|
|
Home | Switchboard | Unix Administration | Red Hat | TCP/IP Networks | Neoliberalism | Toxic Managers |
| (slightly skeptical) Educational society promoting "Back to basics" movement against IT overcomplexity and bastardization of classic Unix | |||||||
|
|
Hypertension affects approximately 75 million adults in the United States and is a major risk factor for stroke, myocardial infarction ( aka heart attack), Coronary artery disease (CAD) and other vascular diseases, diabetis II, and chronic kidney disease. Obesity typically lead to hypertension with as the person ages. So controlling your BMI via diet is probably one of the most important preventive measures.
Obesity can be considered to be professional decease of programmers, especially older programmers and system administrators. So hypertension for them as natural outcome as the fact that they age. If you are a programmer, or system administrator over 50 you need to check you blood pressure. Stress increases probability. So if you unemployed that dobles the risk.
Blood pressure readings are measured in millimeters of mercury (mmHg) and usually given as two numbers. For example, 120 over 80 (written as 120/80 mmHg).
Either single or both of these numbers may be too high. Severe systemic hypertension is the condition when systolic blood pressure > 220 mm Hg and/or diastolic blood pressure >120 mm Hg ; Hypertension is defined as a systolic blood pressure (SBP) above 140 mm Hg, or a diastolic blood pressure (DBP) above 90 mm Hg at rest.
The definition of "rest" is subjective. Omron recommends 30 min sitting before taking measurements which is probably too extreme. But 30 min after running or during some heavy physical job is reasonable: blood pressure and pulse return to "normal" rest levels rather slowly. Actually the rate of return provides important information about the state of your cardiovascular system. Kind of stress test in reverse.
Please note that taking any antihypertensive medication also gets you in this category (see Medical Industrial Complex ) and that alone provides a stream of revenue to pharmaceutical companies (which in many cases is a factor which is more important then your health). In other words there are incentives for doctors in the USA to prescribe you antihypertensive medication. much like with abuse in other areas of US medicine hypertension medication are abused and overprescribed, especially beta blockers. You should be vary to take newer, more dangerous medication such as beta blockers without enough indications. Of source self-diagnosis is not that good idea, but seeking the second opinion is. And being skeptical might help too.
Please also note that blood pressure naturally increases with age due to loss of elasticity of blood vessels and calcification process.
Due to those factors learning to read and analyze your blood pressure is an important self-defense technique against this type of abuse by Medical Industrial Complex
|
Learning to read your blood pressure is an important self-defense technique against this type of abuse by Medical Industrial Complex |
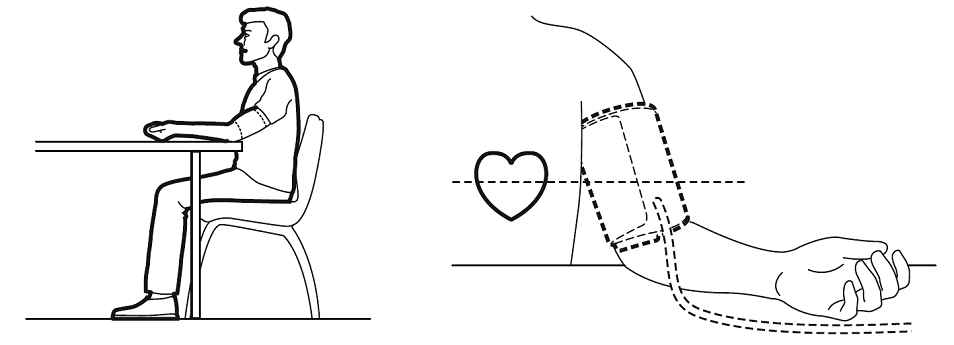
For a measurements of blood pressure to be informative they should taken in a certain time of the day and under identical conditions (sitting, after 30 min rest with left ark from the elbow on the surface of the table( on the level of the heart), right arm can just hand or be put on the table too, no taking, no movement during the measurement). Otherwise you should not consider 120 x 80 as your benchmark on "normal" blood pressure. In doctor office you usually wait for nurse for some time so this condition is more or less satisfied. But you position is far from idea -- while you are sitting you left arm is too low. That partially is compensated by greater accuracy of mercury bases pressure measurements, but still you better be aware of that. If you exited the measurement will be abnormally high, because this is how organism prepared to the danger. Some doctors are paranoid of dishonest and slitting hears over difference in systolic pressure between 130 and 140 (and tend to prescribe pills for higher pressure). Unless they (or you) make systematic measurements they are charlatans. In case of a single non-standardized measurement, even the value 160 does not tell much.
Please note the "consumer devices" like Omron has significant margin of error (around 5-10%) and usually exaggerate the pressure in comparison with mercury measurements with stethoscope. Even two different models (say older model like HEM-741 and a newer model BP785N (HEM-7321-Z)) of Omron blood pressure monitor display slightly different t behaviors. Errors can be in opposite directions for systolic and diastolic pressure: older model might undervalue diastolic pressure and at the same time exaggerate systolic pressure.
To get more-or-less accurate measurement you need to follow instruction precisely (see below) and take several readings. There are two major methods of taking several readings to get a better precision:
The second method is more accurate, but also is a more time consuming. In any case you should understand that error margin might exceed 5% (which is equivalent to 8 mm if you systolic pressure is 160).
Also comparing measurements makes sense if and only if they were made in identical settings. As human body regulates the blood pressure during the day (morning pressure is often higher). That means that the time of the day plays the role in comparison. Also after physical load (and in older people any load) the pressure and pulse return to normal slowly (actually the curve of return to normal can tall a lot about your ficical fitness and the sate of your cardiovascular system). Newer Omron models distinguish between morning and evening pressure average.
It is recommended that you apply the cuff using the following directions:
- Remove tight-fitting clothing from your left upper arm.
- Sit in a chair with your feet flat on the floor.
- Put your left arm through the cuff loop. The bottom of the cuff should be about 1 – 2 cm above your elbow (thickness of your index or middle finger). Adjust the cuff around your arm so that the tubing runs down the centre of your arm in line with your middle finger (palm open and facing upwards).
- Secure the cuff around your arm using the cloth closure. Pull the cuff so that the top and bottom edges are tightened evenly around your arm.
- The cuff should be firmly secured but not too tight – just enough so that it is difficult to slide 2 fingers under the cuff. This space is imperative for an accurate reading. OMRON's digital Blood Pressure Monitors use the Oscillometric method of blood pressure measurement that detects your blood's movement through your brachial artery and converts this movement into a digital reading.
- Relax your arm and place your elbow on the table so that the cuff is at the same level as your heart. Turn the palm of your hand upward.
- Check there are no kinks in the air tubing. Be careful that you do not rest your elbow on the air tube when taking a blood pressure reading.
- Press the ‘O/I START’ or ‘START’ button to begin the blood pressure reading.
For additional information please refer to the Instruction Manual for your device.
A typical "consumer" blood pressure measurement devices have an error margin around 5-10% (less if you very accurately put the cuff and take average of three consecutive measurements; variation within three measurements is between 5% and 8%) as they are not as proficient as human ear in determining the point when heart beating is no longer heard below the cuff as human ear with stethoscope (NSA specialists can definitely help OMRON in this area ;-).
Much depends on the model. For Omron, older models are usually less accurate. In one my experiment when HEM-741 three measurements average was 137/79, while newer BP785N using "TrueRead" mode with 60 sec between measurements was 130/82. Here is a series of average of three measurements using HEM-741 and TrueRead mode of BP785. As you can see the difference can be as large as 14 mm
| SYS1 | DIA1 | Pulse | SYS2 | DIA2 | Pulse2 | sys1-sys2 |
| 137 | 79.25 | 93.5 | 130 | 82 | 89 | 7 |
| 134.75 | 77 | 86.5 | 125 | 83 | 89 | 9.75 |
| 136 | 78 | 71.5 | 127 | 84 | 72 | 9 |
| 141.25 | 80.5 | 73 | 137 | 85 | 73 | 4.25 |
| 130.25 | 77 | 89.25 | 116 | 78 | 88 | 14.25 |
| 136.75 | 77 | 74.75 | 132 | 79 | 74 | 4.75 |
| 131 | 74 | 74 | 118 | 75 | 74 | 13 |
| 128.25 | 73.5 | 73.5 | 130 | 81 | 74 | -1.75 |
| 130.5 | 72.5 | 89.5 | 120 | 80 | 90 | 10.5 |
While the default interval is 60 sec you can change it manually in the range 15 sec -- 120 sec).
Discrepancy in three consecutive measurements is around 6% (or 10 mm/Hg is your blood pressure is around 150). One of the limitations of Omron-style devices is that the sensing is by necessity integrated into the cuff, not provided in a separate tube (like in case of stethoscope).
That means that you typically need three consecutive reading with 30 sec or one minute interval to increase accuracy. Newer Omron devices provide this capability automatically (TrueRead mode in model BP760N, BP761, BP785N ).
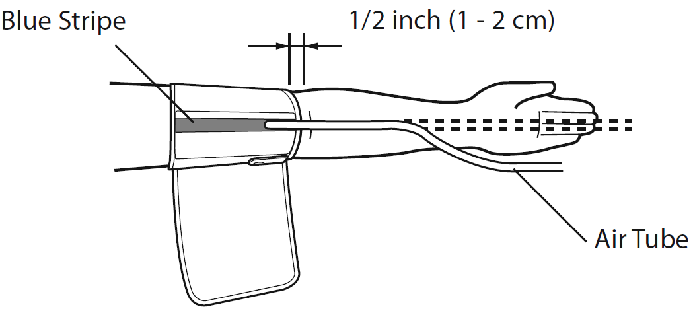
Precision with which you position the "arrow" on the cult against your artery (position of which you usually know from your experience with blood work) greatly affect the accuracy of easement. Too high position of the cult might increases the reading. Other things equal, it make sense to position the cult lower (1 cm or less), then higher to get better accuracy.
Limitation of Omron-style consumer devices mean that measurement of the blood pressure using the stethoscope and mercury based apparatus is more accurate. that's why this method still used in most doctors offices. Hospitals typically have more complex and expensive system that can measure blood pressure automatically and periodically.
There is a significant variation in recommendations as for what consider normal blood pressure for different age groups as the current range if "politically charged" question (affects hypertension drug sales). You also need to take into account other factors (for example it is different for diabetic patients then for "normal adults). And it should be that way. also "medical industrial complex" is pressing for lower figures in order to cell more drugs. that might explain such a low figures in American hear association listed below. They are definitely influenced by 'medical industrial complex". Increase of risk usually does not happen until systolic pressure reached 140 and it approximately doubles when it reaches 180 (Harvard Health). Omron consider limits for "normal" blood pressure to be 135-85, but for older people they can be expended to 140-90.
So to get a more accurate reading you need an average of three consecutive measurements. Blood pressure is measured "in rest" when you are in sitting position and do not move during the measurement. Probably you need a couple of minutes to still still and relax for blood pressure normalize in sitting position before measurement in order for it to be more accurate. Caffeinated beverages and coffee usually affect blood pressure too.
Some consider that for younger people (younger then 55) "pre-hypertension" condition arise is when systolic blood pressure is between 120 and 139 or your diastolic blood pressure is between 80 and 89 on multiple readings. while this condition is not dangerous per se, it looks like such people are more likely to develop hypertension as they age. That's probably a baloney. Often this is connected not with hypertension per se but with lack of exercise and sedentary life style. Those condition are easier to change and should be changed first.
For people younger then 55 the following table from can be used (the figures are average during the day, based on multiple readings, not a single measurement; Most people's numbers are higher during the day and lower during sleep. Stress can boost blood pressure. So can eating a big meal.)
Blood pressure at rest at sitting position fasting at the morning (30 min inactivity before measurement is assumed)
| Stages | Average systolic (top number) |
Average diastolic (bottom number) |
|
|---|---|---|---|
| Prehypertension | 120–139 | OR | 80–89 |
| High blood pressure Stage 1 | 140–159 | OR | 90–99 |
| High blood pressure Stage 2 | 160 or higher | OR | 100 or higher |
While a blood pressure reading of around 120/80 (fasting in the morning) is considered to be the desirable for adults younger then 55 (but even 130/90 is not that bad), this is not true for older people as they have hardening of blood arteries, which lose significant part of their elasticity due to aging. You probably need to add 5 or 10 for each 10 years after 55.
An expert panel convened by the American College of Cardiology (ACC) and the American Heart Association (AHA) recommends the following measurements for older people (cited from High blood pressure guidelines and treatments for older adults. - AARP):
Both are protecting the Medical Industrial complex, not patients (Huffington Post, ):
The American Heart Association (AHA) and the American College of Cardiology (ACC) recently released new cardiovascular disease prevention guidelines . They are an egregious example of much that is wrong with medicine today.The guidelines propose a vast expansion of the use of statins in healthy people, recommending them for about 44 percent of men and 22 percent of healthy women between the ages of 40 and 75. According to calculations by John Abramson, lecturer at Harvard Medical School, 13,598,000 healthy people for whom statins were not recommended based on the 2001 guidelines now fall into the category of being advised to take moderate or high intensity statin therapy.
The American Heart Association (AHA) is a nonprofit organization with a mission to "build healthier lives free of cardiovascular disease and stroke." Yet in its 2011-2012 financial statement , the AHA noted $521 million in donations from non-government and non-membership sources and many well-known large drug companies, including those who make and market statins, contribute amounts in the $1 million range.
Even as many in the medical community suspected the guidelines were a ploy to help the AHA's drug partners sell statins, it was revealed that the guideline's online calculator to determine cardiac disease risk over predicts risk by an astonishing 75 to 150 percent. But the guideline writers are standing firmly behind their faulty calculator.
Many new "blockbuster" hypertension drugs have significant side effects (for example, beta blockers). Do not use them if you are overweigh and losing weight is an option. Try first to normalize your weight.
Moreover there is no consensus what is the "desirable" blood pressure for people over 60. For example, in December 2013, a panel of experts convened by the National Institutes of Health (NIH) released a recommendation that people over age 60 with high blood pressure could settle for a goal of 150/90—not the more stringent standard of 140/90—and still get health benefits (Harvard Health )
| Many anti hypertension drugs have significant side effects (especially beta blockers). Do not use them is losing weight is an option. Moreover there is no consensus what is the "desirable" blood pressure for people over 60. For example, in December 2013, a panel of experts convened by the National Institutes of Health (NIH) released a recommendation that people over age 60 with high blood pressure could settle for a goal of 150/90—not the more stringent standard of 140/90—and still get health benefits (Harvard Health ) |
For diabetics with type II diabetes and with A1C above 6.5 the "desirable" blood pressure should probably be a bit lower as they have higher risk of heart disease, stroke and heart attack.
Also up until about 10 years ago, doctors only paid attention to diastolic hypertension. Now the consensus changes to the view that really systolic hypertension (top number) that matters in older people. Is this new consensus scientific or not we do not know
| Also up until about 10 years ago, doctors only paid attention to diastolic hypertension. Now the consensus changes to the view that really systolic hypertension (top number) that matters in older people. Is this new consensus scientific or not we do not know |
Typically it is the upper number — the systolic pressure — that climbs up for people older then 60, causing concerns. Systolic hypertension occurs when the arteries close to the heart begin to stiffen, making them less responsive to blood flow.
Some seniors develop a condition in which diastolic pressure drops even as systolic pressure climbs. Such a widening gap between the upper and lower numbers (so called "wide pulse pressure") might well represent an additional risk factor for heart disease and stroke. It is important to know that along with cousing diabetus (or increasing sugar level for people with diabetes II) beta blockers also tend to worsen wide pulse pressure.
The most useful lifestyle changes you can make are to restrict the amount of sodium in your diet, lose weight if you're overweight and start a regular exercise program. Loss of weight is especially important as the higher is the body mass the harder heart need to work to deliver the blood to all (often enlarged) organs. AARP recommends to engage in a physical activity, such as brisk walking, for 30 minutes most days of the week
| The most useful lifestyle changes you can make are to restrict the amount of sodium in your diet, lose weight if you're overweight and start a regular exercise program. |
Even if you are resting, blood pressure changes during the day. It is lowest as you sleep and rises when you get up. It also can rise when you are excited, nervous, or active. Even moving of one arm changes (increases) your blood pressure. If you have a blood pressure monitor you can expriment with taking a masument while talking and while silect. Or typing with one arm on computer.
Still, in "ideal condition" for most of your waking hours, your blood pressure should stays pretty much the same when you are sitting for 30 min or more. That level "at rest" and in ideal condition for people younger then 55 is claimed should be in the range 120/80.
In any case, when the level stays high, say, 160/90 or higher, you definitely have high blood pressure and need to take medications. With high blood pressure, the heart works harder, your arteries take a beating, and your chances of a stroke, heart attack, and kidney problems are greater.
People who do not have high blood pressure at age 55 face a 90 percent chance of
developing it during their lifetimes. So high blood pressure is a condition that most
people will have at some point in their lives. About two-thirds of people over age 65 have
blood pressure the blood pressure level of 140/90 mmHg or higher .
Around two third (65% ) of men and three forth (75% )of women have blood pressure above 150/90 when they reach age 70. But only one in three of those men and one in four of those women have it under control. Those who pay close attention and measure it regularly have a chance to live longer.
Left untreated, hypertension increases the chance of a heart attack or stroke.
| A very useful NIH document
Facts
About Lowering Blood Pressure, is available in both HTML and PDF format.
In addition, the National Heart, Lung, and Blood Institute (NHLBI) has developed and Interactive Web site, Your Guide to Lowering High Blood Pressure. These and other documents relating to high blood pressure are available on the page, Cardiovascular Information for the General Public, on the NHLBI Web site. |
Most of the time, there are no symptoms. Symptoms that may occur include:
If you have a severe headache or any of the symptoms above, see your doctor right away. These may be signs of a complication or dangerously high blood pressure called malignant hypertension.
The goal of treatment is to reduce blood pressure so that you have a lower risk of complications. There are many different medicines that can be used to treat high blood pressure, including:
Your doctor may also tell you to exercise, lose weight, and follow a healthier diet. If you have pre-hypertension, your doctor will recommend the same lifestyle changes to bring your blood pressure down to a normal range.
Often, a single blood pressure drug may not be enough to control your blood pressure, and you may need to take two or more drugs. It is very important that you take the medications prescribed to you. If you have side effects, your health care provider can substitute a different medication.
Blood pressure measurements are the result of the force of the blood produced by the heart and the size and condition of the arteries.
Many factors can affect blood pressure, including:
High blood pressure can affect all types of people. You have a higher risk of high blood pressure if you have a family history of the disease. High blood pressure is more common in African Americans than Caucasians. Smoking, obesity, and diabetes are all risk factors for hypertension.
Most of the time, no cause is identified. This is called essential hypertension.
High blood pressure that results from a specific condition, habit, or medication is called secondary hypertension. Too much salt in your diet can lead to high blood pressure. Secondary hypertension may also be due to:
Your health care provider will perform a physical exam and check your blood pressure. If the measurement is high, your doctor may think you have high blood pressure. The measurements need to be repeated over time, so that the diagnosis can be confirmed.
If you monitor your blood pressure at home, you may be asked the following questions:
Other tests may be done to look for blood in the urine or heart failure. Your doctor will look for signs of complications to your heart, kidneys, eyes, and other organs in your body.
These tests may include:
Most of the time, high blood pressure can be controlled with medicine and lifestyle changes.
Adults over 18 should have their blood pressure checked routinely.
Lifestyle changes may help control your blood pressure:
Follow your health care provider's recommendations to modify, treat, or control possible causes of secondary hypertension.
If you have high blood pressure, you will have regularly scheduled appointments with your doctor.
Even if you have not been diagnosed with high blood pressure, it is important to have your blood pressure checked during your yearly check-up, especially if someone in your family has or had high blood pressure.
Call your health care provider right away if home monitoring shows that your blood pressure remains high or you have any of the following symptoms:
|
|
Switchboard | ||||
| Latest | |||||
| Past week | |||||
| Past month | |||||
Jun 09, 2017 | arstechnica.com
The error range of typical "home" devices is enough to sway decisions about taking or stopping medication.
Millions of people stand to benefit from closely monitoring their blood pressure-those suffering with heart disease, diabetes, kidney disease, and pregnancy-induced hypertension, for instance, plus those who just stress in doctors' offices and can't get accurate readings. Yet the gadgets available for home use may not be up to the task .In a study out this week, about 70 percent of home blood-pressure devices tested were off by 5 mmHg or more. That's enough to throw off clinical decisions, such as stopping or starting medication. Nearly 30 percent were off by 10 mmHg or more, including many devices that had been validated by regulatory agencies. The findings, published in The American Journal of Hypertension , suggest that consumers should be cautious about picking out and using such devices-and device manufacturers need to step up their game.
"We were a little surprised to see 70 percent," lead author Raj Padwal told Ars. Dr. Padwal is a professor of medicine at the University of Alberta. He and his colleagues went into the study expecting to find problems with some devices, he admitted. "We thought maybe it would be 40 maybe-maybe 50-but 70 was a lot. That was disappointing."
What doesn't kill youThe researchers had hints from previous data that many blood-pressure monitors were not spot on. Their skepticism was heightened by how the devices have been tested and regulated. Companies often validate their devices by testing them on healthy adults, Padwal and his colleagues point out. But the people using them at home often have conditions that make measuring blood pressure particularly tricky, like obesity, stiffened arteries, or widened pulse pressure. Nevertheless, the devices can be cleared by regulatory agencies, such as the US Food and Drug Administration. And that, too, can be misleading.
People think that if a regulatory agency has signed off on one of these devices, that it must be good and accurate, Padwal said. "But what physicians and patients and the public don't know is that regulatory bodies like the FDA, they don't actually do much," he explains. "As long as the device is not going to kill you, they're happy."
Ars reached out to the FDA about the matter. A spokesperson confirmed that, while the FDA does oversee the devices, the administration doesn't approve them. "These devices are considered Class II devices requiring premarket clearance (not approval) by the FDA," the spokesperson explained in an e-mail. The premarket clearance only demonstrates that the device "is at least as safe and effective, that is, substantially equivalent, to a legally marketed device for the same intended use." In respect to accuracy, the agency only offers a guidance document for manufacturers.
Padwal and colleagues set out to test the accuracy of the devices themselves. Funded by the University of Alberta Hospital Foundation, they compared the home blood-pressure monitors of 85 patients with a gold-standard blood-pressure measurement technique. The patients' monitors varied by type, age, and validation-status. But they all used an automated oscillometric method, which measures oscillations in the brachial artery and uses an algorithm to calculate blood pressure. The gold-standard method was the old-school auscultatory method, which involves the arm-squeezing sphygmomanometer and a clinician listening for thumps with a stethoscope.
Data squeezeOmron devices
Enlarge
% of subjects with 5% difference No. (%)
10% difference
No. (%)15% difference Systolic or diastolic 33 (72%) 15 (33%) 2 (4%) Systolic 23 (50%) 8 (17%) 2 (4%) Diastole 18 (39%) 8 (17%) 0 (0%) For each study participant, the researchers took nine sequential blood pressure readings, switching between using the standard auscultatory method and the home monitors. For the auscultatory method, the researchers had two trained health professionals involved in the measurement, one taking it and another observing. If they disagreed on a measurement by more than 4 mmHg, they tossed the data and took the measurement again. With breaks in between each reading, the whole process usually took about 45 minutes per patient.
Of the 85 home devices, 59 were inaccurate by 5 mmHg or more in either their systolic (the top number that's the maximum pressure of a heart beat) or diastolic (the bottom number that's the minimum between-beat pressure). That's 69 percent inaccurate. Of those, 25 (or 29 percent) were off by 10 mmHg or more. And six devices (seven percent) were off by 15 mmHg or more.
Parsing the data further, the researchers found that devices that were validated were more often accurate than those that weren't (34 percent accurate within 5 mmHg vs. 24 percent, respectively). Devices that used upper arm cuffs were better than those using wrist cuffs (32 percent accurate vs. 17 percent).
And those with soft cuffs tended to be more accurate than those with hard cuffs (35 percent vs. 24 percent). Interestingly, the older devices tended to be more accurate than the newer ones.
Manufacturers really need to work on making these more accurate, Padwal argues. Five or ten off is just not good enough. He's doing more research now to try to figure out how to improve the algorithms that the oscillometric devices use. "Lots of work needs to be done," he added.
In the meantime, he advises patients to go for a validated device with an arm cuff that fits properly-that's key to them measuring correctly, he emphasizes. He also recommends taking several readings in a row to make sure.
American Journal of Hypertension , 2017. DOI: 10.1093/ajh/hpx041 ( About DOIs ).
Oct 15, 2016 | diabeteswell.com
It is essential to know the instructions on how to use an omron blood pressure monitor. It is vital to get accuate readings. Omron makes sure that you have the equipment correctly fitted before use because there is a light or sign telling you that it is attached correctly. It is also important that your posture is correct when taking such readings. For example, position your hand of the bp device on the other elbow when using a wrist monitor. Once again full details and diagram instructions are provided with their equipment. They make blood pressure readings simple and you will quickly incorporate these into your weekly routine. Important – Take a morning and evening readingYou should choose a certain day of the week in terms of regularly checking your blood pressure and stick with it. The procedure is very simple and straightforward. You should take your first reading around one hour after waking up. Note the rating and then take a second reading around one hour before going to bed. This will help get an accurate reading of what your levels are.
We have asked the question; how accurate are Omron blood pressure machines? Now let's ask a much more general question that all of you should understand the answer to;
Why do I need to bother with blood pressure readings?Hypertension may well be the medical term given for high blood pressure, but the name you should associate it with is one which is widely used. That is "The Silent Killer". Many people are unaware that they actually have high levels of blood pressure. They feel the odd twinge or headache, but simply put this down to feeling a little under the weather.
The fact is that although possible symptoms such as severe headaches, fatigue, chest pains, or a feeling of confusion could affect you, many feel that such symptoms are not associated with high blood pressure, or they simply do not get very many of these symptoms.
Consider this; Hypertension is the biggest cause of strokes known, it also has a massive say in the amount of heart related problems we suffer from.
If that is not enough reason for you to take blood pressure readings seriously then I feel nothing will persuade you.
How can you keep those blood pressure levels in the 'healthy zone'?Those who are overweight are increasing their risk of high blood pressure and the more overweight you are the bigger your problems. This makes blood pressure monitors particularly important for this group of people. You really need to address your weight issues, lifestyle and exercise regimen if you are to get yourself back on track. It cannot be overstated just how important looking after yourself is if you are to avoid high blood pressure problems.
Those of us who smoke, drink alcohol to excess and generally eat a poor diet are also leaving ourselves wide-open to high blood pressure.
One diet in particular should help you!There is a really effective diet for those with high blood pressure which is known as the DASH diet. If you have home blood pressure equipment such as the wrist monitor versions that Omron provide and you find that your blood pressure is creeping up the wrong way please ask your doctor about this excellent diet.
It has been devised specifically to bring your blood pressure levels down, and if you follow it to the letter it should have you back to normal in around 2 weeks of use.
Those 2 weeks could be the difference between a new you and a very poorly you!
One of the wisest investments you will make in terms of healthThere may be lots of gimmicks or unnecessary bits of equipment for your health available today, but please rest assured that home monitors for blood pressure are not gimmicks and they are highly useful. So useful they could actually save your life. Try putting a price on that!
This is the other thing, the price of such equipment really is trifling in terms of how low it is, and the peace of mind it will give you and your loved ones will pay for such a purchase many times over.
Hopefully the above has shown you the answer to our question; how accurate are Omron blood pressure machines, and you will use this advice to purchase one of their extensive range to suit your needs. Remember; it could be a life saver!
Jan 23, 2008 | NYTimes.com
It tastes bland and can be a tough daily regimen to follow, so it's not the ideal medicine for high blood pressure. But a low-salt, heart-healthy diet is staging a comeback as some 60-plus drugs fail to rein in staggering rates of hypertension in the United States.
Even the Food and Drug Administration is weighing in, with recent deliberations on whether salt contents should be posted clearly on food labels. After years of acrimonious debate on the true dangers of sodium, anti-salt crusaders contend that the writing is on the wall. "The evidence is overwhelming," said Dr. J. James Rohack, a Texas cardiologist who is working with the American Medical Association to rid the nation of its high-salt habits.
One plan of attack: calling on food companies and restaurants to cut the salt they serve by half over the next 10 years. The move could eventually end one of the major obstacles in fighting hypertension, the self-control and vigilance required when it comes to eating prepared or packaged foods. "People wouldn't have to make a conscious decision," said Dr. Lawrence J. Appel, a heart nutrition expert at Johns Hopkins University. "It could really make a difference."
As many as half of the 70 million people in the United States with hypertension turn out to be sensitive to salt, versus 10 percent of Americans in general. Even so, only 22 percent of patients stick with a hypertension-taming, low-salt DASH diet rich in fruits, vegetables and low-fat dairy. That's down from 30 percent in 1994. "We're going in the wrong direction," said Dr. Phillip Mellen of the Hattiesburg Health Clinic in Mississippi, who has studied nutritional aspects of high blood pressure.
Yet in knocking out one dietary demon, a much larger piece of the lifestyle puzzle still needs to be addressed. Rising rates of obesity, diets shockingly low in fruits and vegetables, and a lack of exercise are all major reasons one in three Americans now suffers from hypertension, experts say.
The sobering results come as pharmaceutical companies appear stalled in creating demonstrably superior new drugs to treat high blood pressure. Despite an expanding range of options, including Tekturna, the only novel hypertension treatment in nearly a decade, hypertension rates remain stubbornly high. For many patients, older, cheaper diuretics may work just as well as, or even better than, more heavily advertised treatments like calcium channel blockers or ACE inhibitors. And the most effective diuretic may be the first one made available, back in 1957.
Lacking a slam-dunk pill, the majority of patients end up relying on two or three drugs to keep their blood pressure under control. That state of affairs, some doctors say, could be better managed with the addition of diet and exercise. "We don't have to worry about side effects from lifestyle changes," said Dr. David C. Goff Jr., professor of epidemiology and public health at Wake Forest University School of Medicine in Winston-Salem, N.C. "But everyone finds it easier to prescribe drugs."
The benefits of a proper diet are hardly a secret, even among those with traditionally less access to health care. One survey found that Latinos and African-Americans living in inner-city neighborhoods knew the dangers of eating poorly, but they also told researchers that restrictive diets are too hard to follow and insufficient to end the need for drugs. Years of bad eating may be impossible to undo. "Most people need to be on two drugs by the time we see them," Dr. Appel said.
That's a shame, because many patients might end at least some of their reliance on medications simply by eating better. The American Medical Association says that limiting sodium to 1,600 milligrams a day - about a teaspoon of salt - can prevent a five-point rise in systolic blood pressure. When combined with the right diet, cutting back on salt can lower blood pressure as well as any single hypertension pill, research shows. Adding protein and healthy monosaturated fats to the DASH diet may lead to even greater reductions in heart attack risk.
The joint national committee on high blood pressure, a government advisory panel, calls such dietary measures indispensable for treating hypertension, since they can lower blood pressure and improve the effectiveness of drugs. Lifestyle changes work best in combination, the group adds.
But until government regulations address the sodium slipped into processed and restaurant foods, experts say, many patients are going to find cutting back a tough battle to win. "Even when people are trying to be good, the deck is stacked against them," Dr. Rohack said.
NewsTarget
New UK research indicates that taking beta-blocker drugs to treat high blood pressure can increase the risk of developing diabetes by 50 percent, compared to newer drugs.
Researchers from Imperial College London studied 14,000 blood pressure patients in the UK, Ireland and Scandanavia. Half the patients were being treated for high blood pressure with the beta-blocker drug Atenolol, along with a diuretic, and half were being treated with a newer calcium channel blocker drug called amlopdipine, along with an ACE inhibitor called perindopril. The researchers found that the group taking the calcium channel blocker and ACE inhibitor experienced a 34 percent lower rate of diabetes than the patients taking beta-blockers.
"The result emphatically adds to the evidence that beta blockers and diuretics can exacerbate that risk [of diabetes] ... We have to stop pretending that it's ok to give people diabetes. These cases are absolutely unnecessary," says the study's lead author, Professor Neil Poulter.
Though conventional doctors are urging patients to seek newer pharmaceutical treatments for their high blood pressure, natural health advocates say the condition can be treated with simple lifestyle and dietary changes.
"None of these drugs are truly safe," says Mike Adams, a consumer health advocate, "and even the ones that don't promote diabetes are dangerous in other ways. Artificially lowering blood pressure by chemically treating the symptom instead of the underlying cause is a sure recipe for disastrous long-term health consequences," he says. "Patients need to lower their blood pressure through dietary changes, exercise and stress reduction, not chemicals that we now know can seriously harm them."
Hypertension may also be brought on by chronic dehydration, so simply drinking more water -- not soda or beverages with caffeine -- can often lower high blood pressure. Patients should also drastically lower their intake of sodium and avoid foods containing sugar and hydrogenated oils, two ingredients that can accelerate the onset of diabetes. However, high blood pressure patients should always work with a qualified health practitioner before altering their treatment strategy.
The surprising news made headlines in December 2002. Generic pills for high blood pressure, which had been in use since the 1950s and cost only pennies a day, worked better than newer drugs that were up to 20 times as expensive.
The findings, from one of the biggest clinical trials ever organized by the federal government, promised to save the nation billions of dollars in treating the tens of millions of Americans with hypertension - even if the conclusions did seem to threaten pharmaceutical giants like Pfizer that were making big money on blockbuster hypertension drugs.
Six years later, though, the use of the inexpensive pills, called diuretics, is far smaller than some of the trial's organizers had hoped.
"It should have more than doubled," said Dr. Curt D. Furberg, a public health sciences professor at Wake Forest University who was the first chairman of the steering committee for the study, which was known by the acronym Allhat. "The impact was disappointing."
The percentage of hypertension patients receiving a diuretic rose to around 40 percent in the year after the Allhat results were announced, up from 30 to 35 percent beforehand, according to some studies. But use of diuretics has since stayed at that plateau. And over all, use of newer hypertension drugs has grown faster than the use of diuretics since 2002, according to Medco Health Solutions, a pharmacy benefits manager.
The Allhat experience is worth remembering now, as some policy experts and government officials call for more such studies to directly compare drugs or other treatments, as a way to stem runaway medical costs and improve care.
The aftereffects of the study show how hard it is to change medical practice, even after a government-sanctioned trial costing $130 million produced what appeared to be solid evidence.
A confluence of factors blunted Allhat's impact. One was the simple difficulty of persuading doctors to change their habits. Another was scientific disagreement, as many academic medical experts criticized the trial's design and the government's interpretation of the results.
Moreover, pharmaceutical companies responded by heavily marketing their own expensive hypertension drugs and, in some cases, paying speakers to publicly interpret the Allhat results in ways that made their products look better.
"The pharmaceutical industry ganged up and attacked, discredited the findings," Dr. Furberg said. He eventually resigned in frustration as chairman of the study's steering committee, the expert group that continues to oversee analysis of data from the trial. One member of that committee received more than $200,000 from Pfizer, largely in speaking fees, the year after the Allhat results were released.
There was another factor: medicine moves on. Even before Allhat was finished, and certainly since then, new drugs appeared. Others, meanwhile, became available as generics, reducing the cost advantage of the diuretics. And many doctors have shifted to using two or more drugs together, helped by pharmaceutical companies that offer combination pills containing two medicines.
So Allhat's main query - which drug to use first - became "an outdated question that doesn't have huge relevance to the majority of people's clinical practices," said Dr. John M. Flack, the chairman of medicine at Wayne State University, who was not involved in the study and has consulted for some drug makers.
Dr. Sean Tunis, a former chief medical officer for Medicare, remains an advocate for comparative-effectiveness studies. But, as Allhat showed, "they are hard to do, expensive to do and provoke a lot of political pushback," said Dr. Tunis, who now runs the nonprofit Center for Medical Technology Policy, which tries to arrange such trials.
"There's a lot of magical thinking," he said, "that it will all be science and won't be politics."
Expensive Pills
Promising better ways to treat high blood pressure, drug companies in the 1980s introduced a variety of medications, including ones known as calcium channel blockers and ACE inhibitors.
Although there was no real evidence the newer pills were better, diuretics fell to 27 percent of hypertension prescriptions in 1992, from 56 percent in 1982. Use of the more expensive pills added an estimated $3.1 billion to the nation's medical bill over that period.
So the National Heart, Lung and Blood Institute, part of the federal National Institutes of Health, decided to compare the various drugs' ability to prevent heart attacks, strokes and other cardiovascular problems. "This was a big-bucks issue," said Dr. Jeffrey Cutler, the Heart, Lung and Blood Institute's project director for the study.
Allhat - short for the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial - began enrolling patients with high blood pressure, age 55 and older, in 1994, with more than 42,000 people eventually participating. Patients were randomly assigned one of four drugs: a diuretic called chlorthalidone; an ACE inhibitor called lisinopril, which AstraZeneca sold as Zestril; a calcium channel blocker, amlodipine, sold by Pfizer as Norvasc; and an alpha blocker, doxazosin, which Pfizer sold as Cardura.
Cardura was added only after Pfizer, which had already agreed to contribute $20 million to the trial's costs, increased that to $40 million, Dr. Cutler said.
Early Trouble Signs
Pfizer's bet on Cardura proved a big mistake. As the Allhat data came in, patients taking Cardura were nearly twice as likely as those receiving the diuretic to require hospitalization for heart failure, a condition in which the heart cannot pump blood adequately. Concerned, the Heart, Lung and Blood Institute announced in March 2000 that it had stopped the Cardura part of the trial.
What happened next provided the first signs that the Allhat evidence might not be universally embraced.
Rather than warn doctors that Cardura might not be suited for hypertension, Pfizer circulated a memo to its sales representatives suggesting scripted responses they could use to reassure doctors that Cardura was safe, according to documents released from a patients' lawsuit against the company.
And in an e-mail message unearthed in those same court documents, a Pfizer sales executive boasted to colleagues that company employees had diverted some European doctors attending an American cardiology conference from hearing a presentation on the Allhat results and Cardura. "The good news," the message said, "is that they were quite brilliant in sending their key physicians to sightsee rather than hear Curt Furberg slam Pfizer once again!"
Pfizer declined to comment on the messages.
The Food and Drug Administration waited a year before convening a meeting of outside experts to discuss Cardura's safety. At that session, some of the experts sharply challenged the conclusions of the Allhat organizers. They argued that the heart failure cases might have been false readings and that an inadequate dose of Cardura had been used in the trial.
By the end of the daylong meeting, Dr. Robert J. Temple, a senior F.D.A. official, was clearly exasperated by the experts' varying interpretations of a supposedly definitive trial.
"This is the largest and best attempt to compare outcomes we are ever going to see," he said. "And people are extremely doubtful about whether it has shown anything at all."
The committee decided that there was no need to issue an urgent warning to doctors and patients about Cardura.
Cardura sales held up in 2000. But the next year, worldwide sales fell to $552 million, from $795 million. Prescriptions for all alpha blockers fell 22 percent from 1999 to 2002 after having risen before then, according to one study.
Pfizer's decision to stop promoting Cardura in late 2000, after the drug lost patent protection, was a factor in the decline. But Allhat clearly was, too.
Cost-Benefit Analysis
The main Allhat results were announced in December 2002 at a news conference in Washington and published in The Journal of the American Medical Association.
In the primary target outcome of the trial - the prevention of heart attacks - the three remaining drugs were proved equal. But patients receiving the Norvasc calcium channel blocker from Pfizer had a 38 percent greater incidence of heart failure than those on the diuretic. And those receiving the ACE inhibitor from AstraZeneca had a 15 percent higher risk of strokes and a 19 percent higher risk of heart failure.
Moreover, the diuretic cost only about $25 a year, compared with $250 for an ACE inhibitor and $500 for a calcium channel blocker. So the diuretic was declared the winner.
But some hypertension experts accused the government of overstating the case for the diuretics, as a way to cut medical spending.
"There was a feeling there was a political and economic agenda as much as a scientific agenda," said Dr. Michael Weber, a professor of medicine at the Health Science Center at Brooklyn, part of the State University of New York, who had been an investigator in the study but afterward became one of its leading critics. "They pushed beyond what the data allowed them to say."
Critics said the rules of the trial had favored the diuretics. If the first drug did not adequately lower blood pressure - as happened in more than 60 percent of cases - a second drug could be added. But that second drug was usually a type that worked better with diuretics than with ACE inhibitors.
There were also more new cases of diabetes among the patients who took diuretics, although experts argued over how meaningful that finding was.
Adding fuel to the debate, an Australian study released two months after Allhat found an ACE inhibitor superior to a diuretic. The proper lesson to draw from Allhat, some critics contended, was that what matters most is how much blood pressure is lowered, not which drug is used to do it. For these and other reasons, European hypertension experts discounted Allhat.
Allhat's proponents discounted the Australian study as less authoritative, and they dismissed the other criticisms.
Still, the arguments "muddied the waters," said Dr. Randall S. Stafford of Stanford, who studied the effect of Allhat on prescriptions. "The message," he said, "was no longer as clear to physicians."
Science Moves On
By the time the Allhat results were released, lisinopril, the ACE inhibitor, had become generic. That meant AstraZeneca and Merck, which sold a version of the compound as Prinivil, had less interest in defending their drugs.
Not so Pfizer. Norvasc was the best-selling hypertension treatment in the world, with sales of $3.8 billion in 2002, and Pfizer's second-biggest drug behind the cholesterol medication Lipitor.
The company set out to accentuate the positive. In a news release after the Allhat results were announced, it said that Norvasc was found to be "comparable to the diuretic in fatal coronary heart disease, heart attacks and stroke." And in a medical journal advertisement, it proclaimed "ALL HATs off" to its drug.
Neither the news release nor the ad, however, included the 38 percent greater risk of heart failure with Norvasc in the Allhat study.
Nor did Hank McKinnell, then Pfizer's chief executive, mention heart failure in lauding the results during his quarterly earnings conference call with analysts a few weeks after the Allhat report was released. "Contrary to what you might have read in the press," Mr. McKinnell said, "Allhat is extremely positive for Norvasc. It will be our job to explain that to the medical community."
Dr. Paul K. Whelton, president of Loyola University Health System and the current chairman of the Allhat steering committee, said that Pfizer and other drug companies "took what was in their best interest and ran with those, and conveniently didn't mention other things."
Pfizer defends its actions. Dr. Michael Berelowitz, the head of Pfizer's global medical organization, said that in the trial's design, heart failure was merely one component of a broader measure of various cardiovascular problems. And in that broader measure, Dr. Berelowitz said, there was no difference between Norvasc and the diuretic. Also, he said, the label for Norvasc already contained a precaution about heart failure.
"Further action regarding the heart failure finding was therefore not considered necessary," he said in a statement in response to questions.
Pfizer was not the only company promoting its drugs. The drug giant Novartis, for example, was spending heavily to market Diovan, a leader among a class of hypertension drugs called angiotensin receptor blockers, which were too new to have been included in Allhat. Diovan, which had more than $5 billion in sales last year, sells for $1.88 to $3.20 a pill on drugstore.com, compared with 8 to 31 cents for a diuretic.
No company, though, was spending money to promote generic diuretics. So the federal Heart, Lung and Blood Institute recruited Allhat investigators, provided them with training and sent them to proselytize fellow physicians. In all, 147 investigators gave nearly 1,700 talks and reached more than 18,000 doctors and other health care providers.
But it was a coffee-and-doughnuts operation compared with the sumptuous dinners that pharmaceutical companies used to market to doctors. Moreover, the steering committee's outreach program did not get under way until about three years after the results were published.
Dr. Stafford of Stanford said the outreach seemed to have had a slight effect on increasing the use of diuretics.
The results of Pfizer's efforts are easier to quantify. Norvasc sales continued to grow to $4.9 billion in 2006, falling only after the drug lost patent protection in the United States in 2007.
Tangles and Strife
Tensions about industry influence reached even the study's own steering committee. Dr. Furberg, the chairman, bluntly accused some members of the committee of being agents of the industry.
One member, Dr. Richard H. Grimm Jr. of the University of Minnesota, had been receiving tens of thousands of dollars a year from Pfizer since at least 1997, according to reports that pharmaceutical companies file in that state.
In 2003, the year after the Allhat results were published, Dr. Grimm's payments from Pfizer soared to more than $200,000 - an increase that The New York Times reported in 2007.
Dr. Grimm said in a recent interview that about half those fees in 2003 came from giving about 100 Pfizer-sponsored talks to doctors about Allhat. Dr. Grimm said he gave mainly the standard Allhat-sanctioned talk. But instead of saying diuretics were outright better than the other drugs, he said they were as good or better.
Meanwhile, Dr. Grimm had led an effort to remove Dr. Furberg from his position on the grounds that he had not been impartial.
"He had a vendetta against the calcium channel blockers," Dr. Grimm said. Dr. Furberg had been publicly questioning the safety of those drugs based on some studies he did in the 1990s. The effort to oust Dr. Furberg failed in 2001. But in August 2004, Dr. Furberg resigned as chairman, contending that there had not been enough effort to disseminate the Allhat message.
Dr. Whelton, who took over as chairman, said that the study's message was never compromised by industry ties on the steering committee.
Changing Practice
Experts see several lessons to be learned from Allhat.
One is that "all trials have flaws" that leave the results open to interpretation, said Dr. Robert M. Califf, a cardiologist at Duke who served on the safety monitoring committee of Allhat.
Another is that providing doctors information is "necessary, but not sufficient" to urge them to change their practices, said Dr. Carolyn M. Clancy, director of the federal Agency for Healthcare Research and Quality, which itself conducts studies comparing different medical treatments.
And while insurers can influence practice through reimbursement policies, they did not seem to have pushed strongly for diuretics after Allhat, in part because some of the other drugs had become generic.
Even the cost-conscious medical system at the Department of Veterans Affairs did not require diuretics, because too many doctors would probably have requested exceptions, said Dr. William C. Cushman, chief of preventive medicine at the department's medical center in Memphis.
Dr. Cushman, a member of the Allhat steering committee, said diuretic use in the system was still "much lower" than he thought it should be.
Dr. Clancy said that her agency was now mainly using insurance records to judge how treatments perform. While clinical trials are the gold standard, she said, they are costly and time-consuming.
And, she added, "You might be answering a question that by the time you are done, no longer feels quite as relevant."
Google matched content |
High blood pressure guidelines and treatments for older adults, elderl... - AARP
Blood pressure goals: How low should you go?
omronhealthcare.com Omron® BP785 IntelliSense® Automatic Blood Pressure Monitor with ComFitTM Cuff.
Hypertension & Women
Symptoms of High Blood Pressure
Headaches & High Blood Pressure
Measuring High Blood Pressure
Stress & High Blood Pressure
Miscellaneous
Related Diseases
Society
Groupthink : Two Party System as Polyarchy : Corruption of Regulators : Bureaucracies : Understanding Micromanagers and Control Freaks : Toxic Managers : Harvard Mafia : Diplomatic Communication : Surviving a Bad Performance Review : Insufficient Retirement Funds as Immanent Problem of Neoliberal Regime : PseudoScience : Who Rules America : Neoliberalism : The Iron Law of Oligarchy : Libertarian Philosophy
Quotes
War and Peace : Skeptical Finance : John Kenneth Galbraith :Talleyrand : Oscar Wilde : Otto Von Bismarck : Keynes : George Carlin : Skeptics : Propaganda : SE quotes : Language Design and Programming Quotes : Random IT-related quotes : Somerset Maugham : Marcus Aurelius : Kurt Vonnegut : Eric Hoffer : Winston Churchill : Napoleon Bonaparte : Ambrose Bierce : Bernard Shaw : Mark Twain Quotes
Bulletin:
Vol 25, No.12 (December, 2013) Rational Fools vs. Efficient Crooks The efficient markets hypothesis : Political Skeptic Bulletin, 2013 : Unemployment Bulletin, 2010 : Vol 23, No.10 (October, 2011) An observation about corporate security departments : Slightly Skeptical Euromaydan Chronicles, June 2014 : Greenspan legacy bulletin, 2008 : Vol 25, No.10 (October, 2013) Cryptolocker Trojan (Win32/Crilock.A) : Vol 25, No.08 (August, 2013) Cloud providers as intelligence collection hubs : Financial Humor Bulletin, 2010 : Inequality Bulletin, 2009 : Financial Humor Bulletin, 2008 : Copyleft Problems Bulletin, 2004 : Financial Humor Bulletin, 2011 : Energy Bulletin, 2010 : Malware Protection Bulletin, 2010 : Vol 26, No.1 (January, 2013) Object-Oriented Cult : Political Skeptic Bulletin, 2011 : Vol 23, No.11 (November, 2011) Softpanorama classification of sysadmin horror stories : Vol 25, No.05 (May, 2013) Corporate bullshit as a communication method : Vol 25, No.06 (June, 2013) A Note on the Relationship of Brooks Law and Conway Law
History:
Fifty glorious years (1950-2000): the triumph of the US computer engineering : Donald Knuth : TAoCP and its Influence of Computer Science : Richard Stallman : Linus Torvalds : Larry Wall : John K. Ousterhout : CTSS : Multix OS Unix History : Unix shell history : VI editor : History of pipes concept : Solaris : MS DOS : Programming Languages History : PL/1 : Simula 67 : C : History of GCC development : Scripting Languages : Perl history : OS History : Mail : DNS : SSH : CPU Instruction Sets : SPARC systems 1987-2006 : Norton Commander : Norton Utilities : Norton Ghost : Frontpage history : Malware Defense History : GNU Screen : OSS early history
Classic books:
The Peter Principle : Parkinson Law : 1984 : The Mythical Man-Month : How to Solve It by George Polya : The Art of Computer Programming : The Elements of Programming Style : The Unix Hater’s Handbook : The Jargon file : The True Believer : Programming Pearls : The Good Soldier Svejk : The Power Elite
Most popular humor pages:
Manifest of the Softpanorama IT Slacker Society : Ten Commandments of the IT Slackers Society : Computer Humor Collection : BSD Logo Story : The Cuckoo's Egg : IT Slang : C++ Humor : ARE YOU A BBS ADDICT? : The Perl Purity Test : Object oriented programmers of all nations : Financial Humor : Financial Humor Bulletin, 2008 : Financial Humor Bulletin, 2010 : The Most Comprehensive Collection of Editor-related Humor : Programming Language Humor : Goldman Sachs related humor : Greenspan humor : C Humor : Scripting Humor : Real Programmers Humor : Web Humor : GPL-related Humor : OFM Humor : Politically Incorrect Humor : IDS Humor : "Linux Sucks" Humor : Russian Musical Humor : Best Russian Programmer Humor : Microsoft plans to buy Catholic Church : Richard Stallman Related Humor : Admin Humor : Perl-related Humor : Linus Torvalds Related humor : PseudoScience Related Humor : Networking Humor : Shell Humor : Financial Humor Bulletin, 2011 : Financial Humor Bulletin, 2012 : Financial Humor Bulletin, 2013 : Java Humor : Software Engineering Humor : Sun Solaris Related Humor : Education Humor : IBM Humor : Assembler-related Humor : VIM Humor : Computer Viruses Humor : Bright tomorrow is rescheduled to a day after tomorrow : Classic Computer Humor
The Last but not Least Technology is dominated by two types of people: those who understand what they do not manage and those who manage what they do not understand ~Archibald Putt. Ph.D
Copyright © 1996-2021 by Softpanorama Society. www.softpanorama.org was initially created as a service to the (now defunct) UN Sustainable Development Networking Programme (SDNP) without any remuneration. This document is an industrial compilation designed and created exclusively for educational use and is distributed under the Softpanorama Content License. Original materials copyright belong to respective owners. Quotes are made for educational purposes only in compliance with the fair use doctrine.
FAIR USE NOTICE This site contains copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available to advance understanding of computer science, IT technology, economic, scientific, and social issues. We believe this constitutes a 'fair use' of any such copyrighted material as provided by section 107 of the US Copyright Law according to which such material can be distributed without profit exclusively for research and educational purposes.
This is a Spartan WHYFF (We Help You For Free) site written by people for whom English is not a native language. Grammar and spelling errors should be expected. The site contain some broken links as it develops like a living tree...
|
|
You can use PayPal to to buy a cup of coffee for authors of this site |
Disclaimer:
The statements, views and opinions presented on this web page are those of the author (or referenced source) and are not endorsed by, nor do they necessarily reflect, the opinions of the Softpanorama society. We do not warrant the correctness of the information provided or its fitness for any purpose. The site uses AdSense so you need to be aware of Google privacy policy. You you do not want to be tracked by Google please disable Javascript for this site. This site is perfectly usable without Javascript.
Last modified: March, 29, 2020