Polymerase chain reaction (PCR) is a chemical reaction harnessed to detect and identify trace bits of DNA, whether from a
virus or bacteria. It have limited value in diagnosing an infection. It has great value for forensic examination in criminal justice and archaeology.
It involves certain number of cycles of amplification of genetic material (this number of called Cr -- the last two letter of the
test abbreviation) and this number of critical for determining
the validity of the case. As a reminder, "cycle thresholds" (Ct) are the level at which widely used polymerase chain
reaction (PCR) test can detect a sample of the COVID-19 virus. The higher the number of cycles,
the lower the amount of viral load in the sample; the lower the cycles, the more prevalent the
virus was in the original sample. Here is one comment from
ZeroHedge
It beggars belief that governments have rarely specified to their health agencies what level of amplification cycles (Ct)
should be used when carrying out PCR tests given its known inappropriateness for detecting CovID-19.
Also, the NY Slimes article from last year refers to 30 Ct, but more recently the figure of 17-24 cycles has been quoted as
appropriate to produce the best result. Above that it goes haywire.
Further, Kary Mullis is on video clearly stating that his PCR test cannot detect any live virus and was never developed to do
that. All it detects is assorted debris and fragments in the human body left over from earlier flu viruses etc.
Unfortunately medical charlatans like Fauci ignored this this metric creating what is called "casedemic".
Facts now suggest that number of amplification used in the USA (40) was too high and created a lot of false positives (noise from
excessive amplification, much like noise when you attempt to amplify very weak sound from mike using electronic amplifier). Looks
like WHO "group of experts" recommended such an excessive number of amplifications, and this is where it gets interesting as
WHO by-and-large is controlled by Big Pharma. In the USA the situation was aggravated because Cr number was not
reported with the test -- suggesting large scale scam and unnecessary hardships inflicted on the population.
We have an epidemic of COVID-positive tests that is substantially larger than the epidemic of identified Relevant
Infectious COVID Disease. In contrast, people with actual, mild cases of COVID-disease aren’t all getting tested. So the data,
on which lockdowns are supposedly justified, are lousy.
The data on COVID hospitalizations and deaths in the US are exaggerated by a government subsidization scheme that
incentivizes the improper use of tests in people without particular risk of the disease.
Avoid getting tested for COVID unless you are symptomatic yourself, have had exposure to someone who was both symptomatic and tested
positive for COVID, or have some other personal reason that makes sense.
Know that getting tested before traveling abroad puts you at a modest risk of getting a false-positive test result, which
will assuredly screw up your trip. It’s a new political risk of travel.
There is a lot more to this viral testing game, and there are a lot of weird incentives. There are gray areas and room for
debate.
Yes, the COVID disease can kill people. But a positive test won’t kill anybody. Sadly, every COVID-positive test empowers
those politicians and bureaucrats who have a natural
bent to control people — the sociopaths and their ilk.
This test became standard for detecting the presence of the SARS CoV-2 coronavirus and is responsible for tremendously
inflated numbers of infected people (aka casedemic). When we see reports of cases of COVID-19 rising, we should know that
they are defining “case” as anyone with a COVID-19-positive test, which, as you might now realize, is really a garbage number.See for example, discussion at
For The First Time, A US
State Will Require Disclosure Of PCR 'Cycle Threshold' Data In COVID Tests - Zero Hedge
We have detailed the controversy surrounding America's COVID "casedemic" and the misleading
results of the PCR test and its amplification procedure in great detail over the past few
months.
As a reminder, "cycle thresholds" (Ct) are the level at which widely used polymerase chain
reaction (PCR) test can detect a sample of the COVID-19 virus. The higher the number of cycles,
the lower the amount of viral load in the sample; the lower the cycles, the more prevalent the
virus was in the original sample.
Numerous epidemiological experts have argued that cycle thresholds are an important metric
by which patients, the public, and policymakers can make more informed decisions about how
infectious and/or sick an individual with a positive COVID-19 test might be. However,
as JustTheNews reports, health departments across the country are
failing to collect that data .
Here are a few headlines from those experts and scientific studies:
2. The Wadworth Center, a New York State laboratory, analyzed the results of its July
tests at the request of the NYT: 794 positive tests with a Ct of 40: " With a Ct threshold of
35 , approximately half of these PCR tests would no longer be considered positive ," said the
NYT.
"And about 70% would no longer be considered positive with a Ct of 30! "
4. A new study from the
Infectious Diseases Society of America , found that at 25 cycles of amplification, 70% of
PCR test "positives" are not "cases" since the virus cannot be cultured, it's dead. And by
35: 97% of the positives are non-clinical.
5. PCR is not testing for disease, it's testing for a specific RNA pattern and this is the
key pivot. When you crank it up to 25, 70% of the positive results are not really "positives"
in any clinical sense , since
it cannot make you or anyone else sick
So, in summary, with regard to our current
"casedemic", positive tests as they are counted today do not indicate a "case" of anything.
They indicate that viral RNA was found in a nasal swab. It may be enough to make you sick, but
according to the New York Times and their experts, probably won't.
And certainly not sufficient
replication of the virus to make anyone else sick. But you will be sent home for ten days
anyway, even if you never have a sniffle. And this is the number the media breathlessly
reports... and is used to fearmonger mask mandates and lockdowns nationwide...
PCR is a technique that is used to amplify trace amounts of DNA (and in some instances, RNA) located in or on almost any liquid
or surface where DNA strands may be deposited. The key to understanding PCR is to know that every human, animal, plant, parasite,
bacterium, or virus contains genetic material such as DNA (or RNA) sequences (nucleotide sequences or pieces of DNA or RNA) that are
unique to their species, and to the individual member of that species. Consequently, if a sample contains segments of DNA or RNA,
PCR is a method used to amplify (make many more identical copies) of these unique sequences so they can then be used to determine
with a very high probability the identity of the source (a specific person, animal, or pathogenic organism) of the trace DNA or RNA
found in or on almost any sample of material. And this amplification number is critical as noise increases with the number of
amplification. Anything about 30 is suspect, but anything below 20 probably indicate that you are infected. The interval from
20 to 30 is a grey zone.
The test was widely abused making 40 amplifications which inflated the number of infected people and introduced huge economic
losses.
PCR amplification is only part of the identifying test, however. Once the amplification is done (see below), the amplified
segments need to be compared to other nucleotide segments from a known source (for example, a specific person, animal, or pathogenic
organism). This comparison of unique segments is often done by placing PCR-generated nucleotide sequences next to known nucleotide
sequences from humans, pathogens, or other sources in a separating gel. Electrical current is run through the gel and the various
nucleotide sequences form bands that resemble a "ladder" according to their electrical charge and molecular size. This is termed gel
electrophoresis. Bands or "ladder" like steps that migrate to the same levels in the gel show identity of nucleotide sequences. This
method is one of the most popular ways PCR tests are completed
Some details of PCR test
The test was invented in 1983 by Kary Mullis, who figured out the basic steps to amplify DNA
sequences. He and Michael Smith were awarded the Nobel Prize for developing this procedure in 1993. There are a few basic steps that
are followed in sequence:
PCR can be done in a single tube with appropriate chemicals and a specially designed heater. The reagents or chemicals needed are
as follows: A sample that contains a nucleotide sequence (from blood, hair, pus, skin scraping, etc.) DNA primers: short
single-stranded DNA that attaches to nucleotide sequences that promotes synthesis of a complementary strand of nucleotides DNA
polymerase: an enzyme that, when the DNA has a primer bound, goes down the DNA segment attaching DNA building blocks to form
complementary base pairs and thus synthesizes a complementary nucleotide strand of DNA (the introduction of a heat-resistant DNA
polymerase, Taq polymerase, derived from heat-resistant bacteria, markedly improved the ability to perform PCR)
A large excess of DNA building blocks termed nucleotides (Adenine, Thymidine, Cytosine, and Guanine, abbreviated as: A, T, C, and
G, respectively) are present in the solution. When these blocks are linked together, they form a nucleotide sequence or a single
strand of DNA. When these building blocks bind their complementary building block by weak hydrogen bonds (for example, A will only
bond with T and G only with C) a complementary DNA nucleotide sequence is formed and bound to the original single-stranded DNA. When
the binding is completed, a complementary double strand DNA is formed in a specific sequence.
PCR, then, begins with a segment of DNA from a sample that is placed in a tube with the reagents listed above. The solution is
heated to at least 94 C (201.2 F); this heat breaks the hydrogen bonds that allow complementary DNA strands to form, so only single
strands exist in the mixture (this is termed denaturation of double-stranded DNA).
The mixture is allowed to cool to about 54 C (129.2 F). At this temperature, the DNA primers and DNA polymerase bind to
individual single-stranded DNA (this is termed annealing of the DNA). Because the building blocks are in excess (high concentration)
in the mixture, the polymerase uses them to make new complementary strands of DNA (termed extension of the DNA) and this process is
more rapid at 72 C (161.6 F). This process creates a new double-stranded DNA molecule from each of the single strands of the
original molecule.
This cycle is repeated about 40 times in a machine termed a thermal cycler that automatically repeats the heating-cooling cycles,
with the amount of each DNA sequence doubling each time the heating-cooling cycle is completed.
What initially was a single short segment of DNA can be amplified to about 100 billion copies after 40 doubling cycles.
The PCR test forms the basis of a number of tests that can answer many different medical questions that help physicians diagnose
and treat patients. For example, PCR tests can detect and identify pathogenic organisms in patients, especially those that are
difficult to cultivate (for example, HIV and other viruses and certain fungi).
Although initial PCR tests amplified DNA, many viruses and other biological components (for example, mitochondria) utilize RNA as
their genetic material.
RT-PCR differs from conventional PCR by first taking RNA and converting the RNA strand into a DNA strand.
This is done by essentially the same method for PCR described above with the exception of using an enzyme termed reverse
transcriptase instead of the DNA polymerase. The reverse transcriptase allows a single strand of RNA to be translated into a
complementary strand of DNA. Once that reaction occurs, the routine PCR method can then be used to amplify the DNA. RT-PCR has been
used to detect and study many RNA viruses. RT-PCR should not be confused with another variation of PCR, termed Real-Time PCR.
Real-Time PCR is a variation of PCR that allows analysis of the amplified DNA during the usual 40 cycles of the procedure.
Although the procedure is similar to conventional PCR with cycling, Real-Time PCR uses fluorescent dyes attached to some of the
building blocks or small nucleotide strands. Depending on the method used, fluorescence occurs when the amplified DNA strands are
formed. The amount of fluorescence can be measured throughout the 40 cycles and allows the investigators to measure specific
products and their amounts during the amplification cycles. This often allows investigators or lab technicians to skip the gel
electrophoresis or other secondary procedures needed for analysis of the PCR products, thus producing more rapid results.
Real-Time PCR and RT-PCR are variations or modifications of the original PCR test. However, there are many more variations (at least 25) that
exist and are used to solve specific problems. They all have different names such as Assembly PCR, Hot-start PCR, Multiplex PCR,
Solid-phase PCR and many others.
PCR is likely to continue to be modified to help answer any other questions in medicine, biology. and other fields of study.
It’s simple, a
massive increase in cases was a direct result of a massive increase in testing.
It all started on
Jan 10th 2020, when WHO reported that there is an outbreak in China caused by a novel coronavirus.
On Jan 17th 2020,
The WHO recommended the use of the Corman-Drosten PCR test as a gold standard for detecting SARS-Cov-2 before the paper
was even submitted for publishing.
On Jan 21 2020,
the Corman-Drosten paper was submitted to the scientific journal Eurosurveillance describing the PCR test.On Jan 22
2020, it was accepted for publication.
On Jan 23rd 2020, it was published.
Keep in mind that
at the point when they started working on the PCR test, the genetic material of the virus was not yet sequenced.
“We aimed to
develop and deploy robust diagnostic methodology for use in public health laboratory settings without having virus
material available.”
“The PCR test was
therefore designed using the genomic sequence of SARS-CoV” “Design and validation were enabled by the close genetic
relatedness to the 2003 SARS-CoV.”
Listen to
Kevin_McKernan @ 10:37 he estimates that they started working on the PCR test at least 2 months prior to the publication
of the paper, so towards the end of Nov 2019.
“You have to
recognise the body of the work that they presented is not something you can do in a week that looks like maybe 2 months
worth of work, which of course begs the question of who tipped them off to making this, early, prior to actually being a
pandemic.
The paper was not
peer-reviewed. It was approved in one day. It takes on average 179 days to peer review an article.
Conflict of
interest was not declared: a) Drosten and his co-author Dr Chantal Reusken happen to be members of the editorial board
of Eurosurveillance.
Olfert Landt, of
Tib-Molbiol, the company that developed the PCR test being used, was also a co-author of the Drosten paper. “they
distributed these PCR-test kits before the publication was even submitted.” They were already in business before the
pandemic started.
In March 2020, the
pandemic happened. The more we tested, the more cases we got, the more we assigned any death with a positive test to
COVID19.
The world went
into lockdown based on a fear of rising cases, asymptomatic transmission, widespread susceptibility, lack of
pre-existing immunity, & lack of acquired immunity after Covid, with complete disregard to the fact that 80% of cases
had no symptoms or mild symptoms and that mortality followed an age gradient. All these fears were not justified and
contradicted our accumulated scientific knowledge. Basic immunological facts were put to question to disinform and
confuse the innocent public.
Countries adopted
an umbrella approach despite the fact that the profile of the vulnerable population was very clear since March 2020:
older individuals with multiple comorbidities were at high risk of developing serious disease that could culminate in a
negative outcome.
In June 2020, the
casedemic happened. As the prevalence of C19 decreased & herd
immunity approached, we started to tally up false (+) ‘cases’. The test was more likely to detect viral debris at this
point than an infectious virus, especially with cycle thresholds above 30.
The WHO &
Corman-Drosten protocol recommended a Ct of 45 cycles. Studies that conducted viral culture showed that with a PCR test
Ct >30, the tests were not detecting an infectious virus anymore. Yet governments turned a blind eye to these findings &
never revised
their Ct.
On the 27th of
November 2020, 23 scientists finally reviewed the Corman- Drosten paper and have demanded it’s retraction.
I'd
only add that the virus was clearly "circulating" well before the Wuhan outbreak in late December 2019.
We
don't know how many people contracted the virus in November, December 2019 and January and February 2020.
But this number is certainly much larger than we have been told ... And plenty of government officials and
public health authorities MUST know this.
7 hours ago
I agree with this story. I do believe there will be a cycle count decrease
corresponding to the mask mandate and the vaccine rollout. The entire Covid-19
from top to bottom is a political system having nothing to do with medical
science.
Err... Any chance now the WHO consider and approve the RT-PCR peer review
published by 22 world-renowned scientists last November and revealing no less than
10 major scientific flaws in the Corman-Drosten RT-PCR test recommended in January
2020 by medical journal Eurosurveillance? 10 major flaws that make that PCR test
totally useless for the diagnostic of covid.
To the peer review is also joined a letter with a request to Eurosurveillance to
retract that article and recommendation of January 2020.
The whole pandemic was based on that PCR testing. And Covid disappeared in China
only when they decided to stop testing. A corollary is that it magically
'reappears' whenever they start testing again...Go figure.
← Craig Kelly MP a true Australian hero warns there could have been 50,000 deaths
from Covid vax. NSW Health - Covid PCR tests at 40 cycles , double the recommended rate
yielding 80 per cent false positives* Jun 28. Posted by Editor, cairnsnews. Letter to the
Editor.
Up to 90 percent of people tested for COVID-19 in Massachusetts, New York and Nevada in
July carried barely any traces of the virus and it could be because today's tests are 'too
sensitive', experts say.
... PCR tests analyze genetic matter from the virus in cycles and today's tests
typically take 37 or 40 cycles, but experts say this is too high because it detects very
small amounts of the virus that don't pose a risk.
Experts say a reasonable cutoff for the virus would be 30 or 35 cycles, according to
Juliet Morrison, a virologist at the University of California, Riverside.
Mina said he would set the cutoff at 30.
New York's state lab Wadsworth analyzed cycle thresholds values in already processed
COVID-19 PCR tests and found in July that 794 positive tests were based on a threshold of
40 cycles.
With a cutoff of 35, about half of those tests would no longer qualify as positive.
About 70 percent would no longer be judged positive if the cycles were limited to 30.
In Massachusetts, from 85 to 90 percent of people who tested positive in July with a
cycle threshold of 40 would have been considered negative if the threshold were 30 cycles,
Mina said.
This one big fraud. And Fauci is implicated. the fact that in the USA the results of the test
do not come with the number of amplifications used speaks volumes about the current medical
establishement.
Notable quotes:
"... With a cutoff of 35, about half of those tests would no longer qualify as positive. About 70 percent would no longer be judged positive if the cycles were limited to 30. ..."
"... It's just kind of mind-blowing to me that people are not recording the C.T. values from all these tests -- that they're just returning a positive or a negative,' Angela Rasmussen, a virologist at Columbia University in New York, said. ..."
Up to 90 percent of people tested for COVID-19 in Massachusetts, New York and Nevada in July
carried barely any traces of the virus and it could be because today's tests are 'too
sensitive', experts say.
... PCR tests analyze genetic matter from the virus in cycles and today's tests typically
take 37 or 40 cycles, but experts say this is too high because it detects very small amounts of
the virus that don't pose a risk.
... ... ...
Experts say a reasonable cutoff for the virus would be 30 or 35 cycles, according to Juliet
Morrison, a virologist at the University of California, Riverside.
Mina said he would set the cutoff at 30.
New York's state lab Wadsworth analyzed cycle thresholds values in already processed
COVID-19 PCR tests and found in July that 794 positive tests were based on a threshold of 40
cycles.
With a cutoff of 35, about half of those tests would no longer qualify as positive.
About 70 percent would no longer be judged positive if the cycles were limited to 30.
In Massachusetts, from 85 to 90 percent of people who tested positive in July with a cycle
threshold of 40 would have been considered negative if the threshold were 30 cycles, Mina
said.
'I would say that none of those people should be contact-traced, not one,' he said.
The Food and Drug Administration said that it does not specify the cycle threshold ranges
used to determine who is positive and 'commercial manufacturers and laboratories set their
own.'
The Centers for Disease Control and Prevention said it is examining the use of cycle
threshold measures for 'policy decision'.
The CDC said its own calculations suggest its extremely hard to detect a live virus in a
sample above a threshold of 33 cycles.
It's just kind of mind-blowing to me that people are not recording the C.T. values from
all these tests -- that they're just returning a positive or a negative,' Angela Rasmussen, a
virologist at Columbia University in New York, said.
Cycle testing - running the same test over and over unitl you get the results you want and
then stopping.
Believe it or not this is the same foolishness that goes into radiometric dating of how
old rocks are. It's why you can take a warm chunk of lava and send it in to the dating lab
and get a result of over 25 million years old.
Trust the science folks - resistance is futile
By the way if the test shows negative after 30 cycles - it means that there is not enough
virus in your system for it be dangerous and that your body can deal with it on its own. By
the time you get to 35 cycles it is amplified so much that it will show any virus fragment in
your system - and at such miniscule amounts that the body does not even know its there - and
its not a problem. When you get 40 cycles and above the test will have to be positive because
there is always some virus fragments in your system. The single fact that they can run +40
cycles and get a negative result shows that this test is actually garbage from the start.
Dr Phuckit 16 hours ago remove link
My own interpretation of Government Data, tells me anything above 25 cycles is
fraudulent.
It looks like the CDC has come to their senses, but still bordering towards fraudulent
data.
At 30 cycles it's 50/50 chance of being right. But right for what exactly because it still
can't detect a virus, can't determine if it was a new infection or an old infection not even
active. Above 40+ even a rock will test positive.
What all this has accomplished though, is Corporations now have DNA samples of most of
worlds population , and these F'wits that weren't sick couldn't opt-in fast enough. Imagine
if these Corporations had said, we want your DNA for our Database, how many would have
volunteered ?
These Corporations now have the capability to target specific people with DNA for any evil
purpose they might have in the future. Perhaps this was the plan all along, DNA
collection.
Dr Phuckit 15 hours ago
The CDC can't stop the flood of lawsuits about to unfold, they are now trying to minimize
the damage to it's control and bank account. And the CDC is nothing but an interface between
All Pharmaceutical Companies and Government. They have no real power to mandate anything, all
they can do is recommend because it's about as Federal as the Federal Reserve.
shakypudding 16 hours ago remove link
The rt-CPR tests were sanctioned per emergency use authorizations (EUA) which means no
prior certification of efficacy. This rendered the lab results useless except for
propaganda.
The vaccines were also issued per emergency use authorization (EUA) which means no prior
certification of efficacy. How and why can this happen? Emergency use authorizations are
permitted when alternative treatments are not officially recognized, such as HCQ, Ivermectin
and vitamin D.
Had the government sanctioned alternative treatments such as HCQ, Ivermectin and vitamin D
millions of drug company profits and government kickbacks would have been forfeited.
Additionally, the opportunity for extending social programs of conditioning and control
would have been forgone by your overlords.
New policies will artificially deflate "breakthrough infections" in the vaccinated, while
the old rules continue to inflate case numbers in the unvaccinated.
The US Center for Disease Control (CDC) is altering its practices of data logging and
testing for "Covid19" in order to make it seem the experimental gene-therapy "vaccines" are
effective at preventing the alleged disease.
They made no secret of this, announcing the policy changes on their website in late
April/early May, (though naturally without admitting the fairly obvious motivation behind the
change).
The trick is in their reporting of what they call "breakthrough infections" – that is
people who are fully "vaccinated" against Sars-Cov-2 infection, but get infected anyway.
Essentially, Covid19 has long been shown – to those willing to pay attention –
to be an entirely created pandemic narrative built on two key factors:
Inflated Case-count. The incredibly broad definition
of "Covid case", used all over the world, lists anyone who receives a positive test as a
"Covid19 case", even if they never experienced any symptoms .
Without these two policies, there would never have been an appreciable pandemic at all , and
now the CDC has enacted two policy changes which means they no longer apply to vaccinated
people.
Firstly, they are lowering their CT value when testing samples from suspected "breakthrough
infections".
From the CDC's instructions for state health authorities on handling "possible breakthrough
infections" (uploaded to their website in late April):
For cases with a known RT-PCR cycle threshold (Ct) value, submit only specimens with Ct
value ≤28 to CDC for sequencing. (Sequencing is not feasible with higher Ct values.)
Throughout the pandemic, CT values in excess of 35 have been the norm, with labs around the
world going into the 40s.
Essentially labs were running as many cycles as necessary to achieve a positive result,
despite experts warning that this was pointless ( even Fauci himself said anything over 35 cycles is meaningless ).
But NOW, and only for fully vaccinated people, the CDC will only accept samples achieved
from 28 cycles or fewer. That can only be a deliberate decision in order to decrease the number
of "breakthrough infections" being officially recorded.
Secondly, asymptomatic or mild infections will no longer be recorded as "covid cases".
That's right. Even if a sample collected at the low CT value of 28 can be sequenced into the
virus alleged to cause Covid19, the CDC will no longer be keeping records of breakthrough
infections that don't result in hospitalisation or death .
As of May 1, 2021, CDC transitioned from monitoring all reported vaccine breakthrough
cases to focus on identifying and investigating only hospitalized or fatal cases due to any
cause. This shift will help maximize the quality of the data collected on cases of greatest
clinical and public health importance. Previous case counts, which were last updated on April
26, 2021, are available for reference only and will not be updated moving forward.
Just like that, being asymptomatic – or having only minor symptoms – will no
longer count as a "Covid case" but only if you've been vaccinated.
The CDC has put new policies in place which effectively created a tiered system of
diagnosis. Meaning, from now on, unvaccinated people will find it much easier to be diagnosed
with Covid19 than vaccinated people.
Consider
Person A has not been vaccinated. They test positive for Covid using a PCR test at 40
cycles and, despite having no symptoms, they are officially a "covid case".
Person B has been vaccinated. They test positive at 28 cycles, and spend six weeks
bedridden with a high fever. Because they never went into a hospital and didn't die they are
NOT a Covid case.
Person C , who was also vaccinated, did die. After weeks in hospital with a high fever and
respiratory problems. Only their positive PCR test was 29 cycles, so they're not officially a
Covid case either.
The CDC is demonstrating the beauty of having a "disease" that can appear or disappear
depending on how you measure it.
To be clear: If these new policies had been the global approach to "Covid" since December
2019, there would never have been a pandemic at all.
If you apply them only to the vaccinated, but keep the old rules for the unvaccinated, the
only possible result can be that the official records show "Covid" is much more prevalent among
the latter than the former.
This is a policy designed to continuously inflate one number, and systematically minimise
the other.
What is that if not an obvious and deliberate act of deception? play_arrow
ArkansasAngie 7 hours ago remove link
Reminds me of money supply numbers. And inflation numbers. And GDP numbers. And
unemployment numbers. Oh ... and votes
JakeIsNotFake 14 hours ago remove link
What is that if not an obvious and deliberate act of deception?
Well, before 3/20, this would have been a FELONY. Each time a lab provided a patient with
KNOWINGLY FALSE test results, the lab and the doctor would have been subject to a 16 month
term in the state penitentiary. For each instance.
Can you imagine getting a positive, terminal prognosis, committing a well deserved murder,
and then not dying?
Though the whole world relies on RT-PCR to "diagnose" Sars-Cov-2 infection,
the science is clear: they are not fit for purpose
Moreover, it is worth mentioning that the PCR tests used to identify so-called COVID-19
patients presumably infected by what is called SARS-CoV-2 do not have a valid gold standard to
compare them with.
This is a fundamental point. Tests need to be evaluated to determine their preciseness --
strictly speaking their "sensitivity"[
1 ] and "specificity" -- by comparison with a "gold standard," meaning the most accurate
method available.
As an example, for a pregnancy test the gold standard would be the pregnancy itself. But as
Australian infectious diseases specialist Sanjaya Senanayake, for example, stated in an
ABC TV interview in an answer to the
question "How accurate is the [COVID-19] testing?" :
If we had a new test for picking up [the bacterium] golden staph in blood, we've already
got blood cultures, that's our gold standard we've been using for decades, and we could match
this new test against that. But for COVID-19 we don't have a gold standard test."
Jessica C. Watson from Bristol University confirms this. In her paper "Interpreting a COVID-19 test result"
, published recently in The British Medical Journal , she writes that there is a
"lack of such a clear-cut 'gold-standard' for COVID-19 testing."
But instead of classifying the tests as unsuitable for SARS-CoV-2 detection and COVID-19
diagnosis, or instead of pointing out that only a virus, proven through isolation and
purification, can be a solid gold standard, Watson claims in all seriousness that,
"pragmatically" COVID-19 diagnosis itself, remarkably including PCR testing itself, "may be
the best available 'gold standard'." But this is not scientifically sound.
Apart from the fact that it is downright absurd to take the PCR test itself as part of the
gold standard to evaluate the PCR test, there are no distinctive specific symptoms for
COVID-19, as even people such as Thomas Löscher, former head of the Department of
Infection and Tropical Medicine at the University of Munich and member of the Federal
Association of German Internists, conceded to us[
2 ].
And if there are no distinctive specific symptoms for COVID-19, COVID-19 diagnosis --
contrary to Watson's statement -- cannot be suitable for serving as a valid gold standard.
In addition, "experts" such as Watson overlook the fact that only virus isolation, i.e. an
unequivocal virus proof, can be the gold standard.
That is why I asked Watson how COVID-19 diagnosis "may be the best available gold standard,"
if there are no distinctive specific symptoms for COVID-19, and also whether the virus itself,
that is virus isolation, wouldn't be the best available/possible gold standard. But she hasn't
answered these questions yet – despite multiple requests. And she has not yet responded
to our rapid response post on her article in which we address exactly the same points, either,
though she wrote us
on June 2nd : "I will try to post a reply later this week when I have a
chance."
NO PROOF FOR THE RNA BEING OF VIRAL ORIGIN
Now the question is: What is required first for virus isolation/proof? We need to know where
the RNA for which the PCR tests are calibrated comes from.
As textbooks (e.g., White/Fenner. Medical Virology, 1986, p. 9) as well as leading virus
researchers such as Luc Montagnier
or Dominic Dwyer state , particle purification -- i.e. the separation of an object from
everything else that is not that object, as for instance Nobel laureate Marie Curie purified
100 mg of radium chloride in 1898 by extracting it from tons of pitchblende -- is an essential
pre-requisite for proving the existence of a virus, and thus to prove that the RNA from the
particle in question comes from a new virus.
The reason for this is that PCR is extremely sensitive, which means it can detect even the
smallest pieces of DNA or RNA -- but it cannot determine where these particles came from
. That has to be determined beforehand.
And because the PCR tests are calibrated for gene sequences (in this case RNA sequences
because SARS-CoV-2 is believed to be a RNA virus), we have to know that these gene snippets are
part of the looked-for virus. And to know that, correct isolation and purification of the
presumed virus has to be executed.
Hence, we have asked the science teams of the relevant papers which are referred to in the
context of SARS-CoV-2 for proof whether the electron-microscopic shots depicted in their in
vitro experiments show purified viruses.
But not a single team could answer that question with "yes" -- and NB., nobody said
purification was not a necessary step. We only got answers like "No, we did not obtain an
electron micrograph showing the degree of purification" (see below).
We asked several study authors "Do your electron micrographs show the purified virus?", they
gave the following responses:
Study 1: Leo L. M. Poon; Malik Peiris. "Emergence of a novel human coronavirus threatening
human health" Nature Medicine , March 2020
Replying Author: Malik Peiris
Date: May 12, 2020
Answer: "The image is the virus budding from an infected cell. It is not purified
virus."
Study 2: Myung-Guk Han et al. "Identification of Coronavirus Isolated from a Patient in
Korea with COVID-19", Osong Public Health and Research Perspectives , February 2020
Replying Author: Myung-Guk Han
Date: May 6, 2020
Answer: "We could not estimate the degree of purification because we do not purify and
concentrate the virus cultured in cells."
Study 3: Wan Beom Park et al. "Virus Isolation from the First Patient with SARS-CoV-2 in
Korea", Journal of Korean Medical Science , February 24, 2020
Replying Author: Wan Beom Park
Date: March 19, 2020
Answer: "We did not obtain an electron micrograph showing the degree of
purification."
Study 4: Na Zhu et al., "A Novel Coronavirus from Patients with Pneumonia in China", 2019,
New England Journal of Medicine , February 20, 2020
Replying Author: Wenjie Tan
Date: March 18, 2020
Answer: "[We show] an image of sedimented virus particles, not purified ones."
Regarding the mentioned papers it is clear that what is shown in the electron micrographs
(EMs) is the end result of the experiment, meaning there is no other result that they could
have made EMs from.
That is to say, if the authors of these studies concede that their published EMs do not show
purified particles, then they definitely do not possess purified particles claimed to be viral.
(In this context, it has to be remarked that some researchers use the term "isolation" in their
papers, but the procedures described therein do not represent a proper isolation (purification)
process. Consequently, in this context the term "isolation" is misused).
Thus, the authors of four of the principal, early 2020 papers claiming discovery of a new
coronavirus concede they had no proof that the origin of the virus genome was viral-like
particles or cellular debris, pure or impure, or particles of any kind. In other words, the
existence of SARS-CoV-2 RNA is based on faith, not fact.
We have also contacted Dr Charles Calisher, who is a seasoned virologist. In 2001,
Science published an "impassioned plea to the younger generation" from several
veteran virologists, among them Calisher, saying that:
[modern virus detection methods like] sleek polymerase chain reaction [ ] tell little or
nothing about how a virus multiplies, which animals carry it, [or] how it makes people sick.
[It is] like trying to say whether somebody has bad breath by looking at his fingerprint."[
3 ]
And that's why we asked Dr Calisher whether he knows one single paper in which SARS-CoV-2
has been isolated and finally really purified. His answer:
I know of no such a publication. I have kept an eye out for one."[
4 ]
This actually means that one cannot conclude that the RNA gene sequences, which the
scientists took from the tissue samples prepared in the mentioned in vitro trials and for which
the PCR tests are finally being "calibrated," belong to a specific virus -- in this case
SARS-CoV-2.
In addition, there is no scientific proof that those RNA sequences are the causative agent
of what is called COVID-19.
In order to establish a causal connection, one way or the other, i.e. beyond virus isolation
and purification, it would have been absolutely necessary to carry out an experiment that
satisfies the four Koch's postulates. But there is no such experiment, as Amory Devereux and
Rosemary Frei
recently revealed for OffGuardian .
The necessity to fulfill these postulates regarding SARS-CoV-2 is demonstrated not least by
the fact that attempts have been made to fulfill them. But even researchers claiming they have
done it, in reality, did not succeed.
One example is a study published in Nature on
May 7 . This trial, besides other procedures which render the study invalid, did not meet
any of the postulates.
For instance, the alleged "infected" laboratory mice did not show any relevant clinical
symptoms clearly attributable to pneumonia, which according to the third postulate should
actually occur if a dangerous and potentially deadly virus was really at work there. And the
slight bristles and weight loss, which were observed temporarily in the animals are negligible,
not only because they could have been caused by the procedure itself, but also because the
weight went back to normal again.
Also, no animal died except those they killed to perform the autopsies . And let's not
forget: These experiments should have been done before developing a test, which is not
the case.
Revealingly, none of the leading German representatives of the official theory about
SARS-Cov-2/COVID-19 -- the Robert Koch-Institute (RKI), Alexander S. Kekulé (University
of Halle), Hartmut Hengel and Ralf Bartenschlager (German Society for Virology), the
aforementioned Thomas Löscher, Ulrich Dirnagl (Charité Berlin) or Georg Bornkamm
(virologist and professor emeritus at the Helmholtz-Zentrum Munich) -- could answer the
following question I have sent them:
If the particles that are claimed to be to be SARS-CoV-2 have not been purified, how do
you want to be sure that the RNA gene sequences of these particles belong to a specific new
virus?
Particularly, if there are studies showing that substances such as antibiotics that are
added to the test tubes in the in vitro experiments carried out for virus detection can
"stress" the cell culture in a way that new gene sequences are being formed that were
not
previously detectable -- an aspect that Nobel laureate Barbara McClintock already drew
attention to in her Nobel Lecture back in
1983 .
It should not go unmentioned that we finally got the Charité – the employer of
Christian Drosten, Germany's most influential virologist in respect of COVID-19, advisor to the
German government and co-developer of the PCR test which was the first to be "accepted" (
not validated! ) by the WHO worldwide – to answer questions on the topic.
But we didn't get answers until June 18, 2020, after months of non-response. In the end, we
achieved it only with the help of Berlin lawyer Viviane Fischer.
Regarding our question "Has the Charité convinced itself that appropriate particle
purification was carried out?," the Charité concedes that they didn't use purified
particles.
And although they claim "virologists at the Charité are sure that they are testing
for the virus," in their paper ( Corman et
al. ) they state:
RNA was extracted from clinical samples with the MagNA Pure 96 system (Roche, Penzberg,
Germany) and from cell culture supernatants with the viral RNA mini kit (QIAGEN, Hilden,
Germany),"
Which means they just assumed the RNA was viral .
Incidentally, the Corman et al. paper, published on January 23, 2020 didn't even go through
a proper peer review process , nor were the procedures outlined therein accompanied by controls
-- although it is only through these two things that scientific work becomes really
solid.
IRRATIONAL TEST RESULTS
It is also certain that we cannot know the false positive rate of the PCR tests without
widespread testing of people who certainly do not have the virus, proven by a method which is
independent of the test (having a solid gold standard).
Therefore, it is hardly surprising that there are several papers illustrating irrational
test results.
For example, already in February the health authority in China's Guangdong province reported
that people have fully recovered from illness blamed on COVID-19, started to test "negative,"
and then tested
"positive" again .
A month later, a paper published in the Journal of Medical Virology showed that 29
out of 610 patients at a hospital in Wuhan had 3 to 6 test results that flipped between
"negative", "positive" and
"dubious" .
A third example is a study from Singapore in which tests were carried out almost daily on 18
patients and the majority went from "positive" to "negative" back to "positive" at least once,
and up to
five times in one patient .
Even Wang Chen, president of the Chinese Academy of Medical Sciences, conceded in February
that the PCR tests are
"only 30 to 50 per cent accurate" ; while Sin Hang Lee from the Milford Molecular
Diagnostics Laboratory sent a l
etter to the WHO's coronavirus response team and to Anthony S. Fauci on March 22, 2020,
saying that:
It has been widely reported in the social media that the RT-qPCR [Reverse Transcriptase
quantitative PCR] test kits used to detect SARSCoV-2 RNA in human specimens are generating
many false positive results and are not sensitive enough to detect some real positive
cases."
In other words, even if we theoretically assume that these PCR tests can really detect a
viral infection, the tests would be practically worthless, and would only cause an unfounded
scare among the "positive" people tested.
This becomes also evident considering the positive predictive value (PPV).
The PPV indicates the probability that a person with a positive test result is truly
"positive" (ie. has the supposed virus), and it depends on two factors: the prevalence of the
virus in the general population and the specificity of the test, that is the percentage of
people without disease in whom the test is correctly "negative" (a test with a specificity of
95% incorrectly gives a positive result in 5 out of 100 non-infected people).
With the same specificity, the higher the prevalence, the higher the PPV.
In this context, on June 12 2020, the journal Deutsches Ärzteblatt published an
article in which the PPV has been calculated with
three different prevalence scenarios .
The results must, of course, be viewed very critically, first because it is not possible to
calculate the specificity without a solid gold standard, as outlined, and second because the
calculations in the article are based on the specificity determined in the study by Jessica
Watson, which is potentially worthless, as also mentioned.
But if you abstract from it, assuming that the underlying specificity of 95% is correct and
that we know the prevalence, even the mainstream medical journal Deutsches Ärzteblatt
reports that the so-called SARS-CoV-2 RT-PCR tests may have "a shockingly low" PPV.
In one of the three scenarios, figuring with an assumed prevalence of 3%, the PPV was only
30 percent, which means that 70 percent of the people tested "positive" are not "positive" at
all . Yet "they are prescribed quarantine," as even the Ärzteblatt notes critically.
In a second scenario of the journal's article, a prevalence of rate of 20 percent is
assumed. In this case they generate a PPV of 78 percent, meaning that 22 percent of the
"positive" tests are false "positives."
That would mean: If we take the around 9 million people who are currently considered
"positive" worldwide -- supposing that the true "positives" really have a viral infection -- we
would get almost 2 million false "positives."
All this fits with the fact that the CDC and the FDA, for instance, concede in their files
that the so-called "SARS-CoV-2 RT-PCR tests" are not suitable for SARS-CoV-2 diagnosis.
positive results [ ] do not rule out bacterial infection or co-infection with other
viruses. The agent detected may not be the definite cause of disease."
Remarkably, in the instruction manuals of PCR tests we can also read that they are not
intended as a diagnostic test, as for instance in those by
Altona Diagnostics and Creative Diagnostics[
5 ].
To quote another one, in the product announcement of the LightMix Modular Assays produced by
TIB Molbiol -- which were developed using the Corman et al. protocol -- and
distributed by Roche we can read:
These assays are not intended for use as an aid in the diagnosis of coronavirus
infection"
And:
For research use only. Not for use in diagnostic procedures."
WHERE IS THE EVIDENCE THAT THE TESTS CAN MEASURE THE "VIRAL LOAD"?
There is also reason to conclude that the PCR test from Roche and others cannot even detect
the targeted
genes .
Moreover, in the product
descriptions of the RT-qPCR tests for SARS-COV-2 it says they are
"qualitative" tests , contrary to the fact that the "q" in "qPCR" stands for
"quantitative." And if these tests are not "quantitative" tests, they don't show how many
viral particles are in the body .
That is crucial because, in order to even begin talking about actual illness in the real
world not only in a laboratory, the patient would need to have millions and millions of viral
particles actively replicating in their body.
That is to say, the CDC, the WHO, the FDA or the RKI may assert that the tests can measure
the so-called
"viral load," i.e. how many viral particles are in the body. "But this has never been
proven. That is an enormous scandal," as the journalist
Jon Rappoport points out .
This is not only because the term "viral load" is deception. If you put the question "what
is viral load?" at a dinner party, people take it to mean viruses circulating in the
bloodstream. They're surprised to learn it's actually RNA molecules.
Also, to prove beyond any doubt that the PCR can measure how much a person is "burdened"
with a disease-causing virus, the following experiment would have had to be carried out (which
has not yet happened):
You take, let's say, a few hundred or even thousand people and remove tissue samples from
them. Make sure the people who take the samples do not perform the test.The testers will never
know who the patients are and what condition they're in. The testers run their PCR on the
tissue samples. In each case, they say which virus they found and how much of it they found.
Then, for example, in patients 29, 86, 199, 272, and 293 they found a great deal of what they
claim is a virus. Now we un-blind those patients. They should all be sick, because they have so
much virus replicating in their bodies. But are they really sick -- or are they fit as a
fiddle?
With the help of the aforementioned lawyer Viviane Fischer, I finally got the Charité
to also answer the question of whether the test developed by Corman et al. -- the so-called
"Drosten PCR test"
-- is a quantitative test.
But the Charité was not willing to answer this question "yes". Instead, the
Charité wrote:
If real-time RT-PCR is involved, to the knowledge of the Charité in most cases
these are [ ] limited to qualitative detection."
Furthermore, the "Drosten PCR test" uses the unspecific E-gene assay as preliminary
assay , while the Institut Pasteur uses the same assay as
confirmatory assay .
According to
Corman et al ., the E-gene assay is likely to detect all Asian viruses , while the other
assays in both tests are supposed to be more specific for sequences labelled "SARS-CoV-2".
Besides the questionable purpose of having either a preliminary or a confirmatory test that
is likely to detect all Asian viruses, at the beginning of April the WHO changed the algorithm,
recommending that from then on a test can be regarded as "positive" even if just the E-gene
assay (which is likely to detect all Asian viruses! )
gives a "positive" result .
This means that a confirmed unspecific test result is officially sold as
specific .
That change of algorithm increased the "case" numbers. Tests using the E-gene assay are
produced for example by Roche
,
TIB Molbiol and
R-Biopharm .
HIGH CQ VALUES MAKE THE TEST RESULTS EVEN MORE MEANINGLESS
Another essential problem is that many PCR tests have a "cycle quantification" (Cq) value of
over 35, and some, including the "Drosten PCR test", even have a Cq of 45.
The Cq value specifies how many cycles of DNA replication are required to detect a real
signal from biological samples.
"Cq values higher than 40 are suspect because of the implied low efficiency and generally
should not be reported," as it says in the MIQE guidelines
.
MIQE stands for "Minimum Information for Publication of Quantitative Real-Time PCR
Experiments", a set of guidelines that describe the minimum information necessary for
evaluating publications on Real-Time PCR, also called quantitative PCR, or qPCR.
If you have to go more than 40 cycles to amplify a single-copy gene, there is something
seriously wrong with your PCR."
The MIQE guidelines have been developed under the aegis of Stephen A. Bustin , Professor of Molecular
Medicine, a world-renowned expert on quantitative PCR and author of the book A-Z of
Quantitative PCR which has been called "the bible of qPCR."
In a recent podcast interview Bustin points out that "the use of such arbitrary Cq
cut-offs is not ideal, because they may be either too low (eliminating valid results) or too
high (increasing false "positive" results)."
And, according to him, a Cq in the 20s to 30s should be aimed at and there is concern
regarding the reliability of the results for any Cq over 35.
If the Cq value gets too high, it becomes difficult to distinguish real signal from
background, for example due to reactions of primers and fluorescent probes, and hence there is
a higher probability of false positives.
Moreover, among other factors that can alter the result, before starting with the actual
PCR, in case you are looking for presumed RNA viruses such as SARS-CoV-2, the RNA must be
converted to complementary DNA (cDNA) with the enzyme Reverse Transcriptase -- hence the "RT"
at the beginning of "PCR" or "qPCR."
But this transformation process is "widely recognized as inefficient and variable,"
as Jessica Schwaber from the Centre for Commercialization of Regenerative Medicine in Toronto
and two research colleagues pointed out in a 2019
paper .
Stephen A. Bustin acknowledges problems with PCR in a comparable way.
For example, he pointed to the problem that in the course of the conversion process (RNA to
cDNA) the amount of DNA obtained with the same RNA base material can vary widely, even by a
factor of 10 (see above interview).
Considering that the DNA sequences get doubled at every cycle, even a slight variation
becomes magnified and can thus alter the result, annihilating the test's reliable informative
value.
So how can it be that those who claim the PCR tests are highly meaningful for so-called
COVID-19 diagnosis blind out the fundamental inadequacies of these tests -- even if they are
confronted with questions regarding their validity?
Certainly, the apologists of the novel coronavirus hypothesis should have dealt with these
questions before throwing the tests on the market and putting basically the whole world under
lockdown, not least because these are questions that come to mind immediately for anyone with
even a spark of scientific understanding.
Thus, the thought inevitably emerges that financial and political interests play a decisive
role for this ignorance about scientific obligations. NB, the WHO, for example has financial
ties with drug companies, as the British Medical Journal
showed in 2010 .
And
experts criticize"that the notorious corruption and conflicts of interest at WHO have
continued, even grown" since then. The CDC as well, to take another big player, is
obviously no better
off .
Finally, the reasons and possible motives remain speculative, and many involved surely act
in good faith; but the science is clear: The numbers generated by these RT-PCR tests do not in
the least justify frightening people who have been tested "positive" and imposing lockdown
measures that plunge countless people into poverty and despair or even drive them to
suicide.
And a "positive" result may have serious consequences for the patients as well, because then
all non-viral factors are excluded from the diagnosis and the patients are treated with highly
toxic drugs and invasive intubations. Especially for elderly people and patients with
pre-existing conditions such a treatment can be fatal, as we have outlined in the article
"Fatal
Therapie."
Without doubt eventual excess mortality rates are caused by the therapy and by the lockdown
measures, while the "COVID-19" death statistics comprise also patients who died of a variety of
diseases, redefined as COVID-19 only because of a "positive" test result whose value could not
be more doubtful.
As reported by FDA/CDC:
FDA - U.S. Food and Drug Administration
CDC - Centers for Disease Control and Prevention
"SINCE NO QUANTIFIED VIRUS ISOLATES OF THE 2019-nCoV were available for CDC use at the time
the test was developed and this study conducted, assays designed for detection of the
2019-nCoV RNA were tested with characterized stocks of in vitro transcribed full length
RNA..."
Scroll to page 42 link:
https://www.fda.gov/media/1...
Kary Mullis: PCR Test Inventor Calls Dr Fauci a Fraud (polymerase chain reaction, or
reverse transcription polymerase chain reaction)
https://odysee.com/@Quantum...
Disturbing Vaccine Facts - (The WHO etc. "Experts & Leaders" of infectious disease
proving from their own mouths Vaccines are not safe)
https://www.bitchute.com/vi...
Posted by: Palinurus | Nov 27 2020 10:21 utc | 102
---------------------------------------------------
The judges in Portugal drew their conclusion basing on the following technicalities:
1.
The judges also said that only a doctor can "diagnose" someone with a disease, and were
critical of the fact that they were apparently never assessed by one .
<--- It says nothing about PCR test "worthless".
2.
In the eyes of this court, then, a positive test does not correspond to a Covid case. The
two most important reasons for this, said the judges, are that, "the test's reliability
depends on the number of cycles used '' and that "the test's reliability depends on
the viral load present .'
<--- The judges simply argued on technicality: the higher the cycle threshold
(Ct) of a PCR test is, the higher the chance of the test turning out
positively.
Several recent publications, based on more than 100 studies, have attempted to propose a
cutoff Ct value and duration of eviction , with a consensus at approximately
Ct >30 and at least 10 days, respectively. However, in an article published in
Clinical Infectious Diseases, Bullard et al reported that patients could not be contagious
with Ct >25 as the virus is not detected in culture above this value.
The real argument is probably whether decision-makers (doctors, public health
authority) should take the lower Ct for PCR tests or not, which affects their consequential
decisions, for example, quarantine time of 10-day vs 14-day, the effectiveness control of
Covid 19 contagion.
@ Posted by: Palinurus | Nov 27 2020 10:21 utc | 102
lulu @ 121 is correct: diagnosis ≠ track and tracing.
PCR is just for track and tracing, not for diagnosis. The diagnosis protocol is much
longer and burdensome, and includes an MRI of the lungs if I'm not mistaken (and can only be
made by a doctor). The Portuguese judges are, therefore, also correct.
@ Posted by: oldhippie | Nov 27 2020 19:23 utc | 127
There are two problems with your theory:
1) Fauci is not a reliable source;
2) China uses a 40-cycle PCR test, used it on Wuhan's entire population (almost 10
million) after a scare and found no positive results.
We already talked about the Portuguese case. The judges were probably amid a labor dispute
and, in a pro-business decision, reiterated that PCR is not diagnosis.
Administer a test 10 million times and every result the same? And you believe this?
Amplify a signal by a trillion and there is never a problem with noise? Oh, it is in Chinese
wonderland, makes perfect sense.
Always apples and oranges with you. Same as it it would be talking to an illiterate. Or a
wall.
As Chris Martenson (PhD in pathology from Duke University) outlines in the 2020 Year in
Review with Dave Collum (PhD Columbia, Chemistry, teaches at Cornell): a medical "case" is
one in which a patient is presenting symptoms and requires medical attention. That's a case.
PCR tests were never meant to discern whether somebody is an "infected case" or not, and as
Collum elaborated in that same interview, "with a Cycle Threshold over 35, you can get a
positive PCR test out of a dog's ass".
Daily new cases of COVID-21 hospitalizations and COVID-19 and COVID-21 related deaths
will exceed medical care facilities capacity. Expected Q1 – Q2 2021.
According to the media, this is true. According to reality, it isn't. In CNN-style "fact
checking" parlance, it would thus score as "partially true".
"Covid Related Deaths" is a well worn catch-all. What is known to anybody keeping track: the
vast majority of COVID fatalities are with COVID, not from it. We all know this, for some
reason it doesn't seem to matter. The overall survival rate for this thing is somewhere around
97% or higher. Most people don't know anybody in their immediate circle of friends and family
that have actually died from it.
It can be terrible virus to catch and become sick with, and it's tragic to die from. But the
majority of people either exhibit flu like symptoms and shrug it off or remain completely
asymptomatic. Overall it causes fewer fatalities to society than either alcohol (3 million
deaths per year, globally) or driving (1.5 million) or for that matter air pollution at 4.2
million.
Enhanced lock down restrictions (referred to as Third Lock Down) will be implemented.
Full travel restrictions will be imposed (including inter-province and inter-city). Expected
Q2 2021.
UK Column News – 22nd January 2021
PART ONE
WHO BELATEDLY ADMITS LIMITATIONS OF PCR TEST
INSTITUTIONAL FRAUD ON GLOBAL SCALE REVEALED
Countries bankrupted, children's future compromised. Nuremberg trials await.
WHO must have known how PCR test worked in Jan 2020. Now they admit, a year later, that tests
are misleading. One day after Biden installed as the illegitimate president of the U.S.
KEEP TESTING AND YOU WILL FIND ANYTHING – EXACTLY WHAT KARY MULLIS SAID
TRANSLATION: SET THE GAIN TOO HIGH AND YOU GET FALSE DETECTIONS
The cycle threshold (Ct) needed to detect virus is inversely proportional to the patient's
viral load.
Kary Mullis won a Nobel Prize for inventing the test so should know its limitations. Sadly he
died, Aug 2019. Mullis said his PCR test should not be used to diagnose illness. PCR test can
detect DNA fragments from past diseases or from your body. Claims of "Covid" detection
actually detects these irrelevant fragments. PCR findings are supposed to be backed up by
clinical diagnosis of illness.
GBP 500 BRIBE FOR A JAB UNDER CONSIDERATION
UK unHEALTH SECRETARY MATT HANDCOCK SEES NO LIMIT TO GOV SPENDING
Environment Sec George Eustace says it's on the table
Mike Robinson: this is probably a trial balloon to see who the narrative fares. 500 a person
will be 450 million a week. UK borrowing hit a record in Dec.
Patrick Henningsen: the question is how much will it cost the gov to find new cases.
PM WON'T COMMIT TO ENDING LOCKDOWN
ANYWAY HE TALKS POSH SO THAT SHOULD PERSUADE YOU.
BoJo talks plum bull, chews words, talks guff, won't commit.
STILL NO INFORMATION ON WHETHER DEATHS ARE RISING OR WHY
NHS REMAINS EFFECTIVELY CLOSED TO ALL ILLNESSES
Are people dying from failure to treat elderly with flu or pneumonia?
MHRA'S CEO JUNE RAINE: NOTHING UNUSUAL IN ADVERSE REACTIONS
EU CRITICISED HASTY APPROVAL
Reports are coming in thick and fast to the yellow card adverse reaction scheme.
Raine is a career civil servant. Been on WHO safety committees. "Risk communication and
patient involvement" is her speciality.
Pfizer jab was "judged safe" and "far outweigh any risk", Raine said in Dec 2020, although
there had been no risk assessment. She also claimed the UK regulator did not cut any corners.
Yet phase three tests were not completed and won't be until Jan 2023. The EU criticised
"hasty" UK approval.
Mike Robinson: the public is the phase three trial. The public at large is the test
group.
UNIONS NOW OBLIGING MEMBERS TO COMPLY WITH VACCINATIONS.
HISTORIC SUPPORT FOR CIVIL LIBERTIES ABANDONED.
Patrick Henningsen: what happened to the left. They used to question the government and
favour liberty. Now unions are channeling gov policy and requiring members to get
vaccinations to work.
Mike Robinson: gov says vaccine is not mandatory but employers and unions are making it
so.
OVER-50s SAGA GROUP FALLS IN LINE WITH VAX PASSPORTS
MEMBERS REBEL AGAINST UNLAWFUL DEMANDS AND VIRTUE SIGNALLING
Saga says members must be "vaccinated" against Covid 14 days before travel. Members say
demand violates Nuremberg code, accuse company of virtue signalling.
Mike Robinson: dozens of companies seek to profit from the security and surveillance space
and health profits.
Patrick Henningsen: this is a gravy train driven by hoped-for profits.
JUST SAY NO -- CONVENTION ON BIOETHICS AND HUMAN RIGHTS
UNESCO ARTICLE 6 GIVES RIGHT TO REFUSE VACCINATION WITH NO RETRIBUTION
"The consent should, where appropriate, be expressed and may be withdrawn by the person
concerned at any time and for any reason without disadvantage or prejudice."
Mike Robinson: the principle is there but it is not binding in any way
NORTHERN IRELAND LOCKDOWN EXTENDED TO MAR 5
HONG KONG LAUNCHES FIRST LOCKDOWN. WEST MAY COPY
Patrick Henningsen: Where China goes, the west follows. Targeted lockdowns, focused on
cities, boroughs, housing estates. Only people with negative tests will be allowed off the
leash
U.S. PRESIDENTIAL INSTALLATION FAKENESS
OFFICIAL PORTRAITS OF BIDEN ARE VERY ORANGE
Trumpian imagery, strange presence of PermaOrange in U.S. presidential photos.
Patrick Henningsen: Lack of attendees blamed on social distancing. loads of sports events see
none of this distancing, the NFL football for instance.
GUSHING MEDIA FINALLY FREE
TRUMP DERANGEMENT SYNDROME ABATES TEMPORARILY
CNN Jeffrey Toobin (fumbulator): Lights laid down from the Lincoln statue to the obelisk were
"like Joe Biden's arms embracing America". Toobin resigned in October after playing with
himself on a Zoom call. CNN was happy to hire him.
CNN Jeff Zeleny: Their majesties Obama, Bush and Clint, recorded a video reflecting "the
majesty of the passage of power, importance of upholding democracy".
Mike Robinson: but Bill Clinson fell asleep!!!
CNN overcome with Biden on stage with Obama "The comforting sight of the Clintons and the
Bushes and the Obamas, the Avengers, the Marvel superheroes back together, with their friend
Joe Biden all of them sharing the view of a lot of Americans that we did narrowly avert
catastrophe all there to butress their buddy Joe Biden."
Patrick Henningsen: see the infantilization of politics. It has become a spectator sport
and politicians have become Marvel superheroes.
EXECUTIVE ORDER: MASK WEARING AND DISTANCING ON FEDERAL PROPERTY
UNLESS YOU ARE DOT GOV
Trump issued the lowest number of executive orders in recent times. Biden issued 17 on day
one and plans dozens in the first weeks of his installation.
BBC: KAMALA HARRIS A PRESIDENT IN WAITING?
ALREADY ASSUMED HAZY KAMALA WILL TAKE OVER
Patrick Henningsen: Joe Biden is not in his prime. He lacks the energy to lead the U.S. -- he
could barely campaign.
MARK SEDWILL RUNNING UK FOREIGN POLICY
NAME APPEARS AS HEAD OF VARIOUS QUASI GOV BODIES
China is a major set piece. Britain makes a play to outdo the EU on its aproach to China.
COP 26 and climate change take prominence. Biden due to visit Britain for G7 in Cornwall in
Jun 2021. D10 floated as democracy election: G7 + India, South Korea and Australia
Mike Robinson: the war narrative is broader than Covid -- aim in this case being to peel
India away from BRICS
MACRON CALLS ON BIDEN FOR GREATER U.S. INVOLVEMENT
OTAN AKBAR!
Obama doctrine, Clinton doctrine is back – arming "moderate rebels", targeting Syria,
Sahel region for western interests. Biden admin will need to make greater commitments on
Syria and Iraq, sending troops back, undoing Trump's withdrawal.
Moneycircus , Jan 23, 2021 5:52 PM Reply to
Moneycircus
UK Column News – 22nd January 2021
PART TWO
MAGICAL BAGHDAD BOMBING DAY AFTER BIDEN INSTALLATION
PROMPTS DEMAND TO ADD THOUSANDS OF U.S. TROOPS TO COMBAT REGIONAL TERROR
Bomb went off in market not far from U.S. embassy. Islamic State claimed responsibility for
two bombs that killed over 30 and injured 100 in central Baghdad.
Patrick Henningsen: we've been told for months that terrorism has been declining in Iraq.
Suddenly with Biden comes a new narrative and bombs. If a third party wanted to influence his
policy this would be the way to do it.
ISIS 'WE BOMBED RANDOM MARKET -- PLEASE OCCUPY IRAQ AGAIN.'
FOREIGN POLICY IS ABOUT BOMBS, INCLUSION AND GENDER
Averil Haines put forward as DNI. Haines is a protégé of Clapper and
Brennan.
Women and minorities are filling all these posts. The appearance of diversity: watch policy
not change.
LIBERTY GROUPS RESIST FURTHER CLAMPDOWN ON "TERROR"
LEADERSHIP CONFERENCE ON CIVIL AND HUMAN RIGHTS STATEMENT https://www.naacpldf.org/wp-content/uploads/No_Domestic_Terrorism_Charge_1_19_2021-1.pdf
Patrick Henningsen: Obama administration saw a mass shooting events every second week –
pipe bombs and country in permanent fear. At least half the terror events were driven by FBI
informants. Dubious events like San Bernardino were used to justify foreign policy adventures
in Syria.
Me: In contrast, apart from Las Vegas just after he took office, Trump admin saw relatively
few mass shootings.
ASSANGE PARDON REPORTEDLY BLOCKED BY MITCH MCCONNELL
TUCKER CARLSON ASSERTS THAT COMPROMISED RINO THREATENED TRUMP
McConnell "sent word over to the White House: if you pardon Julian Assange, we are much more
likely to convice you in an impeachment trial."
Patrick Henningsen: such horse trading would not be unusual. Trump missed a chance to go down
in history as a champion of free speech and an honest press.
Donald Trump shattered a lot of Republican records. That's not going to be reversed by
hunting down Trump and his supporters.
CHATHAM HOUSE MASTERCLASS IN MANIPULATING PUBLIC PERCEPTIONS
JAN 2019 INFLUENZA PREPAREDNESS CONFERENCE
Communication and public engagement – MARC VAN RANST – 9: Importance of using the
media to push messaging:
https://player.vimeo.com/video/320913130
Sitting in the front row was the UK's Jonathn Van Tam, Deputy Chief Medical Officer for
England
Marc van Ranst's Masterclass on Manipulating Public Fear for CFR-Chatham Ho.:
"Day one is so important. You start your comms with the press and people. One voice, one
message . In Belgium they appointed a non politician [van Ranst himself] to do that. You are
then not attacked politically. That was a big advantage. In Brussels you can play the
complete naive guy.
"You have to be omnipresent so you attract media attention. You have to make a contract with
them that if they call you, you will pick up the phone. If you do that you can profit from
these early days to get complete carpet coverage and they are not going to search for
alternative voices. And if you do that it makes things easier.
"Then you say we have a certain number of H1N1 deaths, that are unavoidable. I used a quote
from Sir Donaldson that at the peak of the epidemic, 40 people would die per day in UK, and I
calculated that for Belgium to show there would be 7 deaths a day. That is true in every
year (laughter) but talking about fatalities gets attention because people don't usually
think about anyone dying from influenza.
"A couple of days later you had the first death of H1N1 in the country and the scene was set
and it was already talked about."
Mike Robinson: The point he made about deaths is important. You take a number that is
normal, it happens every year but it is not usually reported. You start reporting it and
people think there is something special about that number. Then you add on the effects of
lockdown and you say this is really serious, even though the excess mortality is little
different to what's happened in history."
From the ZH article; "None of this was for your health. It was to get rid of Orange Man
Bad".
100%. The WHO's revised guidance
effectively says the majority of infection data from PCR testing is meaningless. ZH notes
Florida as a possible exception. The original guidance issued on 2020/12/14 seems to have
been scrubbed from the WHO's website but was archived here: ( https://web.archive.org/web/20210102051357/https://www.who.int/news/item/14-12-2020-who-information-notice-for-ivd-users).
">https://www.who.int/news/item/14-12-2020-who-information-notice-for-ivd-users).">https://web.archive.org/web/20210102051357/https://www.who.int/news/item/14-12-2020-who-information-notice-for-ivd-users).
The revised guidance calls for a retest upon a weak positive* result and publication of the
Ct value along with the result.
*Why no retest after a weak negative, am I missing something re the risk of false negative
results? Otherwise weeding out false positives only looks a lot like a policy to drive down
reported infection rates.
The next stage of course is for the CDC to update their guidance (not updated since
October) and revise the stats - hey presto pandemic over, all under the Biden
administration.
This is the most audacious, yet transparent, PSYOP of all time. I just can't believe
someone, somewhere doesn't have hard intel. on whoever is running it.
Introduction: using a technique to lock down society
All current propaganda on the COVID-19 pandemic is based on an assumption that is
considered obvious, true and no longer questioned:
Positive RT-PCR test means being sick with COVID. This assumption is misleading .
Very few people, including doctors, understand how a PCR test works.
RT-PCR means R eal T ime- P olymerase C hain R eaction.
In French, it means: Réaction de Polymérisation en Chaîne en Temps
Réel.
In medicine, we use this tool mainly to diagnose a viral infection.
Starting from a clinical situation with the presence or absence of particular symptoms in a
patient, we consider different diagnoses based on tests.
In the case of certain infections, particularly viral infections, we use the RT-PCR
technique to confirm a diagnostic hypothesis suggested by a clinical picture.
We do not routinely perform RT-PCR on any patient who is overheated, coughing or has an
inflammatory syndrome!
It is a laboratory, molecular biology technique of gene amplification because it looks for
gene traces (DNA or RNA) by amplifying them.
In addition to medicine, other fields of application are genetics, research, industry and
forensics.
The technique is carried out in a specialized laboratory , it cannot be done in any
laboratory, even a hospital. This entails a certain cost, and a delay sometimes of several days
between the sample and the result.
Today, since the emergence of the new disease called COVID-19 ( CO rona VI rus D isease-20
19 ), the RT-PCR diagnostic technique is used to define positive cases, confirmed as SARS-CoV-2
(coronavirus responsible for the new acute respiratory distress syndrome called COVID-19).
These positive cases are assimilated to COVID-19 cases, some of whom are hospitalized or
even admitted to intensive care units.
Official postulate of our managers: positive RT-PCR cases = COVID-19 patients. [1]
This is the starting postulate, the premise of all official propaganda, which justifies all
restrictive government measures: isolation, confinement, quarantine, mandatory masks, color
codes by country and travel bans, tracking, social distances in companies, stores and even,
even more importantly, in schools [2].
This misuse of RT-PCR technique is used as a relentless and intentional strategy by some
governments , supported by scientific safety councils and by the dominant media, to justify
excessive measures such as the violation of a large number of constitutional rights, the
destruction of the economy with the bankruptcy of entire active sectors of society, the
degradation of living conditions for a large number of ordinary citizens, under the pretext of
a pandemic based on a number of positive RT-PCR tests, and not on a real number of patients
.
Technical aspects: to better understand and not be manipulated
The PCR technique was developed by chemist Kary B. Mullis in 1986. Kary Mullis was awarded
the Nobel Prize in Chemistry in 1993.
Although this is disputed [3], Kary Mullis himself is said to have criticized the interest
of PCR as a diagnostic tool for an infection, especially a viral one.
He stated that if PCR was a good tool for research, it was a very bad tool in medicine, in
the clinic [4].
Mullis was referring to the AIDS virus (HIV retrovirus or HIV) [5], before the COVID-19
pandemic, but this opinion on the limitation of the technique in viral infections [6], by its
creator, cannot be dismissed out of hand; it must be taken into account!
PCR was perfected in 1992.
As the analysis can be performed in real time, continuously, it becomes RT (Real-Time)
– PCR , even more efficient.
It can be done from any molecule, including those of the living, the nucleic acids that make
up the genes:
DNA (deoxyribonucleic acid)
RNA (Ribonucleic Acid)
Viruses are not considered as "living" beings, they are packets of information (DNA or RNA)
forming a genome.
It is by an amplification technique (multiplication) that the molecule sought is highlighted
and this point is very important.
RT-PCR is an amplification technique [7].
If there is DNA or RNA of the desired element in a sample, it is not identifiable as
such.
This DNA or RNA must be amplified (multiplied) a certain number of times , sometimes a very
large number of times, before it can be detected. From a minute trace, up to billions of copies
of a specific sample can be obtained, but this does not mean that there is all that amount in
the organism being tested.
In the case of COVID-19, the element sought by RT-PCR is SARS-CoV-2, an RNA virus [8].
There are DNA viruses such as Herpes and Varicella viruses.
The most well known RNA viruses , in addition to coronaviruses, are Influenza, Measles,
EBOLA, ZIKA viruses.
In the case of SARS-CoV-2, RNA virus, an additional specific step is required, a
transcription of RNA into DNA by means of an enzyme, Reverse Transcriptase.
This step precedes the amplification phase.
It is not the whole virus that is identified, but sequences of its viral genome.
This does not mean that this gene sequence, a fragment of the virus, is not specific to the
virus being sought, but it is an important nuance nonetheless:
RT-PCR does not reveal any virus, but only parts, specific gene sequences of the virus.
At the beginning of the year, the SARS-CoV-2 genome was sequenced.
It consists of about 30,000 base pairs. The nucleic acid (DNA-RNA), the component of the
genes, is a sequence of bases. In comparison, the human genome has more than 3 billion base
pairs.
Teams are continuously monitoring the evolution of the SARS-CoV-2 viral genome as it evolves
[9-10-11], through the mutations it undergoes. Today, there are many variants [12].
By taking a few specific genes from the SARS-CoV-2 genome, it is possible to initiate RT-PCR
on a sample from the respiratory tract.
For COVID-19 disease, which has a nasopharyngeal (nose) and oropharyngeal (mouth) entry
point, the sample should be taken from the upper respiratory tract as deeply as possible in
order to avoid contamination by saliva in particular.
A
ll the people tested said that it is very painful [13].
The Gold Standard (preferred site for sampling) is the nasopharyngeal (nasal) approach , the
most painful route.
If there is a contraindication to the nasal approach, or preferably to the individual being
tested, depending on the official organs, the oropharyngeal approach (through the mouth) is
also acceptable. The test may trigger a nausea/vomiting reflex in the individual being
tested.
Normally, for the result of an RT-PCR test to be considered reliable, amplification from 3
different genes (primers) of the virus under investigation is required .
"The primers are single-stranded DNA sequences specific to the virus. They guarantee the
specificity of the amplification reaction. " [14]
"The first test developed at La Charité in Berlin by Dr. Victor Corman and his
associates in January 2020 allows to highlight the RNA sequences present in 3 genes of the
virus called E, RdRp and N . To know if the sequences of these genes are present in the RNA
samples collected, it is necessary to amplify the sequences of these 3 genes in order to
obtain a signal sufficient for their detection and quantification. "[15].
The essential notion of Cycle Time or Cycle Threshold or Ct positivity threshold [16].
An RT-PCR test is negative (no traces of the desired element) or positive (presence of
traces of the desired element).
However, even if the desired element is present in a minute, negligible quantity, the
principle of RT-PCR is to be able to finally highlight it by continuing the amplification
cycles as much as necessary.
RT-PCR can push up to 60 amplification cycles, or even more!
Here is how it works:
Cycle 1: target x 2 (2 copies)
Cycle 2: target x 4 (4 copies)
Cycle 3: target x 8 (8 copies)
Cycle 4: target x 16 (16 copies)
Cycle 5; target x 32 (32 copies)
Etc exponentially up to 40 to 60 cycles!
When we say that the Ct (Cycle Time or Cycle Threshold or RT-PCR positivity threshold) is
equal to 40, it means that the laboratory has used 40 amplification cycles , i.e. obtained 2
40 copies.
This is what underlies the sensitivity of the RT-PCR assay.
While it is true that in medicine we like to have high specificity and sensitivity of the
tests to avoid false positives and false negatives, in the case of COVID-19 disease, this
hypersensitivity of the RT-PCR test caused by the number of amplification cycles used has
backfired.
This over-sensitivity of the RT-PCR test is deleterious and misleading!
It detaches us from the medical reality which must remain based on the real clinical state
of the person: is the person ill, does he or she have symptoms?
That is the most important thing!
As I said at the beginning of the article, in medicine we always start from the person: we
examine him/her, we collect his/her symptoms (complaints-anamnesis) and objective clinical
signs (examination) and on the basis of a clinical reflection in which scientific knowledge and
experience intervene, we make diagnostic hypotheses.
Only then do we prescribe the most appropriate tests, based on this clinical reflection.
We constantly compare the test results with the patient's clinical condition (symptoms and
signs), which takes precedence over everything else when it comes to our decisions and
treatments.
Today, our governments, supported by their scientific safety advice, are making us do the
opposite and put the test first, followed by a clinical reflection necessarily influenced by
this prior test, whose weaknesses we have just seen, particularly its hypersensitivity.
None of my clinical colleagues can contradict me.
Apart from very special cases such as genetic screening for certain categories of
populations (age groups, sex) and certain cancers or family genetic diseases, we always work in
this direction: from the person (symptoms, signs) to the appropriate tests, never the other way
around.
This is the conclusion of an article in the Swiss Medical Journal (RMS) published in 2007,
written by doctors Katia Jaton and Gilbert Greub microbiologists from the University of
Lausanne :
"To interpret the result of a PCR, it is essential that clinicians and microbiologists
share their experiences, so that the analytical and clinical levels of interpretation can be
combined."
It would be indefensible to give everyone an electrocardiogram to screen everyone who might
have a heart attack one day.
On the other hand, in certain clinical contexts or on the basis of specific evocative
symptoms, there, yes, an electrocardiogram can be beneficial.
Back to RT-PCR and Ct (Cycle Time or Cycle Threshold).
In the case of an infectious disease, especially a viral one, the notion of contagiousness
is another important element.
Since some scientific circles consider that an asymptomatic person can transmit the virus,
they believe it is important to test for the presence of virus, even if the person is
asymptomatic, thus extending the indication of RT-PCR to everyone.
Are RT-PCR tests good tests for contagiousness? [17]
This question brings us back to the notion of viral load and therefore Ct .
The relationship between contagiousness and viral load is disputed by some people [18] and
no formal proof, to date, allows us to make a decision.
However, common sense gives obvious credence to the notion that the more virus a person has
inside him or her , especially in the upper airways (oropharynx and nasopharynx), with symptoms
such as coughing and sneezing, the higher the risk of contagiousness , proportional to the
viral load and the importance of the person's symptoms.
This is called common sense , and although modern medicine has benefited greatly from the
contribution of science through statistics and Evidence-Based Medicine (EBM), it is still based
primarily on common sense, experience and empiricism.
Medicine is the art of healing .
No test measures the amount of virus in the sample!
RT-PCR is qualitative : positive (presence of the virus) or negative (absence of the
virus).
This notion of quantity, therefore of viral load, can be estimated indirectly by the number
of amplification cycles (Ct) used to highlight the virus sought.
The lower the Ct used to detect the virus fragment, the higher the viral load is considered
to be (high).
The higher the Ct used to detect the virus fragment, the lower the viral load is considered
to be (low).
Thus, the French National Reference Centre (CNR), in the acute phase of the pandemic,
estimated that the peak of viral shedding occurred at the onset of symptoms, with an amount of
virus corresponding to approximately 10 8 (100 million) copies of SARS-CoV-2 viral
RNA on average (French COVID-19 cohort data) with a variable duration of shedding in the upper
airways (from 5 days to more than 5 weeks) [19].
This number of 108 (100 million) copies/μl corresponds to a very low Ct.
A Ct of 32 corresponds to 10-15 copies/μl.
A Ct of 35 corresponds to about 1 copy/μl.
Above Ct 35, it becomes impossible to isolate a complete virus sequence and culture it!
In France and in most countries, Ct levels above 35, even 40, are still used even today!
The French Society of Microbiology (SFM) issued an opinion on September 25, 2020 in which it
does not recommend quantitative results, and it recommends to make positive up to a Ct of 37
for a single gene [20]!
With 1 copy/μl of a sample (Ct 35) , without cough, without symptoms, one can understand
why all these doctors and scientists say that a positive RT-PCR test means nothing , nothing at
all in terms of medicine and clinic!
Positive RT-PCR tests, without any mention of Ct or its relation to the presence or absence
of symptoms, are used as is by our governments as the exclusive argument to apply and justify
their policy of severity, austerity, isolation and aggression of our freedoms, with the
impossibility to travel, to meet, to live normally!
There is no medical justification for these decisions, for these governmental choices!
In an article published on the website of the New York Times (NYT) on Saturday, August 29,
American experts from Harvard University are surprised that RT-PCR tests as practiced can serve
as tests of contagiousness, even more so as evidence of pandemic progression in the case of
SARS-CoV-2 infection [21].
According to them, the threshold (Ct) considered results in positive diagnoses in people who
do not represent any risk of transmitting the virus!
The binary "yes/no" answer is not enough, according to this epidemiologist from the Harvard
University School of Public Health.
"It's the amount of virus that should dictate the course of action for each patient
tested. "
The amount of virus (viral load); but also and above all the clinical state, symptomatic or
not of the person!
This calls into question the use of the binary result of this RT-PCR test to determine
whether a person is contagious and must follow strict isolation measures.
According to them: " We are going to put tens of thousands of people in confinement, in
isolation, for nothing. " [22]. 22] And inflict suffering, anguish, economic and
psychological dramas by the thousands!
Most RT-PCR tests set the Ct at 40, according to the NYT. Some set it at 37.
"Tests with such high thresholds (Ct) may not only detect live virus but also gene
fragments, remnants of an old infection that do not represent any particular danger," the
experts said.
A virologist at the University of California admits that an RT-PCR test with a Ct greater
than 35 is too sensitive. " A more reasonable threshold would be between 30 and 35, "
she adds.
Almost no laboratory specifies the Ct (number of amplification cycles performed) or the
number of copies of viral RNA per sample μl.
Here is an example of a laboratory result (approved by Sciensano, the Belgian national
reference center) in an RT-PCR negative patient:
No mention of Ct.
In the NYT, experts compiled three datasets with officials from the states of Massachusetts,
New York and Nevada that mention them.
Conclusion?
" Up to 90% of the people who tested positive did not carry a virus. "
The Wadworth Center, a New York State laboratory, analyzed the results of its July tests at
the request of the NYT: 794 positive tests with a Ct of 40.
" With a Ct threshold of 35 , approximately half of these PCR tests would no longer be
considered positive ," said the NYT.
"And about 70% would no longer be considered positive with a Ct of 30 ! "
In Massachusetts, between 85 and 90% of people who tested positive in July with a Ct of 40
would have been considered negative with a Ct of 30, adds the NYT. And yet, all these people
had to isolate themselves, with all the dramatic psychological and economic consequences, while
they were not sick and probably not contagious at all.
In France, the Centre National de Référence (CNR), the French Society of
Microbiology (SFM) continue to push Ct to 37 and recommend to laboratories to use only one gene
of the virus as a primer.
I remind you that from Ct 32 onwards, it becomes very difficult to culture the virus or to
extract a complete sequence, which shows the completely artificial nature of this positivity of
the test, with such high Ct levels, above 30.
Similar results were reported by researchers from the UK Public Health Agency in an article
published on August 13 in Eurosurveillance
: " The probability of culturing the virus drops to 8% in samples with Ct levels above
35." [23]
In addition, currently, the National Reference Center in France only evaluates the
sensitivity of commercially available reagent kits, not their specificity: serious doubts
persist about the possibility of cross-reactivity with viruses other than SARS-CoV-2, such as
other benign cold coronaviruses. [20]
It is potentially the same situation in other countries, including Belgium.
Similarly, mutations in the virus may have invalidated certain primers (genes) used to
detect SARS-CoV-2: the manufacturers give no guarantees on this, and if the AFP fast-checking
journalists tell you otherwise, test their good faith by asking for these guarantees, these
proofs.
If they have nothing to hide and if what I say is false, this guarantee will be provided to
you and will prove their good faith.
We must demand that the RT-PCR results be returned mentioning the Ct used because beyond
Ct 30, a positive RT-PCR test means nothing.
We must listen to the scientists and doctors, specialists, virologists who recommend the
use of adapted Ct, lower, at 30 . An alternative is to obtain the number of copies of viral
RNA/μl or /ml sample. [23]
We need to go back to the patient, to the person, to his or her clinical condition
(presence or absence of symptoms) and from there to judge the appropriateness of testing and
the best way to interpret the result.
Until there is a better rationale for PCR screening, with a known and appropriate Ct
threshold, an asymptomatic person should not be tested in any way.
Even a symptomatic person should not automatically be tested, as long as they can place
themselves in isolation for 7 days.
Let's stop this debauchery of RT-PCR testing at too high Ct levels and return to clinical,
quality medicine.
Once we understand how RT-PCR testing works, it becomes impossible to let the current
government routine screening strategy, inexplicably supported by the virologists in the safety
councils, continue.
My hope is that, finally, properly informed, more and more people will demand that this
strategy be stopped , because it is all of us, enlightened, guided by real benevolence and
common sense, who must decide our collective and individual destinies.
No one else should do it for us, especially when we realize that those who decide are no
longer reasonable or rational.
Summary of important points :
The RT-PCR test is a laboratory diagnostic technique that is not well suited to clinical
medicine.
It is a binary, qualitative diagnostic technique that confirms (positive test) or not
(negative test) the presence of an element in the medium being analyzed. In the case of
SARS-CoV-2, the element is a fragment of the viral genome, not the virus itself.
In medicine, even in an epidemic or pandemic situation, it is dangerous to place tests,
examinations, techniques above clinical evaluation (symptoms, signs). It is the opposite that
guarantees quality medicine.
The main limitation (weakness) of the RT-PCR test, in the current pandemic situation, is
its extreme sensitivity (false positive) if a suitable threshold of positivity (Ct) is not
chosen. Today, experts recommend using a maximum Ct threshold of 30.
This Ct threshold must be informed with the positive RT-PCR result so that the physician
knows how to interpret this positive result, especially in an asymptomatic person, in order
to avoid unnecessary isolation, quarantine, psychological trauma.
In addition to mentioning the Ct used, laboratories must continue to ensure the
specificity of their detection kits for SARS-CoV-2, taking into account its most recent
mutations, and must continue to use three genes from the viral genome being studied as
primers or, if not, mention it.
Overall Conclusion
Is the obstinacy of governments to use the current disastrous strategy, systematic screening
by RT-PCR, due to ignorance?
Is it due to stupidity?
To a kind of cognitive trap trapping their ego?
In any case, we should be able to question them, and if among the readers of this article
there are still honest journalists, or naive politicians, or people who have the possibility to
question our rulers, then do so, using these clear and scientific arguments.
It is all the more incomprehensible that our rulers have surrounded themselves with some of
the most experienced specialists in these matters.
If I have been able to gather this information myself, shared, I remind you, by competent
people above all suspicion of conspiracy, such as Hélène Banoun, Pierre Sonigo,
Jean-François Toussaint, Christophe De Brouwer, whose intelligence, intellectual honesty
and legitimacy cannot be questioned, then the Belgian, French and Quebec scientific advisors,
etc., know all this as well.
So?
What's going on?
Why continue in this distorted direction, obstinately making mistakes?
It is not insignificant to reimpose confinements, curfews, quarantines, reduced social
bubbles, to shake up again our shaky economies, to plunge entire families into precariousness,
to sow so much fear and anxiety generating a real state of post-traumatic stress worldwide, to
reduce access to care for other pathologies that nevertheless reduce life expectancy much more
than COVID-19! [24]
Is there intent to harm?
Is there an intention to use the alibi of a pandemic to move humanity towards an outcome it
would otherwise never have accepted? In any case, not like that!
Would this hypothesis, which modern censors will hasten to label "conspiracy", be the most
valid explanation for all this?
Indeed, if we draw a straight line from the present events, if they are maintained, we could
find ourselves once again confined with hundreds, thousands of human beings forced to remain
inactive, which, for the professions of catering, entertainment, sales, fairgrounds,
itinerants, canvassers, risks being catastrophic with bankruptcies, unemployment, depression,
suicides by the hundreds of thousands. [25-26-27-28]
The impact on education, on our children, on teaching, on medicine with long planned care,
operations, treatments to be cancelled, postponed, will be profound and destructive.
"We risk a looming food crisis if action is not taken quickly." [29].
It is time for everyone to come out of this negative trance, this collective hysteria ,
because famine, poverty, massive unemployment will kill, mow down many more people than
SARS-CoV-2!
Does all this make sense in the face of a disease that is declining, over-diagnosed and
misinterpreted by this misuse of overly sensitively calibrated PCR tests?
For many, the continuous wearing of the mask seems to have become a new norm.
Even if it is constantly downplayed by some health professionals and fact-checking
journalists, other doctors warn of the harmful consequences, both medical and psychological, of
this hygienic obsession which, maintained permanently, is in fact an abnormality!
What a hindrance to social relations, which are the true foundation of a physically and
psychologically healthy humanity!
Some dare to find all this normal, or a lesser price to pay in the face of the pandemic of
positive PCR tests.
Isolation, distancing, masking of the face, impoverishment of emotional communication, fear
of touching and kissing even within families, communities, between relatives
Spontaneous gestures of daily life hindered and replaced by mechanical and controlled
gestures
Terrified children, kept in permanent fear and guilt
All this will have a deep, lasting and negative impact on human organisms, in their
physical, mental, emotional and representation of the world and society.
This is not normal!
We cannot let our rulers, for whatever reason, organize our collective suicide any
longer.
Translated from French by Global Research. Original source: Mondialisation.ca
Dr Pascal Sacré is a physician specialized in critical care, author and renowned
public health analyst, Charleroi, Belgium. He is a Research Associate of the entre for Research
on Globalization (CRG)
****
Professionals whose references and comments are the basis of this article in its scientific
aspect (especially and mainly on RT-PCR):
The short answer to both of these questions regarding the COVID-19 'casedemic' and the
fallacy of asymptomatic PCR testing is YES and YES!
The only answer was always yes. No one should be surprised that everyone in the political
'health sector' managed to delay or ignore any real science , not in the name of the truth
mind you, but because of their opposition to the administration.
That's right, there's really no other way to put it. We had initial science, which in any
movie script would have been that one moment where the 'nobody' scientist gets called into
the Whitehouse to explain his life saving discovery. Instead, in our reality, those
scientists were ridiculed and told they were either wrong, or the science wasn't accurate
enough (never mind wanting to further support it so we could confirm or deny). These people
played games in hopes of running out the clock.
Put yourself in an alternate role- if you were in a position to make official guidelines
and recommendations and you realized there was science (mind you, people that spend their
careers doing this) that said 'there is a good probability that doing xyz will save a
life'..would you decide not to explore it? Would you decide not to share it with others?
Wonder what would have happened if let's say, the 'pandemic' would have occurred two years
into presidency instead of the last 3/4 of it. Just throwing that out there for thought.
Now, when the dust settles, suddenly the WHO, Fauci and everyone else is willing to admit
the science. I guess better late than never.
Give Me Some Truth 6 hours ago (Edited)
Plus, "new cases" are almost certainly going to plummet on their own . Reasons: We will
soon leave the "cold land flu" season, fewer people will be tested, and the number of people
who have already contracted the virus continues to grow. This means that the pool of people
who could test positive in the future will be much smaller (because people who have already
had the virus now have acquired natural immunity).
Bottom line: The coming huge decline in "new cases" will almost assuredly have nothing to
do with the number of people who have received both doses of the vaccine.
Demologos 6 hours ago remove link
Masks are great for spreading viruses and bacterial infections unless strict protocols are
followed. Remember last year when every news report on Covid ended with a segment on mask
hygiene and proper fitting? Me neither.
Ajax_USB_Port_Repair_Service_ 8 hours ago (Edited)
The CT will be lowered AFTER 100 days of masks and then the Biden miracle happens.
Luci Feric 8 hours ago
* miracle
You're welcome!
Luci
Ajax_USB_Port_Repair_Service_ 8 hours ago
Thank you Luci. I knew that didn't look right.
Luci Feric 8 hours ago
You're welcome!
karzai_luver 9 hours ago
The WHO/NIH/CDC are political grifters.
The leaderships are political hacks.
Why they still have any cred is unreal.
They have been late wrong and lie forever.
The examples are too numerous to post here.
dark pools of soros 9 hours ago
same reason people still eat fast food... the flashy marketing
crow1234 9 hours ago
Here's my surprised face 😮
F all this ****!
Give Me Some Truth 9 hours ago
Excellent analysis and kudos for highlighting the key role of the PCR tests in
establishing the narrative.
However, the key reason the PCR tests WILL be changed was not mentioned: This HAS to
happen to "prove" that the vaccines "work."
Once the PCR tests are changed, cases will plummet by 90 percent. The "miracle vaccines"
will get all the credit.
More importantly, by changing the PCR tests t his precludes the possibility of large
numbers of people "testing positive" AFTER receiving two doses of the vaccine. This would not
be good for the old credibility and trust of authorities and "public health officials" who
have been pushing mass vaccination.
P.S. I still wonder if the tens of thousands of people in the vaccine trial weren't tested
with PCR tests that had already been "adjusted." This would explain those "95 percent
effective" claims.
tangent 9 hours ago
That is likely all true, but it has the ridiculous flaw of people with the vaccine still
getting the same positive rates as those without the vaccine. Very funny! But then again,
people don't seem to snap into reality when they learn the population is still going up same
as last year and the year before that... very foolish thinking to think that is a
pandemic.
"... As a reminder, "cycle thresholds" (Ct) are the level at which widely used polymerase chain reaction (PCR) test can detect a sample of the COVID-19 virus. The higher the number of cycles, the lower the amount of viral load in the sample; the lower the cycles, the more prevalent the virus was in the original sample. ..."
Right On Cue For Biden, WHO Admits High-Cycle PCR Tests Produce COVID False Positives
BY TYLER DURDEN THURSDAY, JAN 21, 2021 - 6:30
Were the 'conspiracy theorists' just proven right about the "fake rescue plan" for
COVID? Did the 'science-deniers' just get confirmation that it was political after all ? The short answer to both of these questions regarding the COVID-19 'casedemic' and the
fallacy of asymptomatic PCR testing is YES and YES!
We have detailed the controversy surrounding America's COVID "casedemic" and the misleading
results of the PCR test and its amplification procedure in great detail over the past few
months. As a reminder, "cycle thresholds" (Ct) are the level at which widely used polymerase chain
reaction (PCR) test can detect a sample of the COVID-19 virus. The higher the number of cycles,
the lower the amount of viral load in the sample; the lower the cycles, the more prevalent the
virus was in the original sample.
Numerous epidemiological experts have argued that cycle thresholds are an important metric
by which patients, the public, and policymakers can make more informed decisions about how
infectious and/or sick an individual with a positive COVID-19 test might be. However,
as JustTheNews reports, health departments across the country are
failing to collect that data .
In fact, as far
back as October, we brought the world's attention to the COVID-19 "casedemic" and the
disturbing reality of high-cycle threshold PCR tests being worse than useless as indicators of
COVID-19 "sickness".
PJMedia's Stacey Lennox said at the time:
Biden will issue national standards, like the plexiglass barriers in restaurants he spoke
about during the debate, and pressure governors to implement mask mandates using the federal
government's financial leverage.
Some hack at the CDC or FDA will issue new guidance lowering the Ct the labs use , and
cases will magically start to fall.
In reality, the change will only eliminate false positives, but most Americans won't know
that.
Good old Uncle Joe will be the hero, even though it is Deep-State actors in the health
bureaucracies who won't solve a problem with testing they have been aware of for months. TDS
is a heck of a drug.
And now,
as Lennox explains in detail below, we have been proved 100% correct as less than one hour
after President Biden's inauguration, the WHO proved us right .
In August of last year, The New York Times published an article stating that as many as
90% of COVID-19 tests in
three states were not indicative of active illness . In other words, they were picking up
viral debris incapable of causing infection or being transmitted because the cycle threshold
(Ct) of the PCR testing amplified the sample too many times.
Labs in the United States were using a Ct of 37-40. Epidemiologists interviewed at the time
said a Ct of around 30 was probably more appropriate. This means the CDC's COVID-19 test
standards for the PCR test would pick up an excessive number of false positives. The Times
report noted the CDC's own data suggested the PCR did not detect live virus over a Ct of 33.
The reporter also noted that clinicians were not receiving the Ct value as part of the test
results.
Yet a PCR test instruction document from the CDC that had been revised five times as of July 13, 2020 ,
specified testing and interpretation of the test using a Ct of 40. On September 28, 2020, a
study published
in the journal Clinical Infectious Diseases from Jaafar et al. had asserted, based on
patient labs and clinical data involving nearly 4,000 patients, that a Ct of 30 was appropriate
for making public policy. An update to the CDC instructions for PCR testing from December 1, 2020 , still uses a
Ct of 40.
"I am concerned about the interpretation of these recommendations and worried it will give
people the incorrect assumption that asymptomatic spread is not of great concern. In fact it
is."
So, of course, the Mendacious Midget™ had spoken, and the guidelines went back to
testing everyone, all the time, with an oversensitive test.
The idea that asymptomatic spread was a concern as of August was just one of many lies Dr.
Fauci told. At the beginning of the pandemic in late January, he said:
The one thing historically that people need to realize is that even if there is some
asymptomatic transmission, in all the history of respiratory borne viruses of any type,
asymptomatic transmission has never been the driver of outbreaks. The driver of outbreaks is
always a symptomatic person. Even if there is a rare asymptomatic person that might transmit,
an epidemic is not driven by asymptomatic carriers.
There is not a single study or meta-analysis that differs from Fauci's original
assessment.
Today, within an hour of Joe Biden being inaugurated and signing an executive order
mandating masks on all federal property, the WHO
sent out a notice to lab professionals using the PCR test . It said:
WHO guidance Diagnostic testing for SARS-CoV-2 states that careful interpretation of weak
positive results is needed ( 1 ).
The cycle threshold (Ct) needed to detect virus is inversely proportional to the patient's
viral load.
Where test results do not correspond with the clinical presentation, a new specimen should
be taken and retested using the same or different NAT technology.
literally one hour after Biden takes the oath, the WHO admits that PCR testing at high
amplification rates alters the predictive value of the tests and results in a huge number of
false positives pic.twitter.com/iDtXmappRw
This translates to "in the absence of symptoms, a high Ct value means you are highly
unlikely to become ill or get anyone else sick in the absence of very recent exposure to an
infected person."
Most PCR assays are indicated as an aid for diagnosis, therefore, health care providers
must consider any result in combination with timing of sampling, specimen type, assay
specifics, clinical observations, patient history, confirmed status of any contacts, and
epidemiological information.
In short, a positive PCR test in the absence of symptoms means nothing at a Ct of higher
than 30, according to the experts interviewed by the New York Times and according to Jaafar et
al. Yet positive tests is the number CNN loves flashing on the screen.
If the percentage found by the Times in August holds, there have been approximately 2.43
million actual cases to date, not 24.3 million.
There is also no way to calculate the deaths from COVID-19 rather than deaths with some dead
viral debris in the nostrils.
What I have referred to as the "casedemic" since September will be magically solved just in
time for Joe Biden to look like a hero. For doing absolutely nothing.
Do not tell me there is not a politicized deep state in our health agencies. Do not ever
tell me I need to listen to Dr. Anthony Fauci again. And every business owner who has been
ruined because of lockdowns due to a high number of "cases" should be livid. Any parent whose
child has lost a year of school should be furious.
None of this was for your health. It was to get rid of Orange Man Bad.
now they will drop the cycle rates and you can watch the curve go negative... like
magic... because the new magic man isn't the bad man and the masks he ordered
worked!!!!!
As an aside, this also clearly explains the disappearance of the "flu" during this season as
the plethora of high Ct PCR Tests supposedly pointing to a surge in COVID are nothing of the
sort.
As
Stephen Lendman noted previously , claiming "lockdowns stopped flu in its tracks,
(outbreaks) plummet(ting) by 98% in the United States" ignored that what's called COVID is
merely seasonal influenza combined with false positives (extremely high Ct) from PCR-Tests.
And for that reason, the great 2020 disappearing flu passes largely under the mass media's
radar. Media proliferated mass deception and the power of repetition get most people to believe
and having successfully "killed the flu", they will now do the same with COVID... and, if
allowed by our betters, we will all return to the new normal they desire.
Give Me Some Truth 5 hours ago remove link
The governor of Florida has proposed a law that is ingenious, or at least very important
(if passed). He simply wrote into his proposed bill that labs have to disclose the cT levels
in all "positive" COVID results.
He obviously put this language in the bill/regulations because he knew "public health
officials" would try to continue to conceal this information.
If this law is enacted, we will learn WHEN the PCR tests were adjusted . We will then be
able to see how the number of "positive cases" changes (read: declines significantly).
Here's hoping this law is enacted (with no loopholes) ... and that many more states enact
the same legislation.
philipat 9 hours ago
Loved that banner at the Vienna protest last weekend "Make Infuenza Great Again"
Fed-up with being Sick and Tired 7 hours ago
...The CT standards have been all over the place and inconsistent. It became quite clear
to my family and myself when we started readin: "ASYMPTOMATIC COVID cases surge" MONTHS
AGO!
The smartest little kid in our family, a young Girl at age 15 and is a BIG fan of Biology
and has decided that Virology will be her studies in college, said: "Daddy, is there a
disease if there are no symptoms?"
NO ONE AROUND THE TABLE had a clear answer. There were attempts and then the press started
talking: "YOU CAN CARRY COVID and not know it, so wear a mask!!!"
The ludicrous nature this entire charade started to unfold! SO, 40 degrees, you are not
stupid, just ignorant of the facts.
Go out and do your own homework before you continue to act like an expert in Virology. YOU
ARE NOT. We are all bystanders to a fraud perpetrated for nefarious reasons.
Boing_Snap 6 hours ago
Educated people know that these Tests were fake, the propaganda used was not for our
consumption, just the masses whom are only looking at headlines, which is the majority of
humanity.
Putting the manipulation of the tests together with a, heavens forbid a "Conspiracy
Theory", kept the indoctrinated away from looking at it. So now that is changing, good.
The Indoctrinated are most of the population, they range across the spectrum, scholars and
professionals included. Getting them to think for themselves will not be easy.
Oceania2020 6 hours ago (Edited)
Some of the dumbest words ever spoken...
"Google it".
checkessential 4 hours ago
At least FB and Twitter will prove that whatever you Google is true regardless of the
facts.
"So far this season, the county has recorded 39 influenza cases, compared to 1,220 cases
at this point last season. Flu season generally runs from October through May, with flu
activity peaking in December and February. The county says it's "very likely" physical
distancing, hand washing, and mask-wearing are contributing to the low flu activity".
As Fed-up with being Sick and Tired stated - you've got to be absolutely clueless and or
completely ignorant to not see these idiotic and contradictory statements by the San Diego
county health dept.....
When the noble coronavirus is the common flu virus to begin with! Yet, there's record
number of people getting covid all while having historically low cases of the flu _ thanks to
the masks! 🤯🤯 wake up ffs
xpxhxoxexnxixx 5 hours ago
So then how would you explain the inability for the WHO, Fauci and anyone else in that
club not using the publicly available data since April, as you said, and revising the way we
test and measure 'cases'? Biden would never go against the media lol so unless you have a
link gtfo.
MrBoompi 4 hours ago
This is a straw man argument. No diagnostic test like this is 100% accurate and nobody
would ever make such a stupid claim. But what if someone had, accurately, stated that the pcr
test is 5% accurate?
THIS IS TRUE
Ophiuchus PREMIUM 9 hours ago
Do you think they will admit Building 7 was a controlled demolition?
Dash8 6 hours ago
There's nothing left of it, it was all shipped to china with the rest of the
evidence...
Ophiuchus PREMIUM 9 hours ago (Edited)
Do you think they will admit that powerful politicians in America are controlled by sex
with young children?
They will never admit to anything.
All politicians in positions of power, rape and murder children. Lin Wood knows. Start
there.............
"Referring to Speaker of the House Dennis Hastert as a "serial child molester", a federal
judge imposed a sentence of 15 months in prison, two years' supervised release, and a
$250,000 fine. Hastert was imprisoned in 2016 and was released 13 months later." --- Why not
15 years? When politicians in D.C. get caught raping children, it's a slap on the wrist.
Suzy Q 8 hours ago
I have not researched this at all and cannot verify any of it, but here it is
Except, I have looked at the part about wrinkled flags. I can only go so far down the
rabbit hole before I have to stop.
JRobby 7 hours ago (Edited)
Yea, just post it anyway. You are probably safe in a secure area.
There are at least 7 or 8 major Psy Ops running right now not to mention hundreds of minor
ones.
Suzy Q 2 hours ago
There are things that cannot be unseen and I'd prefer not to see those things.
daveO 30 minutes ago (Edited)
"G5 said many other people are going to face justice, but only one will have a public
trial -- John Brennan, the Anti-Trump American intelligence official who served as the
Director of the CIA from March 2013 to January 2017. He will have a public trial, and if
convicted, will be hanged."
If so, I hope the hanging is televised.
"Some find it difficult to believe that McCain and GHWB were executed. What is the point
of killing a dying person?
The point is they cannot escape by retiring, resigning or living out. What they have done
remains, and their families are also demonized. The audience is SPECIFICALLY for DEEP
STATE."
This would explain Beijing Biden's inauguration with 200K flags and no civilians.
Livingston 7 minutes ago
A Pay-Per-View of John Brennan being hanged would be a huge money maker. Could probably
balance the budget singlehandedly!
daveO 38 minutes ago
Bingo! It's why Hunter fled Delaware to marry a "movie producer" in May, 2019.
philipat 8 hours ago
No, that's not how these things work. You NEVER admit anything, just bury the facts,
censor as much as possible (to control the narrative) and stick to the official narrative
always no matter how discredited or ridiculous it may be. In fact, the strategy is "If you
can't win the debate don't have the debate".
And BTW, not only Building 7
Hal n back 7 hours ago (Edited)
Look at your car insurance card. After an accident, do not admit you were wrong.
for that, because of frivilous lawsuts there ends up being unnecessary settlement by
insurers to avoid trial.
the plaintiffs and attys usually avoid a counter suit so they have no problem
Would anything really surprise anyone at this point?
JethroBodine_ 5 hours ago (Edited)
Never ever believe anything the CIA says. Everything they say is a limited hangout.
Planes hit the towers but certainly were not the cause of three sky scrappers falling at
near free fall speed, symmetrically and into their own footprint.
That said, a jumbo jet did not hit the pentagon!
systemsplanet 8 hours ago
One day people who rushed out to inject the covid vaccine will begin to question what the
hell they just injected in their arm.
deadcat2 8 hours ago
The kind of sheep that do that are the sort that complain if there are no lamb chops for
dinner.
prairie oysters PREMIUM 7 hours ago
There is (I hope) a very clever metaphor buried in "lamb chops."
Giant Meteor 6 hours ago
Lambs get slaughtered .. eaten
Or placed in petting zoos
SwmngwShrks 5 hours ago
Its a Simpsons reference..."D'Oh!"
JRobby 7 hours ago
No THEY won't
EVER
Same reason they do this totally obvious $h!t.
GreatUncle 7 hours ago
We can only hope we get too hang people for the "intentional" 1st degree murder of
1000's.
Sick Monkey 7 hours ago
The flu is one of many infectious diseases. It's like we traveled through space and landed
on a planet that has only two infectious diseases. They focus on those two like some sort of
marketing campaign. A gold mine for big tech. Get your shot today! Call now and we'll throw
in another 2 of your choice. Buy one and get another two for free. Limited time offer.
Marla Singer 9 hours ago
When you think about the lengths the permanent fusion party had to go to to get their
candidate over the finish line: constant media bombardment against Trump, nation wide
lockdowns, social media blackouts, election fraud, false flag events, and a militarized
inauguration, I have to imagine it's a pretty fragile win.
camel717 6 hours ago
This is what I've been trying to tell people. After everything the democrats, celebrities
pandering, media etc. did to keep Trump out, as well as the mail in ballots (which, if didn't
happen, Trump would've won in a landslide) did to help Biden win, he barely ******* won. HE
BARELY WON.
It was made out to look like the entire world was against Trump and he still won sans
fraud and mail in ballots.
The future isn't as bleak as people think. There will be another red wave in 2022 I
suspect, unless mail ins continue to be the norm which democrats certainly will try because
it's their only path to victory at this point.
Iron Lady 1 hour ago
Xiden's inauguration video on commietube had 16,000 down votes and 4,000 up votes last I
checked. The views were very low.
Trump's farewell at Andrews had 800,000 views in real time at RSBN.
Cautiously Pessimistic 9 hours ago
It has not even been a full 24hrs since Biden was sworn in and already the shenanigans
have started. Once again, Trump, his administration and that small part of the press that
still has journalistic integrity is proven right. This was predicted. It will be interesting
to see what else moves from the conspiracy theory to the CONSPIRACY FACT column over the next
days and weeks.
" A writ of quo warranto is not a petition, but a notice of demand, issued by a demandant,
to a respondant claiming some delegated power, and filed with a court of competent
jurisdiction, to hold a hearing within 3 to 20 days, depending on the distance of the
respondant to the court, to present proof of his authority to execute his claimed powers. If
the court finds the proof insufficient, or if the court fails to hold the hearing, the
respondant must cease to exercise the power. If the power is to hold an office, he must
vacate the office.
The writ is unlike a petition or motion to show cause, because the burden of proof is on
the respondant, not on the demandant. "
Could be highly entertaining.
Ophiuchus PREMIUM 8 hours ago
It matters not as it will never be covered by the controlled media.
thunderchief 9 hours ago
Scamdemic. Enough said.
GreatUncle 7 hours ago
I prefer to view it as a tool.
The virus was intentionally released to create the desired effect and it was equally
useful to get rid of Trump at the same time.
Still think vaccine id - digital id - digital currency and the economic lock for the
globalists is the end game to usher in the great reset where everybody will be made a
slave.
Even now more and more Karen's are pushing for everybody to be forced vaccinated or
excluded from society where they will die a lingering economic death.
Walter Melon 7 hours ago
Up vote - who here knew this was going to happen a year ago?
AAA 7 hours ago
Not a whole year ago but atleast a couple of months :)
Hal n back 7 hours ago
It started when singapore reported its ct was 35. Not 40.
vealparm 1 hour ago
You can research my posts here....I was proclaiming the "ConVid-19 scam" way back in the
early spring.
I am 77 and have been around the block a few times with lying lawyers and politicians, I
called Fauci an actor/operative the second time I saw him and hear his spiel. The more I
learned about him and his past left me with no doubt.
We have all lived a dystopian tyranny for the past year engineered by world wide hard
Leftists.
Neil Patrick Harris 9 hours ago
Sure the timing is suspect but I doubt they will suddenly lift lockdowns and let us go
back to normal. This is about much more than removing Trump, it's The Great Reset.
Ophiuchus PREMIUM 8 hours ago
I call it the 'Great Extermination'.
Suzy Q 8 hours ago
de Blahsio is demanding NYC reopen, as if it was the business owners that demanded the
shut down. What a clown
philipat 8 hours ago
Yes agreed, Covid was a cover vehicle which allowed various different agendas to be
implemented simultaneously. Primarily the Global financial Reset. And since they are still
not ready with that, the covid scam will have to be extended for a good amount of time yet
(At least another 12-18 months). That is why the "beaking news" about mutations to more
deadly strains which will require new measures, new vaccines etc (Except that, just by magic,
the existing vaccines still work just fine against the existing mutations so the vaccination
campaign can continue. But they seemingly already are able to predict that the future mutant
strains will not and will require new vaccines. More gravy for big pharma, more controls
etc.)
Unknown User 1 hour ago
They want to issue electronic documents and money to control all movement and activity of
the entire world.
OutWithLibs 7 hours ago (Edited)
Passed a line of cars yesterday waiting for the control vaccine. No less than 4 miles
long, undoubtedly several hours in their cars. Upon completing errands I returned the same
way and the line was disbursing. Apparently the county ran out of shots. People are so scared
they'll wait in line for something that is not known to cure anything, caused death after
injection, invented faster than any vaccine in history and has never had trials. The control
is almost complete. Just add vaccination certificates to shop, buy gas, go see grandma, and
the communism will be complete.
CaMuPaSh 9 hours ago (Edited)
You know it's about over when:
Astra-Zeneca mfg. facility in India is burning down (today).
Astra-Zeneca mfg. facility in Wales is in danger of flooding (today).
Pfizer (a Rothschild Co. thanks to E. Macron) has fizzled.
Sputnik (RU) is being accepted by an increasing number of countries. EU, ME SA
Mutti Merkle is going for Sputnik.
...and the U.S.?
....a distant last.
The only thing selling in the ussa is masks (made in CN) for the next 100 days.
Oh, the days of reconciliation and roses are upon us with a vengeance.
Not a vaccine more like gene therapy if it does not use any of the viral component in
it.
So you have the gene therapy but you will still catch the virus the intent is for your
body to have been mutated to switch on your immune system more violently to fight it.
Thing is that response is not going to be good for some folks as the response itself puts
pressure on your body just like the virus.
Virus does not kill you the symptomatic response does.
LA_Goldbug 6 hours ago
The lady's English is not perfect, but the information is very valuable,
We told you there was no pandemic. We kept reporting there were no deaths around us and
some posters kept arguing we were covid holocaust deniers. We were right and you were a shill
for an evil agenda.
The world is under attack. Most governments are onboard. Why do you need a vaccine
passport for a pandemic that never happened?
youngman 8 hours ago
because of the money involved.....billions of dollars for the drug companies
Bob Lidd 8 hours ago
it's all about control at this point.......
steve golf 8 hours ago (Edited)
fake vaccination certificates will be easy to print. Problem is getting it on the
database, if there is one, and there will be, but will airlines check the database or just
look at the certificate?
Cobb 8 hours ago
If only there was a digital certificate or better yet a way to insert a gel into the skin
that could provide pertinent data when scanned.
toejam 2 hours ago
What are you talking about? The vaccine is to kill or maim you. How is this not
understood?
pods 8 hours ago
Is anyone shocked? 100 days of diapers combined with a million or so vaccine shots and
voila, gone by spring.
Nobody will hang. The machine will roll on until the next financial blowup. Then probably
aliens will cause us to print 20 trillion more in debt.
We are Rome, circa 470 AD.
buzzsaw99 8 hours ago
Nobody will hang...
we might hang if we complain about it long enough.
Indelible Scars 8 hours ago
It's hard to believe that people are still falling for this AT ALL.
NIRP-BTFD 8 hours ago
Humanity reached peak stupidity.
AlphaDawg 8 hours ago (Edited)
Hands up, in Feb, March I was worried. An engineered P4 lab CCP virus.
By April, after saying wait for next 2 weeks a couple of times, I realised it was a
complete SCAM.
Not to mention the supression of Hydroxy and airports open.
GreatUncle 7 hours ago
Same ... the reality though never became what was being reported so by end of April I
started having very serious doubts over it. Then the more you learned it became to obvious
this was a hoax "lethal" virus although the virus may exist.
Then you find out that most who actually died were unfit overweight with existing medical
condition to me implies there is a virus but not dangerous to many people.
Now the majority of the population in society because of the Karen's are now incarcerated
by unfit overweight people with 2 or more comorbidities.
No-Go zone 6 hours ago
... that sheeple ...
Lanka 9 hours ago
The false positives of the PCR tests were known 6 months ago. Historically, ZH would have
reported that in timely fashion. Another failure of ZH, cow-towing to the MSM.
NIRP-BTFD 9 hours ago
ZH are opportunistic money makers. They got paid of to do covid propaganda early on.
deadcat2 8 hours ago
Not true. I've read number of articles on ZH saying the PCR test was producing false
positives and posters like me have been saying this from the very beginning. I suggest you
read Lew Rockwell's site if you want a really good insight into the covid farce.
BaNNeD oN THe RuN 6 hours ago (Edited)
There are multiple Tylers reporting multiple POVs.
There is "Wuhan Lab" Tyler, who was dominant at the start.
There is "Daily Case Count" Tyler (similar to MSM).
There is "Covid Conspiracy" Tyler (this article)
There are republished 3rd party blogs.
ImpliedVol 2 hours ago
ZH has been reporting on PCR tests. The first article about it was posted in March of
2020.
masks stopped all other flu but not covid. It takes a ****** commie to believe that.
TRM 5 hours ago
It's the longer name man. You know that 0.1 micron "influenza" is stopped but the 0.1
micron "covid-19" isn't. It's all those extra letters in the name that masks, distancing
& lockdowns work on.
HANGTHEOWL 7 hours ago
"Were the 'conspiracy theorists' just proven right about the "fake rescue plan" for
COVID?"
We are not conspiracy theorists,,,we are people telling you the truth,,,,,,
Notice even when they have to admit we were right,,they try to demonize us at the same
time,,,,,,
uchibenkei 6 hours ago
yeah. were the conspiracy theorists right? why not ask "were the mainstreamers lying this
whole time?"
HANGTHEOWL 6 hours ago
egg-zactly,,,,,,
deadcat2 8 hours ago
I'm in the UK (a cesspit on the edge of Europe) and I've been asking from the start,
including emailing members of parliament, who decided that the PCR test should be amplified
45 times? Was it a government minister, some committee of scientists, or the laboratories
themselves? WHO MADE THE DECISION to amplify the PCR test 45 times and why? The creator of
the test, Kerry Mullis, stated that it should never be amplified more than 30 times. He even
said the PCR test wasn't suitable to test for an infection either.
Had the test been limited to 30 times, there would have been next to no 'cases' as they
are called and perfectly healthy people with no symptoms would not find themselves under
house arrest in their millions.
Stinkbug 1 8 hours ago
And where is Kerry Mullis now, when we need him? Dead. A couple of months after exposing
Fauci publicly, died at age 56 of 'pneumonia'.
Parasiticfilth 2 hours ago (Edited)
So if COVID is so contagious, why do they have to go all the way up your nasal cavity,
almost to your brain to get a sample?
Shouldn't there be samples everywhere?
I mean apparently the virus spreads faster than Kamala Harris' legs.
HANGTHEOWL 2 hours ago
That is just another part of this hoax that does not make sense,,,,,,if you dig into the
history of virology,,you find the same nonsense time and time again,,,,,take rabies for
instance,,,they say that rabies is transmitted by the saliva of the animal when it bites
you,,,,but they have to kill the animal and check the brain to actually see if it had
rabies,,,,,,why not just test the saliva,,,???,,why,,,??,,because rabies is just another
fraud,,,,
duck_fur 2 hours ago
I'd never put those two things together. You're right. Why not test the saliva since it
was the alleged vector of transmission? That really does not make sense.
HANGTHEOWL 1 hour ago
Many years ago,,I read an old study from some university they did back in the early
40's,,maybe even 30's,,,where they took the heads of dogs that had died from natural
causes,,and sent them in to be tested for rabies,,,,they came back positive,,,,it seems what
they test for in the brain as a marker for rabies,,,is also found in healthy brains,,,,,,it
is just another one of the fraud Louis Pasteur's scams,,,
duck_fur 2 hours ago
Hehe...that's funny right there. Upvote for you.
WesternCommunity 2 hours ago
Heels Up Harris. Pulled herself up by her kneepads, with the ugly looks like a polished
turd Willie Brown, Speaker of the Calffornia State Assembly.
Cobb 8 hours ago
Day 2 of Biden regime and he's still a huge POS.
Smokey PREMIUM 8 hours ago
Getting huger by the hour
Farmerz 6 hours ago
Trump was stupid not to fire this Fauci guy, another Clinton lapdog.
Eric Post 6 hours ago
Fauci is civil service, it doesn't not come under any president to fire him.
Farmerz 6 hours ago
We all read the tweets Fauci wrote "fawning" over Clinton here on ZH months ago. At
minimum, Trump could have brought out a different face explaining the test cycle standard the
CDC was using. Could have been mentioned at the debates. Wasn't.
Trump just didn't do his homework.
Iron Lady 1 hour ago
Please. If Trump had pushed back at all they would have just called him a science denier
like they do the rest of us.
Red Corvair 6 hours ago
Trump is not part of the establishment, but he was part of the game all along. He never
drained that swamp. And look and behold, that swamp is more alive and kicking than ever.
Hoss N. Pfeffer 4 hours ago
And now after defeating Trump the alligators are emboldened, aggressive, and hungry.
Everybody All American 6 hours ago
Dr. Fauci was brought to the fore by none other than Mike Pence I do beilieve.
Reaper 6 hours ago
Everything the government says is a lie.
Voice_of_Doom 6 hours ago
Just goes to show you the amazing power the globalist have and how well organized they
are.
LA_Goldbug 6 hours ago
They own the Media and the Politicians !!!!
scytalerules 6 hours ago
"globalists" "chicoms" lol
George Bayou 6 hours ago
They still can't prove effectiveness of masks but continue to swear by them.
convid21 7 hours ago
Even with a CT of 30, your still going to get 50% false positives
At 15 you'd get some Negatives but not many false Positives.
This test should not be used it's not accurate, not reliable and not fit for purpose.
It's doesn't have any science in it all.
The Governments are only using this to invoke fear in the Public by finding False
Positives.
In their view it's better to find more than less, and more leads to lockdowns which
demands a VAXX.
Which means the VAXX is a result of Fraud.
Pair Of Dimes Shift 7 hours ago
The nasal test is QUANTITATIVE not QUALITATIVE.
Completely useless for the application.
Even the antibody test isn't 100% because not everybody produces IgG all of the time when
an infection is present.
Anyone who believes in it is a paid-for moron, or maybe just a common or garden idiot.
Obamanism666 2 hours ago
Start wearing the mask or 2 masks then go up to Karens and lambast them for only one mask.
The mask is also good for hiding your mouth when doing sheep sounds...... drive the Karens
crazy.
Made sheep sounds on the subway today, 5 People got really upset.
Could be even better that wearing a MAGA hat to trigger them.
If caught just say "well if I act like a sheep, I might as well sound like one"
You appear to be the last remaining covidtard troll in the group downvoting everyone.
Soon, you will be out of a job trolling on here. 🤣🤣🤪🤪
Klaus Smith 6 hours ago
Creepy Joe just inaugurated and Covid disappears. YES! That's the hero we need! Hail
Biden!
Space-Time Continuum 7 hours ago (Edited)
All thanks to the most popular president of all times, as we've seen all those million
people there at the inauguration cheering for him.
Pro_sanity 1 hour ago
It still sucks to be vindicated. Plus it was so obvious. Anyone who didn't see through
this from very early on is a total nit wit who shouldn't be allowed to even drive a car.
Shirley Yugest 6 hours ago
There is no covid-19 pandemic. There is only covid-19 panic. The reason for this is the
"DEM" in panDEMic is now in the WH.
9-Month Cycle 7 hours ago
We knew that last year. The inventor himself let everybody know what was up with AIDS
testing in Africa years ago. Run it over and over and over and everybody is positive.
Come on, man!! David Icke.... Alex Jones..... do you not gather information online? Only
watch the boob tube?
Pair Of Dimes Shift 7 hours ago
Welcome to what some of us knew 6 months ago, normie sheep!
In the setting of COVID-19, almost every country in the world closed its borders, locked
down its citizens, and forced businesses to close. Today, most governments still restrict
travel, economic activity, and social gatherings.
The justification for these unprecedented measures has been a growing number of COVID-19
cases. This has unleashed an epidemic of COVID testing - with PCR and rapid antigen tests as
the means of identifying positive COVID cases. Our very own Dr. John Hunt examines the science
behind COVID testing, whether the testing paradigms are effective, and the rationality behind
government response to the virus.
What COVID tests mean and don't mean
RT-PCR tests can be designed to be highly sensitive to the presence of the original viral
RNA in a clinical sample. But a highly sensitive test risks poor specificity for actual
infectious disease.
Rapid antigen tests are different. They measure viral protein. They do so by reacting a
clinical sample with one or two lab-created antibodies that are labeled with a measurable
marker. These antigen tests are often poorly specific, meaning they can show as positive in the
absence of any actual viral protein or any COVID disease.
For a lab test, what does it
mean to be sensitive ? What does it mean to be specific ?
I'll use COVID to help explain these terms. In order to do this correctly, we need to avoid
using the language of the media and government because those institutions tend to mislead us
via language manipulation. For example, they've wrongly taught us that a COVID-positive test is
synonymous with COVID- disease. It isn't, as you will soon see.
So for this article, I will use the term "Relevant Infectious COVID Disease" to mean a
condition, caused by COVID-19, in which a patient is sickened by the virus or has (in their
airways) living replicating virus capable of being transmitted to others. This seems a fair
definition of what we should be caring about in this disease. If the patient isn't sick and
isn't capable of transmitting the disease, then any COVID RNA or protein that may appear in a
test is not relevant, nor infectious, and therefore of little to no consequence.
You can think of a test's sensitivity like this: In a group of 100 people who absolutely
have Relevant Infectious COVID Disease, how many people does the test actually report as
"positive?" For a test that is 95% sensitive, 95 of these 100 patients with the true disease
will be reported by the test as COVID positive and 5 will be missed.
Specificity : In a group of 100 people who absolutely do not have Relevant Infectious COVID
Disease, how many will be reported by the test as "negative?" For a test that is 95% specific,
95 of these healthy people will be reported as COVID-negative and 5 will be incorrectly
reported as COVID-positive
Sensitivity and Specificity are inherent characteristics of a test, not of a patient, not of
a disease, and not of a population. These terms are very different than Positive Predictive
Value (PPV) and Negative Predictive Value (NPV). PPV and NPV are affected not only by the
test's sensitivity and specificity but also by the characteristics of the people chosen to be
tested and, particularly, the patients' underlying likelihood of actually having true Relevant
Infectious COVID Disease. The Positive Predictive Value -- the chance a positive test actually
indicates a true disease -- is greatly improved if you test people who are likely to have
COVID, and, importantly, avoid testing people unlikely to have COVID.
If you do a COVID test with 95% sensitivity and 95% specificity in 1,000 patients who are
feverish, have snot pouring out of their noses, are coughing profusely, and are short of
breath, then you are using that test as a diagnostic test in people who currently have a
reasonable up-front chance of having Relevant Infectious COVID Disease. Let's say 500 of them
do actually have Relevant Infectious COVID Disease, and the others have a common cold. This 95%
sensitive test will correctly identify 475 of these people who are truly ill with COVID as
being COVID-positive, and it will miss 25 of them. This same test is also 95% specific, which
means it will falsely label 25 of the 500 non-COVID patients as COVID-positive. Although the
test isn't perfect it has a Positive Predictive Value of 95% in this group of people, and is a
pretty good test overall .
But what if you run this very same COVID test on everyone in the population? Let's
guesstimate that the up-front chance of having Relevant Infectious COVID in the US at this
moment is about 0.5% (suggesting that 5 out of 1000 people currently have the actual
transmittable disease right now, which is a high estimate). How does this same 95%
sensitive/95% specific test work in this screening setting? The good news is that this test
will likely identify the 5 people out of every 1000 with Relevant Infectious COVID! Yay! The
bad news is that, out of every 1000 people, it will also falsely label 50 people as
COVID-positive who don't have Relevant Infectious COVID. Out of 55 people with positive tests
in each group of 1000 people, 5 actually have the disease. 50 of the tests are false positives.
With a Positive Predictive Value of only 9%, one could say that's a pretty lousy test. It's far
lousier if you test only people with no symptoms (such as screening a school, jobsite, or
college), in whom the up-front likelihood of having Relevant Infectious COVID Disease is
substantially lower.
The very same test that is pretty good when testing people who are actually ill or at risk
is lousy when screening people who aren't.
In the first scenario (with symptoms), the test is being used correctly for diagnosis. In
the second scenario (no symptoms), the test is being used wrongly for screening .
A diagnostic test is used to diagnose a patient the doctor thinks has a reasonable chance of
having the disease (having symptoms like fever, cough, a snotty nose, and shortness of breath
during a viral season).
A screening test is used to check for the presence of a disease in a person without symptoms
and no heightened risk of having the disease.
A screening test may be appropriate to use when it has very high specificity (99% or more),
when the prevalence of the disease in the population is pretty high, and when there is
something we can do about the disease if we identify it. However, if the prevalence of a
disease is low (as is the case for Relevant Infectious COVID) and the test isn't adequately
specific (as is the case with PCR and rapid antigen tests for the COVID virus), then using such
a test as a screening measure in healthy people is forcing the test to be lousy. The more it is
used wrongly, the more misinformation ensues.
Our health authorities are recommending more testing of asymptomatic people. In other words,
they are encouraging the wrong and lousy application of these tests. Our health officials are
doing what a first-year medical student should know better than to do. It's enough of a
concerning error that it leaves two likely conclusions:
1) that our leading government health officials are truly incompetent and/or
2) that we, as a nation, are being intentionally gaslighted/manipulated. Or it could be
both.
(Another conclusion you should consider is that my analysis of these tests is incorrect.
I'm open to a challenge.)
So what if you, as an individual, get a positive PCR test result (one that has 95%
specificity) without having symptoms of COVID-19 or recent exposure to a true Relevant
Infectious COVID Disease patient? What do you do? Well, with that positive test, your risk of
having COVID has just increased from less than 5 in 1,000 (the general population risk) to
about somewhere perhaps 5 in 55 (the risk of actual Relevant Infectious COVID Disease in
asymptomatic people with a COVID-19-positive test). That's an 18-fold increase in risk,
amounting to a 9% risk of you having Relevant Infectious COVID Disease (or a 91% chance of you
being totally healthy). That may be a relevant increase in risk in your mind, enough that you
choose to avoid exposing your friends and family to your higher risk compared to the general
population. But if the government spends resources to contact-trace you, then they are
contact-tracing 91% of people uselessly. And they are deciding whether to lock us down based on
the wrong notion that COVID-positive tests in healthy people are epidemiologically accurate
when indeed they are mostly wrong.
For the 50 asymptomatic low-risk people falsely popping positive out of each group of 1,000,
what makes them pop positive? For a rapid antigen test, it is because the test is never meant
for use as a screening test in healthy asymptomatic people because it's not specific enough.
For a PCR test, positivity confidently means that there was COVID RNA in that sample, sure, but
your nose or mouth very likely just filtered some dead bits of viral debris from the dust
particles in the air as you walked through CVS to get the test before you learned you were
supposed to use the drive-through. PCR can be way too sensitive.
A few strands of RNA are irrelevant. Even a few hundred fully intact viral particles are not
likely to infect or cause disease. Humans aren't that wimpy. But keep in mind that there is a
very small chance that the test popped positive because you are about to get sick with
COVID-19, and the test caught you, by pure luck, just before you are to become sick.
On top of this wrong use of diagnostic tests as screening tests, the government has been
subsidizing hospitals for taking care of COVID-19-positive patients. Let's say a hospital
performs a COVID test 4 times during a hospital stay as a screening test in a patient who has
no symptoms of COVID. If that test pops positive once and negative three times, the hospital
will report that patient as having COVID-19, even though the one positive result is highly
likely to have been a false positive. Why do hospitals do this testing so much? In part,
because they'll get $14,000 more from the government for each patient they declare has
COVID-19.
When we see statistics of COVID-19 deaths, we should recognize that some substantial
percentage of them should be called "Deaths with a COVID-19-positive test." When we see reports
of case numbers rising, we should know that they are defining "case" as anyone with a
COVID-19-positive test, which, as you might now realize, is really a garbage number.
Summary:
We have an epidemic of COVID-positive tests that is substantially larger than the
epidemic of identified Relevant Infectious COVID Disease. In contrast, people with actual,
mild cases of COVID-disease aren't all getting tested. So the data, on which lockdowns are
supposedly justified, are lousy.
The data on COVID hospitalizations and deaths in the US are exaggerated by a government
subsidization scheme that incentivizes the improper use of tests in people without
particular risk of the disease.
Avoid getting tested for COVID unless you are symptomatic yourself, have had exposure to
someone who was both symptomatic and tested positive for COVID, or have some other personal
reason that makes sense.
Know that getting tested before traveling abroad puts you at a modest risk of getting a
false-positive test result, which will assuredly screw up your trip. It's a new political
risk of travel.
There is a lot more to this viral testing game, and there are a lot of weird incentives.
There are gray areas and room for debate.
Yes, the COVID disease can kill people. But a positive test won't kill anybody. Sadly,
every COVID-positive test empowers those politicians and bureaucrats who have a
natural bent to control people -- the sociopaths and their ilk.
* * *
John Hunt, MD is a pediatric pulmonologist/allergist/immunologist, a former tenured
Associate Professor and academic medical researcher, who has extensive experience and
publications involving PCR, antigen testing, and analysis of respiratory fluid. He is
internationally recognized as an expert in aerosol/respiratory droplet collection and analysis.
He's also Doug Casey's coauthor for the High Ground novels Speculator, Drug Lord, and the just-released
Assassin , and he is a founding member of the LLC that owns International Man.
* * *
Unfortunately, most people have no idea what really happens when a government goes out of
control, let alone how to prepare How will you protect yourself in the event of an economic
crisis? New York Times best-selling author Doug Casey and his team just released a guide that
will show you exactly how.
Click here to download the PDF now .
Mike Ellwood (Oxon UK) , Jan 9, 2021 1:09 AM Reply to
George Mc
I presume that people who get the vaccine(s) will then start testing positive with the PCR
test, if they are tested soon afterwards, or even some time afterwards. And so they should,
really, since, in a sense, they have been "infected" with some version of the so-called
virus. At least that's more or less how vaccination is supposed to work, isn't it?
If that does start happening, I will be fascinated (in a blackly comic way) to see the
official reaction. I think it's all going to go very pear shaped (even more than it is now),
in ways we probably can't begin to imagine yet.
The origins of the RT-PCR on which it is based our whole strategy against the Covid-19
pandemic, how it was created and in a rush published in a scientific private review, without
obliged previous peer review, and which the conflict of interests are and how some people are
profiting from this pandemic:
WHO (finally) admits PCR tests create false positives Warnings concerning high CT value of
tests are months too late so why are they appearing now? The potential explanation is
shockingly cynical. Kit Knightly
While this information is accurate, it has also been available for months, so we must ask:
why are they reporting it now? Is it to make it appear the vaccine works?
The "gold standard" Sars-Cov-2 tests are based on polymerase chain reaction (PCR). PCR
works by taking nucleotides – tiny fragments of DNA or RNA – and replicating them
until they become something large enough to identify. The replication is done in cycles, with
each cycle doubling the amount of genetic material. The number of cycles it takes to produce
something identifiable is known as the "cycle threshold" or "CT value". The higher the CT
value, the less likely you are to be detecting anything significant.
This new WHO memo states that using a high CT value to test for the presence of Sars-Cov-2
will result in false-positive results.
To quote their own words [our emphasis]:
Users of RT-PCR reagents should read the IFU carefully to determine if manual adjustment
of the PCR positivity threshold is necessary to account for any background noise which may
lead to a specimen with a high cycle threshold (Ct) value result being interpreted as a
positive result.
They go on to explain [again, our emphasis]:
The design principle of RT-PCR means that for patients with high levels of circulating
virus (viral load), relatively few cycles will be needed to detect virus and so the Ct
value will be low. Conversely, when specimens return a high Ct value, it means that many
cycles were required to detect virus. In some circumstances, the distinction between
background noise and actual presence of the target virus is difficult to ascertain.
Of course, none of this is news to anyone who has been paying attention. That PCR tests
were easily manipulated and potentially highly inaccurate has been one of the oft-repeated
battle cries of those of us opposing the "pandemic" narrative, and the policies it's being
used to sell.
Many articles have been
written about it, by many experts in the field, medical
journalists and other
researchers . It's been commonly available knowledge, for months now, that any test using
a CT value over 35 is potentially meaningless.
Dr Kary Mullis, who won the Nobel Prize for inventing the PCR process, was clear that it
wasn't
meant as a diagnostic tool , saying:
with PCR, if you do it well, you can find almost anything in anybody."
And, commenting on cycle thresholds, once said:
If you have to go more than 40 cycles to amplify a single-copy gene, there is something
seriously wrong with your PCR."
Even Dr Anthony Fauci has publicly admitted that a cycle
threshold over 35 is going to be detecting "dead nucleotides", not a living virus.
Despite all this, it is known that many labs around the world have been using PCR tests
with CT values over 35, even into the low 40s.
So why has the WHO finally decided to say this is wrong? What reason could they have for
finally choosing to recognise this simple reality?
The answer to that is potentially shockingly cynical: We have a vaccine now. We don't need
false positives anymore.
Notionally, the system has produced its miracle cure. So, after everyone has been
vaccinated, all the PCR tests being done will be done "under the new WHO guidelines" ,
and running only 25-30 cycles instead of 35+.
Lo and behold, the number of "positive cases" will plummet, and we'll have confirmation
that our miracle vaccine works.
as long as we all do as we're told. Any signs of dissent – masses of people refusing
the vaccine, for example – and the CT value can start to climb again, and they bring back
their magical disease .
Hugo , Dec 21, 2020 4:14 AM
In an interview, Dr. Wodarg said he had checked his own blood oxygen saturation with a
simple test on his finger after wearing a mask for several minutes. It had dropped from 98
to 94 percent. It is different when climbers hike in regions with low oxygen levels; the
organism gets used to this and reacts by producing red blood cells. 50 percent of the
oxygen we take in is consumed by our brain alone.
That is why the consequences for children wearing a mask are so devastating: their
brains are still growing. The constant inhalation of their own carbon dioxide makes them
sleepy, lame, unfocused and listless. In addition, the mask creates a hotbed of moisture in
which germs thrive. If, on the other hand, we snort into the crook of our arms, they dry
out. Open windows prolong life. Especially for smokers, whose organism is pre-damaged, for
example, by a lifelong lack of oxygen.
TFS , Dec 20, 2020 11:09 AM
Former Brexit Party letter to the Secretary of State for Health:
Excellent letter, reply requested by 22 December. A long list of questions to be
answered but, if the Government truly has a grip on what they are doing and can demonstrate
that they have the supporting evidence, the questions should not be difficult to answer.
When I was a civil servant in a London HQ many years ago now, we regularly received
requests like this, often with 24 hours notice to reply, and we would have to drop
everything else to deal with them. All the receiving Minister's office do is send the
request to the appropriate policy unit where responsibility for drafting answers could be
shared between any number of staff – one member of staff might deal with, say, three
simple questions or one more complex question. But meeting the deadline should not be a
problem if one assumes the information is readily accessible as we would be led to believe.
We shall see.
Quote from letter: "We trust that this letter will be taken seriously"
In my best pantomime voice 'Oh no it won't.'
aspnaz , Dec 20, 2020 2:33 AM
Read chapter 11 "What happened to the scientific method" of Kary Mullis's (inventor of
the PCR test) "Dancing in the mind field" ( https://b-ok.cc/book/1523791/8aa4c2 ) to get his
take on why these people are so corrupt.
In summary, he describes what I would call the "Science Industrial Complex" which is
basically useless people leaching money from the government teat by creating "imminent
disasters" that scare the population, and hence motivate the politicians, into handing out
research grants for the most ridiculous projects without any real scientific proof, such as
climate change.
Here is an extract:
Imagine two hypothetical labs competing for public funds.
One of those labs announces in a series of scientific papers that they have found some
unexpected and very interesting phenomena in the upper atmosphere that contradict the
currently accepted theories on the radiogenic formation of carbon-14. This could have a
dramatic impact on the radioisotopic dating of fossils. The time frame for human evolution
might be a tenth of what has previously been concluded. We may have evolved from the
fossils in the Oldavai Gorge in only a couple of hundred thousand years. All of biology may
be much younger than we think. More research would be required to confirm this. Biologists
all over the world are curious and very excited. The lab is requesting a million dollars
from the National Science Foundation to conduct a more detailed study.
A second lab working on upper atmospheric physics calls a press conference to report
preliminary data on what appears to be a giant hole in the ozone layer and warns the
reporters that if something isn't done about it -- including millions of dollars in grants
to study it further -- the world as we know it will be coming to a tragic end. Skin cancer
is epidemic, and there are reports of sheep going blind from looking up to the sky. People
are starting to worry about having sunglasses that shield their eyes from ultraviolet
light. Children begin to learn about it in school, and they are taught to notice the
intensity of the UV light when they get off the bus.
Which one of these two laboratories will get funding? Follow the money trail from your
pocket to the laboratories and notice that it passes through politicians who need you and
by the interest groups who with the media train you.
from "Dancing in the mind field" by Kary Mullis, inventor of the PCR test.
There are different sciences that use different methods. The so-called "scientific
method" itself is based on speculative philosophical principles that cannot be proven in or
by science since they specify the very conditions required for the scientific knowledge
process to exist and to operate.
Mirriam-Webster defines it as: "principles and procedures for the systematic pursuit of
knowledge involving the recognition and formulation of a problem, the collection of data
through observation and experiment, and the formulation and testing of hypotheses".
Can you illustrate your point with some examples of scientific methods that differ from
the above?
I think that Mullis is pointing out where the above scientific method, however you may
want to describe it but involving the fundementals of proof of a hypothesis using empirical
evidence, has been overtaken by commercial interests in a way that uses the credibility of
the scientific method to sell untested hypotheses that provide some financial gain to the
sponsor.
"... PCR-tests (their essential details are not known to you or me) can be easily used to artificially, adjust" the number that you need as a legitimatization for your politics. Yes, there are without doubt that many dead people. ..."
the paper that established the Drosten PCR test for the Wuhan strain of coronavirus that
has subsequently been adopted with indecent haste by the Merkel government along with WHO
for worldwide use–resulting in severe lockdowns globally and an economic and social
catastrophe–was never peer-reviewed before its publication by Eurosurveillance
journal. The critics point out that, "the Corman-Drosten paper was submitted to
Eurosurveillance on January 21st 2020 and accepted for publication on January 22nd 2020. On
January 23rd 2020 the paper was online."
Incredibly, the Drosten test protocol, which he had already sent to WHO in Geneva on 17
January, was officially recommended by WHO as the worldwide test to determine presence of
Wuhan coronavirus, even before the paper had been published.
As the critical authors point out, for a subject so complex and important to world
health and security, a serious 24-hour "peer review" from at least two experts in the field
is not possible.
How is it possible that a credible scientific study in the means to test for COVID-19 is
completed, peer-reviewed and accepted as the general standard in less than a couple of weeks
after China announces the emergence of a new virus ?????
How is it possible that a credible scientific study in the means to test for COVID-19 is
completed, peer-reviewed and accepted as the general standard in less than a couple of
weeks after China announces the emergence of a new virus ?????
Thank you for every word in your post. +++ The frenetic scramble to demonstrate the
infallibility of private financed science over public funded and cautious institutions seems
to be the driver here. As soon as I grasped the Bill Gates link with the WHO it was clear
that neo liberal economics had engulfed the world leading health institution.
You simply cannot believe their blather as it is entirely at the service of neo liberal
economics and therefore propaganda first, second, and third with a veneer of science fact
somewhere.
Down South | Dec 13 2020 21:06 utc | 36 and @vk 30
I applaud you, Down South, and I cannot see the qualification vk has for his claims. I
would not sign each sentence of the Engdahl paper but as a gross evaluation it is
correct.
If you get a PCR test done in Germany you cannot be sure that the ORF-1-gen, that is specific
for CoV-2, has been tested too. So this test may mistake with Corona-something. You cannot
learn the applied number of cycles which is of essential importance for the interpretation of
this test.
The test was not seriously validated. There was no need to speed up with this paper at
Eurosvurveillance, justified only for selling the test. Drosten is co-editor of
Eurosurveillance. Undeclared conflicts of interest are, in my opinion, reason enough to
reject this paper.
And, @vk, I have no idea about your motivation to spread this propaganda. In Germany there is
now very heavy censorship also in social media. What you cite is the standard excuse those
lovers of censorship sell here.
Sorry, that is nonsense. The Drosten paper has not been peer-reviewed. That first. How
deep the scientific flaws in it are neither you or I can assess. And the hair-rising
conflicts of interest were never communicated.
As sad canuck | Dec 13 2020 22:45 utc | 48 showed with a brilliant example these
PCR-tests (their essential details are not known to you or me) can be easily used to
artificially, adjust" the number that you need as a legitimatization for your politics. Yes,
there are without doubt that many dead people. But again: in this politicized
environment neither you nor I know what the reason of their death was.
...Even if we assume that half of the PCR covid results are false positives, what would
that establish? Wouldn't that just demonstrate that the fatality rate is twice as high? And
isn't diagnosis still done by a doctor anyway? The tests are just screening.
Basically, what is with the hyperventilating about false positives? What am I missing
here?
7) China is doing PCRs since the dawn of time and there is not an explosion of new cases
as the anti-PCR squad is claiming. On the contrary: when they decided to re-test all the
Wuhan inhabitants with obligatory PCR tests, they found none, zero, nada positive
results.
Posted by: Down South | Dec 13 2020 17:55 utc | 16
Posted by: vk | Dec 13 2020 18:45 utc | 19
As I understand it, the false positives are a result of poorly conducting the analyses
through putting the samples through too many cycles. If you intensify the concentration of
the virus more than 25 cycles, you are likely to get false positives. This apparently has
been a problem in the US and other EU countries.
Any country that conducts the test properly significantly reduces the probability of false
positives.
None of them are arguing that COVID-19 does not exist, it is that the maximum reasonably
reliable Ct value is 30 cycles.and as you increase the cycles above that you start getting
more false positive results as only non-infectious (dead) viruses are detected.
The issue that the report raised is that the WHO and Drosden are recommending a Ct of
45 . The higher the cycles the more the "cases" the more drastic the action the
government will take to bring the number of "cases" down.
Therefore, to ensure that the government action is reasonable it is necessary to ensure
that the information the government is using to justify such action is indeed reasonable and
justifiable.
You have to be an absolute idiot to think that government diktats should simply be obeyed
and not questioned especially by people who have the necessary credentials to evaluate such
information.
Well, it is sad to note absolute lack of intellectual curiosity about something that most
likely will not pass without profoundly changing western societies. On side note it would be
good to recognise both taoist and christian way of handling the exception of sickness –
being sick of sickness is way less dangerous than people being religiously afraid of
contamination, of sick people, and organising accordingly.
Most likely this, now already mental, curse will not pass before one or all of the
following happens:
– forced vaccination using either public or private coercion or both,
– global (or regional) digital health IDs and tracking systems,
– social, health and education sectors of lesser states will be overridden and forced
open to global international providers,
– not to mention that the precendent of tiers and lockdowns is established and can be
used repeatedly for the purpose of global health imperialism. There'll be the mandate to
force people self-isolate as well.
One could say these are the markings of global sanitary dictature. Or, this could be the
way to make formal the hidden features of the system currently in use. The spooky license
will be made official. All the tracking, etc.
The Drosten testing non-protocol is faulty to the core, and – without doubt –
it is enabling corruption of both politics and science (cormandrostenreview.com).
Resulting actions are criminal in their essence – that is the reason why we are
seeing leaders of nations acting in such a bizarre way. The truth is being established by the
means of spectacle. Once harsh and overdecisive, then lacking in resoluteness – even in
the EU the countries still can not coordinate simple and relevant statistics.
China has nothing to gain from this virus, hence there it is mostly over and done with.
Seems to go for Russia as well.
vk @ 40 said "of course the scientific standards for times of emergency do fall because of
time constraints. That doesn't mean the debunk attempts aren't equally flawed".
I'm sorry but this is not the way science works and cutting corners during emergencies is
an even worse practice. The amplification issue, lack of Standard Operational Protocol, and
clear bias and hijacking of the peer review process for this paper which formed the
foundation of PCR implementation is utterly and completely outrageous. But of course not
surprising. It's clear that all UN agencies including WHO have been corrupted. Right from the
beginning there has been a consistent and widespread effort to discredit any testing method
aside from PCR. Are you not even remotely interested why?
It's easy to see how COVID testing with a flawed PCR testing procedure rolls out and I
will give you an example from a place that I am familiar with. COVID has magically
disappeared in Thailand, but large number of positive cases are appearing in Thai who are
returning and in foreign visitors. These PCR positives are occurring in spite of all
returnees having tested negative just prior to boarding their flight to Thailand. Almost all
of the positives in returning residents are also of the asymptomatic variety. I would wager
that the amplification level for a domestic PCR test is 25 while the returning resident test
level is set at 35 or higher. Lacking transparency and a Standard Operational Protocol for
the RT-PCR test, including a universally accepted amplification level, you can create any
result you want, any time, any place. These are serious issues and you can't label people who
have issues with scientific integrity as deniers or misleading.
The entire justification of PCR as a public health tool (as opposed to a diagnostic tool)
has been vaporized and I cannot for the life of me understand why you don't "get it" or the
wider implications.
Cycle threshold is everything with the PCR test. Anything above 35 is rubbish. 97% false
positives. Chris Martenson just presented some compelling information regarding these tests.
A recent paper basically shoots down a paper ( Corman-Drosten paper ) that was rushed to
press (before any real peer review) in January 2020 that declared the PCR test the end all
best way to test for covid. NOT TRUE. It was never meant for this purpose and is now being
grossly abused by TPTB. The paper says:
3. The number of amplification cycles (less than 35; preferably 25-30 cycles); In case of
virus detection, >35 cycles only detects signals which do not correlate with infectious
virus as determined by isolation in cell culture [reviewed in 2]; if someone is tested by PCR
as positive when a threshold of 35 cycles or higher is used (as is the case in most
laboratories in Europe & the US), the probability that said person is actually infected
is less than 3%, the probability that said result is a false positive is 97% [reviewed in
3]
Most testing sites are using a cycle threshold of 40 or more meaning the results mean
nothing. In fact many labs are using a CT of 47! The paper goes on to say:
3. The number of amplification cycles It should be noted that there is no mention anywhere
in the Corman-Drosten paper of a test being positive or negative, or indeed what defines a
positive or negative result. These types of virological diagnostic tests must be based on a
SOP, including a validated and fixed number of PCR cycles (Ct value) after which a sample is
deemed positive or negative. The maximum reasonably reliable Ct value is 30 cycles. Above a
Ct of 35 cycles, rapidly increasing numbers of false positives must be expected . PCR data
evaluated as positive after a Ct value of 35 cycles are completely unreliable. Review Report
by an International Consortium of Scientists in Life Sciences (ICSLS) - Corman-Drosten et
al., Eurosurveillance 2020 (Updated: 29.11.2020) Citing Jaafar et al. 2020 [3]: "At Ct = 35,
the value we used to report a positive result for PCR, <3% of cultures are positive." In
other words, there was no successful virus isolation of SARS-CoV-2 at those high Ct values.
Further, scientific studies show that only non-infectious (dead) viruses are detected with Ct
values of 35 [22]. Between 30 and 35 there is a grey area, where a positive test cannot be
established with certainty. This area should be excluded. Of course, one could perform 45 PCR
cycles, as recommended in the Corman-Drosten WHO-protocol (Figure 4), but then you also have
to define a reasonable Ct-value (which should not exceed 30). But an analytical result with a
Ct value of 45 is scientifically and diagnostically absolutely meaningless (a reasonable
Ct-value should not exceed 30). All this should be communicated very clearly. It is a
significant mistake that the Corman-Drosten paper does not mention the maximum Ct value at
which a sample can be unambiguously considered as a positive or a negative test-result. This
important cycle threshold limit is also not specified in any follow-up submissions to
date.
Hillary's Fish Taco 6 hours ago remove link
The PCR test will go down in history as the biggest part of this scamdemic. Covid 19 was a
novel virus resulting in a bad flu that killed the elderly and the already ill.
That will be Covid's legacy...the politicians will be shamed for all eternity.
We have detailed the controversy surrounding America's COVID "casedemic" and the misleading
results of the PCR test and its amplification procedure in great detail over the past few
months.
As a reminder, "cycle thresholds" (Ct) are the level at which widely used polymerase chain
reaction (PCR) test can detect a sample of the COVID-19 virus. The higher the number of cycles,
the lower the amount of viral load in the sample; the lower the cycles, the more prevalent the
virus was in the original sample.
Numerous epidemiological experts have argued that cycle thresholds are an important metric
by which patients, the public, and policymakers can make more informed decisions about how
infectious and/or sick an individual with a positive COVID-19 test might be. However,
as JustTheNews reports, health departments across the country are
failing to collect that data .
Here are a few headlines from those experts and scientific studies:
2. The Wadworth Center, a New York State laboratory, analyzed the results of its July
tests at the request of the NYT: 794 positive tests with a Ct of 40: " With a Ct threshold of
35 , approximately half of these PCR tests would no longer be considered positive ," said the
NYT.
"And about 70% would no longer be considered positive with a Ct of 30! "
4. A new study from the
Infectious Diseases Society of America , found that at 25 cycles of amplification, 70% of
PCR test "positives" are not "cases" since the virus cannot be cultured, it's dead. And by
35: 97% of the positives are non-clinical.
5. PCR is not testing for disease, it's testing for a specific RNA pattern and this is the
key pivot. When you crank it up to 25, 70% of the positive results are not really "positives"
in any clinical sense , since
it cannot make you or anyone else sick
So, in summary, with regard to our current
"casedemic", positive tests as they are counted today do not indicate a "case" of anything.
They indicate that viral RNA was found in a nasal swab. It may be enough to make you sick, but
according to the New York Times and their experts, probably won't. And certainly not sufficient
replication of the virus to make anyone else sick. But you will be sent home for ten days
anyway, even if you never have a sniffle. And this is the number the media breathlessly
reports... and is used to fearmonger mask mandates and lockdowns nationwide...
All of which is background for an intriguing decision made by Florida's Department of Health
(and signed off on by Florida's Republican Governor Ron deSantis).
For the first time in the history of the pandemic, a state will require that all labs in the
state report the critical "cycle threshold" level of every COVID-19 test they perform .
All positive, negative and indeterminate COVID-19 laboratory results must be reported to
FDOH via electronic laboratory reporting or by fax immediately. This includes all COVID-19
test types - polymerase chain reaction (PCR), other RNA, antigen and antibody results.
Cycle threshold (CT) values and their reference ranges , as applicable, must be reported
by laboratories to FDOH via electronic laboratory reporting or by fax immediately.
Full press release below:
3 hours ago
Try this on for size, pulled it from the comments at Naturalnews.com :
I have a PhD in virology and immunology. I'm a clinical lab scientist and have tested 1500
"supposed" positive Covid 19 samples collected here in S. California. When my lab team and I
did the testing through Koch's postulates and observation under a SEM (scanning electron
microscope), we found NO Covid in any of the 1500 samples.
What we found was that all of the 1500 samples were mostly Influenza A and some were
influenza B, but not a single case of Covid, and we did not use the B.S. PCR test.
We then sent the remainder of the samples to Stanford, Cornell, and a few of the University
of California labs and they found the same results as we did, NO COVID. They found influenza A
and B.
All of us then spoke to the CDC and asked for viable samples of COVID, which CDC said they
could not provide as they did not have any samples. We have now come to the firm conclusion
through all our research and lab work, that the COVID 19 was imaginary and fictitious. The flu
was called Covid and most of the 225,000 dead were dead through co-morbidities such as heart
disease, cancer, diabetes, emphysema etc. and they then got the flu which further weakened
their immune system and they died. I have yet to find a single viable sample of Covid 19 to
work with. We at the 7 universities that did the lab tests on these 1500 samples are now suing
the CDC for Covid 19 fraud. the CDC has yet to send us a single viable, isolated and purifed
sample of Covid 19.
If they can't or won't send us a viable sample, I say there is no Covid 19, it is
fictitious. The four research papers that do describe the genomic extracts of the Covid 19
virus never were successful in isolating and purifying the samples. All the four papers written
on Covid 19 only describe small bits of RNA which were only 37 to 40 base pairs long which is
NOT A VIRUS. A viral genome is typically 30,000 to 40,000 base pairs. With as bad as Covid is
supposed to be all over the place, how come no one in any lab world wide has ever isolated and
purified this virus in its entirety? That's because they've never really found the virus, all
they've ever found was small pieces of RNA which were never identified as the virus anyway. So
what we're dealing with is just another flu strain like every year... play_arrow 30
play_arrow
Gunston_Nutbush_Hall 3 hours ago (Edited)
Tks my point exactly in general, setting aside any Trump innuendo but keeping straight up
"scientific method(s)"
And if I were to continue my post it would be similar based upon what you have written
hereto:
Sorry Rick DeSantis, the question I would have been really impressed by you asking is not
the back end falsifiable PCR testing but the front end question I have been asking for 12
months!: please provide me from five different independent laboratories, via independent gold
standard, an empirically isolated, separated, purified, and replicated as sole direct
external biological causation agent, for one or all "COVID19" symptoms to any human being, as
"contagious/pathogenic" "virus."
I would nominate Rick DeSantis for the Nobel Prize on that experiment! ;-)
Sardonicus 3 hours ago
No one is testing for, or counting, financial deaths.
There are way more of those.
sparkadore 2 hours ago
The brainwashing is very real. The MSM simply report the daily memo sent to them by the
spin Doctors in the alphabet agencies. Social media and search engine algorithms have been
adjusted to assist you in RightThink.
That leaves the comment section in zh as the voice in the wilderness.
God help us all.
Bastiat 2 hours ago
Heard from a friend the other day: an elderly health compromised couple both got ill and
went to the doctor to get tested for flu. The doctor tested them for COVID and, surprise,
they both came back "positive." No test for flu. So, 2 new "COVID cases" and perhaps another
"COVID" death. Meanwhile flu deaths have dropped off the chart for the season.
Decimus Lunius Luvenalis 3 hours ago
And this is how the imbecile Biden and his ilk will claim 'victory' over the vid. They
chose 'cases' as the benchmark so they'll simply change how a 'case' is defined all the while
hiding behind the 'science' while never citing the 'science' or explaining why their cherry
picked 'science' is valid.
How interesting that 'science' has now been transformed by those that desire to 'rule'
into religious mystery. It must be believed, never questioned, you are guilty of something
and therefore must self-regulate, but they'll provide absolution.
idontcare 2 hours ago (Edited)
Truth if you consider that only 6% of the 277K+ deaths have been categorized as CV19
deaths without co-morbidities according to the CDC's own data. My # just uses the total # of
"reported deaths" ("w/ CV" not necessarily "from CV") accdg to the CDC.
Patrick Bateman Jr. 1 hour ago
I just divided 260,000 by 350 million. My math might be off. But that 99.999 stretches out
even farther into the 9's if we take out the Covid deaths with co-morbidities and use the
6%.
We are destroying an entire way of life and allowing the media, state, and others to
dictate our behavior in our homes over a stronger variant of the flu that has virtually no
chance of killing us. You can go mad thinking about it too much
ThePub'Lick_Hare 2 hours ago
Time for every state to follow Florida by class action suit. This farce has gone on too
long. Kudos to Florida for taking the initiative. Now at last people can ask relevant
questions and insist on proper protocol. The Portuguese High Court saw false COVID testing
for what it is, the spark and flame of a reign of terror. Time to douse the flames and the
douche-bags inflaming the scam-demic.
Ajax_USB_Port_Repair_Service_ 3 hours ago (Edited)
Lowering the test magnification nation wide would be a brilliant covid rescue plan for
whoever wins the presidency.
daveO 3 hours ago
Whoever wins the presidency is not running this SCAMDEMIC. But, yes, they will do it by
spring.
Ajax_USB_Port_Repair_Service_ 2 hours ago (Edited)
" Whoever wins the presidency " Will get the credit.
Agree, covid hysteria is being controlled by some group more powerful than our
president.
deFLorable hillbilly 2 hours ago (Edited)
Ron DeSantis is the best governor, by far, in any of the 57 states.
He is fearless and pro-American.
PS- I forgot about Noem in SD. It’s a tie. That chick rocks red, white and blue
too.
LiberateUS 2 hours ago (Edited)
#3 .Desantis is extremely knowledgeable about the pcr test, extremely intelligent, and a
person of integrity. C 19 is just another annual flu that affects only already sick or very
elderly people. He knows that, and using CT of 25 or lower will reveal only people who have a
virus load that will cause symptoms and illness. Those are the people that need medical
attention. Everyone has small virus particles in their bloodstream, which are harmless.
Vaccines inject viruses into your bloodstream.
bustdriver 2 hours ago
"Approximately 150,000 people die every day, worldwide. That’s 52 million people
that have died so far this year. Cardiovascular diseases (CVDs) are the number 1 cause of
death globally, taking an estimated 17.9 million lives each year. Close to 800,000 people die
due to suicide every year, which is one person every 40 seconds.
Coronavirus has killed 1.5 million people worldwide so far this year.
Perhaps this can offer a little perspective"
fackbankz 2 hours ago
I bet you'll see a marked decrease in deaths from CVDs in 2020 because a lot of them are
being blamed on Covid-1984.
If you are generally aware, the PCR test is used to amplify small amount of genetic
material so as to recognize patterns of DNA by "cycling." (Also, for RNA virus, the RNA is
converted to DNA in order to be detected, it's just the way the test works) This is how we
have been able to recognize the genomes in Egyptian mummies and Wooly Mammoths. It works
because if you amplify and cycle enough times to "grow" legitimate DNA fragments, you get
something with with a fair amount of specificity. W hat is becoming more and more apparent is
that the PCR test was not designed as a diagnostic tool for infection, and really cannot
function as one without having a huge amount of false positives, period.
When it comes to COVID, the presence of viral particles picked up by the PCR technique
does not and has not been quantitatively linked to an active "symptomatic" infection. It
simply cannot be so, because infection threshold as a result of viral load is different for
each patient. It turns out, if you "cycle" over around 25 times, the false positivity of
COVID infection starts getting very high.
I and others have explained in blogs how people can be exposed to virus, and mount a
simple innate immune response and never know any differently. When you test these people with
very low viral loads, who are not sick, you can find the viral RNA code that is used to
"diagnose" if you cycle enough times. The last I read, Labcorp cycles at least 40 times to
detect viral genome fragments. The PCR test was never intended for diagnosis of infection but
as a qualitative test for presence of parts of a virus genome. I know there has been some
confusion circulating the net about what the inventor Kary Mullis had said about that. But we
walk daily with people who have any number of parts of killer virus or bacterial genomes
which one could pick up with a PCR test if one had the specific test for it. Would we claim
that that individual was an infected patient? No!
So given all that, PeakProsperity's Chris
Martenson explains below , in great details, the answer to the most important question you
should ask if you or a loved one gets a positive PCR test result .
"What's the Cycle Threshold (CT) value for that test?"
Sounds wonky but it's actually really important to understand. A low CT value means someone
is loaded with virus. A high value, oppositely, means less of a viral load.
Beyond a certain level the load is insufficient to either infect someone else or be of any
clinical or epidemiological relevance whatsoever.
The problem? Governments all over the country and world are basing their decisions on CT
values that are very high. Too high.
Jon Rappoport (excellent blog) nails it in some of his recent posts.
.
"July 16, 2020, podcast, 'This Week in Virology': Tony Fauci makes a point of saying the
PCR Covid test is useless and misleading when the test is run at '35 cycles or higher.' A
positive result, indicating infection, cannot be accepted or believed.
"Here, in techno-speak, is an excerpt from Fauci's key quote: ' If you get [perform the
test at] a cycle threshold of 35 or more the chances of it being replication-competent [aka
accurate] are miniscule you almost never can culture virus [detect a true positive result]
from a 37 threshold cycle even 36 '
"Too many cycles, and the test will turn up all sorts of irrelevant material that will be
wrongly interpreted as relevant.
"That's called a false positive.
"What Fauci failed to say on the video is: the FDA, which authorizes the test for public
use, recommends the test should be run up to 40 cycles. Not 35.
"Therefore, all labs in the US that follow the FDA guideline are knowingly or unknowingly
participating in fraud. Fraud on a monstrous level, because millions of Americans are being
told they are infected with the virus on the basis of a false positive result, and
"The total number of Covid cases in America -- which is based on the test -- is a gross
falsity.
"The lockdowns and other restraining measures are based on these fraudulent case
numbers.
play_arrow
GenuineAmerican 3 hours ago
Fauci has lied again the PCR maximum cycle for a accurate test results is 25 NOT 35. PCR
is run, or should be run at 21-25 cycles everything else will give a false positive. Had a
friend in Scottsdale MAYO. I had to go to this god-forsaken place to get him out. They were
running the PCR at 42 cycles to keep him in the hospital because he had very, very good UNION
insurance!! The health industries are all crooks, lying to people to get more money being
paid to the orgainizations by the feds.
BaNNeD oN THe RuN 7 hours ago
IQ tests were always seriously flawed, just like the PCR test
U.S TOTAL DEATHS
2015: 2,602,000
2016: 2,744,248
2017: 2,649,000
2018: 2,839,205
2019: 2,909,000
According to usalivestats(dot)com, there are 2,486,700 so far this year. There could be a lag
in reports, but I doubt enough to fulfill their doomsday claims. The CDC still admits only 6%
of these "COVID" are without 2 or more comorbidities, so that's about 25,000 or so. This is a
mild flu season. Here are the recent flu numbers:
FLU DEATHS 2010's
2010: 36,656
2011: 12,447
2012: 42,570
2013: 37,930
2014: 51,376
2015: 22,705
2016: 38,230
2017: 61,099
2018: 34,157
choctaw charley 5 hours ago remove link
so what's the purpose behind the bogus plandemic. In order to institute a one world
plantation several things have to happen. Foremost is the sense of "nationhood". a nation can
be thought of as modeled on the family unit. We look similar, we share religious beliefs,
economic and political views and we have a common history which we take pride in. We trust
rely on and help another. If you have half a brain you don't need me to describe how all
these are under attack. So how does the plandemic play into this? Yesterday you neighbor was
your neighbor. Today he is behind a mask because the government tells you that he is a threat
to you and your family and you to his! The plandemic was used to to hugely expand the mail-in
ballot fraud further driving in the wedge suspicion. Then there is this: when you get your
covid test there will be a permanent file created with your name on it. It will contain your
genetic code and the test result. this will become the social register that is all over
Europe. Get a traffic ticket; late in making a payment; engage in disapproved political
activity as I am doing at this moment? All these will find their way into your file and will
in the future determine the rate you pay on your home mortgage whether you can be employed in
a government job, what you have to endure to board a commercial aircraft etc. There is also a
great likelihood that contained in the vaccine will be a tracking component. Consider also
population segment most vulnerable to covid: older retired people drawing on an already
bankrupt social security ponzi scheme. Hitler referred to these as "Useless Eaters". He had a
system in place to rid society of these. Later these faciliries were expanded to include the
Jewish population.
flyonmywall 9 hours ago
I've done lots of PCR in my life. If you have to do over 35 cycles to detect or amplify
something, you're probably barking up the wrong tree or there is something wrong with your
assay.
Once you ramp up the cycles to past 35-40 cycles, you're just amplifying non-specific
competing amplification products, of which there are always some.
You could have the best designed primers in the world, there is always some random ****
that happens to get amplified at high cycle counts.
Zero-Hegemon 4 hours ago
False positives are beneficial for obtaining COVID money and creating hysteria.
KimAsa 9 hours ago (Edited)
these psychopaths have redesignated the normal course of annual deaths from heart disease,
and other common ailments that old people die from, to Covid 19, to create the illusion of a
deadly pandemic. they claim to have isolated this virus out of one side of their mouth, out
the the other side they claim it has mutated (how many times?) so can't produce proof that
this virus even exists. and out of their ******* they claim to have developed a vaccine?
this is and always has been about the vaccinating the public for free moral agency
prevention.
Ride_the_kali_yuga 9 hours ago
Covid "tests" are an efficient way to feed the false pandemic narrative with nonsensical
numbers of "contaminations". Masks are a mark of submission.
africoman 9 hours ago
Re-posting someone's comment from this article
Here
If the masks work -- Why the six feet?
If the six feet works -- Why the masks?
If both of the above work -- Why the lockdowns?
If all three of the above work -- Why the vaccine?
If the vaccine is safe -- Why protect it with a no liability clause?
If the vaccine is safe---Why not test it on animals first before using it on
humans?
If SARS-CoV-2 exists -- Why has it never been isolated?
If SARS-CoV-2 has never been isolated -- How can an effective vaccine be
developed?
If the RT-PCR test works -- Why so many false positives?
If Kary Mullis, the inventor of the RT-PCR test who conveniently died in August 2019,
says his test shouldn't be used to diagnose infectious diseases -- Why use it to detect
SARS-CoV-2?
If there is an epidemic---Why so many empty hospitals?
If large numbers of people are dying from SARS-CoV-2---Why so many fake causes of death
on death certificates?
If SARS-CoV-2 exists -- Why give doctors financial incentives to diagnose
SARS-CoV-2?
If the official COVID-19 narrative is defensible -- Why censor people who dispute this
narrative?
by John Wear, (retired) lawyer, accountant, and author.
Excellent points, now let's threw a monkey wrench in it to the Operation Warp Speed
play_arrow
Schooey 6 hours ago
Its all BS
KimAsa 9 hours ago (Edited)
these psychopaths have redesignated the normal course of annual deaths from heart disease,
and other common ailments that old people die from, to Covid 19, to create the illusion of a
deadly pandemic. they claim to have isolated this virus out of one side of their mouth, out
the the other side they claim it has mutated (how many times?) so can't produce proof that
this virus even exists. and out of their ******* they claim to have developed a vaccine?
this is and always has been about the vaccinating the public for free moral agency
prevention.
Ms No 8 hours ago
They actually murdered people with the lockdown too though. Knowingly and
premeditated...certainly some of those were also declared covid.
smacker 8 hours ago
" this is and always has been about the vaccinating the public "
Correct.
That has become clear. What we are only now slowing learning is what the sinister motive
is.
kellys_eye 9 hours ago
Is the test for Covid or Covid-19. Can it tell the difference? The 'normal' flu and
influenza are both corona viruses and this is the 'high season' for such cases in the
Northern hemisphere.
Strangely (or not) the incidence of actual flu and influenza are suspiciously MUCH lower
than they should be.
Ergo - tests that prove 'positive' for Covid are likely either false OR reporting on the
flu/influenza.
The LIES keep mounting and mounting.
Harry Tools 5 hours ago
there is no pandemic
RedNeckMother 3 hours ago
I will add another: FDA: 40 recommendation for testing
And let's not forget the comments by Fauci that if they're testing at 35 they're going to
get a lot of false positives.
There's an attorney in Ohio who has filed a FOI to obtain all the ct levels used by the
labs testing in Ohio. It will be very interesting once that is revealed - I'm sure our
governor already knows the answer. If I recall, the NYT itself did an article on this very
topic awhile back and estimated that 90% of the positive results in CT and NY were bogus. And
going from 40 to 35 I believe reduces positives by 63%.
We're being played.
MoreFreedom 5 hours ago remove link
Dr. Martenson's videos are very good. He's clear.
As for "the science" and scientists, we all make mistakes. If we didn't make mistakes, we
wouldn't have scientists pointing out other scientist's mistakes. But it's not a question of
whose science is correct, it's that science is no excuse for taking away peoples'
liberty.
SRV 7 hours ago
The inventor of the test (Dr Kary Mullis) was very outspoken that it was NOT developed for
human virus confirmation...he died of cancer just weeks before the first Covid cases
(hmmmm).
The test procedure was developed as a screening tool in lab research, and he won a Nobel
Prize for it!
It's in your face proof of the scam we're all being subjected to that almost no one ever
questioned (brilliant move really)... ONE cycle above 35 (each cycle doubles the
amplification) will explode the the false positives.
And... if you have no symptoms you DO NOT have the virus (remember how much play the
"asymptomatic" BS story got early on... another psyop). Notice how none of the athletes never
get sick and are back in two weeks... yet it's never questioned by a soul paid to look the
other way!
smacker 9 hours ago
" What is becoming more and more apparent is that the PCR test was not designed
as a diagnostic tool for infection, and really cannot function as one without having
a huge amount of false positives, period. "
This is not knew and didn't need to become "more and more apparent".
The inventor of the PCR test Kary Mullis is on video record stating it. Sadly his
expert
knowledge has been wilfully ignored by the political elites and countless talking heads
and "experts" because it doesn't suit them and didn't fit their agenda.
It's time to prepare the gallows and stock up with rope.
smacker 7 hours ago remove link
The PCR test is used precisely because it can be manipulated to produce as many "cases" as
wanted.
Just turn the dial up on "amplification cycles" and hey presto, you get as many positives
as you want.
The cases are not genuine cases but simply PCR positive tests, but are reported as "cases"
and then
"infections" by MSM who are "In On It".
The idea is "FEAR Management" which allows draconian CovID rules like lockdowns and tiers
and
social distancing to be introduced which accustoms people to being managed and
controlled.
It then ramps up demand for vaccines which is the ultimate objective. Initially (or soon
after), the
vaccines will contain nano-technology - dust-chips - which will be used for surveillance and
control.
Some say they will also contain ingredients to render people infertile (ie population
control).
We are seeing in plain sight the biggest coup ever against mankind.
It must be stopped.
smacker 7 hours ago remove link
The PCR test is used precisely because it can be manipulated to produce as many "cases" as
wanted.
Just turn the dial up on "amplification cycles" and hey presto, you get as many positives
as you want.
The cases are not genuine cases but simply PCR positive tests, but are reported as "cases"
and then
"infections" by MSM who are "In On It".
The idea is "FEAR Management" which allows draconian CovID rules like lockdowns and tiers
and
social distancing to be introduced which accustoms people to being managed and
controlled.
It then ramps up demand for vaccines which is the ultimate objective. Initially (or soon
after), the
vaccines will contain nano-technology - dust-chips - which will be used for surveillance and
control.
Some say they will also contain ingredients to render people infertile (ie population
control).
We are seeing in plain sight the biggest coup ever against mankind.
By Peter Andrews , Irish science journalist and writer based in London. He has a
background in the life sciences, and graduated from the University of Glasgow with a degree in
genetics A peer review of the paper on which most Covid testing is based has
comprehensively debunked the science behind it, finding major flaws. They conclude it's utterly
unsuitable as a means for diagnosis – and the fall-out is immense.
Last week, I reported on a landmark ruling from
Portugal, where a court had ruled against a governmental health authority that had illegally
confined four people to a hotel this summer. They had done so because one of the people had
tested positive for Covid in a polymerase chain reaction (PCR) test – but the court had
found the test fundamentally flawed and basically inadmissible.
Now the PCR testing supremacy under which we all now live has received another crushing
blow. A peer review from
a group of 22 international experts has found 10 "major flaws" in the main protocol for such
tests. The report systematically dismantles the original study , called the
Corman-Drosten paper, which described a protocol for applying the PCR technique to detecting
Covid.
The Corman-Drosten paper was published on January, 23, 2020, just a day after being
submitted, which would make any peer review process that took place possibly the shortest in
history. What is important about it is that the protocol it describes is used in around 70
percent of Covid kits worldwide. It's cheap, fast – and absolutely useless.
Among the fatal flaws
that totally invalidate the PCR testing protocol are that the test:
is non-specific, due to erroneous primer design
is enormously variable
cannot discriminate between the whole virus and viral fragments
has no positive or negative controls
has no standard operating procedure
does not seem to have been properly peer reviewed
Oh dear. One wonders whether anything at all was correct in the paper. But wait – it
gets worse. As has been noted previously , no
threshold for positivity was ever identified. This is why labs have been running 40 cycles,
almost guaranteeing a large number of false positives – up to 97 percent, according to
some
studies.
The cherry on top, though, is that among the authors of the original paper themselves, at
least four have severe conflicts of interest. Two of them are members of the editorial board of
Eurosurveillance, the sinisterly named journal that published the paper. And at least three of
them are on the payroll of the first companies to perform PCR testing!
The 22 members of the consortium that has challenged this shoddy science
deserve huge credit. The scientists, from Europe, the USA, and Japan, comprise senior molecular
geneticists, biochemists, immunologists, and microbiologists, with many decades of experience
between them.
They have issued a demand to Eurosurveillance to retract the Corman-Drosten paper, writing:
" Considering the scientific and methodological blemishes presented here, we are confident
that the editorial board of Eurosurveillance has no other choice but to retract the
publication. '' Talk about putting the pressure on.
It is difficult to overstate the implications of this revelation. Every single thing about
the Covid orthodoxy relies on 'case numbers', which are largely the results of the now
widespread PCR tests. If their results are essentially meaningless, then everything we are
being told – and ordered to do by increasingly dictatorial governments – is likely
to be incorrect. For instance, one of the authors of the review is Dr Mike Yeadon, who
asserts that, in the
UK, there is no 'second wave' and that the pandemic has been over since June. Having seen the
PCR tests so unambiguously debunked, it is hard to see any evidence to the
contrary.
Why was this paper rushed to publication in January, despite clearly not meeting proper
standards? Why did none of the checks and balances that are meant to prevent bad science
dictating public policy kick into action? And why did it take so long for anyone in the
scientific community to challenge its faulty methodology? These questions lead to dark
ruminations, which I will save for another day.
Even more pressing is the question of what is going to be done about this now. The people
responsible for writing and publishing the paper have to be held accountable. But also, all PCR
testing based on the Corman-Drosten protocol should be stopped with immediate effect. All those
who are so-called current 'Covid cases', diagnosed based on that protocol, should be told they
no longer have to isolate. All present and previous Covid deaths, cases, and 'infection rates'
should be subject to a massive retroactive inquiry. And lockdowns, shutdowns, and other
restrictions should be urgently reviewed and relaxed.
Because this latest blow to PCR testing raises the probability that we are not enduring a
killer virus pandemic, but a false positive pseudo-epidemic. And one on which we are destroying
our economies, wrecking people's livelihoods and causing more deaths than Covid-19 will ever
claim.
Think your friends would be interested? Share this story!
The statements, views and opinions expressed in this column are solely those of the author
and do not necessarily represent those of RT.
-reclusive Israeli billionaire, Vivi Nevo, who sounds from the write-up like a latter
day Jeffrey Epstein replacement figure
-use of covid rt-Pcr tests in US under ulterior motives as a HIPPA dodge to mass-collect
DNA for Big data/Big tracking and other purposes.
The PCR test, DNA harvesting and false positives
The validity of the PCR tests in diagnosing Covid-19 has been the subject of much
scientific discussion with a growing number of medical experts and analysts dismissing
the PCR test as unreliable and inconclusive due to the high percentage of false
positives. It is also claimed that this widespread DNA collection under the pretext of
Covid-19 could be a covert genetic information harvest on the pretext of extracting viral
DNA from all the genetic material.
I spoke with a medical expert who will remain anonymous for security reasons and he
informed me that the PCR test is "not designed to diagnose disease." He told me:
"The test identifies a genetic sequence being present in a sample and then copies
it, thereby increasing the amount of genetic material. Each test cycle copies and
increases the genetic material. A specific amount of GM is required to meet a threshold
of detection. The test will keep copying until it is possible to say the virus is
"detected". Therein lies the problem. After "Covid" infection, when the virus has been
removed by the immune system, some viral genetic debris can remain for many months. A
tiny fragment viral, genetic material debris will be found and multiplied by many, many
cycles until the detection threshold is reached. This is a false positive."
He informed me that most labs are running upwards of 40 cycles. "In at least 4
examples of RT PCR testing in the US, it was found that 90% of the positive tests were
actually false."
He also told me "the real reason they are pushing the testing is control. They want a
rapid test to be used every day, multiple times per day to gain entry to school, work,
restaurants, entertainment centres etc. It is conditioning."
The sinister question is whether all this genetic DNA information is passed on to
undisclosed entities for "research purposes" without the patient's knowledge.
By Peter Andrews , Irish science journalist and writer based in London. He has a
background in life sciences, and graduated from the University of Glasgow with a degree in
genetics. Four German holidaymakers who were illegally quarantined in Portugal after one
was judged to be positive for Covid-19 have won their case, in a verdict that condemns the
widely-used PCR test as being up to 97-percent unreliable.
Earlier this month, Portuguese judges upheld a decision from a lower court that found the
forced quarantine of four holidaymakers to be unlawful. The case centred on the reliability (or
lack thereof) of Covid-19 PCR tests.
The
verdict , delivered on November 11, followed an appeal against a writ of habeas corpus
filed by four Germans against the Azores Regional Health Authority. This body had been
appealing a ruling from a lower court which had found in favour of the tourists, who
claimed that they were illegally confined to a hotel without their consent. The tourists
were ordered to stay in the hotel over the summer after one of them tested positive for
coronavirus in a PCR test - the other three were labelled close contacts and therefore made to
quarantine as well.
Unreliable, with a strong chance of false positives
The deliberation of the Lisbon Appeal Court is comprehensive and fascinating. It ruled that
the Azores Regional Health Authority had violated both Portuguese and international law by
confining the Germans to the hotel. The judges also said that only a doctor can "diagnose"
someone with a disease, and were critical of the fact that they were apparently never assessed
by one.
They were also scathing about the reliability of the PCR (polymerase chain reaction) test,
the most commonly used check for Covid.
The conclusion of their 34-page ruling included the following: "In view of current
scientific evidence, this test shows itself to be unable to determine beyond reasonable doubt
that such positivity corresponds, in fact, to the infection of a person by the SARS-CoV-2
virus."
In the eyes of this court, then, a positive test does not correspond to a Covid case. The
two most important reasons for this, said the judges, are that, "the test's reliability
depends on the number of cycles used'' and that "the test's reliability depends on the
viral load present.'' In other words, there are simply too many unknowns surrounding PCR
testing.
Tested positive? There could be as little as a 3% chance it's correct
This is not the first challenge to the credibility of PCR tests. Many people will be
aware that their results have a lot to do with the number of amplifications that are
performed, or the 'cycle threshold.' This number in most American and European labs is
35–40 cycles, but experts have claimed that even 35
cycles is far too many, and that a more reasonable protocol would call for 25–30 cycles.
(Each cycle exponentially increases the amount of viral DNA in the sample).
Earlier this year, data from three US
states – New York, Nevada and Massachusetts – showed that when the amount of the
virus found in a person was taken into account, up to 90 percent of people who tested positive
could actually have been negative, as they may have been carrying only tiny amounts of the
virus.
The Portuguese judges cited a study conducted by "some of the leading European and world
specialists," which was published by Oxford Academic at the end of September. It showed that
if someone tested positive for Covid at a cycle threshold of 35 or higher, the chances of that
person actually being infected is less than three percent, and that "the probability of
receiving a false positive is 97% or higher."
While the judges in this case admitted that the cycle threshold used in Portuguese labs was
unknown, they took this as further proof that the detention of the tourists was unlawful. The
implication was that the results could not be trusted. Because of this uncertainty, they stated
that there was "no way this court would ever be able to determine" whether the tourist
who tested positive was indeed a carrier of the virus, or whether the others had been exposed
to it.
It is a sad indictment of our mainstream media that such a landmark ruling, of such obvious
and pressing international importance, has been roundly ignored. If one were making (flimsy)
excuses for them, one could say that the case escaped the notice of most science editors
because it has been published in Portuguese. But there is a full
English translation of the appeal, and alternative media managed
to pick it up.
And it isn't as if Portugal is some remote, mysterious nation where news is unreliable or
whose judges are suspect – this is a western EU country with a large population and a
similar legal system to many other parts of Europe. And it is not the only country whose
institutions are clashing with received wisdom on Covid. Finland's national health authority
has
disputed the WHO's recommendation to test as many people as possible for coronavirus,
saying it would be a waste of taxpayer's money, while poorer South East Asian countries are
holding off on ordering
vaccines, citing an improper use of finite resources.
Testing, especially PCR testing, is the basis for the entire house of cards of Covid
restrictions that are wreaking havoc worldwide. From testing comes case numbers. From case
numbers come the 'R number,' the rate at which a carrier infects others. From the 'dreaded' R
number comes the lockdowns and the restrictions, such as England's new and baffling tiered
restrictions that come into force next week.
The daily barrage of statistics is familiar to us all by this point, but as time goes on the
evidence that something may be deeply amiss with the whole foundation of our reaction to this
pandemic – the testing regime – continues to mount
Covid-19 is a dangerous disease and I take precautions to protect myself. However, the
public depiction of the disease in the media and the actions being taken by most
governments cannot but raise some very serious questions.
Posted by: Nathan Mulcahy | Nov 1 2020 18:14 utc | 16
Based on this data, the ECDC should publish a weekly map of EU member states, broken down
by regions, to support member states in their decision-making. Areas should be marked in
the following colours:
green if the 14-day notification rate is lower than 25 and the test positivity rate
below 4%
orange if the 14-day notification rate is lower than 50 but the test positivity
rate is 4% or higher or, if the 14-day notification rate is between 25 and150 and the
test positivity rate is below 4%
red if the 14-day notification rate is 50 or higher and the test positivity rate is
4% or higher or if the 14-day notification rate is higher than 150
grey if there is insufficient information or if the testing rate is lower than
300
You will notice how the measures to be taken by individual countries are absolutely (as
in 100%) dependent on the worst metric possible according to the demonstrated
performance of rtPCR tests. We are being recommended to use the wrong metric! None of us
wishes any of our health systems to collapse, however their occupancy objectively varies
with the cumulative individual immune response of the population NOT with the
precariously measured transmissibility of SARS-CoV-2 via rtPCR tests. Remember that the
only reason we are worried about virus transmissibility is because of eventual severe
developments of the disease in a fraction of the population and a possible breakdown of
health systems as a consequence.
The relevant failure of rtPCR testing is its inability to estimate accurately the viral
load (let's not put in question the assumption that viral load is the most important
criteria for a severe development of C-19, while also leaving aside aggravating
comorbidities). rtPCR testing, under the current state of knowledge, is the equivalent of
measuring a patient's temperature with a thermometer but no doctor knows the average body
temperature, and its natural healthy interval, nor would the thermometer provide a number
on a scale, merely reporting that a patient has something other than "0". This would
constitute a USELESS thermometer.
From the same recommendation as above, quote:
Free movement restrictions
Member states should not restrict the free movement of persons travelling to or from
green areas. [LOL - great opening, they know full well under these criteria there will be
barely any in the next months]
If considering whether to apply restrictions, they should respect the differences in
the epidemiological situation between orange and red areas and act in a proportionate
manner. They should also take into account the epidemiological situation in their own
territory.
Member states should in principle not refuse entry to persons travelling from other
member states. Those member states that consider it necessary to introduce restrictions
could require persons travelling from non-green areas to:
undergo quarantine
undergo a test after arrival
Member states may offer the option of replacing this test with a test carried out
before arrival.
Member states could also require persons entering their territory to submit passenger
locator forms. A common European passenger locator form should be developed for possible
common use.
"Test, test, test" remember? The above simply becomes arbitrary according to the
criteria defined. This is not policy based on solid science! Such arbitrary policies
usually serve unstated purposes (I'll refrain here to expand on those) while throwing some
false pretext to the masses in order to seek their consent, exploiting their limited
ability to validate the pretext as legitimate science.
So then... what could be a valid metric that allows us to prevent "eventual severe
developments of the disease and a possible breakdown of health systems"? This is the
question we should be asking! Myself, I would be satisfied, in substitution of rtPCR
testing, with the use of new Hospitalizations, ICU and even Deaths as much better metrics,
since these are true fractions of the disease development against any population and even
allow to calibrate for its health system performance, much less vulnerable to duplications
and false positive accounting.
rtPCR testing is absolutely absurd for the purposes it is being used (ie. country wide
government response policy), instead of being limited to clinical diagnostic tool of the
individual suspect of some respiratory disease to be used by a qualified practitioner, and,
at best, a screening tool to get a handle on local outbreaks (schools, workplaces,
residences, etc).
Hanging on this fallacy lies the destruction of most western economies and an ominous
verge into the police state, neither are overstatements given what we have seen so far.
Thanks for the link, Jen. But it's not that a PCR test cannot detect a SARS-cov2
virus. The problem is that there is no standardized and validated PCR test for detecting
SARS-Cov2 virus. I believe in Germany alone there are 200+ variations of the test currently
being used.
My concerns about the remaining four points remain.
@ Posted by: Vasco da Gama | Nov 1 2020 23:49 utc | 56
Thanks for adding additional meat to my argument, including the issue with "viral load",
which together with the state of the immune system of the host will decide whether or not
an infected person will get sick. PCR can be extremely sensitive but that's only part of
the picture.
And as I have mentioned in my response to Jen I am yet to find good answers to my
remaining the 4 points in my first post (#16)
Lockdowns and hygienic measures around the world are based on numbers of cases and
mortality rates created by the so-called SARS-CoV-2 RT-PCR tests used to identify "positive"
patients, whereby "positive" is usually equated with "infected."
But looking closely at the facts, the conclusion is that these PCR tests are meaningless
as a diagnostic tool to determine an alleged infection by a supposedly new virus called
SARS-CoV-2.
We have a simple message for all countries: test, test, test."
The message was spread through headlines around the world, for instance by
Reuters and the BBC
.
Still on the 3 of May, the moderator of the Heute j ournal -- one of the most
important news magazines on German television -- was passing the mantra of the corona dogma
on to his audience with the admonishing words:
Test, test, test -- that is the credo at the moment, and it is the only way to really
understand how much the coronavirus is spreading."
This indicates that the belief in the validity of the PCR tests is so strong that it
equals a religion that tolerates virtually no contradiction.
So to start, it is very remarkable that Kary Mullis himself, the inventor of the
Polymerase Chain Reaction (PCR) technology, did not think alike. His invention got him the
Nobel prize in chemistry in 1993.
The reason is that the intended use of the PCR was, and still is, to apply it as a
manufacturing technique, being able to replicate DNA sequences millions and billions of
times, and not as a diagnostic tool to detect viruses.
Moreover, it is worth mentioning that the PCR tests used to identify so-called COVID-19
patients presumably infected by what is called SARS-CoV-2 do not have a valid gold standard
to compare them with.
This is a fundamental point. Tests need to be evaluated to determine their preciseness
-- strictly speaking their "sensitivity"[1] and "specificity" -- by comparison with a "gold
standard," meaning the most accurate method available.
As an example, for a pregnancy test the gold standard would be the pregnancy itself. But
as Australian infectious diseases specialist Sanjaya Senanayake, for example, stated in an
ABC TV interview in an answer to
the question "How accurate is the [COVID-19] testing?" :
If we had a new test for picking up [the bacterium] golden staph in blood, we've already
got blood cultures, that's our gold standard we've been using for decades, and we could
match this new test against that. But for COVID-19 we don't have a gold standard test."
Jessica C. Watson from Bristol University confirms this. In her paper "Interpreting a COVID-19 test
result" , published recently in The British Medical Journal , she writes that
there is a "lack of such a clear-cut 'gold-standard' for COVID-19 testing."
But instead of classifying the tests as unsuitable for SARS-CoV-2 detection and COVID-19
diagnosis, or instead of pointing out that only a virus, proven through isolation and
purification, can be a solid gold standard, Watson claims in all seriousness that,
"pragmatically" COVID-19 diagnosis itself, remarkably including PCR testing itself, "may
be the best available 'gold standard'." But this is not scientifically sound.
Apart from the fact that it is downright absurd to take the PCR test itself as part of the
gold standard to evaluate the PCR test, there are no distinctive specific symptoms for
COVID-19, as even people such as Thomas Löscher, former head of the Department of
Infection and Tropical Medicine at the University of Munich and member of the Federal
Association of German Internists, conceded to us[2].
And if there are no distinctive specific symptoms for COVID-19, COVID-19 diagnosis --
contrary to Watson's statement -- cannot be suitable for serving as a valid gold
standard.
In addition, "experts" such as Watson overlook the fact that only virus isolation, i.e. an
unequivocal virus proof, can be the gold standard.
That is why I asked Watson how COVID-19 diagnosis "may be the best available gold
standard," if there are no distinctive specific symptoms for COVID-19, and also whether the
virus itself, that is virus isolation, wouldn't be the best available/possible gold standard.
But she hasn't answered these questions yet – despite multiple requests. And she has
not yet responded to our rapid response post on her article in which we address exactly the
same points, either, though she wrote us on June 2nd : "I will
try to post a reply later this week when I have a chance."
No proof for the RNA being of viral origin
Now the question is: What is required first for virus isolation/proof? We need to know
where the RNA for which the PCR tests are calibrated comes from.
As textbooks (e.g., White/Fenner. Medical Virology, 1986, p. 9) as well as leading virus
researchers such as Luc
Montagnier or Dominic Dwyer state , particle purification -- i.e. the separation of an
object from everything else that is not that object, as for instance Nobel laureate Marie
Curie purified 100 mg of radium chloride in 1898 by extracting it from tons of pitchblende --
is an essential pre-requisite for proving the existence of a virus, and thus to prove that
the RNA from the particle in question comes from a new virus.
The reason for this is that PCR is extremely sensitive, which means it can detect even
the smallest pieces of DNA or RNA -- but it cannot determine where these particles came from
. That has to be determined beforehand.
And because the PCR tests are calibrated for gene sequences (in this case RNA sequences
because SARS-CoV-2 is believed to be a RNA virus), we have to know that these gene snippets
are part of the looked-for virus. And to know that, correct isolation and purification of the
presumed virus has to be executed.
Hence, we have asked the science teams of the relevant papers which are referred to in the
context of SARS-CoV-2 for proof whether the electron-microscopic shots depicted in their in
vitro experiments show purified viruses.
But not a single team could answer that question with "yes" -- and NB., nobody said
purification was not a necessary step. We only got answers like "No, we did not obtain an
electron micrograph showing the degree of purification" (see below).
We asked several study authors "Do your electron micrographs show the purified virus?",
they gave the following responses:
Study 1: Leo L. M. Poon; Malik Peiris. "Emergence of a novel human coronavirus
threatening human health" Nature Medicine , March 2020
Replying Author: Malik Peiris
Date: May 12, 2020
Answer: "The image is the virus budding from an infected cell. It is not purified
virus."
Study 2: Myung-Guk Han et al. "Identification of Coronavirus Isolated from a Patient in
Korea with COVID-19", Osong Public Health and Research Perspectives , February
2020
Replying Author: Myung-Guk Han
Date: May 6, 2020
Answer: "We could not estimate the degree of purification because we do not purify and
concentrate the virus cultured in cells."
Study 3: Wan Beom Park et al. "Virus Isolation from the First Patient with SARS-CoV-2 in
Korea", Journal of Korean Medical Science , February 24, 2020
Replying Author: Wan Beom Park
Date: March 19, 2020
Answer: "We did not obtain an electron micrograph showing the degree of
purification."
Study 4: Na Zhu et al., "A Novel Coronavirus from Patients with Pneumonia in China",
2019, New England Journal of Medicine , February 20, 2020
Replying Author: Wenjie Tan
Date: March 18, 2020
Answer: "[We show] an image of sedimented virus particles, not purified ones."
Regarding the mentioned papers it is clear that what is shown in the electron micrographs
(EMs) is the end result of the experiment, meaning there is no other result that they could
have made EMs from.
That is to say, if the authors of these studies concede that their published EMs do not
show purified particles, then they definitely do not possess purified particles claimed to be
viral. (In this context, it has to be remarked that some researchers use the term "isolation"
in their papers, but the procedures described therein do not represent a proper isolation
(purification) process. Consequently, in this context the term "isolation" is misused).
Thus, the authors of four of the principal, early 2020 papers claiming discovery of a new
coronavirus concede they had no proof that the origin of the virus genome was viral-like
particles or cellular debris, pure or impure, or particles of any kind. In other words, the
existence of SARS-CoV-2 RNA is based on faith, not fact.
We have also contacted Dr Charles Calisher, who is a seasoned virologist. In 2001,
Science published an "impassioned plea to the younger generation" from several
veteran virologists, among them Calisher, saying that:
[modern virus detection methods like] sleek polymerase chain reaction [ ] tell little
or nothing about how a virus multiplies, which animals carry it, [or] how it makes people
sick. [It is] like trying to say whether somebody has bad breath by looking at his
fingerprint."[3]
And that's why we asked Dr Calisher whether he knows one single paper in which SARS-CoV-2
has been isolated and finally really purified. His answer:
I know of no such a publication. I have kept an eye out for one."[4]
This actually means that one cannot conclude that the RNA gene sequences, which the
scientists took from the tissue samples prepared in the mentioned in vitro trials and for
which the PCR tests are finally being "calibrated," belong to a specific virus -- in this
case SARS-CoV-2.
In addition, there is no scientific proof that those RNA sequences are the causative agent
of what is called COVID-19.
In order to establish a causal connection, one way or the other, i.e. beyond virus
isolation and purification, it would have been absolutely necessary to carry out an
experiment that satisfies the four Koch's postulates. But there is no such experiment, as
Amory Devereux and Rosemary Frei
recently revealed for OffGuardian .
The necessity to fulfill these postulates regarding SARS-CoV-2 is demonstrated not least
by the fact that attempts have been made to fulfill them. But even researchers claiming they
have done it, in reality, did not succeed.
One example is a study published in Nature
on May 7 . This trial, besides other procedures which render the study invalid, did not
meet any of the postulates.
For instance, the alleged "infected" laboratory mice did not show any relevant clinical
symptoms clearly attributable to pneumonia, which according to the third postulate should
actually occur if a dangerous and potentially deadly virus was really at work there. And the
slight bristles and weight loss, which were observed temporarily in the animals are
negligible, not only because they could have been caused by the procedure itself, but also
because the weight went back to normal again.
Also, no animal died except those they killed to perform the autopsies . And let's not
forget: These experiments should have been done before developing a test, which is not
the case.
Revealingly, none of the leading German representatives of the official theory about
SARS-Cov-2/COVID-19 -- the Robert Koch-Institute (RKI), Alexander S. Kekulé
(University of Halle), Hartmut Hengel and Ralf Bartenschlager (German Society for Virology),
the aforementioned Thomas Löscher, Ulrich Dirnagl (Charité Berlin) or Georg
Bornkamm (virologist and professor emeritus at the Helmholtz-Zentrum Munich) -- could answer
the following question I have sent them:
If the particles that are claimed to be to be SARS-CoV-2 have not been purified, how
do you want to be sure that the RNA gene sequences of these particles belong to a specific
new virus?
Particularly, if there are studies showing that substances such as antibiotics that
are added to the test tubes in the in vitro experiments carried out for virus detection can
"stress" the cell culture in a way that new gene sequences are being formed that were
not
previously detectable -- an aspect that Nobel laureate Barbara McClintock already drew
attention to in her Nobel Lecture back in
1983 .
It should not go unmentioned that we finally got the Charité – the employer
of Christian Drosten, Germany's most influential virologist in respect of COVID-19, advisor
to the German government and co-developer of the PCR test which was the first to be
"accepted" (
not validated! ) by the WHO worldwide – to answer questions on the topic.
But we didn't get answers until June 18, 2020, after months of non-response. In the end,
we achieved it only with the help of Berlin lawyer Viviane Fischer.
Regarding our question "Has the Charité convinced itself that appropriate
particle purification was carried out?," the Charité concedes that they didn't use
purified particles.
And although they claim "virologists at the Charité are sure that they are
testing for the virus," in their paper ( Corman et
al. ) they state:
RNA was extracted from clinical samples with the MagNA Pure 96 system (Roche, Penzberg,
Germany) and from cell culture supernatants with the viral RNA mini kit (QIAGEN, Hilden,
Germany),"
Which means they just assumed the RNA was viral .
Incidentally, the Corman et al. paper, published on January 23, 2020 didn't even go
through a proper peer review process , nor were the procedures outlined therein accompanied
by controls -- although it is only through these two things that scientific work becomes
really solid.
Irrational rest results
It is also certain that we cannot know the false positive rate of the PCR tests without
widespread testing of people who certainly do not have the virus, proven by a method which is
independent of the test (having a solid gold standard).
Therefore, it is hardly surprising that there are several papers illustrating irrational
test results.
For example, already in February the health authority in China's Guangdong province
reported that people have fully recovered from illness blamed on COVID-19, started to test
"negative," and then
tested "positive" again .
A month later, a paper published in the Journal of Medical Virology showed that 29 out
of 610 patients at a hospital in Wuhan had 3 to 6 test results that flipped between
"negative", "positive" and
"dubious" .
A third example is a study from Singapore in which tests were carried out almost daily
on 18 patients and the majority went from "positive" to "negative" back to "positive" at
least once, and up to five times in one
patient .
Even Wang Chen, president of the Chinese Academy of Medical Sciences, conceded in February
that the PCR tests are
"only 30 to 50 per cent accurate" ; while Sin Hang Lee from the Milford Molecular
Diagnostics Laboratory sent a l
etter to the WHO's coronavirus response team and to Anthony S. Fauci on March 22, 2020,
saying that:
It has been widely reported in the social media that the RT-qPCR [Reverse
Transcriptase quantitative PCR] test kits used to detect SARSCoV-2 RNA in human specimens
are generating many false positive results and are not sensitive enough to detect some real
positive cases."
In other words, even if we theoretically assume that these PCR tests can really detect a
viral infection, the tests would be practically worthless, and would only cause an unfounded
scare among the "positive" people tested.
This becomes also evident considering the positive predictive value (PPV).
The PPV indicates the probability that a person with a positive test result is truly
"positive" (ie. has the supposed virus), and it depends on two factors: the prevalence of the
virus in the general population and the specificity of the test, that is the percentage of
people without disease in whom the test is correctly "negative" (a test with a specificity of
95% incorrectly gives a positive result in 5 out of 100 non-infected people).
With the same specificity, the higher the prevalence, the higher the PPV.
In this context, on June 12 2020, the journal Deutsches Ärzteblatt published
an article in which the PPV has been calculated with
three different prevalence scenarios .
The results must, of course, be viewed very critically, first because it is not possible
to calculate the specificity without a solid gold standard, as outlined, and second because
the calculations in the article are based on the specificity determined in the study by
Jessica Watson, which is potentially worthless, as also mentioned.
But if you abstract from it, assuming that the underlying specificity of 95% is correct
and that we know the prevalence, even the mainstream medical journal Deutsches
Ärzteblatt reports that the so-called SARS-CoV-2 RT-PCR tests may have "a shockingly
low" PPV.
In one of the three scenarios, figuring with an assumed prevalence of 3%, the PPV was
only 30 percent, which means that 70 percent of the people tested "positive" are not
"positive" at all . Yet "they are prescribed quarantine," as even the Ärzteblatt notes
critically.
In a second scenario of the journal's article, a prevalence of rate of 20 percent is
assumed. In this case they generate a PPV of 78 percent, meaning that 22 percent of the
"positive" tests are false "positives."
That would mean: If we take the around 9 million people who are currently considered
"positive" worldwide -- supposing that the true "positives" really have a viral infection --
we would get almost 2 million false "positives."
All this fits with the fact that the CDC and the FDA, for instance, concede in their files
that the so-called "SARS-CoV-2 RT-PCR tests" are not suitable for SARS-CoV-2 diagnosis.
positive results [ ] do not rule out bacterial infection or co-infection with other
viruses. The agent detected may not be the definite cause of disease."
Remarkably, in the instruction manuals of PCR tests we can also read that they are not
intended as a diagnostic test, as for instance in those by
Altona Diagnostics and Creative Diagnostics[
5 ].
To quote another one, in the product announcement of the LightMix Modular Assays produced
by TIB Molbiol -- which were developed using the Corman et al. protocol -- and
distributed by Roche we can read:
These assays are not intended for use as an aid in the diagnosis of coronavirus
infection"
And:
For research use only. Not for use in diagnostic procedures."
Where is the evidence that the tests can measure the "viral load"?
There is also reason to conclude that the PCR test from Roche and others cannot even
detect the targeted
genes .
Moreover, in the product descriptions of the RT-qPCR tests for
SARS-COV-2 it says they are
"qualitative" tests , contrary to the fact that the "q" in "qPCR" stands for
"quantitative." And if these tests are not "quantitative" tests, they don't show how many
viral particles are in the body .
That is crucial because, in order to even begin talking about actual illness in the real
world not only in a laboratory, the patient would need to have millions and millions of viral
particles actively replicating in their body.
That is to say, the CDC, the WHO, the FDA or the RKI may assert that the tests can measure
the so-called
"viral load," i.e. how many viral particles are in the body. "But this has never been
proven. That is an enormous scandal," as the journalist
Jon Rappoport points out .
This is not only because the term "viral load" is deception. If you put the question "what
is viral load?" at a dinner party, people take it to mean viruses circulating in the
bloodstream. They're surprised to learn it's actually RNA molecules.
Also, to prove beyond any doubt that the PCR can measure how much a person is "burdened"
with a disease-causing virus, the following experiment would have had to be carried out
(which has not yet happened):
You take, let's say, a few hundred or even thousand people and remove tissue samples
from them. Make sure the people who take the samples do not perform the test.The testers will
never know who the patients are and what condition they're in. The testers run their PCR on
the tissue samples. In each case, they say which virus they found and how much of it they
found. Then, for example, in patients 29, 86, 199, 272, and 293 they found a great deal of
what they claim is a virus. Now we un-blind those patients. They should all be sick, because
they have so much virus replicating in their bodies. But are they really sick -- or are they
fit as a fiddle?
With the help of the aforementioned lawyer Viviane Fischer, I finally got the
Charité to also answer the question of whether the test developed by Corman et al. --
the so-called "Drosten PCR
test" -- is a quantitative test.
But the Charité was not willing to answer this question "yes". Instead, the
Charité wrote:
If real-time RT-PCR is involved, to the knowledge of the Charité in most cases
these are [ ] limited to qualitative detection."
Furthermore, the "Drosten PCR test" uses the unspecific E-gene assay as preliminary
assay , while the Institut Pasteur uses the same assay as
confirmatory assay .
According to Corman et al., the E-gene assay is likely to detect all Asian viruses , while
the other assays in both tests are supposed to be more specific for sequences labelled
"SARS-CoV-2".
Besides the questionable purpose of having either a preliminary or a confirmatory test
that is likely to detect all Asian viruses, at the beginning of April the WHO changed the
algorithm, recommending that from then on a test can be regarded as "positive" even if just
the E-gene assay (which is likely to detect all Asian viruses! )
gives a "positive" result .
This means that a confirmed unspecific test result is officially sold as
specific .
That change of algorithm increased the "case" numbers. Tests using the E-gene assay are
produced for example by Roche
,
TIB Molbiol and
R-Biopharm .
High CQ values make the test results even more meaningless
Another essential problem is that many PCR tests have a "cycle quantification" (Cq) value
of over 35, and some, including the "Drosten PCR test", even have a Cq of 45.
The Cq value specifies how many cycles of DNA replication are required to detect a real
signal from biological samples.
"Cq values higher than 40 are suspect because of the implied low efficiency and
generally should not be reported," as it says in the MIQE guidelines
.
MIQE stands for "Minimum Information for Publication of Quantitative Real-Time PCR
Experiments", a set of guidelines that describe the minimum information necessary for
evaluating publications on Real-Time PCR, also called quantitative PCR, or qPCR.
If you have to go more than 40 cycles to amplify a single-copy gene, there is something
seriously wrong with your PCR."
The MIQE guidelines have been developed under the aegis of Stephen A. Bustin , Professor of Molecular
Medicine, a world-renowned expert on quantitative PCR and author of the book A-Z of
Quantitative PCR which has been called "the bible of qPCR."
In a recent podcast interview Bustin points out that "the use of such arbitrary Cq
cut-offs is not ideal, because they may be either too low (eliminating valid results) or too
high (increasing false "positive" results)."
And, according to him, a Cq of 20 to 30 should be aimed at, and there is concern regarding
the reliability of the results for any Cq over 35.
If the Cq value gets too high, it becomes difficult to distinguish real signal from
background, for example due to reactions of primers and fluorescent probes, and hence there
is a higher probability of false positives.
Moreover, among other factors that can alter the result, before starting with the actual
PCR, in case you are looking for presumed RNA viruses such as SARS-CoV-2, the RNA must be
converted to complementary DNA (cDNA) with the enzyme Reverse Transcriptase -- hence the "RT"
at the beginning of "PCR" or "qPCR."
But this transformation process is "widely recognized as inefficient and variable,"
as Jessica Schwaber from the Centre for Commercialization of Regenerative Medicine in Toronto
and two research colleagues pointed out in a 2019
paper .
Stephen A. Bustin acknowledges problems with PCR in a comparable way.
For example, he pointed to the problem that in the course of the conversion process (RNA
to cDNA) the amount of DNA obtained with the same RNA base material can vary widely, even by
a factor of 10 (see above interview).
Considering that the DNA sequences get doubled at every cycle, even a slight variation
becomes magnified and can thus alter the result, annihilating the test's reliable informative
value.
So how can it be that those who claim the PCR tests are highly meaningful for so-called
COVID-19 diagnosis blind out the fundamental inadequacies of these tests -- even if they are
confronted with questions regarding their validity?
Certainly, the apologists of the novel coronavirus hypothesis should have dealt with these
questions before throwing the tests on the market and putting basically the whole world under
lockdown, not least because these are questions that come to mind immediately for anyone with
even a spark of scientific understanding.
Thus, the thought inevitably emerges that financial and political interests play a
decisive role for this ignorance about scientific obligations. NB, the WHO, for example has
financial ties with drug companies, as the British Medical Journal
showed in 2010 .
And
experts criticize"that the notorious corruption and conflicts of interest at WHO have
continued, even grown" since then. The CDC as well, to take another big player, is
obviously no better
off .
Finally, the reasons and possible motives remain speculative, and many involved surely act
in good faith; but the science is clear: The numbers generated by these RT-PCR tests do not
in the least justify frightening people who have been tested "positive" and imposing lockdown
measures that plunge countless people into poverty and despair or even drive them to
suicide.
And a "positive" result may have serious consequences for the patients as well, because
then all non-viral factors are excluded from the diagnosis and the patients are treated with
highly toxic drugs and invasive intubations. Especially for elderly people and patients with
pre-existing conditions such a treatment can be fatal, as we have outlined in the article
"Fatal
Therapie."
Without doubt eventual excess mortality rates are caused by the therapy and by the
lockdown measures, while the "COVID-19" death statistics comprise also patients who died of a
variety of diseases, redefined as COVID-19 only because of a "positive" test result whose
value could not be more doubtful.
Addendum: We thank Eleni Papadopulos-Eleopulos and Val Turner in particular who made
valuable contributions to the realization of this article.
*
Note to readers: please click the share buttons above or below. Forward this article to
your email lists. Crosspost on your blog site, internet forums. etc.
Torsten Engelbrecht is an award-winning journalist and author from Hamburg, Germany. In
2006 he co-authored Virus-Mania with Dr Klaus Kohnlein, and in 2009 he won the German Alternate
Media Award . He has also written for Rubikon, Süddeutsche Zeitung, Financial Times
Deutschland and many others.
Konstantin Demeter is a freelance photographer and an independent researcher. Together
with the journalist Torsten Engelbrecht he has published articles on the "COVID-19" crisis in
the online magazine Rubikon, as well as contributions on the monetary system, geopolitics,
and the media in Swiss Italian newspapers.
Belgian daily newspaper Het Laatste Nieuws examined the tests carried out by AZ Delta, one
of the largest labs in the country, and made a stunning discovery. Almost half of all positive
cases reported throughout June, July and August were actually people with an old infection.
The problem, it turns out, lies in the PCR Covid-19 tests. The paper reports that scientific
data reveals virus particles can be detected up to 83 days after the actual infection. This led
to instances where people were no longer contagious, but were still registered as positive
cases. According to HLN, all of these people had to be quarantined.
Belgian experts sounded the alarm in mid-July, when coronavirus numbers spiked after a
relief in June, and even insisted that the second wave had already begun for the country.
"We may have had to deal with old infections largely in the summer months," the lab's
clinical biologist Frederik Van Hoecke told the paper.
S EVIDENCE MOUNTS THAT THE "GOLD STANDARD" TEST FOR DETECTING COVID-19 IS UNRELIABLE, WHY ARE HEALTH OFFICIALS AROUND THE WORLD
CALLING FOR MORE TESTS?
In the months since the COVID-19 panic began health authorities around the world have told the public to "get tested" to help
track the spread of SARS-CoV-2. However, as fear and hysteria subside, the scientific community and public at large are calling into
question the efficacy of the test used to determine a patients status. This article is a brief examination of the evidence that the
PCR test is unreliable and should not be used as a determinant for the number of COVID-19 cases or as a factor in political decisions.
HOUSTON HEALTH AUTHORITY HAS CONCERNS ABOUT PCR TEST
On August 31, I attended a press conference in Houston to
ask the Mayor and Houston Health Authority about reports regarding problems with the Texas Department of State Health Services'
numbers on COVID-19 cases. TLAV has
previously
reported on these concerns with the COVID-19 case numbers in Texas. I also had a chance to ask Houston Health Authority Dr. David
Persse about concerns around the test used to detect COVID-19.
The most common test is a polymerase chain reaction (PCR) lab test. This incredibly sensitive technique was developed by Berkeley
scientist Kary Mullis, for which he was awarded the Nobel Prize in 1993. The test is designed to detect the presence of a virus by
amplifying the virus' genetic material so it can be detected by scientists. The test is viewed as the gold standard, however, it
is not without problems.
The PCR test uses chemicals to amplify the virus's genetic material and then each sample goes through a number of cycles until
a virus is recovered. This "cycle threshold" has become a key component in the debate around the efficacy of the PCR test.
Dr. Persse says that when the labs report numbers of COVID-19 cases to the City of Houston they only offer a binary option of
"yes" for positive or "no" for negative. "But, in reality, it comes in what is called cycle-thresholds. It's an inverse relationship,
so the higher the number the less virus there was in the initial sample," Persse explained. "Some labs will report out to
40 cycle-thresholds, and if they get a positive at 40 – which means there is a tiny, tiny, tiny amount of virus there – that gets
reported to us as positive and we don't know any different."
Persse noted that the key question is, at what value is someone considered still infectious?
"Because if you test me and I have a tiny amount of virus, does that mean I am contagious? that I am still infectious to someone
else? If you are shedding a little bit of virus are you just starting? or are you on the downside?," Dr. Persse asked in the lobby
of Houston City Hall. He believes the answer is for the scientific community to set a national standard for cycle-threshold.
Unfortunately, a national standard would not solve the problems expressed by Dr. Persse and others.
UK PARLIAMENT AND SCIENTISTS HAVE CONCERNS ABOUT PCR TEST
In the first weeks of September a number of important revelations regarding the PCR test have come to light. First, new research
from the University of Oxford's Center for Evidence-Based Medicine and the University of the West of England found that the PCR test
poses the potential for false positives when testing for COVID-19. Professor Carl Heneghan, one of the authors of the study,
Viral cultures for COVID-19 infectivity
assessment – a systematic review , said there was a risk that an increase in testing in the UK will lead to an increase in the
risk of "sample contamination" and thus an increase in COVID-19 cases.
The team reviewed evidence from 25 studies where virus specimens had positive PCR tests. The researchers state that the "genetic
photocopying" technique scientists use to magnify the sample of genetic material collected is so sensitive it could be picking up
fragments of dead virus from previous infections. The researchers reach a similar conclusion as Dr. David Persse, namely that,
"A binary Yes/No approach to the interpretation RT-PCR unvalidated against viral culture will result in false positives with segregation
of large numbers of people who are no longer infectious and hence not a threat to public health."
Heneghan, who is also the the editor of BMJ Evidence-Based Medicine,told the BBC that the binary approach is a problem and tests
should have a cut-off point so small amounts of virus do not lead to a positive result. This is because of the cycle threshold mentioned
by Dr. Persse. A person who is shedding an active virus and someone who has leftover infection could both receive the same positive
test result. He also stated that the test could be detecting old virus which would explain the rise in cases in the UK. Heneghan
also stated that setting a standard for the cycle threshold would eliminate the quarantining and contact tracing of people who are
healthy and help the public better understand the true nature of COVID-19.
The UK's leading health agency, Public Health England, released an update on the testing methods used to detect COVID-19 and appeared
to agree with Professor Heneghan regarding
the concerns on the cycle threshold. On September 9, PHE
released an update which concluded, "all laboratories should determine the threshold for a positive result at the limit of
detection."
This is not the first time Heneghan's work has directly impacted the UK's COVID-19 policies. In July, UK health secretary Matt
Hancock called for an "urgent review" of the daily COVID-19 death
numbers produced by Public Health England after it was revealed the stats included people who died from other causes.
The Guardian reported:
Their analysis suggests PHE cross-checks the latest notifications of deaths against a database of positive test results
– so that anyone who has ever tested positive is recorded in the COVID-19 death statistics.
A Department of Health and Social Care source said: 'You could have been tested positive in February, have no symptoms,
then hit by a bus in July and you'd be recorded as a COVID death.'"
On September 8, Heneghan tweeted out another
study on the limitations of the PCR test. The study,
"SARS-CoV-2 Testing: The Limit of Detection Matters"
, examines the limit of detection (LoD) for RNA. The researchers note similar problems with the PCR test and the cycle threshold,
concluding, "the ultimate lesson from these studies bears repetition: LoD matters and directly impacts efforts to identify, control,
and contain outbreaks during this pandemic."
Heneghan also recently told the BMJ , "one issue
in trying to interpret numbers of detected cases is that there is no set definition of a case. At the moment it seems that a polymerase
chain reaction (PCR) positive result is the only criterion required for a case to be recognised."
"In any other disease we would have a clearly defined specification that would usually involve signs, symptoms, and a test
result," Heneghan explained. "We are moving into a biotech world where the norms of clinical reasoning are going out of the
window. A PCR test does not equal covid-19; it should not, but in some definitions it does."
Heneghan says he is concerned that as soon as there is the appearance of an outbreak there is panic and over-reacting. "This
is a huge problem because politicians are operating in a non-evidence-based way when it comes to non-drug interventions," he
stated.
THE EVIDENCE FOR FALSE POSITIVES IS OVERWHELMING
A recent
report from NPR outlines the dangers of false positives with the PCR tests. Andrew Cohen, director of the Center for Research
on Aquatic Bioinvasions, was hired by the state of California to study an invasion of non-native mussels. The researchers took water
samples and used a PCR test to search for genetic material from the mussels. After the tests came back overwhelmingly positive, Cohen
grew suspicious.
"I began to realize that many of these -- if not all of these -- were false positives, especially when they started being reported
in waters that had chemistry that would not allow the mussels to reproduce and establish themselves," he told NPR. NPR notes
that, depending on the lab, there was a 2 to 8 percent false positive rate.
Once COVID-19 was declared a pandemic, Cohen said he began asking if the reports of people with absolutely no symptoms and positive
PCR test results could be false positives. "I began wondering whether these asymptomatic carriers weren't in large part or in
whole part the human counterparts of those false-positive results of quagga and zebra mussels in all those water bodies across the
West," he said.
Cohen emphasized the importance of researchers taking potential false positive PCR results seriously. "As near as we can tell,
the medical establishment and public health authorities and researchers appear to be assuming that the false-positive rate in in
the PCR based test is zero, or at least so low that we can ignore it."
Cohen is correct that the scientific authorities need to take false positives seriously, especially when a person can be sent
to isolate or quarantine for weeks due to a positive test result. Even the
U.S. FDA's own fact sheet on testing acknowledges the
dangers posed by false positives:
"The CDC 2019-nCoV Real-Time RT-PCR Diagnostic Panel has been designed to minimize the likelihood of false positive test
results. However, in the event of a false positive result, risks to patients could include the following: a recommendation for
isolation of the patient, monitoring of household or other close contacts for symptoms, patient isolation that might limit contact
with family or friends and may increase contact with other potentially COVID-19 patients, limits in the ability to work, the delayed
diagnosis and treatment for the true infection causing the symptoms, unnecessary prescription of a treatment or therapy, or other
unintended adverse effects."
Professor Heneghan believes the confusion around COVID-19 has come as a result of a shift away from "evidence-based medicine."
In a recent opinion piece
published at
The Spectator , Heneghan and Tom Jefferson, a senior associate tutor and honorary research fellow at the Centre for Evidence-Based
Medicine, University of Oxford, wrote that patients have become a "prisoner of a system labelling him or her as 'positive' when we
are not sure what that label means." The two scientists offer this conclusion and warning:
Governments are producing a series of contradictory and confusing policies which have a brief shelf life as the next crisis
emerges. It is increasingly clear the evidence is often ignored. Keeping up to date is a full time occupation, and the advances
of the last 30 years have at best been put on hold.
The duties of a
good doctor
include working in partnership with patients to inform them about what they want or need in a way they can understand, and respecting
their rights to reach decisions with you about their treatment and care. Questions need to be asked as to how this will occur
if you don't see your doctor, particularly if all you have to do is queue in at a drive in to get your answer.
And ultimately what is a 'good test'? We think it's the test which helps your doctor narrow the uncertainty around the origins
and management of your problem.
In the past, our reports raising questions about the accuracy of COVID-19 tests have been met with accusations of 'fearmongering'
and spreading 'misinformation'.
In the past, our reports raising questions about the accuracy of COVID-19 tests have been met with accusations of 'fearmongering'
and spreading 'misinformation'.
Any test with a cycle threshold above 35 is too sensitive, agreed Juliet Morrison, a virologist at the University of California,
Riverside. "I'm shocked that people would think that 40 could represent a positive," she said.
In Massachusetts, from 85 to 90 percent of people who tested positive in July with a cycle threshold of 40 would have been deemed
negative if the threshold were 30 cycles, Dr. Mina said. "I would say that none of those people should be contact-traced, not one,"
he said.
Notable quotes:
"... PCR tests still have a role, he and other experts said. For example, their sensitivity is an asset when identifying newly infected people to enroll in clinical trials of drugs. ..."
The usual diagnostic tests may simply be too sensitive and too slow to contain the spread of the virus.
Tests authorized by the F.D.A. provide only a yes-no answer to infection, and will identify as positive patients with low
amounts of virus in their bodies. Credit... Johnny Milano for The New York Times
Some of the nation's leading public health experts are raising a new concern in the endless debate over
coronavirus testing in
the United States: The standard tests are diagnosing huge numbers of people who may be carrying relatively insignificant amounts
of the virus.
Most of these people are not likely to be contagious, and identifying them may contribute to bottlenecks that prevent those who
are contagious from being found in time. But researchers say the solution is not to test less, or to skip testing people without
symptoms, as recently suggested
by the Centers for Disease Control and Prevention .
"The decision not to test asymptomatic people is just really backward," said Dr. Michael Mina, an epidemiologist at the Harvard
T.H. Chan School of Public Health, referring to the C.D.C. recommendation.
"In fact, we should be ramping up testing of all different people," he said, "but we have to do it through whole different mechanisms."
In what may be a step in this direction, the Trump administration announced on Thursday that it would purchase 150 million rapid
tests.
The most widely used diagnostic test for the new coronavirus, called a PCR test, provides a simple yes-no answer to the question
of whether a patient is infected.
But similar PCR tests for other viruses do offer some sense of how contagious an infected patient may be: The results may include
a rough estimate of the amount of virus in the patient's body.
"We've been using one type of data for everything, and that is just plus or minus -- that's all," Dr. Mina said. "We're using
that for clinical diagnostics, for public health, for policy decision-making."
But yes-no isn't good enough, he added. It's the amount of virus that should dictate the infected patient's next steps. "It's
really irresponsible, I think, to forgo the recognition that this is a quantitative issue," Dr. Mina said.
The PCR test amplifies genetic matter from the virus in cycles; the fewer cycles required, the greater the amount of virus, or
viral load, in the sample. The greater the viral load, the more likely the patient is to be contagious.
This number of amplification cycles needed to find the virus, called the cycle threshold, is never included in the results sent
to doctors and coronavirus patients, although it could tell them how infectious the patients are.
In three sets of testing data that include cycle thresholds, compiled by officials in Massachusetts, New York and Nevada, up to
90 percent of people testing positive carried barely any virus, a review by The Times found.
On Thursday, the United States recorded 45,604 new coronavirus cases, according to a database maintained by The Times. If the
rates of contagiousness in Massachusetts and New York were to apply nationwide, then perhaps only 4,500 of those people may actually
need to isolate and submit to contact tracing.
One solution would be to adjust the cycle threshold used now to decide that a patient is infected. Most tests set the limit at
40, a few at 37. This means that you are positive for the coronavirus if the test process required up to 40 cycles, or 37, to detect
the virus.
Tests with thresholds so high may detect not just live virus but also genetic fragments, leftovers from infection that pose no
particular risk -- akin to finding a hair in a room long after a person has left, Dr. Mina said.
Any test with a cycle threshold above 35 is too sensitive, agreed Juliet Morrison, a virologist at the University of California,
Riverside. "I'm shocked that people would think that 40 could represent a positive," she said.
A more reasonable cutoff would be 30 to 35, she added. Dr. Mina said he would set the figure at 30, or even less. Those changes
would mean the amount of genetic material in a patient's sample would have to be 100-fold to 1,000-fold that of the current standard
for the test to return a positive result -- at least, one worth acting on.
Image
"It's just kind of mind-blowing to me that people are not recording the C.T. values from all these tests, that they're just
returning a positive or a negative," one virologist said. Credit... Erin Schaff/The New York Times
The Food and Drug Administration said in an emailed statement that it does not specify the cycle threshold ranges used to determine
who is positive, and that " commercial manufacturers and
laboratories set their own."
The Centers for Disease Control and Prevention said it is examining the use of cycle threshold measures "for policy decisions."
The agency said it would need to collaborate with the F.D.A. and with device manufacturers to ensure the measures "can be used properly
and with assurance that we know what they mean."
The C.D.C.'s own calculations suggest that it is extremely difficult to detect any live virus in a sample
above a threshold of 33 cycles
. Officials at some state labs said the C.D.C. had not asked them to note threshold values or to share them with contact-tracing
organizations.
For example, North Carolina's state lab uses the Thermo Fisher coronavirus test, which automatically classifies results based
on a cutoff of 37 cycles. A spokeswoman for the lab said testers did not have access to the precise numbers.
This amounts to an enormous missed opportunity to learn more about the disease, some experts said.
"It's just kind of mind-blowing to me that people are not recording the C.T. values from all these tests -- that they're just
returning a positive or a negative," said Angela Rasmussen, a virologist at Columbia University in New York.
"It would be useful information to know if somebody's positive, whether they have a high viral load or a low viral load," she
added.
Officials at the Wadsworth Center, New York's state lab, have access to C.T. values from tests they have processed, and analyzed
their numbers at The Times's request. In July, the lab identified 872 positive tests, based on a threshold of 40 cycles.
With a cutoff of 35, about 43 percent of those tests would no longer qualify as positive. About 63 percent would no longer be
judged positive if the cycles were limited to 30.
In Massachusetts, from 85 to 90 percent of people who tested positive in July with a cycle threshold of 40 would have been deemed
negative if the threshold were 30 cycles, Dr. Mina said. "I would say that none of those people should be contact-traced, not one,"
he said.
Other experts informed of these numbers were stunned.
"I'm really shocked that it could be that high -- the proportion of people with high C.T. value results," said Dr. Ashish Jha,
director of the Harvard Global Health Institute. "Boy, does it really change the way we need to be thinking about testing."
Dr. Jha said he had thought of the PCR test as a problem because it cannot scale to the volume, frequency or speed of tests needed.
"But what I am realizing is that a really substantial part of the problem is that we're not even testing the people who we need to
be testing," he said.
The number of people with positive results who aren't infectious is particularly concerning, said Scott Becker, executive director
of the Association of Public Health Laboratories. "That worries me a lot, just because it's so high," he said, adding that the organization
intended to meet with Dr. Mina to discuss the issue.
The F.D.A. noted that people may have a low viral load when they are newly infected. A test with less sensitivity would miss these
infections.
But that problem is easily solved, Dr. Mina said: "Test them again, six hours later or 15 hours later or whatever," he said. A
rapid test would find these patients quickly, even if it were less sensitive, because their viral loads would quickly rise.
PCR tests still have a role, he and other experts said. For example, their sensitivity is an asset when identifying newly infected
people to enroll in clinical trials of drugs.
But with 20 percent or more of people testing positive for the virus in some parts of the country, Dr. Mina and other researchers
are questioning the use of PCR tests as a frontline diagnostic tool.
People infected with the virus are most infectious from a day or two before symptoms appear till about five days after. But at
the current testing rates, "you're not going to be doing it frequently enough to have any chance of really capturing somebody in
that window," Dr. Mina added.
Highly sensitive PCR tests seemed like the best option for tracking the coronavirus at the start of the pandemic. But for the
outbreaks raging now, he said, what's needed are coronavirus tests that are fast, cheap and abundant enough to frequently test everyone
who needs it -- even if the tests are less sensitive.
"It might not catch every last one of the transmitting people, but it sure will catch the most transmissible people, including
the superspreaders," Dr. Mina said. "That alone would drive epidemics practically to zero."
An earlier version of this article, using information provided by a laboratory spokesman, misstated the number of positive coronavirus
tests in July processed by Wadsworth Center, New York's state lab. It was 872 tests, not 794. Based on that error, the article also
misstated the number of tests that would no longer qualify as positive with a C.T. value of 35 cycles. It is about 43 percent of
the tests, not about half of them. Similarly, the article misstated the number of tests that would no longer qualify as positive
if cycles were limited to 30. It is about 63 percent of the tests, not about 70 percent.
Apoorva Mandavilli is a reporter for The Times, focusing on science and global health. She is the 2019 winner of the Victor Cohn
Prize for Excellence in Medical Science Reporting. @ apoorva_nyc A
version of this article appears in print on Aug. 30, 2020 , Section A, Page 6 of the New York edition with the headline: You're Positive.
But Are You Contagious? Tests May Be Too Sensitive, Experts Say . Order Reprints
| Today's Paper |
Subscribe
PCR stands for polymerase chain
reaction , a molecular biology technique for amplifying segments of DNA, by generating
multiple copies using DNA polymerase enzymes under controlled conditions. As little as a single
copy of a DNA segment or gene can be cloned into millions of copies, allowing detection using
dyes and other visualization techniques.
Developed in 1983, the process of PCR has made it possible to perform DNA sequencing and identify
the order of nucleotides in individual genes. The method uses thermal cycling or the repeated
heating and cooling of the reaction for DNA melting and replication. As PCR continues, the
"new" DNA is used as a template for replication and a chain reaction ensues, exponentially
amplifying the DNA template.
PCR techniques are applied in many areas of biotechnology including protein engineering , cloning,
forensics (DNA fingerprinting), paternity testing, the diagnosis of hereditary and/or
infectious diseases, and for the analysis
of environmental samples.
In forensics, in particular, PCR is especially useful because it amplifies even the smallest
amount of DNA evidence. PCR can also be used to analyze DNA that is thousands of years old, and
these techniques have been used to identify everything from an 800,000-year-old mammoth to
mummies from around the world.
PCR ProcedureInitialization
This step is necessary only for DNA polymerases that require hot-start PCR. The reaction is
heated to between 94 and 96 °C and held for 1-9 minutes.
Denaturation
If the procedure does not require initialization, denaturation is the first step. The
reaction is heated to 94-98 °C for 20-30 seconds. The DNA template's hydrogen bonds are
disrupted and single-stranded DNA molecules are created.
Annealing
The reaction temperature is lower to between 50 and 65 °C and held for 20-40 seconds.
The primers anneal to the single-stranded DNA template. The temperature is extremely important
during this step. If it's too hot, the primer might not bind. If it's too cold, the primer
might bind imperfectly. A good bond is formed when the primer sequence closely matches the
template sequence.
Extension/Elongation
The temperature during this step varies depending upon the type of polymerase. The DNA
polymerase synthesizes a completely new DNA strand.
Final Elongation
This step is performed at 70-74 °C for 5-15 minutes after the final PCR
cycle.
Final Hold
This step is optional. The temperature is kept at 4-15 °C and strops the
reaction.
Three Stages of the PCR ProcedureExponential Amplification
During every cycle, product (the specific piece of DNA that is being replicated) is
doubled.
Leveling-off Stage
As the DNA polymerase loses activity and consumes reagents, the reaction
slows.
From comments: "Article is poorly written by someone who does not know medical science. There
are no viral "cells" so the headline is a put off right away. The comment about "sensitivity" is
misplaced as PCR tests are too sensitive: ergo false positives. I believe "specificity" is the
word the author was searching for. If a test lumps true positives with false positives, then it
lacks specificity."
That's because new research from the University of Oxford's Center for Evidence-Based
Medicine and the University of the West of England has found that the swab-based technique used
for most COVID-19 testing is at risk of returning "false positives" since copies of the virus's
RNA detected by the tests might simply be dead, inactive material from a weeks-old infection.
Although patients infected with COVID-19 are typically only infectious for a week or less,
tests can be triggered by virus genetic material left over from a weeks-old infection.
The team's research involved analyzing 25 studies on the widely used polymerase chain
reaction test. PCR tests use material collected with a swab - the most common type of test
around the world, and especially in the US - then utilize a "genetic photocopying" technique
that allows scientists to magnify the small sample of genetic material collected, which they
can then analyze for signs of viral RNA.
What the researchers here have effectively found is that these PCR tests just aren't
sensitive enough to distinguish if the viral material is active and infectious, or dead and
inert.
For those who desire a more comprehensive understanding of how these tests work, the chart
below can be helpful.
Professor Carl Heneghan, one of the authors of the study, said there was a risk that a surge
in testing across the UK was increasing the risk of this sample contamination occurring and it
may explain why the number of Covid-19 cases is rising but the number of deaths is static.
"Evidence is mounting that a good proportion of 'new' mild cases and people re-testing
positives after quarantine or discharge from hospital are not infectious, but are simply
clearing harmless virus particles which their immune system has efficiently dealt with," he
told the Spectator.
Professor Heneghan added that international scrutiny might be required to avoid "the dangers
of isolating non-infectious people or whole communities." ZKnight 14 minutes ago
Fake science. How about purify the virus first and establish a gold standard for testing
first. No, of course not because the CDC has a patent for Covid-19 and nobody is allowed to try
find it to see if it exists. play_arrow LogicFusion 27 minutes ago
Everybody is a Covid-19 / Coronavirus expert now!
Read about the failed coin dealer and convicted felon's performance. It's hilarious!
Covid -19 has been so politicized that I don't believe a word of any publication for or
against testing, existence of the Virus, or anything that provokes testing or issues opinions
about locking down communities. Just like the riots, Covid news is just plain boring.
play_arrow ominous 3 hours ago
"Give me control of a nation's money, and I care not who makes the laws" - Mayer Amschel
Rothschild. play_arrow play_arrow tangent 4 hours ago remove link
People who recommend a vaccine for an entirely cured virus should lose their license to
practice medicine. 99.9% cure rate applying to people who take it before being hospitalized is
one of the biggest success stories in the history of medicine for HCQ. Not only that, but there
are multiple other likely cures that simply have not been studied well. You'd think people
would appreciate the fact that the common cold has been cured, but instead they just whine that
big pharma isn't getting those bucko bucks.
I honestly expected a ticker tape parade like in the movies when that first cure study came
out. But instead they took a massive **** on the study and on the doctor... ****ty world we
live in. ay_arrow Pair Of Dimes Shift 2 hours ago
An exec (55+) at my company is gung ho about the vaccine.
Unfortunately, I just had to give him a "wait and see" response although I know vaccines for
coronaviruses are impossible. play_arrow 2 play_arrow ThanksIwillHaveAnother 4 hours ago
(Edited)
Viruses are not full cells. They are DNA/RNA wrapped with a protein the clings to a cell
then the cell imports the DNA/RNA to start making its proteins. So what is inactive? If that
person sneezes on another person depending on immune system status that other person could get
a bad infection. y_arrow 4 CrabbyR 3 hours ago
viruses utilizes CELL structures and host DNA to replicate dna or rna according to the
viruses genetic code, the protein jacket is the final product to
disguise the virus from detection and to bind on another cell after the compromised cell
RUPTURES, there's more to it but if it cannot copy itself effectively it can become nonviable
and unable to infect another cell. It replicates DNA inside a host cell, It is not a complete
organism and cannot replicate unless it can inject its DNA into a host cell. Antibodies cling
to viruses and destroy this ability to bind to a target cell. A non viable virus has a damaged
coat or DNA RNA that has to many Dimers (damage or code breaks) Bacteria is more in line with
what you think a virus is y_arrow onewayticket2 4 hours ago (Edited) remove link
they lost me when they changed the definition of "death" to include "presumed, untested"
cases (while bI@#$% ing at me that we needed to "follow the science")....and even got busted
for the laughable motorcycle accident being classified as a covid death and the Labs that were
sending in 100% positive results. (until they were caught) play_arrow OutaTime43 4 hours ago
remove link
The test detects RNA. Not necessarily viable virus. Also, it will detect RNA presence in an
individual who may already have antibodies and may be immune. We are bombarded daily by viruses
of which we already have immunity. play_arrow sun tzu 10 hours ago
Shocking news that the South Koreans already discovered and published back in May. Western
big pharma driven medicine is garbage 😂😂😂
Interesting play_arrow play_arrow Jack Mehoff 1 more time 9 hours ago
Business as usual play_arrow play_arrow Argon1 7 hours ago
Preparation for agenda 2021 in 2017. play_arrow 1 play_arrow CrabbyR 4 hours ago
WOW.......ties a few strands from other sources together into a real ugly picture play_arrow
play_arrow Welsh Bard 10 hours ago
The professor who won the Nobel prize for work in this field, said that the way this test is
being operated with over forty cycles, means that any results are entirely meaningless.
In Britain, having spent over £15 billion setting up PCR testing systems and a shaky
test and trace apparatus on top of that, it appears that 90% of positive results now appear to
be false. This is compounded by the fact that when a hot spot develops, more testing is done to
show a rapid increase in more false positive results, meaning further new lockdowns and even
more testing to prove yet more false positive results ad infinitum.
Now whether this is by design or ineptitude, people must decide for themselves but the
outcome is utter chaos.
For those countries who have not followed the Swedish model especially countries like
Australia and New Zealand who have set up complete isolation, now face a future perpetually cut
off from the rest of the world.
Okay, new techniques will and are coming along to treat the disease like HCQ when used
correctly maybe as a prophylactic and a vaccine that will need to be constantly upgraded like
the Flu vaccine, means that the whole world has painted itself into a corner unless drastic
revision is now made to the whole sorry mess.
In the meantime, we will now be stuck with digital currency and the introduction of ID
Health Cards that will limit people in how they travel where they work and access to a whole
heap of things like government services.
Welcome to the new world order! play_arrow 1 KuriousKat 11 hours ago (Edited) remove
link
Don't tell the Shameless Aussie gov that after arresting hundreds for simply voicing doubt
on need to lockdown entire city...Next time it will be thousands and not a damn thing they can
do to stop it..These people are trickling us the truth how worthless the tests are when pretty
much everyone knows. play_arrow espirit 12 hours ago remove link
Lessee.
WHO
Imperial College
John Hopkins
CDC
Line all those peeps up against the wall, and the first one to rat gets to live.
I'll provide my own ammo... ay_arrow Sick Monkey 6 hours ago
Not everyone working in these agencies are dishonest but like you and I we have to work and
eat.
Most of them are trapped in this mess with bills to pay threatened by NDA.
play_arrow 1 Urban Roman 12 hours ago
Not particularly new news. Been talked about since April at least -- it's an RNA virus, it
has its own polymerase, and it leaves lots of RNA fragments in its wake.
The Corona family of viruses make 5 or 6 strands with partial copies of their RNA molecule.
negative copies are made first, and then copied again into positive copies. Finally the one big
RNA is made with the entire genome on it.
So about a dozen RNA molecules are made for each finished virus particle that is produced.
And finally, a variety of different primers are used for the PCR tests, some are matched to the
small partial RNA copies and others are matched to various features on the large whole-virus
RNA. They can give different results for the same sample.
So, someone who registers on a PCR test has probably been exposed to the virus, but the test
gives no clue as to whether it is an active infection, or the person is contagious, or they are
just coming down with it, or they got over it six months ago. play_arrow 4 play_arrow 1
10 play_arrow gordo 12 hours ago remove link
Sweden, no masks, no lock downs, ALL SCHOOLS OPEN, herd immunity, no second wave.
Still think your masks and lock downs are working muppets?
1 play_arrow The 3rd Dimentia 13 hours ago
https://youtu.be/sjYvitCeMPc
SARS-CoV2 and the Rise of Medical Technocracy. Lee Merritt, M.D. play_arrow 3 play_arrow
hugin-o-munin 13 hours ago
I'm glad to see that many are starting to counter the official narrative.
We've been asleep for too long and allowed these agendas to fester to the point we're at now
where a college dropout software salesman and a former 3rd world communist terrorist (neither
of whom have any medical degree) are dictating to the world how everyone needs to get a DNA
altering vaccine and a medical ID. It's completely nuts and bonkers yet more or less the entire
planet's governments follow in 'lockstep' with ever more draconian laws and regulations
incarcerating people in their own homes, making them wear masks causing oxygen deprivation and
shutting down the entire world economy.
lay_arrow Warthog777 , 13 hours ago
Article is poorly written by someone who does not know medical science. There are no viral
"cells" so the headline is a put off right away. The comment about "sensitivity" is misplaced
as PCR tests are too sensitive: ergo false positives. I believe "specificity" is the word the
author was searching for. If a test lumps true positives with false positives, then it lacks
specificity.
Anyone who would use the term "virus cells", has no clue what they're talking about and
should be completely disregarded. Viruses are not cells. PCR tests are searching for
something your body produces in response to a virus as well. They are not produced
specifically for a singular virus either. The entire concept of PCR testing is garbage. This
**** was a scam from the get-go.
hugin-o-munin , 13 hours ago
Yes it is evident now that this entire pandemic is false and political. The goal seems to
be to vaccinate entire populations and the question people need to ask is - why? what for?
Aside from the obvious economic motives there are some more sinister plans that most people
will have a hard time accepting but these need to be looked at. Several years ago there were
a group of doctors and researchers that died of suspicious suicides who were collaborating
and studying vaccines and the link to autism.
The effort was led by Dr.Jeffrey Bradstreet who was researching the natural substance
GcMAF and how this could boost the immune system. What he discovered was that many vaccines
had a compound/substance called Nagalase in them that is unnatural and has a detrimental
effect on the immune system and function of GcMAF (which is produced by our own bodies) and
has no business at all being in vaccines. Just before he was able to blow the whistle on this
he also died of a suspicious 'suicide' and today most of the clinics and research groups
working on GcMAF have been destroyed and ruined. Draw your own conclusions.
snblitz , 14 hours ago
Dr. Kary Mullis invented the PCR test. He said it was ineffective for this purpose.
Though he was addressing its use in a prior virus hoax unleashed upon the world.
I bet you didn't know this scam has been used before.
That is why I was able to call out the scam right from the start. The second I saw them
using the PCR again, I knew it was from the same playbook.
snblitz , 14 hours ago
So many lies.
Viruses are not alive. They have no metabolic functions. They cannot move.
Don't believe me? Get a degree is virology or microbiology or just a read a book on the
subject. Or capture a wuhan-virus yourself and watch it under a microscope. It won't move. It
won't consume anything. It will just sit there inert.
The problem is that you are being lied to at a scale you cannot imagine.
I know, off to the fema re-education camp for me for spreading false information about the
wuhan-virus.
Though I am not the one spreading fear and hysteria.
aldousd , 13 hours ago
There article is confused, but the work of the doctor is not. Viruses use your cells to
reproduce. When your immune system targets the virus it actually kills your own cell which
has become host to the virus. The virus particles and markers, and the DNA of the virus can
be detected in these dead cells, but dead cells cannot serve as a factory for more viruses.
So it's effectively a dead virus infected cell. Not a dead virus cell.
So while the transcription of the idea here was done by an idiot, it's not an idiotic
idea. The tests cannot tell if the virus came in a living cell that is actively producing
more viruses or a dead host cell that has been assassinated by your immune system. That's
what they're talking about here.
mstyle , 11 hours ago
what about the chromosome 8 stuff that has been mentioned lately?
(since you appear to be rather intelligent)
hugin-o-munin , 11 hours ago
Thanks. Well the chromosome 8 discovery in the PCR test specifications/details is strange
and worrying because it makes you wonder why it's part of this at all. Some believe it's to
get more false positive results while others believe it is what the mRNA vaccines are
intended to target and if that's right then it's really sinister. What exactly is the plan?
To make all of us get Downs Syndrome? I don't know but judging by all their other lies and
schemes it wouldn't surprise me.
IRC162 , 14 hours ago
Fuggin progressives and their pandemic political prop. But really this reaction is the
same as their reaction to 'racial injustice'. They focus on feelings before the facts are
known in order to achieve their end, and then do their best to bury/ignore the facts when
they are gathered later.
94% COVID deaths with multiple comorbidities.
10 unarmed blacks killed by police in 2019 (6 were in self-defense).
adr , 15 hours ago
Why didn't you mention that nearly all labs are running 35-40 cycles which guarantees a
positive test, simply from noise.
The inventor of the test said if you don't find anything after 15 cycles, it probably
isn't there. After 20 cycles the noise starts to be greater than any real information. By 30,
the test is mostly noise. More than 35, the test is completely worthless.
Of course I've been saying this for five months, but most people didn't listen. After the
NYT article came out, people I know started saying, "How did you know?"
I said, "Because I have critical thinking skills. Why didn't you believe me? Name a time
I've steered you wrong."
Antiduck , 14 hours ago
333 labs in florida had 100% positivity. (stupid word.)
ZenStick , 12 hours ago
Exactly correct.
Nobody will touch this line of reasoning in public or on media.
Bastages.
Identify as Ferengi , 15 hours ago
See above, Born2Bwired.
The PCR test is not useful for what they are using it for apparently. This has been
known since the beginning. Here is quote regarding AIDS:
"Kary Mullis, who won the Nobel Prize in Science for inventing the PCR, is thoroughly
convinced that HIV is not the cause of "AIDS". With regard to the viral load tests, which
attempt to use PCR for counting viruses, Mullis has stated: "Quantitative PCR is an
oxymoron." PCR is intended to identify substances qualitatively, but by its very nature is
unsuited for estimating numbers. Although there is a common misimpression that the viral
load tests actually count the number of viruses in the blood, these tests cannot detect
free, infectious viruses at all; they can only detect proteins that are believed, in some
cases wrongly, to be unique to HIV. The tests can detect genetic sequences of viruses, but
not viruses themselves.
What PCR does is to select a genetic sequence and then amplify it enormously. It can
accomplish the equivalent of finding a needle in a haystack; it can amplify that needle
into a haystack. Like an electronically amplified antenna, PCR greatly amplifies the
signal, but it also greatly amplifies the noise. Since the amplification is exponential,
the slightest error in measurement, the slightest contamination, can result in errors of
many orders of magnitude."
The problem of false positives from Covid-19 tests means UK is inflating its numbers – and taking wrong decisions
Rob Lyons
Rob Lyons
is a UK journalist specialising in science, environmental and health issues. He is the author of '
Panic
on a Plate: How Society Developed an Eating Disorder'.
A sign is seen at a drive-through coronavirus disease
(COVID-19) testing facility in Hyde Park, following the outbreak of the coronavirus disease, London, Britain, June 11,
2020
When seven staff at a Scottish football club tested positive for coronavirus, alarm bells went off. But really alarming was
when six of those results turned out to be wrong. Such inaccurate tests are exaggerating the problem.
Last weekend, at very
short notice, the UK reintroduced quarantine measures for people arriving from Spain. For those already in Spain, or for whom
it was too late to postpone their trip, the decision is very inconvenient. For those who can't work at home when they return,
it may mean missing out on wages for the two weeks they will have to spend in isolation when they get back. But what if the
apparent rise in cases has been exaggerated by seemingly small flaws with testing?
The potential for problems
was illustrated by Scottish football team St Mirren last week. The club, based in Paisley, a town just west of Glasgow,
reported seven positive test results for Covid-19 among its staff. Alarm bells went off about what this might mean for the new
Scottish football season. But this
"cluster"
was a mirage. When the seven people
were re-tested using a more accurate method,
just
one
of them was found to be Covid-positive.
In Spain, half of the
reported
cases
have
been in people who had no symptoms. We know that many people who test positive never suffer any symptoms. But what if many of
these people don't have Covid-19 at all?
If that sounds
implausible, it's important to know that tests are not perfect. There are currently two kinds of tests to see if you have the
disease. One kind, the molecular real-time polymerase chain reaction (RT-PCR) test, looks for genetic material from the virus.
This kind seems to be very accurate, but it's expensive and time-consuming. The other kind, the antigen test, detects specific
proteins on the surface of the virus. This is quicker, easier and cheaper, but it's much less accurate. In developed
countries, RT-PCR testing is the norm, but poorer countries may have to make do with antigen testing.
The difficulty at the
moment is that there are relatively few cases of Covid-19 in the community, but more and more testing is being done. So even
if the RT-PCR test has a high
"specificity"
– that is, a tiny fraction of test
results are false positives – the number could actually be quite significant. For example, let's say that 99.9 percent of the
time, a test correctly identifies someone without the disease as negative. Just 0.1 percent of tests produce false positives.
Recently, in the UK, it
was estimated that 0.04 percent of people had the virus outside of care homes and hospitals. So, if we tested 10,000 people,
we should find four cases of Covid-19, on average. Of the 9,996 other people tested, in this hypothetical example, 0.1 percent
who don't have the virus would also test positive – that's 9.996 – in other words, 10 people. So, even if the test is very
accurate indeed, we could easily end up with four positive tests from people who really do have the virus and 10 false
positives from people who don't.
For any particular
individual, the chances of the test being a false positive is small. But when we look at the big picture, we could easily be
fooled into thinking that there are many more cases than there really are. Indeed, with a test accuracy of 99.9 percent, if
you tested a million people, none of whom actually had the disease, you would produce 1,000 positive results. And for tests
with less accuracy – as with St Mirren FC – the situation could be even worse.
The UK government has now
performed nearly 11 million tests. Could there be 11,000
"cases"
that are simply
a
mistake
? In turn, that means governments and other authorities might be introducing additional restrictions on people's
lives that are actually unnecessary.
The problem of false positives is much less significant when the disease really is in wide circulation. It doesn't change the
picture much for the period from mid-March through to the start of June. (In any event, in the UK at least, there was very
little testing capacity thanks to the jaw-dropping incompetence of bodies like Public Health England.)
Let's look at the latest
figures. On Sunday, July 26, for example, 142,954 tests were processed. Of these, 747 were found to be positive. If 0.1
percent of tests are false positives, we would expect 142 of those 747 positives to be false. If the test turns out to be
slightly less accurate – perhaps 'only' 99.5 percent accurate (which still seems very good), then 710, almost all the reported
positives, could be false.
We should also bear in
mind, when trying to assess the overall situation, that there will be some false negatives. There will also be people who
don't show symptoms who do have the virus and never get tested. But this understanding shows that we do need to be careful
about reading too much into every small blip in the number of cases. We should be particularly sceptical about imposing new
restrictions like mandatory quarantine. And if we rely solely on these tests, we could have the crazy situation where Covid-19
apparently never disappears, even when nobody has got it.
Think your friends would be
interested? Share this story!
Study identifies six different "types" of COVID-19
A new study of COVID-19 , based on
data from a symptom tracker app, determined that there are six distinct "types" of the disease involving different clusters of symptoms.
The discovery could potentially open new possibilities for how doctors can better treat individual patients and predict what level
of hospital care they would need.
Researchers from
King's College London
studied data from approximately 1,600 U.K. and U.S. patients who regularly logged their symptoms in the COVID Symptom Tracker App
in March and April.
Typically, doctors will look for
key symptoms
such as cough, fever and
loss
of the sense of smell to detect COVID-19. The study, which has not been peer-reviewed, says the six different "types" of COVID-19
can vary by severity and come with their own set of symptoms.
"I think it's very, very interesting," Dr. Bob Lahita, who is not affiliated with the study, told CBSN anchors Vladimir Duthiers
and Anne-Marie Green. "Among the patients I see, those who recovered, many of them present different ways: some people with fever
and some without fever, and some with
nausea and vomiting, some people with diarrhea , etc."
The six clusters of symptoms outlined in the study are:
Flu-like with no fever: Headache, loss of smell, muscle pains, cough, sore throat, chest pain, no fever.
Flu-like with fever: Headache, loss of smell, cough, sore throat, hoarseness, fever, loss of appetite.
Gastrointestinal: Headache, loss of smell, loss of appetite, diarrhea, sore throat, chest pain, no cough.
Severe level one, fatigue: Headache, loss of smell, cough, fever, hoarseness, chest pain, fatigue.
Severe level two, confusion: Headache, loss of smell, loss of appetite, cough, fever, hoarseness, sore throat, chest
pain, fatigue, confusion, muscle pain.
Severe level three, abdominal and respiratory: Headache, loss of smell, loss of appetite, cough, fever, hoarseness,
sore throat, chest pain, fatigue, confusion, muscle pain, shortness of breath, diarrhea, abdominal pain.
The first level, "flu-like with no fever," is associated with headaches, loss of smell, muscle pains, cough, sore throat and chest
pain. Patients at this level have a 1.5% chance of needing breathing support such as oxygen or a ventilator.
The second type, "flu-like with fever," includes symptoms like loss of appetite, headache, loss of smell, cough, sore throat,
hoarseness and fever. Researchers say about 4.4% of patients at this level needed breathing support.
Patients with the third type, simply described as "gastrointestinal," do not have a cough as part of their illness. Instead, they
experience headache, diarrhea, loss of smell, loss of appetite, sore throat and chest pain, and about 3.3% needed breathing support.
Lahita referred to the following three clusters of COVID-19 as the "really severe types."
In type four, or "severe level one," patients experience fatigue along with headache, loss of smell, cough, fever, hoarseness
and chest pain. Patients at this level needed breathing support at a rate of 8.6%.
Type five, "severe level two," includes the symptoms of type four along with loss of appetite, sore throat and muscle pain, and
is mainly distinguished by
confusion
.
"That means you don't know where you are or where you live, whether you are in or out of the hospital, who your relatives are,"
Lahita explained. "That is very scary." Almost 10% of patients at that level need breathing support.
The most severe type of COVID-19 is referred to as "severe level three, abdominal and respiratory," and has all the above symptoms
along with abdominal pain, shortness of breath and diarrhea. Nearly 20% of these patients need breathing support.
"Those are the severe level threes who wind up on a ventilator, and then it is touch-and-go as to whether they survive the
infection entirely," Lahita said.
The U.K. researchers also found that only 16% of patients with type one COVID-19 required hospitalization, compared with nearly
half of the patients with type six.
Patients in the severe clusters also tended to be older or with pre-existing conditions and weakened immune systems, compared
to those in the first three.
Scientists hope the discovery, once further studied, could help predict what types of care patients with COVID-19 might need,
and give doctors the ability to predict which patients would fall into which category.
"I'm very happy that these six types have been identified and can give us an idea of a prognosis going forward for patients who
are afflicted with this virus," Lahita said.
By Dr. Sherri Tenpenny – May 21, 2020 – an osteopathic medical doctor,
board-certified in three specialties. She is the founder of Tenpenny Integrative Medical Center, a medical clinic located
near Cleveland, Ohio. Her company, Courses4Mastery.com provides online education and
training regarding all aspects of vaccines and vaccination.
_____________________________
In 1965, scientists identified the first human coronavirus; it was associated with the
common cold. The Coronavirus family, named for their crown-like appearance, currently includes
36 viruses.
Within that group, there are 4 common viruses that have been causing infection in humans for
more than sixty years. In addition, three pandemic coronaviruses that can infect humans: SARS,
MERS, and now, SARS-CoV-2.
As the news of deaths in China, South Korea, Italy, and Iran began to saturate every form of
media 24/7, we became familiar with a new term: COVID-19. To be clear, the name of the newly
identified coronavirus is SARS-CoV-2, short for Severe Acute Respiratory Syndrome
Coronavirus-2. This virus is associated with fever, cough, chest pain, and shortness of breath,
the complex of symptoms that form the diagnosis of COVID-19.
The Trump administration declared a public health emergency on January 31, 2020, then on
February 2 placed a ban on the entry of most travelers who had recently been in China. On
February 4, Alex Azar, the Secretary of Health and Human Services (HHS) issued a declaration of
public health emergency and activated the Public Readiness and Emergency Preparedness Act,
otherwise known as the PREP
Act. This nefarious legislation provides complete protection of manufacturers from
liability for all products, technologies, biologics, or any vaccine developed as a medical
countermeasure against COVID-19. For those nervously waiting for the vaccine to become
available, be sure to understand the PREP Act
before rushing to the get in line.
Calls for testing – to see if a person is or isn't infected – began soon after
the emergency was declared, but performing those tests was initially slow due to an inadequate
number of test kits. As the kits became available, those
developed by the CDC had a defect: The reagents reacted to the
negative control sample , making the test inaccurate and the kits unusable.
In various
countries, thousands of test kits purchased from China were found to be contaminated with
the SARS-CoV-2 viruses. No one really knows how that happened, but theories spread like
wildfire. Could the test kit infect the person being tested? Or, did it mean the test would
return a false-positive result, driving up the numbers of those said to be infected so those in
power could implement stronger lockdowns and accelerate the hockey-stick unemployment rates?
Neither of those questions has been adequately answered.
Mandatory Testing of what?
Authorities claim that testing is important for public health officials to assess if their
mitigation efforts – "shelter in place" and "social distancing" and "wearing a mask"
– are making a difference to "flatten the curve." Officials also claim that testing is
necessary to know how many persons are infected within a community and to understand the nature
of how coronaviruses spread.
Are these reasons sufficient to give up our health freedom and our personal rights, being
tested and shamed in public?
Despite the challenges with test kits, testing began. By the end of March 2020, more than 1
million people had been tested across the US. By May 9, the number tested had grown to over
8.7M. Testing methods include a swab of the
nasal passages or by inserting a long, uncomfortable swab through the nose to scrape the back of the
throat. Specimens have also been obtained bronchoalveolar lavage, from
sputum , and from stool
specimens.
The call for mandatory testing has been gathering steam and becoming ever more onerous. In
Washington state, Governor Inslee
has declared:
Individuals that refuse to cooperate with contact tracers and/or refuse testing, those
individuals will not be allowed to leave their homes to purchase basic necessities such as
groceries and/or prescriptions. Those persons will need to make arrangements through friends,
family, or state provided 'family support' personnel .
But what do the results really mean?
Who Should Be Tested
On May 8, 2020, the CDC has listed specific priorities
for when testing should be done. As of May 16, more than 11-million samples have been
collected and more than 3700 specimens have not yet been evaluated.
High Priority
Hospitalized patients with symptoms
Healthcare facility workers, workers in living settings, and first responders with
symptoms
Residents in long-term care facilities or other congregate living settings, including
prisons and shelters, with symptoms
Priority
Persons with symptoms of potential COVID-19 infection, including fever, cough, shortness
of breath, chills, muscle pain, new loss of taste or smell, vomiting or diarrhea, and/or sore
throat
Persons without symptoms who are prioritized by health departments or clinicians
, for any reason, including but not limited to public health monitoring, sentinel
surveillance, or screening of asymptomatic individuals according to state and local
plans.
Read that last priority again: That means virtually everyone can be required to get a
test.
Is that a violation of your personal rights? And, if you submit to testing, what does a
"positive test" actually mean?
Types of Testing: RT-PCR
PCR, short for polymerase chain reaction , is a highly specific laboratory technique. The
key to understanding
PCR testing is that PCR can identify an individual specific virus within a viral
family.
However, a PCR test can only be used to identify DNA viruses; the SARS-CoV2 virus is an RNA
virus. Therefore, multiple steps must be taken to "magnify" the amount of genetic material in
the specimen. Researchers used a method called RT-PCR, reverse transcription-polymerase chain
reaction, to specifically identify the SARS-CoV-2 virus. It's a complicated process. To read
more about it, go
here and here.
If a nasal or a blood sample contains a tiny snip of RNA from the SARS-CoV-2 virus, RT-PCR
can identify it, leading to a high probability that the person has been exposed to the
SARS-CoV-2 virus.
However – and this is important – a positive RT-PCR test result does not
necessarily indicate a full virus is present. The virus must be fully intact to be
transmitted and cause illness.
RT-PCR Testing: The Importance of Timing
Even if a person has had all the symptoms associated with a coronavirus infection or has
been closely exposed to persons who have been diagnosed with COVID-19, the probability of a
RT-PCR test being positive decreases with the number of days past the onset of symptoms.
For a nasal swab, the percentage chance of a positive test declines from about 94% on day
0 to about 67% by day 10. By day 31, there is only a 2% chance of a positive result.
For a throat swab , the percentage chance of a positive test declines from about 88% on
day 0 to about 47% by day 10. By day 31, there is only a 1% chance of a positive result.
In other words, the longer the time frame between the onset of symptoms and the time a
person is tested, the more likely the test will be negative.
Repeat testing of persons who have a negative test may (eventually) confirm the presence of
viral RNA, but this is impractical. Additionally, repeated testing of the same person can lead
to even more confusing results: The test may go from negative, to positive, then back to
negative again as the immune system clears out the coronavirus infection and moves to
recovery.
And what makes this testing even more confusing is that the
FDA admits that "The detection of viral RNA by RT-PCR does not necessarily equate with an
infectious virus."
Let's break that down:
You've had all the symptoms of COVID19, but your RT-PCR test for SARS-CoV-2 is
negative.
Does that mean you're "good to go" – you can go to work, go to school or you can
travel? OR
Does that mean your influenza-like illness was caused by some other pathogen, possibly
one of the four coronaviruses that have been in circulation for 60 years? OR
Does that mean the result is a false-negative and you still have the infection, but it
isn't detectable by current tests? OR
Does that mean it was a sample was inadequately taken due to the faulty technique by the
technician? OR
Does that mean you have not been exposed, and you are susceptible to contracting the
infection, and you need to stay in quarantine?
So, what does a "positive" test actually mean? And that's the problem:
No one knows for sure.
Another Type of Testing: Antibodies
According to the nonprofit Foundation for Innovative New Diagnostics
(FIND) , more than 200 serologic blood tests, to test for antibodies, are either now
available or in development.
There are two primary types of antibodies that are assessed for nearly any type of
infection: IgM and IgG. While several new testing devices are being touted as a home test, they
are not the same as a home pregnancy test or a glucometer to you're your blood sugar. The blood
spot or saliva specimen can be collected at home, must it must then be sent to a laboratory for
analysis. It can take a few days – or longer – to get the results. With so many
tests in the pipeline, the ability to test at home will be changing over time.
The first antibody to rise is IgM. It rises quickly after the onset of the infection and is
usually a sign of an acute, or current, infection. The IgM levels diminish quickly as the
infection resolves. The
FDA admits they do not know how long the IgM remains present for SARS-CoV-2 as the
infection is being cleared.
The interpretation of an IgG antibody is more difficult. This antibody is an indicator of a
past infection. The test is often not specific enough to determine if the past infection was
caused by the SARS-CoV-2 virus or one of the four common coronaviruses that cause
influenza-like illness.
Because serology testing can yield a negative test result even if the patient is actively
infected (e.g., the body has not yet developed in response to the virus) or maybe falsely
positive (e.g., if the antibody indicates a past infection by a different coronavirus), this
type of testing should not be used to diagnose an acute or active COVID-19 infection.
Similarly, the CDC says the
following regarding antibody testing:
If you test positive:
A positive test result shows you have antibodies as a result of an infection with
SARS-CoV-2, or possibly a related coronavirus.
It's unclear if those antibodies can provide protection (immunity) against getting
infected again. This means that we do not know at this time if antibodies make you immune
to the virus.
If you have no symptoms, you likely do not have an active infection and no additional
follow-up is needed.
It's possible you might test positive for antibodies and you might not have or have
ever had symptoms of COVID-19. This is known as having an asymptomatic infection [ie you
have a healthy immune system!]
An antibody test cannot tell if you are currently sick with COVID-19.
If you test negative
If you test negative for antibodies, you probably did not have a previous infection.
However, you could have a current infection because antibodies don't show up for 1 to 3
weeks after infection.
Some people may take even longer to develop antibodies, and some people may not
develop antibodies.
An antibody test cannot tell if you are currently sick with COVID-19.
What? Wait!
Doesn't the vaccine industry call the IgG a "protective antibody"?
Isn't this the marker of immunity they assess after you've had an infection with measles
or chickenpox or mumps to determine if you are immune to future infections?
Isn't this the marker of induced immunity they are trying to achieve by administering a
vaccine?
If the FDA does not know if an IgG antibody to SARS-CoV-2 after recovering from the
infection is protective against a future infection, then they certainly don't know if an
antibody caused by a vaccine will prevent infection either.
Doesn't this completely eliminate the theory that antibodies afford protection and
antibodies from vaccines are necessary to keep you from getting sick?
Until we have a vaccine to defeat this dreaded disease, contact tracing in order to
understand the full breadth and depth of the spread of this virus is the only way we will be
able to get out from under this.
H.R.6666 would authorize the Secretary of Health and Human Services (HHS), acting through
the Director of the CDC to award grants to eligible entities to conduct diagnostic testing and
then to trace and monitor the contacts of infected individuals. The contact tracers would be
authorized to test people in their homes and as necessary, quarantine people in place.
Where do they intend to do this testing? Besides mobile units to test people in their homes,
the bill identifies eight specific locations where the testing and contract tracing could
occur: schools, health clinics, universities, churches, and "any other type of entity" the
secretary of HHS wants to use.
The bill would allocate $100 billion in
2020 "and such sums as may be necessary for fiscal year 2021 and any subsequent fiscal year
during which the emergency period continues."
But what are they looking for?
Is your test supposed to be positive – saying you've been exposed and you've
possibly recovered?
Or is your test supposed to be negative , meaning, you are healthy?
Or does a completely negative test – negative RT-PCR test and no IgG antibody mean
you're susceptible to infection and you need to stay in quarantine?
The virus is rapidly mutating, which is rather typical of RNA viruses. In a
study published in April 2020, researchers have discovered that the novel coronavirus has
mutated into at least 30 different genetic variations. If your RT-PCR test is positive, does
this identify exposure to the pandemic virus or exposure to one of the genetic variations? The
same can be said about the vaccines under development: With each mutation, is the vaccine more
likely to be all risk and no benefit when it reaches the market?
What You Can Do
Across the nation, police are being told to not apprehend criminals but instead, to arrest
parents at playgrounds, to arrest lone surfers on public beaches, to fine ministers and
congregation members sitting in their cars listening to a service on the radio, and to restrict
movement by creating one-way sidewalks.
People have had enough. They are beginning to see the huge scam that has been perpetrated on
the entire world over a viral infection with a global death rate of
1.4% (meaning, 1.4% of people infected with SARS-CoV-2 have a fatal outcome, while 98.6%
recover). This is far fewer deaths than a severe flu season.
We're already starting to see the thrust to take our power back:
In Virginia, people went to the beaches en mass,
ignoring social distancing and the orders of the Governor to stay home.
The central California city of Atwater has declared itself a "sanctuary
city," allowing business owners and churches to open, openly defying Democratic
California
Gov. Gavin Newsom's coronavirus-related stay-at-home order.
The truth about wearing
masks is starting to come out and people are voting with their feet. Retired
neurosurgeon, Dr. Russell Blaylock, warns that not only do face masks fail to protect healthy
people from contracting an illness, but they create serious health risks to the wearer.
While they shut us down and held us hostage in our homes, they changed our society, our
lives, our world.
I am not willing to accept this is the "new normal."
I won't submit to testing.
I will refuse mandatory vaccination.
I will stop wearing a mask.
I will not be afraid of standing next to a friend or family member and will not obey the
concept of "social distancing."
I will understand that an asymptomatic carrier is a normal, healthy person and I will not
buy into the fear that I might "catch something" from a normal, healthy person.
It's time for Americans to resist with non-violent civil disobedience. Be brave. Be bold.
Put on the full armor of God, as found in Ephesians
6:10-20 in the Bible, to stand against the world rulers of this present darkness. With God
on our side, all things are possible.
*
Note to readers: please click the share buttons above or below. Forward this article to your
email lists. Crosspost on your blog site, internet forums. etc.
"The current work suggests that while the G614 variant may be more infectious, it is not
more pathogenic. There is a hope that as SARS-CoV-2 infection spreads, the virus might become
less pathogenic,"
WHO now says asymptomatic spread of coronavirus is 'very rare'
Jun. 09, 2020 - 4:06 - World Health Organization changes its tune on asymptomatic patients
spreading COVID-19; reaction from Fox News medical contributor Dr. Marc Siegel.
Although numerous studies have suggested people can spread the virus before they show
symptoms, the WHO has largely dismissed those as anecdotal or pointed out that they were
based on modelling.
Babak Javid, an infectious diseases doctor at Cambridge University Hospital, says many
scientists are persuaded by the studies published so far and think WHO should publish the
data it is citing to explain why it believes transmission of the disease in people without
symptoms is "rare".
"If you're going to make a really important statement like that, it would be good to
back it up," Javid said. "I think WHO is an important organisation, but they've made a lot
of statements that have been misleading."
Try doing a search on Kary Mullis, creator of the PCR process. He died last year so we can
only go by past statements. He always stated that PCR was completely inappropriate and
meaningless for diagnostics or for any other clinical purpose.
CDC guidance on PCR until earlier this year was that doctors do diagnosis, not
laboratories. Doctors were allowed to consider PCR results as a factor, cautioned not to rely
on them. In current situation PCR results are the definition of COVID.
If the test is allowed to run too many cycles any sample will test positive.
And it is never entirely certain how many cycles have elapsed, clock does not tell exactly
what the RNA is up to.
"... According to the Mayo Clinic, a normal pulse oximeter oxygen level reading is between 95% and 100% , and anything less than 90% is considered dangerously low, or hypoxic. Some doctors have reported COVID-19 patients entering the hospital with oxygen levels at 50% or below . ..."
Some doctors are recommending these small, inexpensive devices to help monitor
symptoms.
A pulse oximeter attaches to a finger and uses light to detect the level of oxygen in your blood.
As
coronavirus
testing efforts
continue to ramp up and
face masks
are now a part of everyday life, a small diagnostic tool that clips to the tip of your
finger is fast becoming a must-have gadget in the
fight
against the coronavirus
. It's called a pulse oximeter, and it painlessly checks your blood oxygen
level, which can be affected by lung diseases such as COVID-19.
The device was already starting to surge in popularity as word got around
that people with the
coronavirus
frequently
arrive
at the hospital with abnormally low oxygen levels
. After an
op-ed
piece in The New York Times
recommended the use of pulse oximeters to detect a frightening
condition called "silent hypoxia," sales of the devices
skyrocketed
.
Many models are sold out or on lengthy backorder online. Same with brick-and-mortar drug stores,
supermarkets and box stores.
The latest round of 'surveillance' testing for coronavirus antibodies was
done on first responders, and found that the number who tested positive was once again
surprisingly high.
For the past few weeks, more than 50 scientists have been working diligently to do something
that the Food and Drug Administration mostly has not: Verifying that 14 coronavirus
antibody tests now on the market actually deliver accurate results.
These tests are crucial to reopening the economy, but public health experts have raised
urgent concerns about their quality. The new research, completed just days ago and posted
online Friday, confirmed some of those fears: Of the 14 tests, only three delivered consistently reliable results . Even the
best had some flaws.
The research has not been peer-reviewed and is subject to revision. But the results are
already raising difficult questions about the course of the epidemic.
Surveys of residents in the Bay Area, Los Angeles and New York this week found that
substantial percentages tested positive for antibodies to SARS-CoV-2, the official name of the
new coronavirus. In New York City, the figure was said to be as high as 21 percent. Elsewhere,
it was closer to 3 percent.
The idea that many residents in some parts of the country have already been exposed to the
virus has wide implications. At the least, the finding could greatly complicate plans to reopen
the economy.
Already Americans are scrambling to take antibody tests to see if they might escape
lockdowns. Public health experts are wondering if those with positive results might be allowed
to return to work.
But these tactics mean nothing if the test results can't be trusted.
In the new research, researchers found that only one of the tests never delivered a
so-called false positive -- that is, it never mistakenly signaled antibodies in people who did
not have them.
Two other tests did not deliver false-positive results 99 percent of the time. But the
converse was not true. Even these three tests detected antibodies in infected people only 90
percent of the time, at best.
The false-positive metric is particularly important. The result may lead people to
believe themselves immune to the virus when they are not, and to put themselves in danger by
abandoning social distancing and other protective measures.
It is also the result on which scientists are most divided.
"There are multiple tests that look reasonable and promising," said Dr. Alexander Marson, an
immunologist at the University of California, San Francisco, and one of the project's leaders.
"That's some reason for optimism."
Dr. Marson is also an investigator in the Chan Zuckerberg Biohub, which partly funded the
study.
Other scientists were less sanguine than Dr. Marson. Four of the tests produced
false-positive rates ranging from 11 percent to 16 percent; many of the rest hovered around 5
percent.
"... By JoNel Aleccia, Senior Correspondent at Kaiser Health News, who previously reported for The Seattle Times, NBCNews.com, TODAY.com and MSNBC.com. Originally published at Kaiser Health News ..."
By JoNel Aleccia, Senior Correspondent at Kaiser Health News, who previously reported
for The Seattle Times, NBCNews.com, TODAY.com and MSNBC.com. Originally published at
Kaiser Health News
After hearing for months about serious access issues involving tests that diagnose COVID-19
based on swabs from the nose or throat, Americans are being inundated with reports about
promising new tests that look for signs of infection in the blood.
There are high hopes for these antibody tests, which detect proteins that form in blood as
part of the body's immune response to an invading virus. Communities across the U.S. have been
rolling out the results of serological surveys that examine blood samples from people who
haven't been diagnosed with COVID-19 to see if they were, in fact, previously infected.
The thinking is, if there are blood markers that can detect when people have been infected,
such tests should be able to tell us how widely the novel coronavirus has spread. And equally
optimistic: those same antibodies could convey immunity to the disease, signaling someone is
safe from reinfection and able to get back to work.
Such high hopes, however, are running smack into the roadblocks of reality.
Infectious disease experts are raising pointed questions about the reliability of the early
tests and the studies that hinge on their results. And they warn that state and local
governments -- as well as individuals -- should be wary of shaping policy or changing behavior
based on any single report.
In the sharpest caution to date, officials with the World Health Organization on Saturday
warned against plans for proposed "immunity passports," which would allow people who have
recovered from the coronavirus to resume unrestricted travel and work.
"There is currently no evidence that people who have recovered from COVID-19 and have
antibodies are protected from a second infection," the agency wrote in a scientific brief.
Even before the WHO weighed in, other experts were urging restraint in interpreting early
results of antibody screening.
"The science is catching up," said Dr. Liise-anne Pirofski, chief of the division of
infectious diseases at the Albert Einstein College of Medicine and Montefiore Health System.
"Our ability to make a test at the moment is much greater than our understanding of what those
antibodies we are testing for mean."
In the past few weeks, more than 180 academic centers, hospitals and private manufacturers
have notified the federal Food and Drug Administration that they intend to create serology
tests for COVID-19, spokesperson Stephanie Caccomo said in an email. They've been able to jump
into the fray because the FDA in March
relaxed regulations for developing tests as part of its emergency response to the
pandemic.
But the FDA has not reviewed the vast majority of tests on the market, and their validity,
particularly point-of-care blood tests that promise rapid results within minutes, isn't clear,
said Dr. Michael Busch, director of the Vitalant Research Institute and a professor of
laboratory medicine at the University of California-San Francisco.
"Some of them have sensitivities that are quite poor," he said. "You may even miss some
infected people completely."
Other tests may flag people as positive for COVID-19 when they're not infected. That's
especially true in regions of the country with little spread of the novel virus. If the
prevalence of a disease is low, less than 5%, even an accurate test would yield a high number
of false positive results because of the way such screening tools operate.
So when people see advertisements for finger-prick antibody tests becoming widely available
at urgent care centers and medispas, they should think twice.
For one, antibody tests can't be used to diagnose the disease. Antibodies may not be present
in high enough levels to be detected in the earliest days of an infection. And because there
are several other known coronaviruses -- including those that cause the common cold -- people
infected with those viruses could produce antibodies that cross-react with those produced in
response to the new virus.
Scientists still know too little about whether antibodies to COVID-19 convey immunity that
could allow people to put away masks and halt social distancing, said Dr. Mary Hayden, director
of the division of clinical microbiology at Rush University Medical Center in Chicago.
Immunity to a virus is a complicated process that takes place over one to two weeks, the WHO
noted. The immune system makes antibodies in response to an infection. But the body also makes
T-cells that recognize and eliminate other cells infected with the virus, creating what's known
as cellular immunity. Those two processes together may help a person recover and prevent
reinfection. But it is not yet clear whether cellular immunity is required to bolster recovery
and prevent subsequent infection with COVID-19.
"We do not know whether or not the antibodies detected are protective," Hayden told
reporters last week on a call organized by the
Infectious Diseases Society of America . "We recommend that people with antibodies not
change their behavior in any way."
Scientists are hoping, however, that future COVID-19 studies may demonstrate immunity that
could last for one or two years.
Concerns about the validity of the tests have cast a shadow on several recent reports aiming
to quantify the spread of the virus in specific regions. Last week, New York Gov. Andrew Cuomo
revealed the results of a serological survey that suggested that 1 in 5 New
York City residents had been infected with the coronavirus. Statewide, the figure was
13.9%, according to the study of 3,000 New Yorkers in 19 counties who were recruited at grocery
stores.
But the results quickly drew criticism. Dr. Demetre Daskalakis, who directs the city's
disease control, warned that the tests could produce
"false negative or false positive results. " Florian Krammer, a microbiology professor at
the Icahn School of Medicine at Mount Sinai who designs such tests, tweeted -- and later
deleted -- that the results were "BS."
"I think this is too high," he said in a later tweet. "It is
possible. But a 20% plus infection rate seems too high for NYC due to a number of reasons. I
would think 6-8%, maybe 10% are closer to the truth. It would be nice to know more about the
test, its sensitivity and specificity and the test population."
Similarly, two serology studies in California, one in Santa Clara County and one in Los
Angeles County, drew wide criticism about the recruitment of subjects and the analyses
used.
In the Santa Clara study ,
Stanford University researchers tested 3,330 volunteers for antibodies showing exposure to
COVID-19; about 1.5% were positive. They concluded that meant from 48,000 to 81,000 people were
infected with the virus in the county.
"It was completely inadequate to interpret the results that 50,000 to 80,000 people were
infected," Busch said.
The L.A. study, conducted by University of Southern California researchers, concluded that
2.8%
to 5.6% of the county's adult population had been exposed to the coronavirus. That
translates to 221,000 to 422,000 adult residents who have been infected. Critics, however,
argued that the study sample was too small and that details of the methodology weren't
immediately available.
Busch understands the drive to conduct such tests.
"People are asking the questions: What's the real denominator to judge the case counts and
the death counts against?" he said. "People are urgently trying to get data."
Unfortunately, that data simply is not available yet, other experts said. This coronavirus
has never been seen before, so the science that will inform efforts to help communities respond
and recover is playing out in real time.
"The problem is that the science has not kept up with the tests," Hayden said. "Now we need
to do the research to tell what the results mean."
On the positive side, most of the scientific community has pivoted to focus on finding
solutions, said Pirofski, who was also on the IDSA call. "We just have to slow our roll."
"This is our first dive in trying to understand what's going on," she said. "I would say
it's a start."
"(A PCR test) detects viral genetic code that does not exist in the human body otherwise," Cioe-Pena explained. "They're
sensitive to the point where it will even detect fragments," which can mean that someone who was sick but then recovered could
still test positive, he said.
The Last but not LeastTechnology is dominated by
two types of people: those who understand what they do not manage and those who manage what they do not understand ~Archibald Putt.
Ph.D
FAIR USE NOTICEThis site contains
copyrighted material the use of which has not always been specifically
authorized by the copyright owner. We are making such material available
to advance understanding of computer science, IT technology, economic, scientific, and social
issues. We believe this constitutes a 'fair use' of any such
copyrighted material as provided by section 107 of the US Copyright Law according to which
such material can be distributed without profit exclusively for research and educational purposes.
This is a Spartan WHYFF (We Help You For Free)
site written by people for whom English is not a native language. Grammar and spelling errors should
be expected. The site contain some broken links as it develops like a living tree...
You can use PayPal to to buy a cup of coffee for authors
of this site
Disclaimer:
The statements, views and opinions presented on this web page are those of the author (or
referenced source) and are
not endorsed by, nor do they necessarily reflect, the opinions of the Softpanorama society.We do not warrant the correctness
of the information provided or its fitness for any purpose. The site uses AdSense so you need to be aware of Google privacy policy. You you do not want to be
tracked by Google please disable Javascript for this site. This site is perfectly usable without
Javascript.
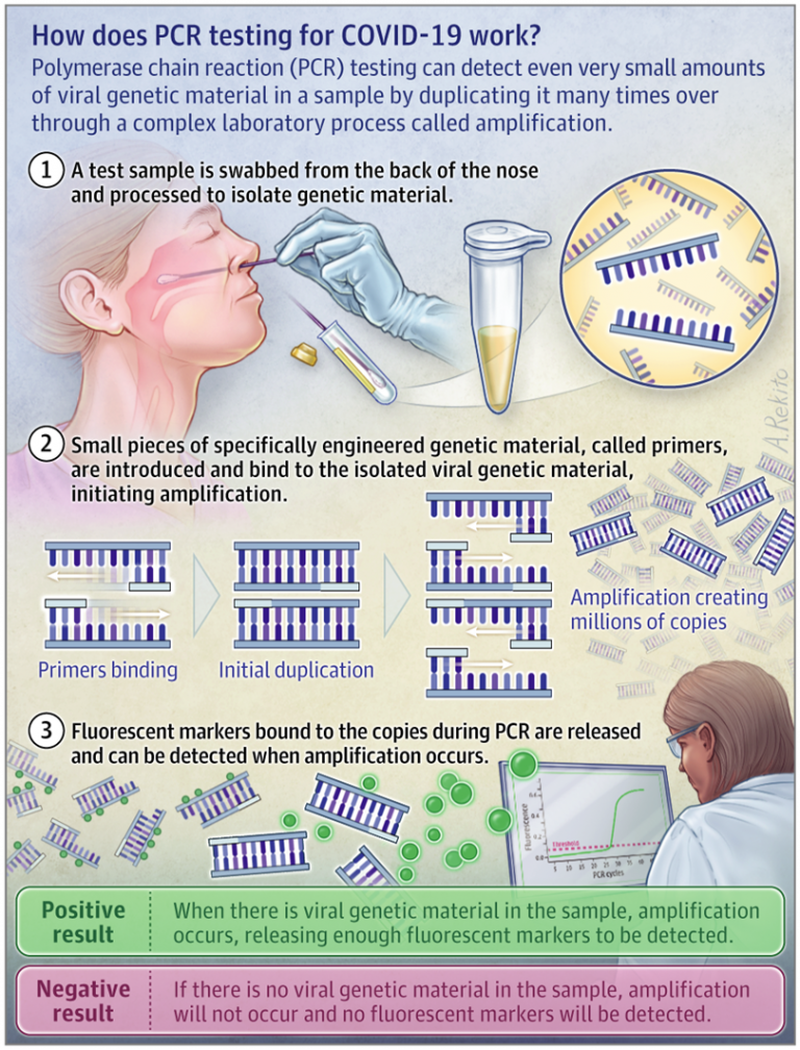
A
Immunity for YEARS or DECADES: Covid resistance may last much longer than previously thought, says new research
I'm an epidemiology professor and I have some genuine concerns about the AstraZeneca Covid vaccine. Here's why Sshhh – don't tell anyone
2327
FILE PHOTO © Global Look Press / Frank Hoermann / SVEN SIMON 66 Follow RT on
Over a half of coronavirus infections revealed this summer by one of Belgium's biggest labs were old and no longer contagious, but were still reported as new cases, local media discovered.
97,209


I'd only add that the virus was clearly "circulating" well before the Wuhan outbreak in late December 2019.
We don't know how many people contracted the virus in November, December 2019 and January and February 2020. But this number is certainly much larger than we have been told ... And plenty of government officials and public health authorities MUST know this.
I agree with this story. I do believe there will be a cycle count decrease corresponding to the mask mandate and the vaccine rollout. The entire Covid-19 from top to bottom is a political system having nothing to do with medical science.
I'm surprised Fauci admitted to high PCR enough counts leading to zero accuracy like here: https://twitter.com/jimgris/status/1326518250386063361
Err... Any chance now the WHO consider and approve the RT-PCR peer review published by 22 world-renowned scientists last November and revealing no less than 10 major scientific flaws in the Corman-Drosten RT-PCR test recommended in January 2020 by medical journal Eurosurveillance? 10 major flaws that make that PCR test totally useless for the diagnostic of covid.
To the peer review is also joined a letter with a request to Eurosurveillance to retract that article and recommendation of January 2020.
The whole pandemic was based on that PCR testing. And Covid disappeared in China only when they decided to stop testing. A corollary is that it magically 'reappears' whenever they start testing again...Go figure.
https://cormandrostenreview.com/report/