both were ignored far a long time it seems, and 84 in particular are being watched (roommates, friends, hospital workers not alerted
for several days, the usual). But no one knows every place they had been since becoming infected.
Oh, and they have tested a handful of people. No worry?
I can't see anyway that this level of incompetency is an accident. Spring break is just starting usually a 100's of thousand tourist
bonanza.
So the question is do they want to kill us, or just keep us in fear?
I think the later. But the end result is a crap shoot. So once again, it is a gamble with our lives.
Archie1954
7h
The business of America is business. Sometimes that can go too far and this is one of those times. Making money from the loss,
distress, harm and suffering of others is perverse beyond belief.
Highly recommended !An excellent, if technical video from 27 Feb. The speaker is a HK Chinese (English speaking)
Epidemiologist.
He point out "family clustering" of Chinese cases and most cases originating from Hubey
province, not local clusters. He also pointed out the Wuhan has large cluster of old
population.
John Snow Lecture Theatre, LSHTM
WHO Collaborating Centre. The University of Hong Kong Center for Infectious Disease
Epidemiology and Control
Highly recommended !Notable quotes:
"... the official Chinese numbers as unreliable, with large error bars in unpredictable directions. Look to South Korea and Singapore for reliable data; both are actively and aggressively testing, and both are strong open information societies. ..."
It is possible that a known pharmaceutical called remdesivir
inhibits the reproduction of the Covid-19 coronavirus. It inhibits (some) RNA dependendent RNA Polymerases -- the type of enzyme
the virus uses to replicated its genome and express its genes. It is
known that it is a potent inhibitor of the
RNA dependendent RNA Polymerases used by the MERS coronavirus
update: here is a good site for Covid-19 data.
likbez , March 2, 2020 6:51 pm
> The risk of business as usual is a small chance of tens of millions of deaths, because drug shortages prevent effective
control of the epidemic
Does not look this way. In China epidemic is almost over with mortality between 2 and 3%. Cases in other countries has mortality
on 0.1% much like for a regular flu.
I think chances of infection of a billion people are non-existent. Trump might have a point that spring can help -- coronaroviruses
worst period of spreading is winter (although there are exceptions)
As the virus is very similar (I think 80% of the genome) to chicken flu the creation of vaccine is possible. Israeli scientists
claim that 'In a few weeks, we will have coronavirus vaccine'
https://www.jpost.com/HEALTH-SCIENCE/Israeli-scientists-In-three-weeks-we-will-have-coronavirus-vaccine-619101/
[BUT] after scientists sequenced the DNA of the novel coronavirus causing the current worldwide outbreak, the MIGAL researchers
examined it and found that the poultry coronavirus has high genetic similarity to the human one, and that it uses the same
infection mechanism, which increases the likelihood of achieving an effective human vaccine in a very short period of time,
Katz said.
"All we need to do is adjust the system to the new sequence," he said. "We are in the middle of this process, and hopefully
in a few weeks we will have the vaccine in our hands. Yes, in a few weeks, if it all works, we would have a vaccine to prevent
coronavirus."[.]
"Given the urgent global need for a human coronavirus vaccine, we are doing everything we can to accelerate development,"
MIGAL CEO David Zigdon said. The vaccine could "achieve safety approval in 90 days," he said.[.] (emphasis added)
I think the danger of the pandemic was exaggerated. In no way this is a new Spanish flu. Not even close.
Which means chances of tens million of more death are very exaggerated, highly unrealistic estimate.
Robert Waldmann , March 2, 2020 7:04 pm
There is no basis for the 0.1% death rate outside of China assertion. The ratio of deaths to cases is greater than that and
many people are in serious or critical condition. The death rate is not statistically signficantly higher in China than in other
countries. https://www.worldometers.info/coronavirus/
Other countries have neither the public health competence nor the ruthlessness of China (I am thinking mostly of other developing
countries but the USA does seem to have problems with testing kits).
A candidate vaccine will be available soon. It will not be proven safe and effective and then mass produced soon. The argument
that it is better to consider costs and benefits and not stick to the rule that first second and third do no harm applies to vaccines
much more than to remdesivir (known to be safe can be quickly tested for effectiveness).
All experts agree that a vaccine will be available in a year or two. They know that candidate vaccines will exist soon. They
know that the problem is proving safety and effectiveness and then producing a lot. A vaccine could be available in much less
than a year. It would be used well within a year if people listened to me. But they won't.
It probably won't be like the Spanish Flu, because of vigorous quarantine type counter measures. A vaccine will help, but could
be too late for tens of millions. Remdesivir will probably work and this will be proven fairly soon. I will probably make a difference.
It could make a larger difference.
Erik , March 2, 2020 8:02 pm
All commenters: please note that official numbers from China are almost certainly inaccurate, both in numerator and denominator.
The total number of cases diagnosed is limited by test kits, which have recently moved from 300 kits manufactured per day to
4000 kits/day. Which is still at least an order of magnitude lower than the number of known cases. And anecdotal data coming from
Chinese physicians and health workers indicates both a higher patient population than official, and many deaths not attributed
to Covid (an epidemic of "pneumonia" deaths in Wuhan preceding the announcement of Covid, for example). Much is being hidden –
not from us, they don't care about us; they're hiding the information from their own people, which they do as a general policy
on most subjects.
Which is all mostly to say, treat the official Chinese numbers as unreliable, with large error bars in unpredictable directions.
Look to South Korea and Singapore for reliable data; both are actively and aggressively testing, and both are strong open information
societies.
likbez , March 2, 2020 9:43 pm
> There is no basis for the 0.1% death rate outside of China assertion
Low mortality rate for COVID-19 is masked by high (15%) mortality rate of persons over 80.
For people younger then 40 it is a reasonable assertion as deaths concentrate on the age group starting from 50-59. Men are
approx. twice more susceptible then women.
Case-Fatality Rates (CFR) China by Age as of 2/11/20
Per country currently the worst in 4.4% (Iran.) With 8,000-Plus deaths in US alone, flu is far more deadly than the coronavirushttps://gisanddata.maps.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6
The most cruel experiment was with the Diamond Princess cruise ship (close space, high level of contact between passengers,
lack of qualified medical personnel and supplied, etc)
Six people died and 700 people were infected out of 3700. For all other the immune system managed to kill the virus. Which
suggests susceptibility rate of around 20%. It suggests 0.2% mortality
Two Japanese passengers – an 87-year-old man and an 84-year-old woman – were the first to die from the disease on February
19.
In the USA out six deaths at least four have been among residents of a long-term care facility called Life Care Center, where
more than 50 residents and staff members have shown symptoms of the virus.
Only 14% of cases are more severe then a regular flu:
Spectrum of disease (N = 44 415)
I believe your hypothetic case about the possibility of the pandemic with high mortality rate is without merit.
We do not need to contribute to the panic, which already started in the USA with population buying masks, isopropyl alcohol
and hand sanitizers as if there no tomorrow (a friend told me that bottle of hand sanitizer on Amazon today in $60 or so ;-).
And masks are effective mostly for sick people (block spreading of infected aerosol from lungs) , mush less for healthy people
as they do no follow proper decontamination procedures anyway.
BTW in China epidemics is already subsiding. Again only 14 percent of cases are severe (which means more serere than a regular
flu):
The health ministry on Tuesday announced just 125 new cases of the virus detected over the past 24 hours, the lowest number
since authorities began publishing nationwide figures on Jan. 21. Another 31 deaths were reported, all of them in the hardest-hit
province of Hubei. The figures bring China's total number of cases to 80,151 with 2,943 deaths.
China's U.N. ambassador says the government believes that "victory" over the coronavirus won't be far behind the coming
of spring.
Geo February
27, 2020 at 2:36 pm
"The 20th century model of [pandemic] containment was protecting lives. The 21st century
model is protecting markets."
https://twitter.com/jonst0kes/status/1233088857060626433?s=21
At a news conference Wednesday, the president announced that the president was doing a
wonderful job handling the coronavirus, a statement that filled me with confidence, as it came
from the president himself. The vice president and HHS head also announced that the president
was doing a great job, and the president, at that point, officially put the vice president in
charge of coordinating the outbreak response.
...What's best is that even if he gets overwhelmed, Jared Kushner is there, a man who can be
counted upon to provide
a solution to any issue , no matter how complicated.
... ... ...
"I want you to understand something that shocked me when I saw it," the
president said at Wednesday's news conference. " I think most people are amazed to hear it.
The flu in our country kills from 25,000 people to 69,000 people a year. That was shocking to
me." This is just a sign of how the president is working carefully to understand the issue!
Once his great brain is applied to it, we need fear nothing.
Also, we do not need to worry
about the cuts to health programs his budget was asking for; we can always hire more doctors!
Once we hire them, it will turn out that they have been working on the virus for months and
developing expertise in combating it. Passionately, in their spare time, the same way the
response was being coordinated.
Highly recommended !
likbez , February 27, 2020 10:57 pm
There is a silver lining in any dark cloud.
Trump might not survive the Coronavirus, literally (he is over 70 and has a high range of
contacts; the mortality to this age group is close to 10%), or figuratively as voters might
not forgive him inadequate and/or incompetent response (which is given) .
Unfortunately, Bernie is at even higher risk as mortality for 80+ is over 15%, and
pre-existing cardiovascular disease is a serious negative factor.
One can wonder if this will be " Straw that broke the camel's
back " for Trump. With 10% drop of S&P500 (aka "correction") it is difficult to
talk about booming economy on rallies ( 20% decline marker defines a recession and some
stocks -- like oil sector are already in this territory ). High yield bonds are also going
down, although more slowly. Now suddenly, Trump has nothing to talk about on his rallies, and
he knows it.
A part of rich retirees who are overexposed to stocks constitutes a sizable part of
remaining avid "Trumpers" voter block (kind of double stupidity, if you wish :-) , and some
of them might not forgive Trump the liberty of depriving them honestly earned in 2019 ~10% of
their 401K accounts.
IMHO troubles for Trump just started. Being incompetent DJT and his merry band of grifters
will almost definitely botch the response.
They already made three blunders.
1. When asked if, and when, a vaccine is produced, would the vaccine be affordable to
everyone? They replied; We'll let the "market" decide that. And some part of electorate
probably noted that.
2. The last December, they cut the budget for the CDC (center for disease control).
3. They exposed government workers to the virus without any need to do that, only due to
bureaucratic incompetence:
https://science.slashdot.org/story/20/02/27/2353236/us-health-workers-responding-to-coronavirus-lacked-training-and-protective-gear-whistle-blower-says
In this sense appointing Pence as the head of the coronavirus response may be a smart move
by Trump. When and if the pandemic hits big time, exposing the mass incompetence and
unpreparedness of the US government, in combination with the tanking of the stock market,
Trump can, of course, blame Christian Zionist neoconservative Israeli apartheid supporter
Pence for his troubles :-)
But, unfortunately, that will not do him any good.
Paraphrasing Chomsky: When the press focuses on the health status of the population reach
for your pocket, and see who's pulling out your wallet.
Tim Jenkins
Oh well, studying the stats, at first glance, this looks like a sound chemical attempt to
resolve the pension fund crisis
Excuse the skeptic, now withdrawing gracefully.
Gall
If I was being cynical I'd agree.
RobG
Many people are speculating that this coronavirus malarky is all about the coming global
financial meltdown.
The way coronavirus is being mega fear hyped, along with unprecedented 'lock-downs' and
enforced quarantine for huge numbers of people, does seem to suggest that the psychopaths who
rule us know that when the global financial meltdown comes there'll be mega civil unrest, and
what better way to control this unrest than a Frankenstein bug?
Highly recommended !Notable quotes:
"... There currently 80,348 cases, or 0.000011% of the global population. Over 77,000 (97%) cases, and 2664 deaths (98%) are from China, and a large portion of those were "clinically diagnosed" (ie. untested). The 2707 deaths (allegedly) due to Coronavirus mean it has death rate of just 3.4%. (For cases outside China, that number drops to 1.6%) Conversely, over 40,000 cases are considered mild, and over 27,000 have been cured. ..."
"... Some (including US Secretary of State Mike Pompeo ) are claiming the disease is being under-reported by China (and Iran), and the panic is a response to much more alarming but hidden statistics. ..."
"... similar claims were made about SARS, Swine Flu and all the other non-event overhyped 'death bugs' we have been told about in recent times. ..."
"... At this stage, it might seem more likely that 'new CV' is just another one of these. The latest scare tactic being used to close down rational thinking in the world populace and normalise increased government control. ..."
"... coronavirus is definitely being used to spread and deepen Sinophobic hatred, by organisations of Evil like the villainous BBC. ..."
In Hubei Province, China, where the 'new' virus was first diagnosed, and where the vast majority of the cases have occurred, it's
no longer considered necessary to test for the presence of CV antibodies before diagnosing the disease.
Let's say that again.
The epicentre of the so-called new virus outbreak is currently diagnosing new cases of the disease without testing for the
virus.
Instead they are relying on 'clinical diagnosis'
, which is defined as [our emphasis]:
The estimated identification of the disease underlying a patient's complaints based merely on signs, symptoms and medical history
of the patient rather than on laboratory examination or medical imaging.
Which means physicians look at presenting symptoms and make a guess on what is causing them.
Now if you're talking about something like Smallpox that option can make some sense � because Smallpox presents with one very
distinct clinical feature � a recognisable rash � that makes it fairly easy to distinguish from other viral agents or other disease
processes.
But the 'new' coronavirus does not do that. In fact, symptoms of the 'new' CV are exactly like symptoms of the numerous 'old'
CVs, and indeed of the common cold or flu. Cough, fever, malaise, upper respiratory tract inflammation and (in severe cases) lung
involvement � up to and including full-blown pneumonia.
The only way to differentiate a case of 'new' CV from severe regular flu, viral pneumonia or even environmental lung disease,
is by testing for antibodies. If they aren't doing this, physicians in Hubei Province are now at grave risk of essentially diagnosing
every single case of pneumonia or lung inflammation they see as the new CV.
Which goes quite a long way to explaining the sudden increase in cases [our emphasis]:
China's Hubei province reported an additional 242 deaths and 14,840 new cases as of Feb. 12 -- a sharp increase from the previous
day. The province said it is starting to include "clinically diagnosed" cases in its figures and that 13,332 of the new cases
fall under that classification .
By CNBC's figures, fully
89% of the "new cases" reported in Hubei province have never been tested for the virus .
According to Our World in Data , roughly 180,000 people die
of pneumonia in China every year. Under this new system, all of those people could be diagnosed with coronavirus .
Further, "signs of pneumonia" don't have to be a sign of any disease at all. Pneumonic symptoms can come simply as the result
of
being
exposed to a heavily polluted air , something very common in China's densely populated urban centres.
A major question here has to be � why? Why take a step that inevitably increases the number of false positives? Why intentionally
inflate the apparent caseload? What rational benefit can there be in that?
Is it some form of hyper-caution? They would rather throw the net too wide than risk missing cases?
Or is it, as Jon Rappoport suggests , a cynical bid to drive up
the numbers in pursuit of ever-valuable fear porn?
That this alleged outbreak is being used to promote fear as a backing for a number of control-based agendas is undeniable, and
we have already pointed this out in previous articles
(not to mention the financial
aspect ). The simple truth is that the reality of this 'new' virus, even as defined by those promoting panic, does not merit
the fear being sold to us on its behalf.
Here are some stats for you, compiled by Kit Knightly.
There currently 80,348 cases, or 0.000011% of the global population. Over 77,000 (97%) cases, and 2664 deaths (98%) are from
China, and a large portion of those were "clinically diagnosed" (ie. untested). The 2707 deaths (allegedly) due to Coronavirus mean
it has death rate of just 3.4%. (For cases outside China, that number drops to 1.6%) Conversely, over 40,000 cases are considered
mild, and over 27,000 have been cured.
For the sake of further reassurance, study these tables:
<table omitted -- see the original for full text>
Essentially, unless you are either elderly or already sick, there's very little chance you are in danger.
On what rational basis can a disease with this profile possibly justify the government and media response worldwide? Are we really
approaching a
"tipping point" ? Does this sound like a
"public health emergency" ?
Why is Italy going into lockdown and
granting itself
"emergency powers" based on seven deaths from a disease with a mortality rate about the
same as severe regular flu ?
Why has the UK government
granted itself similar powers based on a disease that has infected only
13 citizens, 8 of whom are already recovered ?
Why are
hotels and
cruise ships
being quarantined?
Some (including US Secretary of State
Mike Pompeo ) are claiming the disease is being under-reported by China (and Iran), and the panic is a response to much more
alarming but hidden statistics.
Well, that is possible of course. But similar claims were made about SARS, Swine Flu and all the other non-event overhyped
'death bugs' we have been told about in recent times.
At this stage, it might seem more likely that 'new CV' is just another one of these. The latest scare tactic being used to
close down rational thinking in the world populace and normalise increased government control.
That the Chinese government might be party to any such idea might seem unthinkable to those who like their geopolitics simple
and binary, but can't be rationally excluded.
Time will tell of course. But if � as we consider overwhelmingly likely � this 'new' scare bug turns out to have been as overhyped
as all the rest, maybe those panicking in our comments and elsewhere will learn a valuable lesson, and decline to play along with
this particular sick little game next time?
Tutisicecream
Thank god for a bit of sanity in all of this Kit and Catty.
Perception management is clear in all of this. Remember..Sadam's weapons of mass destruction [the front and then the back story]?
Then of late it's all been gathering pace the problem being where to start and where to finish.
So here's a sample: Maidan revolution in Ukraine [really a coup]; MH-17 an enquiry hijacked; Assad with his daily gassing of
his people and the epic survival of the last hospital in Aleppo; Little Bana and her amazing communication skills; Russian hackers
with the help of Putin running [or should that be ruining] the WW media; Novichok and the Porton Down disaster scenario. No ducks
died but 2 Russian's disappeared into Her Majesties safe custody never to be heard of again. And then in broad Day light Julian
Assange abducted into a Kangaroo court of epic proportions.
Coronavirus may just be the experimental excuse to close descent down.
Answendi Lee
I am an Asian Australian man originally from Indonesia. I have been to China once for a period of a month 20 years ago and have
not left Australia for over a year now. Yesterday, a woman covered her nose and mouth with her hand on the footpath as she approached
me about 4-5m from me and uncovered her orifices again 4-5m after she had passed me. Hysteria, you said? It's simply dumb, brainless,
and downright racist and all other idiotic phobias combined!
John Thatcher
A sane and sensible piece, thank you
Antonym
The Chinese government might even cause
deaths with their wild cat quarantines. It does look hysterical; XR could learn a thing or two from that in the run up to the
End of their World in 2029.
This Corona flu does fill up the headlines in the MSM, so I have to wonder what are they trying to hide this time? First guess:
the dire fundamentals of the US stock markets blown totally out of proportions by Quantitative Easing (=blind fiat money printing)
and stock buybacks. That would undermine the status of the US dollar; which would undermine the US an Chinese billionaires getting
even richer from stocks in dollars, plus the limitless funds for the CIA and the MIC.
Gall
Gee what a surprise? Pharma stock took off like a rocket but the strange thing was they were starting to trend upward prior to
the coronavirus. Either they've got shareholders who are psychics or there's something else going on. As they say criminals always
leave clues at the scene of the crime just like those "unfortunately lucky investors" on 9/11.
Fair dinkum
The $$$$$$$$$$$hark$$$$$$$$$$$$
Dungroanin
Fucking brilliant
'Cutting-edge tech to combat COVID-19 virus. 3D-printed protective gear, developed by Beijing University of Chemical Technology,
has reportedly been produced to combat the disease, and it is expected to aid in realizing mass production.'
I finally have a reason to get a 3D printer � maybe I can knock up a tin foil hat to stop all the bs frying my brain and gonads.
Dungroanin
Btw
COVID-19 infection of different severity, according to WHO
-- �
Hubei province figures are approaching 4% if all deaths are proved to be nCov � not just Covid.
binra
In case they were not seen before: http://theinfectiousmyth.com/book/CoronavirusPanic.pdf
http://theinfectiousmyth.com/book/coronavirus.mp3
http://theinfectiousmyth.com/book/SARS.pdf
Jon Rappoport takes a more socio-political critique of mind-control approach � IE there may very likely be political agenda
using the virus as cover story for very bad air pollution (Wuhan) and probable citizen unrest. https://www.youtube.com/watch?v=bBoy9MXRCSE
As he points out there are also huge money interests involved in captured revenue streams and a leverage of globally applied
martial law and ability to disregard human rights.
None of it makes any scientific sense if you actually look at it.
This 'highly infectious disease' operates by publicity and hysteria.
Shock testing systems is part of refining them as well as conditioning the institutions and subjects to being medically compliant.
Question the root definitions by which these stories are invested with fear � and thus with power of 'protection'.
Real nursing � and an understanding of the body's healing processes � and underlying psychic-emotional condition � is health
support.
Post-truth means narrative dictate � as a sealed system with no user access.
And yes � the tipping point is the targeted population by fear and division � and nothing to do with a runaway greenhouse.
Many accept lies that seem to serve their 'side' or funding, career or security and privilege. But once precedents are set or
legislation passed � anything can then be inserted. IE mandating and regulating everything via an IoT and a trained network of
incentivised spying.
Going right down to our core values may not seem 'activism' but unless we defuse the fear-mind, it operates as if it is our
own thinking � and with a few suggestions can be noceboed to hopelessness and surrender of life to despair.
Fear (thinking) is contagious to the unwary and runs as invisible code on an already hacked mind.
The human world could be crashing to destruction � or we can be on a crash course of re-evaluatiing everything to discern truth
� so as to have a basis for NOT running on lies that inherently operate destructive agenda to living and sharing in anything true.
We are all going to die � in terms of this particular focus � sooner or later � anyway.
Tim Jenkins
Oh well, studying the stats. , at first glance, this looks like a sound chemical attempt to resolve the pension fund crisis
Excuse the skeptic, now withdrawing gracefully. 🙂
Dungroanin
3:11 pm Feb 25
South Korea vows to test 200,000 sect members as a wild coronavirus outbreak fear hit the country. The Shincheonji Church of
Jesus, the sect, has agreed to provide the authorities with the names of all its members in the country.
East China's Anhui, downgraded its COVID-19 emergency response level from the highest to the second level, becoming the seventh
region to lower its emergency level in recent days, indicating visible results from the prevention and control work.
Thom
Yes, the headlines seem completely out of proportion to what has actually happened.
It strikes me with the coronavirus scare that either the intention is to stir up panic and cause stock markets to crash (thereby
reducing asset prices for wealthy buyers during the brief window before a cure is 'found'); or the markets/world economy were
going to crash anyway and the powers that be need to an excuse for the events that does not involve political or financial incompetence.
RobG
Well, we both posted at about the same time, and we both have a similar take on it all.
I would say that the psychopaths who rule us probably don't want the markets to collapse, but who knows?
Dungroanin
It's been a bubble heading for correction � a black swan is a good excuse to scalp all who piled in on 'record highs'
Schiller index has been blinking red for quite a while.
I'm waiting for 'correction' event before piling back in � cash is king now and for these hardy enough a bear punt! But not
being a algo investor or having a hedge fund I'll stick with my amateur efforts that are based on fundamentals.
RobG
Many people are speculating that this coronavirus malarky is all about the coming global financial meltdown.
The way coronavirus is being mega fear hyped, along with unprecedented 'lock-downs' and enforced quarantine for huge numbers
of people, does seem to suggest that the psychopaths who rule us know that when the global financial meltdown comes there'll be
mega civil unrest, and what better way to control this unrest than a Frankenstein bug?
DavidKNZ
Just back from China; we had intended to spend Kiwi and Chinese NY wandering round.
In Shenzhen, the place was shuttered for the Autumn Festival, double shuttered for the Corona Virus so I had explore time.
Scanning the 300 TV channels for the Chinese POV, I was impressed by Xi Jingping claiming leadership of the countries response.
If he fails, he's gone, and he knows it. There was a lot of emphasis on a united response and many examples of individuals placing
the needs of the community over their own.
Simultaneously I had access to the western media via cellphone roaming. A different world. Pretty much never miss a chance
to knock China, either by innuendo, mis reporting or straight falsity. I suppose its nothing new, but disappointing in view of
the concerted, organised and substantial efforts made by PRC to protect its people. What would have been the outcome if the virus
had emerged in India??
Coming back, many airlines cancelled. Finally got to HongKong (via 6 temperature checks, 4 police checkpoints ) before the
borders were closed. 4 hours later and we would have been detained in HKG, probably in one of the centers subsequently torched
by HKG Chinese.
Back to the Land of the Long White Shroud, we were greeted by two nurses manning a small table.
So the Chinese can build 2 hospitals in less time than it takes the NZ health system to organise a useful website.
Dungroanin
The western hysteria is about the imperialists global robber barons not ever letting a good crises going to waste.
For profit. Or to sweep a bunch of crap under the carpet.
This for instance is a classic piece of unreported in western media skullduggery:-
'"biggest tax heist in Germany", kicked the financial institution's longtime chairman, Christian Olearius, as well as co-owner
Max Warburg, a direct descendant of the founders, out of their board roles, and reportedly cost the German authorities at least
10 billion euros in lost budget revenues.'
https://sputniknews.com/business/202002251078403160-jewish-bank-that-survived-hitler-embroiled-in-germanys-biggest-tax-heist --
reports/
paul
It could be they have moved to "clinical diagnosis" because the existing CV test is only about 50% effective. But you have to
expect skulduggery and chicanery from all the usual suspects and it pays to be skeptical.
Willem
Paraphrasing Chomsky: When the press focuses on the health status of the population reach for your pocket, and see who's pulling
out your wallet.
What kills people in droves (out of despair), is class, but this will hardly be discussed by the press
This is actually from Nobel Prize winner, Angus Deaton (one of the few where they got it right)
https://muse.jhu.edu/book/72589
Richard Le Sarc
Coronavirus may or may not be a bio-weapon, but it seems passing strange that another Imperial target, Iran suddenly has an outbreak,
seemingly ex nihilo. And coronavirus is definitely being used to spread and deepen Sinophobic hatred, by organisations of
Evil like the villainous BBC.
Miller
A very, very "sick little game" indeed. Panicked headlines in Italy shout Three More Coronavirus Deaths! replete with pictures
of everyone wearing masks and looking fearful. The age of deaths? 83, 84, and 91, with no mention of any underlying/pre-existing
health issues, just another open and shut case: DEATH BY CORONAVIRUS. BE VERY AFRAID!
Ridiculous.
George Mc
" .will learn a valuable lesson, and decline to play along with this particular sick little game next time?"
No chance. On a more general level, I would say that the capitalist system is all out of carrots and will be issuing nothing
but sticks from now on. Turn round, drop 'em and bend over! Thrashity thrashity thrash!
Ken
Like the Patriot Act, the Model State Emergency Health Powers Act (MSEHPA) was essentially already put together, waiting in the
wings, and then rolled out shortly after 9/11. We're going to see further health related hysteria and attendant clampdown on whatever
token and illusory liberties we still have left. The ignorant, frightened masses will be the end of us.
Since Foxconn is getting into mask development, we're surprised Apple hasn't released plans
for an iMask, or scheming Elon Musk hasn't touted a Cybermask.
To sum up, we could all be wearing masks one day – if you think that's crazy just look
at what's happening across Asia. Mask wearing is coming to America – it's only a matter
of time.
Old and
grumpy
February 15, 2020 at 2:35 pm GMT
Is the American deep state that good in being a perfectly timed evil? Wasn't the deep state
designed to assist multinational corporations in stealing foreign resources? Yet the
corporate supply chain is being interrupted in what will be devastating for the bottom line.
The stock market is about all Trump has. The scenario outlined above just quite doesn't add
up, despite its plausibility. Unless it is not about China, but purging Trump .maybe?
The main achievement of neoliberal and imperial (warmongering) propaganda in the USA is that it achieved the complete,
undisputed dominance in MSM
Pot Calling the Kettle Black: "The Kremlin’s propaganda and disinformation machine is being unleashed via new platforms and continues to grow in Russia and
internationally. Russia seeks to destroy the very idea of an objective, verifiable set of facts as it attempts to influence opinions
about the United States and its allies. It is not an understatement to say that this new form of combat on the information battlefield
may be the fight of the 21st century."
Notable quotes:
"... Back in the 1960s, the CIA official Cord Meyer said the agency needed to "court the compatible left." ..."
"... The CIA therefore secretly worked to influence American and world opinion through the literary and intellectual elites. ..."
"... Then in 1977, Carl Bernstein wrote a long piece for Esquire – “The CIA and the Media” – naming names of journalists and media (The New York Times, CBS, etc.) that worked hand-in-glove with the CIA, propagandizing the American people and the rest of the world. ..."
Back in the 1960s, the CIA official Cord Meyer said the agency needed to "court the compatible left."
Right-wing and left-wing collaborators were needed to create a powerful propaganda apparatus that would be capable of hypnotizing
audiences into believing the myth of American exceptionalism and its divine right to rule the world.
The CIA therefore secretly worked to influence American and world opinion through the literary and intellectual elites.
Frances Stonor Saunders comprehensively covers this in her 1999 book, The Cultural Cold War: The CIA And The World Of Arts
And Letters How the CIA Tricked the World’s Best Writers
By the mid-1970s, as a result of the Church Committee hearings, it seemed as if the CIA, NSA, FBI, etc. had been caught in flagrante
delicto and disgraced, confessed their sins, and resolved to go and sin no more.
Then in 1977, Carl Bernstein wrote a long piece for Esquire – “The CIA and the Media” – naming names of journalists and media
(The New York Times, CBS, etc.) that worked hand-in-glove with the CIA, propagandizing the American people and the rest of the world.
It seemed as if all would be hunky-dory now with the bad boys purged from the American “free” press. Seemed to the most naïve,
that is, by which I mean the vast numbers of people who wanted to re-stick their heads in the sand and believe, as Ronald Reagan’s
team of truthtellers would announce, that it was “Morning in America” again with the free press reigning and the neo-conservatives,
many of whom had been “converted” from their leftist views, running things in Washington.
... ... ...
...read
Lansing’s July 10, 2019 testimony before the House Appropriations Sub-Committee on State , Foreign Operations and Related Programs:
“United States Efforts to Counter Russian Disinformation and Malign Influence.”
Here is an excerpt:
USAGM provides consistently accurate and compelling journalism that reflects the values of our society: freedom, openness,
democracy, and hope. Our guiding principles—enshrined in law—are to provide a reliable, authoritative, and independent source
of news that adheres to the strictest standards of journalism…
Russian Disinformation . And make no mistake, we are living through a global explosion of disinformation, state propaganda,
and lies generated by multiple authoritarian regimes around the world. The weaponization of information we are seeing today is
real. The Russian government and other authoritarian regimes engage in far-reaching malign influence campaigns across national
boundaries and language barriers.
The Kremlin’s propaganda and disinformation machine is being unleashed via new platforms and continues to grow in Russia and
internationally. Russia seeks to destroy the very idea of an objective, verifiable set of facts as it attempts to influence opinions
about the United States and its allies. It is not an understatement to say that this new form of combat on the information battlefield
may be the fight of the 21st century.
Then research the history of Radio Free Europe/Radio Liberty, the Voice of America, Radio and Television Marti, etc. You will
be reassured that Lansing’s July testimony was his job interview to head National Propaganda Radio.
Edward Curtin writes, and his writing on varied topics has appeared widely over many years. He writes as a public
intellectual for the general public, not as a specialist for a narrow readership. He believes a non-committal sociology is an
impossibility and therefore sees all his work as an effort to enhance human freedom through understanding. His website is
edwardcurtin.com
Notable quotes:
"... Imagine you are a horny 15 year old boy and you have been promised sex with an incredible Hollywood talent. Driven by surging hormones your anticipation and excitement are off the scale. You are taken to the place where the tryst will happen. And you open the door. Waiting of you is Barney Fife. ..."
Imagine you are a horny 15 year old boy and you have been promised sex with an incredible Hollywood talent. Driven by surging
hormones your anticipation and excitement are off the scale. You are taken to the place where the tryst will happen. And you open
the door. Waiting of you is Barney Fife.
That sort of sums up what is likely to happen tomorrow when Robert Mueller testifies before the House Judiciary and the House
Intelligence committees. I have shut off almost all cable news. I cannot stomach the relentless hype about tomorrow's supposed "big
day."
Blackberet ,
23 July 2019 at 02:18 PM
Hmmm, given how the legacy media has managed to completely misinterpret what Mueller's Report actually says, imagine what a field
day they will have interpreting "nothing" to mean something. Now, I wonder what that something might be...?
Curtis , Jun 26, 2019 6:12:43 PM |
54
michaelj72 #37I am gross and perverted
I may be vile and pernicious
You will obey me while I lead you
The Rev Kev
January 31, 2019 at 8:08 am
Do you think that the Guardian will shortly report that Iraq's WMD were snuck out of Iraq
and hidden in Venezuela all those years ago?
Colonel Smithers
January 31, 2019 at 8:36 am
Thank you, Kev.
Please don't give the scoundrels at King's Place any ideas.
Softpanorama Recommended
[Jul 06, 2021] Israeli officials say Pfizer vaccine less effective as Delta variant spreads Published on Jul 06, 2021 | www.bostonglobe.com
[Jul 01, 2021] Experts -- US COVID-19 positivity rate high due to 'too sensitive' tests by Marlene Lenthang Published on Aug 30, 2020 | www.msn.com
[Jun 26, 2021] 26 fully vaccinated people have died from Delta variant Published on Jun 26, 2021 | news.yahoo.com
[Jun 26, 2021] Surgeon Fired From College Of Medicine For Voicing Concerns About COVID Shots For Kids Published on Jun 26, 2021 | www.zerohedge.com
[Jun 24, 2021] Exclusive- Athlete Who Recovered From COVID Facing Very Different Future After Second Dose of Pfizer Vaccine Triggers Myoca by Megan Redshaw Published on Jun 22, 2021 | peckford42.wordpress.com
[Jun 08, 2021] Science has lost its way, at a big cost to humanity by MICHAEL HILTZIK Published on Oct 27, 2013 | www.latimes.com
[May 22, 2021] Michael Yeadon -- No need of vaccine, COVID-19 pandemic effectively over - FoxExclusive Published on May 22, 2021 | foxexclusive.com
[May 22, 2021] Warning
about Faucism From Former Pfizer Chief Scientist by Michael Yeadon Published on May 18, 2021 | www.investmentwatchblog.com
[May 03, 2021] Teachers abusing kids. Disgusting. Pfizer and Moderna experimenting on kids. Criminal Published on May 03, 2021 | off-guardian.org
[Apr 26, 2021] Genetic Vaccines -- Are They the New Thalidomide by Dr. Lee Merritt Published on Apr 26, 2021 | thenewamerican.com
[Apr 09, 2021] Distrust of the establishment plays a role in vaccine hesitancy, but it's probably time to back off on the prevailing commentary suggesting that those avoiding vaccines are irresponsible, uninformed or politically manipulated Published on Apr 09, 2021 | www.wsj.com
[Dec 06, 2020] Tested 'Positive' For COVID-19- Be Sure To Ask This Question Published on Dec 06, 2020 | www.zerohedge.com
[Sep 28, 2020] No wonder Pompey and his friend Jeffries won't give up on Syria! No wonder Published on Sep 28, 2020 | turcopolier.typepad.com
[Sep 28, 2020] Truth be told: political operatives own and run our MSM. This is why the press is called the 'Fourth Estate' Published on Aug 21, 2020 | www.unz.com
[Sep 06, 2020] Inactive fragments on virus RNA trigger false positives in most common COVID test due to way too many cycles of amplification which amplifies noise along with the signal and efffectly turns noise (inactive fragments on RNA) into signal, new study finds Published on Sep 05, 2020 | www.zerohedge.com
[Aug 01, 2020] Length of interaction with tan infected person matter Published on Aug 01, 2020 | www.zerohedge.com
[Jun 29, 2020] Gilead Will Charge More Than $3,000 For A Course Of COVID-19 Drug Remdesivir Published on Jun 29, 2020 | www.zerohedge.com
[Jun 10, 2020] Yale has published research that shows HCH + AZ has 50-fold benefits and insignificant risks Published on Jun 10, 2020 | www.moonofalabama.org
[May 24, 2020] Private Equity Is Ruining Health Care, Covid Is Making It Worse: Investors have been buying up doctor s offices, cutting costs, and, critics say, putting pressure on physicians by Heather Perlberg Published on May 20, 2020 | www.bloomberg.com
[Apr 28, 2020] Consumer Beware Coronavirus Antibody Tests Are Still A Work In Progress Published on Apr 28, 2020 | www.nakedcapitalism.com
[Apr 28, 2020] Coronavirus Fact-Check #4: "Why are so many healthcare workers dying?" Published on Apr 28, 2020 | off-guardian.org
[Apr 28, 2020] Who is at RISK from COVID-19 -- UK DOCTOR -- Covid-19 Vlog #15 Published on Apr 28, 2020 | www.youtube.com
[Apr 26, 2020] Who is an idiot here: What's not fair is that you go out running, you bloody idiot! shouted a Spanish woman apparently filming the encounter Published on Apr 26, 2020 | en.as.com
[Apr 13, 2020] American health care, as we call it today, and for all its high-tech miracles, has evolved into one of the most atrocious rackets the world has ever seen. By racket, I mean an enterprise organized explicitly to make money dishonestly by James Howard Kunstler Published on Apr 13, 2020 | www.zerohedge.com
[Apr 13, 2020] The Whistle-giver: the story of Ai Fen, the director of the emergency department of Wuhan Central Hospital Published on Apr 13, 2020 | scienceintegritydigest.com
[Apr 11, 2020] The country that glorifies profit at any cost and ruthless unethical competition will fare bad in case of any virus epidemic. That includes "Typhoid Mary" cases of selfish anti-social behaviour Published on Apr 11, 2020 | www.moonofalabama.org
[Apr 11, 2020] 'Never in my country': COVID-19 and American exceptionalism by Jeanne Morefield Published on Apr 07, 2020 | responsiblestatecraft.org
[Apr 10, 2020] Tucker: In crisis, nothing is more important than staying connected to reality Published on Apr 10, 2020 | www.youtube.com
[Apr 09, 2020] And b has posted previously directions for making masks. The advantage is you can throw them in the washing machine to clean, or even hand wash as they are small items Published on Apr 09, 2020 | www.moonofalabama.org
[Apr 06, 2020] Wearing a mask is a rare case when a selfish motive to save your own life produce a greater good Published on Apr 06, 2020 | www.unz.com
[Apr 05, 2020] The big mistake in the U.S. and Europe, in my opinion, is that people aren't wearing masks Published on Apr 05, 2020 | www.sciencemag.org
[Mar 30, 2020] If you get COVID-19 infection in the shop, office or transport, you probably will be sick two weeks, but if you get if from your wife - probably four, and mother-in-law -- six Published on Mar 30, 2020 | time.com
[Mar 29, 2020] Why Didn't We Test Our Trade's 'Antifragility' Before COVID-19 by Gene Callahan and Joe Norman Published on Mar 28, 2020 | www.theamericanconservative.com
[Mar 27, 2020] Not Just China U.S. Reliance on Foreign Medical Supplies is Staggering by Alan Tonelson Published on Mar 27, 2020 | www.theamericanconservative.com
[Mar 26, 2020] Reflections on a Century of Junk Science Published on Mar 26, 2020 | www.unz.com
[Mar 24, 2020]
The US
Department of Justice announced Sunday it had shut down a website claiming to sell a coronavirus vaccine Published on Mar 22, 2020 | news.yahoo.com
[Mar 24, 2020] Joe Rogan Experience #1439 - Michael Osterholm Published on Mar 24, 2020 | www.youtube.com
[Mar 22, 2020] Intelligence agencies and the virus Published on Mar 22, 2020 | www.moonofalabama.org
[Mar 21, 2020] Tucker Senator Burr sold shares after virus briefing Published on Mar 21, 2020 | www.youtube.com
[Mar 21, 2020]
Don't forget our congress critter Senator Kelly Loeffler Published on Mar 21, 2020 | caucus99percent.com
[Mar 19, 2020] I look to the narrative we get in North America, irrespective of the topic, and the pattern is the same Published on Mar 19, 2020 | www.unz.com
[Mar 16, 2020] The USA now experience the period when the medical personnel became the most prominent victim of the authorities incompetence Published on Mar 15, 2020 | angrybearblog.com
[Mar 14, 2020] Honest Government Ad Published on Mar 14, 2020 | youtu.be
[Mar 11, 2020] Joe Rogan interview today with Michael Osterholm is an internationally recognized expert in infectious disease epidemiology Published on Mar 11, 2020 | www.moonofalabama.org
[Mar 10, 2020] Soap is probably more effective
or as effective against COVID-19 as alcohol-based hand sanitizer Published on Mar 10, 2020 | www.moonofalabama.org
[Mar 09, 2020] COVID-19 and the Working Class by Jack Rasmus Published on Mar 09, 2020 | www.counterpunch.org
[Mar 09, 2020] Momento Mori - Unpopular Thoughts on Corona Virus by Craig Murray Published on Mar 09, 2020 | craigmurray.org.uk
[Mar 07, 2020] The Neoliberal Plague by Rob Urie Published on Mar 07, 2020 | www.counterpunch.org
[Mar 04, 2020] Why Are We Being Charged? Surprise Bills From Coronavirus Testing Spark Calls for Government to Cover All Costs by Jake Johnson Published on Mar 03, 2020 | www.commondreams.org
[Mar 04, 2020] Nowcasting COVID-19 for public health control: learning from the Chinese experience for global preparedness by Gabriel Leung Published on Feb 27, 2020 | lshtm.ac.uk
[Mar 03, 2020] Coronavirus hype vs reality Published on Mar 03, 2020 | angrybearblog.com
[Feb 28, 2020] The impact of coronavirus on Trump reelection chances Published on Feb 28, 2020 | angrybearblog.com
[Feb 25, 2020] Coronavirus Hysteria reaches tipping point by Catte Black Published on Feb 25, 2020 | off-guardian.org
Recent and interesting
Myth busters
World Health Organization Exponential function (please note that virus does not propagate exponentially outside a small initial period; in case of the USA
that was March 1-March 21 during which number of positively tested increased 33% a day)
Lectures and presentations
Statistics' and maps
NOTE: Data vary depending on the source.
Spanish Flu pandemic
World health organization information
World Health Organization, Coronavirus
CDC information
Trump administration response
YouTube information
General information:
Critical voices
Medical sites Comparison with the Spanish flu epidemic
Examples of negative coverage and fear mongering
Measles
The Measles Virus Is Back (But
Why?) by Matthew Ferrari March 6, 2020 nationalinterest.org
Society
Groupthink :
Two Party System
as Polyarchy :
Corruption of Regulators :
Bureaucracies :
Understanding Micromanagers
and Control Freaks : Toxic Managers :
Harvard Mafia :
Diplomatic Communication
: Surviving a Bad Performance
Review : Insufficient Retirement Funds as
Immanent Problem of Neoliberal Regime : PseudoScience :
Who Rules America :
Neoliberalism
: The Iron
Law of Oligarchy :
Libertarian Philosophy
Quotes
War and Peace
: Skeptical
Finance : John
Kenneth Galbraith :Talleyrand :
Oscar Wilde :
Otto Von Bismarck :
Keynes :
George Carlin :
Skeptics :
Propaganda : SE
quotes : Language Design and Programming Quotes :
Random IT-related quotes :
Somerset Maugham :
Marcus Aurelius :
Kurt Vonnegut :
Eric Hoffer :
Winston Churchill :
Napoleon Bonaparte :
Ambrose Bierce :
Bernard Shaw :
Mark Twain Quotes
Bulletin:
Vol 25, No.12 (December, 2013) Rational Fools vs. Efficient Crooks The efficient
markets hypothesis :
Political Skeptic Bulletin, 2013 :
Unemployment Bulletin, 2010 :
Vol 23, No.10
(October, 2011) An observation about corporate security departments :
Slightly Skeptical Euromaydan Chronicles, June 2014 :
Greenspan legacy bulletin, 2008 :
Vol 25, No.10 (October, 2013) Cryptolocker Trojan
(Win32/Crilock.A) :
Vol 25, No.08 (August, 2013) Cloud providers
as intelligence collection hubs :
Financial Humor Bulletin, 2010 :
Inequality Bulletin, 2009 :
Financial Humor Bulletin, 2008 :
Copyleft Problems
Bulletin, 2004 :
Financial Humor Bulletin, 2011 :
Energy Bulletin, 2010 :
Malware Protection Bulletin, 2010 : Vol 26,
No.1 (January, 2013) Object-Oriented Cult :
Political Skeptic Bulletin, 2011 :
Vol 23, No.11 (November, 2011) Softpanorama classification
of sysadmin horror stories : Vol 25, No.05
(May, 2013) Corporate bullshit as a communication method :
Vol 25, No.06 (June, 2013) A Note on the Relationship of Brooks Law and Conway Law
History:
Fifty glorious years (1950-2000):
the triumph of the US computer engineering :
Donald Knuth : TAoCP
and its Influence of Computer Science : Richard Stallman
: Linus Torvalds :
Larry Wall :
John K. Ousterhout :
CTSS : Multix OS Unix
History : Unix shell history :
VI editor :
History of pipes concept :
Solaris : MS DOS
: Programming Languages History :
PL/1 : Simula 67 :
C :
History of GCC development :
Scripting Languages :
Perl history :
OS History : Mail :
DNS : SSH
: CPU Instruction Sets :
SPARC systems 1987-2006 :
Norton Commander :
Norton Utilities :
Norton Ghost :
Frontpage history :
Malware Defense History :
GNU Screen :
OSS early history
Classic books:
The Peter
Principle : Parkinson
Law : 1984 :
The Mythical Man-Month :
How to Solve It by George Polya :
The Art of Computer Programming :
The Elements of Programming Style :
The Unix Hater�s Handbook :
The Jargon file :
The True Believer :
Programming Pearls :
The Good Soldier Svejk :
The Power Elite
Most popular humor pages:
Manifest of the Softpanorama IT Slacker Society :
Ten Commandments
of the IT Slackers Society : Computer Humor Collection
: BSD Logo Story :
The Cuckoo's Egg :
IT Slang : C++ Humor
: ARE YOU A BBS ADDICT? :
The Perl Purity Test :
Object oriented programmers of all nations
: Financial Humor :
Financial Humor Bulletin,
2008 : Financial
Humor Bulletin, 2010 : The Most Comprehensive Collection of Editor-related
Humor : Programming Language Humor :
Goldman Sachs related humor :
Greenspan humor : C Humor :
Scripting Humor :
Real Programmers Humor :
Web Humor : GPL-related Humor
: OFM Humor :
Politically Incorrect Humor :
IDS Humor :
"Linux Sucks" Humor : Russian
Musical Humor : Best Russian Programmer
Humor : Microsoft plans to buy Catholic Church
: Richard Stallman Related Humor :
Admin Humor : Perl-related
Humor : Linus Torvalds Related
humor : PseudoScience Related Humor :
Networking Humor :
Shell Humor :
Financial Humor Bulletin,
2011 : Financial
Humor Bulletin, 2012 :
Financial Humor Bulletin,
2013 : Java Humor : Software
Engineering Humor : Sun Solaris Related Humor :
Education Humor : IBM
Humor : Assembler-related Humor :
VIM Humor : Computer
Viruses Humor : Bright tomorrow is rescheduled
to a day after tomorrow : Classic Computer
Humor
The Last but not Least Technology is dominated by
two types of people: those who understand what they do not manage and those who manage what they do not understand ~Archibald Putt.
Ph.D
Copyright � 1996-2021 by Softpanorama Society www.softpanorama.org
was initially created as a service to the (now defunct) UN Sustainable Development Networking Programme (SDNP )
without any remuneration. This document is an industrial compilation designed and created exclusively
for educational use and is distributed under the Softpanorama Content License .
Original materials copyright belong
to respective owners. Quotes are made for educational purposes only
in compliance with the fair use doctrine.
FAIR USE NOTICE
This is a Spartan WHYFF (We Help You For Free)
site written by people for whom English is not a native language. Grammar and spelling errors should
be expected. The site contain some broken links as it develops like a living tree...
Disclaimer:
The statements, views and opinions presented on this web page are those of the author (or
referenced source) and are
not endorsed by, nor do they necessarily reflect, the opinions of the Softpanorama society. We do not warrant the correctness
of the information provided or its fitness for any purpose. The site uses AdSense so you need to be aware of Google privacy policy. You you do not want to be
tracked by Google please disable Javascript for this site. This site is perfectly usable without
Javascript.
Last modified: August 12, 2021